Embed Size (px)
Citation preview

COMPENDIUM
NCMDM BASIC COURSE FOR SEAFARERS’ DOCTORS
Compiled date Revision No. Revised date
2014 13 16.10.2018
Document name GK SL E Compendium
2
1 CONTENTS
1 Contents 2 2 Preface 6 3 introduction ....................................................................................................................................... 6
3.1 Learning outcomes ................................................................................................................ 6 4 Course overview ................................................................................................................................ 7
4.1 Distance learning at home including pre course test ............................................................ 7 4.2 A three day taught course with final test .............................................................................. 8
4.2.1 Syallbus ................................................................................................................................ 8 4.3 Final test ................................................................................................................................. 9 4.4 After completion of the course.............................................................................................. 9 4.5 Evaluation of the course and information to authorities ...................................................... 9 4.6 Qualification after successful completion of this course ....................................................... 9
5 references 10 5.1 International conventions of importance to this course ..................................................... 10 5.2 International guidelines of importance to this course ........................................................ 10 5.3 Norwegian legislation of importance to this course ............................................................ 10 5.4 Guidance to the regulations ................................................................................................ 10 5.5 Supplementary reading ....................................................................................................... 10
6 Topic 1: The shipping industry and working at sea ......................................................................... 11 7 Topic 2: Medical treatment possibilities at sea ............................................................................... 11
7.1 the International Legal Basis for providing medical care at sea .......................................... 11 7.2 Access to medical care at sea .............................................................................................. 11
7.2.1 Ships without a doctor ...................................................................................................... 11 7.2.2 Ships that carry a doctor ................................................................................................... 12 7.2.3 Availability of medical advice – Telemedical Maritime Assistance Service (TMAS).......... 13 7.2.4 Medical evacuation - MEDEVAC ........................................................................................ 13
8 Topic 3A: Regulations of 5 June 2014 No 805 on medical examination of employees on Norwegian Ships and mobile offshore units ................................................................................... 14
9 Topic 3B: Guidance to regulations on the medical examination of employees on Norwegian ships and mobile offshore units ............................................................................................ 14
10 Topic 3C: use of a web-based system for issuANCE OF medical certificates and declarations of unfitness ....................................................................................................................... 15
10.1 the online registration system ............................................................................................. 15 10.2 How to get access to the online system .............................................................................. 15 10.3 completing the medical certificate and declaration of unfitness ........................................ 16
11 Topic 3D – Organization of the Norwegian Health Service and the Health Personnel Act ............. 16 11.1 Norwegian Health Service Organization .............................................................................. 16
11.1.1 Hospitals and specialist service ......................................................................................... 16 11.1.2 General Practice ................................................................................................................ 17 11.1.3 HEALTH SUPERVISION .................................................................................................. 17
11.2 THe Norwegian Health Personnel Act ................................................................................. 17

3
11.3 Objective and scope of the HPA – Article 1 and 2 ............................................................... 18 11.4 Responsible conduct – Article 4 ........................................................................................... 18 11.5 the Issuing of certificates ..................................................................................................... 18 11.6 Other provisions of the HPA ................................................................................................ 19
12 Topic 3E: Approval procedures, quality system requirements, risk based audit of approved doctors ......................................................................................................................... 19
12.1 Approval as a NMA Approved Seafarers’ Doctor and the doctor’s obligations .................. 19 12.1.1 A BASIC course FOR SEAFARERS’ DOCTORS APPROVED BY THE NMA has to be completed
20 12.2 Quality system requirements for approved seafarers’ doctors........................................... 20
13 More information on what should be included in a quality system is provided in the Guidance.Topic 4: Norwegian Public administration procedures ............................... 20
13.1 Introduction ......................................................................................................................... 20 13.1.1 Scope of the Act ................................................................................................................ 21 13.1.2 “Individual decisions” ........................................................................................................ 21
13.2 The rights of the seafarer and the obligations of the seafarer’s doctor according to the Public Adminsitration Act (PAA) .......................................................................................... 21
13.2.1 Conflicts of interest – Article 6 of the PAA ........................................................................ 21 13.2.2 Duty to provide guidance – Article 11 of the PAA............................................................. 21 13.2.3 Rights for the seafarer to be assisted by an agent – Article 12 of the PAA ...................... 22 13.2.4 Duty of secrecy – Article 13 of the PAA ............................................................................ 22 13.2.5 Duty to clarify the case and to provide information – Article 17 of the PAA.................... 22 13.2.6 The decision shall be in writing and grounds shall be given – Articles 23 and 24 of the
PAA .................................................................................................................................... 22 13.3 Appeal and reversal of administrative decisions – Chapter VI – Article 28-36 of the PAA . 22
13.3.1 Referral of the decision by the seafarer’s doctor ............................................................. 22 13.3.2 Time limit for appeal of the individual decision of the seafarer’s Doctor - Article 29 of the
PAA .................................................................................................................................... 23 13.3.3 the appellate body ............................................................................................................ 23
13.4 Review, exemption and appeal............................................................................................ 23 13.4.1 Introduction and background ........................................................................................... 23 13.4.2 The seafarer’s doctor’s decision........................................................................................ 23 13.4.3 The applicant’s possibility to have decisions made by the seafarer’s doctor reviewed ... 24 13.4.4 Appeals and applications for exemptions with the appellate body – case preparation by
the seafarer’s doctor ......................................................................................................... 25 13.4.5 Case handling by the appellate body ................................................................................ 25
14 Topic 5: Introduction to Medical Selection ..................................................................................... 27 14.1 Definition ............................................................................................................................. 27
14.1.1 Negative selection ............................................................................................................. 27 14.1.2 Positive selection ............................................................................................................... 27
14.2 the medical consultation ..................................................................................................... 28 14.2.1 The role of the doctor ....................................................................................................... 28
14.3 Standards and criteria .......................................................................................................... 29 14.4 the purpose OF MEDICAL selection ..................................................................................... 29 14.5 THe timeline ......................................................................................................................... 29 14.6 the medical condition .......................................................................................................... 30 14.7 job demands of the seafarer ................................................................................................ 30 14.8 mitigating measures ............................................................................................................ 30
15 Topic 6: medical selection – assessment of the safety risk ............................................................. 31

4
15.1 the purpose of the medical examination of seafarers according to the Norwegian regulations ........................................................................................................................... 31
15.2 assessment of the safety risk related to the medical condition .......................................... 31 15.2.1 possible medical incidents ................................................................................................ 31 15.2.2 THE LIKELIHOOD OF a medical incident occurring during the validity period of the
certificate .......................................................................................................................... 31 15.2.3 the Likelihood of a medical incident occurring in this particular seafarer ........................ 32
15.3 the Consequences of a medical incident in the specific position of THE SEAFARER ........... 33 15.3.1 testing of physical capability – the additional positive selection ...................................... 33
15.4 Calculation of un-mitigated safety risk ................................................................................ 33 15.5 Mitigating measures ............................................................................................................ 34 15.6 overall evaluation of the safety risk ..................................................................................... 35 15.7 Conclusion and justification ................................................................................................. 35
16 Topic 7: VIsion: contrast, night, colour, distance, near vision and visual fields .............................. 36 17 Topic 8: Hearing and Hearing requirements ................................................................................... 36 18 Topic 9: Diabetes and other endocrine diseases ............................................................................. 36 19 Topic 10: Epilepsy, Loss of consciousness, epilepsy, altered awareness and sleep disorders ........ 37 20 Topic 11: Chronic neurological diseases .......................................................................................... 37 21 Topic 12: Alcohol and drug abuse.................................................................................................... 37 22 Topic 13A: Psychiatry - homework .................................................................................................. 38
22.1 HOMEWORK CASE: .............................................................................................................. 38 22.1.1 self declaration – medical hisTory as told by the candidate ............................................. 38 22.1.2 from the previous approved seafarers doctors ................................................................ 39 22.1.3 medical report From the department of psychiatry, Hospital A – three years ago .......... 39 22.1.4 From the department of psychiatry (Hospital A) – 3 months after THE DISCHARGE
mentioned above .............................................................................................................. 40 22.1.5 From the department of psychiatry (Hospital A) – 2 years ago ........................................ 40 22.1.6 from the chief consultant, department of psychiatry, Hospital A – recently ................... 40
23 Topic 13B: Psychiatry – clinical case discussion .............................................................................. 41 24 Topic 14A: Cardiovascular diseases – homework ............................................................................ 41
24.1 HOmework case: .................................................................................................................. 41 24.1.1 self declaration – medical history as told by the candidate.............................................. 41 24.1.2 What you find in the medical records ............................................................................... 42 24.1.3 information from the cardiologist – one month ago ........................................................ 42 24.1.4 medical report from the department of neurology, 8 months ago .................................. 42
25 Topic 14B: Cardiovascular disease – clinical case discussion .......................................................... 43 26 Topic 15: lungs and airways - clinical case discussion .................................................................... 43 27 Topic 16: Gastrointestinal disease – clinical case discussion .......................................................... 43 28 Topic 17: Cancer and other malignancies ........................................................................................ 44 29 Topic 18: Physical requirements and physical testing ..................................................................... 44 30 Topic 19: Obesity – CLinical case discussion .................................................................................... 44 31 Topic 20: Urogenital conditions ....................................................................................................... 45 32 Topic 21: Infectious diseases and vaccinations ............................................................................... 45 33 Topic 22: Oral and dental disesases ................................................................................................ 45 34 Topic 23: Medication ....................................................................................................................... 46 35 Topic 24: allergies ............................................................................................................................ 46 36 Topic 25: DIseases of the Blood and bloodforming organs ............................................................. 46 37 Topic 26: Questions, discussion, summing up ................................................................................. 47 38 course evaluation ............................................................................................................................ 47 39 final course test ............................................................................................................................... 47

5
40 APPENDICES ..................................................................................................................................... 48 40.1 APPENDIX 1 – Assessment of medical fitness form (to form part of the seafarer’s medical
record) ................................................................................................................................. 48 40.2 APPENDIX 2 – Declaration of unfitness form ....................................................................... 56 40.3 APPENDIX 3 – Health certificate for seafarers ..................................................................... 57 40.4 APPENDIX 4 - Declaration from the seafarer’s doctor regarding use of regular medicine . 58 40.5 Appendix 5 - Medical Certificates approved for service on board Norwegian vessels ....... 59 40.6 APPENDIX 6 - Regulations on tuberculosis control .............................................................. 59 40.7 APPENDIX 7 - Physical requirements related to different job demands ............................. 60

6
2 PREFACE
Welcome to the “NCMDM Basic course for seafarers’ Doctors”.
This compendium has been developed as an adjunct to the course and a part of the distance learning component of the course (15 hours). It should be studied prior to attending the taught part of the course (20 hours).
Throughout the compendium, for ease and clarity, we refer to the seafarer and the seafarer’s Doctor as ‘he’ to include all persons irrespective of gender.
The compendium is written to follow the syllabus of the course. For each topic there is a recommendation for reading to be completed before the course and in some cases there is additional information within the compendium. This information is there to supplement the other sources of learning material and may be discussed further within the taught course.
3 INTRODUCTION
This course is designed to meet the requirements for competence of medical Doctors who will conduct the medical examinations of seafarers in accordance with the standards set by the Norwegian Maritime Authority (NMA).
3.1 LEARNING OUTCOMES
On completion of this course, the participants shall
I. be able to
a. conduct the medical examinations of seafarers in accordance with the parties’
statutory requirements regarding such examinations, with which they should be
entirely familiar.
b. conduct the medical examination in accordance with medical best practice and proper
case consideration, obtaining relevant additional specialist advice and investigation
where appropriate.
c. assess the safety risk which relates to the seafarer’s medical condition in general, to
his or her regular and emergency duties and within a time perspective corresponding
to the validity period of the medical certificate.
d. personalise the safety risk assessment relating to individual workers with medical
conditions, and the consequences this may have for the individual him/herself, the
safe operation of the ship and to other crew members.
e. assist the seafarer in cases of complaints and applications for exemption, and prepare
a proper case for the appellate body.
II. understand
a. the limitations and challenges regarding medical treatment of ill and injured seafarers
whilst at sea including knowledge of the available medical resources on board and the
possibilities for evacuation

7
b. the characteristics of working places on board ships, and the different physical and
mental demands which relate to different types of work on board ships
c. the different roles of Doctors in different positions (Approved Doctors, Company
Doctors, General Practioners, Specialists etc.) and be aware of his/her own role whilst
conducting medical examination of seafarers
d. the consequences of a declaration of unfitness for the individual.
It is intended that this course provides the basic training required for a Doctor to be approved by the NMA as a seafarer’s Doctor. As in all areas of medicine, learning is a continuous programme and it is expected that the Doctor will undertake relevant continuing medical education in this area, to include attending a Refresher Course as required by the NMA.
4 COURSE OVERVIEW
The course is composed of two different parts.
4.1 DISTANCE LEARNING AT HOME INCLUDING PRE COURSE TEST
Distance learning must be completed and a test completed before attending the course. This test will be in the form of an open book multiple choice test and must be sent to the course coordinator before the date advised upon registration for the course. This test must be passed in order for you to complete the course and obtain your certificate.
Prior to attending the taught course it is compulsory to familiarise yourself with the following:
the regulations,
the guidance to the regulations, and
this compendium
You should also familiarise yourself with the forms which will be used (Appendix 1 - 4).
In addition you will find suggested reading for further in-depth study with links to the relevant sources.
You must also prepare two case studies and submit a word document slide outlining your thoughts and decision as instructed. These cases will be discussed during the course and you should be prepared to present your decision making process and conclusion. You will not receive personal feedback on the documents submitted but they may be used, anonymously, during the course.
The scenario in both cases is that a seafarer sees you as an approved seafarer’s doctor and demands a medical certificate.
The following questions should be answered:
I. Which medical incidents/episodes/situations must be taken into consideration, given the medical diagnoses of the seafarer?
II. How do you assess the likelihood that any of these may occur to a person with the same diagnosis within the next two years, based on available evidence for the diagnostic group the employee belongs to?
III. How will you individualise the likelihood of such an event occurring in this particular seafarer, based on your knowledge of his individual medical history?
IV. What is your assessment of the unmitigated safety risk that is connected to this seafarer’s medical condition in a two-year perspective?
V. Are there any mitigating measures you could implement, to reduce the safety risk or the likelihood of a medical incident/episode occurring? If so, what?

8
VI. How do you evaluate the overall risk, taking the mitigating measures into account? VII. How do you assess the seafarers request against the requirements of the regulations?
You should use the approach discussed in Chapter 13 and base your assessment on the information that he has normal physical capacities and no concomitant somatic illness or disease.
4.2 A THREE DAY TAUGHT COURSE WITH FINAL TEST
The participants will meet for three days where lectures are presented and different clinical conditions discussed in conjunction with case presentations.
Mentometer will be used extensively in the case discussions and the teaching will include methods and techniques to ensure that all participants involve themselves in the learning opportunities.
You must be present throughout the whole course and this will be monitored.
4.2.1 SYALLBUS
NO TOPIC Taught
course
(minutes)
Distance
learning
(minutes)
1 The Shipping Industry and working at sea 45 45
2 Medical treatment possibilities at sea 45
3a Regulations of 5 June 2014 No 805 on medical examination of employees on
Norwegian Ships and mobile offshore units
45 45
3b Guidance to regulations on the medical examination of employees on
Norwegian ships and mobile offshore units
45 45
3c Procedures, forms, how to use the web-based system for issuance of medical
certificates
45
3d Organization of the Norwegian Health Service and the Health Personnel Act 45
3e Approval procedures, quality system requirements, risk based audit of approved
doctors
45
4 Act of 10 February 1967 No. 00 relating to procedure in cases concerning the
public administration
45 45
5 Introduction to Medical selection 45
6 Risk assessment in medical selection 45
7 Vision and eye disorders 45 45
8 Hearing and ear disorders 45
9 Clinical case discussion: Diabetes Mellitus and other endocrine disorders 45
10 Clinical case discussion: Loss of consciousness, epilepsy, altered awareness and
sleep disorders
45
11 Clinical case discussion: Chronic neurological conditions 45
12 Clinical case discussion: Alcohol and drug abuse 45
13a Homework discussion: Psychological /psychiatric case 45 45
13b Clinical case discussion: Psychological demands, psychological conditions 45
14a Homework discussion: Cardiovascular case 45 45
14b Clinical case discussion: Cardiovascular disease 45
15 Clinical case discussion: Respiratory disease 45
16 Clinical case discussion: Gastrointestinal disease 45
17 Malignancies 45
18 Physical demands and physical testing. Musculoskeletal diseases 45

9
19 Clinical case discussion: Obesity 45
20 Genitourinary medicine 30
21 Infectious diseases and vaccinations 30
22 Oral health and dental inspections 30
23 Case discussion: Medication 45
24 Allergies 30
25 Blood disorders 30
26 General questions and answers 30
27 Course evaluation 45
28 Examination 60 60
TOTAL HOURS 19,5 14,5
4.3 FINAL TEST
By the end of the course all participants will be expected to demonstrate the principles of good judgement in the clinical assessment and risk assessment of a seafarer with a variety of medical conditions within the relevant national and international guidelines.
The final course test is an open book multiple choice test. All references that you would use on a regular working day in your office can be used at the test. However you should complete the test individually without discussion with other candidates.
To pass the test you must achieve at least 80% correct answers.
If you fail, you will get an opportunity to try once more. If you also fail this test, you will have to attend another course to be certified as a NMA approved seafarer’s doctor.
4.4 AFTER COMPLETION OF THE COURSE
A course certificate will be sent to all participants who have successfully completed and passed the course. If you fail on either of the tests, you will be notified by email and you will have the opportunity to take the test again. If you are still unsuccessful you will need to repeat the whole course. The organisers will send a list of all participants who have successfully passed the course to the Norwegian Maritime Authority (NMA).
4.5 EVALUATION OF THE COURSE AND INFORMATION TO AUTHORITIES
The course will be evaluated by the participants, and reports from each course will be sent to the NMA along with a list of participants who have successfully completed the course.
4.6 QUALIFICATION AFTER SUCCESSFUL COMPLETION OF THIS COURSE
This course meets the competence requirements of the NMA to become a seafarer’s doctor.

10
5 REFERENCES
5.1 INTERNATIONAL CONVENTIONS OF IMPORTANCE TO THIS COURSE
International Convention for the Safety of Life at Sea (SOLAS), 1974
The STCW Convention 1978, as amended 2012
Maritime Labour Convention 2006
5.2 INTERNATIONAL GUIDELINES OF IMPORTANCE TO THIS COURSE
ILO/IMO Guidelines on Medical Examinations of Seafarers
5.3 NORWEGIAN LEGISLATION OF IMPORTANCE TO THIS COURSE
Regulations of 5 June 2014 No. 805 on medical examination of employees on Norwegian ships and mobile offshore units
Employment protection etc. for employees on board ships (The Ship Labour Act) (6/21/2013 102)
Act of 10 February 1967 No. 00 relating to Procedure in Cases concerning the Public Administration (The Public Administration Act) (6/14/2013 42)
Act of 19 May 2006 No. 16 relating to the right of access to documents held by public authorities and public undertakings (The Freedom of Information Act) (5/19/2006 16)
Act of 16 February 2007 No. 9 relating to Ship Safety and Security (The Ship Safety and Security Act) (2/16/2007 9)
Act of 2 July 1999 No. 64 relating to Health Personnel etc.
5.4 GUIDANCE TO THE REGULATIONS
Guidance to the Medical Examination of Employees on Norwegian Ships and Mobile offshore units
5.5 SUPPLEMENTARY READING
Handbook for seafarer medical examiners, written by Professor Tim Carter, is freely available on the web-pages of the NCMDM. http://handbook.ncmm.no/
Textbook of maritime medicine- http://textbook.ncmm.no/textbook-of-maritime-medicine
Tim Carter: Fitness to drive – ISBN 1 853156515
Maritime and Coastguard Agency Doctors Manual 2010 https://www.gov.uk/government/publications/the-approved-doctors-manual
• ‘Brackenridge’s “Medical Selection of Life Risks” is the reference book for insurers. It gives useful information on the way of thinking, but obviously has a different purpose, as the book is about choosing candidates for buying insurance at the same time as the lifetime risk of dying is so low that there is a low enough risk that a claim will be received.
• UpToDate (www.uptodate.com) is a very good review database, easy to search. • BMJ Best Practice (http://bestpractice.bmj.com/best-practice/welcome.html). is a
comprehensive database which is very useful as a reference, targeted to general practitioners, but also useful for others.
• Fitness for Work. The medical aspects [Paperback] Keith T Palmer (Editor), Robin A F Cox (Editor), Ian Brown (Editor). ISBN-10: 0199215650 | ISBN-13: 978-0199215652.
11
SYLLABUS 6 TOPIC 1: THE SHIPPING INDUSTRY AND WORKING AT SEA
This lecture is part of the taught course.
Recommended reading before this lecture:
Textbook of Maritime Medicine
Chapter 2 The Sea as a Working Place
Chapter 3 The Shipping Industry
7 TOPIC 2: MEDICAL TREATMENT POSSIBILITIES AT SEA
This lecture is part of the taught course.
Recommended reading before this lecture:
Textbook of Maritime Medicine
Chapter 8 Medical Care on Board
7.1 THE INTERNATIONAL LEGAL BASIS FOR PROVIDING MEDICAL CARE AT SEA
The legal basis outlining the standard of care that should be available for a seafarer who is injured or becomes unwell whilst at sea is included in the Maritime Labour Convention (MLC) 2006 (ILO) Standard A4.1 1(b).
“seafarers are given health protection and medical care as comparable as possible to that which is generally available to workers ashore, including prompt access to the necessary medicines, medical equipment and facilities for diagnosis and treatment and to medical information and expertise”
Other conventions such as STCW, SOLAS and guidelines from the World Health Organisation (WHO) also cover various aspects of the medical care of seafarers at sea.
The signatories to the conventions have the right to produce national guidelines based on the international agreement; hence the legislation in each country may vary slightly leading to differences in standards and expectations amongst seafarers.
In addition there are other pieces of legislation that cover the management of hazardous cargoes etc.
7.2 ACCESS TO MEDICAL CARE AT SEA
Only ships with 100 or more persons on board and ordinarily engaged on international voyages of more than 3 days duration are required to carry a medical Doctor. Ships that are capable of reaching medical facilities within eight hours should have at least one designated seafarer trained in medical care to a competency of STCW A-VI/4.1 approved medical first-aid training. All other ships should have at least one designated seafarer for medical care approved to STCW A-VI/4.2.
7.2.1 SHIPS WITHOUT A DOCTOR
The majority of seafarers will serve on ships without a Doctor and with only ships officers (trained to a standard set out in STCW) able to provide medical care in the event of illness or accident. The training requirements are part of the original STCW and were not updated in the recent amendments, making

12
them out of date in some cases. The standard of the training given to the officers varies from country to country and between providers, leading to little consistency in the competency of ship’s officers.
Each ship is also required to carry a medical chest of drugs and equipment, although the contents of this are not stated in any international convention. The WHO has produced a guide and within the European Union there is a Directive specifying the generic groups of medications that must be carried. There is also a requirement for each Ship to have a dedicated place to treat sick or injured crew. In practice this is often crowded, also used for other purposes and a long way from the bridge and any means of communication off the ship.
The WHO also produce the International Medical Guide for Ships, now in its 3rd edition, with the aim of providing a generic textbook to be carried on board and referred to as necessary by the ship’s officers. There are concerns as to whether or not this book adequately meets the needs of those managing illness and injury at sea, however there are currently no plans or budget to revise and update it. Several traditional maritime nations produce their own national guides, which vary in size, the degree of detail given and in the style of presentation. They generally relate more closely to the training and medical chest requirements in their countries of origin than do any of the international guides or lists, but this means that seafarers trained elsewhere may have to relearn their practices and approaches to meet the requirements of the flag of the ship on which they are serving.
In summary the medical care afforded to seafarers on board a ship without a Doctor is very variable. However the current legally based requirements do ensure that even the least concerned ship operator and maritime authority must have some basic systems in place for the management of medical emergencies at sea.
7.2.2 SHIPS THAT CARRY A DOCTOR
As stated above vessels that carry more than 100 people and undertake international voyages of more than three days are required to have a Doctor on board. In reality this usually means the cruise industry where crew have access to the same medical care as the passengers, and the military. Other shipping companies may choose to place a Doctor or other medically trained professional on board. Examples include Color Line ferries from Oslo to Kiel and many offshore standby vessels.
Guidelines produced by the American College of Emergency Physicians are widely accepted within the cruise industry as good practice for the qualification of medical staff at sea and for the equipment and capability that each ship should have. Some national maritime authorities have also produced their own requirements, however there is little in the way of international agreement in these areas and therefore the standard can vary widely.
Even in the best equipped ship’s medical centre and with the best trained Doctors and nurses, there remains a limit to the care that can be offered on board any ship.

13
7.2.3 AVAILABILITY OF MEDICAL ADVICE – TELEMEDICAL MARITIME ASSISTANCE SERVICE (TMAS)
The provision of telemedical advice to ships is an obligation placed on maritime states according to a number of international conventions, recommendations, regulations and guidelines from different UN Agencies1.
However, the reality is that whilst the traditional maritime nations do provide such services, normally freely available for use by ships of all nations, few other countries do so. The Norwegian service, Radio Medico Norway has been in operation since 1949, and now forms part of the Norwegian Centre for Maritime and Diving Medicine.
The scope of the national services that are provided varies hugely. In some cases an obligation is put on ship operators to make private provision and a number of countries provide services linked to their coastguard and search and rescue facilities. Here the primary concern is the management and evacuation of the seriously ill or injured and little, if any, assistance is offered in the care of minor illnesses or injuries. Other services may additionally provide assistance with the handling of all medical conditions, including more than the typical emergencies and some offer direct access for seafarers to obtain confidential clinical advice.
One of the major problems between the ship and the Telemedical Maritime Assistance Service (TMAS) is language, as medical terms do not form part of standard maritime English. Most services rely on voice and email communication - the enhanced communications capability offered by maritime satellite broadband, for instance, the use of video consultation and the transmission of real time clinical measurements has largely not been developed. The cruise industry and some companies undertaking marine work in very remote locations are notable exceptions in this area.
7.2.4 MEDICAL EVACUATION - MEDEVAC
When it is agreed by those involved that the seafarer cannot be cared for on board and requires urgent and specialised medical care, options for evacuation (medevac) will be considered. It is important to remember that in large parts of the world’s oceans there is no evacuation option as the ship is outside of helicopter or rescue craft range. In this situation it may be possible for a ship to seek assistance from a naval vessel or a ship carrying a Doctor but this may or may not be available.
Closer to shore, options for disembarking a sick or injured seafarer include diversion to the nearest port, increasing speed to reach the planned destination sooner, or helicopter or boat transfer of the patient to shore. All of these carry risks and costs and the available options vary depending on the exact location of the ship. Boat and helicopter transfers are distance and weather dependent and require the appropriate personnel to be available to continue the care of the patient during transfer. Helicopter transfers in particular carry a potential risk to the ship itself in case of accidents and in many
1 (I) International Convention for the Safety of Life at Sea (SOLAS), 1974; (II) International Convention on Standards of Training, Certifiaction and Watchkeeping for Seafarers (1978) – as amended; (III) International Convention on Maritime Search and Rescue (1979) SAR Convention; (IV) IAMSAR Manual I, II, III; (V) ITU List of Radiodetermination and Special Service Stations; (VI) INMARSAT Convention; (VII) UN Convention on the Law of the Sea; (VIII) R 106 Medical Advice at Sea Recommendation, 1958 (ILO); (IX) C 164 Health Protection and Medical Care (Seafarers) Convention, 1987 (ILO); (X) Maritime Labour Convention 2006 (MLC 2006), ILO; (XI) Council Directive 92/29/EEC of 31 March 1992 on the minimum safety and health requirements for improved medical treatmen on board vessels; (XII) Res. Msc. 70(69) 1998 Adoption of amendments to the international convention on maritime search and rescue, 1979; (XIII) Msc. Circ 960 (2000) Medical assistance at sea
14
cases night flying is not possible. Sometimes the ship construction itself makes hoisting of a stretcher by helicopter dangerous.
Whilst arranging a medevac it should also be remembered that the seafarer must be taken to appropriate medical care ashore in appropriate transportation. All of this may be arranged by the company, agent or TMAS provider but it cannot always be guaranteed that the nearest port can provide appropriate care. Once the seafarer has received any initial, emergency care ashore they will need to be repatriated to their country of origin for ongoing care.
In summary the medical care that can be offered to a seafarer whilst at sea is variable and can be extremely limited. It is therefore vital that appropriate medical selection is carried out to reduce the likelihood of illness or severity of injury and consequently the risks to the ship, the other crew members and to the seafarer himself.
8 TOPIC 3A: REGULATIONS OF 5 JUNE 2014 NO 805 ON MEDICAL EXAMINATION OF EMPLOYEES ON NORWEGIAN SHIPS AND MOBILE OFFSHORE UNITS
All participants are required to familiarize themselves with the text of the Regulations prior to attending the taught course. All procedural requirements are to be found directly in the text of the Regulations, and in the Public Administration Act
All material requirements, i.e. standards and criteria for medical selection are to be found in Attachments A-E of the Regulations:
Attachment A: Vision
Attachment B: Hearing
Attachment C: Physical requirements
Attachment D: Use of medicines
Attachment E: Diagnostic entities classified in accordance with ICD10.
9 TOPIC 3B: GUIDANCE TO REGULATIONS ON THE MEDICAL EXAMINATION OF EMPLOYEES ON NORWEGIAN SHIPS AND MOBILE OFFSHORE UNITS
Norway has around 280 approved seafarers’ doctors abroad and more than 500 approved seafarer’s doctors within Norway. Seafarers’ doctors are required to speak an appropriate level of Norwegian or English or both. This is the reason why this guidance is produced in English only.
You can follow the link to the Guidance earlier in this compendium, or access the document through the NMA webpages:
Go to the tab “Shipping”
Go to the tab “Seafarers”
Go to the tab “Seafarer’s doctors”
Go to “Medical examinations of employees on Norwegian ships and mobile offshore units”
Under the heading “Guidance to the Regulations” you will find a link to the pdf-version of the Guidance.
The guidance is dynamic, and will be updated at regular intervals. It is therefore recommended that you make use of the version found online, and NOT a downloaded version.

15
Course participants are required to familiarize themselves with this guidance and to be able to use the guidance during the course, and later in daily work as a seafarers’ doctor.
The medical part of the guidance is mainly composed of background evidence intended for the assessment of the likelihood of medical incidents that can threaten safety on board. The rules and limits for judgement are to be found in the Regulations and their attachments, rather than in the guidance.
10 TOPIC 3C: USE OF A WEB-BASED SYSTEM FOR ISSUANCE OF MEDICAL CERTIFICATES AND DECLARATIONS OF UNFITNESS
10.1 THE ONLINE REGISTRATION SYSTEM
The Norwegian Maritime Authority (NMA) has developed a system for the registration and submission of electronic medical certificates. The system is part of the Norwegian reporting portal Altinn and it is mandatory for all NMA approved seafarer’s Doctors to use it. The system gives the NMA approved seafarer’s Doctors an overview of all submitted medical certificates and declarations of unfitness concerning the seafarer.
10.2 HOW TO GET ACCESS TO THE ONLINE SYSTEM
NMA approved seafarer’s doctors outside of Norway must apply to the Brønnøysund Register Centre in Norway for a D-number (id-number). The D number is used to identify the approved seafarer’s Doctor to the Norwegian Authorities and is mandatory in order to access the online registration system.
1. Use the following link to get the correct application form: https://www.brreg.no/wp-content/uploads/BR-1016E.pdf
2. Complete Part 2 of the form, the NMA will fill in Part 1.This is in contradiction to the online instructions.
Please see the Brønnøysund Register Centre’s web page for further information: https://www.altinn.no/en/Forms-and-Services/Etater/The-Bronnoysund-Register-Centre/Request-for-assignment-of-a-D-number1/ Once you have completed Part 2 you should send the form to:
The Norwegian Maritime Authority P. O. Box 2222 N-5509 Haugesund Norway
Make sure that you enclose a certified copy of a valid proof of identity that contains a photo, your full name, date of birth and gender, the expiry date and your nationality. We highly recommend using a valid passport. Please remember that the copy must either be certified by a Norwegian Foreign Service Mission or an entity with notary powers.
The NMA will send the application form to the Brønnøysund Register Centre, once the Director General of Shipping and Navigation has signed Part 1 of the form. The Brønnøysund Register Centre will notify the NMA when a D number is allocated and the NMA will then contact you by email with your D number and instructions on how to order PIN codes. Once you have applied for the PIN codes as instructed you will receive these by ordinary

16
mail from the Agency for Public Management and e-Government (Difi). Please be aware that it may take three to four weeks before the PIN codes arrive. Once you have received the PIN codes please inform the NMA by email and they will send further instructions regarding how to register as a new user and how to use the electronic submission system. In the event that you lose your PIN codes you must contact Difi to request new ones.
10.3 COMPLETING THE MEDICAL CERTIFICATE AND DECLARATION OF UNFITNESS
Please see the guidance to completing the certificates on the NMA web page for further information: Guidance of submitting the form. This will also be covered in depth during the taught course.
As part of your medical examination you should complete a paper copy of form KS 0497 E and retain a copy of this in your office with the patient record. Please see Appendix 3.
If you have any additional questions or comments regarding access to the online system please contact Line Myklebust at the NMA by e mail, [email protected] or by telephone on + 47 52 74 51 26.
11 TOPIC 3D – ORGANIZATION OF THE NORWEGIAN HEALTH SERVICE AND THE HEALTH PERSONNEL ACT
11.1 NORWEGIAN HEALTH SERVICE ORGANIZATION
11.1.1 HOSPITALS AND SPECIALIST SERVICE
Unlike many other countries, Norway’s health system is run mainly by the state. The public hospitals are run by four Regional Health Trusts (or regional health authorities) and 50 local health trusts. Although organized as private companies, all of them are 100% owned by the state.
Their activities are regulated by a separate act – the Act of 15th June 2001 No 93 concerning Health Trusts.
The map below depicts the regional organization of the hospital service in Norway:
The Regional Health Authorities are as follows:
Northern Norway Regional Health Authority
Central Norway Regional Health Authority
Western Norway Regional Health Authority
South-Eastern Norway Regional Health Authority

17
The Boards of the regional health authorities are appointed by the general assembly of the Regional Health Trusts – which is one single person only – the Minister of Health and Care Services. Their only responsibility is to run the hospitals and ambulance services.
Each of the Regional Health Authorities is divided into smaller Health Trusts, like this example from the Western Norway Regional Health Authority where the region is divided into four local areas.
Helse Førde
Helse Bergen
Helse Fonna
Helse Stavanger
11.1.2 GENERAL PRACTICE
Most Doctors working in general practice and family medicine have a contractual relationship with the community in which they are working and the Norwegian Labour and Welfare Administration (NAV). The Doctors are financed partly by each of them – the community administration paying per patient on the Doctor’s list, and NAV paying per consultation the doctor carries out. The list of patients is administered by NAV.
Some Doctors practise without a contractual relation with NAV, earning their income directly from their patients only.
11.1.3 HEALTH SUPERVISION
A separate National Board of Health supervision carries out inspections to ensure that municipalities and county councils are fulfilling their public health obligations, and deals with complaints on the work doctors and hospitals carry out. The local representative of this Board of Health Supervision is the County Governor, represented by the County Medical Officer.
11.2 THE NORWEGIAN HEALTH PERSONNEL ACT
In the following section some important aspects of the Act of 2 July 1999 No. 64 relating to Health Personnel etc. (The Health Personnel Act – “HPA”) will be described. Parts of the text are quotations from the text of the Act. For the complete text and the context, the text of the Act should be visited.
Note that The Public Administration Act (“PAA”) will apply to all administrative procedures for the medical examination of seafarers, but the medical content of the examination, as well as the sound judgment, must be in accordance with the HPA.
Breech of the provision of either the PAA or the HPA will be assessed by the appellate body on behalf of the NMA.
Although the HPA does not directly apply to overseas Doctors practicing in countries other than Norway , it clearly describes the expectations that Norway has of Doctors approved by the NMA for the medical examinations of seafarers.
The act describes the
• Requirements for professional conduct of health personnel • Requirements for the organization of facilities • Special rules in connection with authorization
18
• Duty of confidentiality and the right of disclosure • Duty of disclosure • Notification requirements • Duty relating to documentation. • Conditions relating to the granting of authorization, license and certificate of completion of
specialist training. • Granting and expiration of authorization, license and certificate of completion of specialist
training. • Consequences to breach of the provisions of this Act. • The Norwegian Board for Health Personnel and the Norwegian Pharmacy Appeals Board § 71
Judicial review
11.3 OBJECTIVE AND SCOPE OF THE HPA – ARTICLE 1 AND 2
According to Article 1, the objective of the HPA is to contribute to safety for patients and quality within the health service as well as to trust in both health personnel and the health service.
The Act applies to health personnel and the facilities where health care is being provided. As per Article 2, and as determined by the King in the regulations, this Act shall apply to persons on board Norwegian ships engaged in foreign trade, to Norwegian civil aircraft in international traffic and to installations and vessels at work on the Norwegian continental shelf and within Norwegian rescue area.
11.4 RESPONSIBLE CONDUCT – ARTICLE 4
This is one of the most relevant parts of the act regarding the medicals conducted by the seafarer’s Doctors. Article 4 describes what is meant by responsible conduct. It says that health personnel shall conduct their work in accordance with the requirements of professional responsibility and diligent care that can be expected based on their qualifications, the nature of their work and the situation in general.
Health personnel shall act in accordance with their professional qualifications and assistance shall be obtained and patients referred on to others if this is necessary and possible. If the patient’s needs so indicate, the examination shall be performed through co-operation and inter-action with other qualified personnel.
11.5 THE ISSUING OF CERTIFICATES
This act has the following general statement on the issue of certificates
§ 15 Requirements to medical reports, medical certification etc.
“Anyone who issues medical certification, medical reports etc. shall be careful, precise and objective. A medical report etc. shall be correct, and contain only such information that is necessary for its intended purpose. Health personnel that are disqualified pursuant to the Public Administration Act section 6 shall not issue a medical report, medical certification etc.”
The medical report shall contain all of the information which is important for the recipient and for the intended purpose. The health personnel shall make it clear if the statement or certificate is based on only a limited part of the available information.
When health personnel understand that the way sensitive information is described in a certificate, statement etc. is of special importance, it must be discussed with the patient.

19
When health information is given to an insurance company and the company can understand the information as an indication of a serious disease, the patient must be informed if he is unaware of the circumstance.
The Ministry may issue regulations with specific rules for medical certificates, statement etc.
The requirements for carefulness, precision, objectivity, correct information, limited information and all information which is pertinent for the purpose, are fundamental. Equally basic is the right of the patient to be informed about the importance of conveying the information and not holding back information.
11.6 OTHER PROVISIONS OF THE HPA
It is beyond the scope of this course to go into further details regarding other provisions of the HPA.
The seafarer’s Doctor is advised to review the appropriate text of the HPA regarding questions of
• the duty of confidentiality and the rights of disclosure (Chapter 5 – Articles 21-29), • the duty of disclosure (Chapter 6 – Articles 30-34), as well as • the duty for medical record keeping (Chapter 8 – Articles 39-47).
12 TOPIC 3E: APPROVAL PROCEDURES, QUALITY SYSTEM REQUIREMENTS, RISK BASED AUDIT OF APPROVED DOCTORS
12.1 APPROVAL AS A NMA APPROVED SEAFARERS’ DOCTOR AND THE DOCTOR’S OBLIGATIONS
In order to become an approved seafarer’s Doctor you must meet the requirements in Section 7 of the Health Regulations.
Medical practitioners with a practice in Norway are approved as seafarer’s Doctors by the Norwegian Maritime Authority.
Medical practitioners with a practice outside of Norway are approved as seafarer’s Doctors by a Foreign Service mission on behalf of the Norwegian Maritime Authority.
See https://www.sjofartsdir.no/en/shipping/seafarers/approved-seafarers-doctors/medical-examinations-of-employees-on-norwegian-ships-and-mobile-offshore-units/ for more information about the approval process.
It is not possible to issue a valid medical certificate pursuant to the Health Regulations without first being approved by the NMA or a Norwegian Foreign Service mission.
Please note that the individual doctor must himself seek approval with the NMA or the Royal Norwegian Embassy in the country of concern. Approval is not automatic on completion of the course and will depend on other factors such as the number of seafarer’s Doctors locally, the perceived need for medical examinations in that area etc.
An application form must be completed and can be found at: KS-0416 Application for approval as seafarer’s doctor
Medical practitioners already approved must apply for renewal of their approval no later than one month before the expiry date of the current approval period. This is important in order to avoid the situation where the doctor is without approval for a period while the application for renewal is being processed.

20
In exceptional cases, the Norwegian Maritime Authority may grant exemptions from the requirements for approved seafarer’s doctors.
12.1.1 A BASIC COURSE FOR SEAFARERS’ DOCTORS APPROVED BY THE NMA HAS TO BE COMPLETED
Medical practitioners already approved as a seafarer’s doctor will be included in the transitional arrangement of Section 19 of the Health Regulations, and will therefore have 5 years from the date of entry into force of the Regulations – 1st July 2014 – in order to complete a course in maritime medicine.
Medical practitioners not approved as a seafarer’s doctor when the Regulations enter into force will have to complete a course for seafarer’s Doctors approved by the NMA before seeking approval.
Seafarer’s Doctors must complete a refresher course approved by the NMA during each approval period in order to have their approval renewed.
12.2 QUALITY SYSTEM REQUIREMENTS FOR APPROVED SEAFARERS’ DOCTORS
Pursuant to the Regulations of 5 June 2014 no. 805 on the medical examination of employees on Norwegian ships and mobile offshore units (Health Regulations), seafarer’s doctors are required to have a quality system in place that ensures that their work is carried out in accordance with the requirements of the Health Regulations. The quality system shall be in accordance with an internationally recognised standard.
The Health Regulations entered into force on 1 July 2014, and Doctors who were approved as seafarer’s doctors at this time are covered by the transitional arrangement of section 19 of the Regulations, and must therefore implement a quality system by 1 July 2019. Doctors not approved as seafarer’s Doctors when the Regulations entered into force will have to implement a quality system before they can be approved.
The form “Self-declaration – quality system for approved seafarer’s doctor” (KS-0418) shall be enclosed with the application.
If the quality system is change or replaced for any reasons, a new self-declaration form shall be submitted to the NMA. This is the responsibility of the seafarer’s Doctor.
13 MORE INFORMATION ON WHAT SHOULD BE INCLUDED IN A QUALITY SYSTEM IS PROVIDED IN THE GUIDANCE.TOPIC 4: NORWEGIAN PUBLIC ADMINISTRATION PROCEDURES
13.1 INTRODUCTION
This section describes very briefly the most important points in the Norwegian Public Administration’s procedures, with emphasis on those relevant to seafarer’s doctors.
The Act of 10 February 1967 relating to procedure in cases concerning the public administration as subsequently amended, most recently by Act of 17th December 2010 No 85 (short title: Public Administration Act) is the act regulating the administrative procedures that shall be followed by any representative who makes individual decisions on behalf of the state.

21
13.1.1 SCOPE OF THE ACT
According to Article 1 of the Public Administration Act (the Act), the Act applies to such activities as are conducted by administrative agencies unless otherwise provided by or pursuant to statute.
Any central or local governmental body shall be considered to be an administrative agency.
A private legal person shall be considered to be an administrative agency in cases where such person makes individual decisions or issues regulations.
An approved seafarer’s Doctor is considered to be an administrative agency because his authority has been delegated to him by the NMA.
13.1.2 “INDIVIDUAL DECISIONS”
The decision by an NMA approved seafarer’s Doctor is an “individual decision” according to the Public Administration Act.
This means that the procedures described in the Act must be followed by a Doctor who issues medical certificates for seafarers.
Different aspects of these obligations are reviewed in more detail below, although the text of the Act should be visited for a complete overview.
13.2 THE RIGHTS OF THE SEAFARER AND THE OBLIGATIONS OF THE SEAFARER’S DOCTOR ACCORDING TO THE PUBLIC ADMINSITRATION ACT (PAA)
13.2.1 CONFLICTS OF INTEREST – ARTICLE 6 OF THE PAA
A public official – in this context a NMA seafarer’s Doctor – shall be disqualified from preparing the basis for a decision or from making any decision in an administrative case if:
he himself is a party to the case of issuing a medical certificate
he is related by blood or by marriage to the person in direct line of ascent or descent or collaterally as close as a sibling,
he is or has been married or is engaged to the person, or is the foster parent or the foster child of the person,
he is the guardian or agent of the person, or has been the guardian or agent of the person
he is the head of, or holds a senior position in, or is a member of the executive board or the corporate assembly of a company which is a party to the case
He is similarly disqualified if there are any other special circumstances which are apt to impair confidence in his impartiality.
For a more complete discussion of the question of disqualification the original text of the Public Administration Act should be visited.
13.2.2 DUTY TO PROVIDE GUIDANCE – ARTICLE 11 OF THE PAA

22
The seafarer’s Doctor has a general duty to provide guidance to the person asking for a medical examination on the right to complain or the right to ask for an exemption from the regulations. The seafarer’s doctor must assist the seafarer in these processes as required.
This duty to provide guidance has the purpose of ensuring that all parties of a case are able to safeguard their interest in the specific case in the best possible way. The extent of such guidance must be adapted to the situation and the capacity of the Doctor to undertake such activity.
13.2.3 RIGHTS FOR THE SEAFARER TO BE ASSISTED BY AN AGENT – ARTICLE 12 OF THE PAA
In accordance with Article 12 in the PAA, the person seeking a medical certificate has the right to call on the assistance of an advocate or other agent at all stages of the proceedings. Any person who is of age or any organization of which the party concerned is a member may be employed as an agent.
13.2.4 DUTY OF SECRECY – ARTICLE 13 OF THE PAA
In accordance with Article 13 of the Public Administration Act, the Doctor has the duty to keep confidential all information he gets to know during the medical examination and handling of the case. This duty adds to the duty of secrecy derived from the Health Personnel Act.
13.2.5 DUTY TO CLARIFY THE CASE AND TO PROVIDE INFORMATION – ARTICLE 17 OF THE PAA
The seafarer’s Doctor shall ensure that the case is clarified as thoroughly as possible before any administrative decision is made. This does not mean that all possible information should be gathered, rather that the case must be clarified to an extent which makes sound assessment possible, as well as reaching a correct conclusion in accordance with the regulations. One should not have reason to believe that further information would change the basis for the decision to such an extent that a different decision would be taken.
The PAA also includes more detailed information on the different parts of case consideration, to ensure responsibility in all aspects. Visit the PAA itself for more detailed information.
13.2.6 THE DECISION SHALL BE IN WRITING AND GROUNDS SHALL BE GIVEN – ARTICLES 23 AND 24 OF THE PAA
When the seafarer’s Doctor has reached a decision in the case, he shall issue the appropriate certificate. In addition a written explanation giving the grounds for the decision shall be given to the person of concern.
The grounds should contain at least a medical professional explanation and the legal basis for the decision, with reference to the Regulations and the Guidelines.
The person of concern has the right to see all documents of the case – see Article 18.
13.3 APPEAL AND REVERSAL OF ADMINISTRATIVE DECISIONS – CHAPTER VI – ARTICLE 28-36 OF THE PAA
13.3.1 REFERRAL OF THE DECISION BY THE SEAFARER’S DOCTOR
23
A decision by the seafarer’s Doctor can be appealed to the Appellate Body concerning medical certificates for employees on Norwegian ships and mobile offshore units.
The seafarer’s Doctor has the duty to inform the person regarding the possibility to appeal, to guide him and even to assist him in the process if needed.
Appeals by the seafarer should be given or sent to the seafarer’s Doctor who has issued the certificate of concern. Only the seafarer can start the process of appeal but he must be guided as necessary by the seafarer’s Doctor.
When the seafarer’s Doctor receives such an appeal, he has the duty to revisit the documents, reconsider the decision and, if appropriate, to change the decision.
If the seafarer’s Doctor finds that the decision should not be changed, he has the duty to carry out such further investigation as the case requires, collect and review all relevant documents, and prepare the case for the NMA/Appellate Body and send the documents with his recommendation to the NMA/Appellate Body.
13.3.2 TIME LIMIT FOR APPEAL OF THE INDIVIDUAL DECISION OF THE SEAFARER’S DOCTOR - ARTICLE 29 OF THE PAA
If the seafarer wishes to appeal the individual decision of the seafarer’s Doctor to the Appellate Body he must do so within three weeks from the date on which the seafarer received the notification of the original decision (see PAA Article 29 and Section 15 of the Regulations).
13.3.3 THE APPELLATE BODY
The Appellate Body is described in Section 13 of the Regulations. The Appellate Body practices according to the PAA, Chapter VI, Articles 28-36, where the Appellate Body equals the Appellate Instance of the PAA.
The Appellate Body shall follow the rules in the PAA and their decision is final. The only way a decision by the Appellate Body can be challenged is through the courts.
13.4 REVIEW, EXEMPTION AND APPEAL
13.4.1 INTRODUCTION AND BACKGROUND
The seafarer’s Doctor can issue a health certificate with or without time limitations and\or restrictions or a certificate of unfitness (temporary or permanent). The seafarer can appeal against this decision or request an exemption by application to the appellate body concerning medical certificates for employees on Norwegian ships and mobile offshore units. The seafarer’s Doctor should know how to prepare the case for consideration by the Appellate Body.
The assessment of the health condition of the applicants and the risk assessment are described in other parts of this compendium.
13.4.2 THE SEAFARER’S DOCTOR’S DECISION
The seafarer’s Doctor shall collect all of the necessary information on the health condition of the applicant and his line of work that is required to be able to decide whether a health certificate can be
24
issued or not. This is as discussed previously and as per the statutory requirements of the Public Administration Act and the Health Personnel Act.
After the medical examination, if the seafarer’s Doctor finds that the seafarer meets the health requirements, he shall immediately issue a health certificate on a dedicated form. Alternatively, the seafarer’s Doctor may apply time limitations and/or restrictions to the certificate or issue a permanent, temporary or provisional declaration of unfitness. Restrictions may be made to the position held on board, the sailing area or as outlined in the Guidance for specific medical conditions. If it is thought that further restrictions are necessary the case must be referred to the Appellate Body.
Practically, this implies that the seafarer’s doctor after the examination may make one of these decisions:
Issue an unrestricted, unlimited health certificate with valid for the maximum time period.
Issue a health certificate with a limited time period or restricted with regards to a particular trade area or service on board.
Issue a certificate of unfitness (permanent, temporary or provisional)
In some cases the seafarer’s doctor will not issue any certificate, but will inform the applicant that a decision cannot be made until further information has been collected and request that the seafarer returns after a period of time. This is only likely to be an option if the doctor has a good relationship with the seafarer built on trust and the timescales involved are short. In most cases, a certificate of temporary unfitness should be issued, whilst the case is investigated.
13.4.3 THE APPLICANT’S POSS IBILITY TO HAVE DECISIONS MADE BY THE SEAFARER’S DOCTOR REVIEWED
If the seafarer does not agree with the Doctor’s decision, he has two options:
He may submit the case to Appellate Body for appeal
He may apply for an exemption It is the duty of the seafarer’s Doctor to inform the seafarer about his right to have his case reviewed by the Appellate Body and to assist him in this process. The Doctor must also advise the seafarer that it would be sensible to apply for exemption in cases where the health requirements are formally not met, but where his situation is such that it appears defensible, from a safety point of view, to give him a health certificate with conditions.
The regulations make it clear that a review of the individual decision taken by the seafarer’s Doctor shall be made by the Appellate Body. However, there is no formal impediment for a seafarer to see another seafarer’s Doctor for a second opinion. In this situation, Section 8 in the regulations states that the seafarer shall give information about his state of health as completely as possible. A fair and full interpretation of this would be that the seafarer should inform the second seafarer’s Doctor about the examination made by the other Doctor.
If a seafarer’s Doctor is approached in this way it would be preferable to recommend that the seafarer has his case reviewed by the Appellate Body. However a practical exemption from this “rule” or recommendation would be in a case where the seafarer presents new, objective information about his health condition(s) to a second Doctor, which was not available to the Doctor who made the first examination. In this situation a new decision from the second seafarer’s Doctor is defensible since new information is available. It is considered good practice for a seafarer’s Doctor to always review the decision made by the last seafarer’s Doctor seen by the patient before making their own decision.

25
13.4.4 APPEALS AND APPLICATIONS FOR EXEMPTIONS WITH THE APPELLATE BODY – CASE PREPARATION BY THE SEAFARER’S DOCTOR
If the seafarer wishes to appeal against the decision made by the seafarer’s Doctor, the appeal must be made within three weeks of the seafarer receiving notification of the decision, as described in the Public Administration Act (PAA).
If the seafarer wishes to apply for an exemption or if he wishes to make a general complaint the same procedure should be followed, but there is no deadline for when an application can be sent.
The Doctor must assist the seafarer in the process of appeal or exemption and practically, the case should be prepared as follows:
Ask the seafarer to write a letter to the Appellate Body/NMA in which he appeals the decision, or applies for an exemption.
Explain to the seafarer that he should send the letter to you (the seafarer’s Doctor) and that you will forward it to the Appellate Body.
On receipt of the appeal – reconsider your original decision. You may choose to issue a health certificate if there is information in the letter which indicates that the health requirements are indeed met. This is not usually relevant if the seafarer is applying for an exemption but may still be good practice.
Ensure that the case is clarified as thoroughly as possible for the Appellate Body. When forwarded it should contain:
i. Appeals’ document ii. Self-declaration
iii. Medical examination form / patient’s record iv. Job description and job tasks v. Relevant medical information from (consultant’s reports and the like)
vi. Copy of your information to the applicant regarding the decision and the justification
vii. Copy of your reconsideration viii. Your safety risk assessment and recommendation to the Appellate Body
If you feel that the seafarer should be granted an exemption you should make a statement to this effect and explain your reasons. Likewise if the seafarer has made an application for an exemption but you do not think this is reasonable you must say so, with justification.
13.4.5 CASE HANDLING BY THE APPELLATE BODY
The mandate of the Appellate Body is described in the first paragraph of Section 13 of the regulations:
“The appellate body shall base their decision on section 1 and the appendix of these Regulations when considering an application for exemption or an appeal against a decision made by a seafarer's doctor”
The Appellate Body is an administrative appeal body for appeals against decisions made by seafarer's Doctors. A decision made by the Appellate Body is an administrative decision pursuant to the Public Administration Act, and shall follow the rules of procedure set forth in the Act.
The Appellate Body has three members and consists of a medical practitioner who acts as the head of the Appellate Body, a trade union representative and a representative from the Norwegian Maritime Authority. The trade union representative must be knowledgeable about the occupational category to which the employee belongs.
26
Members of the Appellate Body have a duty of confidentiality regarding any information about personal matters that might emerge.
Once the appeal/request for exemption/complaint is received by the NMA it prepares the case administratively. The case is then handed over to the Appellate Body where it is reviewed from a medical and legal perspective. Once a decision is made it is then reviewed by the other members of the body. This is often done electronically although meetings are held as necessary.
Based on the documents received the Appellate Body independently considers the medical and administrative/legislative aspects of the case.
The Appellate Body may uphold the seafarer’s Doctor’s decision or it may decide that a health certificate can be issued with specific limitations and restrictions. Following a decision by the Appellate Body, the seafarer’s Doctor shall issue a certificate to this effect, and insert the restrictions and/or limitations specified by the Appellate Body. The Appellate Body does not itself issue certificates.
13.4.5.1 APPEALS AND COMPLAINTS
The handling of appeal and complaint cases is described in Section 15 of the Regulations and shall follow the requirements of the Public Administration Act.
The assessment in cases of Appeal will have two separate aspects:
Assessment as to whether the case consideration has been correct in accordance with the PAA.
Assessment as to whether the medical assessment has been justifiable and whether the decision is in accordance with the Regulations.
13.4.5.2 APPLICATIONS FOR EXEMPTIONS
When the seafarer applies for an exemption, the Appellate Body will consider whether the applicant meets the paramount requirements of Section 1 of the Regulations. The Appellate Body can never grant exemptions from this Section of the Regulations.
In Section 16 of the regulations it is stated that an exemption can only be granted when particular reasons exist and when safety considerations are still met. The Appellate Body may exempt an employee from one or more of the requirements of the Regulations if one of the following requirements is met:
It is established that the requirement is not a minimum requirement from a binding international standard, is not essential, and that the exemption is considered justifiable in terms of safety, cf. Section 1 of these Regulations.
It is established that the requirement is not a minimum requirement from a binding international standard and that compensating measures will maintain the same level of safety as required by these Regulations.
The Appellate Body will carry out an independent safety risk assessment based on the documentation provided by the seafarer’s Doctor.

27
14 TOPIC 5: INTRODUCTION TO MEDICAL SELECTION
14.1 DEFINITION
Medical selection is about picking the right individuals to carry out defined tasks on the basis of a medical assessment of their fitness in accordance with specific standards.
There is no official definition of this professional area, but it is clearly different from what is taught in medical school, and different from the tasks and daily life of a clinical practitioner.
To carry out the process of medical selection it is important to understand what is meant by fitness and to consider the different factors involved in the process of making a fitness decision. This compendium provides some of the information but this will be discussed in more depth during the course.
14.1.1 NEGATIVE SELECTION
The process of negative selection is to regard everybody as fit, and then exclude those with a medical condition who are judged unfit according to specific guidelines. The process is strictly medical, and concerned with medical conditions.
A negative selection method is completely dependent on finding a “medical condition”. By use of this method, you can conclude that you have not found that a person is unfit, but you cannot actually conclude that you have found him fit for a particular role or task. If you are actually going to demonstrate fitness, you have to add positive selection methods.
With negative selection the candidate is regarded as FIT, unless proven UNFIT.
On completion of this process you have demonstrated the fitness based on the absence of unfitness.
Those who are on disability pension will not qualify, and are regarded permanently unfit.
Those who are under occupational rehabilitation will be regarded as temporarily unfit in accordance with the Regulations. They might be able to work later on.
Some workers may have a loss of function which limits their ability to carry out certain parts of the job, but can manage others. In the case of seafarers these workers may be issued with a limited and restricted certificate. However the possibilities to adjust the job description and role on board ships are limited. Lean manning systems make it difficult to accept individuals with reduced performance, as this will overburden others, and sometimes lead to an unacceptable safety risk.
14.1.2 POSITIVE SELECTION
The process of positive selection starts with a position where you regard everybody as unfit. Then you select those who pass certain tests, and meet qualifying criteria. This is a physical and sometimes psychological process, more than a strict medical process.

28
With positive selection the candidate is regarded as UNFIT until proven FIT and on completion you have demonstrated fitness for a particular role or task. This process is used for the selection of candidates for military schools, police academies, fire brigade training etc. The medical standards for seafarers are largely based on negative selection, and in some areas positive selection is added (obesity, present neurological conditions, cardiovascular or pulmonary diseases and conditions etc.)
14.2 THE MEDICAL CONSULTATION
When undertaking a medical consultation for the purpose of selection there are a number of variables that must be considered. The consultation is different to that usually undertaken in other clinical situations.
14.2.1 THE ROLE OF THE DOCTOR
The role of the Doctor in medical selection is different from other roles that a physician may undertake and that may be more familiar to you. Depending on the role that a Doctor is undertaking he will view the person he is examining in a different way, will have a different focus for the consultation and will be working under different legislation, rules and regulations.
For example, the General Practitioner or primary care physician works under some sort of “Health & Care-Legislation”. In Norway that means the Health and Care Act. The individual coming to see him is in the role of being a “patient” and the GP focuses on the patient’s best interests. His tools are the medical condition(s), diagnoses and their treatment, perhaps also secondary or tertiary prevention.
The occupational physician works under the “Working Environment Legislation”. In Norway that means the Working Environment Act. The individual seeing him does this in the capacity of being an employee in the company where the Doctor is employed or contracted to do his work. The occupational physician focuses on the working environment (chemical, physical, psychological, social), and is looking for factors in the working environment that could harm the individual’s health and lead to a loss of performance in that individual. The real “patient” of the occupational physician is the working environment, and the individual is in a way both the target person and measuring instrument regarding the wellbeing of the working environment. The tools of the occupational physician are measures for the improvement of working conditions and individual protection of workers.
The seafarer’s Doctor works in accordance with the “Health Requirement Legislation”. The individual coming into his office is a candidate who hopes for a “pass” and the issuance of a medical certificate. The Doctor is going to assess whether certain health criteria are met, and decide whether the candidate shall pass or fail against those criteria. The tools of the Doctor are probability or likelihood

29
assessments, consequence analysis, assessment of risk to other people, to the ship, and lastly also to the candidate himself.
More examples could be mentioned, for example, Doctors working for insurers or for a national health and welfare administration. They have different approaches, different tasks, different ways of looking at the individuals, and different requirements on which to base their decisions.
The role of the doctor determines his mind-set, as described above.
Having several roles at the same time includes a danger of not being able to practise these roles appropriately, and a danger of confusing them. The individual may be unsure as to which role(s) the Doctor has, as the aims and objectives are different in each and in some cases may seem to oppose each other. Ensuring that both the seafarer and the Doctor are aware of the roles they have and that there are no conflicts of interest is key to a successful and open consultation.
14.3 STANDARDS AND CRITERIA
Medical selection standards and criteria vary. An individual with a certain condition may receive a different outcome or ‘result’ depending on which standards and criteria are used during the selection process.
Some standards are given by the industry, some by the authorities. Some are regional (e.g. European Union), others are bilateral (or trilateral, like the Norwegian-United Kingdom-Netherlands agreement for the acceptance of seafarer’s medical certificates), whilst some may be truly international, like the Guidelines on the Medical Examination of Seafarers from the ILO and IMO.
14.4 THE PURPOSE OF MEDICAL SELECTION
The purpose of the medical selection examination being undertaken may vary widely. It may be to:
• Protect the individual’s health • Ensure the performance of the worker • Ensure enough working force in the population • Avoid medical treatment on board ship • Avoid evacuation and repatriation • Avoid insurance claims • Ensure regularity of ship operations • Reduce unemployment • Identify future world champions
The perspective for the medical examination will vary according to the purpose of the medical selection process.
14.5 THE TIMELINE
A GP will give health advice taking into account the rest of the patient’s life. When guidelines for medical selection are developed they usually have a shorter and defined timeline i.e. how long the certificate to be issued is valid for.

30
A seafarer’s Doctor has a time horizon of a maximum of 2 years ahead. What is expected to happen in ten or twenty years’ time may be interesting but may well be irrelevant with regards to the decision whether or not to issue a medical certificate for a maximum of two years.
14.6 THE MEDICAL CONDITION
The medical condition is, of course, of the utmost importance. What is the likelihood of the person falling ill or suffering a complication or acute deterioration of a known disease during a certain period of time?
The General Practitioner will regard this likelihood as an “individual health risk” – which is the likelihood that the individual will suffer from some illness, medical incident, complication or similar. The risk is of falling ill and its impact on the patient.
The seafarer’s Doctor will look at this “individual health risk” as equal to the likelihood for an incident to occur, that could compromise the safety of the ship and people on board. The risk is connected to what happens to the ship, the crew, any passengers, the ship’s operation and to the individual themselves. It is not the mere question of falling ill. All of these added together make the “safety risk for the ship”.
It is challenging to combine the usual mind-set of looking at the “individual health risk” and the selection mind-set of the assessment of the “safety risk for the ship”. This is discussed further below.
14.7 JOB DEMANDS OF THE SEAFARER
Without knowledge of the job tasks and the responsibilities the seafarer is required to carry out, it is impossible to carry out an individual risk assessment. Job descriptions vary a lot.
Some understanding is quite general and there are common denominators, for example, for navigators and those working in the engine department or in the galley. However the actual tasks involved in a particular role do vary between the types of ship, different shipping companies, manning levels etc. A description of typical work tasks can be found in the Guidance, but we would highly recommend that you speak to the seafarer himself and discuss what tasks he is required to undertake and/or request a copy of his job description if necessary.
14.8 MITIGATING MEASURES
The likelihood of a medical incident occurring and the severity of the consequences i.e. the safety risk may for the ship be reduced by certain mitigating measures. This could be restrictions of working position, restrictions in where the seafarer may sail, limitation in the time the certificate is valid for, or that a medical certificates is issued with certain conditions as outlined for specific health conditions in the guidelines.
Setting restrictions, limitations and specific conditions for the medical certificate can sometimes mitigate the risk sufficiently to make it possible for the doctor to issue a medical certificate.
31
15 TOPIC 6: MEDICAL SELECTION – ASSESSMENT OF THE SAFETY RISK
15.1 THE PURPOSE OF THE MEDICAL EXAMINATION OF SEAFARERS ACCORDING TO THE NORWEGIAN REGULATIONS
The purpose is given in § 1 of the Regulation on health requirements for the medical examination of employees on Norwegian ships and mobile offshore units
§1 Purpose
“These Regulations shall ensure that the employee is medically fit for service on board, is not suffering from a medical condition likely to be aggravated by service at sea or to endanger the health and safety of other persons on board.”
The regulation is first and foremost there to ensure safety. It is about safety for other workers and for the safe running of the ship or vessel but also to ensure that the seafarer’s condition is not exacerbated by being at sea.
Of course if the seafarer’s condition was to deteriorate and he was unable to perform his regular or safety duties this would potentially represent a danger to others and to the safe running of the ship/vessel in an environment where everybody is dependent on each other and where most of the work carries great responsibility. An error may have serious consequences and even if the consequences of the disease do not affect others directly, they may do so indirectly.
15.2 ASSESSMENT OF THE SAFETY RISK RELATED TO THE MEDICAL CONDITION
15.2.1 POSSIBLE MEDICAL INCIDENTS
Based on knowledge about the individual candidate’s medical history and examination, the seafarer’s doctor will be able to identify the medical incidents that may be expected to occur within the validity period of the certificate i.e. a maximum of two years ahead.
15.2.2 THE LIKELIHOOD OF A MEDICAL INCIDENT OCCURRING DURING THE VALIDITY PERIOD OF THE CERTIFICATE
It is then necessary to estimate how likely it is that such an incident/complication/acute deterioration will occur over the next two years in any person with the same illness or diagnosis.
Unfortunately very few studies have been carried out with such endpoints. Studies done on survival, rehospitalization, reoperations or other interventions e.g. another heart attack or new epileptic fit(s) are often carried out with a different perspective, and completely without this aspect of risk analysis.
The end-points we are interested in include that the seafarer suffers a medical problem with the result that he:
• Can no longer carry out his duties • has to be replaced by others • must be taken out of work, with the result of overburdening of others • needs medical treatment and medical care on board • needs evacuation • can make mistakes or errors which increase the risk of injury to people and damage to the
equipment/ship/operations.

32
That is, we want to know the likelihood/probability that the seafarer’s condition can imply a safety threat.
Readmission to hospitals, re-surgery and other re-episodes do not necessarily reflect this and studies done on elderly people do not necessarily reflect the epidemiology of people at a working age. Equally studies done in some populations may not reflect the prevalence or incidence of a particular disease in another population. However, when looking under such subheadings as the natural course, prognosis, complications, follow-up, epidemiology, side effects, etc., it is still possible to find something of interest. However, care must be taken when extrapolating or transferring results.
The most recent information can be obtained from review databases like UpToDate, BMJ Best Practice, and The Cochrane Database or similar. The Guidance to the regulations will also provide some evidence useful for the risk assessment
15.2.3 THE LIKELIHOOD OF A MEDICAL INCIDENT OCCURRING IN THIS PARTICULAR SEAFARER
Based on the knowledge about the individual employee, achieved by self-declaration, the medical history, medical examination, medical reports, specialist advice, and laboratory findings etc., the seafarers Doctor will be able to assess the likelihood of an incident occurring in this seafarer as compared to the average for the group of people who have the same diagnosis.
Age, sex, chronicity of the condition, stage and grading, comorbidity, response to treatment and other characteristics of a clinical case, may all influence the individual likelihood, and convince the Doctor that the candidate has a higher or lower probability than average.
15.2.3.1 REQUESTING SPECIALIST ADVICE
Specialist advice may be useful at this point and also may help to ensure that “case is clarified as thoroughly as possible before any administrative decision is rendered” as required by the PAA. However it is important to be clear about the role of the specialist and to ask the ‘right’ question to provide the information you require to assist in the risk assessment. Asking simply for a copy of the medical reports may well not be useful in this setting. It is important to ask what you need to know to complete the risk assessment and to provide the specialist with the background knowledge of the seafarer’s working and living conditions to enable him to answer the questions asked.
More information can be found in a paper from the NCMDM and published in International Maritime Health2. It must always be remembered that specialist input forms a part of the risk assessment and we are not asking the specialist to make the final decision as to whether or not the seafarer is fit to work at sea. That is the decision of the seafarer’s Doctor.
2 Stannard SL. Seeking specialist advice in the context of the pre-employment medical examination. Getting the ‘right’ answer to the ‘right’
question. International, Maritime Health 2016;67, 4:185-186

33
15.3 THE CONSEQUENCES OF A MEDICAL INCIDENT IN THE SPECIFIC POSITION OF THE SEAFARER
It is important that the seafarer’s doctor has familiarized himself with the job tasks for the individual candidate. Consequences of a medical incident for the safety of the seafarer, other crew and the ship are highly dependent on the actual position and job tasks of concern. This assessment must include the routine job tasks expected of the seafarer’s position but also any emergency duties he will be expected to carry out e.g. firefighting.
Some important questions to ask include but are not limited to:
Will the candidate have to
• climb long ladders? • work at heights? • operate dangerous machinery and equipment? • work safely in a noisy environment? • monitor instruments for prolonged periods of time and respond adequately to alarms? • work alone for extended periods of time? • work in monotonous and tedious situations? • work shifts? • carry out physically demanding job tasks? • discern colours, either lanterns, lights, cable codes or screen colour codes? • work in electromagnetic fields? • carry out extraordinary tasks in cases of evacuation? • master a Man Over Board boat? • carry out fire-fighting with breathing device? • be a part of a rescue team?
15.3.1 TESTING OF PHYSICAL CAPABILITY – THE ADDITIONAL POSITIVE SELECTION
The testing of physical capacity is indicated in some cases, e.g. in workers with known cardiovascular or pulmonary disease, or obesity. The need for the seafarer to enter a confined space and his ability to do so must also be taken into consideration when deciding on the need for additional testing.
The seafarer’s doctor is free to decide which methods to use, as long as he/she uses standardized methods which can be repeated. More information is given in the Guidance.
15.4 CALCULATION OF UN-MITIGATED SAFETY RISK
After these steps have been completed, it is possible to “calculate” the un-mitigated safety risk.
During work on board a ship, an individual medical incident is far more than an individual experiencing ill health due to that medical incident occurring. It has to do with other people on board and the safe operation of the ship. The “individual health risk” as discussed earlier should be regarded as equal to the “likelihood” of an incident occurring. The consequences are not primarily individual, but also relate to ship, crew and passengers.
This is why we use the word “LIKELIHOOD” (and not “health risk”) for the probability that an individual will suffer from a medical incident, and “CONSEQUENCES” for what may happen to the ship, operation, crew and passengers, in addition to the seafarer, when or if this incident happens. “RISK” in our
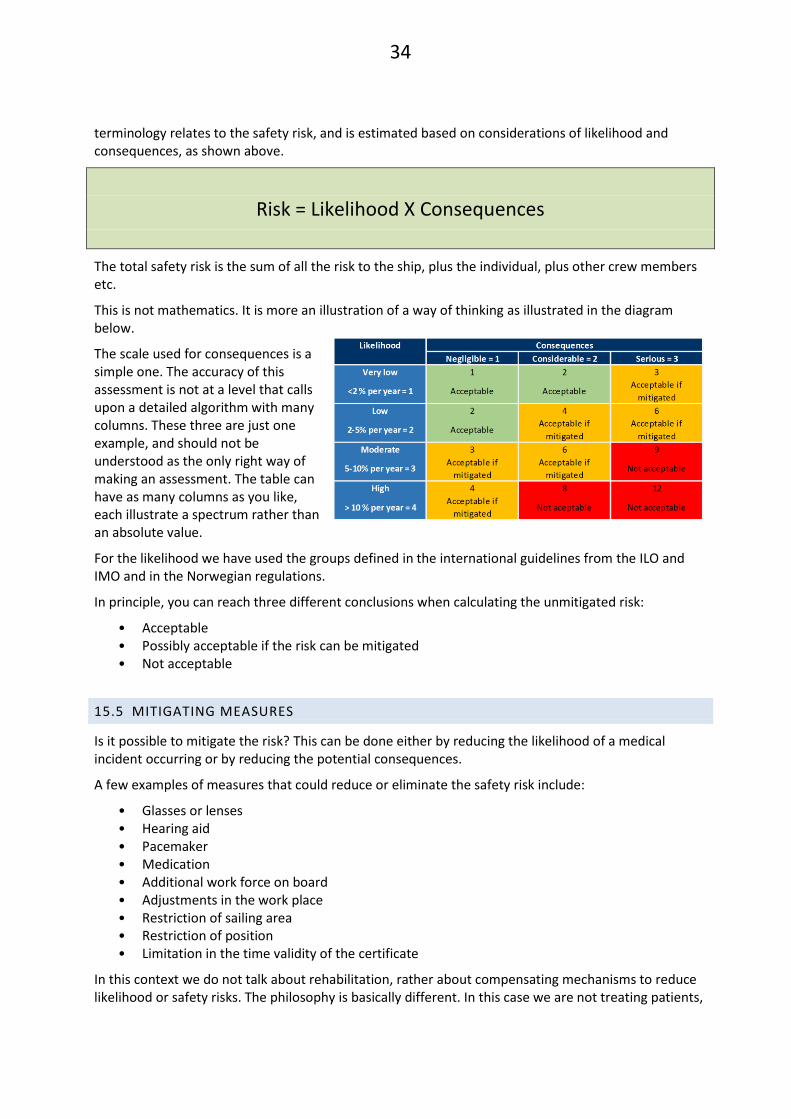
34
terminology relates to the safety risk, and is estimated based on considerations of likelihood and consequences, as shown above.
Risk = Likelihood X Consequences
The total safety risk is the sum of all the risk to the ship, plus the individual, plus other crew members etc.
This is not mathematics. It is more an illustration of a way of thinking as illustrated in the diagram below.
The scale used for consequences is a simple one. The accuracy of this assessment is not at a level that calls upon a detailed algorithm with many columns. These three are just one example, and should not be understood as the only right way of making an assessment. The table can have as many columns as you like, each illustrate a spectrum rather than an absolute value.
For the likelihood we have used the groups defined in the international guidelines from the ILO and IMO and in the Norwegian regulations.
In principle, you can reach three different conclusions when calculating the unmitigated risk:
• Acceptable • Possibly acceptable if the risk can be mitigated • Not acceptable
15.5 MITIGATING MEASURES
Is it possible to mitigate the risk? This can be done either by reducing the likelihood of a medical incident occurring or by reducing the potential consequences.
A few examples of measures that could reduce or eliminate the safety risk include:
• Glasses or lenses • Hearing aid • Pacemaker • Medication • Additional work force on board • Adjustments in the work place • Restriction of sailing area • Restriction of position • Limitation in the time validity of the certificate
In this context we do not talk about rehabilitation, rather about compensating mechanisms to reduce likelihood or safety risks. The philosophy is basically different. In this case we are not treating patients,

35
but judging the potential safety risk of the candidates at certain working places against a set of standards and criteria in the Regulations.
A seafarer’s Doctor can place restrictions on the position the seafarer takes on board, on the time the certificate is valid for and in certain other specific medical conditions as outlined in the regulations. If any additional mitigating measures or restrictions are required the case must be referred to the Appellate Body.
15.6 OVERALL EVALUATION OF THE SAFETY RISK
Taking mitigating measures into account, the “net” safety risk needs to be evaluated. Has the risk been reduced to an acceptable level?
How does your evaluation fit with the requirements of the Regulations?
15.7 CONCLUSION AND JUSTIFICATION
Your conclusion shall be in writing, and should be done at the same time as you issue the medical certificate. It is difficult to compose the justification afterwards, and the seafarer has the right to receive your justification of the decision at the same time as your decision is given.
Your conclusion shall contain:
• The legal basis for your decision in the Regulations • The medical justification for your assessment and conclusion
It may be useful to outline your thought process in a systematic way such as the one shown here.
A. Possible incidents (relate to diagnosis and medication)
B. Individual Likelihood
C. Consequences of an incident
D. Risk calculation
E. Possible mitigation
F. Risk evaluation
G. Conclusion

36
16 TOPIC 7: VISION: CONTRAST, NIGHT, COLOUR, DISTANCE, NEAR VISION AND VISUAL FIELDS
This lecture is part of the taught course.
Recommended reading before the course:
• Regulations of 5 June 2014 No. 805 on medical examination of employees on Norwegian ships and mobile offshore units
o Attachment A • Guidance to the Regulations
o Chapter 13: Vision • Handbook for seafarer medical examiners
o Chapter 4: Vision
The requirements for vision for employees on Norwegian ships and mobile offshore units are described in Attachment A and further elaborated in the Guidance.
It is important to note that the minimum requirements for vision for seafarers are set in a binding international standard, and that the Appellate Body cannot grant dispensation from those minimum requirements.
The requirements are listed in the STCW-Convention Table A-I/9.
17 TOPIC 8: HEARING AND HEARING REQUIREMENTS
The topic will NOT be covered during the taught course. It may, however, be tested during the final course test.
Recommended reading:
• Regulations of 5 June 2014 No. 805 on medical examination of employees on Norwegian ships and mobile offshore units
o Attachment B: Hearing • Guidance to the Regulations
o Chapter 14: Hearing. • Handbook for seafarer medical examiners
o Chapter 5: Hearing.
Requirements for hearing capacity are based on the STCW Convention from the IMO and the Maritime Labour Convention 2006 from the ILO. More information is provided in the Guidance.
18 TOPIC 9: DIABETES AND OTHER ENDOCRINE DISEASES
The topic will be included as a clinical case discussion during the taught course.
Recommended reading:
• Regulations of 5 June 2014 No. 805 on medical examination of employees on Norwegian ships and mobile offshore units
o Attachment E, ICD code E00-90 Endocrine, nutritional and metabolic disease • Guidance to the Regulations
o Chapter 17.5: E00-90 Endocrine, nutritional and metabolic disease

37
• Handbook for seafarer medical examiners o Chapter 12: Diabetes and its treatment
19 TOPIC 10: EPILEPSY, LOSS OF CONSCIOUSNESS, EPILEPSY, ALTERED AWARENESS AND SLEEP DISORDERS
The topic will be included as a clinical case discussion during the taught course.
Recommended reading:
• Regulations of 5 June 2014 No. 805 on medical examination of employees on Norwegian ships and mobile offshore units
o Attachment E, ICD code G40-47 Diseases of the nervous system • Guidance to the Regulations
o Chapter 17.7 ICD code G40-47 Diseases of the nervous system • Handbook for seafarer medical examiners
o Chapter 15: Loss of consciousness, altered awareness, epilepsy and sleep disorder (ILO/IMO Guidelines Appendix E G40-47)
20 TOPIC 11: CHRONIC NEUROLOGICAL DISEASES
The topic will be included as a clinical case discussion during the taught course.
Recommended reading:
• Regulations of 5 June 2014 No. 805 on medical examination of employees on Norwegian ships and mobile offshore units
o Attachment E, ICD code G00-99 Other organic neurological diseases • Guidance to the Regulations
o Chapter 17.7.5 ICD code G00-99 Other organic neurological diseases
21 TOPIC 12: ALCOHOL AND DRUG ABUSE
The topic will be included as a clinical case discussion during the taught course. It may, however, be tested during the final course test.
Recommended reading:
• Regulations of 5 June 2014 No. 805 on medical examination of employees on Norwegian ships and mobile offshore units
o Attachment E, ICD code F10, F11-19 • Guidance to the Regulations
o Chapter 17.6.1: Alcohol abuse and dependency o Chapter 17.6.2: Drug dependence/persistent substance abuse
• Handbook for seafarer medical examiners o Chapter 14: Mental disorders, including cognitive and behavioural impairment, alcohol
and substance misuse (ILO/IMO Guidelines Appendix E G00-99)
38
22 TOPIC 13A: PSYCHIATRY - HOMEWORK
22.1 HOMEWORK CASE:
As discussed earlier, this case should be prepared before the taught course using the approach in Chapter 15 and you must:
Answer the multiple choice question regarding this case
Be prepared to present the case and to discuss your decision and justification (you may wish to use the table in Section 15.7)
22.1.1 SELF DECLARATION – MEDICAL HISTORY AS TOLD BY THE CANDIDATE
The candidate is a 48 year old male Chief Engineer, currently without a job contract on a ship following medical treatment. He wants to go to sea again. On the self-declaration he has marked ‘yes’ to the question regarding psychiatric problems. When you discuss this in more detail he tells you that he had a psychological disorder 12 and 3 years ago, both times in connection with adultery. He received appropriate support from the health service the first time, but the second time he feels he was not listened to.
He tells you that 3 years ago, whilst he was cleaning up after a fire on board ship, he got a telephone call from his step daughter with information which gave him a “shock”. He did not feel well, needed some fresh air, stepped outside but fell over board and into the sea.
He states that the accident report from the master about him falling over board, contained several errors. It seems that there was a conflict between the seafarer and the master, and the seafarer suggests that this could be the reason why the master wrote these things in the report.
He was disappointed by the employer after this accident. He spoke to some of the crew members after the accident, and he advises that they wished him a quick recovery and wanted him back on the ship. They had not found him to be difficult or paranoid. Only the master had got this impression of him.
In the psychiatric department at Hospital A, there were so many different doctors dealing with him, that he questions whether any of them obtained sufficient information and observation time to reach on a diagnosis. He states that he was given the diagnosis of Bipolar I at the Hospital A.
He has researched the diagnosis on the internet and understands that it is a serious illness and can be inherited. None of his family has had a similar diagnosis. People have commented that he has recovered very quickly after having been given such a diagnosis. He felt that the psychiatric department was not a good place to be. He did not receive appropriate treatment for his concurrent somatic illness, and he was threatened that he would lose his job if he did not obey staff as requested. He got the impression that he needed to agree that he had bipolar disease, and that the doctors and nurses behaved more gently after he did so.
He was told that he could continue work at sea.
One year ago, two years after the initial diagnosis was made, he asked for a second opinion. The reaction from the psychiatric department at Hospital A was that it would not serve any purpose, as the diagnosis was correct. However, he applied for a second opinion through his GP.
39
He went to the psychiatric department at Hospital B, but they sent all their papers to Hospital A, where he got an appointment with the Chief Consultant. The Chief Consultant asked him to reduce and then stop the medicines.
He has now been off medication for 1 year. His experience is that nobody wants to be involved, and his application for a second opinion led to nothing.
He has searched the web and found that 69% who have a diagnosis of bipolar disease are diagnosed incorrectly.
He has no problems with alcohol, is almost a total abstainer. He is not depressed, has good relations with everybody, is in a good mood, does not suffer from anxiety and has no metabolic disease. He wants someone to assess him and the diagnosis.
While he was on sick leave, he contacted another seafarer’s Doctor, and got the impression that a time limited medical certificate, restricted to near coastal traffic, and no safety function on board, would be the best he could expect. He asks himself what kind of a job that would be for him. He has decided that he does not want to go back to that seafarer’s Doctor, and wants you to assess the case instead.
For the time being, he has been off medication for one year, in his own opinion he is completely stable, and he asks for a medical certificate without restrictions or limitations, so that he can start working again.
You feel that you need more information, and seek that from several sources.
22.1.2 FROM THE PREVIOUS APPROVED SEAFARERS DOCTORS
The seafarer’s Doctor sends copies of earlier medical reports which confirm three earlier hospitalizations due to a psychotic condition because of bipolar disease.
He also attaches a specialist report which cannot confirm that the likelihood for recurrence is low.
He concludes by saying that as far as he can understand, the candidate should be declared permanently unfit, but there remains a possibility to seek an exemption from the Appellate Body.
22.1.3 MEDICAL REPORT FROM THE DEPARTMENT OF PSYCHIATRY, HOSPITAL A – THREE YEARS AGO
Diagnosis: Bipolar affective disease, manic episode, no psychotic symptoms
He was admitted with the diagnosis of mania. After being discharged from the hospital, the situation again escalated, with clear symptoms of mania without psychosis. Nine years prior to this admission he had a similar manic episode. At that time, he worked as a seafarer on a supply-ship off the coast of Brazil, five weeks on and five weeks off.
On the admission three years ago he was compulsorily detained for two months under the suspicion of a manic episode, but was transferred to voluntary hospitalization when he was considered to have had an adequate reaction to treatment and to be in a neutral emotional state. As part of the same admission he was then transferred to the surgical department for management of an acute cholecystitis. He did not want to go back to the psychiatric ward after somatic treatment.
During recovery from surgery, he developed manic symptoms requiring treatment. The seafarer regards this as a reaction to a chronic somatic illness that needed treatment. He has realized that he has a bipolar affective condition, and has received advice on a structured and regular conduct of life. At discharge he showed a neutral emotional state, no signs of hypomania or mania, and without psychotic symptoms or signs.
40
Medication on discharge from hospital: Orfiril (Valproate) and Zyprexa (Olanzapine).
22.1.4 FROM THE DEPARTMENT OF PSYCHIATRY (HOSPITAL A) – 3 MONTHS AFTER THE DISCHARGE MENTIONED ABOVE
He was seen at the outpatient clinic three times after discharge from the hospital. He attended appointments on time, demonstrated good insight into his own condition, demonstrated a stable and neutral emotional state, without signs of depression, mania or psychotic symptoms.
He got his driver’s licence back after dispensation from the County Governor and was on sick leave from his work on a supply-ship. The employer had not been able to find him work ashore, and he is not interested in that anyway. He wants to resume his work on board ship.
Throughout the period he was adequate and stable, and it is difficult to argue against a return to his usual work. He described that the possibilities are good for regular sleeping periods and regular meals on board, and he does not think that the job is stressful.
The conflict with his former wife is past. He thinks that was the reason why he got the episode of mania 6 months ago. There should be nothing now that will cause problems on return to his regular job. He needs to clarify with a seafarer’s Doctor, who knows the rules better regarding what can be allowed for service at sea.
22.1.5 FROM THE DEPARTMENT OF PSYCHIATRY (HOSPITAL A) – 2 YEARS AGO
The report confirms that he has been given a diagnosis of bipolar disease type I. He was hospitalized one year previously because of manic symptoms. Earlier he was admitted to hospital ten years ago because of a manic episode, and allegedly functioned well without medication in the period between the hospitalizations.
He is taking Orfiril (Valproate) with good effect. It is difficult to estimate the risk of a relapse of episodes of mania. He claims that he has not had any depressive episodes. During follow-up he demonstrated insight into his own condition, and was motivated for continued medication.
22.1.6 FROM THE CHIEF CONSULTANT, DEPARTMENT OF PSYCHIATRY, HOSPITAL A – RECENTLY
The Chief Consultant is summarising the case after the candidate requested a second opinion from the Chief Consultant at Hospital B, who has looked through the complete medical record of 48 pages from Hospital A, and stated his opinion:
• It seems quite clear that the patient is vulnerable for near psychotic or psychotic reactions in the form of mania if he gets heavy rational strains at home at the same time as he is doing a demanding job. An alternative explanation on his condition is agitated depression, which sometimes can be very difficult to discern from mania.
• The late onset (36 years old) of mania is relatively rare, and often has a somatic cause. MRI of his brain is, however, normal.
• He was thoroughly examined. He had a cholecystitis with a CRP above 300 on the latest admission.
• The fact that he has been healthy until 36 years of age, and had no problems in the nine years between the two admissions 12 and three years ago, is the reason why the Chief Consultant is in doubt, as to whether or not it is justifiable to burden him with psycho-pharmaceuticals like Valproate.
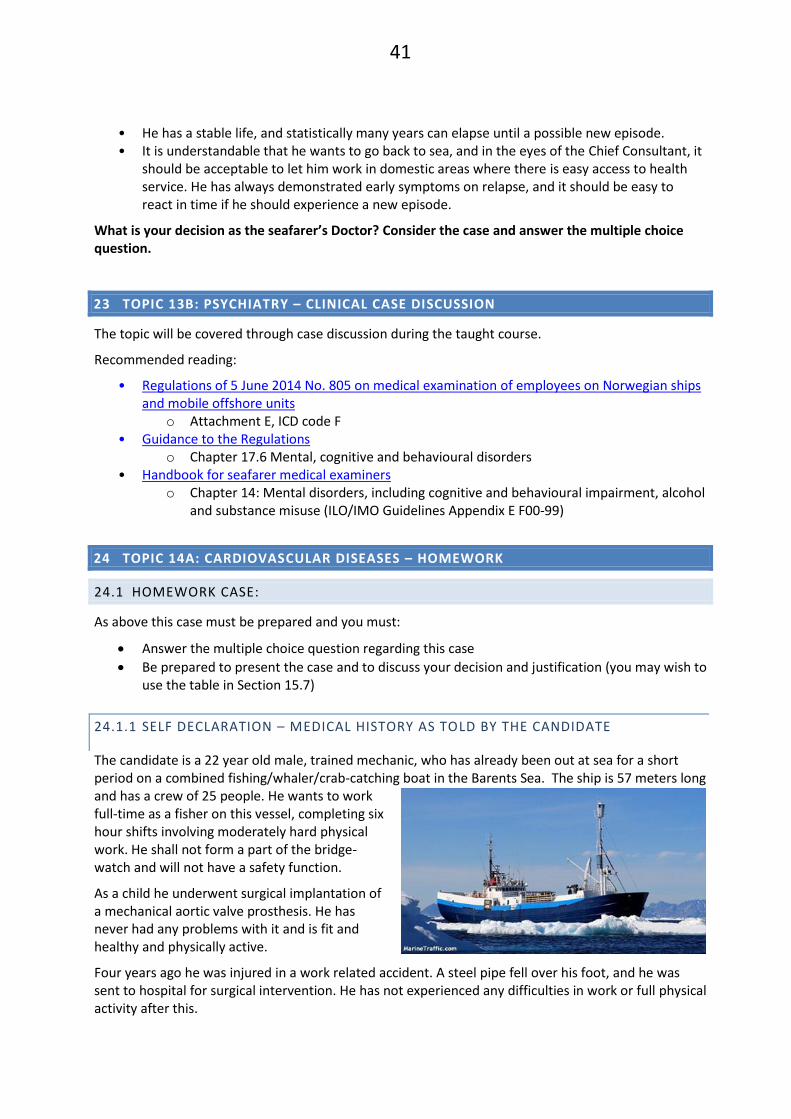
41
• He has a stable life, and statistically many years can elapse until a possible new episode. • It is understandable that he wants to go back to sea, and in the eyes of the Chief Consultant, it
should be acceptable to let him work in domestic areas where there is easy access to health service. He has always demonstrated early symptoms on relapse, and it should be easy to react in time if he should experience a new episode.
What is your decision as the seafarer’s Doctor? Consider the case and answer the multiple choice question.
23 TOPIC 13B: PSYCHIATRY – CLINICAL CASE DISCUSSION
The topic will be covered through case discussion during the taught course.
Recommended reading:
• Regulations of 5 June 2014 No. 805 on medical examination of employees on Norwegian ships and mobile offshore units
o Attachment E, ICD code F • Guidance to the Regulations
o Chapter 17.6 Mental, cognitive and behavioural disorders • Handbook for seafarer medical examiners
o Chapter 14: Mental disorders, including cognitive and behavioural impairment, alcohol and substance misuse (ILO/IMO Guidelines Appendix E F00-99)
24 TOPIC 14A: CARDIOVASCULAR DISEASES – HOMEWORK
24.1 HOMEWORK CASE:
As above this case must be prepared and you must:
Answer the multiple choice question regarding this case
Be prepared to present the case and to discuss your decision and justification (you may wish to use the table in Section 15.7)
24.1.1 SELF DECLARATION – MEDICAL HISTORY AS TOLD BY THE CANDIDATE
The candidate is a 22 year old male, trained mechanic, who has already been out at sea for a short period on a combined fishing/whaler/crab-catching boat in the Barents Sea. The ship is 57 meters long and has a crew of 25 people. He wants to work full-time as a fisher on this vessel, completing six hour shifts involving moderately hard physical work. He shall not form a part of the bridge-watch and will not have a safety function.
As a child he underwent surgical implantation of a mechanical aortic valve prosthesis. He has never had any problems with it and is fit and healthy and physically active.
Four years ago he was injured in a work related accident. A steel pipe fell over his foot, and he was sent to hospital for surgical intervention. He has not experienced any difficulties in work or full physical activity after this.

42
He has always been physically active, playing football and different other types of sport. In recent years he has been going to an exercise studio for weight-lifting and physical conditioning.
He is on medication of warfarin and omeprazole, and wears contact lenses of – 3,75 on both eyes.
24.1.2 WHAT YOU FIND IN THE MEDICAL RECORDS
He was born with a congenital aortic stenosis, and underwent valvotomy 22 years ago. He then had a mechanical aortic valve prosthesis 14 years ago. He has follow-up by a cardiologist once a year; his last appointment was one month ago. He measures his own INR and adjusts the dosage of warfarin himself. His weekly dose is 33 tablets, and his INR level should be kept in the range 2.5-3.5. He only rarely checks the INR with the GP.
Eight months ago he was admitted to hospital because of left sided paresis. An MRI scan showed no abnormality and the symptoms were considered to be due to a transient ischaemic attack, (TIA), secondary to a low INR and mechanical aortic valve prosthesis.
He suffered a compartment syndrome in his left leg three years ago and required a skin transplant afterwards. There are no ongoing sequelae.
He has a history of a hiatus hernia and gastro oesophageal reflux problems for which he takes omeprazole on demand. He reports that this is only occasionally.
On examination his height is 183 cm weight 90kg and BMI 26,9.
On auscultation of his heart the click from the aortic valves can be heard without a stethoscope. He has a regular pulse. Otherwise there are no abnormal findings on general medical examination of vision (wearing lenses) and hearing.
24.1.3 INFORMATION FROM THE CARDIOLOGIST – ONE MONTH AGO
The report confirms the diagnosis of congenital aortic stenosis, with a valvotomy 22 years ago and an implanted mechanical valve 14 years ago. There have been no problems with the valve and his INR is stable. His blood pressure is 130/70 pulse 48 and regular. Auscultation reveals a sharp valve click with a hoarse systolic murmur that can be heard over the whole precordial area. There is no ankle oedema.
Echocardiography shows a normally functioning left ventricle and an implanted aortic valve. Doppler studies show a gradient of 24 mmHg over the aortic valve, and a modest insufficiency. ECG shows sinus bradycardia.
Assessment: Unchanged gradient. The recommendation is for repeat assessment in 12 months.
24.1.4 MEDICAL REPORT FROM THE DEPARTMENT OF NEUROLOGY, 8 MONTHS AGO
Diagnosis: Unspecified transitory cerebral ischaemic attack (TIA)
Aortic valve mechanic implant, anticoagulant user (ongoing).
He was admitted after three days of an acute pulsating headache, followed by a light paresis in the left upper and lower extremities and problems with speech. The symptoms on the left side fluctuated before spontaneous regression after three hours although his headache continued. He was admitted with the suspicion of a TIA.
43
His BP was 128/71 with normal findings on somatic medical examination, including neurological examination. His INR was 1.4 the day after admission, and 2.4 on the second day. A CT and MRI of his head showed no pathology.
What is your decision as the seafarer’s Doctor? Consider the case , answer the multiple choice question and complete the table outlining your thought process and decision.
25 TOPIC 14B: CARDIOVASCULAR DISEASE – CLINICAL CASE DISCUSSION
The topic will be covered through case discussion during the taught course.
Recommended reading:
• Regulations of 5 June 2014 No. 805 on medical examination of employees on Norwegian ships and mobile offshore units
o Attachment E, ICD code I 00-99 • Guidance to the Regulations
o Chapter 17.9 Diseases of the circulatory system • Handbook for seafarer medical examiners
o Chapter 17: Cardiac events
26 TOPIC 15: LUNGS AND AIRWAYS - CLINICAL CASE DISCUSSION
The topic will be covered through case discussion during the taught course.
Recommended reading:
• Regulations of 5 June 2014 No. 805 on medical examination of employees on Norwegian ships and mobile offshore units
o Attachment E, ICD code J00-99 Diseases of the Respiratory system • Guidance to the Regulations
o Chapter 17.10 Diseases of the Respiratory system • Handbook for seafarer medical examiners
o Chapter 8: Pulmonary Tuberculosis (PTB) o Chapter 18: Asthma
27 TOPIC 16: GASTROINTESTINAL DISEASE – CLINICAL CASE DISCUSSION
The topic will be covered through case discussion during the taught course.
Recommended reading:
• Regulations of 5 June 2014 No. 805 on medical examination of employees on Norwegian ships and mobile offshore units
o Attachment E, ICD code K 00-99 • Guidance to the Regulations
o Chapter 17.11 Digestive system • Handbook for seafarer medical examiners
o Does not discuss these conditions

44
28 TOPIC 17: CANCER AND OTHER MALIGNANCIES
The topic will NOT be covered during the taught course. It may, however, be tested during the final course test.
Recommended reading:
• Regulations of 5 June 2014 No. 805 on medical examination of employees on Norwegian ships and mobile offshore units
o Attachment E, ICD code C00- D48 • Guidance to the Regulations
o Chapter 17.3 Neoplasms • Handbook for seafarer medical examiners
o Chapter 11: Cancer, including sarcoma, leukemia etc.
29 TOPIC 18: PHYSICAL REQUIREMENTS AND PHYSICAL TESTING
The topic will NOT be covered specifically during the taught course but may be discussed as part of other case discussions. It may also be tested during the final course test.
Recommended reading:
• Regulations of 5 June 2014 No. 805 on medical examination of employees on Norwegian ships and mobile offshore units
o Attachment C: Physical capability requirements • Guidance to the Regulations
o Chapter 15: Physical capability requirements • Handbook for seafarer medical examiners
o Chapter 6: Assessment of physical capabilities
30 TOPIC 19: OBESITY – CLINICAL CASE DISCUSSION
The topic will be covered through case discussion during the taught course.
To read:
• Regulations of 5 June 2014 No. 805 on medical examination of employees on Norwegian ships and mobile offshore units
o Attachment C: Physical capability requirements o Attachment E: ICD-code E65-68
• Guidance to the Regulations o Chapter 17.5.3 Obesity and overweight
• Handbook for seafarer medical examiners o Chapter 12: Obesity
45
31 TOPIC 20: UROGENITAL CONDITIONS
The topic will NOT be covered during the taught course. It may, however, be tested during the final course test.
To read:
• Regulations of 5 June 2014 No. 805 on medical examination of employees on Norwegian ships and mobile offshore units
o Attachment E, N00-N17, N03-05, N18-19 • Guidance to the Regulations
o Chapter 17.13.5 • Handbook for seafarer medical examiners
o Chapter Urine testing abnormalities
32 TOPIC 21: INFECTIOUS DISEASES AND VACCINATIONS
The topic will NOT be covered through the taught course. It may, however, be tested during the final course test.
Recommended reading:
• Regulations of 5 June 2014 No. 805 on medical examination of employees on Norwegian ships and mobile offshore units
o Attachment E, ICD code A00-B99 Infectious and parasitic diseases • Guidance to the Regulations
o Chapter 17.2.1-17.2.7 • Handbook for seafarer medical examiners
o Chapter 9: Infections transmitted in body fluids: HIV o Chapter 10: Infections transmitted in body fluids: Hepatatis (non A)
33 TOPIC 22: ORAL AND DENTAL DISESASES
The topic will NOT be covered during the taught course. It may, however, be tested during the final course test.
Recommended reading:
• Regulations of 5 June 2014 No. 805 on medical examination of employees on Norwegian ships and mobile offshore units
o Attachment E, ICD code K00-93 Gastrointestinal diseases • Guidance to the Regulations
o Chapter 17.11.1 • Handbook for seafarer medical examiners
o Chapter 19: Oral Health and dental inspection

46
34 TOPIC 23: MEDICATION
The topic will be covered through case discussion during the taught course.
Recommended reading:
• Regulations of 5 June 2014 No. 805 on medical examination of employees on Norwegian ships and mobile offshore units
o Attachment D: Medication • Guidance to the Regulations
o Chapter 16: Use of medication • Handbook for seafarer medical examiners
o Chapter 4: Medication
35 TOPIC 24: ALLERGIES
The topic will NOT be covered through case discussion during the taught course. It may, however, be tested during the final course test.
Recommended reading:
• Regulations of 5 June 2014 No. 805 on medical examination of employees on Norwegian ships and mobile offshore units
o Attachment E, General, T78, Z88 • Guidance to the Regulations
o Chapter 17.15.12 • Handbook for seafarer medical examiners
o Chapter 21: Allergies
36 TOPIC 25: DISEASES OF THE BLOOD AND BLOODFORMING ORGANS
The topic will NOT be covered through case discussion during the taught course. It may, however, be tested during the final course test.
Recommended reading:
• Regulations of 5 June 2014 No. 805 on medical examination of employees on Norwegian ships and mobile offshore units
o Attachment E, D50-89 • Guidance to the Regulations
o Chapter 17.4 D50-89 • Handbook for seafarer medical examiners
o Not mentioned in the book. Some under Chapter 11 (Leukeamia)

47
37 TOPIC 26: QUESTIONS, DISCUSSION, SUMMING UP
At the end of each day there will be a short summary session and the possibility to pose questions and discuss matters of interest.
38 COURSE EVALUATION
At the end of the course candidates are requested to provide feedback on the course which is reviewed and passed to the NMA.
39 FINAL COURSE TEST
The course test will last for up to 1 ½ hours (90 minutes). Altogether there are 20 questions. You may leave when you have completed the test.
48
40 APPENDICES
40.1 APPENDIX 1 – ASSESSMENT OF MEDICAL FITNESS FORM (TO FORM PART OF THE SEAFARER’S MEDICAL RECORD)
This form can be found at: https://portal.sjofartsdir.no/pdf/KS-0497%20Helseunders%C3%B8kelse%20ENG.pdf

49

50
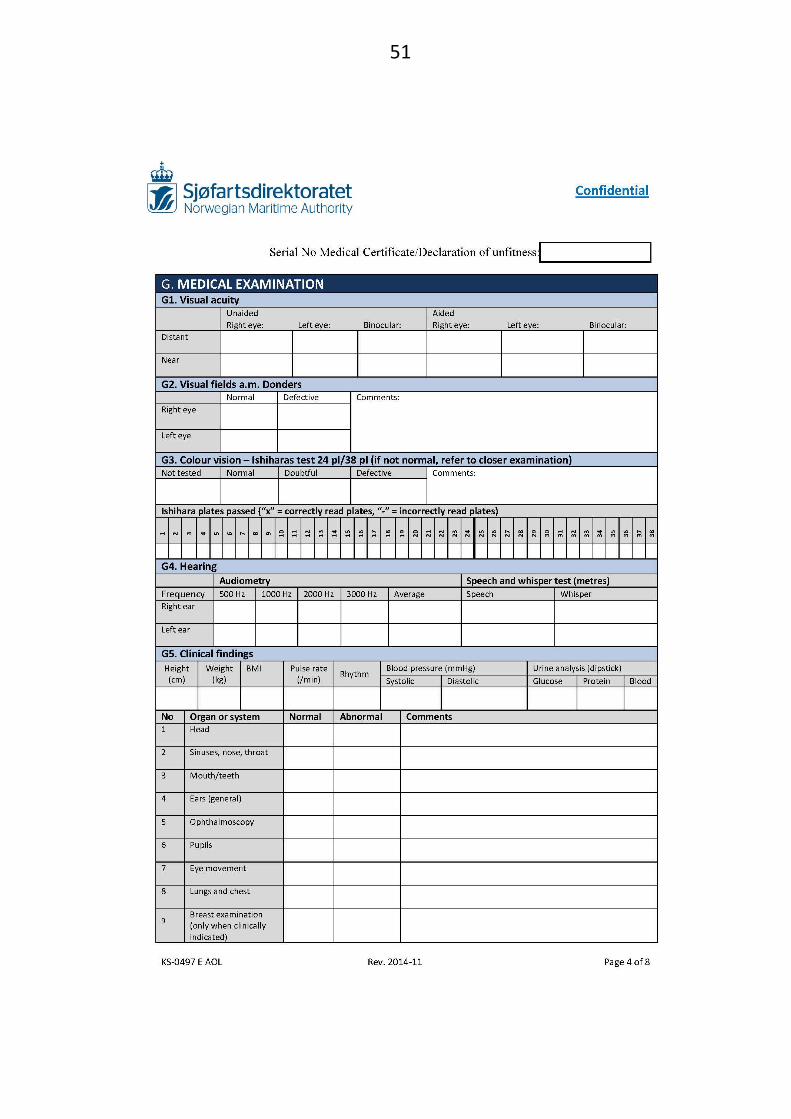
51
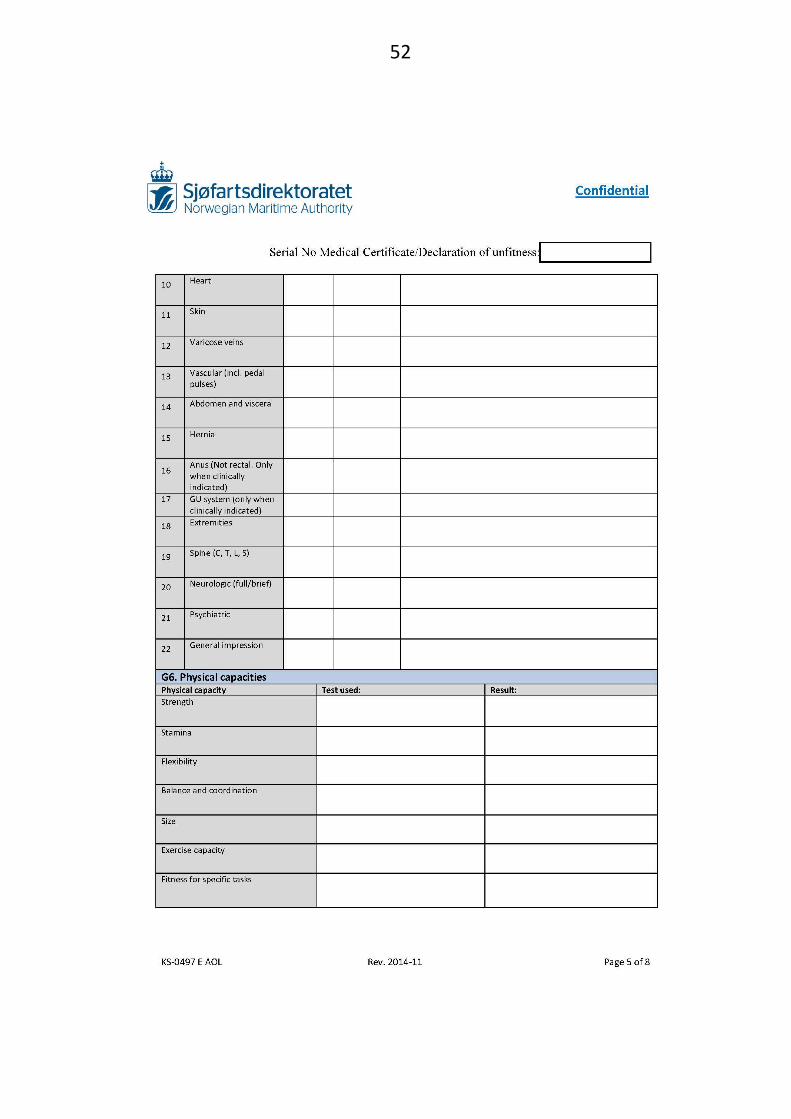
52

53
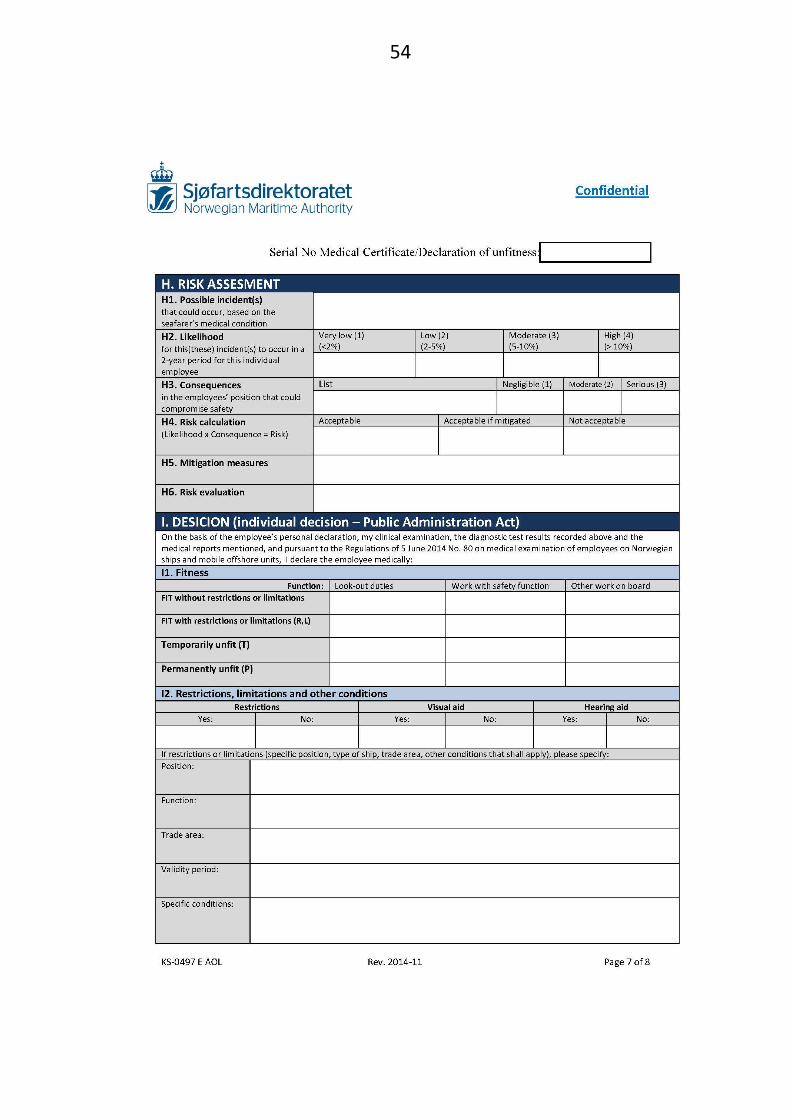
54

55

56
40.2 APPENDIX 2 – DECLARATION OF UNFITNESS FORM
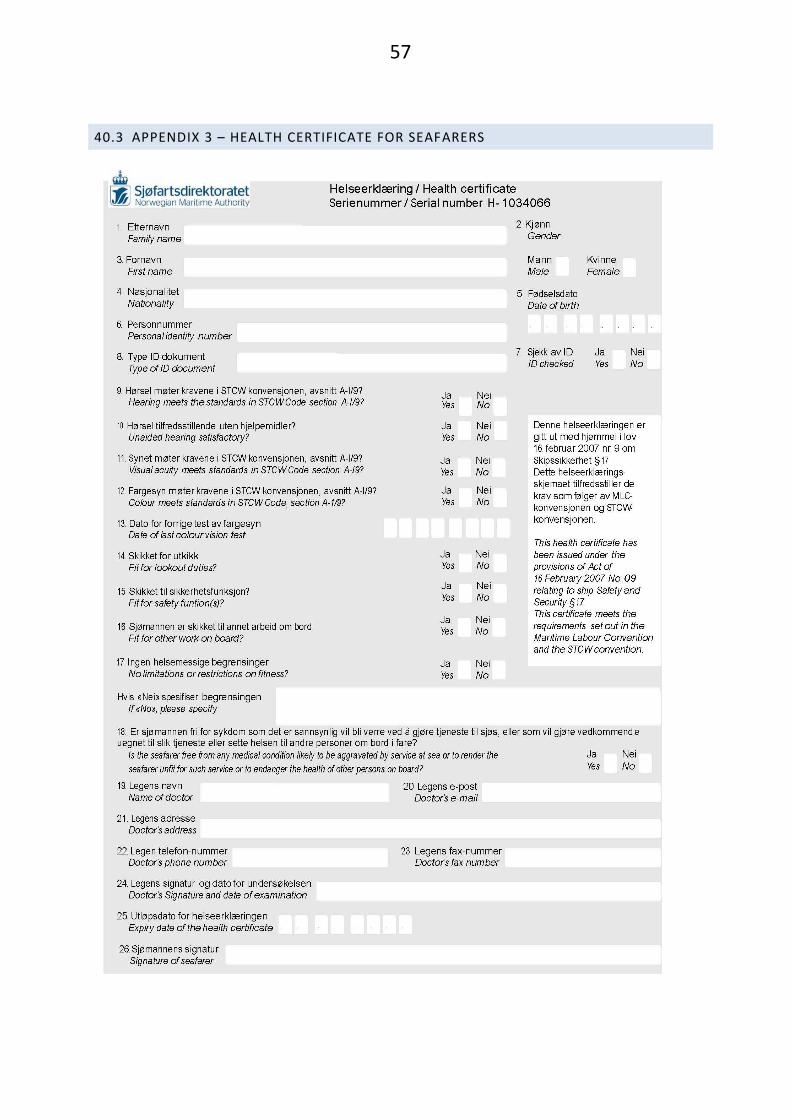
57
40.3 APPENDIX 3 – HEALTH CERTIFICATE FOR SEAFARERS

58
40.4 APPENDIX 4 - DECLARATION FROM THE SEAFARER’S DOCTOR REGARDING USE OF REGULAR MEDICINE

59
40.5 APPENDIX 5 - MEDICAL CERTIFICATES APPROVED FOR SERVICE ON BOARD NORWEGIAN VESSELS
According to the Regulations of 5 June 2014 No. 805 on the medical examination of employees on Norwegian ships and mobile offshore units section 4, paragraph three, employees may use medical certificates issued by flag states approved by the NMA.
This implies the following alternatives:
1. The employee may have a medical certificate issued by a seafarer’s doctor approved by Norwegian authorities. A list of approved seafarer’s doctors can be found on the Norwegian Maritime Authority website.
2. Employees living in an EEA country (home country or most recent country of residence) may alternatively have a medical certificate issued in accordance with the requirements for medical certificates in this country, cf. Section 4.
3. Employees may have a medical certificate issued by flag states approved by the Norwegian Maritime Authority, c.f. Section 4. At present the UK, the Netherlands, Germany and the People’s Republic of China are approved flag states.
The list will be updated and adjusted continuously.
40.6 APPENDIX 6 - REGULATIONS ON TUBERCULOSIS CONTROL
http://app.uio.no/ub/ujur/oversatte-lover/data/for-20090213-0205-eng.pdf
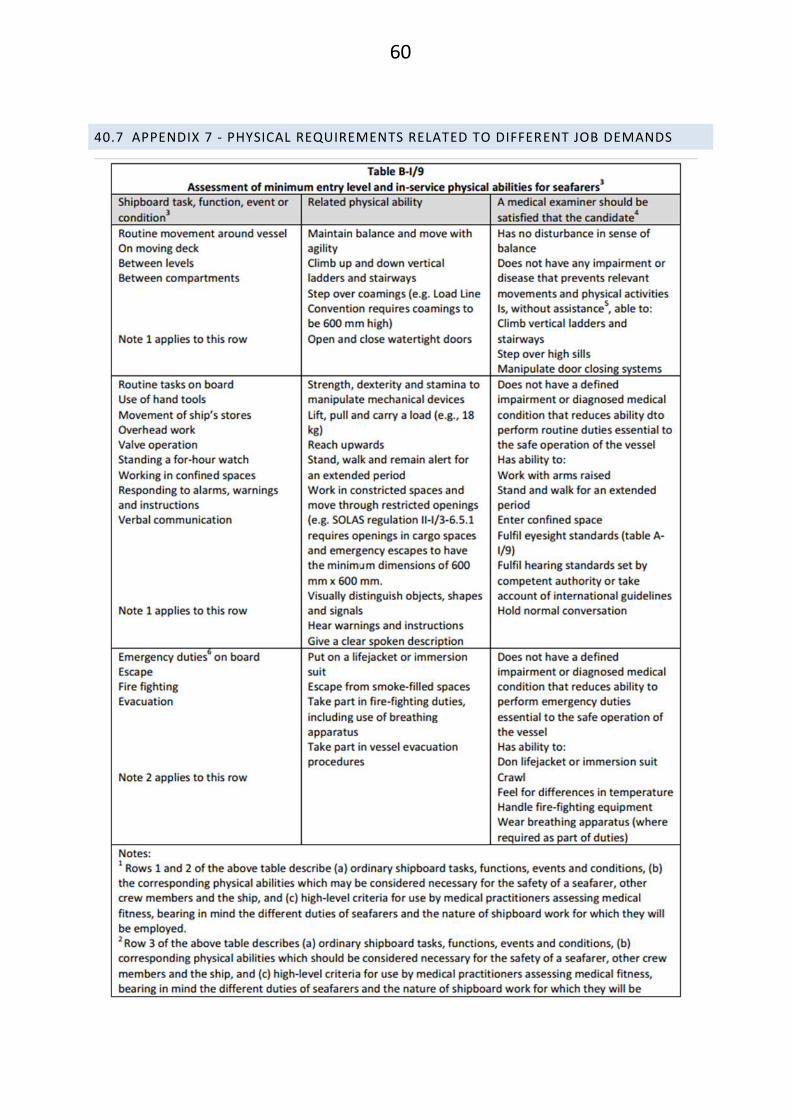
60
40.7 APPENDIX 7 - PHYSICAL REQUIREMENTS RELATED TO DIFFERENT JOB DEMANDS





























