Embed Size (px)
Citation preview

FULL ARTICLE
Comparison of pulsed photothermal radiometry, opticalcoherence tomography and ultrasound for melanomathickness measurement in PDMS tissue phantoms
Tianyi Wang*; 1, Srivalleesha Mallidi1, Jinze Qiu1, Li L. Ma2, Amit S. Paranjape1,Jingjing Sun1, Roman V. Kuranov1; 3, Keith P. Johnston2, and Thomas E. Milner1
1 Department of Biomedical Engineering, University of Texas at Austin, Austin, Texas 78712, USA2 Department of Chemical Engineering, University of Texas at Austin, Austin, Texas 78712, USA3 Department of Ophthalmology, University of Texas Health Science Center at San Antonio, San Antonio, Texas 78229, USA
Received 29 June 2010, revised 10 September 2010, accepted 30 September 2010Published online 16 October 2010
Key words: malignant melanoma, PDMS tissue phantom, pulsed photothermal radiometry, optical coherence tomography,ultrasound, Monte Carlo simulation, three-dimensional heat transfer model
1. Introduction
Cutaneous malignant melanoma (MM) is a serioustype of cancer [1], accounting for 75% of all deathsassociated with skin cancer [2]. Around 160,000 new
cases of MM are diagnosed worldwide each year [3].The American Cancer Society (ACS) estimates thatthere will be 68,130 cases of melanoma (38,870 casesin males; 29,260 cases in females) and 8,700 melano-
# 2011 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim
Journal of
BIOPHOTONICS
Melanoma accounts for 75% of all skin cancer deaths.Pulsed photothermal radiometry (PPTR), optical coher-ence tomography (OCT) and ultrasound (US) are non-invasive imaging techniques that may be used to meas-ure melanoma thickness, thus, determining surgical mar-gins. We constructed a series of PDMS tissue phantomssimulating melanomas of different thicknesses. PPTR,OCT and US measurements were recorded from PDMStissue phantoms and results were compared in terms ofaxial imaging range, axial resolution and imaging time.A Monte Carlo simulation and three-dimensional heattransfer model was constructed to simulate PPTR meas-urement. Experimental results show that PPTR and UScan provide a wide axial imaging range (75 mm–1.7 mmand 120–910 mm respectively) but poor axial resolution(75 and 120 mm respectively) in PDMS tissue phantoms,while OCT has the most superficial axial imaging range(14–450 mm) but highest axial resolution (14 mm). TheMonte Carlo simulation and three-dimensional heattransfer model give good agreement with PPTR meas-
urement. PPTR and US are suited to measure thickermelanoma lesions (>400 mm), while OCT is better tomeasure thin melanoma lesions (<400 mm).
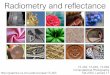
Schematic diagram of PPTR instrumentation.
* Corresponding author: e-mail: [email protected], Phone: +01 512 529 5886
J. Biophotonics 4, No. 5, 335–344 (2011) / DOI 10.1002/jbio.201000078

ma deaths (5,670 in males; 3,030 in females) in theUnited States in 2010 [4]. The lifetime risk for devel-oping MM has increased from 1 in 1500 in 1930 to1 in 50 in 2010 in the United States [5, 6]. Theaetiology of MM is uncertain but is thought to re-late to increased exposure to ultraviolet radiation[7]. The MM invasion depth named Breslow thick-ness [8] is the single most important factor forMM staging and closely related to survival rate [9].The five-year survival rate is 95–100% if melano-ma thickness is less than 1 mm, while the survivalrate is reduced to 50% if the tumor thickness isgreater than 4 mm. Current surgical treatment forprimary MM has often been an excision with amargin determined by the thickness of MM. Sincethe risk of local recurrence is dependent on melano-ma thickness, a narrow margin of 5 mm is recom-mended for in-situ melanomas, 1 cm for tumors lessthan 1 mm, 1–2 cm for tumors between 1.01 and2 mm, and 2 cm for tumors thicker than 2.01 mm[10]. Because sentinel lymph node highly correlateswith the metastatic status of MM, a sentinel lymphnode dissection (SLND) procedure is also performedon patients with intermediate thickness (1–4 mm) le-sions [11, 12].
The assessment of MM in the clinical setting isoften difficult, and important features such as depthand lateral extent of MM remain unknown until thepathology report is received. Non-invasive assess-ment to melanoma thickness in vivo for preoperativestaging purposes would offer a basis for guidance indefining surgical margins, operating on patients in asingle procedure avoiding further re-excision andearly planning of treatment options like SLND. Op-tical coherence tomography (OCT) is an emergingmedical diagnostic imaging technique that providesin vivo structure and function of tissues by measuringbackscattered or backreflected light. OCT is based onthe principle of Michelson interferometry. The lightsources used for OCT imaging of skin are broad-bandsuperluminescent diodes operating at a wavelengthof about 1300 nm or tunable laser sources [13]. OCTwas originally developed for diagnosis in ophthalmol-ogy and has been used clinically to evaluate a widerange of retinal-macular diseases [14]. Currently, thetechnology has been advanced to micromorphologyof highly scattering tissues such as skin and gavepromising results [15, 16]. A recent study of MMcharacterization by OCT examined a panel of mela-nomas and benign nevi and demonstrated that mela-nomas showed increased architectural disarray, lessdefined dermal-epidermal borders, and vertically or-iented icicle-shaped structures not seen in nevi [17].The utility of OCT for early-stage melanoma (i.e.,<1 mm) thickness measurement has not been fullyestablished because sensitivity and/or specificity stu-dies for melanoma detection by OCT have not beenreported.
Ultrasound (US) is an analogy to OCT – themain difference being that broadband light source isreplaced by ultrasound pulses. An ultrasound trans-ducer transmits sound pulses and then receives back-scattered echo signals. Because the interfaces be-tween tissues have different acoustic impedancesand therefore different reflectivities, the received ul-trasound signal contains boundary information of tis-sue with different properties. US is used to visualizesubcutaneous structures including muscles, tendons,vessels and internal organs to identify pathologies orlesions [18–20]. A prospective study and systematicreview of literature from 1987 to 2007 on melanomathickness measurement using 20 MHz ultrasound re-ported that ultrasound was able to measure melano-ma thicknesses between 0.4 and 7.6 mm, and demon-strated a linear correlation between ultrasound andhistology in melanoma thickness measurements [21].
Pulsed photothermal radiometry (PPTR) is basedon the time-resolved acquisition of infrared (IR)emission from a sample after pulsed laser exposure.PPTR was applied to depth profiling of stronglyscattering or absorbing tissues and tissue phantoms[22, 23], including blood vessels in port wine stain(PWS) birthmarks in human skin [24]. Inasmuch asdifferent chromophore thicknesses can provide dif-ferent laser induced initial temperature profiles andeventually produce different radiometric tempera-tures [25], the authors propose that relationship be-tween melanoma thickness and detected radiometrictemperature increase can be determined using PPTR.
In order to better understand the advantages anddisadvantages of each of these candidate imagingtechniques on MM thickness measurement for pre-operative staging and surgical margin definition pur-poses, it is important to compare PPTR, OCT andUS in terms of axial imaging range, axial resolutionand imaging time in PDMS tissue phantoms simulat-ing MM. Recommendations for future studies aremade on the basis of comparisons.
2. Materials and methods
2.1 Preparation of tissue phantoms
In a previous paper a two-layered skin-tissue phan-tom for simulating pigmented skin lesions has beendescribed [26]. The basic structure consists of a le-sion layer and a skin layer. In this study, a series ofpolydimethylsiloxane (PDMS) tissue phantoms (Fig-ure 1a) are prepared in a two-layered geometry(top-layer and substrate for simulating MM lesionand skin respectively) with different top-layer thick-nesses (Figure 1b) simulating melanomas of differentthicknesses. The top-layer (120 mm, 250 mm, 450 mm,
Tianyi Wang et al.: Comparison of PPTR, OCT and US for melanoma thickness measurement in tissue phantoms336
Journal of
BIOPHOTONICS
# 2011 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim www.biophotonics-journal.org

730 mm, 910 mm, 1.3 mm, 1.7 mm, 2.3 mm and 2.8 mm)is composed of PDMS, nanorose (a strong NIR ab-sorber [27]) and TiO2, while the substrate (10 mm) iscomposed of only PDMS and TiO2. The top-layerswere produced by pouring a PDMS solution onto amicroscope slide with two identical spacers posi-tioned near the ends of the slide. A second micro-scope slide was placed on top of the PDMS solutionand gently pressed against the spacers. When poly-merization was complete after 24 hours, the top slidewas carefully removed, exposing a layer of uniformthickness.
2.2 Experimental setup
PPTR
A lens coupled fiber optic laser (Opto Power, Inc.;Model FCTS/B) with adjustable output power and amaximum 5 W output at a wavelength of 800 nm wasused to irradiate tissue phantoms. The pulse durationwas 30 ms. A small fraction of incident laser energywas reflected using a dichroic onto a radiant energymeter. The first several pulses were blocked fromimpinging on the tissue phantom until stable energymeter readings were obtained. A 50 mm diameterlens (f ¼ 40 cm) was used to produce a 6 mm diam-eter laser beam on the tissue phantom surface. TheIR signal (radiometric temperature) from the tissuephantom was reflected by the same dichroic andthen recorded by an infrared camera (FLIR ThermalInfrared Camera Systems, Inc.; Model: Thermo-Vision SC6000 with an InSb detector (3.0–5.0 mm)).Instrumentation for the PPTR measurement is ar-ranged as depicted in Figure 2.
OCT
A swept source (SS) laser (Santec, Inc; Model HSL-2000) scanning at a repetition rate of 20 KHz wasused in the laboratory prototype of the intensityOCT system. The laser provided real time imagingat a rate of 20 B-scans per second (1024 A-scans per
B-scan), and was set to produce an average outputpower of 7 mW with a Gaussian-shape FWHM spec-tral bandwidth of 100 nm, centered at 1320 nm. Thesample arm power was 2.3 mW. The power returnedfrom reference arm to the detector was set to 20 mWto give optimal system SNR. These parameters cor-responded to a measured free space axial resolutionof 20 mm. The B-scan image acquisition time wasapproximately 50 ms. Scan depth was approximately3.5 mm. The OCT signal was sampled with an isotro-pic frequency sampling clock which allowed real-time OCT image acquisition and display [28]. A por-tion of source laser light was directed into a Mach-Zehnder clock interferometer. The output of theclock interferometer was converted into electricalsignal by a balanced detector, combined with an arti-ficial clock by a fast electrical switch and used as aninput of the external clock port of the ADC card(Figure 3).
Figure 1 (online color at:www.biophotonics-journal.org)(a) Digital image of PDMS tissuephantom. (b) Schematic diagram ofa two-layered tissue phantom struc-ture.
Figure 2 (online color at: www.biophotonics-journal.org)Schematic diagram of PPTR instrumentation to measurethe radiometric temperature increase of two-layered PDMStissue phantoms in response to pulsed laser (800 nm) irra-diation.
J. Biophotonics 4, No. 5 (2011) 337
FULLFULLARTICLEARTICLE
# 2011 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheimwww.biophotonics-journal.org

US
A pulser (Panametrics, Inc; Model 5910PR) and asingle element ultrasound transducer (f# ¼ 2) with acentral frequency of 25 MHz and a bandwidth of70% were used to generate and receive high-fre-quency ultrasound signals. The characteristics of thetransducer determined the resolution of the labora-tory prototype of the US system. The central fre-quency, bandwidth and f# of the ultrasound transdu-cer provided a lateral resolution of 120 mm and anaxial resolution of 50 mm in free space. The transdu-cer was immersed in water inside a plastic containerwith an opening at the top. The PDMS tissue phan-tom was placed inside the container under the trans-ducer. A mechanical stage provided lateral scanningof the transducer, which allowed recording a cross-sectional B-scan image. The received ultrasound sig-nals first underwent 64 dB amplification, and werethen digitized by an 8-bit, 500 MS/s digitizer (Fig-ure 4).
Monte Carlo simulation andthree-dimensional heat transfer model
A Monte Carlo simulation in combination with athree-dimensional heat transfer model was com-pleted to compute fluence distribution and radio-metric temperature increase in tissue phantoms. Op-tical properties of the tissue phantoms simulatingMM for Monte Carlo simulation are given in Table 1[29].
We derived an expression for PPTR radiometrictemperature increase DR(x, y, t) as a convolution in-tegral (see Eq. (2) below) in terms of the initialthree-dimensional temperature increase DT3-D(x, y, z,t ¼ 0) in the tissue phantom immediately followingpulsed laser irradiation. For the purpose of our ana-lysis we assumed that the tissue phantom occupieda semi-infinite half-space and that the plane posi-tioned at z ¼ 0 was coincident with the boundarysurface. Radiative and convective thermal losses atthe air-material interface were modeled with a Ro-bin boundary condition:
kd DT
dzjz¼0 ¼ h DT jz¼0 ð1Þ
At the tissue phantom surface (z ¼ 0), heat fluxQ ¼ �kd DT=dz is proportional to the surface tem-perature increase Q ¼ �h DT, where assumed val-ues of thermal conductivity (k) and heat transfercoefficient (h) are, respectively, 0.15 W �m�1 �K�1
and 50 W �m�2 �K�1 [30]. The algebraic expressionfor the PPTR radiometric temperature increase [31–33] is given by:
DRðx; y; tÞ ¼Ð
x
Ð
h
Ð
&
dx dh d& � DT3�Dðx; h; &; t ¼ 0Þ
�KTðx� x; y� h; &; tÞ ð2ÞWhere KT is the three-dimensional thermal pointspread function given by:
KTðx� x; y� h; &; tÞ ¼ Krðx� x; y� h; tÞKzð&; tÞ ð3Þand consists of two physically distinct terms (seeEq. (4a–b) below) that represent respectively heatdiffusion along lateral (Kr) and longitudinal (Kz) di-rections,
Krðx; y; tÞ ¼ 1=½pð4DtÞ� � e�ðx2þy2Þ=4Dt ð4aÞ
Figure 3 (online color at: www.biophotonics-journal.org)Schematic diagram of the intensity OCT system.
Figure 4 (online color at: www.biophotonics-journal.org)Schematic diagram of ultrasound imaging system.
Table 1 Refractive index (n), absorption coefficient (ma),scattering coefficient (ms), anisotropy factor (g) and singlelayer thickness (d) parameters for Monte Carlo simulationof light transport in PDMS tissue phantoms.
Layer n ma (cm�1) ms (cm�1) g d(mm)
1 1.43 8 120 0.9 0.12–2.82 1.43 0.33 120 0.9 10
Tianyi Wang et al.: Comparison of PPTR, OCT and US for melanoma thickness measurement in tissue phantoms338
Journal of
BIOPHOTONICS
# 2011 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim www.biophotonics-journal.org

Kzð&; tÞ ¼ ðmIR=2Þ � e�&2=4DtferfcxðuþÞ þ erfcxðu�Þ� f2ðh=kÞ=½ðh=kÞ � mIR�g½erfcxðuþÞ� erfcxðu1Þ�g ð4bÞ
Here, erfcx(u) ¼ exp (u2) erfc(u) is the exponentialcomplementary error function and u�, 1 are functions(Eq. (5)) of space (z), time (t), thermal diffusivity(D) and IR absorption coefficient (mIR):
u� ¼ mIR
ffiffiffiffiffiffiDtp
� z=ð2ffiffiffiffiffiffiDtpÞ; u1 ¼ h
ffiffiffiffiffiffiDtp
þ z=ffiffiffiffiffiffiDtp
ð5Þ
3. Results and discussion
PPTR
PPTR measurements of nine two-layered PDMStissue phantoms with different top-layer thicknesses(120 mm–2.8 mm) were recorded. A thirty-secondmovie was recorded by the infrared camera at 40frames per second. Figure 5a–b shows the measuredradiometric temperature increase at the center ofthe laser beam on the surface of the PDMS tissuephantoms. The initial radiometric temperature in-crease at phantom surface after the laser pulse was
normalized. Normalization did not introduce discre-pancies since our analysis of PPTR signals was direc-ted at decay time. PPTR signals were recorded fromeach PDMS phantom with three pulses at the samelocation, and an average was computed and plotted.The nine measured PPTR signals corresponding todifferent top-layer thicknesses were distinguishedfrom one another in plots of radiometric tempera-ture versus time. Thicker top-layers produced slowerradiometric temperature decays. Using the initialtemperature distribution determined from the MonteCarlo simulation, the radiometric temperature in-crease versus time was computed from the three-dimensional heat transfer model (Eq. (2)) and dis-played in Figure 5c–d. Both experimental and simu-lated results showed that when the top-layer wasthicker than 1.7 mm, no significant change in decayof radiometric temperature increase was observedover the thirty-second recording period.
Decay time is defined as the time required forthe peak radiometric temperature increase to decayto 37% of the maximum [34]. Based on experimentaland simulated results, the decay times of the PDMStissue phantoms with different top-layer thicknessesare compared (Figure 6). The decay time becomeslonger as the top-layer thickness increases from120 mm to 2.8 mm. No significant change in decaytime is observed when the top-layer is thicker than
Figure 5 (online color at:www.biophotonics-journal.org)(a) Measured radiometric tempe-rature increase from PDMS tissuephantoms (top-layer is 120 mm–2.8 mm thick respectively). (b)Measured radiometric temperatureincrease in the window indicated in(a). (c) Simulated radiometric tem-perature increase. (d) Simulatedradiometric temperature increasein the window indicated in (c). Thedashed lines in (a, c) indicate whenpeak radiometric temperature in-crease decays to 37% of the maxi-mum.
J. Biophotonics 4, No. 5 (2011) 339
FULLFULLARTICLEARTICLE
# 2011 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheimwww.biophotonics-journal.org

1.7 mm. The trend of decay times for experimentalresults and simulation are nearly equal. Decay timesfor simulation are smaller than experimental resultswhen the top-layer thicknesses are less than 450 mmand larger when the top-layer thicknesses are great-er than 450 mm. The axial resolution of PPTR iscomputed to be 75 mm from the error bars in Fig-ure 6. PPTR is able to distinguish top-layer thick-nesses between 75 mm and 1.7 mm.
OCT
A series of B-scan OCT images were recorded fromPDMS tissue phantoms with different top-layerthicknesses. Recorded OCT images of the tissuephantoms with top-layer thicknesses ranging from120 mm to 730 mm are shown in Figure 7. Plots ofgray value versus depth along white lines in all OCTimages are shown. The axial resolution of OCT iscomputed to be 14 mm from Eq. (5).
RPDMS ¼ Rf =nPDMS ð5ÞWhere RPDMS, Rf , nPDMS are, respectively, axialresolution in PDMS tissue phantom, axial resolutionin free space and refractive index of PDMS tissuephantom. Sharp boundaries between the two layersof PDMS are identified in phantoms with top-layerthicknesses of 120 mm, 250 mm, 450 mm (Figure 7a–c),but not 730 mm (Figure 7d). Therefore, in experi-ments reported here OCT is able to distinguish top-layer thicknesses between 14 mm and 450 mm.
US
A series of B-scan ultrasound images were recordedfrom the PDMS tissue phantoms with differenttop-layer thicknesses. The ultrasound images of thetissue phantoms with top-layer thicknesses rangingfrom 120 mm to 1.3 mm are shown in Figure 8. Plotsof gray value versus depth along white lines in allultrasound images are shown. Sharp boundaries be-tween the two layers of PDMS are seen in phantomswith top-layer thicknesses of 250 mm, 450 mm, 730 mm,
Figure 6 Decay time of the PDMS tissue phantoms withdifferent top-layer thicknesses from experiment (squarebox) and simulation (dashed line).
Figure 7(a–d) B-scan OCT imagesof PDMS tissue phantoms withtop-layer thicknesses of 120 mm,250 mm, 450 mm and 730 mm respec-tively. Transversal range of B-scanis 5 mm. Arrow(s) in each grayvalue plot points to the boundarydepth of top-layer.
Tianyi Wang et al.: Comparison of PPTR, OCT and US for melanoma thickness measurement in tissue phantoms340
Journal of
BIOPHOTONICS
# 2011 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim www.biophotonics-journal.org

910 mm (Figure 8b–e), but not 1.3 mm (Figure 8f).Boundary was not clearly observed in the phantomwith a top-layer thickness of 120 mm (Figure 8a).Therefore, in experiments reported here US has theaxial resolution of 120 mm and is able to distinguishtop-layer thicknesses between 120 mm and 910 mm.
Based on simulation and experimental results, a1.7 mm thick top-layer can be distinguished by PPTRin the PDMS tissue phantoms simulating MM. How-ever, PPTR is not able to distinguish thicker top-layers (i.e., 2.0–5.0 mm). Possible reasons are: (1) re-cording time was not sufficiently long to observe adifference in decay of radiometric temperature in-crease in tissue phantoms with a thick top-layer; (2)laser fluence we used in our experiments was insuffi-cient to cause sufficient heating at deeper positionsin tissue phantoms; (3) laser wavelength (800 nm) inour experiments was based on small absorption andscattering coefficients in both melanoma and normaltissue, but was not optimal. Using longer irradiationwavelengths, light can penetrate deeper and largerdecay time differences between tissue phantoms with
thicker top-layers can possibly be observed. The com-puted decay times of simulation results are longer (i.e.,less than 0.7 s) than those in experimental resultswhen top-layer thickness is greater than 450 mm.Although we use a three-dimensional heat transfermodel, several assumptions (i.e., we assume that thetissue phantom occupies semi-infinite half-space) aremade to generate simulation results. In the MonteCarlo simulation and three-dimensional heat transfermodel, we select parameter values for optical prop-erties (i.e., absorption coefficient, scattering coeffi-cient, anisotropy factor) and thermal properties (i.e.,thermal conductivity, thermal diffusivity, heat trans-fer coefficient, infrared absorption coefficient) of thePDMS tissue phantoms. Each parameter is a candi-date source of error, for instance, decay times insimulation results are reduced when the absorptioncoefficient or scattering coefficient increases. An-other factor which may reduce the decay time is thatTiO2 is not homogeneously distributed in PDMSbecause of the action of gravity and a relatively longpolymerization process at room temperature, so that
Figure 8(a–f) B-scan ultrasoundimages of PDMS tissue phantomswith top-layer thicknesses of120 mm, 250 mm, 450 mm, 730 mm,910 mm and 1.3 mm respectively.Transversal range of B-scan is5 mm. Arrow(s) in each gray valueplot points to the boundary depthof top-layer.
J. Biophotonics 4, No. 5 (2011) 341
FULLFULLARTICLEARTICLE
# 2011 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheimwww.biophotonics-journal.org

the initial temperature distribution immediately afterpulsed laser irradiation does not precisely follow anexponential decay in the top-layer, which may resultin faster decay of the radiometric temperature.
OCT is a high resolution optical imaging tech-nique based on differences in tissue scattering prop-erties due to refractive index mismatches [35]. Animportant limitation of OCT is penetration depth.The maximum penetration depth of OCT is currentlybetween 1–2 mm, dependent on the tissue type.Although the use of longer light wavelengths (i.e.,1750 nm) may improve penetration depth, no data isavailable to suggest that penetration depth greaterthan 4 mm is possible in the near future [36]. There-fore, OCT is currently not a good candidate in sta-ging of advanced MMs in which a greater pene-tration depth is required (i.e., >1 mm). Real timefeedback is crucial for the clinical applications. Forthis purpose, high-speed digitizers operating with aninternal sample clock and swept-source lasers usedfor OCT must have a calibration performed betweenthe non-linear sweep of the laser and the constantsampling frequency of the digitizer. The problem canbe solved using a frequency uniform clock [37]. Un-fortunately, no real-time frequency uniform clock forhigh sweep rate (i.e., tens of kHz) and low duty cycle(i.e., <90%) tunable lasers is available commercially.Here we utilized a frequency clock interferometertogether with an artificial clock to ensure real-timeacquisition and display of OCT signal.
Diagnostic ultrasound uses frequencies rangingfrom 1 to 20 MHz. Currently, ultrasound at thefrequency of 2–15 MHz is routinely used clinically[38], while 10–40 MHz ultrasound is mainly used forsmall animal imaging [39, 40]. Ultrasound at higherfrequencies has decreased penetration depth, whereasat lower frequencies less energy is absorbed super-ficially and penetration into deeper tissues is possi-ble [41]. Mallidi et al. measured a penetration depthof 10 mm at the frequency of 25 MHz by using an-other ultrasound phantom (polyvinyl alcohol (PVA)phantom filled with silica and graphite particles) [42].The penetration depth at the frequency of 25 MHzin PDMS phantom is an order of magnitude smallerthan that in PVA phantom due to the difference ofultrasound attenuation coefficient in these two med-ia. According to Kharine’s power law model [43] forPVA, the attenuation coefficient in PVA at thefrequency of 25 MHz is estimated to be 15.6 dB/cmwhereas in PDMS attenuation coefficient is esti-mated to be greater than 64.3 dB/cm [44]. Using anultrasound transducer operating at lower frequencies(i.e., 2–15 MHz) may increase the penetration depth,however, the axial resolution will be compromised.To obtain a better comparison of US with PPTR andOCT, a more appropriate tissue phantom with ultra-sonic and optical properties similar to those of cuta-neous tissue should be explored.
Compared with OCT and US, PPTR requires arelatively long imaging time (30 seconds in our study)to record a series of frames. The imaging time ofOCT and ultrasound is 0.05 s and 0.5 s respectivelyin our study. Therefore, both OCT and US can beused in real-time or near real-time applications.Comparison of PPTR, OCT and US in terms of axialimaging range, axial resolution and imaging time islisted in Table 2.
Because PPTR and US have deeper penetrationdepth than OCT, they are candidates to measureMM thickness prior to surgical resection. If MMthickness is within the range of OCT detection (i.e.,<400 mm), OCT can be applied to better visualizemicrostructures of MM. Because imaging time ofPPTR measurement is relatively longer than that forOCT and US, clinical use of PPTR for MM thicknessmeasurement will need to provide some additionaladvantages such as sensitivity and/or specificity.
4. Conclusion
Because OCT has the highest axial resolution andmost superficial axial imaging range, OCT is best sui-ted to measurement of thin malignant lesions. PPTRand US have relatively lower axial resolution butwider axial imaging range, therefore, PPTR and USare more capable in thicker malignant lesion meas-urement. Our study demonstrates that PPTR, OCTand US can help determining surgical margins basedon measured MM thickness. We believe that PPTR,OCT and US are non-invasive imaging techniquesthat can be used in preoperative assessment of MMthickness, permitting better choice of surgical mar-gins in a single operation, reduce number of unne-cessary biopsies and in some cases avoid a secondwide local excision. They can even be combined withSLND once melanoma is in metastatic progression,minimize the number of re-interventions and, there-fore, prove to be a time and cost saving procedure.Moreover, accurate preoperative measurement ofMM thickness may offer the possibility of savingpart of the primary melanoma routinely processed inhistology examination for research use that may pro-
Table 2 Comparison of PPTR, OCT and US in terms ofaxial imaging range, axial resolution and imaging time(transversal range of B-scan is 5 mm in OCT and US) inPDMS tissue phantoms.
imagingmodalities
axial imagingrange (mm)
axial reso-lution (mm)
imagingtime (s)
PPTR 0.075–1.7 �75 30OCT 0.014–0.45 �14 0.05 (/B-scan)US 0.12–0.91 �120 0.5 (/B-scan)
Tianyi Wang et al.: Comparison of PPTR, OCT and US for melanoma thickness measurement in tissue phantoms342
Journal of
BIOPHOTONICS
# 2011 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim www.biophotonics-journal.org

vide greater understanding of the mechanisms ofmelanoma characteristics and metastatic progression.Based on the results of this tissue phantom study,further in vivo experimentation is warranted.
Acknowledgements The authors thank James Tunnell,Ph.D., Stepan Baranov, Ph.D. and Seungyup Ryoo, MSfor helpful discussions and technical assistance in complet-ing this study. The authors also thank Steven Jacques,Ph.D. and Lihong Wang, Ph.D. for providing MCML soft-ware to complete Monte Carlo simulations.
Tianyi Wang received his B.E. degree in electronic in-formation engineering from Wuhan University, P.R.China, in 2005, and his M.E. degree in optical engineer-ing from Wuhan University, P.R. China, in 2007. He iscurrently working towards his Ph.D. degree in the De-partment of Biomedical Engineering at the Universityof Texas at Austin. He is mainly interested in biome-dical applications of pulsed photothermal radiometry,photothermal wave imaging and optical coherence to-mography.
Srivalleesha Mallidi received her Ph.D. in the Depart-ment of Biomedical Engineering from the University ofTexas at Austin in 2009. Her research involved usinggold nanoparticles and multi-wavelength photoacousticimaging for early detection of cancer with Dr. StanislavEmelianov. Her post-doctoral research at Wellman La-boratories with Dr. Tayyaba Hasan focuses on under-standing the dynamics of singlet oxygen during photo-dynamic therapy.
Jinze Qiu received his B.S. degree in 2003 in appliedphysics from University of Science and Technology,P.R. China, and his Ph.D. in the Department of Biome-dical Engineering at the University of Texas at Austinin 2010. His thesis research includes long pulse laserlithotripsy using Ho : YAG and Er : YAG lasers, and ul-trashort laser lithotripsy using femtosecond lasers. Heis also interested in application of femtosecond laser toskin modification.
Li L. Ma graduated from Tsinghua University, P.R.China, in 2004 with B.E. and M.E. degrees in chemicalengineering. He is pursuing a chemical engineeringresearch program supervised by Professor Keith P.Johnston towards his Ph.D. degree in the University ofTexas at Austin. His research focused on synthesis ofnear-infrared absorbing and magnetic nanoclusters andtheir applications in targeted cellular imaging and ther-apy to treat cancer and atherosclerosis.
Amit S. Paranjape received his B.E. degree in electricalengineering from Mumbai University, India, in 2003,and his M.E. degree in electrical engineering from Uni-versity of Houston in 2004. He is currently a Ph.D. can-didate in the Biomedical Engineering Laser Laboratoryat the University of Texas at Austin. He is mainly inter-ested in clinical applications of Polarization SensitiveOCT for retinal diagnostics and OCT for cardiovascu-lar applications.
Jingjing Sun received her B.S. degree in electronic in-formation engineering form Wuhan University of Tech-nology, P.R. China, in 2005. From 2008 to 2009, she wasa visiting scholar in the Department of BiomedicalEngineering at the University of Texas at Austin. She iscurrently working towards her M.S. degree in theSchool of Human Ecology at the University of Texas atAustin. She is mainly interested in signal/image proces-sing, biostatistics and 3-D human body scanning andmodeling.
Roman V. Kuranov is an instructor/researcher in theDepartment of Ophthalmology at the University ofTexas Health Science Center at San Antonio (UTHSC-SA). He received his M.S. degree in physics from Loba-chevsky State University, Russia, in 1995. He earnedhis Ph.D. degree in laser physics from the Institute ofApplied Physics RAS, Russia, in 2003. He joined thefaculty of the Department of Ophthalmology at theUTHSCSA in 2009.
Keith P. Johnston holds the M.C. (Bud) and Mary BethBaird Endowed Chair and is Professor of Chemical En-gineering at the Univeresity of Texas at Austin. He re-ceived his Ph.D. degree in chemical engineering at theUniversity of Illinois in 1981. His research interests in-clude colloid and interface science, materials chemistry,and nanocomposite materials. He applies these disci-plines to biomedical and pharmaceutical nanotechnol-ogy, including imaging and drug delivery and to nano-technology for energy, specifically energy storage, oilrecovery and CO2 sequestration.
Thomas E. Milner, Ph.D. is a Marion E. Forsman Cen-tennial Professor in Engineering in the Department ofBiomedical Engineering at the University of Texas atAustin. His research is directed toward the develop-ment of novel optical imaging modalities and laser sur-gical procedures for diagnosis and treatment of diseasein humans. He has authored more than 120 publica-tions in the peer-reviewed literature, is an inventor ofmore than 20 patents and has co-founded two compa-nies. He resides in Austin, TX with his wife and chil-dren.
J. Biophotonics 4, No. 5 (2011) 343
FULLFULLARTICLEARTICLE
# 2011 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheimwww.biophotonics-journal.org

References
[1] D. Parkin, F. Bray, J. Ferlay, and P. Pisani, CA CancerJ. Clin. 55(2), 74–108 (2002).
[2] A. F. Jerant, J. T. Johnson, C. D. Sheridan, and T. J.Caffrey, Am. Fam. Physician. 62(2), 357–368 (2000).
[3] L. Ries, M. Eisner, C. Kosary, B. Hankey, B. Miller,and L. Clegg, SEER Cancer Statistics Review, 1975–2000 (National Cancer Institute, Bethesda, 2003), Ta-bles XV1–9.
[4] American Cancer Society. Cancer facts and figures2010. http://www.cancer.org/acs/groups/content/@epidemiologysurveilance/documents/document/acspc-026238.pdf.
[5] D. M. King and J. H. K. Coll. Radiol. 7, 66–69 (2004).[6] American Cancer Society. http://www.cancer.org/
Cancer/SkinCancerMelanoma/DetailedGuide/melanoma-skin-cancer-key-statistics. Last medical re-view March 5, 2010.
[7] D. L. Ronald, L. A. Applegate, R. S. Padilla, and T. D.Stuart, J. Photochem. Photobiol. 50(1), 1–5 (2008).
[8] A. Breslow, Ann. Surg. 172, 902–908 (1970).[9] M. C. Mihm, G. F. Murphy, and N. Kaufman, Patho-
biology and Recognition of Malignant Melanoma(United States and Canadian Academy of Pathology,New York, 1988), pp. 29–50.
[10] M. J. Sladden, C. Balch, D. A. Barzilai, D. Berg, A. Frei-man, T. Handiside, S. Hollis, M. B. Lens, and J. F.Thompson, Cochrane Database Syst. Rev. 4, 1–34(2009).
[11] C. M. Balch and M. I. Ross, Ann. Surg. Oncol. 6(5),416–417 (1999).
[12] M. H. Kanzler and S. Mraz-Gernhard, JAMA. 285(14),1819–1821 (2001).
[13] D. Huang, E. A. Swanson, C. P. Lin, J. S. Schuman,W. G. Stinson, W. Chang, M. R. Hee, T. Flotte, K. Gre-gory, C. A. Puliafito, and J. G. Fujimoto, Science 254,1178–1181 (1991).
[14] J. Welzel, Skin Res. Technol. 7, 1–9 (2001).[15] T. Gambichler, G. Moussa, M. Sand, D. Sand, P. Alt-
meyer, and K. Hoffmann, J. Dermatol. Sci. 40(2), 85–94 (2005).
[16] N. D. Gladkova, G. A. Petrova, N. K. Nikulin, S. G.Radenska-Lopovok, L. B. Snopova, Y. P. Chumakov,V. A. Nasonova, V. M. Gelikonov, G. V. Gelikonov,R. V. Kuranov, A. M. Sergeev, and F. I. Feldchtein,Skin Res. Technol. 6, 6–16 (2000).
[17] T. Gambichler, P. Regeniter, F. G. Bechara, A. Orli-kov, R. Vasa, G. Moussa, M. Stucker, P. Altmeyer, andK. Hoffmann, J. Am. Acad. Dermatol. 57(4), 629–637(2007).
[18] J. Shia, Y. P. Zheng, X. Chen, and Q. H. Huang, Med.Eng. Phys 29(4), 472–479 (2007).
[19] R. Aaslid, P. Huber, and H. Nornes, JNS 112(2), 37–41 (2010).
[20] E. M. Tuzcu, O. Bayturan, and S. Kapadia, Heart 96,1318–1324 (2010).
[21] L. Machet, V. Belot, M. Naouri, M. Boka, Y. Mourta-da, B. Giraudeau, B. Laure, A. Perrinaud, M. Machet,and L. Vaillant, Ultrasound Med. Biol. 35(9), 1411–1420 (2009).
[22] T. E. Milner, D. J. Smithies, D. M. Goodman, A. Lau,and J. S. Nelson, Appl. Optics 35, 3379–3385 (1996).
[23] M. Milanie, B. Majaron, and J. S. Nelson, Laser Med.Sci. 22, 279–284 (2007).
[24] B. Li, B. Majaron, J. A. Viator, T. E. Milner, Z. Chen,Y. Zhao, H. Ren, and J. S. Nelson, J. Biomed. Opt.9(5), 961–966 (2004).
[25] T. Wang, J. Qiu, A. S. Paranjape, and T. E. Milner,SPIE Proceed 7175, 71750L1–71750L9 (2009).
[26] M. Lualdi, A. Colombo, A. Mari, S. Tomatis, andR. Marchesini, J. Laser Appl. 14(2), 122–127 (2002).
[27] L. L. Ma, M. D. Feldman, J. M. Tam, A. S. Paranjape,K. K. Cheruku, T. A. Larson, J. O. Tam, D. R. Ingram,V. Paramita, J. W. Villard, J. T. Jenkins, T. Wang, G. D.Clarke, R. Asmis, K. Sokolov, B. Chandrasekar, T. E.Milner, and K. P. Johnston, ACS Nano 3(9), 2686–2696 (2009).
[28] R. V. Kuranov, A. B. McElroy, N. Kemp, S. Baranov,J. Taber, M. D. Feldman, and T. E. Milner, Photon.Technol. Lett. (accepted for publication).
[29] T. Vo-Dinh, Biomedical Photonics Handbook (The In-ternational Society for Optical Engineering, Washing-ton, 2003), pp. 39–53.
[30] J. Brewer, A. Burchianti, C. Marinelli, E. Mariotti,L. Moi, K. Rubahn, and H. G. Rubahn, Appl. Surf.Sci. 228, 40–47 (2004).
[31] T. E. Milner, D. M. Goodman, B. S. Tanenbaum, andJ. S. Nelson, J. Opt. Soc. Am. 12(7), 1479–1487 (1995).
[32] J. H. Torres, J. S. Nelson, B. S. Tanenbaum, T. E. Mil-ner, D. M. Goodman, and B. Anvari, IEEE J. Sel.Top. Quan. Electron. 5(4), 1058–1066 (1999).
[33] T. E. Milner, D. M. Goodman, B. S. Tanenbaum, B. An-vari, L. O. Svaasand, and J. S. Nelson, Phys. Med. Biol.41, 31–44 (1996).
[34] B. Choi and A. J. Welch, Laser Surg. Med. 29, 351–359 (2001).
[35] J. J. Bowman, T. B. Senior, and P. L. E. Uslenghi,Electromagnetic and Acoustic Scattering by SimpleShapes (Summa, New York, 1987), pp. 25–31.
[36] M. E. Brezinski and J. G. Fujimoto, IEEE J. Sel. Top.Quan. Electron. 5(4), 1185–1192 (1999).
[37] M. A. Choma, K. Hsu, and J. A. Izatt, J. Biomed. Opt.10(4), 0440091–0440096 (2005).
[38] S. E. Bendeck and H. T. Jacobe, Dermatol. Ther. 20(2),86–92 (2007).
[39] F. S. Foster, M. Y. Zhang, Y. Q. Zhou, G. Liu, J. Mehi,E. Cherin, K. A. Harasiewicz, B. G. Starkoski, L. Zan,D. A. Knapik, and S. L. Adamson, Ultrasound Med.Biol. 28(9), 1165–1172 (2002).
[40] F. S. Foster, M. Y. Zhang, A. S. Duckett, V. Cucevic,and C. J. Pavlin, Invest. Ophthalmol. Vis. Sci. 44,2361–2366 (2003).
[41] C. R. Denegar, Therapeutic Modalities for Athletic In-juries (Human Kinetics, Champaign, 2000), pp. 162–163.
[42] S. Mallidi, S. R. Aglyamov, A. B. Karpiouk, S. Park, andS. Y. Emelianov, Proc. SPIE 6147, 61470Y (2006).
[43] A. Kharine, S. Manohar, R. Seeton, R. G. M. Kolk-man, R. A. Bolt, W. Steenbergen, and F. F. Mul, Phys.Med. Biol. 48, 357–370 (2003).
[44] J. K. Tsou, J. Liu, A. I. Barakat, and M. F. Insana,Ultrasound Med. Biol. 34(6), 963–972 (2008).
Tianyi Wang et al.: Comparison of PPTR, OCT and US for melanoma thickness measurement in tissue phantoms344
Journal of
BIOPHOTONICS
# 2011 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim www.biophotonics-journal.org