Embed Size (px)
Citation preview

Spine Deformity 2 (2014) 308e315www.spine-deformity.org
Comparison of Typical Thoracic Curves and Atypical Thoracic CurvesWithin the Lenke 1 Classification
Takahito Fujimori, MDa,b, Tracey P. Bastrom, MAa, Carrie E. Bartley, MAa,Peter O. Newton, MDa,*, Harms Study Group
aDepartment of Orthopedic Surgery, Rady Children’s Hospital, 3030 Children’s Way, Suite 410, San Diego, CA 92123, USAbDepartment of Orthopedic Surgery, Sumitomo Hospital, 5-3-20 Nakanoshima, Kita Ward, Osaka, Osaka Prefecture 530-0005, Japan
Received 3 December 2013; revised 5 March 2014; accepted 24 March 2014
Abstract
Study Design: Retrospective study.Objectives: To examine the characteristics of Lenke type 1 curves based on the level of the apical vertebra.Summary of Background Data: The Lenke classification is the most used system for adolescent idiopathic scoliosis, with approximately50% of the curves falling into the Lenke 1 curve type category.Methods: A total of 611 Lenke 1 curves in a prospectively collected multicenter adolescent idiopathic scoliosis study were analyzed.Minimum follow-up was> 2 years. Curves were subdivided into 3 groups according to their apex: the typical Lenke 1 curve group includedapices from T7/8 to T10 (511 patients), the proximal group included apices from T4 to T7 (45 patients), and the distal group included apicesfrom T10/11 to T11/12 (50 patients). Preoperative and postoperative radiographic and clinical outcomes were compared among the 3groups.Results: The proximal and distal groups included significantly more left thoracic curves (proximal: 29%; typical: 1.8%; distal: 19%; p !.01). Flexibility of the main thoracic curve was significantly different among the 3 groups (proximal: 32% � 17%; typical: 46% � 18%;distal: 57% � 18%; p ! .001). The distal group included significantly more ‘‘A’’ lumbar modifiers (proximal: 29%; typical: 53%; distal:96%; p ! .01) and had curves characteristics similar to King type 4 curves (L4 tilted to the right: Lenke 1AR). The average lowest in-strumented vertebra was significantly lower in the distal group (proximal: T12; typical: L1; distal: L2; p ! .01). The proximal group hadsignificantly greater thoracic kyphosis (proximal: 30� � 18�; typical: 20� � 13�, distal: 20� � 10�; p ! .001) and more fusion segments(proximal: 10; typical: 9; distal: 9; p ! .03).Conclusions: Curves categorized as Lenke 1 curves were less homogeneous than expected. Using only the Lenke type 1 designation todefine a study population may introduce unintended bias to the study design.� 2014 Scoliosis Research Society.
Keywords: Lenke classification; King classification; Apex distribution; Atypical curves; Adolescent idiopathic scoliosis
Author disclosures: TF (none); TPB (grants from Setting Scoliosis
Straight Foundation); CEB (grants from Setting Scoliosis Straight Founda-
tion); PON (grant from Setting Scoliosis Straight Foundation; consulting
fee/honorarium from DePuy Spine; support for travel to meetings from
DePuy Spine; board membership with POSNA, Harms Study Group Foun-
dation, Scoliosis Research Society, Children’s Specialist Foundation; con-
sultancy for DePuy Spine, Stanford University; employment with
Children’s Specialists of San Diego; expert testimony for NorCal, law firm
Carroll, Kelly, Trotter, Franzen, and McKenna, law firm Smith, Haughey,
Rice, and Roegge; grants from National Institutes of Health (Grant No:
R21AR049587), Orthopaedic Research and Education Foundation, POS-
NA, SRS, Harms Study Group Foundation, DePuy Synthes Spine, Axial
Biotech, Biospace/Med/EOS Imaging; payment for lectures including
service on speakers bureaus from DePuy Spine, patents from DePuy Syn-
thes Spine; royalties from DePuy Synthes Spine, Thieme Publishing; pay-
ment for development of educational presentations from DePuy Synthes
Spine; stock/stock options from Nuvasive); HSG (grants from Setting
Scoliosis Straight Foundation).
This study was supported in part by a research grant from Depuy Spine
to the Setting Scoliosis Straight Foundation and a grant-in-aid from the Ya-
mada Science Foundation.
*Corresponding author. Department of Orthopedic Surgery, Rady Chil-
dren’s Hospital, 3030 Children’s Way, Suite 410, San Diego, CA 92123,
USA. Tel.: (858) 966-6789; fax: (858) 966-7494.
E-mail address: [email protected] (P.O. Newton).
2212-134X/$ - see front matter � 2014 Scoliosis Research Society.
http://dx.doi.org/10.1016/j.jspd.2014.03.009

309T. Fujimori et al. / Spine Deformity 2 (2014) 308e315
Introduction
Ideal classification systems accurately characterize adisorder, guide treatment and decision making, and form abasis for the uniform reporting of treatment results that maylead to an evidence-based approach to care [1]. For scoli-osis, a classification system should include the followingcomponents: systematic categorization of similar disorders,prognosis regarding natural history and outcomes of treat-ment, correlation with health status or severity of defor-mity, and guide for optimal treatment [2].
A nominal classification system for scoliosis was firstintroduced by the Scoliosis Research Society [3] that hadcategories based on etiology: idiopathic, congenital,neuromuscular, associated with neurofibromatosis, mesen-chymal, traumatic, resulting from irritative phenomena, andother. Etiological classification is important for under-standing the condition’s natural history and because out-comes in scoliosis treatment are different depending on thecause of the scoliosis [4,5]. However, the classificationsystem based on etiology is limited in that it provides littleguidance for the treatment of specific curve types.
In the treatment of adolescent idiopathic scoliosis (AIS),much attention has been paid to radiographic parameters,especially coronal curve patterns. The first classificationsystem to describe curve patterns in AIS was developed bySchulthess in 1905 [6]. His classification system classifiedcurves based on their location within the spine (cervico-thoracic, thoracic, thoracolumbar, lumbar, and combinedthoracic and lumbar). In 1950, Ponseti and Friedman [7]described the natural history of scoliosis based on curvetypes. In 1954, James [8] reported that the evolution ofidiopathic scoliosis was determined by the site of the pri-mary curve and by the age of onset in early- and late-onsetscoliosis. These reports on the natural history of scoliosisemphasize the importance of curve type being at the centerof the classification systems for AIS [9].
In 1983, King et al. [10] introduced 5 major curve typesbased on curve severity and curve flexibility. Although theKing classification provides useful information for thetreatment of thoracic deformities, it is criticized for nothaving high reliability and reproducibility [11-13]. Anotherproblem of the King classification is that it does not includesagittal, thoracolumbar, or triple major curves.
In 2001, Lenke et al. [13] introduced a new system forclassifying AIS curves that incorporates sagittal parametersin addition to coronal and flexibility measurements. TheLenke classification is currently widely used for classifyingAIS and provides guidelines for surgical planning [13,14].However, there seem to be variations in treatment evenwithin specific Lenke subtypes because by definition, theLenke 1 category includes curves with a wide range ofapices [13]. Lenke 1 curves are the most common curvetype and account for as much as 50% of all curves,although this category includes several subtypes anddifferent curve patterns [15,16].
In the current study, the authors focused on someanomalous curves within the Lenke 1 category. The pur-pose of this study was to compare the characteristics andoutcomes of curves with atypical apices to curves withapices typical of a primary thoracic curve within the Lenketype 1 category.
Materials and Methods
A prospective, multicenter database of consecutivelyenrolled AIS patients was queried for Lenke type 1 curves.Patients from 11 centers who underwent surgery between1995 and 2010, were 10e21 years of age at the time ofsurgery, and had completed a minimum 2-year follow-upwere included. The diagnosis of AIS was based ondetailed medical interview, radiography, and neurologicalexamination including superficial abdominal reflex. In pa-tients with suspected non-idiopathic scoliosis, furthermagnetic resonance imaging was performed.
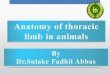
A total of 611 patients met the criteria and wereincluded. The mean follow-up period was 2.3 � 0.4 years.The apex of the curve was defined as the most deviateddisc or vertebra from midline on the posteroanteriorradiograph. All curves were subdivided into 3 groups ac-cording to the position of their apex and its distribution(Fig. 1). Based on the relatively normal distribution of theapex levels, the proximal and distal tails of the bell curvewere considered atypical. The apices of the groups were asfollows: typical group T7/8eT10, proximal group T4eT7,and distal group T10/11 to T11/12. Preoperative andpostoperative clinical outcomes and radiographic parame-ters were compared among the 3 groups. Selection ofsurgical approach (anterior or posterior) and fusion lengthwere also examined.
Clinical parameters included age at surgery, gender,Scoliosis Research Society (SRS-22) outcomes question-naire scores, shoulder height, coronal decompensation,angle of trunk rotation as measured by scoliometer, andtrunk shift. Radiographic parameters included coronalcurve direction, coronal curve magnitude, correction rate,flexibility, thoracic kyphosis (T5eT12), lumbar lordosis(T12eS1), and lumbar modifier. Curves with an A lumbarmodifier were further classified as Lenke 1AR or 1ALbased on the tilt of the L4 vertebra [17]. Lenke 1AR curves(L4 tilted to the right) have characteristics similar to Kingtype 4 curves.
The researchers used analysis of variance to comparecontinuous data among the 3 groups. Chi-square analysiswas used for categorical outcome variables. Alpha levelwas set at .05 to declare significance. The authors used posthoc Bonferroni method to control for multiple statisticaltests among the 3 groups (protection against Type 1 error).All statistical analyses were performed using SPSS statis-tical software (IBM SPSS Statistics, version 20; IBM,Armonk, NY).

Fig. 1. Distribution of apices for all 611 patients with Lenke 1 curves.
310 T. Fujimori et al. / Spine Deformity 2 (2014) 308e315
Results
Demographic data
There were 516 patients (84.4%) in the typical apexgroup, 45 (7.4%) in the proximal apex group, and 50(8.2%) in the distal apex group (Fig. 2). The average ageof the entire cohort was 14.6 � 2.1 years, with no sig-nificant differences among the 3 groups (typical: 14.6 �2.1 years; proximal: 15.1 � 2.1 years; distal: 15.2 � 2.2years; p O .2) (Table 1). There was no significant dif-ference in the distribution of gender among the 3 groups(p 5 .2).
Fig. 2. Examples of Lenke 1 curves with a proximal
Fusion length and surgical approach
The mode for the lowest instrumented vertebra wassignificantly lower in the distal group (proximal: T12;typical: L1; and distal: L2; p ! .01) (Table 1). Fusionlength was significantly longer in the proximal group(proximal: 10 levels; typical: 9 levels; and distal: 9 levels;p 5 .028). The typical group included twice as manyanterior surgeries as the other 2 groups (proximal: 9%;typical: 23%; distal: 10%; p 5 .009).
Focusing on posterior surgeries, the distal groupincluded significantly more short posterior fusions (fusion
(left), typical (middle), and distal apex (right).

Table 1
Demographic data of 3 groups divided by apex location.
Group Proximal apex Typical apex Distal apex p value
Main effect P vs. T P vs. D T vs. D
Apex T4eT7 T7/8eT10 T10/T11eT11/T12
Patients, n (%) 45 (7.4) 516 (84.4) 50 (8.2)
Age, years 15.1�2.1 14.6�2.1 15.2�2.2 .04 .2 1.0 .2
Gender, male (%) 18 16 26 .2 1.0 1.0 .2
Upper instrumented vertebra T3 T4 T5 !.001 .001 .001 .001
Lower instrumented vertebra T12 L1 L2 !.001 .05 .001 .001
Vertebral levels fused, n 10 9 9 .03 .03 .4 1.0
Anterior surgical approach (%) 9 23 10 .009 .07 1.0 .09
Posterior short fusion (length < 6) (%) 7 1 13 .01 .02 1.0 !.001
Surgical time, minutes 301�138 298�124 281�108 .6 1.0 1.0 1.0
Estimated blood loss, mL 1,118�824 844�705 928�650 .04 .04 .6 1.0
Length of hospitalization, d 6.3�1.9 6.6�3.4 5.6�1.4 .1 .5 .7 .5
D, distal; P, proximal; T, typical.
Bold data are statistically significant.
311T. Fujimori et al. / Spine Deformity 2 (2014) 308e315
length < 6) than the typical group (typical: 1%; distal:13%; p ! .001).
Coronal parameters
Therewas a significant difference in curve direction amongthe 3 groups (Table 2). The proximal and distal groupsincluded significantly more left thoracic curves than thetypical group (proximal: 29%; typical: 1.8%; distal: 19%; p!.001). The average preoperativemajor Cobb anglewas similaramong the 3 groups (proximal: 49� � 10�; typical: 51� � 9�;distal: 49� � 7�; pO .1). Flexibility of themain thoracic curvewas significantly different (proximal: 32% � 17%; typical:46%� 18%; distal: 57%� 18%; p! .001). The preoperativeCobb angle of the upper thoracic curve was significantly
Table 2
Coronal curves of the 3 groups.
Group
Proximal Apex Typical Apex
Curve direction to left (%) 29 1.8
Upper thoracic
Preoperative Cobb (degrees) 19�9 26�7
Postoperative Cobb (degrees) 10�7 14�6
Change in Cobb (degrees) �9�7 �11�6
Flexibility (%) 31�42 39�22
Correction rate (%) 44�35 44�20
Main thoracic
Preoperative Cobb (degrees) 49�10 51�9
Postoperative Cobb (degrees) 21�8 20�8
Change in Cobb (degrees) �28�11 �31�10
Flexibility (%) 32�17 46�18
Correction rate (%) 56�16 60�15
Lumbar
Preoperative Cobb (degrees) 35�11 33�9
Postoperative Cobb (degrees) 17�9 15�8
Change in Cobb (degrees) �18�10 �18�8
Flexibility (%) 73�17 73�20
Correction rate (%) 52�23 56�22
D, distal; P, proximal; T, typical.
Bold data are statistically significant.
smaller in the proximal group (proximal: 19� � 9�; typical: 26�
� 7�; distal: 25� � 6�; p! .001). ThepreoperativeCobb angleof the lumbar curve was significantly smaller in the distalgroup (proximal: 35� � 11�; typical: 33� � 9�; distal: 28� �8�; p! .001).
The correction rate of the main thoracic curve tendedto be greater in the distal group than in the proximalgroup (proximal: 56% � 16%; distal: 63% � 15%; p 5.09). Postoperative Cobb angle of the upper thoraciccurve was significantly smaller in the proximal group(proximal: 10� � 7�; typical: 14� � 6�; distal: 16� � 6�;p ! .001). Postoperative Cobb angle of the lumbarcurve was significantly smaller in the distal group(proximal: 17� � 9�; typical: 15� � 8�; distal: 8� � 6�;p ! .001).
p value
Distal Apex Main effect P vs. T P vs. D T vs. D
19 .001 .001 .4 .001
25�6 .001 .001 .001 1.0
16�6 .001 .001 .001 .06
�9�5 .001 .009 1.0 .003
43�27 .047 .09 .05 .9
35�20 .01 1.0 .1 .01
49�7 .1 .4 1.0 .3
18�7 .057 1.0 .1 .07
�31�9 .2 .2 .3 1.0
57�18 .001 .001 .001 .001
63�15 .09 .5 .09 .4
28�8 .001 .5 .001 .001
8�6 .001 .4 .001 .001
�20�7 .4 1.0 .9 .5
83�19 .002 1.0 .03 .02
72�20 .001 .8 .001 .001

Table 3
Coronal parameters of the 3 groups.
Group p value
Proximal Apex Typical Apex Distal Apex Main effect P vs. T P vs. D T vs. D
C7-CSVL, mm
Preoperative �0.8�2.3 �0.1�2.0 1.3�2.1 .001 .06 .001 .001
Postoperative �0.4�1.8 �0.58�1.4 0.19�1.3 .002 1.0 .1 .001
Change 0.4�2.3 �0.4�2.0 �1.1�2.1 .001 .02 .001 .08
Apical vertebral translation, mm
Preoperative 2.2�4.3 4.6�2.3 3.0�3.4 .001 .001 .4 .001
Postoperative 0.98�1.8 1.7�1.3 1.0�1.5 .001 .005 1.0 .003
Change �1.2�2.9 �3.0�2.2 �2.0�2.6 .001 .001 .3 .007
Apex-CSVL, mm
Preoperative 1.2�4.0 4.5�3.1 4.2�4.9 .001 .001 .001 1.0
Postoperative 0.6�1.6 1.1�1.5 1.2�1.8 .07 .08 .2 1.0
Change �0.64�3.8 �3.4�2.8 �3.1�3.8 .001 .001 .001 1.0
Th/L apical vertebral translation, mm
Preoperative �1.3�2.7 �1.3�1.3 �0.1�0.8 .001 1.0 .001 .001
Postoperative �0.4�1.8 �0.9�1.2 0.1�0.6 .001 .04 .2 .001
Change 0.87�1.7 0.4�1.1 0.16�0.6 .006 .02 .006 .5
T1 tilt (degrees)
Preoperative 0.9�8.0 4.3�3.7 4.0�3.4 .001 .001 .001 1.0
Postoperative 5.0�4.3 4.6�3.5 5.6�3.4 .1 1.0 1.0 .2
Change �4.4�8.2 0.2�4.6 1.6�3.2 .001 .001 .001 .1
Lumbar modifier
A/B/C (%) 29/21/51 53/25/22 96/4/0 .001 .001 .001 .001
AR/AL (%) 39/61 62/38 100/0 .001 .3 .001 .001
CSVL, central sacral vertical line; D, distal; P, proximal; T, typical; Th/L, thoracolumbar/lumbar.
Bold data are statistically significant.
Table 4
Sagittal and clinical parameters of the 3 groups.
Group p value
Proximal Typical Distal Main effect P vs. T P vs. D T vs. D
Thoracic kyphosis (T5/T12) (degrees)
Preoperative 30�18 20�13 20�10 .001 .001 .01 1.0
Postoperative 23�9 22�9 25�10 .2 1.0 1.0 .2
Change �5�15 1�13 4�10 .002 .009 .02 .3
Lumbar lordosis (T12/S1) (degrees)
Preoperative �58�13 �58�12 �56�11 .4 1.0 1.0 .5
Postoperative �58�12 �58�12 �63�12 .03 1.0 .2 .03
Change �1�22 �0.1�18 �7�12 .04 1.0 .4 .03
Shoulder height, mm
Preoperative 1.7�1.1 1.3�1.1 0.9�0.8 .008 .3 .2 1.0
Postoperative 0.7�0.5 0.9�0.7 1.0�0.7 .2 .01 .001 .02
Change 1.0�1.3 0.4�1.3 �0.13�1.2 .001 .01 .001 .02
Coronal decompensation, mm
Preoperative 1.7�1.1 1.3�1.0 1.9�1.3 .006 .1 1.0 .02
Postoperative 1.1�1.8 0.7�0.8 0.7�0.7 .4 .5 1.0 1.0
Change �0.7�1.2 �0.5�1.0 �0.8�1.3 .03 .3 1.0 .06
Rib hump thoracic, mm
Preoperative 12.9�5.0 14.4�4.6 12.2�4.8 .002 .1 1.0 .006
Postoperative 8.2�5.0 6.8�3.8 4.3�3.4 .001 .2 .001 .001
Change �5.4�4.8 �6.6�6.1 �7.5�5.3 .2 .6 .2 .8
Rib hump lumbar, mm
Preoperative 6.8�4.2 6.8�4.4 5.2�3.9 .07 1.0 .3 .07
Postoperative 3.4�3.0 3.3�3.3 3.3�3.7 1.0 1.0 1.0 1.0
Change �3.4�4.8 �2.9�4.6 �2.0�4.4 .3 1.0 .4 .6
Trunk shift, mm
Preoperative 1.1�1.1 1.9�1.5 2.7�1.3 .001 .004 .001 .002
Postoperative 0.9�0.7 0.95�0.04 0.87�0.1 .8 1.0 1.0 1.0
Change 0.25�1.2 0.78�1.7 1.35�1.6 .008 .1 .006 .07
D, distal; P, proximal; T, typical.
Bold data are statistically significant.
312 T. Fujimori et al. / Spine Deformity 2 (2014) 308e315

Table 5
Scoliosis Research Societye22 questionnaire scores for the 3 groups.
Group p value
Proximal apex Typical apex Distal apex Main effect P vs. T P vs. D T vs. D
Pain
Preoperative 4.0�0.7 4.2�0.7 3.9�0.7 .047 .5 1.0 .1
Postoperative 4.4�0.6 4.4�0.6 4.1�0.8 .016 1.0 .3 .01
Change 0.4�1.6 0.6�1.9 0.5�1.4 .7 1.0 1.0 1.0
Self-image
Preoperative 3.2�0.7 3.5�0.6 3.4�0.6 .1 .1 .4 1.0
Postoperative 4.4�0.6 4.5�0.6 4.4�0.6 .4 1.0 1.0 .7
Change 1.2�1.5 1.2�1.8 1.1�1.1 1.0 1.0 1.0 1.0
General function
Preoperative 4.5�0.5 4.5�0.6 4.4�0.6 .7 1.0 1.0 1.0
Postoperative 4.7�0.3 4.7�0.5 4.5�0.6 .2 1.0 .4 .2
Change 0.3�1.6 0.6�2.0 0.4�1.3 .5 .9 1.0 1.0
Mental health
Preoperative 3.9�0.7 4.1�0.7 4.0�0.6 .2 .3 1.0 1.0
Postoperative 4.3�0.5 4.3�0.6 4.2�0.7 .4 1.0 1.0 .6
Change 0.4�1.4 0.6�1.9 0.5�1.4 .8 1.0 1.0 1.0
Satisfaction
Preoperative 3.7�0.9 3.7�1.0 3.5�1.1 .4 1.0 .9 .6
Postoperative 4.6�0.6 4.6�0.7 4.5�0.8 .5 1.0 1.0 .8
Change 0.9�1.8 1.5�2.2 1.4�1.5 .2 .2 1.0 1.0
Total
Preoperative 3.9�0.5 4.0�0.4 3.9�0.4 .09 .3 1.0 .3
Postoperative 4.5�0.4 4.5�0.4 4.3�0.5 .06 1.0 .4 .049
Change 0.6�1.4 0.8�1.8 0.7�1.2 .8 1.0 1.0 1.0
D, distal; P, proximal; T, typical.
Bold data are statistically significant.
313T. Fujimori et al. / Spine Deformity 2 (2014) 308e315
The correction rate of the upper curve was significantlysmaller in the distal group than in the typical group (typical:44% � 20%; distal: 35% � 20%; p! .001). The correctionrate in the lumbar curvewas significantly greater in the distalgroup (proximal: 52% � 23%; typical: 56% � 22%; distal:72% � 20%; p ! .001). The preoperative apical vertebraltranslation (AVT) was significantly greater in the typicalgroup (proximal: 2.2� 4.3 cm; typical: 4.6� 2.3 cm; distal:3.0 � 3.4 cm; p ! .001) (Table 3). The postoperative AVTand change in AVT were significantly greater in the typicalgroup (AVT: proximal: 1.0 � 1.8 cm; typical: 1.7 � 1.3 cm;distal: 1.0� 1.5 cm; p! .001; AVT change: proximal�1.2� 2.9 cm; typical: �3.0 � 2.2 cm; distal: �2.0 � 2.6 cm;p5 .007).
Lumbar modifier
There was a significant difference in the distribution oflumbar modifiers. The distal (A 96%, B 4%, C 0%) andtypical (A 53%, B 25%, C 22%) groups were predomi-nantly lumbar modifier A and the proximal group consistedprimarily of lumbar modifier C (A 29%, B 21%, C 51%;p! .001) (Table 3). The distal group included significantlymore Lenke 1AR curves than the other 2 groups (proximal:39%; typical: 62%; distal: 100%; p ! .001).
Sagittal parameters
Preoperative thoracic kyphosis was significantly greaterin the proximal group (proximal: 30� � 18�; typical: 20� �
13�; distal: 20� � 10�; p 5 .01) (Table 4). Change ofthoracic kyphosis was significantly less in the proximalgroup (proximal: �5� � 15�; typical: 1� � 13�; distal: 4� �10�; p 5 .02). Postoperative thoracic kyphosis was similaramong groups (proximal: 23� � 9�; typical: 22� � 9�;distal: 25� � 10�; p O .2).
Preoperative lumbar lordosis was similar among thegroups (proximal: �58� � 13�; typical: �58� � 12�; distal:�56� � 11�; p O .4); however, postoperative lumbarlordosis was significantly greater in the distal group(proximal: �58� � 12�; typical: �58� � 12�; distal: �63�
� 12�; p 5 .03). Change in lumbar lordosis was signifi-cantly greater in the distal group than in the typical group(typical: �0.1� � 18�; distal, �7� � 12�; p 5 .03).
Clinical parameters
The proximal group had a significantly greater differ-ence in shoulder height postoperatively, as well as agreater change in shoulder height difference from pre-operative to postoperative (Table 4). The distal group hadsignificantly greater preoperative trunk shift, greater cor-onal decompensation, and smaller thoracic rib hump.Preoperatively, SRS-22 scores were not significantlydifferent among the 3 groups (proximal: 3.9; typical: 4.0;distal: 3.9; p 5 .09) (Table 5), although postoperatively asignificant difference was observed in SRS-22 total scoresbetween the typical and distal groups (typical: 4.5 � 0.4;distal: 4.3 � 0.5; p 5 .049).

314 T. Fujimori et al. / Spine Deformity 2 (2014) 308e315
Discussion
Classification systems for AIS can be helpful in under-standing the condition, creating a common language amongsurgeons, and guiding surgical decision making. Theseclassification systems should strive to create categories ashomogeneous as possible so that treatments can be appro-priately tailored and outcomes can be evaluated moreclearly. The Lenke classification system is currently themost used system for AIS. This system has previously beenshown to have high interobserver (0.92) and intra-observer(0.83) kappa values among the 5 investigators whodesigned the system [13]. Although Ogon et al. [17] re-ported that the kappa value of the Lenke classification(0.62) was lower than that of the King classification (0.73),other studies reported that the Lenke classification has ahigher reliability measurement than the King classifica-tion [12,18].
According to the Lenke classification, thoracic curvesare defined as curves with apices from T2 to T11/T12,thoracolumbar curves as curves with apices from T12 toL1, and lumbar curves as curves with apices from L1/L2 toL4/L513. Generally, Lenke 1 curves correspond to mainthoracic curves and Lenke 5 curves correspond to thor-acolumbar curves. Sponseller et al. [16] studied 1,912 AISpatients and reported that 50% of all curves fell into theLenke 1 category, followed by Lenke 2 (19%), Lenke 5(14%), and Lenke 6 (8%).
Numerous studies have used specific Lenke curve typesas part of their inclusion criteria [19-21]. The current studydemonstrated that the Lenke 1 category is heterogeneous.Typical main thoracic curves comprised 84.4% of Lenke 1curves and the remaining 15.6% had characteristicsdifferent from the typical thoracic curves. Ignoring thevariability in curve characteristics within this group maycreate potential bias in a comparative study. This issue mayarise, for example, when evaluating outcomes betweenanterior surgery and posterior surgery for Lenke 1 curves.Our data showed that the typical group was twice as likelyas the other groups to be treated with an anterior surgery.Although this is to some extent dictated by surgeon pref-erence, it is also acknowledged that there are some curvepatterns that are more amenable to anterior surgery.
Alam et al. [22] reported that the separation betweenthoracic curves with distal apices and thoracolumbar curvesis less clear. They reported that curves with T11 or T11/T12apices have characteristics similar to those found in Lenke5 curves. The current results supported those of Alamet al.’s, which found that curves with distal apices havecharacteristics different from curves within the typical apexgroup. The current finding that the distal group includedsignificantly more short posterior fusions (fusion length <6) than the typical group suggests that some curves in thedistal group were treated with a strategy similar to that ofLenke 5 curves.
The distal group had significantly greater flexibility ofthe primary curve and thus the correction rate tended to behigh. Coronal parameters in the distal group, such as C7-CSVL and clinical deformity of trunk shape as deter-mined by coronal decompensation, thoracic rib hump, andtrunk shift, significantly varied from the typical group,perhaps because many in the distal group had a long Cshape curve.
The distal group included significantly more lumbar Amodifiers, all of which were Lenke 1AR patterns. Miyanjiet al. [15] distinguished the Lenke 1AL and 1AR curvesbased on L4 tilt, with the Lenke 1AR curve typically beinga long thoracic curve similar to the King type 4 pattern.These Lenke 1AR curves are different in form and treat-ment from Lenke 1AL curves. Considering this previousresearch and the current study’s finding that most of thedistal group included Lenke 1AR curves, it is not surprisingthat the distal apex group was treated differently from thetypical apex group.
The proximal group had significantly more left thoraciccurves, greater lumbar Cobb magnitudes, more C modifiers,and greater thoracic kyphosis preoperatively. The fusionlength in the proximal group was significantly longer thanin the other 2 groups. The decrease in thoracic kyphosisafter surgery was significantly greater in the proximalgroup than in the other 2 groups. Postoperative hypo-kyphosis in the thoracic spine is a potential concern whenusing segmental pedicle screw fixation techniques for AIS[23]. However, the proximal group had significantly greaterthoracic kyphosis preoperatively than that of the typicalgroup. This difference in thoracic kyphosis of the proximalgroup can potentially bias a study if an inordinate numberof a proximal apex subjects is included.
The curves categorized as Lenke 1 were less homo-geneous than expected. Although each classificationsystem has its pros and cons, the authors think that theLenke classification system is the most comprehensiveand reliable system currently in use. Nevertheless, thisdoes not preclude the need for an individualizedapproach to each curve during the preoperative planningfor instrumentation.
The curves classified as Lenke type 1 are a heteroge-neous population with significant differences in preopera-tive curve characteristics, surgical strategies, andpostoperative results. Using only the Lenke 1 designation todefine a study population has the potential to introduceunintended bias and the lumbar modifier may not be suf-ficient to eliminate this bias. The authors suggest usingapex location as further inclusion for studies focused onLenke type 1 curves.
References
[1] Garbuz DS, Masri BA, Esdaile J, et al. Classification systems in or-
thopaedics. J Am Acad Orthop Surg 2002;10:290e7.

315T. Fujimori et al. / Spine Deformity 2 (2014) 308e315
[2] Lowe T, Berven SH, Schwab FJ, et al. The SRS classification for
adult spinal deformity: building on the King/Moe and Lenke classifi-
cation systems. Spine (Phila Pa 1976) 2006;31:S119e25.[3] Goldstein LA, Waugh TR. Classification and terminology of scoli-
osis. Clin Orthop Relat Res 1973;93:10e22.
[4] Bjure J, Nachemson A. Non-treated scoliosis. Clin Orthop Relat Res
1973;93:44e52.[5] Collis DK, Ponseti IV. Long-term follow-up of patients with idio-
pathic scoliosis not treated surgically. J Bone Joint Surg Am
1969;51:425e45.
[6] Schulthess W. Die pathologie und Therapie der Ruckgratsverkrum-
mungen. Chirugie HBO 1905:1.
[7] Ponseti IV, Friedman B. Prognosis in idiopathic scoliosis. J Bone
Joint Surg Am 1950;32:381e95.
[8] James JI. Idiopathic scoliosis; the prognosis, diagnosis, and operative
indications related to curve patterns and the age at onset. J Bone Joint
Surg Br 1954;36:36e49.
[9] Weinstein SL. Natural history. Spine (Phila Pa 1976) 1999;24:
2592e600.
[10] King HA, Moe JH, Bradford DS, et al. The selection of fusion levels in
thoracic idiopathic scoliosis. J Bone Joint Surg Am 1983;65:1302e13.
[11] Behensky H, Giesinger K, Ogon M, et al. Multisurgeon assessment of
coronal pattern classification systems for adolescent idiopathic scoliosis:
reliability and error analysis. Spine (Phila Pa 1976) 2002;27:762e7.
[12] Cummings RJ, Loveless EA, Campbell J, et al. Interobserver reli-
ability and intraobserver reproducibility of the system of King,
et al. for the classification of adolescent idiopathic scoliosis.
J Bone Joint Surg Am 1998;80:1107e11.
[13] Lenke LG, Betz RR, Harms J, et al. Adolescent idiopathic scoliosis: a
new classification to determine extent of spinal arthrodesis. J Bone
Joint Surg Am 2001;83:1169e81.
[14] Lenke LG, Betz RR, Clements D, et al. Curve prevalence of a new
classification of operative adolescent idiopathic scoliosis: does classi-
fication correlate with treatment? Spine (Phila Pa 1976) 2002;27:
604e11.
[15] Miyanji F, Pawelek JB, Van Valin SE, et al. Is the lumbar modifier
useful in surgical decision making? Defining two distinct Lenke 1A
curve patterns. Spine (Phila Pa 1976) 2008;33:2545e51.[16] Sponseller PD, Flynn JM, Newton PO, et al. The association of pa-
tient characteristics and spinal curve parameters with Lenke classifi-
cation types. Spine (Phila Pa 1976) 2012;37:1138e41.
[17] Ogon M, Giesinger K, Behensky H, et al. Interobserver and intraob-
server reliability of Lenke’s new scoliosis classification system. Spine
(Phila Pa 1976) 2002;27:858e62.
[18] Lenke LG, Betz RR, Bridwell KH, et al. Intraobserver and interob-
server reliability of the classification of thoracic adolescent idiopathic
scoliosis. J Bone Joint Surg Am 1998;80:1097e106.
[19] Abul-Kasim K, Ohlin A. Patients with adolescent idiopathic scoliosis
of Lenke type-1 curve exhibit specific pedicle width pattern. Eur
Spine J 2012;21:57e63.
[20] Matsumoto M, Watanabe K, Ogura Y, et al. Short fusion strategy for
Lenke type 1 thoracic curve using pedicle screw fixation. J Spinal
Disord Tech 2013;26:93e7.[21] Newton PO, Marks MC, Bastrom TP, et al. Surgical treatment of
Lenke 1 main thoracic idiopathic scoliosis: results of a prospective,
multicenter study. Spine (Phila Pa 1976) 2013;38:328e38.
[22] Alam M, Newton PO, Yaszay B, et al. Are thoracic curves with a low
apex (T11 or T11/T12) really thoracic curves? Spine Deformity
2013;1:139e43.
[23] LonnerBS, Lazar-AntmanMA, Sponseller PD, et al.Multivariate anal-
ysis of factors associatedwith kyphosismaintenance in adolescent idio-
pathic scoliosis. Spine (Phila Pa 1976) 2012;37:1297e302.






![Cumulative dose-response curves for assessing combined ... · Fifteen patients meeting American Thoracic Society (ATS) criteria for asthma [14] entered the study (table 1); all had](https://img.pdfslide.us/doc/110x75/5d15c00d88c993a82b8b498c/cumulative-dose-response-curves-for-assessing-combined-fifteen-patients.jpg)