Embed Size (px)
Citation preview
Intensive Care Medicine© Springer-Verlag 2003DOI 10.1007/s00134-003-1660-z
Original
Comparison of effectiveness of two urinarydrainage systems in intensive care unit: aprospective, randomized clinical trialMarc Leone (✉) · Franck Garnier · François Antonini · Marie-Christine Bimar · JacquesAlbanèse · Claude Martin
M. Leone · F. Garnier · F. Antonini · M.-C. Bimar · J. Albanèse · C. MartinIntensive Care Unit and Trauma Center,Nord Hospital, Marseilles University Hospital System,AP-HM, Marseilles School of Medicine, 13915 Marseille cedex 20, France
✉ M. LeonePhone: +33-4-91968650Fax: +33-4-919682818E-mail: [email protected]
Received: 20 November 2002 / Accepted: 10 December 2002 / Published online: 8 February 2003
Abstract Objective In a previous nonrandomized study we observed no difference in the rate of
acquisition of bacteriuria between a complex closed drainage system (CCDS) and a two-chamber
drainage system (TCDS) in ICU patients. To confirm this result we performed a statistically
powerful study assessing the effectiveness of the CCDS and the TCDS in ICU patients.
Design and setting Randomized, prospective, and controlled study in the medicosurgical
intensive care unit (16 beds) in a teaching hospital.
Patients and interventions We assigned 311 patients requiring indwelling urinary catheter for
longer than 48 h to TCDS or CCDS to compare the rate of acquisition of bacteriuria.
Measurements and results Patients did not receive prophylactic antibiotics during placement
management or catheter withdrawal. Urine samples were obtained weekly for the duration of
catheterization and within 24 h after catheter removal, and each time symptoms of urinary infection
were suspected. There was no statistical difference in the rate of bacteriuria between the two
1
groups: 8% with TCDS and 8.5% with CCDS. Rates of urinary tract infection were 12.1 episodes
with TCDS and 12.8 episodes with CCDS per 1000 days of catheter.
Conclusions This randomized study on the effectiveness of TCDS and CCDS in ICU patients
confirms the findings of our previous study. No differences were noted between the two systems.
The higher cost of CCDS is not justified for ICU patients.
Keywords Catheter associated urinary tract infection · Closed system drainage · Bacteriuria
An erratum to this article can be found at http://dx.doi.org/10.1007/s00134-003-2079-2
IntroductionCatheter-related urinary tract infection) is the most common nosocomial infection [1, 2]. It is
associated with increased morbidity, mortality, and cost [3]. The maintenance of a closed sterile
drainage system is reported to be the most successful method of reducing the incidence of urinary
tract infections [4, 5, 6, 7, 8, 9, 10, 11, 12, 13]. In intensive care unit (ICU) the optimization of
nursing cares procedures and respect for antibiotic prescription rules are strongly recommended
for the control of nosocomial infections. Most patients admitted to an ICU require an indwelling
urinary catheter to monitor diuresis. Using a closed drainage system is strongly recommended to
prevent catheter-associated urinary tract infections [8, 14]. However, we performed a nonrandomized
comparative trial between open and closed drainage system in ICU patients and did not confirm
the evidence of this recommendation [15].
The present study was designed to compare the rate of nosocomial urinary tract infections in
ICU patients catheterized with a two-chamber drainage system (TCDS) or a complex closed
drainage system (CCDS).
Methods
Patients
Between September 1997 and September 1999 we enrolled all 311 patients admitted to our ICU
requiring the placement of an indwelling urinary catheter (Fig. 1). The study was carried out at
Nord Hospital, a 550-bed tertiary care center affiliated with the University of the Mediterranean
Sea. The 16-bed ICU admits medical, surgical, and trauma patients. The Simplified Acute
2
Physiology Score II (SAPS II) that includes 17 variables (12 physiology variables, age, type of
admission, and three underlying disease variables) was used to determine prognosis [16]. Written
protocols for the management of urinary catheters were followed, these protocols having been
implemented in the ICU 5 years previously. The randomized, prospective, controlled trial was
approved by the ethics committee of the University Hospital of Marseilles, and informed consent
was obtained from patients or next of kin.
Fig. 1. The two-chamber drainage urinary drainage system. A No filter and no antireflux valve; B port with
no filter, opened when urine samples are needed; C no filter and no antireflux valve.
Study protocol
Patients requiring urinary catheter were randomly assigned to receive either TCDS (n=149) or
CCDS (n=162) using a table of random numbers to allocate patients. To be eligible for evaluation
they had to have an initial culture free of bacterial growth and an indwelling urethral catheter for
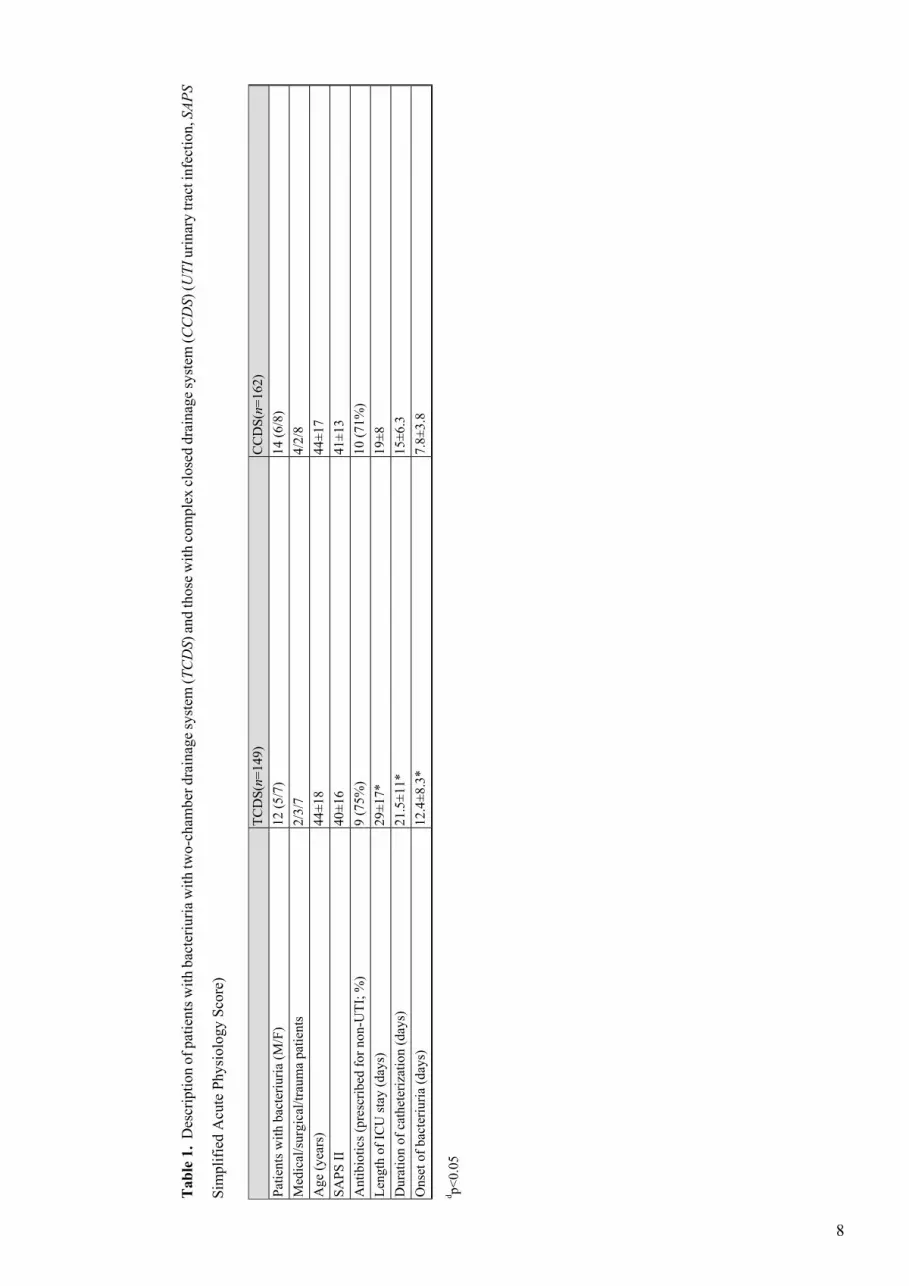
more than 48 h. The study groups were similar at admission to ICU and at study inclusion (Table 1).
[Table 1. will appear here. See end of document.]
The TCDS (Appareil pour la diurèse ouverte, 964.00, Vygon, Ecouen, France; Fig. 2) contains
a Foley catheter connected to an output measure recipient and a urine collection bag. The CCDS
(Curity Infection Control System, 8120, Kendall, Boston, Mass., USA) comprises a preconnected
coated latex catheter, a tamper discouraging seal at the catheter-drainage tubing junction, a drip
chamber, an antireflux valve, a drainage bag vent, and a povidone-iodine releasing cartridge at
the drain port of the urine collection bag.
Fig. 2. Flow chart describing the study inclusions
A team of trained nurses practiced catheterization and drainage system cares according to the
French National General Guidelines and Intensive Care Recommendations [14]. The aim of these
recommendations is to obtain a nontraumatic, sterile catheterization. A careful attention is given
to the drainage system, limiting the duration of catheterization, disposing of the urine accumulated
in the collection bag, replacing a malfunctioning collecting system and keeping the system closed
3
when a closed system is used. The insertion of indwelling urethral catheter was performed after
surgical hand washing, wearing sterile gloves, a face mask, and a cap and using sterile drapes.
Routine meatal and perineal hygiene with povidone-iodine, water, and nonsterile gloves was
performed once daily or more if the perineal zone was soiled. The same urinary drainage system
was maintained for a patient during the whole study period.
A urine sample was obtained aseptically within 24 h of catheter insertion, then weekly for the
duration of catheterization, and within 24 h after removal of the catheter and each time symptoms
of urinary infection were suspected. A catheter-associated bacteriuria was defined as at least
105 cfu/ml with no more than two different species of organisms, according to the criteria of the
Centers for Disease Control [17].
Statistical analysis
Data were analyzed on intention-to-treat basis and are presented as mean ±standard deviation. The
Mantel-Haenszel χ2 statistic was calculated for stratified analysis of occurrence of infection between
the two groups. Continuous variables were compared using Student’s t test for normally distributed
variables and Wilcoxon’s rank sum test for nonnormally distributed variables. A p value less than
0.05 was considered statistically significant. Kaplan-Meier cumulative frequency of infection
analysis was used to assess differences between the TCDS group and the CCDS group. To provide
80% power to detect a 10% difference between the CCDS group and the TCDS group (α=5%),
we needed to enroll at least 300 patients.
ResultsThe rate of catheter-associated bacteriuria was 8.0% in the TCDS group and 8.6% in the CCDS
group (n.s.; Table 1). Duration of catheterization and length of stay in ICU were significantly
longer in the TCDS group than in the CCDS group. Bacteriuria occurred on day 12.4±8.3 in the
TCDS group and 7.8±3.8 in the CCDS group of catheterization (p>0.05). Escherichia coli was
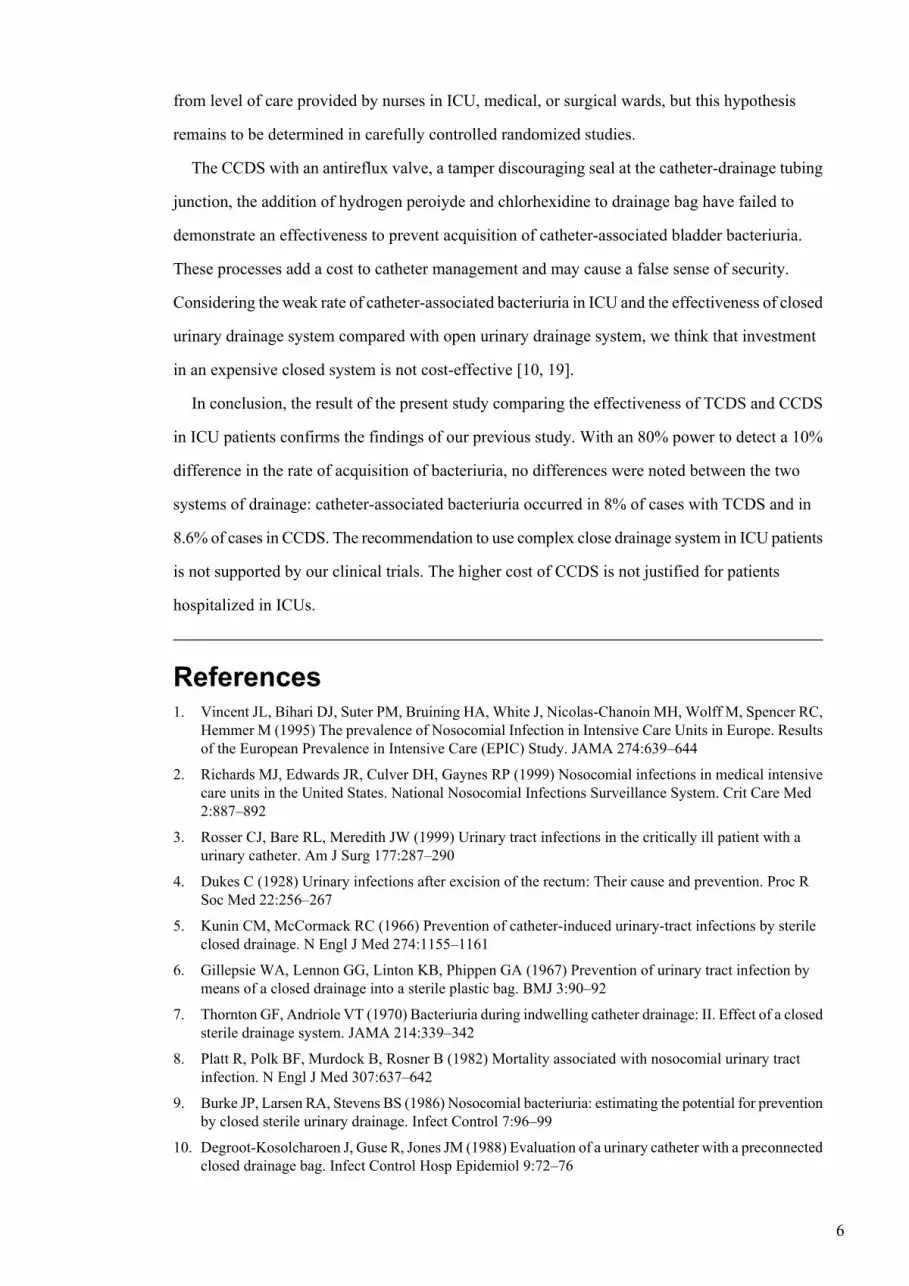
the most frequently isolated organism. As shown in Fig. 3, the analysis of the Kaplan-Meier
estimates of the risk of bacteriuria according to the duration of catheter placement demonstrated
the lack of difference between the two systems of urinary drainage.
4

Fig. 3. Probability of remaining uninfected during until removal of catheter with a two-chamber drainage
system (TCDS) and a complex closed drainage system (CCDS). Kaplan-Meier curves demonstrating the
lack of difference between the two system of urinary drainage. The data on uninfected patients were collected
on the day of catheter removal. Comparisons between the time distribution of the two groups were performed
by means of the log rank (Mantel-Cox) test; p=0.215
DiscussionThe main finding of the present study was a lack of difference between the two systems of urine
drainage in the rate of urinary tract infections. In a previous study we compared the rate of
acquisition of bacteriuria in two groups of 224 consecutive patients who underwent bladder
catheterization with a TCDS during the first 6 months and with a CCDS during the next 6 months.
Bacteriuria occurred in 11.5% of TCDS patients and in 13.5% of CCDS patients (p>0.05) [14].
Together, the TCDS and the CCDS were assessed in 535 ICU patients for 2 years. No differences
were noted between the two systems.
Historically the drainage catheters of “open system” were inserted into the glass bottles, often
below the level of urine. Urine was stagnant, and bacteria could easily grow and ascent through
the drainage catheter [5]. The effectiveness of closed drainage system was compared with that of
a two-chamber drainage system. The TCDS that was tested is a quite simple device with no filter
and nonantireflux valve between the three components of system: Foley catheter, output measure
recipient, and urine collection bag. A port without filter is opened when urine samples are needed.
The TCDS was equipped with a urine collection bag emptied when needed without disconnecting
the system.
Most well-conducted clinical trials assessing different devices of urinary drainage fail to
demonstrate the effectiveness of most complex devices [10, 13, 18]. A study comparing a simple
closed drainage system and a CCDS during the first 5 days after catheter insertion in surgical
patients concluded that complex features aimed at preventing intraluminal spread of bacteria do
not reduce the risk of urinary tract infection [13]. A recent prospective, controlled, randomized
trial failed to demonstrate the effectiveness of a device that slowly releases silver ions onto the
inner surface of the drainage system [18]. This is at variance with the results of a previous study
that found a 6% rate of bacteriuria with a complex closed drainage system releasing povidone-iodine
vs. 23% with a simple drainage system [11]. The difference between the two systems should vary
5
from level of care provided by nurses in ICU, medical, or surgical wards, but this hypothesis
remains to be determined in carefully controlled randomized studies.
The CCDS with an antireflux valve, a tamper discouraging seal at the catheter-drainage tubing
junction, the addition of hydrogen peroiyde and chlorhexidine to drainage bag have failed to
demonstrate an effectiveness to prevent acquisition of catheter-associated bladder bacteriuria.
These processes add a cost to catheter management and may cause a false sense of security.
Considering the weak rate of catheter-associated bacteriuria in ICU and the effectiveness of closed
urinary drainage system compared with open urinary drainage system, we think that investment
in an expensive closed system is not cost-effective [10, 19].
In conclusion, the result of the present study comparing the effectiveness of TCDS and CCDS
in ICU patients confirms the findings of our previous study. With an 80% power to detect a 10%
difference in the rate of acquisition of bacteriuria, no differences were noted between the two
systems of drainage: catheter-associated bacteriuria occurred in 8% of cases with TCDS and in
8.6% of cases in CCDS. The recommendation to use complex close drainage system in ICU patients
is not supported by our clinical trials. The higher cost of CCDS is not justified for patients
hospitalized in ICUs.
References1. Vincent JL, Bihari DJ, Suter PM, Bruining HA, White J, Nicolas-Chanoin MH, Wolff M, Spencer RC,Hemmer M (1995) The prevalence of Nosocomial Infection in Intensive Care Units in Europe. Resultsof the European Prevalence in Intensive Care (EPIC) Study. JAMA 274:639–644
2. Richards MJ, Edwards JR, Culver DH, Gaynes RP (1999) Nosocomial infections in medical intensivecare units in the United States. National Nosocomial Infections Surveillance System. Crit Care Med2:887–892
3. Rosser CJ, Bare RL, Meredith JW (1999) Urinary tract infections in the critically ill patient with aurinary catheter. Am J Surg 177:287–290
4. Dukes C (1928) Urinary infections after excision of the rectum: Their cause and prevention. Proc RSoc Med 22:256–267
5. Kunin CM, McCormack RC (1966) Prevention of catheter-induced urinary-tract infections by sterileclosed drainage. N Engl J Med 274:1155–1161
6. Gillepsie WA, Lennon GG, Linton KB, Phippen GA (1967) Prevention of urinary tract infection bymeans of a closed drainage into a sterile plastic bag. BMJ 3:90–92
7. Thornton GF, Andriole VT (1970) Bacteriuria during indwelling catheter drainage: II. Effect of a closedsterile drainage system. JAMA 214:339–342
8. Platt R, Polk BF, Murdock B, Rosner B (1982) Mortality associated with nosocomial urinary tractinfection. N Engl J Med 307:637–642
9. Burke JP, Larsen RA, Stevens BS (1986) Nosocomial bacteriuria: estimating the potential for preventionby closed sterile urinary drainage. Infect Control 7:96–99
10. Degroot-Kosolcharoen J, Guse R, Jones JM (1988) Evaluation of a urinary catheter with a preconnectedclosed drainage bag. Infect Control Hosp Epidemiol 9:72–76
6
11. Al-Juburi AZ, Cicmanec J (1989) New apparatus to reduce urinary drainage with urinary tract infections.Urology 33:97–101
12. Huth TS, Burke JP, Larsen RA, Classen DC, Stevens LE (1992) Clinical trial of junction seal for theprevention of urinary catheter-associated bacteriuria. Arch Intern Med 152:807–812
13. Wille JC, Blusse Van Oud Alblas A, Thewessen EA (1993) Nosocomial catheter-associated bacteriuria:a clinical trial comparing two closed urinary drainage systems. J Hosp Infect 25:191–198
14. REANIS (1994) Prévention des infections urinaires nosocomiales In: REANIS (ed) Guide pour laprévention des infections nosocomiales en réanimation. Arnette, Paris, pp 40–52
15. Leone M, Garnier F, Dubuc M, Bimar MC, Martin C (2001) Prevention of nosocomial urinary tractinfection in intensive care unit patients: comparison of effectiveness of two urinary drainage systems.Chest 120:220–224
16. Le Gall JR, Lemeshow S, Saulnier F (1993) A new Simplified Acute Physiology Score (SAPS II) basedon an European/North American multicenter study. JAMA 270:2957–2963
17. Garner JS, Jarvis WR, Emori TG, Horan TC, Hughes JM (1988) CDC definitions for nosocomialinfections. Am J Infect Control 16:128–140
18. Reiche T, Lisby G, Jorgensen S, Christensen AB, Nordling J (2000) A prospective, controlled,randomized study of the effect of a slow-release silver device on the frequency of urinary tract infectionin newly catheterized patients. BJU Int 85:54–59
19. Scheckler WE (1980) Hospital costs of nosocomial infections: a prospective three-month study in acommunity hospital. Infect Control 1:150–152
7
Tab
le 1. Description of patients with bacteriuria with two-chamber drainage system (TCDS) and those with complex closed drainage system (CCDS) (UTI urinary tract infection, SAPS
Simplified Acute Physiology Score)
CCDS(n=162)
TCDS(n=149)
14 (6/8)
12 (5/7)
Patients with bacteriuria (M/F)
4/2/8
2/3/7
Medical/surgical/trauma patients
44±17
44±18
Age (years)
41±13
40±16
SAPS II
10 (71%)
9 (75%)
Antibiotics (prescribed for non-UTI; %)
19±8
29±17*
Length of ICU stay (days)
15±6.3
21.5±11*
Duration of catheterization (days)
7.8±3.8
12.4±8.3*
Onset of bacteriuria (days)
d p<0.05
8