Embed Size (px)
Citation preview

Comparison of resection–intersection algorithms and projection
geometries in radiostereometry
Niclas Borlin
Department of Computing Science, Umea University, Umea SE-901 87, Sweden
Received 31 October 2001; accepted 3 May 2002
Abstract
Three resection– intersection algorithms were applied to simulated projections and clinical data from radiostereometric
patients. On simulated data, the more advanced bundle-adjustment-based algorithms outperformed the classical Selvik
algorithm, even if the error reductions were small for some parameters. On clinical data, the results were inconclusive. The two
different projection geometries had a much larger influence on the error size and distribution. For the biplanar configuration, the
position and motion errors were small and almost isotropic. For the uniplanar configuration, the position errors were
comparably high and anisotropic, but still resulted in a high accuracy for some motion parameters at the expense of others. The
simplified resection– intersection algorithm by Selvik may still be considered a good and robust algorithm for radiostereometry.
More studies will have to be performed to find out how the theoretical advantages of the bundle methods can be utilized in
clinical radiostereometry.
D 2002 Elsevier Science B.V. All rights reserved.
Keywords: radiostereometry (RSA); resection; projection geometry; X-ray photogrammetry; orthopaedic measurements
1. Introduction
1.1. Radiostereometry
Radiostereometric analysis (RSA) as defined by
Selvik in 1974 (Selvik, 1989) has been widely used in
orthopaedics for studying e.g. prosthetic implant
migration and wear, joint stability and kinematics,
bone growth, and fracture healing (Karrholm, 1989;
Stokes, 1995; Karrholm et al., 1997).
In the last 10 years, RSA has seen an increasing
use and Selvik-based systems are currently installed at
all university hospitals in Sweden and numerous other
locations in Europe, North America, and Australia.
To get reliable landmarks in the skeleton, RSA
uses implanted spherical markers (F=0.5–1.0 mm)
made of Ta73, a radio-dense, biocompatible metal. The
markers are inserted into the bone during surgery. If
an implant is part of the study, markers are attached to
the implant as well.
1.1.1. RSA procedure
After initial surgery, each RSA examination con-
sists of the following steps:
(1) Dual simultaneous X-ray exposure of the patient
together with a reference cage.
0924-2716/02/$ - see front matter D 2002 Elsevier Science B.V. All rights reserved.
PII: S0924-2716 (02 )00068 -0
E-mail address: [email protected] (N. Borlin).
www.elsevier.com/locate/isprsjprs
ISPRS Journal of Photogrammetry & Remote Sensing 56 (2002) 390–400

(2) Measurements of the projected marker coor-
dinates on the two radiographs.
(3) Reconstruction of the projection geometries
(resection).
(4) Reconstruction of the 3D-coordinates of the
patient markers (intersection).
Given two or more examinations, the relative rigid-
body motion between different group of markers
(segments) may be calculated.
1.1.2. RSA applications
RSA effectively enables relative motion measure-
ments of ‘‘anything you can put markers in’’.
Implant migration. With markers in an implant and
the surrounding bone, the migration pattern of an
implant can be studied. This allows different implant
designs, bone cement, operating techniques, etc., to be
evaluated.
Polyethylene wear. With markers in the polyethy-
lene liner of a hip implant, femoral head penetration
into the liner may be measured using the femoral head
as an additional marker. This enables assessment of
creep (deformation) and wear of the liner.
Joint kinematics and stability. With markers in the
bones on both sides of a joint, e.g. the knee, the
shoulder, vertebrae in the spine, etc., joint kinematics
may be evaluated. This applies to joints with or
without implants and may be used to understand the
joint behaviour, to compare healthy vs. pathological
joints, or to evaluate joint prostheses. Joint stability
may be assessed by calculating motions between
loaded and unloaded states.
Bone growth. Inserting markers in bone growth
zones enables studies of e.g. treatments for growth
disorders in children.
Fracture healing. Inserting markers on both sides
of a bone fracture enables measurements of healing
patterns.
For further details, see e.g. Karrholm (1989),
Stokes (1995) and Karrholm et al. (1997).
1.1.3. Aim of this paper
Several improvements of the original RSA proce-
dure have been presented, e.g. algorithms for efficient
calculation of the rigid-body motion (Soderkvist and
Wedin, 1993, 1994), solutions of two correspondence
problems and loose marker detection (Nystrom et al.,
1994). In the last 10 years, the development has been
concentrated to the measurement step, which until a
few years ago was performed manually using a high-
precision measurement table (Karrholm et al., 1997).
A number of papers have been presented on measure-
ments in digital radiographs (Borlin and Karrholm,
1997; Østgaard et al., 1997; Vrooman et al., 1998;
Valstar et al., 2000; Borlin et al., 2002). Two of those
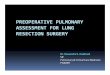
Fig. 1. The two X-ray set-ups used in RSA. In the biplanar set-up (left), the reference cage is placed around the body part of interest. In the
uniplanar set-up (right), the reference cage is placed below or behind the object of interest. Drawing not to scale.
N. Borlin / ISPRS Journal of Photogrammetry & Remote Sensing 56 (2002) 390–400 391

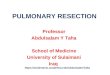
Fig. 2. Examples of RSA images. The fiducial markers ( f ) and control points (c) are attached to the cage. The bone markers (b) and prosthetic
markers ( p) are inside the patient. Images are negative, i.e. in bright areas, most of the radiation was blocked. In the knee patients, prosthetic
markers were also inserted into the plastic insert between the metallic components. The markers in parentheses are known to be there, but were
either obscured by the prostheses or were too dark to be seen.
N. Borlin / ISPRS Journal of Photogrammetry & Remote Sensing 56 (2002) 390–400392

(Borlin and Karrholm, 1997; Borlin et al., 2002) show
improved results on clinical images compared to
manual measurement.
In contrast, the resection–intersection algorithms
have remained unaltered since 1974. In the original
algorithm, the calibration planes of the cage are used
one at a time, and the resection is performed by sol-
ving two mathematical problems in sequence. When
studying the photogrammetric literature, it became
clear to the author that by coupling the two problems,
bundle-like algorithms could be constructed. The
assumption is that since such algorithms use more
information about the photogrammetric set-up, they
should be able to increase the precision of radio-
stereometric measurements.
The aim of this paper is to investigate whether this
assumption holds and that the Selvik algorithm should
be replaced. Furthermore, the error propagation is
studied through the whole calculation chain from
measurements via 3D positions to relative motions.
1.2. Photogrammetric set-up
RSA uses two different photogrammetric set-ups,
biplanar and uniplanar, illustrated in Fig. 1. A refer-
ence cage with markers attached at predefined posi-
tions defines a laboratory coordinate system in object
space and is used for resection.
The biplanar cage (called cage 10) is an open-
ended rectangular box with X-ray film cassettes
attached to the bottom and one side wall. The two
cage planes closest to the films each contain nine
markers, called fiducial1 markers. One of the fiducial
markers in the bottom defines the origin of the
laboratory coordinate system. The opposite planes
contain nine markers each, called control points. Both
marker types are arranged in a rectangular pattern in
their respective planes. The total volume spanned by
the cage markers is 249�160�249 mm (x�y�z). At
the examination, the object of interest, e.g. a knee,
ankle, or elbow, is placed inside the cage. The X-ray
beams are approximately orthogonal. The typical
principal distance is about 1 m.
The uniplanar cage is shaped as an inverted ‘‘T’’,
with the cassettes placed parallel at the bottom of the
cage. In one design (called cage 41), the bottom two
plates have nine fiducial markers each. The top of the
inverted ‘‘T’’ has seven control points in a straight
line, used in both images. In a more recent design
(cage 43), the number of fiducial markers have
increased to 13 and 19 control points and are arranged
in three parallel lines. The origin is defined to be at the
centre of the base plate. The total volume spanned by
the cage markers is 510�240�208 mm. At the
examination, the X-ray central beams are angled
20–40j apart, each about 10–20j off the z axis.
The patient is placed above or in front of the cage
during exposure. The typical principal distance is
1.4–1.8 m. The exposure geometry is largely dictated
by anatomical (e.g. feasible marker placements) and
geometrical (e.g. cage size) constraints.
The typical film-to-fiducial plane distance is about
10–20 mm for the biplanar cage and 25–35 mm for
the uniplanar cage.
Examples of radiostereometric images are given in
Fig. 2.
2. Reconstruction algorithms
Three resection–intersection algorithms are com-
pared in this paper; the classic algorithm by Selvik,
the ICDLT (Iterative Constrained DLT), and the
ICDLTI (Iterative Constrained DLT and Intersection).
The algorithmic details are given in Appendices A,
Appendices B, Appendices C, but briefly, the Selvik
algorithm uses a simplified resection, with the fiducial
markers acting as fiducial marks. A projective trans-
formation between the film and fiducial planes is
calculated by minimizing the error in image space.
The transformation is used to rectify all measured
image coordinates and transform them to the labora-
tory coordinate system. The object space position of
the X-ray focus (projection centre) is approximated to
the point that minimizes the distance to the bundle of
rays going through the control points. The object
marker positions are calculated by minimizing the
object space error between pairs of X-rays from the
two foci.
1 For historical reasons, the use of the term fiducial in RSA
differs slightly from its conventional use in photogrammetry, e.g.
their positions are defined in 3D object space. For a motivation on
the choice of terms, see Selvik (1989, p. 7). See also Section 2 and
Appendix A.
N. Borlin / ISPRS Journal of Photogrammetry & Remote Sensing 56 (2002) 390–400 393

In the ICDLT algorithm, the DLT formulation of
the collinearity equation is used. Orthonormality con-
straints on the image space coordinate system are
imposed to reduce the number of degrees of freedom
from 11 to 9, resulting in a self-calibration bundle
adjustment problem. The problem is solved for one
focus at a time with all cage markers used as control
points. The object marker positions are calculated by
minimizing the image space error between pairs of X-
rays from the two calculated foci.
The ICDLTI algorithm formulates and solves a
dual-station self-calibration bundle adjustment prob-
lem with the object markers appearing as unknowns.
The solution to this problem thus contains the projec-
tion parameters of both foci and the positions of the
patient markers.
3. Clinical material
To get clinically relevant material, examinations of
10 total hip replacement patients (cage 41, uniplanar)
and 10 total knee replacement patients (cage 10,
biplanar) from the Borlin and Karrholm (1997) study
were analysed. The patient markers were grouped into
a reference segment (bone) and a moving segment
(prosthesis). The patients were examined twice about
15 min apart with some intermediate patient exercise,
a procedure known as a double examination. The
hypothesis is that no relative motion of the segments
should occur between the two examination, so all
calculated ‘‘motions’’ between the segments may be
attributed to measurement errors. Double examina-
tions are used clinically to evaluate the relative motion
precision (Karrholm, 1989; Karrholm et al., 1997).
The images were scanned at 300 DPI with a Sharp
JX-610 flatbed scanner (Sharp, Japan) and measured
by UmRSA Digital Measure v2.2.5 (RSA Biomedical,
Umea, Sweden).
For each patient, the projection geometries and
patient marker positions of both examinations were
recovered by the ICDLT algorithm, resulting in four
sets of projection parameters and two sets of patient
marker coordinates, P1 and P2. For the biplanar
examinations, the principal distance varied between
0.92 and 1.04 m and the angle between the central
beams was 78–83j. The corresponding values for
the uniplanar configuration was 1.47–1.74 m and
24–28j. The patient marker configurations are
given in Table 1.
The absolute rigid-body motions of both segments
between P1 and P2 and their condition numbers were
calculated as described in Soderkvist and Wedin
(1993). Absolute motion is the motion in relation to
the cage, and reflects the difference in patient place-
ment between examinations. The condition number is
related to the geometrical configuration of the markers
in a segment. A high condition number indicates that
the geometrical configuration is almost degenerate, i.e.
close to a straight line, and therefore sensitive to
measurement errors. The absolute motion statistics is
given in Table 2 with the rigid-body motion separated
Table 1
Clinical patient marker configurations
Volume range [mm] Position [mm] Markers
x y z x y z Ref. Mov.
Knee 42–71 42–83 36–52 �38–49 1–42 68–153 7–9 3–6
Hip 34–58 46–157 28–71 �33–34 �3–28 441–597 5–9 3–6
Ranges for the spanned volume, position of marker centre of gravity, and number of markers in the two segments are given.
Table 2
Absolute motions between double examinations
Euler angles [j] Translation [mm] Condition number
x y z x y z Ref. Mov.
Knee �3–4 �9–9 �2–1 �21–8 �4–8 �12–10 12–33 19–113
Hip �3–1 �5–47 �3–8 �337–42 �28–36 �24–164 20–48 38–145
Ranges for Euler angles, translation of centre of gravity, and segment condition numbers are given.
N. Borlin / ISPRS Journal of Photogrammetry & Remote Sensing 56 (2002) 390–400394

into a rotation about the segment centre of gravity
(Euler angles) and a translation of the segment centre
of gravity.
The calculated absolute motion of the reference
segment was applied to all markers in P1 to get a
synthetic position PV2 which was approximately at P2
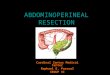
Fig. 3. Results based on 10,000 simulated knee and hip double examinations, respectively. The position and translation errors are given along
each axis. The rotation error is given for each of the Euler angles. The mean error of rigid body fitting is given for both segments. Error bars
show meanF2 standard deviations for Appendix A (– ), Appendix B (���), Appendix C (– – ), and Appendix C (– �), except for the fitting error
where the RMS of the fitting residuals+2 standard deviations is shown.
N. Borlin / ISPRS Journal of Photogrammetry & Remote Sensing 56 (2002) 390–400 395

but with a relative segment motion between P1 and PV2of exactly zero.
4. Evaluation
The synthesized projections and patient marker
positions P1 and PV2 were taken as ‘‘ground truth’’ in
simulated exposures of the patient markers.
For each clinical set-up, marker projections in the
two images were simulated by Eq. (B.1). White
Gaussian noise of a reasonable standard deviation
r=50 Am was added to simulate measurement errors.
The projection geometries and patient marker
positions were reconstructed from the ‘‘measured’’
coordinates by the Selvik algorithm (Appendix A),
the ICDLT algorithm (Appendix B), the ICDLTI
algorithm with one patient marker (Appendix C),
and the ICDLTI algorithm with all patient markers
(Appendix C). The average difference between the
reconstructed and the true marker positions were
recorded in each of n=1000 simulations of the 20
biplanar and 20 uniplanar projections. Furthermore,
the relative segment motion between the simulated
double examinations was calculated. The mean error
of rigid-body fitting, i.e. the root mean square of the
marker fitting residuals (Selvik, 1989), was also
recorded.
The evaluation of the synthetic data was supple-
mented with the corresponding relative motions cal-
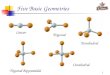
Fig. 4. Results based on double examination of 10 knee and 10 hip patients. Same layout as Fig. 3, except that the position error cannot be
estimated.
N. Borlin / ISPRS Journal of Photogrammetry & Remote Sensing 56 (2002) 390–400396

culated from the clinical data (i.e. between P1 and
P2).
5. Results
The simulation results are illustrated in Fig. 3. The
biplanar position error is almost isotropic, approxi-
mately (45, 33, 49) Am ((x,y,z), two standard devia-
tions). The corresponding figures for the uniplanar
configuration is (186, 135, 612) Am, i.e. approxi-
mately 4� larger for the x and y directions, and
12� larger in the z direction.
Similar relations between the axes are seen for the
translation errors, but while the biplanar errors are
approximately doubled, the uniplanar errors are
reduced by approximately 30%, 20%, and 60% for
the three axes, respectively.
The pattern for the rotation angles is rather differ-
ent. The biplanar angle errors (0.21, 0.18, 0.23)j((x,y,z), two standard deviations) has about the same
proportions as the biplanar translation errors, but the
uniplanar angle errors (0.40, 0.50, 0.17)j are roughly
inversely proportional to the uniplanar translation
error, with the largest error about the y axis and the
smallest about the z axis.
The average fitting error is about 80 Am for the
knee segments and 90 Am for the hip segments.
A comparison of the reconstruction algorithms
consistently shows the more complex algorithms to
be equal or better than the simpler ones. However, for
the biplanar simulations, the differences between
Appendices B and C are very small. Compared to
Appendix A, the position errors are reduced by about
25% and the other errors by 2–7%.
The improvements for the uniplanar set-up are
more varied. The 28% reduction of the position error
by Appendix C is comparable to the biplanar
improvements, while the improvements for Appendi-
ces B and C (6% and 15%, respectively) are not.
Appendices B and C shows similar translation, rota-
tion, and fitting reductions (13%, 2%, and 27–29%,
respectively), with Appendix C topping the list with
19%, 5%, and 33% reductions, respectively.
For the clinical results, illustrated in Fig. 4, the
relations between axes and configurations are similar
to the simulations. However, the algorithmic differ-
ences are small and inconsistent. For the most sensi-
tive parameters in the uniplanar configuration—z
translations and y rotations—the improvements are
similar to the simulations. For some other parameters,
the smallest error is produced by Appendix A.
6. Discussion
Several comparisons between different photogram-
metric reconstruction algorithms have been perform-
ed (e.g. Hatze, 1988; Gazzani, 1993). Their applic-
ability to radiostereometry was however considered
uncertain, since they were performed in optical set-
tings including lens distortion effects, something not
appearing in X-ray photogrammetry (Selvik, 1989).
An investigation of the performance of different
reconstruction algorithms on radiostereometric set-
ups was therefore considered interesting, especially
since the Selvik algorithm may be considered a sim-
plification of a bundle adjustment problem. Yuan and
Ryd (2000) performed a similar analysis on the re-
section– intersection part of radiostereometry, but
used the Selvik algorithm ‘‘backwards’’ to simulate
the projection, and it is unclear whether the relation-
ship between the focus position and the projective
transformation parameters was retained.
The algorithmic results for the synthetic data show
that the most advanced Appendix C reduces the
translation error with 7% for the biplanar configura-
tion and 19% for the uniplanar configuration. The
corresponding reductions for the rotation angles are
2% and 5%, respectively. However, Appendix C
requires the correspondence problem between images
to be solved beforehand, which is judged less feasible
and renders an independent verification of the recon-
structed markers more difficult. A single marker
correspondence needed by Appendix C is probably
more reasonable to expect, but since the performance
of the simpler Appendix B is essentially the same, it
should be favoured. Appendix B also allows the cor-
respondence problem to be solved independently by,
e.g. the Nystrom et al. (1994) algorithm.
On the clinical data, the results are inconclusive. A
possible explanation for this is the relatively small
differences in algorithm performance together with
the low number of patients. Modelling errors is another
possibility; the formulation of the bundle algorithms
assigns the whole error budget to the 2D measure-
N. Borlin / ISPRS Journal of Photogrammetry & Remote Sensing 56 (2002) 390–400 397

ments. In reality, a number of other error sources are
present, e.g. imperfect cages, film unflatness, patient
motion between nonsimultaneous exposures, and the
size of the X-ray focal spot. Furthermore, the 2D
measurement errors are assumed to be isotropic and
the image coordinate system is assumed to be orthog-
onal and without scaling errors, which may or may not
be true.
The results in this paper show that the uniplanar
configuration has an anisotropic error distribution,
which is consistent with previous findings, e.g. Wol-
tring et al. (1985). The size of the error is higher than
for the biplanar configuration. This is probably a
combined effect of the weak projection geometry
and that the measurements are performed outside the
calibrated volume. It is interesting that the relatively
high position errors—4–12� higher than the biplanar
configuration—correspond to motion errors that for
some parameters (x and y translation, z rotation) are
comparable with the biplanar set-up. The relations
between the motion parameter errors are consistent
with previous clinical RSA results (Karrholm et al.,
1997).
Algorithmic changes for medical applications
should be done conservatively, and the arguments for
a change should be strong. This is currently not the
case. Furthermore, it could be argued that the Selvik
algorithm is more robust due to its linear subproblems.
Further studies with more patients and/or phantoms
will have to be performed in order to find out how
much of the improvements seen in the simulated data
can be carried over to clinical radiostereometry.
Appendix A. The Selvik reconstruction algorithm
In the Selvik reconstruction algorithm (Selvik,
1989), the resection is performed in two steps fol-
lowed by intersection.
Consider a projective transformation between a
fiducial marker p in the fiducial plane and its projec-
tion q in the film plane
q ¼ hðpÞ ¼ ATpþ b
vTpþ 1;
where A is a 2�2 matrix and b and v are two-vectors.
Given the known fiducial plane coordinates pi and the
measured film plane coordinates qi, the parameters of
the projective transformation are calculated by solving
the problem
minA;b;v
X
i
NhðpiÞ � qiN2: ðA:1Þ
This nonlinear least squares problem is solved
iteratively with a Gauss–Newton algorithm with
line-search (see e.g. Nash and Sofer, 1996, chaps.
10 and 13).
Given the solution of Eq. (A.1), the measured
coordinates are rectified by the inverse projection
h�1. For a fiducial plane parallel to the xy-plane,
the fiducial plane coordinate si=[h�1(qi)
T,z0]T, where
z0 is the (constant) level of the fiducial plane.
The position of the focus is calculated as the
‘‘closest point of convergence’’ of the bundle of
rays S i(a)=api+(1�a)(si�pi) passing through the
true control point coordinates ci and their rectified
fiducial plane coordinates si. The focus f is thus
calculated as the solution of the linear least squares
problem
minf ;ai
X
i
Nf � S iðaiÞN2: ðA:2Þ
The 3D position pi of each patient marker is
calculated by minimizing the object space distance
to the two X-rays going from the foci f (1) and f (2) to
the projection points si(1) and si
(2), respectively. This
corresponds to the linear least squares problem
minpi;a1;a2
Npi � S 1ða1ÞN2 þ Npi � S 2ða2ÞN2; ðA:3Þ
where S j(a)=af ( j)+(1�a)(si( j)�f ( j)) are the lines con-
necting the two foci with the marker projection point
si( j) in the fiducial planes.
Appendix B. The ICDLT algorithm
In the Iterative Constrained DLT reconstruction, all
cage marker are used as control points, and the
relation between the focus, the cage, and the image
is found in one step.
To simplify the notation of the following problems,
define the central projection triplet h={A,b,v}, whereA is a 3�2 matrix, b is a two vector, and v is a three
N. Borlin / ISPRS Journal of Photogrammetry & Remote Sensing 56 (2002) 390–400398

vector. Furthermore, define the central projection
function
CPðh; pÞ ¼ ATpþ b
vTpþ 1; ðB:1Þ
which is the DLT version of the collinearity equations.
The elements in A, b, and v correspond to the L1, L2,
. . ., L11 parameters in Eqs. (4.40) and (4.41) of
McGlone (1989, p. 47) and may be used to calculate
the inner and outer orientation parameters, see e.g.
McGlone (1989, p. 47, Eqs. (4.43) and (4.44))2 or
Melen (1995).
A central projection h is called orthonormal if it
satisfies the orthonormality conditions
ðaT1a2ÞðvTvÞ ¼ ðaT1vÞðaT2vÞ;
ðaT1a1 � aT2a2ÞvTv ¼ ðaT1vÞ2 � ðaT2vÞ
2; ðB:2Þ
where a1 and a2 are the columns of A. The constraints
(Eq. (B.2)) correspond to Eq. (4.45) in McGlone
(1989, p. 48)3 and specifies that the axes of the image
coordinate system are orthogonal and have the same
scale.
With the above definitions, and given the known
cage marker coordinates pi and their measured film
plane coordinates qi, the actual problem solved is the
following constrained nonlinear least squares problem
minh;fqig
X
i
Nqi � qiN2; ðB:3aÞ
s:t: qi ¼ CPðh; piÞ; ðB:3bÞ
h orthonormal: ðB:3cÞ
Eqs. (B.3a)–(B.3c) has 9 degrees of freedom and is
mathematically equivalent to the self-calibration bun-
dle adjustment problem.
Eqs. (B.3a)–(B.3c) is formulated for each focus
independently and solved iteratively with a SQP-
based method (Nash and Sofer, 1996, chap. 15).
Given the solution h1 for focus 1 and h2 for focus2, the position of each patient marker pi is calculated
from its measured coordinates qi(1) and qi
(2) in the two
images as the solution of
minpi;q
ð1Þi;q
ð2Þi
Nqð1Þi � qð1Þi N2 þ Nqð2Þi � q
ð2Þi N2
; ðB:4aÞ
s:t: qð1Þi ¼ CPðh1; piÞ; ðB:4bÞ
qð2Þi ¼ CPðh2; piÞ; ðB:4cÞ
i.e. by minimizing the image space error rather than
the object space error as in Eq. (A.3). Eqs. (B.4a)–
(B.4c) is solved by the same algorithm as Eqs.
(B.3a)–(B.3c).
Appendix C. The ICDLTI algorithm
In the Iterative Constrained DLT and Intersection
algorithm, the two projection geometries and the
position of one or more of the patient markers are
found simultaneously.
Denote a set of patient markers P and the focus 1
and focus 2 cage markers C1 and C2, respectively.
Then the mathematical problem is
min
h1; fqð1Þi g;h2; fqð2Þi g;
P
X
i
Nqð1Þi � qð1Þi N2 þ
X
i
Nqð2Þi � qð2Þi N2
;
ðC:1aÞ
s:t: qð1Þi ¼ CPðh1; piÞ; bpia P;C1; ðC:1bÞ
h1 orthonormal; ðC:1cÞ
qð2Þi ¼ CPðh2; piÞ; bpia P;C2; ðC:1dÞ
h2 orthonormal; ðC:1eÞ
which is solved with the same algorithm as Eqs.
(B.3a)–(B.3c).
2 However, note the following typographic errors; in Eq. (4.43),
x0 should be xp and y0 should be yp in the cx and cy equations,
respectively; the kappa equation should read j=cos�1(m11/cos /),and one of the sides of Eq. (4.44) should have the opposite sign.
3 However, note that the first equal sign of Eq. (4.45) should be a
minus sign and should thus read (L12+L2
2+L32)�(L5
2+L62+L7
2)+���.
N. Borlin / ISPRS Journal of Photogrammetry & Remote Sensing 56 (2002) 390–400 399

Given the solution of Eqs. (C.1a)– (C.1e), the
position of any remaining patient markers not used
in the resection is calculated as the solution of Eqs.
(B.4a)–(B.4c).
References
Borlin, N., Karrholm, J., 1997. Radiostereometry based on digitized
radiographs. Proceedings of the 43rd Annual Meeting of The
Orthopaedic Research Society. ORS, San Francisco, CA, p. 626,
Feb.
Borlin, N., Thien, T., Karrholm, J., 2002. The precision of radio-
stereometric measurements. Manual vs. digital measurements.
Journal of Biomechanics 35 (1), 69–79.
Gazzani, F., 1993. Comparative assessment of two algorithms for
calibrating stereophotogrammetric systems. Journal of Biome-
chanics 26 (12), 1449–1454.
Hatze, H., 1988. High-precision three-dimensional photogrammetric
calibration and object space reconstruction using a modified
DLT-approach. Journal of Biomechanics 21 (7), 533–538.
Karrholm, J., 1989. Roentgen stereophotogrammetry, review of or-
thopaedic applications. Acta Orthopaedica Scandinavica 60 (4),
491–503.
Karrholm, J., Herberts, P., Hultmark, P., Malchau, H., Nivbrant, B.,
Thanner, J., 1997. Radiostereometry of hip prostheses—review
of methodology and clinical results. Clinical Orthopaedics and
Related Research (344), 94–110.
McGlone, J.C., 1989. Analytical data-reduction schemes in non-
topographic photogrammetry. In: Karara, H.M. (Ed.), Non-
Topographic Photogrammetry, 2nd edn. American Society for
Photogrammetry and Remote Sensing. Bethesda, MD, pp. 37–
57, chap. 4.
Melen, T., 1995. An ambiguity free decomposition of the direct
linear transformation (DLT) matrix. In: Gruen, A., Kahmen,
H. (Eds.), Optical 3-D Measurement Techniques III. Wich-
mann-Verlag, Heidelberg, pp. 496–505.
Nash, S.G., Sofer, A., 1996. Linear and Nonlinear Programming
McGraw-Hill, NY.
Nystrom, L., Soderkvist, I., Wedin, P.-A., 1994. A note on some
identification problems arising in roentgen stereophotogrammet-
ric analysis. Journal of Biomechanics 27 (10), 1291–1294.
Østgaard, S.E., Gottlieb, L., Toksvig-Larsen, S., Lebech, A., Talbot,
A., Lund, B., 1997. Roentgen stereophotogrammetric analysis
using computer-based image-analysis. Journal of Biomechanics
30 (9), 993–995.
Selvik, G., 1989. Roentgen stereophotogrammetry, a method for the
study of the kinematics of the skeletal system. Acta Orthopaed-
ica Scandinavica 60 (4), 1–51, suppl. 232. Reprint of the 1974
thesis.
Soderkvist, I., Wedin, P.-A., 1993. Determining the movements of
the skeleton using well-configured markers. Journal of Biome-
chanics 26 (12), 1473–1477.
Soderkvist, I., Wedin, P.-A., 1994. On condition numbers and algo-
rithms for determining a rigid-body movement. BIT (Nordic
Journal for Information Processing) 34 (3), 424–436.
Stokes, I.A.F., 1995. X-ray photogrammetry. In: Allard, P., Stokes,
I.A.F., Blanchi, J.-P. (Eds.), Three-Dimensional Analysis of
Human Movement. Human Kinetics, Champaign, IL, pp.
125–141, chap. 7.
Valstar, E.R., Vrooman, H.A., Toksvig-Larsen, S., Ryd, L., Nelis-
sen, R.G.H.H., 2000. Digital automated RSA compared to man-
ually operated RSA. Journal of Biomechanics 33 (12), 1593–
1599.
Vrooman, H.A., Valstar, E.R., Brand, G.J., Admiraal, D.R., Rozing,
P.M., Reiber, J.H.C., 1998. Fast and accurate automated meas-
urements in digitized stereophotogrammetric radiographs. Jour-
nal of Biomechanics 31 (5), 491–498.
Woltring, H.J., Huiskes, R., de Lange, A., Veldpaus, F.E., 1985.
Finite centroid and helical axis estimation from noisy landmark
measurements in the study of human joint kinematics. Journal of
Biomechanics 18 (5), 379–389.
Yuan, X., Ryd, L., 2000. Accuracy analysis for RSA: a computer
simulation study on 3D marker reconstruction. Journal of Bio-
mechanics 33 (4), 493–498.
N. Borlin / ISPRS Journal of Photogrammetry & Remote Sensing 56 (2002) 390–400400