Embed Size (px)
Citation preview

Journal of Clinical Neuroscience 20 (2013) 367–372
Contents lists available at SciVerse ScienceDirect
Journal of Clinical Neuroscience
journal homepage: www.elsevier .com/ locate/ jocn
Clinical Study
Comparison of covered stents with detachable balloons for treatmentof posttraumatic carotid-cavernous fistulas
Bo Yin, Han-Song Sheng, Rui-Li Wei, Jian Lin, Hui Zhou, Nu Zhang ⇑Department of Neurosurgery, The Second Affiliated Hospital & Yuying Children’s Hospital of Wenzhou Medical College, No. 109, Xue Yuan Road,Wenzhou, Zhejiang Province 325027, China
a r t i c l e i n f o
Article history:Received 29 January 2012Accepted 8 February 2012
Keywords:Carotid-cavernous fistulaCCFCovered stentDetachable balloonEndovascular treatmentTrauma
0967-5868/$ - see front matter � 2012 Elsevier Ltd. Ahttp://dx.doi.org/10.1016/j.jocn.2012.02.030
⇑ Corresponding author. Tel./fax: +86 577 8883269E-mail address: [email protected] (N. Zhang).
a b s t r a c t
Treatment of posttraumatic direct carotid-cavernous fistula (DCCF) with detachable balloons (DB) is asso-ciated with relatively low complete occlusion rates. We aimed to compare the angiographic and clinicalresults of treatment with covered stents with the results of treatment with DB. Thirty-four patients withposttraumatic DCCF were selected for treatment with DB (n = 19, group A) or covered stents (n = 15,group B). Data on the technical success, duration of initial procedure and hospital stay, initial and finalangiographic results, mortality, morbidity and final clinical outcomes were collected and analyzed within12 months. DB deployment and covered stent placement were technically successful in all patients,except one patient in group B in whom the covered stent failed to navigate to the target DCCF. The initialangiographic results for the 33 patients with successful procedures showed complete occlusion in 16patients in group A (84.2%; 95% confidence interval [CI]: 66%, 102%) and 11 patients in group B (78.6%;95% CI: 54%, 103%; p > 0.05). The 12-month angiographic results indicated complete occlusion in 12patients in group A (63.2%; 95% CI: 39%, 87%) and 14 patients in group B (100%; p = 0.013). The averageinitial procedure time was 120.0 ± 17.76 minutes in group A and 93.15 ± 8.12 minutes in group B(p < 0.001). No significant differences were seen between the two groups in technical success, mortality,morbidity or final clinical outcomes. In this nonrandomized, prospective study of posttraumatic DCCFtreatment, the 12-month angiographic results of treatment with covered stents was superior to that ofBD.
� 2012 Elsevier Ltd. All rights reserved.
1. Introduction
Posttraumatic direct carotid-cavernous fistula (DCCF) is aninfrequent complication resulting from craniomaxillofacial injuriesor basilar skull fracture. Transarterial balloon occlusion of carotid-cavernous fistulas (CCF) has been widely accepted as the preferredmethod for treating DCCF in many centers around the world be-cause it is easy and cheap in a highly expensive medical marketand has a high rate of successful occlusion of the fistula and pres-ervation of the internal carotid artery (ICA).1–5 However, residualCCF or recurrence, as well as pseudoaneurysm formation, arefrequently major complications of balloon occlusion of CCF dueto incomplete occlusion of the orifice with the detachable balloon(DB), especially in patients with difficult or complex CCF.
To overcome these disadvantages, covered stents have beenused to manage posttraumatic CCF, and very attractive results havebeen achieved.6–10 They preserve or reconstruct the pathologicparent vessel, simplify the endovascular procedure, shorten the
ll rights reserved.
3.
procedure time and reduce the cost because they can be placedacross the ostium of the fistula. Here we present the results of anonrandomized prospective trial of endovascular treatment ofposttraumatic DCCF with a DB or covered stent, with the goal ofcomparing the efficacies of these two treatments within a12-month period.
2. Materials and methods
2.1. Study design
The study was approved by our Institutional Review Board, andwritten informed consent was obtained from all patients or theirimmediate relatives. From June 2007 to September 2011, patientsreferred for endovascular treatment of posttraumatic DCCF withDB (group A) or a covered stent (group B) were screened for inclu-sion in this nonrandomized, prospective trial, and subsequentlyunderwent follow up at our hospital.
Patients were included in the final analysis if they met the fol-lowing criteria: (i) definite posttraumatic unilateral DCCF (type A,Barrow et al. classification11), as demonstrated by arterial

Table 1Comparison of baseline characteristics of two groups treated for direct carotid-cavernous fistula (DCCF)
Detachableballoon (n = 19)
Covered stent(n = 15)
p value
Age (years) 31.11 ± 9.90 33.43 ± 8.22 0.480Male/female (No.) 12/7 9/6 0.947Duration of DCCF (months) 1.63 ± 0.76 1.79 ± 0.80 0.578
EtiologyTraffic accident 19 (100%) 15 (100%) 0.999
Data are mean ± standard deviation, or number (%) unless noted.
368 B. Yin et al. / Journal of Clinical Neuroscience 20 (2013) 367–372
angiography; (ii) good tolerance of the balloon occlusion test(BOT); (iii) the diameter of the parent artery was <5.0 mm; and(iv) at least one control angiogram was taken >6 months afterthe initial treatment. Patients were excluded if any of the followingwas present: (i) a tortuous vessel proximal to the parent arteryand/or lack of appropriate access routes, thereby rendering the pa-tient unsuitable for endovascular treatment; (ii) an inability of thepatient to undergo general anesthesia or endovascular interven-tion; or (iii) expected patient survival of <1 year because of otherco-existing diseases.
2.2. Detachable balloon deployment
We used a single microcatheter for DB deployment (Goldbal;BALT Extrusion, Montmorency, France), and the balloon wasinflated with hypertonic, water-soluble contrast material. The bal-loon-mounted microcatheter was negotiated slowly in to the fistulaby flow guidance. The balloon was sometimes partially inflated forflow-direction to the fistula orifice, and in addition microwires wereused to support the assembly for proper navigation. In order toconfirm the location of the balloon and to characterize the targetedfistula, a contrast agent was injected through the guiding catheter.Once the balloon was satisfactorily positioned, it was graduallyinflated to assess the status of the fistula. If obliteration of the fistulawith the preservation of the ICA was not demonstrated with cere-bral angiography, the balloon was repositioned inside the fistuloussac for proper closure of the fistulous site. Last, the balloon was de-tached. Often more than one balloon or replacement balloon wasused to occlude large compartments of the cavernous sinus. Postop-eratively, low-molecular heparin was given to patients for 48 hours,and all patients had absolute bed rest for up to 48 hours, withrestrictions on head movement. Head radiographs were taken at1, 3 and 7 days after the procedure.
2.3. Covered stent placement
We used the Jostent Coronary Covered Stent (Abbott Vascular,Redwood City, CA, USA), which is a commonly used composite bal-loon-expandable stent with an ultrathin layer of expandablepolytetrafluroethylene sandwiched between two stainless steelstents; a conventional angioplasty balloon is manually compressedwithin this device.12,13 The technique of placing the covered stentand periprocedure management has been described previ-ously.12,13 Briefly, all procedures were performed under generalanesthesia. After positioning a 6-French Envoy (Cordis, MiamiLakes, FL, USA) guiding catheter in the ICA, a microguidewire(Transend Floppy; Boston Scientific, Natick, MA, USA) was navi-gated into a distal branch of the middle cerebral artery. With road-map guidance, the covered stent was navigated over themicroguidewire and bridged the orifice of the fistula. Angiographywas performed immediately after the balloon deflation to confirmthe correct placement of the stent and a satisfactory occlusion ofthe fistula.
Prior to the procedure, the patients took aspirin (100 mg/day)and clopidogrel (75 mg/day) for three consecutive days. Patientsreceived a bolus of 5000 IU heparin at the start of the procedure,followed by a continuous infusion of 1000 IU/hour, with the aimof keeping the activated clotting time above 300 seconds. Heparinwas given for 48 hours after the procedure, and the patients wereinstructed to take aspirin (100 mg/day) and clopidogrel (75 mg/day) orally for 6 months to avoid thrombosis and in-stent stenosis.
2.4. Follow-up and postoperative outcome evaluation
The follow-up protocols were performed at 1, 3, 6 and12 months, and included both clinical and angiographic examina-
tions. Data on the technical success, initial and final angiographicresults, mortality, morbidity and final clinical outcome were retro-spectively collected and analyzed at the time of discharge and atthe end of the follow ups.
The angiographic data were categorized into two groups: (i)complete occlusion, no residual cavity and no endoleak; and (ii)incomplete occlusion, a residual cavity or an endoleak.14–16 Theclinical follow ups were graded into four types: (i) a full recoveryfrom the neurologic symptoms, (ii) improved neurologic symp-toms, (iii) unchanged symptoms and (iv) a deterioration in theneurologic symptoms.7,14–16
To compare the efficacies of these two treatment approaches,we ended the angiographic follow up at 12 months. Within the12-month period, we generally did not perform any further treat-ment, including DB deployment or covered stent placement forminimal residual or recurrence of DCCF or pseudoaneurysm forma-tion, unless a recovery slowed or improved neurologic symptomsdeteriorated again. Patients with residual or recurrent CCF orpseudoaneurysms were treated with DB, coiling or covered stentsafter the 12-month angiographic follow up.
2.5. Statistical analysis
Descriptive data are given as the mean ± SD. The Mann-Whitney U test was used to compare continuous variables. Thechi-squared test and unpaired t-test were used for comparing thecategorical variables if all expected frequencies were greater thanor equal to five. Otherwise, Fisher’s exact test was used. All statis-tical analyses were performed using the Statistical Package for theSocial Sciences, version 13.0 (SPSS, Chicago, IL, USA).
3. Results
3.1. Patients
From June 2007 to September 2011, 42 patients with posttrau-matic DCCF were enrolled in this study. Initially, the study popula-tion consisted of 23 patients in the DB group (group A) and 19patients in the covered stent group (group B). Of these, eight pa-tients did not meet the final inclusion criteria, with angiographicfollow-ups later than the 6-month cut-off in five patients and fol-low-up loss in three patients (one in group A and two in group B).So, a final total of 19 and 15 patients were included in group A andgroup B, respectively. The demographic and clinical characteristicsof the 34 patients with posttraumatic DCCF are summarized inTable 1. The patients included 21 men and 13 women with a meanage of 32.09 ± 9.16 years (range: 15–52 years).
3.2. Primary procedural results
The clinical outcomes within the 12-month period for the twogroups are shown in Table 2. Endovascular DB deployment and

Table 2Comparison of clinical outcomes within a 12-month period of two groups treated fordirect carotid-cavernous fistula (DCCF)
Detachableballoon (n = 19)
Covered stent(n = 14)a
pvalue
Complete occlusion at initialangiography
16 (84%) 11 (79%) 0.607
Initial procedure time(minutes)
120.0 ± 17.76 93.15 ± 8.12 <0.001
Hospital stay (days) 5.16 ± 4.16 5.71 ± 1.54 0.299Culminate morbidity 9 2 0.067
Transient neurologic deficit 1 (5.3%) 1 (7.1%)Vasospasm 2 (10.5%) 1 (7.1%)Acute thrombosis 0 (0%) 0 (0%)Pseudoaneurysm 6 (31.6%) 0 (0%)Stenosis 0 (0%) 0 (0%)
Complete occlusion at 12-month angiography
12 (63%) 14 (100%) 0.013
Full recovery at 12-monthclinical follow up
18 (95%) 12 (86%) 0.561
Data are mean ± standard deviation, or number (%).a The one patient in whom the covered stent failed to navigate to the target DCCF
was excluded.
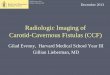
Fig. 1. A 23-year-old male with pulsatile exophthalmos, retroorbital bruit and chemosisof the left internal carotid artery showing a direct carotid-cavernous fistula (DCCF). (Bshowing complete occlusion of the CCF. (C) Lateral cerebral angiography of the left intersegment at 6-month follow up. (D) Lateral cerebral angiograph showing complete occluangiograph performed 3 months after the covered-stenting procedure showing total obl
B. Yin et al. / Journal of Clinical Neuroscience 20 (2013) 367–372 369
covered stent placement were technically successful in all patients,except one patient in whom the covered stent failed to navigate tothe target DCCF. The average initial procedure time was120.0 ± 17.76 minutes in group A and 93.15 ± 8.12 minutes ingroup B (p < 0.001).
In group A, complete DCCF occlusion was obtained in 16 pa-tients (84.2%; 95% CI: 66%, 102%; Fig. 1) and incomplete occlusionwas obtained in three patients at the end of the initial procedure.In group B, complete DCCF occlusion without endoleak wasachieved in 11 patients (78.6.9%; 95% CI: 54%, 103%; Fig. 2) andtransient endoleaks were observed in three patients immediatelyafter initial covered stent deployment. There was no significant dif-ference between the two groups in the success rate as measured bycomplete DCCF occlusion.
3.3. Procedural complications
One patient in each group experienced a transient neurologicdeficit due to a parent artery spasm related to DB deployment orstent placement, without permanent neurologic deficits. No newischemic foci were found on the subsequent head CT scans of these
in the left eye after a traffic accident 2 weeks earlier. (A) Lateral cerebral angiograph) Lateral cerebral angiography immediately after detachable balloon deployment
nal carotid artery showing the presence of a pseudoaneurysm (arrow) of the left C4sion of the aneurysm immediately following stent placement. (E) Lateral cerebral
iteration of the aneurysm with patency of the parent artery.

Fig. 2. A 34-year-old female with a pulsatile exophthalmos, retroorbital bruit, chemosis and ophthalmoplegia in the right eye after a traffic accident 2 months earlier. (A)Lateral cerebral angiograph of the right internal carotid artery showing a carotid-cavernous fistula (CCF). (B) Lateral cerebral angiograph showing single covered stent(between the two arrows) for the treatment of the CCF. (C) Lateral cerebral angiograph immediately after the covered stent deployment showing occlusion of the fistula withpatency of the parent artery.
370 B. Yin et al. / Journal of Clinical Neuroscience 20 (2013) 367–372
patients. Obvious intracranial vasospasm was observed in two pa-tients in group A and one patient in group B, which were resolvedby dilute papaverine hydrochloride infusion through the guidingcatheter.
In the remaining 29 patients (16 in group A and 13 in group B),no morbidity or mortality occurred during or after treatment. Fur-thermore, head CT scans taken immediately postprocedure and atdischarge confirmed that the procedures were uneventful, with noevidence of ischemia.
3.4. Follow-up angiographic results
The final 12-month follow-up angiographs exhibited completeocclusion in 12 group A patients (63.2%; 95% CI: 39%, 87%) andan incomplete occlusion in seven patients (Table 2). In three pa-tients with incomplete occlusion after the initial procedure, twopatients displayed spontaneous DCCF resolution. In the remainingpatient, the minimal residual DCCF failed to spontaneously resolveitself within the 1-year period, and was treated with coils. For 16patients displaying complete occlusion after the initial procedure,six (37.5%) displayed pseudoaneurysm formation (Fig. 1). Threeof the six pseudoaneurysms were treated with covered stents afterthe 1-year period, which resulted in complete occlusion of thepseudoaneurysms (Fig. 1). The other three pseudoaneurysms weresmall and asymptomatic, and the patients remain underobservation.
In group B, the final angiographs indicated complete occlusionin the 14 group B patients with 14 DCCF in whom stent placementwas technically successful. Three patients had a residual endoleakafter the initial procedure. By 3-month follow up, all three patientshad had spontaneous endoleak resolution and DCCF obliterationwith ICA reconstruction. No patient displayed in-stent stenosisduring the 1-year period.
The rate of complete DCCF occlusion in the final angiograph wassignificantly higher in group B than in group A (p = 0.013, Table 2).
3.5. Follow-up clinical results
A clinical follow up was available in all 33 patients with techni-cally successful procedures within the 12-month period (one pa-tient had a failed stent placement). In group A, 18 patients
experienced full recovery and one patient displayed improvementby the final clinical follow up. In group B, full recovery (n = 12) andimprovement (n = 2) were achieved in all 14 patients. There was noworsening of the preliminary clinical presentation and no occur-rence of ischemia or rebleeding in any patient in either group. Nosignificant difference in the full recovery rates was observed be-tween the two groups.
4. Discussion
The DB, which has been widely used for more than three dec-ades, is currently the endovascular approach that is first recom-mended for posttraumatic DCCF treatment in many centersaround the world, because it is easy and cheap in a highly expen-sive medical market and has a high success rate (75–88%) forocclusion of fistulas and preservation of the ICA.1–5 However,approximately 15–20% of patients17–19 with type A carotid cavern-ous fistulas still require occlusion of the ICA for successful treat-ment. Moreover, residual or recurrent CCF are major problemswith balloon occlusion of CCF, due to incomplete occlusion of theorifice with the DB. Also, even with 100% CCF occlusion after initialtreatment, there still remains a relatively high rate of pseudoaneu-rysm formation (30–44%) shown by long-term follow-upangiography.4,20
Direct surgical repair or clipping of CCF is usually not practicalbecause bony obstacles in this area make access and control diffi-cult. Surgery usually involves a high perioperative risk and a greatrisk of surgical trauma. In addition, CCF treated this way have a rel-atively high recurrence rate.1,21 Transarterial or transvenous coilembolization, with and without stent assistance, are seen by someas effective alternatives for the treatment of DCCF because the de-vices are easy to retrieve, reposition or exchange when neces-sary.22,23 However, coil treatment has a high cost and is notalways safe and effective2,24,25 due to mass effect and recurrenceof the fistula or aneurysm through coil compaction.22,26,27 Further-more, there is a risk of parent artery occlusion due to herniation ofa coil loop into the parent artery. Therefore, coil embolization isnot a good approach for treatment of posttraumatic CCF, becauseit is very difficult to permanently exclude the CCF from the circu-lation and to anatomically cure posttraumatic CCF.

B. Yin et al. / Journal of Clinical Neuroscience 20 (2013) 367–372 371
The availability of stents suitable for use in the intracranial vas-culature has increased the tools that are available to treat posttrau-matic CCF. Occlusion of posttraumatic CCF with covered stentplacement is an active, rather than a passive, procedure, and it ispossible to close the CCF orifice completely without endoleak.The drawbacks of residual or recurrent CCF, as well as pseudoaneu-rysm formation, coil impaction and migration, do not occur oncethe fistula is completely occluded. Even if an incomplete occlusionoccurs with an endoleak, the CCF disappears completely during fol-low up. Therefore, the covered stent provides a true anatomic curefor posttraumatic CCF and permanently excludes the CCF fromcirculation.
Covered stents have been successfully used for the treatment ofDCCF and its complications.6–10,28–30 With a covered stent, it is easyand quick to close the orifice of the CCF completely withoutendoleaks. However, clinical use of the covered stent for posttrau-matic CCF has been limited due to the often tortuous ICA, and theabsence of longitudinal flexibility in the stent, which makes it dif-ficult to navigate into lesions. To overcome this limitation, a longsheath, a guide catheter and a stiff exchange wire are needed tostraighten the vessel.8 Moreover, the delivery system should begently navigated into the intracranial lesion to prevent the occur-rence of complications caused by friction between the distal edgeof a stent and the arterial wall, such as dissection along the edgeof a stent or deformation of a stent. Therefore, neurosurgeonsand interventional neuroradiologists have been developing dedi-cated intracranial covered stents.31,32
In this study, our results showed improved final completeocclusion rates, reduced procedure times and no recanalizationwhen using covered stents as compared with BD deployment.The significant improvement in the complete occlusion rates dur-ing the 12-month period seemed to be predominantly attributableto the occlusion of the orifice of the DCCF. We saw no obviousdifferences in the clinical outcomes, overall mortality, morbidityor survival between the groups, although there were no deathsduring the study period. Although there were some difficulties innavigating the covered stent through the ICA, the covered stentseems to be more effective than DB with regard to complete occlu-sion of the CCF.
Recently, a flexible Willis covered stent, designed for dedicatedintracranial use, was developed by MicroPort Medical Company(Shanghai, China), and has been used for the treatment of intracra-nial aneurysms and DCCF.6,7,14–16 Preliminary results suggest goodflexibility and efficacy in cranial internal carotid artery (CICA)aneurysm treatment in patients without an extremely tortuousICA. The Willis covered stent has just finished phase IV (four) clin-ical trials, and we look forward to using this flexible covered stentin a future study.
Compared with DB deployment and coil embolization,4,16,20 theadvantages of a covered stent include: high final overall completeocclusion rates; it is a relatively simple and rapid procedure; andthere is no coil herniation into the parent artery, no delayed migra-tion, no coil loop protrusion, no mass effect in large pseudoaneu-rysms and no CCF recanalization and recurrence. Of theseadvantages, the high overall complete occlusion rates are the mostimportant.
Our results have important clinical implications. Use of acovered stent rather than coils in patients with CICA aneurysmswill substantially increase the complete occlusion and anatomiccure rates, and eliminate recanalization and mass effect occur-rence. In addition, considerable savings can be achieved by avoid-ing the costs of repeated coiling, and the treatment of recurrentposttraumatic CCF.
Our study has some limitations. First, this was a single-centerstudy, not a randomized controlled study. Second, the sample sizewas relatively small, and the long-term efficacy of the approach for
managing posttraumatic DCCF remains to be determined in a largeseries. The sample may be too small to generalize the results, andthese biases might prevent us from detecting possible differencesbetween the two groups (type II error). Third, the possibility of clo-sure of side branches (the inferolateral trunk, the posteroinferiorhypophyseal artery, the lateral clival artery, the recurrent arteryof the foramen lacerum, and the lateral artery of the gasserianganglion) stemming from the covered segment of the artery mightoccur after the stent placement and was not adequately assessed.In addition, in-stent stenosis might occur if the patient does notadhere to a regular anticoagulation regimen following stent place-ment and longer follow-up is needed to assess this.
5. Conclusion
In conclusion, in this nonrandomized, prospective trial, our re-sults indicated that the use of covered stents for posttraumaticDCCF was associated with superior intermediate-term angio-graphic results compared with the currently recommendedapproach of DB deployment. Further longer follow-up and ex-panded clinical trials are still needed.
References
1. Higashida RT, Halbach VV, Tsai FY, et al. Interventional neurovasculartreatment of traumatic carotid and vertebral lesion: results in 234 patients.AJR 1989;153:577–82.
2. Luo CB, Teng MM, Yen DH, et al. Endovascular embolization of recurrenttraumatic carotid-cavernous fistulas managed previously with detachableballoons. J Trauma 2004;56:1214–20.
3. Gupta AK, Purkayastha S, Krishnamoorthy T, et al. Endovascular treatment ofdirect carotid cavernous fistulae: a pictorial review. Neuroradiology2006;48:831–9.
4. Debrun G, Lacour P, Vinuela F, et al. Treatment of 54 traumatic carotid-cavernous fistulas. J Neurosurg 1981;55:678–92.
5. Lewis AI, Tomsick TA, Tew JM, et al. Long-term results in direct carotid-cavernous fistulas after treatment with detachable balloons. J Neurosurg1996;84:400–4.
6. Wang W, Li YD, Li MH, et al. Endovascular treatment of posttraumatic directcarotid-cavernous fistulas: a single-center experience. J Clin Neurosci2011;18:24–8.
7. Li MH, Li YD, Gao BL, et al. A new covered stent designed for intracranialvasculature: application in the management of pseudoaneurysms of the cranialinternal carotid artery. AJNR Am J Neuroradiol 2007;28:1579–85.
8. Felber S, Henkes H, Weber W, et al. Treatment of extra cranial and intracranialaneurysms and arteriovenous fistulae using stent grafts. Neurosurgery2004;55:631–8.
9. Gomez F, Escobar W, Gomez AM, et al. Treatment of carotid cavernous fistulasusing covered stents: midterm results in seven patients. AJNR 2007;28:1762–8.
10. Wang C, Xie X, You C, et al. Placement of covered stents for the treatment ofdirect carotid cavernous fistulas. AJNR 2009;30:1342–6.
11. Barrow DL, Spector RH, Braun IF, et al. Classification and treatment ofspontaneous carotid-cavernous sinus fistulas. J Neurosurg 1985;62:248–56.
12. Saatci I, Cekirge HS, Ozturk MH, et al. Treatment of internal carotid arteryaneurysms with a covered stent: experience in 24 patients with mid-termfollow-up results. AJNR Am J Neuroradiol 2004;25:1742–9.
13. Maras D, Lioupis C, Magoufis G, et al. Covered stent-graft treatment oftraumatic internal carotid artery pseudoaneurysms: a review. CardiovascIntervent Radiol 2006;29:958–68.
14. Li YD, Li MH, Gao BL, et al. Endovascular treatment of recurrent intracranialaneurysms with re-coiling or covered stents. J Neurol Neurosurg Psychiatry2010;81:74–9.
15. Li MH, Li YD, Tan HQ, et al. Treatment of distal internal carotid artery aneurysmwith the willis covered stent: a prospective pilot study. Radiology2009;253:470–7.
16. Li MH, Leng B, Li YD, et al. Comparative study of covered stent with coilembolization in the treatment of cranial internal carotid artery aneurysm: anonrandomized prospective trial. Eur Radiol 2010;20:2732–9.
17. Halbach VV, Higashida RT, Barnwell SL, et al. Transarterial platinum coilembolization of carotid-cavernous fistulas. AJNR Am J Neuroradiol1991;12:429–33.
18. Bavinzski G, Killer M, Gruber A, et al. Treatment of posttraumatic carotico-cavernous fistulae using electrolytically detachable coils: technical aspects andpreliminary experience. Neuroradiology 1997;39:81–5.
19. Jansen O, Dorfler A, Forsting M, et al. Endovascular therapy of arteriovenousfistulae with electrolytically detachable coils. Neuroradiology 1999;41:951–7.

372 B. Yin et al. / Journal of Clinical Neuroscience 20 (2013) 367–372
20. Lewis AI, Tomsick TA, Tew Jr JM. Management of 100 consecutive directcarotid-cavernous fistulas: results of treatment with detachable balloons.Neurosurgery 1995;36:239–44.
21. Charbel FT, Gonzales-Portillo G, Hoffman W, et al. Distal internal carotid arterypseudoaneurysms: technique and pitfalls of surgical management: twotechnical case reports. Neurosurgery 1999;45:643–8.
22. van Rooij WJ, Sluzewski M, Beute GN. Ruptured cavernous sinus aneurysmscausing carotid cavernous fistula: incidence, clinical presentation, treatment,and outcome. AJNR Am J Neuroradiol 2006;27:185–9.
23. Ahn JY, Lee BH, Joo JY. Stent-assisted Guglielmi detachable coils embolisationfor the treatment of a traumatic carotid cavernous fistula. J Clin Neurosci2003;10:96–8.
24. Klisch J, Huppertz HJ, Spetzger U, et al. Transvenous treatment of carotidcavernous and dural arteriovenous fistulae: results for 31 patients and reviewof the literature. Neurosurgery 2003;53:836–56.
25. Remonda L, Frigerio SB, Bühler R, et al. Transvenous coil treatment of a type acarotid cavernous fistula in association with transarterial trispan coilprotection. AJNR Am J Neuroradiol 2004;25:611–3.
26. Kobayashi N, Miyachi S, Negoro M, et al. Endovascular treatment strategy fordirect carotid-cavernous fistulas resulting from rupture of intracavernouscarotid aneurysms. AJNR Am J Neuroradiol 2003;24:1789–96.
27. Morón FE, Klucznik RP, Mawad ME, et al. Endovascular treatment of high-flowcarotid cavernous fistulas by stent-assisted coil placement. AJNR Am JNeuroradiol 2005;26:1399–404.
28. Tiewei Q, Ali A, Shaolei G, et al. Carotid cavernous fistulas treated byendovascular covered stent grafts with follow-up results. Br J Neurosurg2010;24:435–40.
29. Choi BJ, Lee TH, Kim CW, et al. Endovascular graft-stent placement fortreatment of traumatic carotid cavernous fistulas. J Korean Neurosurg Soc2009;46:572–6.
30. Fusonie GE, Edwards JD, Reed AB. Covered stent exclusion of blunt traumaticcarotid artery pseudoaneurysm: case report and review of the literature. AnnVasc Surg 2004;18:376–9.
31. Schonholz C, Krajcer Z, Carlos Parodi J, et al. Stent-graft treatment ofpseudoaneurysms and arteriovenous fistulae in the carotid artery. Vascular2006;14:123–9.
32. Magoufis GL, Vrachliotis TG, Stringaris KA. Covered stents to treat partialrecanalization of onyx-occluded giant intracavernous carotid aneurysm. JEndovasc Ther 2004;11:742–6.