-
British Journal of Oral and Maxillofacial Surgery 51 (2013)
863867
Available online at www.sciencedirect.com
Comparison of different autografts foraesthetic rhinoplasty: is
the tragal caralternative?
Max J. Z a, b c, PaMark M tin HRobert A. Mischkowskia Department
of Oral and Craniomaxillofacial Surgery, University Cologne,
Germanyb Clinic for Facial Surgery, Cologne, Germanyc Department of
Plastic Surgery, Clinic Cologne-Merheim, Germanyd Departmente
Department
Accepted 1 AAvailable onl
Abstract
Auricular cainvestigationindications,were tragusfor
operatiocompared wintraclass coscapha. Thegrafts were pHarvesting
tis a good alt 2013 The
Keywords: Tr
Hereby wthe past 5 yeainterest. Thesstock or otherpayments
for
CorresponGermany. Tel
E-mail a
0266-4356/$ http://dx.doi.oof Trauma and Orthopaedics, Clinic
Cologne-Merheim, Germanyof Biomedicine, University of Basel,
Switzerlandpril 2013ine 21 May 2013
rtilage is an important source of grafts for various
reconstructive procedures such as aesthetic rhinoplasty. The
purpose of thiswas to compare tragal cartilage with auricular
cartilage harvested from the concha and scapha, and describe its
clinical viability,
and morbidity in rhinoplasty. A total of 150 augmentation
rhinoplasties with a total of 170 grafts were included. The donor
sites(n = 136), concha (n = 26), and scapha (n = 8). The time
needed to harvest the grafts, the donor site morbidity, and the
indicationsn were recorded. The anthropometric changes to 4
auricular variables after the cartilage had been harvested were
analysed andith those on the opposite side in 48 patients using
Students paired t-test. Intraobserver reliability was assessed
using Pearsonsrrelation. The mean (SD) harvesting time was 27 (8)
min for the concha, 4.5 (1.4) min for the tragus, and 5.7 (1.6) min
for thelargest graft was taken from the concha (28 19 mm), followed
by the tragus (20 12 mm), and the scapha (18 6 mm). Thelaced at the
following sites: tip grafts (n = 123), columella struts (n = 80),
shield (n = 20), rim (n = 17), and dorsal onlay (n = 15).
ragal cartilage is safe, simple, fast, and has a low morbidity,
but it can affect the patients ability to wear earphones. Tragal
cartilageernative for nasal reconstruction if a graft of no longer
than 20 mm is required.British Association of Oral and
Maxillofacial Surgeons. Published by Elsevier Ltd. All rights
reserved.
agus; Scapha; Concha; Grafts; Rhinoplasty; Morbidity
e disclose any commercial associations, current and withinrs,
that might pose a potential, perceived or real conflict of
e include grants, patent licensing arrangements,
consultancies,equity ownership, donations, advisory board
memberships orconducting or publicising the study.ding author at:
Eugen Langen Strasse 12, 50968 Kln,
.: +49 171 8349256.ddress: [email protected] (M.J.
Zinser).
Introduction
Since the fundamental work of Ortiz-Monasterio et al.,1Tardy et
al.,2 Peck,3 and Sheen,4 autogenous cartilage hasbeen the graft
material of choice in nasal surgery in termsof safety, durability,
and versatility. Most surgeons preferthe septum as their first
choice of donor site, followedby the conchal cartilage.5,6 Only a
few surgeons promotethe use of allografts as their first choice in
augmentationrhinoplasties.7,8 Cartilaginous grafts can be obtained
from the
see front matter 2013 The British Association of Oral and
Maxillofacial Surgeons. Published by Elsevier Ltd. All rights
reserved.rg/10.1016/j.bjoms.2013.04.001inser , Mathias Siessegger ,
Oliver Thammaegele d, Lutz Ritter a, Matthias Kreppel a, Mar
aaural cartilage intilage graft a viable
nangiotis Theodorou c,. Sailer e, Joachim E. Zller a,
-
864 M.J. Zinser et al. / British Journal of Oral and
Maxillofacial Surgery 51 (2013) 863867
Fig. 1. Distrib
nose, the senal ear provwhen the ssecondaryprefer concplasties,
bumainly poshypertrophconchal ca
Cochransince introdgraft-deplehensive stuand scaphaassessed
thsibility insite morbideach graft.
Materials
This retrosplasties do(Table 1); 1primary, 35cleft lip rep
Only paconcha, orwhom septcartilage grscaphal grawere donegal
cartilagwomen (68(32%), mea
The grastructure odefects, sm
. Technd at the
ur (assynd
and thsigne
inki pr
ssmensis
r siteded focomp
that rts inclonor s
48 phad besite uneerdaangleeen th
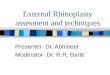
andopomperatiution of donor sites and properties of auricular
cartilage grafts.
ptum, the rib, and the external auricle.2 The exter-ides a
viable alternative in graft-depleted patients
eptal cartilage had already been used, ideally forand tertiary
rhinoplasties.913 Most surgeons stillhal grafts for
augmentation-reconstruction rhino-t Grobbelaar et al.14 reported a
morbidity of 2.2%,toperative deformities of the ear, haematomas,
andic scarring. The mean time needed to harvest thertilage ranges
between 25 and 30 min.2,11,13
and DeFatta9 and Kotzur and Gubitsch10 haveuced the tragal
cartilage as a viable alternative in
ted patients. The purpose of the present compre-dy was to
compare tragal cartilage with conchall cartilage for augmentation
rhinoplasty. We havee different clinical indications, viability,
and fea-cluding the time taken to harvest the graft, donority, and
anthropometric changes of the ear for
and methods
pective study comprised 150 augmentation rhino-ne between
February 2001 and April 201140 were done for aesthetic reasons, and
100 were
Fig. 2marke
contoroofskinjectsHels
Asseanaly
Donorecor
earlypainplainthe d
Inlageoppoby Wsionbetwsuredanthrpostosecondary, and 5 tertiary.
Ten patients had had aair and required reconstruction of the cleft
nose.tients who had auricular cartilage grafts (tragus,scapha) were
included (Fig. 1, Table 1). Patients inal cartilage was used were
excluded. A total of 170afts (136 tragal (80%), 26 conchal (15%),
and 8fts (5%)) were harvested (Fig. 1). All operationsby 3
experienced surgeons. In 10 patients, tra-e was harvested from both
sides. There were102%), mean (SD) age 25 (5) years, and 48 menn
(SD) age 26 (5) years.fts were used to: reconstruct the
cartilaginousf cleft noses, cover bony and cartilaginousooth out
irregularities, stabilise (as batten grafts),
Grafting te
The scaphaccording t
The mingal cartilagtragal rimto the antersection witfacilitates
t1012 mmthe whole2 mm wideique for harvesting tragal cartilage. The
incision line must beposterior border of the edge of the
tragus.
shield grafts), refine the nasal tip, avoid openrome, and
prevent formation of scars between thee bone, particularly if the
skin was thin. All sub-d consent forms according to the Declaration
ofeoperatively.
t of donor site morbidity and anthropometric
morbidity and harvesting time of each graft werer each patient.
This included documentation oflaints, including haematoma and
perioperativeesolved within 3 weeks, and irreversible com-uding
scarring, sensory disturbances, and pain atites.atients the
anthropometric changes after carti-en harvested were compared with
those from theaffected ear according to the protocol described
.15 The width, length of the auricles, the protru-of the
mastoidauricular plane, and the distancee tragus and the lateral
canthus, were mea-
compared with those of the unaffected side. Theetric
measurements were made at least 6 monthsvely when the swelling had
completely resolved.chniques
al and conchal cartilage grafts were harvestedo the technique
described by Nolst Trenit.16imally invasive approach to the
harvesting of tra-e is shown in Fig. 2.10 From an incision in
the
at the inner border, we dissect subperichondrallyior and
posterior of the tragal cartilage. Hydrodis-h local anaesthetic
solution containing adrenalinehe preparation. The facial nerve is
located aboutanterior to the lower end of the cartilage.
Nearlytragus can be removed, leaving only a small rimat the site of
the incision for structural support.
-
M.J. Zinser et al. / British Journal of Oral and Maxillofacial
Surgery 51 (2013) 863867 865
Table 1Morbidity of donor and recipient sites of external
cartilage of the ear (n = 170). Data are number (%) of
patients.Variable Tragus (n = 136) Concha (n = 26) Scapha (n = 8)
Total (n = 170)Rhinoplasty 8 150
Primary 8 100Secondary 8 5Tertiary 5Cleft nose 10
Recipient site Tip/onlay g 6 123Dorsum on 15Rim/batten 2
17Columella 80Shield graf 20
Donor site moEarly (reve 1 7(4)
Haemato 5Perioper 2
Late (not re 1 10 (7)Scarring 5Pain on p 2Hypoaes 2Clicking 1
1Unable t
Harvesting timDressing
Properties ofSize (mm)ShapeQuality
The woundto prevent a
Statistical a
All data wcal PackagInc., ChicKolmogorosoft tissuedistributedto
assessanthropomvested comassess interthe anthrotified
usinProbabilitiecant.
Results
The types oIt was possIt was necewho requir(such as a
e for srtilage
r site126 2689 930 66 21 9
raft 100 17lay graft 4 11graft 9 6
strut 60 20t 10 10rbidity
rsible) 2 (1) 5ma 1 4ative pain 1 1versible) 5 (4) 6
1 4ressure 1 1
thesia 1 1sensation
o wear earplugs 2 e (min) 5 27
45cartilage
20 20 28 19Thin, straight ConvexFirm Stiff
can be closed with a transtragal mattress suturehaematoma. No
additional dressing is needed.
nalysis
choictal ca
Donoere analysed with the help of the Statisti-e for the Social
Sciences (version 17.0, SPSSago). The distribution was assessed by
thevSmirnov test and found to be normal. Allvariables of the
external ear were normally
, allowing the use of Students paired t-testthe significance of
the difference between theetric variables after the graft had been
har-pared with those on the unaffected side. To
observer reliability, two different surgeons madepometric
measurements. Reliability was quan-g Pearsons intraclass
correlation coefficient.s of less than 0.05 were accepted as
signifi-
f graft and their distribution are shown in Table 1.ible to use
the tragal cartilage in 136 cases (80%).ssary to use conchal
cartilage in 26 patients (15%)ed extensive reconstruction of the
cartilage framecleft nose). Grafts from the ears were our first
The early awhose scarposterior au
There wgrafts (Figwere nearl
Fig. 3. Technprepared andtragal border
6
18 6 Straight Flexible
econdary and tertiary rhinoplasties when the sep-had already
been used.
morbiditynd late morbidity are shown in Table 1. One
patientretracted and who had an adhesion between thericle and the
mastoid skin required revision.as less early morbidity after
harvest of tragal
. 3, Table 1). Following tragal harvest, the scarsy invisible
(Fig. 3) and were of better quality
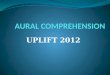
ique for harvesting tragal cartilage. An anterior flap must bea
strip of cartilage 1.52 mm wide preserved at the posteriorto ensure
structural support.
-
866 M.J. Zinser et al. / British Journal of Oral and
Maxillofacial Surgery 51 (2013) 863867
Fig. 4. Technique for harvesting tragal cartilage: almost the
entire cartilagecan be harvested.
than the chonchal grafts (Fig. 4). The tragal cartilage
alsoshowed superior results as far as late morbidity was
concerned(Table 1 and Fig. 5).
Harvesting time and properties of the grafts
A further focus of this study was the time taken to harvest
thegraft, including the size and shape of the monolayer
cartilage(Fig. 1 and Table 1), and tragal grafts took less time,
and didnot require dressing. Fig. 1 illustrates the properties of
eachcartilage graft.
Fig. 5. Appeagraft.
Anthropometric analysis
Four soft tissue variables were chosen to evaluate the
anthro-pometric charvested,there was aharvesting(p < 0.45).(p
< 0.52).gus and thmean variaThe inter-o
Discussion
Numerousfunctionalmost recenhigh-densitsimilar toever, the
firUnfortunatularly in sefrom differproblem wture, their cand
cannotcartilage grThe conchamultiple, b
plastiesectiurrellamewephalowo
eaHowegrafthologectedsonabrhinoand r
Mlar frthe cthe tlage.auralmorpunaffis rearance of the almost
invisible scar after harvest of the tragal
the ears.20Murrell
frameworkcartilage btion, the hplacementoperative dforming.
Tragal chas other eit is both teasier and fneed for
sphaematomahanges to the ears after the cartilage had beenand these
did not differ significantly. Althoughmean difference in length of
the conchal grafts,of scaphal or tragal cartilage had no effectThe
difference in width amounted to 2.3 mmThe mean difference in
distance between the tra-e lateral canthus was 1.3 mm (p <
0.341) and thetion in the protrusion angle was 2.1 (p <
0.61).bserver reliability (0.814).
materials have been described for grafting inas well as in
aesthetic rhinoplasty. Niechajev8tly published excellent long-term
results usingy polyethylene implants, which have a
morbidityprocedures that involve autologous grafts. How-st choice
for most authors is still septal cartilage.17ely, enough of this is
not always available, partic-condary rhinoplasty revisions.
Auricular cartilageent sites around the ear is the second choice.18
Theith conchal cartilage grafts is their irregular struc-urvature,
and the fact that the cartilage is elasticbe crushed. Some authors
also combine auricularafts with bone grafts or cartilage from the
ribs.19l cartilage is a beneficial source of cartilage when
igger pieces of cartilage are needed, for instance ines for
cleft lip or nasal reconstructions after traumaon of tumours.12
reported changes in the aesthetics of the auricu-ork including
distortion of the auricle, changes inauricular angle that result in
asymmetry betweenrs, or visible scarring after harvest of the
carti-ver, our results showed that none of the external
s (tragus, scapha, or concha) showed significantical differences
between the operated side and theside. Independently of the
surgical intervention, itle to assume that there is normal
variation between
12 further stated that changes in the auricularcan be avoided by
preserving a central strut of
etween the cymba and cavum concha. In addi-arvesting of conchal
cartilage also requires theof a cumbersome and often uncomfortable
post-ressing, or bolster, to prevent a haematoma from
artilage avoids many of these complications andssential
advantages, the biggest of which is thathin and straight.
Harvesting from the tragus isaster than harvesting from the concha.
There is noecial postoperative dressings, there is less risk of,
and a straight graft can be obtained that is firmer
-
M.J. Zinser et al. / British Journal of Oral and Maxillofacial
Surgery 51 (2013) 863867 867
than one taken from the concha. However, haematomas canbe
prevented simply and effectively when harvesting tragalcartilage by
insertion of a single transtragal mattress suture,which can be
removed 48 h postoperatively.
Tragal cartilage has many different applications in rhino-plasty
surgery. Because of its shape it is ideal for the
slightaugmentation of the nasal dorsum, to smooth
irregularities,and to hide an open roof. It can also be used for
alar contour(rim) grafts, for which the cartilage is cut into 3 15
mmpieces and then placed in an undermined pocket to help cor-rect
minor alar retraction or to strengthen the alar side wall.For
patients with collapsed nasal valves, tragal cartilage issuitable
for use as alar batten grafts. It is particularly well-suited for
grafts of the nasal tip such as shield grafts, onlaytip grafts, and
columella struts, because it is pliable and
notparticularlyexcellent sosal augmenor irregularwork. Howcartilage
isumellar strgrafts benot the castragal graftwe have noularly
thinprevent theskeleton.
A drawbever, the pietypically mquality forcaused usrently
useborne in miharvestingearphones.they workwith the pa
The scawe have almlimited amflat quality
corrective measures, and cannot be recommended for casesin which
substantial structural change is needed.
References
1. Ortiz-Monasterio F, Olmedo A, Oscoy LO. The use of cartilage
grafts inprimary aesthetic rhinoplasty. Plast Reconstr Surg
1981;67:597605.
2. Tardy Jr ME, Denneny III J, Fritsch MH. The versatile
cartilage autograftin reconstruction of the nose and face.
Laryngoscope 1985;95:52333.
3. Peck GC. Secondary rhinoplasty. Clin Plast Surg
1988;15:2941.4. Sheen JH. Tip graft: a 20-year retrospective. Plast
Reconstr Surg
1993;91:4863.5. Guerrerosantos J. Nose and paranasal
augmentation: autogenous, fascia
and cartilage. Clin Plast Surg 1991;18:6586.6. Rodriguez-Camps
S. Augmentative rhinoplasty with an auricular gibbus.
Aesthetic Plast Surg 1998;22:196205.chajev
l and hichajevedpore)chran Crnative8;138:
tzur A,sthetic Pe M, Ca
versalrrell GLg 2008
ticocheas as a dobbelaatilage gerda Httgart: Tlst Treninoplasu
BR.gery. Panovicnt in cinologye Y, Kimed use osal
onlaschkownor-site8;121:
thier DDphonesthick. Its uniform, smooth contour makes it anurce
of onlay grafts for minimal amounts of dor-tation, or for
camouflaging localised depressionsities of contour in the
osseocartilagenous frame-ever, Cochran and DeFatta9 reported that
the tragalless suitable for structural grafting such as col-
uts, lateral crural strut grafts, and dorsal spreadercause it is
not sufficiently strong or thick. This ise according to our
experience; we routinely useds as columellar or lateral crural
strut grafts, andt found any limitations. In patients with
partic-skin it can also be used to camouflage scars andir formation
between the skin and the bony nasal
ack of tragal cartilage is its limited supply. How-ce of tragal
cartilage that can usually be harvestedeasures 20 12 mm and is
usually of sufficientthe applications described. These results
have
to change our clinical conception, and we cur-predominantly
tragal grafts, although it must bend that Pothier and Charaklias21
found that tragalsignificantly affects the patients ability to
wearThis can be an important issue (for example, if
in security or the police) and should be discussedtients.phal
cartilage also gave low morbidity. However,
ost completely abandoned its use because of theount that can be
harvested and the rather thin and
of the cartilage. It may best be used for small
7. Nieica
8. Nie(M
9. Coalte200
10. KoAe
11. Leand
12. MuSur
13. Orear
14. Grcar
15. WeStu
16. NoRh
17. Nesur
18. JovplaRh
19. Lebindor
20. MiDo200
21. PoearI. Porous polyethylene implants for nasal
reconstruction: clin-stologic studies. Aesthetic Plast Surg
1999;23:395402.I. Facial reconstruction by porous high-density
polyethylene: long-term results. Aesthetic Plast Surg
2012;36:91727.S, DeFatta RJ. Tragal cartilage grafts in
rhinoplasty: a viablein the graft-depleted patient. Otolaryngol
Head Neck Surg
1669.Gubisch W. Tragal cartilage grafts in aesthetic
rhinoplasty.last Surg 2003;27:2328.llahan S, Cochran CS. Auricular
cartilage: harvest techniqueity in rhinoplasty. Am J Otolaryngol
2011;32:54752.. Tragal cartilage grafts in
rhinoplasty.OtolaryngolHeadNeck
;139:1767.M. A new method for total reconstruction of the nose:
the
onor area. Clin Plast Surg 1981;8:481505.r AO, Matti BA, Nicolle
FV. Donor site morbidity post conchalrafting. Aesthetic Plast Surg
1997;21:902.. Basic principles. In: Weerda H, editor. Surgery of
the ear.hieme; 2004. p. 110 [in German].it GJ. Grafts in nasal
surgery. In: Nolst Trenit GJ, editor.ty. Amsterdam: Klugerer
Publications; 1998. p. 4966.Combined conchal cartilageethmoid bone
grafts in nasallast Reconstr Surg 2000;106:1715.S, Berghaus A.
Autogenous auricular concha cartilage trans-orrective rhinoplasty.
Practical hints and critical remarks.1991;29:2739.
J, Lee E. Lengthening of the postoperative short nose: com-f a
gull-wing concha composite graft and a rib costochondraly graft.
Plast Reconstr Surg 2000;105:2190201.ski RA, Domingos-Hadamitzky C,
Siessegger M, et al.morbidity of ear cartilage autografts. Plast
Reconstr Surg
7987., Charaklias N. Tragal cartilage harvesting and in the
ear
: a pilot study. J Laryngol Otol 2006;120:13.
Comparison of different autografts for aural cartilage in
aesthetic rhinoplasty: is the tragal cartilage graft a viable
alternative?IntroductionMaterials and methodsAssessment of donor
site morbidity and anthropometric analysisGrafting
techniquesStatistical analysis
ResultsDonor site morbidityHarvesting time and properties of the
graftsAnthropometric analysis
DiscussionReferences

























![[ 176 ] THE BEHAVIOUR AND FATE OF SKIN AUTOGRAFTS AND](https://img.pdfslide.us/doc/110x75/586a0fbd1a28ab136b8bafdb/-176-the-behaviour-and-fate-of-skin-autografts-and-.jpg)
