Embed Size (px)
Citation preview

CinscahastagfrDt
M
D(fft
LAs
0d
Comparison of Coronary Restenosis Rates in Matched PatientsWith Versus Without Diabetes Mellitus
Peter W. Radke, MDa,b,*, Klara Friese, MSb, Andrea Buhr, MSb, Bernard Nagel, MSb,Lars-Christian Harland, MDa, Axel Kaiser, MDa,b, Marko Remmel, MDa, Peter Hanrath, MDb,
Heribert Schunkert, MDa, and Rainer Hoffmann, MDb
Diabetes mellitus (DM) is an established risk factor for stent restenosis, in part as a resultof the smaller vessel dimensions and longer lesions. This study compared the magnitude ofacute lumen gain and late lumen loss after elective coronary stent implantation in patientswith and without DM using a matched-pair analysis. A total of 133 patients with DM and192 coronary lesions were included in this analysis. A group of 192 lesions in 182 patientswithout DM were matched in a pairwise fashion, stratifying for reference diameter,minimal luminal diameter, and lesion length. The binary restenosis rate at the 5-monthfollow-up angiography was 25% in the DM group and 14% in the non-DM group (p <0.01).Acute angiographic lumen gain (1.47 � 0.41 vs 1.56 � 0.38 mm, p � 0.03) and late lumenloss (0.64 � 0.42 vs 0.55 � 0.36 mm, p � 0.02) were significantly different between the DMand non-DM groups. In conclusion, suboptimal acute procedural results and an exagger-ated neointimal proliferation contributed by about 50% to the lower net lumen gain in theDM group. Patients with DM had a significantly higher restenosis rate even when matchedfor preprocedural angiographic lesion dimensions. Mechanistically, inferior proceduralresults, as well as exaggerated neointimal proliferation, are, quantitatively, equally impor-tant in this process. © 2006 Elsevier Inc. All rights reserved. (Am J Cardiol 2006;98:
1218–1222)s1gibat
flftwcpwremAdg
pdbata
linically, patients with diabetes mellitus (DM) and signif-cant coronary artery disease who are undergoing percuta-eous coronary interventions not only have higher resteno-is rates, but also experience significantly more adverseardiac events.1–6 DM-specific angiographic baseline char-cteristics (i.e., smaller vessel dimensions, longer lesions),owever, are strong predictors of restenosis in patients withnd without DM.1,2,5,6 Furthermore, despite the initial as-umption that inferior angiographic and clinical results inhe patients with DM are mainly attributable to an exagger-ted neointimal proliferation,4 recent data have also sug-ested inferior procedural results in patients with DM.1,7 Tourther evaluate the mechanisms of acute lumen gain andestenosis in patients with DM compared with those withoutM, we performed a single-center matched-pair observa-
ional study.
ethodsPatients and procedures: A total of 160 patients with
M (62 � 8 years; 81% men) with 225 de novo lesions�50% diameter stenosis) in native coronary arteriesormed the study population. All patients had an indicationor percutaneous treatment (typical symptoms and/or posi-ive findings on a stress test), and stent implantation was
aMedical Clinic II, University of Schleswig-Holstein, Campus Lübeck,übeck; and bMedical Clinic I, RWTH University Hospital Aachen,achen, Germany. Manuscript received January 28, 2006; revised manu-
cript received May 31, 2006 and accepted June 5, 2006.*Corresponding author: Tel: 49-451-500-2421; fax: 49-451-500-2463.
wE-mail address: [email protected] (P.W. Radke)
002-9149/06/$ – see front matter © 2006 Elsevier Inc. All rights reserved.oi:10.1016/j.amjcard.2006.06.015
uccessfully performed in each lesion. Of these patients,33 (83%) with 192 lesions (85%) underwent control an-iography 5 � 2 months after intervention. DM treatmentncluded insulin therapy in 39 patients (29%), oral antidia-etic drug use in 68 patients (51%), and dietary measureslone in 26 patients (20%). DM was defined according tohe American Diabetes Association 1997 classification.8
The control group of patients without DM was recruitedrom a prospective registry of 993 patients with de novoesions in native coronary arteries who underwent success-ul stent implantation. The angiographic follow-up rate inhis group was 84% (834 patients). Only bare metal stentsere used. This database included all relevant demographic,
linical, and angiographic data. A group of 192 lesions (182atients) with angiographic follow-up data were matchedith the former DM group for lesion length (�1 mm),
eference diameter (�0.2 mm), and minimal luminal diam-ter (MLD) (�0.2 mm) in a pairwise fashion using a manualatching process that only included the matching variables.ll other clinical and angiographic variables were blindeduring the matching process. A comparison of the 2 patientroups is provided in Table 1.
In the 2 groups, heparin was administered during therocedure according to standard practice. Aspirin (100 mg/ay) and clopidogrel (300 mg loading dose) were startedefore the procedure. Stent implantation was performedccording to standard protocols. Direct stenting was left tohe operator’s discretion. After the procedure, in addition tospirin, clopidogrel (75 mg/day) was administered for 4
eeks. All patients gave written informed consent. Thewww.AJConline.org
ep
iaaaQpmefwnvoerlcsat
glSsibdnaldwdi
Meclpda
mutbsfap
R
orb(agw1Ta
TB
V
LAMWBHHLPCGGC
o
TQ
V
P
P
F
C
1219Coronary Artery Disease/Mechanisms of Restenosis in Diabetes
thical committee of the University Aachen approved therotocol.
In-hospital and six-month clinical outcomes: All clin-cal data were verified by independent hospital chart reviewnd source documentation. Procedural success was defineds a �30% final diameter stenosis (in-stent analysis) and thebsence of major clinical complications (in-hospital death,-wave myocardial infarction, or emergency coronary by-ass surgery). All patients were contacted at 30 days and 6onths after the procedure for any major adverse cardiac
vent, defined as death, myocardial infarction, or the needor target lesion revascularization. Myocardial infarctionas defined as the presence of typical symptoms accompa-ied by an increase of creatine kinase-MB or troponin Talues �99% percentile of the reference sample or theccurrence of new pathologic Q waves on a follow-uplectrocardiogram. To control for operator bias regardingeinterventions in the follow-up angiographic studies, targetesion reintervention was only performed when patientsomplained of recurrent symptoms and/or had positivetress findings in the territory supplied by the target lesionnd a �75% in-segment (or in-stent) diameter stenosis ofhe target lesion on follow-up angiography.
Quantitative coronary angiography: Quantitative an-iographic analysis was performed at an independent coreaboratory of the University Aachen using the CAAS IIystem (PieMedical, Maastricht, The Netherlands), as de-cribed previously.9 In brief, the quantitative measurementsncluded the reference diameter, lesion length, and MLDefore and after the procedure and at follow-up. A user-efined reference luminal diameter of an angiographicallyormal-appearing segment was chosen. After the procedurend at follow-up, the MLD was determined for the targetesion, defined as the in-stent segment plus the proximal andistal 5-mm edge segments, and for the stented segmentithout the adjacent edge segments. Acute gain wasefined as the change in MLD from before to after the
able 1aseline characteristics
ariable DM p Value
Yes No
esions (patients) 192 (133) 192 (182)ge (yrs) 62 � 8 60 � 10 0.03en 154 (80%) 160 (83%) 0.51eight (kg) 79.6 � 13.8 77.9 � 11.8 0.20
ody mass index (kg/m2) 27.5 � 3.7 26.1 � 3.2 �0.01yperlipidemia* 123 (64%) 111 (58%) 0.26ypertension† 146 (76%) 129 (67%) 0.07eft anterior descending location 84 (44%) 81 (42%) 0.84revious coronary angioplasty 39 (29%) 52 (27%) 0.16reatinine (mg/dl) 1.00 � 0.41 0.98 � 0.22 0.55lucose (mg/dl) 138 � 32 98 � 18 �0.01lycosylated hemoglobin Alc 7.4 � 1.4% 5.4 � 0.9% �0.01-peptide (ng/ml) 1.9 � 0.7 0.7 � 0.8 �0.01
* Hypercholesterolemia �160 mg/dl low-density lipoprotein cholesterolr on lipid-lowering medication.
† Blood pressure �140/90 mm Hg or on antihypertensive medication.
ntervention, late lumen loss was defined as the change in r
LD from just after the intervention to the follow-upxamination, and net lumen gain was defined as thehange in MLD from before the intervention to the fol-ow-up examination. In-stent restenosis was classified asreviously described.10 Restenosis was defined as �50%iameter stenosis within the target lesion at follow-upngiography.
Statistical analysis: Continuous data are presented asean � SD. Comparisons between groups were performed
sing the unpaired t test for continuous variables. Qualita-ive data are presented as frequencies, and comparisonsetween quantitative data were performed using chi-squaretatistics. Univariate and multivariate analyses were per-ormed to identify predictors for angiographic restenosisfter stent implantation in patients with and without DM. Avalue �0.05 was considered statistically significant.
esultsPatient and procedural characteristics: A comparison
f the 2 patient populations is provided in Table 1. As aesult of the matching process, the 2 groups were well-alanced regarding lesion length, vessel size, and MLDTable 2). Additional preprocedural angiographic variablesnd demographic data were also comparable between the 2roups (Tables 1 and 2). In the DM group, direct stentingas performed in 102 of 192 lesions (53%) compared with10 of 192 lesions (57%) in the control group (p � 0.46).he maximum implantation pressure in the patients withnd without DM was 14.1 � 1.5 and 12.3 � 1.5 atm,
able 2uantitative coronary angiography
ariable DM p Value
Yes(192 lesions)
No(192 lesions)
reprocedureRD (mm) 2.93 � 0.50 2.97 � 0.46 0.42MLD (mm) 1.01 � 0.50 1.06 � 0.51 0.33DS (%) 67 � 12 68 � 12 0.41Lesion length (mm) 13.3 � 5.0 13.9 � 4.8 0.23ostprocedureRD (mm) 2.93 � 0.47 2.97 � 0.44 0.39In-lesion MLD (mm) 2.21 � 0.54 2.25 � 0.42 0.41In-stent MLD (mm) 2.53 � 0.46 2.58 � 0.40 0.26ollow-upRD (mm) 2.88 � 0.48 2.95 � 0.43 0.13In-lesion MLD (mm) 1.72 � 0.65 1.85 � 0.60 0.04In-stent MLD (mm) 1.89 � 0.71 2.02 � 0.36 0.02In-lesion DS (%) 40 � 18 37 � 15 0.08In-stent DS (%) 34 � 8 31 � 12 0.04Binary restenosis rate (%) 25 14 �0.01hange in MLDIn-lesion acute gain (mm) 1.15 � 0.56 1.24 � 0.60 0.13In-stent acute gain (mm) 1.47 � 0.41 1.56 � 0.38 0.03In-lesion late loss (mm) 0.49 � 0.42 0.41 � 0.50 0.09In-stent late loss (mm) 0.64 � 0.42 0.55 � 0.36 0.02In-lesion net gain (mm) 0.66 � 0.62 0.83 � 0.67 0.01In-stent net gain (mm) 0.83 � 0.66 1.01 � 0.71 0.01
DS � diameter stenosis; RD � reference diameter.
espectively (p �0.01).
raggll0(ptgit
1aD(pnf(
dggialwMgmgld
es
D
Ilat(itDdeorh
TP
V
AAMBIS�HFCC
1220 The American Journal of Cardiology (www.AJConline.org)
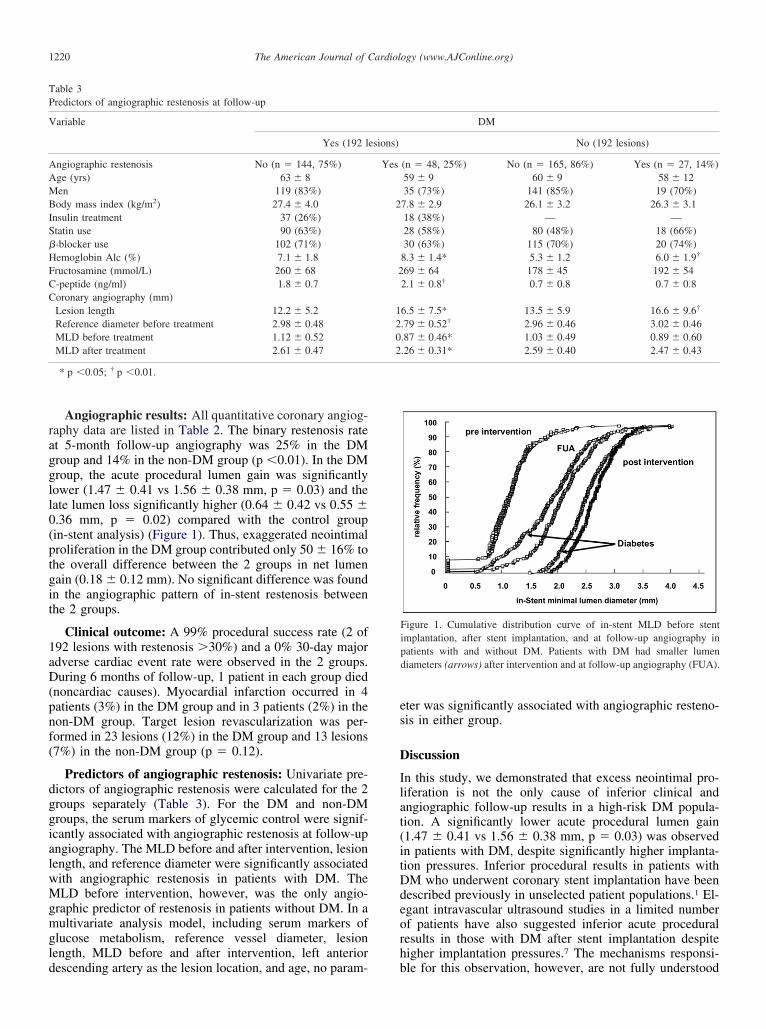
Angiographic results: All quantitative coronary angiog-aphy data are listed in Table 2. The binary restenosis ratet 5-month follow-up angiography was 25% in the DMroup and 14% in the non-DM group (p �0.01). In the DMroup, the acute procedural lumen gain was significantlyower (1.47 � 0.41 vs 1.56 � 0.38 mm, p � 0.03) and theate lumen loss significantly higher (0.64 � 0.42 vs 0.55 �.36 mm, p � 0.02) compared with the control groupin-stent analysis) (Figure 1). Thus, exaggerated neointimalroliferation in the DM group contributed only 50 � 16% tohe overall difference between the 2 groups in net lumenain (0.18 � 0.12 mm). No significant difference was foundn the angiographic pattern of in-stent restenosis betweenhe 2 groups.
Clinical outcome: A 99% procedural success rate (2 of92 lesions with restenosis �30%) and a 0% 30-day majordverse cardiac event rate were observed in the 2 groups.uring 6 months of follow-up, 1 patient in each group died
noncardiac causes). Myocardial infarction occurred in 4atients (3%) in the DM group and in 3 patients (2%) in theon-DM group. Target lesion revascularization was per-ormed in 23 lesions (12%) in the DM group and 13 lesions7%) in the non-DM group (p � 0.12).
Predictors of angiographic restenosis: Univariate pre-ictors of angiographic restenosis were calculated for the 2roups separately (Table 3). For the DM and non-DMroups, the serum markers of glycemic control were signif-cantly associated with angiographic restenosis at follow-upngiography. The MLD before and after intervention, lesionength, and reference diameter were significantly associatedith angiographic restenosis in patients with DM. TheLD before intervention, however, was the only angio-
raphic predictor of restenosis in patients without DM. In aultivariate analysis model, including serum markers of
lucose metabolism, reference vessel diameter, lesionength, MLD before and after intervention, left anterior
able 3redictors of angiographic restenosis at follow-up
ariable
Yes (192 l
ngiographic restenosis No (n � 144, 75%)ge (yrs) 63 � 8en 119 (83%)ody mass index (kg/m2) 27.4 � 4.0
nsulin treatment 37 (26%)tatin use 90 (63%)-blocker use 102 (71%)emoglobin Alc (%) 7.1 � 1.8ructosamine (mmol/L) 260 � 68-peptide (ng/ml) 1.8 � 0.7oronary angiography (mm)Lesion length 12.2 � 5.2Reference diameter before treatment 2.98 � 0.48MLD before treatment 1.12 � 0.52MLD after treatment 2.61 � 0.47
* p �0.05; † p �0.01.
escending artery as the lesion location, and age, no param- b
ter was significantly associated with angiographic resteno-is in either group.
iscussion
n this study, we demonstrated that excess neointimal pro-iferation is not the only cause of inferior clinical andngiographic follow-up results in a high-risk DM popula-ion. A significantly lower acute procedural lumen gain1.47 � 0.41 vs 1.56 � 0.38 mm, p � 0.03) was observedn patients with DM, despite significantly higher implanta-ion pressures. Inferior procedural results in patients withM who underwent coronary stent implantation have beenescribed previously in unselected patient populations.1 El-gant intravascular ultrasound studies in a limited numberf patients have also suggested inferior acute proceduralesults in those with DM after stent implantation despiteigher implantation pressures.7 The mechanisms responsi-
Figure 1. Cumulative distribution curve of in-stent MLD before stentimplantation, after stent implantation, and at follow-up angiography inpatients with and without DM. Patients with DM had smaller lumendiameters (arrows) after intervention and at follow-up angiography (FUA).
DM
No (192 lesions)
(n � 48, 25%) No (n � 165, 86%) Yes (n � 27, 14%)59 � 9 60 � 9 58 � 1235 (73%) 141 (85%) 19 (70%)
7.8 � 2.9 26.1 � 3.2 26.3 � 3.118 (38%) — —28 (58%) 80 (48%) 18 (66%)30 (63%) 115 (70%) 20 (74%)
8.3 � 1.4* 5.3 � 1.2 6.0 � 1.9†
69 � 64 178 � 45 192 � 542.1 � 0.8† 0.7 � 0.8 0.7 � 0.8
6.5 � 7.5* 13.5 � 5.9 16.6 � 9.6†
.79 � 0.52† 2.96 � 0.46 3.02 � 0.46
.87 � 0.46* 1.03 � 0.49 0.89 � 0.60
.26 � 0.31* 2.59 � 0.40 2.47 � 0.43
esions)
Yes
2
2
1202
le for this observation, however, are not fully understood

bweegotcdhp
tgtSDf0ollTosltru
s2gnfwawgtsdma
rtTrIttrDdLnpPht
tpitrfeetItpp
1
1
1
1
1
1
1221Coronary Artery Disease/Mechanisms of Restenosis in Diabetes
ut are likely related to structural alterations of the vesselall in patients with DM.11,12 Hyperglycemia causes non-
nzymatic glycosylation of proteins, including collagen andlastins (advanced glycosylation end products).13 Advancedlycosylation end products interact with matrix proteinsf the vessel wall, leading to protein cross-linking and,hereby, increasing the stiffness of the vessel wall.14 Clini-ally, the decreased distensibility of the vessel wall is wellocumented,14,15 and the operators in the present series usedigher implantation pressures in the patients with DM. Therocedural results, however, remained inferior.
Most importantly, this study allowed for calculation ofhe relative contribution of inferior procedural results (acuteain) and exaggerated neointimal proliferation (late loss) tohe significantly lower net lumen gain in patients with DM.urprisingly, the exaggerated neointimal proliferation in theM group contributed only 50 � 16% to the overall dif-
erence in net lumen gain between the 2 groups (0.18 �.12 mm). These data clearly suggest that operators need toptimize the procedural results in DM by using larger bal-oons and/or higher implantation pressures to improve theong-term outcomes after coronary stent implantation.his concept may be relevant even after the introductionf drug-eluting stents (DESs) into clinical practice, whichignificantly improved the angiographic and clinical fol-ow-up results in patients with DM.16,17 However, pa-ients with DM remain at high risk of restenosis, witheported restenosis rates of �24% in cases of long lesionssing DESs.18
Finally, a separate analysis of the predictors for resteno-is in patients with and without DM was performed. In the
patient groups, glycemic control (as assessed by hemo-lobin A1c levels) was significantly associated with reste-osis, as described previously for those with DM19 and evenor those without DM.20 These data suggest that patientsith a pre-DM metabolic state (i.e., insulin resistance) are
lready at a higher risk of developing restenosis. Patientsith DM on insulin treatment represent the highest riskroup in this context.1 This study showed a nonsignificantrend toward a higher restenosis rate in those patients. In-ulin per se is a growth factor, and preclinical studies haveemonstrated a significant effect of insulin and smoothuscle cell proliferation21; however, insulin treatment may
lso reflect the duration of the disease.The patients included in this analysis represented a low-
isk population regarding restenosis (elective stent implan-ation, “de novo” lesions, mean diameter 2.9 � 0.5 mm).he binary restenosis rate of 25% in the patients with DM
eflects the lower limit of previously published studies.2,22,23
n the low-risk BENESTENT studies (I and II), however,he restenosis rates in patients with DM differed from 21.4%o 27.3%.2 Lesion length was identified as a predictor ofestenosis in the 2 patient populations. Only in patients withM, however, were vessel size and the pre- and postproce-ural dimensions associated with restenosis in this analysis.arger patient populations using bare metal and DESs areeeded to further elucidate the differences in angiographicredictors of restenosis in patients with and without DM.atient age was not a predictor of restenosis in either group;owever, patients with restenosis tended to be younger in
he DM and non-DM groups.Only bare metal stents were used in this study. However,he principal finding that acute gain is significantly lower inatients with DM remains. Although neointimal proliferations reduced using DESs, the difference in neointimal prolifera-ion between patients with and without DM is also likely toemain. Because of a significantly lower level of neointimaormation using DESs, the relative importance of the differ-nce in acute gain may play an even greater role regarding theffectiveness of DESs in patients with and without DM. Fur-hermore, intravascular ultrasound was not used in this study.ntravascular ultrasound technology allows quantification ofhe lumen, as well as vessel dimensions and would clearly haverovided important data on the mechanisms of the inferiorrocedural results in patients with DM.
1. Schofer J, Schlüter M, Rau T, Hammer F, Haag N, Mathey DG.Influence of treatment modality on angiographic outcome after coro-nary stenting in diabetic patients: a controlled study. J Am Coll Cardiol2000;35:1554–1559.
2. West NE, Ruygrok PN, Disco CM, Webster MW, Lindeboom WK,O’Neill WW, Mercado NF, Serruys PW. Clinical and angiographicpredictors of restenosis after stent deployment in diabetic patients.Circulation 2004;109:867–873.
3. Mathew V, Gersh BJ, Williams BA, Laskey WK, Willerson JT, Til-bury RT, Davis BR, Holmes DR Jr. Outcomes in patients with diabetesmellitus undergoing percutaneous coronary interventions in the currentera. Circulation 2004;109:476–480.
4. Kornowski R, Mintz G, Kent KM, Pichard AD, Satler LF, Bucher TA,Popma JJ, Leon MB. Increased restenosis in diabetes mellitus aftercoronary interventions is due to exaggerated intimal hyperplasia: aserial intravascular ultrasound study. Circulation 1997;95:1366–1369.
5. Elezi S, Kastrati A, Pache J, Wehinger A, Hadamitzky M, DirschingerJ, Neumann FJ, Schomig A. Diabetes mellitus and the clinical andangiographic outcome after coronary stent placement. J Am Coll Car-diol 1998;33:1866–1873.
6. Elezi S, Kastrati A, Neumann FJ, Hadamitzky M, Dirschinger J,Schomig A. Vessel size and long-term outcome after coronary stentplacement. Circulation 1998;98:1875–1880.
7. Syeda B, Wexberg P, Gyongyosi M, Denk S, Beran G, Sperker W,Yahyam Glogar D. Mechanism of lumen gain during coronary stentdeployment in diabetic patients compared with non-diabetic patients.Coronary Artery Dis 2002;13:263–268.
8. The Expert Committee on the Diagnosis and Classification of DiabetesMellitus. Report of the Expert Committee on the diagnosis and clas-sification of diabetes mellitus. Diabetes Care 1997;20:1183–1197.
9. Radke PW, Kobella S, Kaiser A, Franke A, Schubert D, Grube E,Hanrath P, Hoffmann R. Treatment of in-stent restenosis using apaclitaxel eluting stent: acute results and long-term follow-up ofa matched comparison with intracoronary �-radiation therapy. EurHeart J 2004;25:920–925.
0. Mehran R, Dangas G, Abizaid AS, Mintz GS, Lansky AJ, Satler LF,Pichard AD, Kent KM, Stone GW, Leon MB. Angiographic patternsof in-stent restenosis: classification and implications for long-termout-come. Circulation 1999;100:1872–1878.
1. Rasmussen LM, Ledet T. Aortic collagen alterations in human diabetesmellitus: changes in basement membrane collagen content and in thesusceptibility of total to cyanogen bromide solubilisation. Diabetolo-gia 1993;36:445–453.
2. Mautner SL, Lin F, Roberts WC. Composition of atheroscleroticplaque in the epicardial coronary arteries in juvenile (type I) diabetesmellitus. Am J Cardiol 1992;70:1264–1268.
3. Brownlee M, Vlassara H, Cerami A. Nonenzymatic glycosylation andthe pathogenesis of diabetic complications. Ann Intern Med 1984;101:527–537.
4. Airaksinen KE, Salmela PI, Linnaluoto MK, Ikaheimo MJ, Ahola K,Ryhanen LJ. Diminished arterial elasticity in diabetes: association withfluorescent advanced glycosylation end products in collagen. Cardio-vasc Res 1993;27:942–945.
5. Christensen T, Neubauer B. Increased arterial wall stiffness and thick-
ness in medium-sized arteries in patients with insulin-dependent dia-betes mellitus. Acta Radiol 1988;29:299–302.
1
1
1
1
2
2
2
2
1222 The American Journal of Cardiology (www.AJConline.org)
6. Sabate M, Jimenez-Quevedo P, Angiolillo DJ, Gomez-Hospital JA,Alfonso F, Hernandez-Antolin R, Goicolea J, Banuelos C, Escaned J,Moreno R, Fernandez C, Fernandez-Aviles F, Macaya C, for theDIABETES Investigators. Randomized comparison of sirolimus-elutingstent versus standard stent for percutaneous coronary revascularization indiabetic patients: the diabetes and sirolimus-eluting stent (DIABETES)trial. Circulation 2005;112:2175–2183.
7. Hermiller JB, Raizner A, Cannon L, Gurbel PA, Kutcher MA, WongSC, Russell ME, Ellis SG, Mehran R, Stone GW, for the TAXUS-IVInvestigators. Outcomes with the polymer-based paclitaxel-elutingTAXUS stent in patients with diabetes mellitus: the TAXUS-IV trial.J Am Coll Cardiol 2005;45:1172–1179.
8. Popma JJ, Leon MB, Moses JW, Holmes DR, Cox R, Fitzpatrick M,Douglas J, Lambert C, Mooney M, Yakubov S, Kuntz RE, for theSIRIUS Investigators. Quantitative assessment of angiographic reste-nosis after sirolimus-eluting stent implantation in native coronary
arteries. Circulation 2004;110:3773–3780.9. Mazeika P, Prasad N, Bui S, Seidelin PH. Predictors of angiographicrestenosis after coronary intervention in patients with diabetes melli-tus. Am Heart J 2003;145:1013–1021.
0. Radke PW, Voswinkel M, Reith M, Kaiser A, Haager PK, Hanrath P,Hoffmann R. Relation of fasting insulin plasma levels to restenosisafter elective coronary stent implantation in patients without diabetesmellitus. Am J Cardiol 2004;93:639–641.
1. Aronson D, Bloomgarden Z, Rayfield EJ. Potential mechanisms promot-ing restenosis in diabetic patients. J Am Coll Cardiol 1996;27:528–535.
2. Van Belle E, Perie M, Braune D, Chmait A, Meurice T, Abolmaali K,McFadden EP, Bauters C, Lablanche JM, Bertrand ME. Effects ofcoronary stenting on vessel patency and long-term clinical outcomeafter percutaneous coronary revascularization in diabetic patients.J Am Coll Cardiol 2002;40:410–417.
3. Gilbert J, Raboud J, Zinman B. Meta-analysis of the effect of diabeteson restenosis rates among patients receiving coronary artery stenting.
Diabetes Care 2004;27:990–994.




























