Embed Size (px)
Citation preview

FOOT & ANKLE INTERNATIONAL
Copyright © 2002 by the American Orthopaedic Foot & Ankle Society, Inc.
Comparison of Foot Pronation and Lower Extremity Rotation in PersonsWith and Without Patellofemoral Pain
Christopher M. Powers, PhD., P.T.'; Pan-Yo Chen, M.S., P.P; Stephen F. Reischl, D.P.T., o.c.s.:Jaquelin Perry, MD., D.Sc. (Hon)'
Los Angeles and Long Beach, CA
ABSTRACT
Abnormal foot pronation and subsequent rotation of thelower extremity has been hypothesized as being contributory to patellofemoral pain (PFP). The purpose of thisstudy was to test the hypothesis that subjects with PFPwould exhibit larger degrees of foot pronation, tibia internal rotation, and femoral internal rotation compared toindividuals without PFP.Twenty-four female subjects witha diagnosis of PFP and 17 female subjects without PFPparticipated. Three-dimensional kinematics of the foot,tibia, and femur segments were recorded during selfselected free-walking trials using a six-camera motionanalysis system (VICON). No group differences werefound with respect to the magnitude and timing of peakfoot pronation and tibia rotation. However, the PFP groupdemonstrated significantly less femur internal rotationcompared the comparison group. These results do notsupport the hypothesis that individuals with PFP demonstrate excessive foot pronation or tibial internal rotationcompared to nonpainful individuals. The finding ofdecreased internal rotation in the PFP group suggeststhat this motion may be a compensatory strategy toreduce the quadriceps angle.
1. Assistant Professor and Director, Musculoskeletal BiomechanicsResearch Laboratory, Department of Biokinesiology and Physical Therapy,University of Southern California, Los Angeles, CA
2. Masters Student, Department of Biokinesiology and Physical Therapy,University of Southern California, Los Angeles, CA
3. Adjunct Assistant Professor of Clinical Physical Therapy, Department ofBiokinesiology and Physical Therapy, University of Southern California,Los Angeles, CA; Owner, Reischl Physical Therapy, Long Beach, CA
4. Chief Emeritus, Pathokinesiology Service, Rancho Los Amigos NationalRehabilitation Center, Downey CA; Professor Emeritus, University ofSouthern California, Los Angeles, CA
Corresponding Author:Christopher M. Powers, Ph.D., P.T.Department of Biokinesiology and Physical TherapyUniversity of Southern California1540 Alcazar Street, CHP 155Los Angeles, CA 90089-9006Phone: (323) 442-1928Fax: (323) 442-1515E-mail: [email protected]
Key Words: Patellofemoral Pain; Pronation; LowerExtremity Kinematics
INTRODUCTION
Although patellofemoral pain (PFP) is one of the mostcommon lower extremity conditions encountered, theetiology of this disorder remains relatively unclear.Patellar subluxation as a result of an increased Q angle,diminished depth of the trochlear groove, quadricepsmuscle weakness, or vasti muscle imbalance has beenproposed as a likely cause.4•5,8,14 ,20 25 ,28 In addition, abnormal lower extremity kinematics has been commonlycited as a predisposing factor to PFP.227 One area offocus from a clinical standpoint has been the influenceof foot pronation on lower extremity rotation andpatellofemoral joint mechanics.
As part of normal walking, subtalar joint pronationbegins immediately after initial contact and reaches apeak value of approximately 4 to 6° by 14% of gait cycle(i.e. early rnldstance)." During pronation, the calcaneous everts and the head of the talus slides mediallyand inferiorly resulting in medial rotation of the talus. Asa result of the tight fit of the talus within ankle joint mortise, the tibia internally rotates and reaches a peakvalue of 6 to 10° by 10% of the gait cycle (loadingresponse).":' In late midstance, the subtalar jointreverses its function and begins to supinate resulting inexternal rotation of the tibia.
As a result of screw-home mechanism of the knee,the tibia must be internally rotated relative to the femurto permit flexion.":" Given as such, internal rotation ofthe tibia during loading response functionally serves to"unlock" the knee allowing for shock absorption duringweight acceptance. Conversely, the tibia must be externally rotated relative to the femur to allow for kneeextension during midstance.6,7.12,23,24
Excessive or prolonged subtalar joint pronation duringstance would theoretically delay external rotation of thelower leg, thus limiting the screw home mechanics ofthe knee. In order to compensate for the competing
634
at Midlands State University on December 21, 2014fai.sagepub.comDownloaded from

Foot & Ankle InternationalNol. 23, No. 7/July 2002 PATELLOFEMORAL PAIN: EFFECT ON PRONATION 635
InstrumentationMotion analysis was performed with a computer aided
video motion analysis system (VICON; Oxford MetricsLtd., Oxford, England) that used six cameras. Eachcamera contained infrared light-emitting diodes thatflashed at a rate of 50 Hz. Prior to data collection, eachcamera was calibrated and the average spatial resolution was found to be less than 3 mm over a measuredvolume of 4 m x 1.2 m x 1.8 m. The overall system errorwith respect to angular measurements (using a calibrated frame) was determined to be 0.18°. In addition, thereliability of obtaining transverse plane motion with thissystem (using the coefficient of multiple correlation withten subjects) was found to be r=0.54 for the hip andr=0.71 for the knee, whereas the reliability of obtainingfrontal plane motion of the foot was r=0.84.21
(comparison group). The groups were similar withrespect to average age, height, and weight (Table 1). Theindividuals with PFP were recruited from orthopaedicclinics in Los Angeles area and were screened to rule outligamentous instability, internal derangement, or patellartendinitis.
Participants were assigned to the PFP group if theyhad:
1.pain (vague or localized) originating from thepatellofemoral joint articulation and;
2. readily reproducible pain with at least two activitiescommonly associated with PFP (e.g., squatting,stair climbing, kneeling, prolonged sitting, isometricquadriceps femoris muscle contraction)."
Persons with PFP were excluded from this study ifthey reported having:
1.any previous knee surgery,2.a history of traumatic patellar dislocation, or;3.any neurological involvement that would influence
gait.The comparison group was recruited from the student
population at the University of Southern California andRancho Los Amigos Medical Center (Downey, CA).These subjects were selected based on the same criteriaused for the PFP group except that these individuals had:
1.no history or diagnosis of knee pathology or trauma,2.no knee pain with any of the activities described, and;3.no limitations that would influence gait.
Table 1: Subject Characteristicsrequirements of the tibia and to allow knee extensionduring midstance, Tiberio" describes a scenario inwhich individuals with PFP may excessively internallyrotate the femur such that the tibia is in relative externalrotation. While this compensatory strategy would serveto ensure normal knee mechanics, there may be a deleterious effect on the patellofemoral joint. For example,increased femoral internal rotation would move the center of the patella to a more medial position in relation tothe anterior superior iliac spine, thus increasing thequadriceps angle (Ovanqle)." A larger Q angle wouldincrease the lateral force vector acting on the patellaand may contribute to lateralization of the patella.
Although the theory of compensatory internal rotationof the femur proposed by Tiberio" appears plausible, nodata exist to support or refute this theoretical construct.Recent work by Reischl and colleaques" suggest thattibia and femur rotation are independently of each other,and that a specific lower extremity kinematic patterncannot be inferred based on the magnitude and timingof foot pronation during walking. These results, however, were based on data obtained from healthy subjects.
To date, only two studies have studied foot pronationand/or transverse plane knee kinematics in personswith PFP. Eng and Pierrynowski" evaluated the influence of soft foot orthotics on three-dimensional lowerlimb kinematics during walking and running. However,motion data were reported as ranges (as opposed tomagnitudes). Therefore, the total amount of motion in agiven direction (i.e. pronation vs. supination) could notbe discerned. Furthermore, no comparisons were madeto individuals without PFP. Messier and colleaques"compared maximum pronation during running andfound no differences between persons with and withoutPFP. This study did not evaluate the influence of pronation on lower extremity rotation.
Given the limited work in this area, the purpose of thisstudy was to compare the magnitude and timing of footpronation, tibia rotation and femoral rotation in subjectswith PFP and pain-free controls. It was hypothesizedthat subjects with PFP would exhibit larger degrees offoot pronation, tibia internal rotation, and femoral internal rotation compared to individuals without PFP.Results obtained from this study will provide objectiveinformation in understanding how lower extremity kinematics may influence patellofemoral joint mechanics.
MATERIALS AND METHODS
SubjectsForty-two females ranging from 15 to 47 years of age
participated in this study. Twenty-four subjects were diagnosed as having PFP (PFP group), whereas the remaining 18 subjects were free of any knee pain or pathology
Age (yrs)Height (ern)Weight (kg)
PFP group25.4±7.3
164.9±10.863.6±10.1
Comparisongroup
27.6±4.8165.8±7.659.6±7.5
p value0.270.780.16
at Midlands State University on December 21, 2014fai.sagepub.comDownloaded from

636 POWERS, PON-YO CHEN, REISCHLAND PERRY Foot & Ankle InternationalNol. 23, No. 7/July 2002
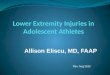
Fig. 1: Frontal (left) and lateral (right) views of the marker arrangement used to quantify footpronation, tibial rotation and femoral rotation.
Stride characteristics andfoot-floor contact patterns wererecorded with compressionclosing foot switches (StrideAnalyzer System; B&LEngineering,Santa Fe Springs, CA). Thesefoot switches contained sensorsat the heel, first metatarsalhead, fifth metatarsal head, andthe great toe, which respondedto compressive forces greaterthan 3 psi. Variables obtainedfrom this system included velocity, cadence and stride length.
All gait analysis was performed along a 10-m walkwaywith the middle 6 m designatedfor data collection. The data collection area was delineated byphotoelectric light switches,which were used to trigger thedata acquisition computer.
ProceduresAll procedures were explained
to each subject, and the informed consent was obtained(as approved by the InstitutionalReview Board of Rancho LosAmigos Medical Center). Priorto testing, foot switches weresized and taped to the subjects'bare feet, and the reflectivemotion markers were placed onthe posterior calcaneus, dorsal foot (middle cuneiform),and the first and fifth metatarsal heads. For the tibia,femur and pelvis, markers were placed on the lateraland medial malleolus, anterior tibia, medial and lateralepicondyles of the femur, anterior thigh, greatertrochanter, the sacrum, and the contralateral and ipsilateral anterior superior iliac spine (Fig. 1). These markers were used to define embedded coordinate systemsof the thigh, shank, and foot segments, as described byApkarian et al.1
Subjects were instructed to walk at a self-selected freewalking velocity along the 10-m walkway. Two trials ofdata (an average of four to five strides per subject) wereobtained with motion and stride characteristic data beingcollected simultaneously.
Foot ModelAs described in a previous publlcation," the foot was
modeled as an entire segment because pronation isconsidered a triplanar motion that includes movement
at the joints of the rearfoot, midfoot, and forefoot. Usingthe marker arrangement described above, pronation atthe subtalar and midtarsal joints during stance resultedin inferomedial movement of the dorsal foot marker,eversion of the calcaneal marker, and frontal planemovement of the metatarsal head markers. Frontalplane motion of the foot segment (foot sole plane)about the long axis of the foot inversion/eversion wasconsidered representative of the combined movementsof the rearfoot, midfoot, and toretoot." By modeling thefoot as a segment, it was our intent to obtain an overall indication of total foot pronation, as is the customarypractice when assessing a patient clinically.
Data AnalysisTo facilitate interpretation of the kinematic data, trans
verse plane rotation of the femur and tibia, and frontalplane motion of the foot segment was referenced to thelaboratory coordinate system. The magnitude of peakfoot pronation was reported as the difference between
at Midlands State University on December 21, 2014fai.sagepub.comDownloaded from

Foot & Ankle InternationalNol. 23, No. 7/July 2002 PATELLOFEMORAL PAIN: EFFECT ON PRONATION 637
Table 2: Stride Characteristics
Table 3: Comparison of Foot Pronation between Groups
SO= standard deviationpositive value = internal rotation; negative value =external rotation
Stride CharacteristicsDuring free walking, the average veloci
ty of the PFP group was significantly slower than that of the comparison group (71.6vs. 82.9 m/min; p=0.0002). The reductionof walking velocity in the PFP group was afunction of a significantly decreased stridelength (1.3 vs. 1.4 m; p=0.008) and diminished cadence (113.9 vs. 122.1 steps/min;p=0.0009) (Table 2).
the foot position at initial contact and maximum eversion during stance. Timing ofpeak pronation was expressed as a percentage of the gait cycle, which was determined through the foot switch data. Themagnitude of the peak transverse rotationof the femur and tibia was reported as thedifference between the initial contact position and the peak rotation value duringstance. Similarly, the timing of peak rotation of femur and tibia was expressed as apercentage of the gait cycle. All data frommultiple strides were averaged for statistical analysis.
RESULTS
Statistical AnalysisIndependent t-tests (two-tailed) were
used to assess group differences for stridecharacteristics (velocity, stride length,cadence). Similarly, Independent t-tests(one-tailed) were used to assess groupdifferences for the following variables:peak foot pronation, timing of peak footpronation, peak tibial rotation, timing ofpeak tibial rotation, peak femoral rotation,and timing of peak femoral rotation. Allsignificant levels were set at p<0.05. Allanalysis was performed using MicrosoftExcel 97 (Version 8.0).
Kinematic DataThere was no statistically significant dif
ference in the magnitude of peak footpronation between the two groups (PFPgroup: 8.9°, Comparison group: 8.3°;p=0.29). In addition, the timing of peak footpronation was similar between groups(PFP group: 19.8% gait cycle, Comparisongroup: 19.8% gait cycle; p=0.49) (Table 3).Similarly, there was no statistically significant difference in the magnitude of peak
0.49
0.26
0.008
0.0009
0.0002
p value0.25
p value0.29
1.40.1
1.2-1.7
19.86.9
10.5-32.0
82.910.6
65.8-111.4
12.03.5
7.0 to 19.0
122.17.8
109.0-137.5
Comparison group4.11.9
1.6-8.2
Comparison group8.33.7
0.8-14.0
1.30.1
1.0-1.5
19.89.3
10.5-37.7
71.68.5
57.9-85.0
11.15.7
5.0 to 33.0
PFP group4.52.2
1.3-10.6
PFP group Comparison group p value
PFP group8.92.9
4.3-14.7
113.98.0
102.4 -138.2
Velocity (meters/min)MeanSORange
Stride Length (meters)MeanSORange
so = standard deviation
SO= standard deviation
Peak Tibia RotationTiming (% gait cycle)
MeanSORange
Peak PronationTiming (% gait cycle)
MeanSORange
Peak PronationMagnitude (degrees)
MeanSORange
Cadence (steps/minute)MeanSORange
rable 4: Comparison of Tibia Rotation between Groups
Peak Tibia RotationMagnitude (degrees)
MeanSORange
at Midlands State University on December 21, 2014fai.sagepub.comDownloaded from

638 POWERS, PON- YO CHEN, REISCHL AND PERRY Foot & Ankle InternationalNol. 23, No. 7/July 2002
Table 5: Comparison of Femur Rotation between Groups
SD= standard deviationpositive value = internal rotation; negative value =external rotation
tibia internal rotation (PFP group: 4S, Comparisongroup: 4.10
; p=0.25), or the timing of peak tibia internalrotation (PFP group: 11.1 % gait cycle, Comparisongroup: 12.0% gait cycle; p=0.26) (Table 4).
The only significant difference with respect to lowerextremity kinematics was found at the femur. On theaverage, the PFP group demonstrated 2.1 0 of externalrotation, which was significantly different from theaverage value of 1.60 of internal rotation observed inthe comparison group. Peak femur rotation was foundto occur significantly later in the PFP group (17.0%gait cycle) compared to 13.4% of the gait cycle in thecomparison group (Table 5).
DiscussionAbnormal foot pronation and subsequent lower
extremity rotation has been implicated as being a contributory factor with respect to numerous lower extremity conditions, including PFP. However, the results of thisstudy found that subjects with PFP did not demonstrateexcessive or prolonged pronation or excessive internaltibial torsion compared to individuals without PFP. Thissuggests that abnormal pronation is not a universalfinding in this population and care must be made inattributing the cause of PFP symptoms to such motion.Our findings are in agreement with the data of Messieret al." who found no differences in pronation betweenrunners with and without PFP, and concluded thatpronation and the velocity of pronation were not significant etiological factors with respect to the developmentof this disorder.
The mean values for peak pronation and the timing ofpeak pronation for both groups were found to be normally distributed and are consistent with previouslyreported datay2 Further analysis revealed that of the 24PFP subjects evaluated in the current study, approxi-
0.05
p value0.03
mately 14% had peak pronation valuesthat were greater than one standard deviation from the group mean, while 23% hadtiming values that were greater than onestandard deviation from the group mean.These percentages were similar to that ofthe control group (6% and 18% for magnitude and timing respectively).
As with foot pronation, there were no differences in tibial rotation between the twogroups. All subjects evaluated demonstrated internal rotation of the tibia duringinitial stance with magnitude and timingvalues being similar to that reported previously.1011,22 These data are consistent withthe biomechanical premise that footpronation and tibial internal rotation occursimultaneously. Several authors have
characterized the relationship between foot eversionand tibial internal rotation using a "coupling ratio" andhave reported ratios ranging from 1.5:1 to 1.8:1 duringrunninq.":" Further analysis of the data obtained in thecurrent investigation revealed average eversion-tibialinternal rotation ratios of 2.1 and 2.5 for the PFP andcomparison groups, respectively. Although the discrepancy in our ratios and those reported previously arelikely related to the inherent differences between walking and running, the fact that the average ratios from thePFP and comparison groups were similar provides further evidence refuting the premise of a direct linkbetween foot mechanics and PFP.
Although both groups exhibited similar kinematics at thefoot and tibia, small but significant differences wereobserved with respect to the magnitude and timing ofpeak femoral rotation.The comparison group demonstrated an average of 1.60 of internal rotation that occurred by13% of the gait cycle, while the PFP group demonstratedan average of 2.1 0 of external rotation that occurred by17% of the gait cycle. This finding does not support thepremise proposed by Tlberio," who stated that individualswith PFP would likely demonstrate compensatory internalrotation of the femur to ensure knee extension during midstance. To the contrary, it is possible that the reducedinternal rotation observed in the PFP subjects may havebeen a compensatory strategy. Such compensation woulddecrease the Q-angle and lateral force vector on thepatella as reduced femoral internal rotation would bringthe patella more in line with the anterior superior iliacspine. Tiberio's premise assumes that abnormal kinematic patterns are a cause of PFP. However, one cannot ruleout the possibility that abnormal kinematic patterns are anattempt by individuals with PFP to minimize pain.
Despite the fact that the PFP group demonstrated anaverage of 2.10 of femoral external rotation, care must be
13.44.0
8.5-24.0
Comparison group1.65.6
-10.5-7.2
7.110.1
6.0-45.7
PFP group2.16.7
-18.8-9.0
Peak Femur RotationTiming (%Gait cycle)
MeanSDRange
Peak Femur RotationMagnitude (degrees)
Mean-SDRange
at Midlands State University on December 21, 2014fai.sagepub.comDownloaded from

Foot & Ankle InternationalNol. 23, No. 7/July 2002
made in generalizing this pattern of motion to the entirePFP population as only 13 of 24 individuals with PFP(54%) exhibited external rotation posture as oppose tointernal rotation. In addition, the PFP group demonstrated a wide range of femoral rotation, ranging from 18.8° ofexternal rotation to 9.0° of internal rotation. On the otherhand, the comparison group showed a much more consistent pattern of femoral rotation with 13 of 18 subjects(72%) demonstrating internal rotation.
In the present study, the motions of foot and shankwere closely linked as all subjects demonstrated footpronation and tibial internal rotation during early stance.However, the motion of the femur did not follow a consistent pattern indicating that the rotary forces acting on thetibia were not consistently transferred upward. Thisimplies that tibia rotation created through foot pronationmay be at least partially absorbed at the knee. The lackof synchronous rotation of the tibia and femur is consistent with the data of Reischl and colleaques" who reported that the timing and magnitude of tibial rotation did notpredict the magnitude and timing of femoral rotation.
One of the limitations of the foot model used was thatrearfoot motion could not be differentiated from forefootmotion. Previous work has suggested that total footpronation consists of two events:
1.rearfoot eversion, which occurs primarily duringweight acceptance loading (i.e. loading response)and,
2.forefoot loading, which occurs during early midstance."
For both groups, peak tibia rotation occurred at a timethat corresponded to the end of loading response (10 to12% GC) indicating that tibia rotation was likely dictatedprimarily by rearfoot motion (i.e. subtalar joint). The factthat peak femur rotation occurred later in the gait cycle,and was much more variable, (particularly in the PFPgroup) suggests that factors other then foot pronationand tibial rotation could be influencing the femur. Forexample, rotation of the pelvis can have an effect onfemoral rotation and could be used as means by whichpersons with PFP limit internal rotation. Further researchis necessary to fully elucidate the factors influencingfemoral rotation in persons with PFP.
On the average, the PFP subjects were found to havea 14% slower self-selected free walking velocity compared to the comparison group. The slower gait speedwas a function of both a reduced stride length anddiminished cadence. This result is consistent with previous studies that have reported that individuals with PFPadopt a slower gait speed in an attempt to reduce theground reaction forces and the loading of the lower limbduring weight acceptance." Although the magnitude ofpronation and the rotary forces acting on the segmentsof the lower extremity would likely increase with walking
PATELLOFEMORAL PAIN: EFFECT ON PRONATION 639
velocity," it is not known if such a modest decrease ingait speed would have had a significant influence onpronation and lower limb rotation in the PFP group. Asthe purpose of this study was to evaluate the PFP subjects during their "customary" gait pattern, no attemptwas made to control for walking speed between the twogroups. Future studies may want to control for walkingspeed and evaluate the influence of gait velocity onlower limb kinematics in the PFP population.
Although the mean pronation data of both groupswere similar, it is possible that certain individuals maydemonstrate abnormal foot pronation (and subsequentlower extremity rotation) that could be contributory toPFP. However, the results of this study indicate thatcare must be taken in overgeneralizing the influence offoot pronation as being contributory to this disorder. Apatient-by-patient lower extremity evaluation wouldappear to be necessary to ascertain the possible contribution of the various segments with respect to PFP.
CONCLUSIONS
The results of this study do not support the hypothesis that persons with PFP demonstrate excessive footpronation or tibial internal rotation compared to nonpainful individuals. Care must be made in overgeneralizinq the symptoms of PFP to a specific lower extremitykinematic pattern. The finding of decreased femoralinternal rotation in the PFP group suggests, however,that this motion may be a compensatory strategy toreduce the Q-angle.
REFERENCES
1. Apkarian, J; Naumann, S; Cairns, B: A three-dimensional kinematic and dynamic model of the lower limb. J Biomechanics22:143-153,1989
2. Eng, JJ; Pierrynowski, MR: Evaluation of soft foot orthotics in thetreatment of patellofemoral pain syndrome. Phys Ther 73:62-70,1993
3. Eng, JJ; Pierrynowski, MR: The effect of soft foot orthotics onthree-dimensional lower limb kinematics during walking andrunning. Phys Ther 74:836-844, 1994.
4. Fox, JM; Del Pizzo, W: The patellofemoral joint, New York:McGraw-Hili, Inc., 1993
5. Fulkerson, JP; Hungerford, DS: Disorders of the patellofemoraljoint, Baltimore: Williams & Wilkins, 1990
6. Greenfield, BH: Rehabilitation of the knee: a problem-solvingapproach, Philadelphia: FA Davis, 1993
7. Griffin, LV: Rehabilitation of the injured knee, St. Louis: Mosby,1995
8. Insall, J: "Chondromalacia patella": patellar malalignment syndrome. Orthop Clin North Am 10:117-127,1979
9. Knutsen, KM; Price, A: Lower extremity static and dynamic relationships with rearfoot motions in gait. J Am Podiatr Assoc.84:171-190, 1994.
10.LaFourtune, MA; Cavanagh, PR; Sommer, HJ; Kalenak, A:Foot inversion-eversion and knee kinematics during walking. JOrthop Res 12:412-420, 1994
at Midlands State University on December 21, 2014fai.sagepub.comDownloaded from

640 POWERS, PON- YO CHEN, REISCHL AND PERRY Foot & Ankle InternationalNol. 23, No. 7/July 2002
11.Levens, AS; Inman, VT; Blosser, JA: Transverse rotation of thesegments of the lower extremity in locomotion. J Bone Joint Surg30A:859-872, 1949
12.Mangine, RE: Physical therapy of the knee, New York: ChurchillLivingstone, 1995
13.McClay, I; Bray, J: The subtalar angle: a proposed measure ofrearfoot structure. Foot Ankle Int 17:499-502, 1996
14.Messier, SP; Davis, SE; Curl, WW; Lowery, RB; Pack, RJ:Etiologic factors associated with patellofemoral pain in runners.Med Sci Sports Exerc 23:1008-1015,1991
15.Nawoczenski, DA; Saltzman, CL; Cook, TM: The effect of footstructure on the three-dimensional kinematic coupling behavior ofthe leg and rear foot. Phys Ther 78:404-416, 1998
16.Perry, P: Gait analysis: normal and pathological function,Thorofare N.J: SLACK Inc., 1992.
17.Powers, CM; Maffucci, R; Hampton, S: Rearfoot posture in subjects with patellofemoral pain. J Orthop Sports Phys Ther 22:15560, 1995
18.Powers, CM; Landel, R; Perry, J: Timing and intensity of vastusmuscle activity during functional activities in subjeots with andwithout patellofemoral pain. Phys Ther 76:946-955, 1996
19.Powers, CM; Heino, J.G; Rao, S; Perry, J: The influence ofpatellofemoral pain on lower limb loading during gait. ClinicalBiomechanics 14:722-8, 1999
20. Powers, CM: Patellar kinematics, Part II: The influence of thedepth of the trochlear groove in subjects with and withoutpatellofemoral pain. Phys Ther, 80:965-973, 2000.
21. Rao, S; Clayton, RM; Driessen, KM; Torburn, L; Winstein, CJ;Perry, J: Vicon measurement error and reliability of joint kinematics in free and fast walking. Phys Ther 72:S66, 1992
22. Reischl, SF; Powers, CM; Rao, S; Perry, J: Relationshipbetween foot pronation and rotation of the tibia and femur duringwalking. Foot Ankle Int 20:513-520, 1999
23. Scott, WN: The Knee, St. Louis: Mosby, 199424. Smith, LK; Weiss, EL; Lehmkuhl, LD: Brunnstrom's clinical kine
siology, Philadelphia: F.A. Davis, 199625. Souza, DR; Gross, MT: Comparison of vastus medialis obliquus:
vastus lateralis muscle integrated electromyographic ratiosbetween healthy subjects and patients with patellofemoral pain.Phys Ther 71:310-316, 1991
26. Soderberg, GL: Kinesiology: application to pathological motion,Baltimore: Williams & Wilkins, 1997
27. Tiberio, D: The effect of exercise subtalar joint pronation onpatellofemoral mechanics: a theoretical model. J Orthop SportsPhys Ther 9:160-165,1987
28. Winslow, J; Yoder, E: Patellofemoral pain in female balletdancers: correlation with iliotibial band tightness and tibial externalrotation. J Orthop Sports Phys Ther 22: 18-21, 1995
at Midlands State University on December 21, 2014fai.sagepub.comDownloaded from