Embed Size (px)
Citation preview
Comparison of Traditional Didactic Seminar to High-FidelitySimulation for Teaching Electroconvulsive Therapy
Technique to Psychiatry TraineesKiran Rabheru, MD, CCFP, FRCPC, DABPN,*Þ Andrew Wiens, MD, BMedSc,*þ§Bismil Ramprasad, MBBS, MD,*Þ Luc Bourgon, MD,*Þ Ruxandra Antochi, MD,*Þ
and Stanley J. Hamstra, PhD§||¶
Objectives: Traditional training of electroconvulsive therapy (ECT)consists of a combination of didactic and hands-on demonstrations usingECT equipment. Our goal was to explore the potential of a high-fidelitypatient simulator (HPS) to train these skills. To our knowledge, this isthe first time an HPS has been used for skills training in psychiatry.Methods: Nineteen psychiatry residents participated in this random-ized controlled trial to compare traditional training (n = 9) versustraining using an HPS (n = 10). Two blinded raters assessed performanceusing a newly developed checklist and global rating scale for this task(ECT-OSATS) (Objective Structured Assessment of Technical Skills).Residents also completed a pretest-posttest knowledge test and confi-dence survey.Results: Residents in the HPS group performed significantly better interms of ECT-OSATS when compared with the control group (P G
0.001). All 10 of the HPS group received a ‘‘pass’’ rating followingtraining, whereas only 1 of the 9 control group received a ‘‘pass’’ rating.There were no significant group differences in posttest confidence (P =0.21) or total knowledge gain scores from pretest to posttest (P = 0.36).Conclusions: The level of clinical skill acquired by trainees in psy-chiatry for performing ECT is significantly superior using HPS- basedtraining, in contrast to the domains of knowledge and confidence, whichappear to be equally imparted using either training modality. The ac-quisition of skills in administering ECT seems to be an independentvariable in relation to a clinician’s level of knowledge and confidence inperforming ECT.
Key Words: electroconvulsive therapy, simulation, residents,education, skills training
(J ECT 2013;29: 291Y296)
E lectroconvulsive therapy (ECT) is a safe and effective treat-ment for many patients with major psychiatric disorders. The
Canadian Network for Mood and Anxiety Treatments guide-lines1 recommends ECT as a first-line therapy for patients whoare severely ill with mood disorders and a second-line treatmentoption for patients who are treatment resistant or unable totolerate medication. According to the Canadian Electroconvul-sive Therapy Survey2 conducted between 2007 and 2009, 175providers of ECT in Canada deliver approximately 75,000 ECTtreatments, annually. Although evidence for the efficacy of ECTis impressive, there seems to be a dearth of data for the effec-tiveness of training programs for clinicians in developing skillsto perform ECT.
In 1986, Rothman3 stated, ‘‘No other treatment deemedeffective is so much the stepchild in training as ECT, a factwhich again reduces its legitimacy among psychiatrists, otherphysicians, and then by extension, the public.’’ In 1990, a sur-vey done by Jaffe et al4 of senior psychiatric residents in theUnited States showed that only 7% of respondents felt com-fortable performing unsupervised ECT. In 1991, a Canadiansurvey of senior residents conducted by Goldbloom andKussin5 found that only 25% of 158 respondents felt they couldperform the procedure independently, and 20% had never ad-ministered ECT. They concluded that ‘‘training in the theoryand administration of ECT in the United States and the UnitedKingdom has been substandard and erratic’’ and recommendedthe need to set academic standards. Subsequently, guidelineshave been published in Canada and the United States with re-spect to ECT training in psychiatry residency programs. Anevaluation of the impact of these guidelines was published byYuzda et al6 in 2002, assessing training and attitudes of 133final-year Canadian psychiatric residents toward ECT. Al-though 88% of the respondents felt that ECT training should bemandatory during residency training, no marked improvementwas shown in level of competence in administering ECT com-pared with earlier surveys. Despite the fact that 59.3% antici-pated working in an inpatient unit, only 18% of respondents feltcompletely competent administering ECT. The guidelines hadapparently made little impact on training in and attitudes towardECT, with very few feeling competent to administer ECT aftercompleting their training. The bar for residency training pro-grams in psychiatry for ECT is set fairly low as outlined in the2007 American accreditation standards, which require thattrainees are competent in ‘‘understanding the indications anduses’’ of ECT.7 The outcome of such standards is reflected in astudy published in 20108 of a survey of the quality of trainingresidents received in ECT within 91 US training programscompared with the standards recommended by the AmericanPsychiatric Association’s Task Force on ECT in 2001.9 Fewprograms met the recommended standards of training in ECT.Most programs reported less than 4 hours of lectures, 75%
ORIGINAL STUDY
Journal of ECT & Volume 29, Number 4, December 2013 www.ectjournal.com 291
From the *Department of Psychiatry, University of Ottawa; †Department ofPsychiatry, The Ottawa Hospital; ‡Royal Ottawa Mental Health Centre;§University of Ottawa Skills and Simulation Centre; ||Departments of Med-icine, Surgery, and Anesthesia, University of Ottawa; and ¶Academy forInnovation in Medical Education, Faculty of Medicine, University of Ottawa,Ottawa, Ontario, Canada.Received for publication December 13, 2012; accepted March 4, 2013.Reprints: Kiran Rabheru, MD, CCFP, FRCPC, DABPN, Geriatric Psychiatry
& ECT Service, The Ottawa Hospital, 501 Smyth St, Ottawa, Ontario,Canada K1H 8L6 (e-mail: [email protected]).
This work was awarded Best Oral Presentation at the Academy for Innovationin Medical Education annual research day, Ottawa, Ontario, Canada,March 23, 2012.
Dr Rabheru is on the advisory board for Astra Zeneca, Lundbeck, and BristolMeyers and has received honoraria for speaking for those companies.Dr Hamstra has received honoraria for speaking for Laerdal. For theremaining authors, no conflicts of interest were declared.
Supplemental digital contents are available for this article. Direct URLcitations appear in the printed text and are provided in the HTML and PDFversions of this article on the journal’s Web site (www.ectjournal.com).
Copyright * 2013 by Lippincott Williams & WilkinsDOI: 10.1097/YCT.0b013e318290f9fb
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

reported ‘‘some clinical exposure,’’ and 37% reported that res-idents participated in 10 ECTs or less, and 27% reported resi-dents caring for fewer than 5 ECT patients. This phenomenon isobserved internationally. A 2008 survey of psychiatric residentsin Ireland revealed deficiencies in ECT training and supervi-sion. Twelve percent of trainees had never administered or ob-served ECT, and 19% of trainees had minimal or no confidencein their ability to administer ECT.10 In another survey of 490Irish psychiatrists who prescribe ECT, 35% felt the need forfurther training.11 The unmet needs with respect to training andcredentialing for skills in performing ECT are well summarizedby Jaffe12 in his 2005 editorial.
Clothier et al13 explored attitudes and basic knowledge ofsecond-year medical students in the United States and foundthem to have generally negative attitude with poor level of basicknowledge about ECT largely influenced by films. Interesting-ly, the group that described themselves as highly knowledgeableabout psychiatric illness had a greater bias against ECT. Thestigma among medical students and residents on ECT appearsto lessen with greater exposure to training and knowledge,highlighting the importance of initiating these interventionsduring the formative years of one’s training.14,15
Rationale for the Current StudyCurrently, ECT skills and knowledge are taught at national
and international courses by a combination of didactic andhands-on demonstrations of routine ECT equipment. Moreover,even though some jurisdictions require evidence of prior expe-rience or training in ECT, there is no standardized methodavailable for assessing trainees’ competence in performing theseskills. With limited clinical exposure and training in ECT, cur-rent and future generations of psychiatrists are potentially morelikely to compromise patient safety and expose patients to in-creased risk of complications while performing ECT in the ab-sence of a standardized and valid approach to training andassessment.
Trainees are often taught ECT skills during the normalcourse of providing care to live patients. During this process,novice trainees are often intercepted by experienced clinicalstaff, especially when the trainee encounters any difficulty. As aresult, the trainee is often relegated to being told what to do orto learning by observation only. Active learning is thereforeinhibited as the cycle of participation, reflection, interpretation,testing, and integration into a new skill and knowledge acqui-sition is fragmented. Learning in this setting is therefore verycomparable to learning during crises in the clinical setting.
Within psychiatry, ECT is the most invasive procedurerequiring a very high level of skill and proficiency in its users. Itis postulated that the advantages of the use of simulation inanesthesia and surgery are also applicable to the training, eval-uation of proficiency, and maintenance of skills in the use ofECT. The present study is designed to compare the effect of2 methods of training on ECT. The outcome measure includesthe acquisition of skills, knowledge, and confidence in per-forming this important technique. To our knowledge, this is thefirst such study of its kind using patient simulators to addressthis unmet need.
Research QuestionsThe primary research question we attempted to answer
was: Does hands-on practice lead to better performance in ECTskills, as assessed using a high-fidelity patient simulator (HPS)and a standardized assessment scale (ECT-OSATS) (ObjectiveStructured Assessment of Technical Skills)? Two secondaryresearch questions were also considered: (1) Will this training
lead to improved confidence in considering ECT for treatmentwhen clinically indicated? (2) Will knowledge of ECT be sig-nificantly enhanced as measured by on a pretest and comparedwith a posttest on multiple choice questions?
HypothesisOur hypothesis was that, compared with traditional train-
ing methods, HPS-based training would improve acquisition ofECT skills. In addition, it would allow residents to feel moreconfident and knowledgeable in considering ECT as a treatmentoption when clinically indicated.
MATERIALS AND METHODS
Study ParticipantsThis study took place at the University of Ottawa Skills
and Simulation Centre (uOSSC). Two cohorts of residents inpsychiatry from the University of Ottawa training program werevoluntarily recruited and participated in this study. Because oflogistical reasons, only 19 of the expected 24 residents were ableto participate on the actual study day. All 19 residents were giventhe opportunity to learn about the study and ask questions to theirsatisfaction before enrolment. This study was approved by TheOttawa Hospital Research Ethics Board. All participants receivedan information session and letter outlining the proposed researchand signed an informed consent form before enrollment in thestudy. Following completion of the study, all residents were of-fered debriefing, and members of the control group were offeredthe opportunity to receive ECT training using the HPS.
ProcedureAt the start of the day, all residents completed a pre-
test consisting of multiple-choice questions designed to assesstheir level of knowledge of ECT, as well as a brief survey onprior experience with ECT. (For the ECT Prior ExperienceSurvey, see Appendix, Supplemental Digital Content 1, athttp://links.lww.com/JECT/A8.) Each resident also completedthe ECT Skills and Knowledge Confidence (ECT-C) Scale,adapted from Powell and Myers16 to assess their level of con-fidence with specific aspects of ECT. (To review the ECT Skillsand Knowledge Confidence Scale, see Appendix, SupplementalDigital Content 2, at http://links.lww.com/JECT/A9.) Followingthis, all residents received comprehensive didactic lectures onseveral fundamental aspects of ECT.
To reduce the risk of pretest contamination during thestudy, scrupulous attention was paid to ensure that the onlyvariable between the 2 groups was the type of training eachgroup received before the testing procedure. The followingmeasures were taken to control for all other independent vari-ables: (1) To familiarize all the residents to the physical layoutof the uOSSC, a group orientation of the center was conductedby a nonstudy staff member. (2) At this time, all residents alsoreceived general exposure to the HPS, including a hands-ondemonstration of the various uses of HPS for nonYECT-relatedtraining. The HPS were capable of ‘‘communicating’’ with theparticipants through embedded speakers and microphones. Theexact same HPSs were later used to carry out the study protocol.At this time, each of the 19 residents was randomly assigned byan independent third party to a control or experimental group.(3) As part of the consent procedure for the study, each residenthad expressly agreed to refrain from discussing their experiencewith other residents during the course of the study day. (4)Residents were not randomized until just before the study por-tion of the day. (5) Once randomized, the 2 groups were im-mediately and completely segregated until the end of the studyperiod, including having separate areas for their nourishment
Rabheru et al Journal of ECT & Volume 29, Number 4, December 2013
292 www.ectjournal.com * 2013 Lippincott Williams & Wilkins
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

breaks and washroom facilities. (6) When residents werewaiting their turn to be trained or examined, they were given theopportunity to watch the movie, ‘‘One Flew Over the Cuckoo’sNest’’17 and the TED talk on ECT.18 The 2 presentations wereneutral to the outcome of the study and served a dual purpose.The primary purpose was to reduce the risk of contaminatingthe study by limiting opportunities for residents to discuss theirexperiences before undergoing testing. The secondary purposewas to maintain the educational theme related to ECT and ed-ucate them about the stigma associated with ECT from a pastand present era. (7) The randomization codes were available toonly one of the authors who had no direct role in either teachingor testing the residents. (8) Strict adherence to the study pro-tocol was maintained by the 5 teaching faculty members. (9)They met several times in advance to plan the sessions andbecame very familiar with the manikins, protocols, ratingscales, and equipment. (10) Over numerous sessions, all of thetrainers and raters developed excellent interrater reliability. (11)Three of the 5 teaching faculty members were totally blindedwith respect to the resident training status, that is, control orexperimental. (12) Only the blinded raters who were not in-volved with the training portion of the study were responsiblefor the ECT-OSATS testing portion of the study.
As is traditionally taught at the national and internationalECT courses, the control group received skills training in smallgroups on scalp preparation, electrode placement, ECT equip-ment, and interpretation of electroencephalographic strips.The control group was taught by 3 faculty members who wereblinded to the HPS portion of the study protocol. The experi-mental group received HPS-based training sessions of equalduration by specially trained faculty. Both groups of traineeswere tested to assess acquisition of technical skills and knowl-edge of ECT, immediately after ECT training. During the as-sessment phase, the HPS was used in conjunction with actorswho represented team members from anesthesia and nursing.This made it possible to capture the domains of respect, com-munication, and professionalism in the primary outcome mea-sure. The testing for all candidates was performed by blindedraters using newly developed standardized ECT tests consistingof an ECT-Checklist and a global rating scale, ECT-OSATS.(For the ECT-OSATS Checklist, see Appendix, SupplementalDigital Content 3, at http://links.lww.com/JECT/A10; for theECT-OSATS Global Rating Scale, see Appendix, SupplementalDigital Content 4, at http://links.lww.com/JECT/A11.) TheOSATS was chosen as a model for the development of our as-sessment instruments because the content of that scale relatesclosely to the technical skills assessed in the current study, andthere is a substantial body of evidence supporting the reliabilityand validity of the OSATS.19Y23
Both standardized tests were created by unanimous con-sensus over each item of the scales to assist the trainers andraters with each aspect of the candidate’s ECT experience, andboth were adapted from Grober et al.24 The behavioral anchorsused to define performance on the scales were clearly observ-able and easily rated. This greatly facilitated ease of use andinterrater reliability, which was tested multiple times before theactual study day. The ECT-Checklist has 20 items, which in-corporate fundamental aspects of each ECT session, includingskin and scalp preparation, electrode placement, stimulus dosestrategies, seizure monitoring, missed or aborted seizures, andpossible remedies. Each item on the checklist is rated as thecandidate is observed performing the procedure and is markedas ‘‘done correctly,’’ ‘‘done incorrectly,’’ or ‘‘not done.’’
The global performance was then rated immediately fol-lowing the completion of the procedure using the OSATS-ECT,
to help the assessor evaluate 5 global domains. These domainsare ‘‘respect for patient,’’ ‘‘efficiency,’’ ‘‘knowledge,’’ ‘‘com-munication,’’ and ‘‘overall impression of performance.’’ The 5global domains capture each of the 7 aspects of the CanMEDSPhysician Competency Framework developed by The RoyalCollege of Physicians and Surgeons of Canada (RCPSC): (1)medical expert (knowledge), (2) communicator (communicator),(3) collaborator (advocate, communicator), (4) manager (effi-ciency), (5) health advocate (communicator), (6) scholar (knowl-edge), and (7) professional (respect). The ‘‘final global rating’’ isbased on an integration of ratings of the 5 global domains of theOSATS-ECT and observations from the ECT-Checklist. It is adichotomous ‘‘pass or fail’’ outcome, based on the examiner’sintegrated impression of the evidence of both scales. It indicateswhether the examiner feels that the candidate would be safe toperform ECT independently on the next live patient or not.
Outcome MeasuresVAssessment InstrumentsThe independent variable was the type of training received,
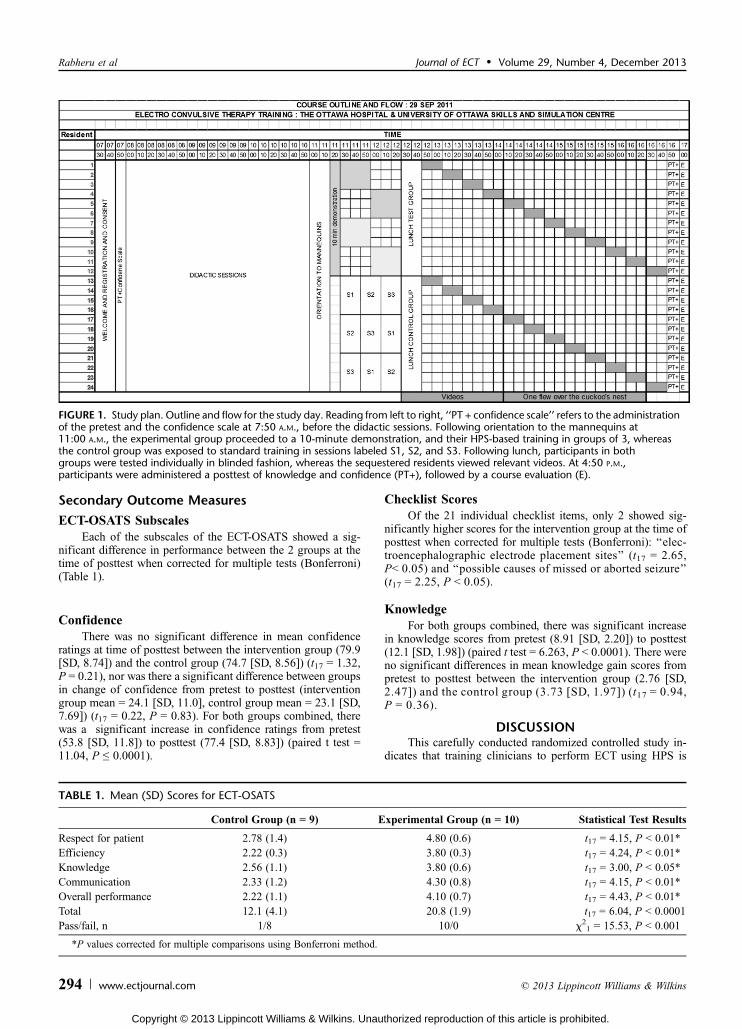
and the primary outcome was the score on the ECT-OSATS atposttraining, as a measure of ECT technical skills acquisition.The self-rating of level of confidence in conducting ECT wasused as a secondary measure of ECT skills and knowledge ac-quisition. The primary research question was answered bycomparing the mean differences in performance using a t testfor independent groups with > set to 0.05. We were aware of nostudies that have systematically evaluated the relative educa-tional effectiveness of simulator versus nonsimulator trainingfor ECT. However, there have been many studies looking at theeffect of using simulators to teach technical skills in surgery,anesthesia, and medicine, which are based on effect sizes, whichare typically in the range of 0.8 to 2.0.25Y27 Although our testablenull hypothesis was that there would be no difference in perfor-mance between our 2 teaching interventions, we would consideran effect size of 1.0 to be significant enough to warrant a changein standard educational practice. Based on an > = 0.05, power =0.8, and an estimated effect size of d = 1.0, we estimated 13 res-idents would be required to address this research question. How-ever, because of program capacity constraints, only 12 residentsper group were initially recruited. We recognize the approximatenature of the power calculations and estimated number of resi-dents required (Fig. 1).
RESULTS
DemographicsThere were no differences between the experimental and
control groups in any of the demographic data: sex (interventiongroup: male-female ratio = 4/6, control group = 1/8) (W21 = 2.16,P = 0.14), post-graduate year (PGY) training level (interventiongroup PGY 1/2/3/4/5: n = 1/2/3/2/1, control group = 0/1/1/4/3)(W25 = 5.83, P = 0.32), or previous experience with ECT (interven-tion group yes/no = 7/3; control group = 4/5) (W21 = 1.28, P = 0.26).
Primary Outcome MeasureVECT-OSATS GlobalRating of Performance
Participants in the intervention group, which receivedhands-on training, had significantly higher mean ECT-OSATSglobal rating total scores at posttest (20.8 [SD, 1.93]) than didthe control group (12.1 [SD, 4.08]) (t17 = 6.04, P G 0.0001).This difference was statistically significant with a very largeeffect size (Cohen d = 2.8) in favor of the educational inter-vention. This effect was also observed for the global impressionof the experts in terms of pass/fail: intervention group pass/fail = 10/0; control group pass/fail = 1/8 (W21 = 15.53, P G 0.001).
Journal of ECT & Volume 29, Number 4, December 2013 Simulation Training in ECT
* 2013 Lippincott Williams & Wilkins www.ectjournal.com 293
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Secondary Outcome Measures
ECT-OSATS SubscalesEach of the subscales of the ECT-OSATS showed a sig-
nificant difference in performance between the 2 groups at thetime of posttest when corrected for multiple tests (Bonferroni)(Table 1).
ConfidenceThere was no significant difference in mean confidence
ratings at time of posttest between the intervention group (79.9[SD, 8.74]) and the control group (74.7 [SD, 8.56]) (t17 = 1.32,P = 0.21), nor was there a significant difference between groupsin change of confidence from pretest to posttest (interventiongroup mean = 24.1 [SD, 11.0], control group mean = 23.1 [SD,7.69]) (t17 = 0.22, P = 0.83). For both groups combined, therewas a significant increase in confidence ratings from pretest(53.8 [SD, 11.8]) to posttest (77.4 [SD, 8.83]) (paired t test =11.04, P e 0.0001).
Checklist ScoresOf the 21 individual checklist items, only 2 showed sig-
nificantly higher scores for the intervention group at the time ofposttest when corrected for multiple tests (Bonferroni): ‘‘elec-troencephalographic electrode placement sites’’ (t17 = 2.65,PG 0.05) and ‘‘possible causes of missed or aborted seizure’’(t17 = 2.25, P G 0.05).
KnowledgeFor both groups combined, there was significant increase
in knowledge scores from pretest (8.91 [SD, 2.20]) to posttest(12.1 [SD, 1.98]) (paired t test = 6.263, P G 0.0001). There wereno significant differences in mean knowledge gain scores frompretest to posttest between the intervention group (2.76 [SD,2.47]) and the control group (3.73 [SD, 1.97]) (t17 = 0.94,P = 0.36).
DISCUSSIONThis carefully conducted randomized controlled study in-
dicates that training clinicians to perform ECT using HPS is
TABLE 1. Mean (SD) Scores for ECT-OSATS
Control Group (n = 9) Experimental Group (n = 10) Statistical Test Results
Respect for patient 2.78 (1.4) 4.80 (0.6) t17 = 4.15, P G 0.01*Efficiency 2.22 (0.3) 3.80 (0.3) t17 = 4.24, P G 0.01*Knowledge 2.56 (1.1) 3.80 (0.6) t17 = 3.00, P G 0.05*Communication 2.33 (1.2) 4.30 (0.8) t17 = 4.15, P G 0.01*Overall performance 2.22 (1.1) 4.10 (0.7) t17 = 4.43, P G 0.01*Total 12.1 (4.1) 20.8 (1.9) t17 = 6.04, P G 0.0001Pass/fail, n 1/8 10/0 W
21 = 15.53, P G 0.001
*P values corrected for multiple comparisons using Bonferroni method.
FIGURE 1. Study plan. Outline and flow for the study day. Reading from left to right, ‘‘PT + confidence scale’’ refers to the administrationof the pretest and the confidence scale at 7:50 A.M., before the didactic sessions. Following orientation to the mannequins at11:00 A.M., the experimental group proceeded to a 10-minute demonstration, and their HPS-based training in groups of 3, whereasthe control group was exposed to standard training in sessions labeled S1, S2, and S3. Following lunch, participants in bothgroups were tested individually in blinded fashion, whereas the sequestered residents viewed relevant videos. At 4:50 P.M.,participants were administered a posttest of knowledge and confidence (PT+), followed by a course evaluation (E).
Rabheru et al Journal of ECT & Volume 29, Number 4, December 2013
294 www.ectjournal.com * 2013 Lippincott Williams & Wilkins
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

feasible and effective with significant improvements in skillscompared with traditional methods of training. The study hasthe potential to have a significant impact on the way ECT skillsare taught to clinicians. A very interesting finding of this studyis that the acquisition of skills in administering ECT seems to beindependent of a clinician’s level of knowledge and confidencein performing ECT. This is in line with other recent findings inmedical education, which question the validity of self-assessedskills.28 The usual method of teaching ECT, which is didacticlectures followed by small group learning, is effective in im-proving knowledge and confidence, but not necessarily theskills to perform ECT independently. In contrast, the HPS-trained group was clearly superior compared with the usualmethod of teaching with respect to acquisition of ECT-relatedskills. This important and significant finding may have a ma-jor impact on how ECT skills are taught to clinicians to be safeECT practitioners.
The reader should bear in mind the limitations of thisstudy, including the fact that it was conducted at a single insti-tution. Because of logistical reasons, the number of residentsavailable for recruitment was limited, particularly for a planned3-month retention test, which was therefore not completed.Despite this, this study yielded adequate statistical power todemonstrate a significant difference between groups on themain outcome variable. This study should be replicated at otherinstitutions to test for generalizability and to allow for continuedimprovements in the assessment instruments.
The use of simulators as a training tool in anesthesia hasproven efficacy on the immediate acquisition of technicalskills29 and has contributed significantly to their proliferation inCanada.30 The use of HPS also allows for practice of scenarios,which are rare, unplanned, and critical for skills acquisition thattrainees may not otherwise be exposed to. In contrast to thelearning process that occurs during routine clinical care, HPS-based training can allow the trainees to participate duringdifficult scenarios without the fear of harming the patient orsupervisor intervention. We anticipate that training clinicians toperform ECT with HPS will help close the gap in ECT skills,which is difficult to teach using traditional methods. We alsopredict that the ability to practice performing ECT on a patientsimulator will allow trainees to feel more comfortable, confi-dent, and knowledgeable when prescribing and performing thistreatment. The use of a standardized assessment instrument fordocumenting performance of ECTwill be a major step forwardin ensuring adequate skills and knowledge of cliniciansperforming ECT safely. High-fidelity patient simulatorYbasedECT training and testing can also be used by institutions forcredentialing of ECT practitioners for privileges to performECT and maintaining their privileges to do so. Smaller mentalhealth programs would be able to send their staff for ECTtraining to a center with patient simulator facilities, confidentwith the knowledge that this training has been demonstrated tobe effective.
In Canada, RCPSC31 is responsible for setting the stan-dards for specialty medical education in addition to monitoringlifelong learning for specialist physician members. At this time,none of the RCPSC documents outlining ECT training re-quirements for psychiatry residents or geriatric psychiatrysubspecialty residents refer to specific training or testing re-quirements to perform ECT. The Structured Assessment ofClinical Evaluation Report32 for PGY 4 and PGY 5 residents ingeneral psychiatry simply requires residents to ‘‘communicate acomprehensive treatment plan including biological therapies(pharmacotherapy, ECT, TMS [transcranial magnetic stimula-tion], etc).’’ The Objectives for Training in General Psychiatry33
require the resident to ‘‘demonstrate a proficiency in imple-menting an effective management plan in collaboration withpatients and their families, including assessing suitability for,prescribe and deliver appropriate somatic treatments (eg, ECT)across the life span.’’ It also requires the resident to ‘‘demon-strate effective, appropriate, and timely performance of thera-peutic procedures relevant to psychiatry including, but notlimited to ECT.’’ The Final In-Training Evaluation Report/Comprehensive Competency Report34 for psychiatry residentsrequires them to be able to ‘‘assess suitability for, prescribe anduse appropriate somatic therapies (ECT).’’ The newly approvedsubspecialty of geriatric psychiatry in Canada requires the res-ident in its Final In-Training Evaluation Report/ComprehensiveCompetency Report35 to ‘‘demonstrate safe, effective, appro-priate, and timely performance of electroconvulsive therapy(ECT), minimizing risks and discomforts to elderly patients.’’The Objectives of Training in the Subspecialty of GeriatricPsychiatry36 require the resident to be able to ‘‘implement amanagement plan in collaboration with a patient and theirfamily or other caregivers including assessing suitability forprescribing and delivering somatic treatments such as electro-convulsive therapy (ECT) in elderly patients.’’ The SpecificStandards of Accreditation for Residency Programs in GeriatricPsychiatry37 specify that ‘‘there should be active clinicalteaching services in Psychiatry specialty areas of particularimportance to geriatric psychiatry such as ECT.’’ Incorporatingspecific and standardized training and testing requirements forresidents and specialists in psychiatry would go a long waytoward raising the bar for this highly effective but stigmatizedtreatment modality.
An intensely supervised ‘‘hands-on’’ training and assess-ment program in ECT have recently been proposed for intro-duction in the Royal Australian and New Zealand College ofPsychiatrists Competency-Based Fellowship Program.38 Simi-larly, the Royal Australian and New Zealand College of Psy-chiatrists recommends that nurses who serve as critical teammembers during the performance of ECT should be appropri-ately trained in modern ECT practice.39 A recent Canadianstudy suggests that attitudes toward ECT increase favorablywhen individuals are provided with training and experience.40
Live demonstration and viewing a videotape appear to be ef-fective methods for teaching medical students about ECT.41
Using a video or information pamphlet has the ability to in-crease students’ knowledge and improve attitudes towardECT.42 The time has come for our professional regulatingbodies to set more rigorous standards in training clinicians toperform ECT, the most invasive biological treatment modalityin psychiatry. It is no longer acceptable to rely purely on a senseof confidence and knowledge in one’s abilities to perform ECT.The skill to perform ECT competently and safely must bedemonstrated using standardized assessment tools before beingexposed to treatment of live patients. The authors suggest thatthe RCPSC and other similar regulatory bodies may wish to payspecial attention to the results of this study with the goal ofincorporating them into the core training requirements andcredentialing for ECT.
ACKNOWLEDGMENTSThe authors thank the Department of Psychiatry, AFP, for
financial support, and the following individuals for assistancein running the study: Drs Huntington, Lau, and Khan for as-sistance with small-group ECT training, Monique Fink andAvril McIntosh of The Ottawa Hospital; Dr Heidi King, Psy-chiatry Resident, University of Ottawa; the BioMedical De-partment and staff of The Ottawa Hospital; and the staff of the
Journal of ECT & Volume 29, Number 4, December 2013 Simulation Training in ECT
* 2013 Lippincott Williams & Wilkins www.ectjournal.com 295
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
uOSSC: Kevin Thomas, Kim Tardioli, Kathy Labelle, StephanieGibson, Julie Ghatalia, Leanne McHardy, and volunteers of theuOSSC for acting as anesthesiologists.
REFERENCES
1. Kennedy SH, Milev R, Giacobbe P, et al. Canadian Network for Moodand Anxiety Treatments (CANMAT) Clinical guidelines for themanagement of major depressive disorder in adults. IV. Neurostimulationtherapies. J Affect Disord. 2009;117(suppl 1):S44YS53.
2. Delva NJ, Graf P, Patry S, et al. Access to electroconvulsive therapyservices in Canada. (Canadian Electroconvulsive Therapy SurveyCANECTS). J ECT. 2011;27:300Y309.
3. Rothman DJ. ECT: the historical, social, and professional sources ofthe controversy. Psychopharmacol Bull. 1986;22:459Y463.
4. Jaffe R, Shoyer B, Siegel L, et al. An assessment of psychiatricresidents’ knowledge and attitudes regarding ECT. Acad Psychiatry.1990;14:204Y210.
5. Goldbloom DS, Kussin DJ. Electroconvulsive therapy training inCanada: a survey of senior residents in psychiatry. Can J Psychiatry.1991;36:126Y128.
6. Yuzda E, Parker K, Parker V, et al. Electroconvulsive therapy trainingin Canada: a call for greater regulation. Can J Psychiatry.2002;47:938Y944.
7. Dolenc TJ, Philbrick KL. Achieving competency in electroconvulsivetherapy: a model curriculum. Acad Psychiatry. 2007;31:65Y67.
8. Dinwiddie SH, Spitz D. Resident education in electroconvulsivetherapy. J ECT. 2010;26:310Y316.
9. Weiner RD, Coffey C, Fochtmann L , for the American PsychiatricAssociation. The Practice of ECT: Recommendations for Treatment,Training, and Privileging. 2nd ed. Washington, DC: AmericanPsychiatric Press; 2001.
10. Akinsola O, Sundram F, Bangaru R. Electroconvulsive therapy trainingand confidence in administration: a national survey of psychiatrictrainees in Ireland. J ECT. 2011;27:127Y130.
11. Blaj A, Worrall A, Chaplin R. Electroconvulsive therapy: the practiceand training needs of referring psychiatrists in the United Kingdomand Republic of Ireland. J ECT. 2007;23:78Y81.
12. Jaffe R. ECT training: can the case be made for certification? J ECT.2005;21:73Y74.
13. Clothier JL, Freeman T, Snow L. Medical student attitudes andknowledge about ECT. J ECT. 2001;17:99Y101.
14. Szuba M, Guze B, Liston E. Psychiatry resident and medical studentperspectives on ECT: influence of exposure and education. J ECT.1992;8:110Y117.
15. Gazdag G, Kocsis-Ficzere N, Tolna J. Hungarian medical students’knowledge about and attitudes toward electroconvulsive therapy. J ECT.2005;21:96Y99.
16. Powell LE, Myers AM. The Activities-specific Balance Confidence(ABC) scale. J Gerontol Med Sci. 1995;50:M28YM34.
17. One Flew Over the Cuckoo’s Nest. 1975; based on the 1962 novel OneFlew Over the Cuckoo’s Nest by Ken Kesey. Available at:http://www.imdb.com/title/tt0073486/. Accessed January 19, 2013.
18. TED Talk: Sherwin Nuland: How Electroshock Therapy Changed Me.Filmed February 2001. Available at: http://www.ted.com/talks/sherwin_nuland_on_electroshock_therapy.html. Accessed January 19, 2013.
19. Winckel CP, Reznick RK, Cohen R, et al. Reliability and constructvalidity of a structured technical skills assessment form. Am J Surg.1994;167:423Y427.
20. Faulkner H, Regehr G, Martin J, et al. Validation of an objectivestructured assessment of technical skills for surgical residents. AcadMed. 1996;71:1363Y1365.
21. Martin JA, Regehr G, Reznick R, et al. Objective Structured Assessment OfTechnical Skill (OSATS) for surgical residents.Br J Surg. 1997;84:273Y278.
22. Reznick R, Regehr G, MacRae H, et al. Testing technical skill via aninnovative ‘‘bench station’’ examination. Am J Surg. 1997;173:226Y230.
23. Regehr G, MacRae H, Reznick R, et al. Comparing the psychometricproperties of checklists and global rating scales for assessingperformance on an OSCE-format examination. Acad Med.1998;73:993Y997.
24. Grober ED, Hamstra SJ, Wanzel KR, et al. The educational impactof bench model fidelity on the acquisition of technical skill: the use ofclinically relevant outcome measures. Ann Surg. 2004;240:374Y381.
25. Matsumoto ED, Hamstra SJ, Radomski SB, et al. The effect of benchmodel fidelity on endourologic skills: a randomized controlled study.J Urol. 2002;167:1243Y1247.
26. Naik V, Matsumoto ED, Houston P, et al. Fiberoptic orotracheal intubationon anesthetized patients. Domanipulation skills learned on a simplemodeltransfer into the operating room? Anesthesiol. 2001;95:343Y348.
27. Park JP, MacRae H, Musselman LJ, et al. Randomized control trial ofvirtual reality simulator training: transfer to live patients. Am J Surg.2007;194:205Y211.
28. Eva KW, Regehr G. ‘‘I’ll never play professional football’’ and otherfallacies of self-assessment. J Contin Educ Health Prof. 2008;28:14Y19.
29. Fletcher G, Flin R, McGeorge P, et al. Anaesthetists’ Non-TechnicalSkills (ANTS): evaluation of a behavioural marker. Br J Anaesth.2003;90:580Y588.
30. Wong AK. Full scale computer simulators in anesthesia training andevaluation. Can J Anaesth. 2004;51:455Y464.
31. RCPSC main Web site. Available at: http://www.royalcollege.ca/portal/page/portal/rc/about. Accessed August 27, 2012.
32. RCPSC Structured Assessment of Clinical Evaluation Report(STACER)VPsychiatry Clinical Evaluation for Senior Residents.Available at: http://rcpsc.medical.org/residency/certification/stacers/psychiatry_e.pdf. Accessed August 27, 2012.
33. RCPSCVObjectives of Training in Psychiatry. Available at: http://rcpsc.medical.org/residency/certification/objectives/psychiatry_e.pdf.Accessed August 27, 2012.
34. RCPSCVPsychiatry FITER (2011). Available at: http://rcpsc.medical.org/residency/certification/fiters/psychiatry_e.pdf.Accessed August 27, 2012.
35. RCPSCVGeriatric Psychiatry FITER (2011). Available at: http://rcpsc.medical.org/residency/certification/fiters/geriatric-psych_e.pdf.Accessed August 27, 2012.
36. RCPSCVObjectives of Training in the Subspecialty of GeriatricPsychiatry. Available at: http://rcpsc.medical.org/residency/certification/objectives/geriatric-psych_e.pdf. Accessed August 27, 2012.
37. RCPSCVSpecific Standards of Accreditation for Residency Programsin Geriatric Psychiatry. Available at: http://rcpsc.medical.org/residency/accreditation/ssas/geriatric-psych_e.pdf. Accessed August 27, 2012.
38. Port N, Weiss A, Maudsley I. Electroconvulsive therapy training: can itbe a model of an entrustable professional activity in a competencyprogram? Australas Psychiatry. 2012;20:242Y245.
39. Munday J, Deans C, Little J. Effectiveness of a training program forECT nurses. J Psychosoc Nurs Ment Health Serv. 2003;41:20Y26.
40. Oldewening K, Lange RT, Willan S, et al. Effects of an education trainingprogram on attitudes to electroconvulsive therapy. J ECT. 2007;23:82Y88.
41. Warnell RL, Duk AD, Christison GW, et al. Teaching electroconvulsivetherapy to medical students: effects of instructional method onknowledge and attitudes. Acad Psychiatry. 2005;29:433Y436.
42. Andrews M, Hasking P. Effect of two educational interventions onknowledge and attitudes towards electroconvulsive therapy.J ECT. 2004;20:230Y236.
Rabheru et al Journal of ECT & Volume 29, Number 4, December 2013
296 www.ectjournal.com * 2013 Lippincott Williams & Wilkins
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.





























