Embed Size (px)
Citation preview

Comparative Pathology of Hepatitis AVirusand Hepatitis E Virus Infection
John M. Cullen1 and Stanley M. Lemon2
1Department of Population Health and Pathobiology, North Carolina State University College of VeterinaryMedicine, Raleigh, North Carolina 27607
2Lineberger Comprehensive Cancer Center, Departments of Medicine and Microbiology & Immunology,The University of North Carolina at Chapel Hill, Chapel Hill, North Carolina 27599-7030
Correspondence: [email protected]
Hepatitis Avirus (HAV) andhepatitis E virus (HEV) cause acute, self-limiting hepatic infectionsthat are usually spread by the fecal–oral route in humans. Naturally occurring andexperimental infections are possible in a variety of nonhuman primates and, in the case ofHEV, a number of other species. Many advances in understanding the pathogenesis of theseviruses have come from studies in experimental animals. In general, animals infected withthese viruses recapitulate the histologic lesions seen in infected humans, but typically withless severe clinical and histopathological manifestations. This review describes the histopath-ologic changes associated with HAV and HEV infection in humans and experimentalanimals.
Of the five hepatotropic human virusesclassically associated with hepatitis in hu-
mans, hepatitis A virus (HAV) and hepatitis Evirus (HEV) are distinguished by being pre-dominantly transmitted by the fecal–oral routeand by rarely causing chronic liver injury as-sociated with persistent infection. Progressiveliver disease associated with persistent infec-tion has never been documented with HAV,and only recently have long-lasting infectionswith HEV been recognized in immunocom-promised persons (Kamar et al. 2011). Thus,both viruses cause primarily acute, self-limit-ing liver injury. Fulminant infections associat-ed with massive hepatocellular necrosis canoccur with either virus, and prolonged chole-stasis is a well-recognized complication ofHAV
infection (Taylor et al. 2006; Jung et al. 2010;Agrawal et al. 2012), but typically there is littleneed for invasive diagnostic measures includingbiopsy of the liver. Thus, primary humanmaterial is rarely available for histopathologicexamination. On the other hand, infectionswith either virus, both naturally acquired andexperimental, are possible in multiple speciesof nonhuman primates (see Li and Wakita2018) and, to a lesser extent, smaller mammals.Most of what we know of the pathogenesis ofHAV and HEV comes from studies in experi-mental animals. In general, animals infectedwith these viruses recapitulate the histologic le-sions seen in infected humans, albeit typicallywith less severe clinical and histopathologicalmanifestations.
Editors: Stanley M. Lemon and Christopher WalkerAdditional Perspectives on Enteric Hepatitis Viruses available at www.perspectivesinmedicine.org
Copyright © 2018 Cold Spring Harbor Laboratory Press; all rights reservedAdvanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a033456
1
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org

HEPATITIS AVIRUS
HAV infection results in hepatic inflammationthat is most often self-limiting. Clinically, how-ever, there is a broad range of possible outcomesfollowing infection (see Shin and Jeong 2018).Liver disease is generally considered to be rela-tively mild and often asymptomatic in veryyoung children (Benenson et al. 1980). Liverinjury is more significant in adults in whomjaundice is more likely. Fulminant hepatitis oc-curs in ∼0.5% of infected persons, and the casefatality rate is ∼0.2% (Jung et al. 2010). HAVantigen has been detected in organs other thanthe liver, but no associated inflammation hasbeen reported.
HAV is highly conserved antigenically, andonly a single serotype exists. However, sevenHAV genotypes have been identified: four geno-types (I, II, III, and VII) are of human origin andthe other three (IV, V, VI) are of nonhuman pri-mate origin (see Smith and Simmonds 2018).The primate viruses are similar to human HAV,although they are genetically heterogeneous(Lemon et al. 1987). Naturally occurring HAVinfection occurs in nonhuman primates, includ-ing the great apes (chimpanzee), Old Worldmacaques (cynomolgus and stump-tailed ma-caques), baboons, and the African vervet mon-key, as well as NewWorld species (owl monkeys,marmosets, and tamarins) (Dienstag et al. 1976;Coursaget et al. 1981; Lemon et al. 1982; Burkeand Heisey 1984; Balayan 1992; Bennett et al.2016). Experimental infections have been pro-duced by either oral or intravenous inoculationin all of these species, except baboons. Clinicallyevident disease is usually not apparent in theseanimals, although fulminant hepatitis A hasbeen reported in a chimpanzee (Abe and Shikata1982). In addition to nonhuman primates, natu-rally occurring infections with closely relatedhepatoviruses have recently been discoveredin bats, rodents, seals, shrews, and hedgehogs(Drexler et al. 2015; Siebert et al. 2017; see Sanderet al. 2018). However, detailed descriptions ofhepatic histopathology are lacking in these othermammals. Some evidence suggests that guineapigs are permissive for infection with HAV, butthey do not develop disease (Hornei et al. 2001).
In contrast, genetically modified mice with spe-cific deficits in type 1 interferon signaling sup-port robust replication of the virus and sometypes of genetic knockouts develop severe he-patic inflammation (Hirai-Yuki et al. 2016).
Histopathology of Acute Hepatitis Ain Humans
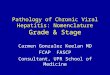
Acute type A viral hepatitis has a typical histo-logic appearance in humans (Teixeira et al.1982). HAV appears to be noncytopathic invivo, as it generally is in cell culture. The earlieststages of infection are attended by little histolog-ic response, although variation in the stainingquality of hepatocytes can be seen. Once hostimmune responses are initiated, the affected liv-er is characterized by a combination of inflam-matory cell infiltration with macrophages andendothelial cell activation, and injury to or ne-crosis of hepatocytes. Typical histologic featuresinclude hepatocellular ballooning: a swelling ofviable hepatocytes up to twice the normal diam-eter, with clearing of the cytoplasm and varia-tion in the size and shape of both nuclei andcytoplasm (Fig. 1A). These changes are accen-tuated in the centrilobular region of the liverparenchyma. Hepatocyte swelling, apoptoticdeath, and necrosis of hepatocytes leads to adisordered arrangement of the hepatic platesreferred to as lobular disarray (Fig. 1A).
Hepatic inflammation generally peaks coin-cident withmaximal serum alanine aminotrans-ferase (ALT) elevation. The inflammatory cellpopulation consists of lymphocytes primarily.However, plasma cells can be abundant in theinflamed HAV-infected liver, leading to somehistologic overlap with autoimmune hepatitis.This distinguishes hepatitis A from other typesof acute viral hepatitis in which plasma cells areless common in the inflammatory infiltrate.There is also a tendency for greater inflamma-tory involvement of the periportal region thanwith other viruses. Portal inflammation may ex-tend beyond the margins of the portal tract intothe adjacent parenchyma causing hepatocyte in-jury, a process termed piecemeal necrosis (Fig.1B,C). This typically involves <25% of the cir-cumference of the portal tract, but the presence
J.M. Cullen and S.M. Lemon
2 Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a033456
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org

of piecemeal necrosis can suggest a diagnosis ofother forms of hepatitis (Abe et al. 1982; Krygerand Christoffersen 1983).
Individual affected hepatocytes may bedeeply eosinophilic in hematoxylin and eosin(H&E)-stained sections, often with condensed,deeply basophilic nuclear remnants. The mor-
phologic appearance of such dying cells, whichare referred to as acidophilic bodies or Council-man bodies in the older literature (after theAmerican pathologist, William Councilman),is suggestive of an apoptotic death. Such cellsare typically found within the parenchyma ad-jacent to lymphocytes. Fragments of apoptotic
bdbd
artpv
c
b
a
d
B
A
C
d
cbd
bd
Figure 1. Section of liver from a human patient with acute hepatitis A stained with hematoxylin and eosin (H&E).(A) The normal arrangement of the hepatic plates is disordered by hepatocyte swelling and parenchymalinflammatory infiltrates causing lobular disarray. Affected hepatocytes (a) are swollen and the cytoplasm has alacy appearance. Clusters of plasma cells (b) are present within the parenchyma. (B) A portal tract inflammatoryinfiltrate consisting of lymphocytes and macrophages extends through the limiting plate and is associated withinjured hepatocytes (c), resulting in piecemeal necrosis. (C) Piecemeal necrosis (c) associated with adjacentremnants of necrotic or apoptotic hepatocytes. Scale bars, 50 µm. bd, bile ducts; pv, portal vein; art, hepatic arterybranch; d, apoptotic hepatocyte.
Comparative Pathology of HAV and HEV Infections
Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a033456 3
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org

hepatocytes can be extruded into the sinusoidsand phagocytosed byKupffer cells, liver residentmacrophages. Edema can enlarge the outline ofthe portal tracts, and reticulin stains can revealexpansion of the portal tract connective tissuewith focal areas of hepatocyte loss. The Kupffercells are typically reactive, characterized by hy-perplasia and hypertrophy. The cytoplasm is ex-panded and often contains glycogen or otherpolysaccharides staining with Periodic AcidSchiff (PAS) stain and/or hemosiderin (Fig. 2A).
In some cases, the major lesion within theliver is perivenular injury. Cholestasis also oc-curs. It is marked histologically by the formation
of bile plugs (Fig. 2B), typically most evident inthe centrilobular canaliculi, and can vary fromminimal to marked. Cholestasis may be dispro-portionate to the degree of hepatocellular injury,and occasionally persists for weeks followingpeak enzyme elevation (Gordon et al. 1984). Fi-brosis is not a feature of the pathology caused bythe acute nature of the infection.
The relative proportion of each of these fea-tures may vary with the magnitude of the inoc-ulum size, age of the infected individual, as wellas the duration of infection and individualvariation in the host inflammatory response.Genetic variation in the virulence of different
a
A
C
B
b
ro
ro
Figure 2. Acute hepatitis A in a human. Staining with hematoxylin and eosin (H&E). (A) Aggregates of pig-mented macrophages (a) within the parenchyma are a common feature of hepatitis A virus (HAV) infection.Scale bar, 50 µm. (B) Cholestasis (b) is often evidentwithin canaliculi of the centrilobular region. Scale bar, 12.5 µm.(C) Rosette formation (ro) caused by hepatocytes arranged around a dilated canaliculusmayoccurwhen cholestasisis prominent. Scale bar, 50 µm.
J.M. Cullen and S.M. Lemon
4 Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a033456
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org

HAV strains has been suggested, but it is not welldocumented (Fujiwara et al. 2002). In aminorityof patients, regions of necrosis can bridge portaltracts or form connections to central regions.Necrosis that affects entire lobules is termed“massive necrosis” with “submassive necrosis,”describing necrosis affecting only portions ofthe lobule. Hepatocellular necrosis is often ac-companied by a prominent periportal prolifer-ation of bipotential precursor cells capable offorming biliary ducts or hepatocytes (Fig. 2C).These small basophilic cells form cords or smallductules in a process called a ductular reaction.With sufficient loss of viable parenchyma, ful-minant hepatic failure and death may ensue,although this is quite uncommon.
During recovery, thickened hepatic platestwo cells across and multinucleate hepatocytesmay be present. Kupffer cell activation oftenpersists. Hepatocellular mitoses become morecommon.
Histopathology of HAV Infection in theChimpanzee
Chimpanzees (Pan troglodytes) were the firstnonhuman primates shown to develop hepatitisfollowing inoculation with HAV (Deinhardtet al. 1962; see Li and Wakita 2018). Histologiclesions tend to recapitulate those seen in infect-ed humans, although there is a tendency for thechimpanzees to be less severely affected thanadult humans (Dienstag et al. 1975; Maynard1975; Maynard et al. 1975; Popper et al. 1980).Age-related effects, however, may be involved asinfected human infants tend to have mildersymptoms than adults, and many of the chim-panzees that have been studied are relativelyyoung. Despite the tendency to have milder dis-ease than humans, fulminant hepatitis has beendescribed in an HAV-infected chimpanzee (Abeand Shikata 1982; Theamboonlers et al. 2012).
The most thorough characterization of thehistopathology of the liver in HAV-infectedchimpanzees was reported by Popper et al. in1980 (Popper et al. 1980). The initial alteration,coincidentwith elevations of serumaminotrans-ferase activities, was observed 1 to 5 weeks fol-lowing oral or percutaneous inoculation of the
virus and consisted of focal necrosis (Fig. 3B).Hepatocellular alterations developed mainly inthe periportal region. Periportal infiltrates con-sisted primarily of lymphocytes and macro-phages containing PAS-positive, diastase-resistantmaterial. Necrotic hepatocytes were intermixedwith the periportal inflammatory infiltrate (Fig.3B). Lymphocytes andmacrophages were aggre-gated in the portal tracts alongwith considerablenumbers of plasma cells.
At a later stage in the infection, there waspiecemeal necrosis, characterized by disruptionof the limiting plate of the portal tract (Fig. 3B),adjacent hepatocellular necrosis, and a prolifer-ation of bile ductules. In some cases, bridgingportal-to-portal necrosis was present. Portaltracts were conspicuously expanded, and broadbands of inflammatory infiltrates appeared tobridge adjacent portal tracts. At the time ofmax-imal inflammation (Fig. 3C), foci of necrotic/apoptotic cells were evident throughout muchof the parenchyma, although the centrilobularzone was usually unaffected. Apoptotic bodieswere present within the sinusoids and betweenintact hepatocytes. Cellular infiltration was par-ticularly dense around bile ducts, sometimes in-volving the duct wall, although the epitheliumremained intact. The frequency of hepatocellu-lar mitoses was increased, but the number ofmultinuclear giant cells remained relativelyconstant. Also, scattered mononuclear inflam-matory cells were noted in the wall of large trib-utaries of the hepatic veins.
Over the ensuing 6 to 8 weeks, the intralob-ular inflammation and apoptosis was seen torecede (Fig. 3D). The portal inflammation be-came less conspicuous, but hemosiderin-con-taining macrophages remained numerous. Se-rum enzyme levels returned to normal beforethe resolution of the histologic lesions.
HAV Infection in Cynomolgus Macaques
Cynomolgus macaques (Macaca fasicularis)have been found to be naturally infected withHAV (Burke and Heisey 1984). While closelyrelated, the virus recovered from cynomolgusmacques appears to be specific to these primatesas it differs genetically from human HAV and is
Comparative Pathology of HAV and HEV Infections
Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a033456 5
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org

classified in a distinct genotype (Nainan et al.1991; see Smith and Simmonds 2018). Cyno-molgus macaques are also susceptible to infec-tion with human HAV (Shevtsova et al. 1988;Amado et al. 2010), and the histopathology ofthe liver following intravenous inoculation witha human HAV isolate (HAF-203) has been de-scribed (Amado et al. 2010). Initially, swelling ofhepatocytes and microvesicular steatosis wereevident by day 7 postinoculation. The highestlevel of fecal shedding of HAV occurred 15days after inoculation and was accompanied bythe first evidence of hepatic inflammation andserum ALT elevations. This sequence is verysimilar towhat has been observed in experimen-tally infected chimpanzees (Lanford et al. 2011).Scattered apoptotic hepatocytes were present atday 17 postinfection, as were typical balloonedhepatocytes and reactive Kupffer cells. The por-tal tracts were maximally infiltrated by lympho-cytes and other mononuclear cells, causing ex-pansion of the portal tracts at around 20–45 dayspostinfection when ALT levels weremost elevat-ed. Multinucleate hepatocytes were evident assoon as 7 days postinfection and again in biop-sies at 30 days postinfection. Infected animals
were not clinically ill at any point following in-fection. No significant hepatic lesions were ob-served in a single control animal.
As mentioned above, autochthonouslytransmitted nonhuman primate viruses are ge-netically distinct from human isolates, and thismay affect their pathogenicity (Emerson et al.1991; Tsarev et al. 1991).
Old World primates, other than cynomol-gus macaques, may not be good models of hu-man HAV infection as they generally developlittle or no evidence of liver injury when infectedwith human strains of HAV (see Li and Wakita2018). Rhesus macaques and stump-tailed ma-caques (Macaca arctoides) developed hepatitiswhen infected with nonhuman primate-derivedvirus, but not human-derived HAV (And-zhaparidze et al. 1987). In another study, stump-tailed macaques developed enzyme elevationsfollowing infection with a human-derived virus,but no histologywas described (Mao et al. 1981).Similarly, an HAV isolate from African greenmonkeys (AGM-27) was shown to cause diseasein New World tamarins (Saguinas mystax) andsome Old World primates (African green mon-key [Chlorocebus sp.] andcynomolgusmacaques
a
b
A B C D
b
Figure 3. Sequential liver biopsies taken from an acutely infected adult chimpanzee (Pan troglodytes) inoculatedintravenously with HM175 virus. Staining with hematoxylin and eosin (H&E). (A) Pre-infection; alanineaminotransferase (ALT) = 25 IU/L. There is modest periportal inflammation (a) with hemosiderin-laden mac-rophages. (B) 3 weeks postinoculation; ALT = 319 IU/L. Periportal inflammatory infiltrates are significantlyincreased and extend into the parenchyma, representing early piecemeal necrosis (b) with a prominent apopto-tic/necrotic hepatocyte bordered by inflammatory cells. The hepatic plates are moderately disorganized. (C) 4weeks postinoculation; ALT = 392 IU/L (peak value). There is more prominent inflammation extending into theparenchyma with diffuse moderate-to-severe hepatocellular swelling and a binucleate hepatocyte. There ismarked lobular disarray with disorganized hepatic cords. (D) 10 weeks postinoculation; ALT = 35. Inflammatoryinfiltrates are reduced and the normal architecture of the hepatic plates has been restored. (Images from Lanfordet al. 2011; reproduced, with permission, from The National Academy of Sciences © 2011.)
J.M. Cullen and S.M. Lemon
6 Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a033456
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org

[M. fasicularis]), but not in chimpanzees (Em-erson et al. 1991).
New World Primates: Owl Monkeys
Owl monkeys (Aotus trivirgatus) were recog-nized to be susceptible to infection with HAVfollowing the discovery of extensive transmis-sion of virus (PA-21 strain) among newly cap-tured animals held within a primate colony inPanama (Lemon et al. 1982). Subsequent studiesshowed that infection can be achieved experi-mentally by either oral or intravenous inocula-tion of virus. The course of infection and theseverity of hepatitis varies between studies andindividual animals (Keenan et al. 1984; Asheret al. 1995). A study of the natural history ofexperimental infection via the intravenous routeshowed viral shedding in feces within 4 days,with fecal shedding peaking just before bio-chemical evidence of liver inflammation (Le-mon 1994).
In a hallmark study of orally infected owlmonkeys by Asher et al. (1995), histologic ab-normalities were described in liver tissue fromanimals necropsied 4 or 24 hours after infection.The changes described included increased eo-sinophilic cytoplasmic staining in centrilobularhepatocytes, pyknotic nuclei, and individualiza-tion of hepatocytes surrounding the terminalhepatic venules. An important caveat, however,is that these animals were not biopsied beforeinfection for comparison. At 3 days, diffuseswelling of hepatocytes was present throughoutthe hepatic lobules with clusters of polymorpho-nuclear leucocytes in sinusoids. Neutrophils of-ten bordered ballooned hepatocytes. Only a fewneutrophils were present in sinusoidal spaces at5 days and only a few hepatocytes had increasedcytoplasmic eosinophilia. At 7 days, in additionto occasional neutrophils in sinusoids, diffusefatty changes were seen in hepatocytes. Twoweeks postinoculation, changes in the liverwere similar to those found in an animal ne-cropsied 3 days after inoculation: hepatocytesagain showed diffuse ballooning with clear cy-toplasm andnumerous clusters of neutrophils inthe lobules. Neutrophils were the only inflam-matory cells seen at that time; they were not
numerous and were distributed randomlythroughout the lobules although the centrilobu-lar regions were spared. The accumulation ofiron in Kupffer cells and portal macrophagesas well as in macrophages of spleens and lymphnodes was first noted. Portal inflammation andhepatocellular necrosis (Fig. 4A) were observedin these orally infected owl monkeys 3 weeksinto the infection, when infectious virus was re-covered in cell cultures inoculated with serum,fecal extracts, and throat washings (Asher et al.1995). At that time, hepatocytes had diffuseaccumulations of microvesicular fat in the cyto-plasm and enlarged pale nuclei. Occasionalapoptotic hepatocytes, not accompanied byinflammatory cells, were also present in the lob-ules. Portal inflammation was mild and consist-ed mostly of lymphocytes and enlarged mac-rophages that were filled with hemosiderin. By4 weeks after infection, the portal tracts wereexpanded by an influx of inflammatory cells(Fig. 4B), most of which were lymphocytes,and macrophages surrounding bile ducts. Sub-sequently, inflammation involved all portal ar-eas and extended across the limiting plates intothe lobules. Piecemeal necrosis, characterized bydamage to the limiting plate and apoptotic he-patocytes (acidophilic bodies), was evident. By 8weeks after inoculation, inflammatory infiltratescomprised of small lymphocytes, plasma cells,and macrophages were still extensive but con-fined to portal areas without signs of hepatocel-lular necrosis. Over the course of the infection,the amount of iron in Kupffer cells increased,and was accompanied by hypertrophy and pro-liferation of these cells (Asher et al. 1995).
In a second study by Keenan et al. (1984),liver biopsies were obtained between 16 and 24days postintravenous inoculation of two differ-ent strains of HAV: PA-21 (gtIII), which was re-covered from owl monkeys in Panama (Lemonet al. 1982), and HM175 virus (genotype [gt]I),recovered from an infected human in Australia(see Lemon and Walker 2018). Histopathologicchanges were variable but, generally similar tothose in the orally infected animals in the Asherstudy, were present in both. However, there wasno evidence of inflammation in the region of theterminal hepatic venules. Hepatic lipidosis was
Comparative Pathology of HAV and HEV Infections
Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a033456 7
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org

not evident and there were fewer neutrophilsseen. By 28–35 days postinoculation, liver en-zymes had returned close to baseline and mostlesions were diminished in severity, althoughsome mild residual inflammation persisted inportal tracts in several animals. Cholestasis wasnot evident histologically (nor in the Asherstudy above), and there was no difference inthe clinical course or hepatic histopathology ofanimals infected with HAV from these two ge-notypes.
Viral antigen was detected by staining withmonoclonal anti-HAV antibodies in epithelialcells of intestinal crypts and in the lamina pro-pria of the ileum in owl monkeys following oralchallenge, but inflammation was not observed(Asher et al. 1995). These microscopic findingsrepresent the best evidence available that HAV iscapable of infecting cells within the gastrointes-tinal tract. Careful efforts were made to confirm
the specificity of the staining. Virus was alsoisolated in cell culture from jejunum, ileum,and colonic tissue, but could also be isolatedfrom intestinal contents. However, similar stud-ies performed in tamarins (Saguinus mystax; seeLi and Wakita 2018) failed to find any evidenceof HAV antigen within intestinal tissues (Ma-thiesen et al. 1980).
New World Primates: Marmosetsand Tamarins
Marmosets (Callithrix sp.) were among the firstspecies to be confirmed to support transmissionof HAV and were extensively used in early stud-ies of hepatitis A pathogenesis (Deinhardt et al.1967; Holmes et al. 1969). At least three speciesof marmosets are susceptible to infection, in-cluding S. mystax, Saguinas labiatus, and otherspecies in this genus, as well asCallithrix jacchus
pv
b
b
A B
C D
cv
bd
bd
bd
a
c
Figure 4.Acute hepatitis A in a NewWorld owlmonkey (Aotus trivirgatus). Staining with hematoxylin and eosin(H&E). (A) Portal tracts are infiltrated with lymphocytes and macrophages primarily. There is no piecemealnecrosis and no derangement of the lobular architecture. Scale bar, 100 µm. bd, bile duct; pv, portal vein; cv,central vein. (B) Inflammation within the parenchyma is characterized by scattered lymphocyte aggregates (a) andaccompanied by modest lobular disarray. Ballooning degeneration (b) of hepatocytes is also evident. (C) Bal-looning degeneration (b) of hepatocytes generally occurs early in hepatitis Avirus infection in owl monkeys. (D)Kupffer cell aggregates (c) may form in the later stages of hepatitis A infection, with or without iron, as seen here.
J.M. Cullen and S.M. Lemon
8 Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a033456
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org

(Deinhardt et al. 1975; Ebert et al. 1978; Baptistaet al. 1993). Following either oral or intravenousinoculation, the activities of liver enzymes (iso-citrate dehydrogenase [ICD]) become increasedin the serum, histologic evidence of hepatic in-jury is evident and, with time, anti-HAV anti-bodies develop.Hepatic inflammation can occuras soon as 11 days following infection, and typ-ically peaks at ∼4–6 weeks following infection(Ebert et al. 1978). The timing and extent ofenzyme increases and hepatic inflammationvary with the inoculum, and especially its infec-tious titer. In early studies, fecal shedding ofvirus was reported to persist in the face of en-zyme elevation (Bradley et al. 1977; Ebert et al.1978). This differs from what has been observedwith chimpanzees and owl monkeys, in whichfecal shedding typically is diminished with theonset of hepatic inflammation. However, theseearly studies predate the availability of quanti-tative polymerase chain reaction (PCR)-basedmethods for assessing viral shedding.
HAV-infected marmosets show histologicchanges that closely resemble those seen in in-fected human patients (Deinhardt et al. 1975).Initial histologic changes occur before enzymeelevations are evident and include an increase inthe number and reactivity of sinusoidal liningcells, as well as scattered foci of individual hepa-tocyte necrosis and inflammatory infiltrates ofthe portal tracts. When enzyme elevations are attheir peak, hepatocytes become heterogeneouswith regard to staining qualities of the cytoplasmand nuclei. Most often, altered hepatocytes havea densely eosinophilic cytoplasm or patches ofdense eosinophilia. Dense areas do not stainwith PAS, indicating that there is a low glycogencontent in these areas, but the PAS stain doesaccentuate the differences between hepatocytescaused by differences in glycogen content. Bal-looned hepatocytes are present, characterized byexpansion of the hepatocyte surface area in sec-tions with diaphanous cytoplasm and clear, ir-regular vacuoles typical of glycogen. There arenumerous infiltrates of lymphocytes andmacro-phages in the parenchyma, with scattered foci ofhepatocellular necrosis and isolated acidophilic(apoptotic) hepatocytes. Regions of hepatocel-lular necrosis and inflammation can be large.
There may be inflammation of the connectivetissue of the central veins, with thickening ofthe vein wall and activation of endothelial cells.Kupffer cells becomemore prominent and oftencontain PAS-positive, diastase-resistant non-glycogenic material. Aggregates of these liningcells can form in the sinuosids.
Most strikingly, portal tract inflammation isprominent and diffuse, with inflammatory infil-trates consisting of lymphocytes, plasma cells,macrophages, and smaller numbers of neutro-phils. Damage to the hepatocytes forming thelimiting plate (piecemeal necrosis) can be evi-dent (Deinhardt et al. 1975; Baptista et al. 1993).Plasma cells can be prominent, which is a char-acteristic feature of inflammation within theHAV-infected human liver. Proliferation ofsmall-caliber bile ductules also occurs. Histolog-ic lesions may persist in the liver despite thereturn of enzymes to the normal range (Dein-hardt et al. 1967). In the cotton-topped mar-moset (C. jacchus), there may be inflammationwithout significant enzyme elevations (Baptistaet al. 1993).
Tamarins (Saguinus sp.), closely related tomarmosets are also susceptible to infection withHAV (Karayiannis et al. 1986). Elevated serumliver enzyme activities and hepatic inflamma-tion similar to that seen in marmosets havebeen described following experimental infection(Karayiannis et al. 1990).
Rodent Models: Guinea Pigs
Infectious HAV challenge of guinea pigs doesnot result in clinical evidence of infection orelevation of liver-related enzyme activities in se-rum, although HAV was detected in serum andfeces by reverse transcription PCR (RT-PCR) orcell culture isolation for several weeks followinginoculation of virus adapted to growth in guineapig cell culture (Hornei et al. 2001). Hepatocyteswelling and rounding with cytoplasmic pallorwas described. A proportion of hepatocyteshad a deeply acidophilic cytoplasm and irregu-lar outlines with evidence of nuclear pyknosis.Inflammatory cells, mainly lymphocytes, plas-ma cells, and macrophages in varying pro-portions were most abundant in regions with
Comparative Pathology of HAV and HEV Infections
Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a033456 9
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org

hepatocellular damage. Inflammatory cells, pri-marily lymphocytes, were observed surroundingindividual hepatocytes, andmultinucleate hepa-tocytes and activated Kupffer cells (commonfeatures of HAV infection in other species)were present. In this study, however, a controlanimal kept in the same room as the infectedanimals also developed confluent necrosis ofthe liver, raising some concern about the under-lying cause of liver injury in animals challengedwith HAV. The findings suggest that guinea pigsmight be able to support limited HAV replica-tion, but hepatic histopathology is not reflectiveof that seen in infected humans or nonhumanprimates.
Genetically Modified Mice
Whereas normal mice are not susceptible to in-fection with HAV, amodel of human hepatitis A
has been described recently in knockout micelacking expression of the type 1 interferon re-ceptor (Ifnar1−/− mice) (Hirai-Yuki et al. 2016,2018). Similar to primates, HAV replicates ro-bustly in a highly hepatotropic fashion in thesegenetic knockouts, leading to viremia, fecalshedding of virus via the biliary tract, serumALT elevations, and impressive inflammatorychanges in the liver (Fig. 5). The histopathologyof infectedmice is characterized bymultiple fociof apoptotic hepatocytes surrounded by smallaggregates of lymphocytes and macrophages(Fig. 5A). In Ifnar1−/− mice challenged intra-venously with high titer virus, the normalliver architecture may be completely destroyed,with large, confluent areas of inflammation.F4/80+CD11B+ macrophages and CD3−NK1.1+
natural killer (NK) cells are sharply increasedin number, and both CD4+ and CD8+ CD3+
T lymphocytes are found in infiltrates. Remark-
a
a
a
a
A B
C
b
b
a
a
a
Figure 5.Hepatitis A in genetically deficient Ifnar1−/−mice that lack expression of the type I interferon (IFN)a/breceptor. Mice were inoculated intravenously with mouse-passaged HM175 virus (Hirai-Yuki et al. 2016). (A)Hematoxylin and eosin (H&E)-stained liver 28 days after inoculation of a 9-week-old female mouse. Serumalanine aminotransferase (ALT) was 57 IU/L, down from 474 IU/L on day 7 postinoculation (upper limits ofnormal = 30.2 IU/L). Scale bar, 50 µm. Inflammatory infiltrates comprised of foci of lymphocytes and macro-phages are scattered throughout the parenchyma, in most cases surrounding remnants of apoptotic hepatocytes(a). Portal inflammation is not evident. (B) Liver collected 41 days after intravenous inoculation of a femaleIfnar1−/−Ifngr1−/− double-knockout mouse with third mouse-passage virus; ALT was 201 IU/L. An inflamma-tory focus is associated with numerous apoptotic hepatocytes (a). Scale bar, 20 µm. (C) Liver from a maleIfnar1−/− mouse collected at necropsy 161 days after inoculation with fifth mouse-passage virus at 9 weeks ofage; ALTwas 100 IU/L after peaking at 414 IU/L on day 7. Extensive parenchymal infiltrates surround numerousapoptotic hepatocytes (b). Scale bar, 100 µm.
J.M. Cullen and S.M. Lemon
10 Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a033456
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org

ably, however, there is little to no inflammationof portal tracts distinguishing the inflammatorypicture observed in these mice from that in ex-perimentally infected nonhuman primates. Thisis likely reflective of the immunodeficient stateof these animals. Appreciable amounts of viralRNA are present in the spleens of these miceduring the peak stages of the infection, but thereare no changes in the histology of the spleen.
Other murine genetic knockouts are alsosusceptible to HAV infection, including micelacking expression of mitochondrial antiviralsignaling protein (Mavs−/− mice) and inter-feron regulatory factors (Irf3−/−Irf7−/− double-knockout mice). However, these knockouts donot develop any evidence of hepatic inflamma-tion when infected with HAV, despite the virusreplicating as well if not better than in Ifnar1−/−
mice (Hirai-Yuki et al. 2016, 2018). These dif-ferences, coupled with evidence for IRF3 activa-tion in the livers of infected Ifnar1−/− mice,suggest that hepatic inflammation arises fromintrinsic hepatocellular apoptosis caused byMAVS- and IRF3-dependent (but interferon-independent) induction of proapoptotic inter-feron-stimulated genes (ISGs).Micewith specif-ic defects in adaptive immunity (NSG andRag1−/−mice) were nonpermissive for HAV in-fection, and prior depletion of T cells, NK/NK Tcells, or macrophages had no impact on the de-velopment of inflammation in Ifnar1−/− mice(Hirai-Yuki et al. 2016).
HEPATITIS E VIRUS
There are four HEV genotypes that have distinctregional distributions and different host speciesrange (see Smith and Simmonds 2018). gtI andgtII have caused large epidemics of hepatitis indeveloping countries, whereas gtIII and gtIV in-fect both a variety of animals as well as humansand cause sporadic outbreaks of hepatitis.UnlikeHAV, HEV infections in humans often have azoonotic origin. The virus is transmitted via thefecal–oral route through consumption of con-taminated water or by ingestion of undercookedmeats, especially pork, but also wild boar andvenison (Matsuda et al. 2003; Malcolm et al.2007). Infection is generally acute and self-limit-
ing, but unlike HAV can persist in persons whoare immunocompromised (Kamar et al. 2011).The clinical course of acute infection can varyfrom the common mild form of the disease to afatal, fulminant hepatitis, which is particularlycommon in pregnant women (Rein et al. 2012).There is an increasing number of animal speciesknown to be naturally infected with HEV. Theseinclude domestic and wild pigs, deer, rabbits,rats, chickens, moose, mongoose, ferrets, bats,and trout. Serologic evidence of infection extendstorhesusandcynomolgusmacaques,goats, sheep,and cattle (Kabrane-Lazizi et al. 1999; Yugo et al.2014). Cross-species susceptibility and zoonotictransmission have been shown (Yugo et al. 2014).
Histopathology of HEV Infection in Humans
There is less information available concerningthe histopathology of HEV infection in humanscomparedwith other types of viral hepatitis. Theclassical pattern of liver injury in acute hepatitisE includes typical types of lesions found in otherforms of acute hepatitis (Peron et al. 2007b).These include ballooning of hepatocytes, scat-tered apoptotic (acidophilic) bodies, and infil-tration of the portal tracts with lymphocytes.Neutrophils are relatively common in the paren-chyma and the portal tracts, a feature not seen inother types of viral hepatitis, but lymphocytesare the predominant infiltrating cell type. Thereis also a cholestatic response to HEV infection.Cholestasis can be mild or moderate withplugged canaliculi, and lead to dilated ductulesor a pseudoglandular arrangement of hepato-cytes, particularly in the periportal regions. In-fections marked by strong cholestatic responsesmay have less hepatocellular injury than moretypical cases, and, in some regards, the chole-static form of hepatitis E can resemble HAVinfection. HEV-associated destructive cholangi-tis also has been described (Wendum et al.2005). In more severe cases, there can be wide-spread hepatocellular necrosis and collapse ofthe parenchyma with a prominent ductular re-action (Fig. 6A). Surviving hepatocytes may bedistended with foamy cytoplasm and pigmentedmacrophages are scattered throughout the pa-renchyma. Portal tracts are surrounded by a
Comparative Pathology of HAV and HEV Infections
Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a033456 11
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org

prominent ductular reaction. Inflammation ofvessel wall and Kupffer cell hyperplasia canalso be present. Reports from Western Europeindicate that autochthonousHEV infectionmaybe associated with substantial portal inflamma-tion, piecemeal necrosis, cholangiolitis, paren-chymal injury, and even fulminant hepatic fail-ure, and that histopathologic changes may bemore severe than in patients with infectionsacquired in more endemic regions (Malcolmet al. 2007; Peron et al. 2007a).
HEV Infection in Animals
Generally speaking, animals infected with HEVhave less hepatic inflammation and liver injuryand more modest ALT elevations than infectedhumans (Halbur et al. 2001; Meng 2010). How-ever, this may reflect a bias against the identifi-cation of mild infections in humans because of a
lack of readily available diagnostic tests. A widerange of nonhuman primate species are suscep-tible to infection with various genotypes ofHEV, including great apes (chimpanzees), OldWorld monkeys (cynomolgus, rhesus, andstump-tailed macaques, patas monkeys (Eryth-rocebus patas), and African green monkeys, aswell as New World primates such as owl mon-keys, squirrel monkeys (Saimiri sciureus), andtamarins (Fig. 7) (Wang and Wang 2016). Ofthese many species, cynomolgus macaqueshave been used most successfully in research.
Susceptible animal species can be infectedby either oral or intravenous inoculation of vi-rus, with the latter route considered most effi-cient (Gupta et al. 1990; Tsarev et al. 1994). Thecourse of the infection parallels that in infectedhumans, with a 3- to 8-week incubation preced-ing peak elevation of liver enzyme activity inserum (Uchida et al. 1990; Ticehurst et al.
b
a
A B
Figure 6.Hepatitis E in a hepatitis E virus (HEV)-infected patient. (A) Hematoxylin and eosin (H&E) stain. Theperiportal parenchyma contains a marked ductular reaction characterized by a proliferation of small-caliberducts lined with pale basophilic epithelial cells extending from the margin of the portal tract. Prominentextracellular matrix separates the ductules. Abutting hepatocytes are in disarray and prominent bile plugs areevident in distended canaliculi and ductules. A mild lymphocytic infiltrate is dispersed through the portal tractand adjacent parenchyma. (B) H&E stain. Higher-magnification image from the same patient. Prominentcholestasis is evident in distended canaliculi with formation of small bile lake at the interface of a prominentductular reaction on the right and a focus of hepatocytes (a) that are lightly vacuolated and lack normal sinusoidalarrangement. Scale bar, 100 µm.
J.M. Cullen and S.M. Lemon
12 Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a033456
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org

1992). Fecal viral shedding and viremia tend topeak simultaneously during the incubation andearly phase of disease. Liver inflammation de-velops along with liver enzyme elevations. Theinfection is self-limited, and resolution occursin all cases. Persistent infection, as described inimmunocompromised patients, has not beenobserved in nonhuman primates.
Nonhuman Primates: HEV Infectionin Chimpanzees
Chimpanzees (P. troglodytes) are variably sus-ceptible to infection with HEV, with host factorslikely affecting the severity of the disease. Serumaminotransaminase elevations occur followingintravenous inoculation of the virus, but theyare generally mild, rarely exceeding 100 IU/L(Yu et al. 2010) or 400 IU/L (Popper et al.1980). Chimpanzees appear to have less ALTelevation following HEV infection than similar-ly infected cynomolgus and rhesus macaques(Purcell et al. 2013). Histologic features havebeen described by several investigators (Pfeiferet al. 1980; Popper et al. 1980; Feinstone et al.1981; Purcell and Emerson 2001; Yu et al. 2010).Following an incubation period of 2–12 weeks,there may be swelling of hepatocytes with vari-ation in their staining and alterations of the cy-toplasm including clumping and lipid vacuoli-zation (Popper et al. 1980). Sinusoidal liningcells may be diffusely reactive. Periportal lym-phocytic infiltrates may develop, without piece-
meal necrosis, as well as focal necrosis within thehepatic parenchyma (Yu et al. 2010). Lymphoidfollicles are evident in some infected chimpan-zees, although eosinophils are present withinportal infiltrates in others (Popper et al. 1980).Occasionally, lymphocytes are seen to surroundbile ducts or ductules with the biliary epitheliumdisplaying mild variation in size and ratio ofnucleus to cytoplasmic surface area. Lympho-cytic infiltrates may also develop within the pa-renchyma along with an increase in macro-phages and scattered PAS-positive Kupffer cells.Focal necrosis may develop and moderate num-bers of apoptotic (acidophilic bodies) may bescattered within the parenchyma. During thecourse of the infection, there may be a transientalteration in the size of the nucleus in hepato-cytes and the appearance of multinucleated he-patocytes (Popper et al. 1980). Cholestasis hasnot been reported. During recovery, there maybe persistent evidence of activated sinusoidallining cells, characterized by increased size andmore prominent cytoplasm, particularly in thecentrilobular regions, and irregular dilation ofthe sinusoids.
HEV Infection in Old World Monkeys:Cynomolgus Macaques
Naturally occurring HEV infection has been re-ported in cynomolgus and rhesus macaques(M. fasicularis), although the histology of theseinfections is not well characterized (Arankalle
A B
ha
cb
cv
a
pv
Figure 7. Hepatitis E in a rhesus macaque. (A) The hepatic architecture is well preserved. Focal lymphocyticinfiltrates (a) are scattered throughout the parenchymawithmild lymphocytic infiltration (b) of the portal region.Scale bar, 100 µm. pv, portal vein; cv, central vein; ha, hepatic artery branch. (B) Focal lymphocytic parenchymalinflammatory infiltrate surrounding several necrotic hepatocytes.
Comparative Pathology of HAV and HEV Infections
Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a033456 13
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org

et al. 1994; Hirano et al. 2003; Yugo et al. 2014).Experimental infection of cynomolgus ma-caques with HEV produced no outward clinicalsigns (Bradley et al. 1987; Ticehurst et al. 1992).However, serum ALTelevations began∼25 daysfollowing inoculation, coincident with evidenceof hepatic inflammation. Increases in serumALT activity are generally no more than three-fold increased over baseline, although in onestudy the ALT level reached 600 IU/L in an in-dividual animal. The severity of hepatic injuryfollowing HEV inoculation may vary with thetiter of the inoculum as well as the responses ofthe individual animal, as might be expected inan outbred species (Soe et al. 1989; Tsarev et al.1993; Purcell et al. 2013).
The characteristic histologic response in in-fected cynomolgus monkeys is marked by mildlymphocytic portal inflammatory infiltrates.The infiltrates have been described as less exten-sive than those seen in infected owl monkeys(Ticehurst et al. 1992). Ballooning hepatocytes,scattered apoptotic hepatocytes associated withlymphocytes and macrophages, and parenchy-mal lymphocytes are typical (Krawczynski et al.2011). One severely affected animal was foundto have lymphocytic infiltrates and edema of theportal tracts, focal hepatic necrosis, and bothmicro- and macrovesicular lipid in hepatocytes(Tsarev et al. 1993). Neutrophils were found inthe portal tracts around portal veins as well aswithin the parenchyma. Therewas neither fibro-sis nor other residual lesions.
Rhesus Macaque
Rhesus macaques (Macaca mulatta), like chim-panzees and cynomolgus macaques, are suscep-tible to infection with all four genotypes of HEV(Wang andWang 2016). Histologic changes aresimilar to those seen in cynomolgus macaques(Tsarev et al. 1995; Krawczynski et al. 2011).
HEV Infection in New World Monkeys:Owl Monkeys
Owl monkeys (A. trivirgatus) infected intrave-nously with HEV derived from an outbreak inMexico did not have overt signs of disease
(Ticehurst et al. 1992). SerumALT levels peaked22–26 days following inoculation but were onlymodestly elevated (three to four times baseline)and there was only a minimal increase in serumbilirubin. Histologic changes in the liver weresimilarly limited. By day 23, lymphocytic infil-trates were evident in the portal tracts of three offive animals. One animal developed piecemealnecrosis with multiple apoptotic hepatocytes(acidophilic bodies), whereas another developeda parenchymal inflammatory infiltrate with aninflux of plasma cells. However, two of five an-imals did not develop histologic evidence of in-flammation. Swollen hepatocytes were apparentin one animal 69 days following inoculation(Ticehurst et al. 1992).
HEV Infection in Marmosets
Infected marmosets (Callithrix sp.) show rela-tively modest hepatic injury with minor eleva-tions in serum ALT activity (Feinstone et al.1981; Inoue et al. 1986). Histologic changes inexperimentally infected animals consist mainlyof lymphocytic infiltration of the portal tractsalong with the presence of pigment-laden mac-rophages in both portal tracts and parenchyma,multifocal individual hepatocyte necrosis, occa-sional lymphocytic sinusoidal infiltration, andKupffer cell activation (Inoue et al. 1986; Wata-nabe et al. 1987). Lymphocytes are frequentlyadjacent to injured hepatocytes. Cholestasishas not been observed. Hepatocyte ballooningand clumped cytoplasm was noted in one study,along with a general lack of parenchymal in-flammation. Later in the course of infection,Kupffer cell proliferation was prominent aswere apoptotic hepatocytes (acidophilic bodies),anisocytosis, and variations in the shape of thenucleus in hepatocytes (Feinstone et al. 1981;Bradley et al. 1987).
HEV Infection in Nonprimate Species: Rabbits
Rabbits can be naturally infected with a gtIIIstrain of HEV and have been experimentallyinfected with gtIV virus (Cossaboom et al.2011, 2012). Natural infection is widespread insome regions, and virus recovered from rabbits
J.M. Cullen and S.M. Lemon
14 Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a033456
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org

is capable of infecting pigs as well as nonhumanprimates. Histologic changes in the liver of in-fected adult rabbits are not well characterized,but inflammation appears to coincide with se-rum ALT elevation. Isolated foci of lymphocyticand histiocytic infiltrates were seen in one ofseveral infected rabbits and foci of necrosis inanother animal (Ma et al. 2010).
Pigs
There is widespread infection of domestic pigswith gtIII and gtIV viruses. Infected animals donot develop overt clinical signs, and generallyhave only minimal-to-moderate evidence of in-flammation (Meng et al. 1997). Hepatic inflam-mation was more severe in pigs infected withHEV derived from a human source than withHEV recovered from pigs, suggesting some dif-ferences between strains (Halbur et al. 2001).Natural infection is associated with mild lym-phocytic and plasmacytic portal and parenchy-mal infiltrates. Lymphocytes may be distributedalong the sinusoids. Swollen hepatocytes andmild focal necrosis may occasionally occur.Pigs infected with a human strain, US-2, hadsimilar, but more prominent lesions. Inflamma-tion was maximal 20 days following intravenousinoculation of the virus and persisted for up to55 days, with lesions diminishing toward theend of the infection (Halbur et al. 2001). Infect-ed pigs can be a source of infection in humansconsuming undercooked pork sausage or liver(Peron et al. 2007a,b).
Chickens
Avian HEV infection is widespread in the U.S.poultry population (Huang et al. 2002). Exper-imental infection of specific-pathogen-freechickens with avian HEV produces a mild hep-atitis. Lymphocytic and heterophilic perivascu-litis and vaculitits have been reported (Billamet al. 2005, 2009).
Rodents
Rats have been recognized to be naturally infect-ed with HEV infection since 2009 (Johne et al.
2010). There are no overt clinical signs associat-ed with the infection (Purcell et al. 2011; Li et al.2013), and liver enzyme activity is not increasedin serum (Purcell et al. 2011). There are onlylimited descriptions of histologic changes ac-companying infection in laboratory rats. Mildhepatitis characterized by light lymphocyticportal inflammation and aggregates of lympho-cytes within the parenchyma were noted. Scat-tered Kupffer cell aggregates were also present.We have tried, without success, to infectIfnar1−/− knockout mice by intravenous inocu-lation of HEV.
CONCLUDING REMARKS
Animal models, particularly nonhuman pri-mates, have significantly contributed to currentunderstanding of the pathogenesis of HAV andHEV. Nonhuman primates are susceptible toinfection with both HAV and HEV recoveredfrom infected humans, and the inflammatoryresponses in the liver parallel those seen in in-fected humans. Experimental animal modelshave been exceptionally valuable in developingan understanding of the impact of these viruseson the histologic appearance of the liver, as livertissue is rarely available for study from humansexperiencing typical, uncomplicated hepatitis Aor hepatitis E.
The pattern and timing of hepatic inflamma-tion following infectionwithHAV in susceptiblenonhuman primate species closely resemblesthat seen in infected humans. However, the de-gree of liver injury, reflected in enzyme eleva-tions and hepatic inflammation, has generallybeen reported to be milder in nonhuman pri-mates than in infected humans. There may behistologic evidence of cholestasis in infectednonhuman primates, but icterus and other overtclinical signs of disease such as lethargy and in-appetence are not observed, despite being com-mon in infected humans. To some extent, thismay reflect the age of experimentally infectedanimals, as HAV infection is often mild andnot recognized clinically in young children (Be-nenson et al. 1980). Nonetheless, in a carefullyexecuted vaccine trial involving healthy childrenaged 2–16years, eachof the 25placebo recipients
Comparative Pathology of HAV and HEV Infections
Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a033456 15
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org

who became infected was symptomatic and hadelevated serum ALT activity (mean 1383 U/Lwith a range of 240–2850) and half were icteric(Werzberger et al. 1992). Similar overt evidenceof liver injury has rarely been observed in exper-imentally infected nonhuman primates, al-though fulminant disease was reported in onechimpanzee (Theamboonlers et al. 2012). HEVinfection similarly appears to result in lesser de-grees of liver injury in experimentally infectedanimals than in humans. However, it seems like-ly that only the most severe HEV infections arerecognized clinically in humans, and there is stillmuch tobe learned about the complete spectrumof human HEV infection.
Despite these potential differences in se-verity of the inflammatory response, the natureof the host response and clearance of infectionseem to be quite similar, especially for hepatitisA. Distinctive features of HAV infection, whichhas a tendency toward more robust inflamma-tion in the portal and periportal regions of theliver, at times progressing to piecemeal necrosis,is recapitulated in primate models, particularlyin chimpanzees. The presence of large numbersof plasma cells is also a feature common to bothanimal models of HAV infection and infectionin humans. Prominent cholestasis, on the otherhand, is not commonly observed in animalmodels of HAV infection. Similarly, of the twomain types of histopathologic response to HEVinfection (inflammatory and cholestatic), in-flammation is reproduced in animal models, al-beit perhaps with less severity than in humans.Cholestatic responses to HEV infection have notbeen observed in animal models, but additionalstudies will be needed to accurately comparehuman and animal responses to HEV infectionat a fine level of detail.
REFERENCES�Reference is also in this collection.
Abe K, Shikata T. 1982. Fulminant type Aviral hepatitis in achimpanzee. Acta Pathol Jpn 32: 143–148.
Abe H, Beninger PR, Ikejiri N, Setoyama H, Sata M, Tani-kawa K. 1982. Light microscopic findings of liver biopsyspecimens from patients with hepatitis type A and com-parison with type B. Gastroenterology 82: 938–947.
Agrawal V, Goel A, Rawat A, Naik S, Aggarwal R. 2012.Histological and immunohistochemical features in fatalacute fulminant hepatitis E. Indian J Pathol Microbiol 55:22–27.
Amado LA, Marchevsky RS, De Paula VS, Hooper C, FreireMdS, Gaspar AMC, Pinto MA. 2010. Experimental hep-atitis A virus (HAV) infection in cynomolgus monkeys(Macaca fascicularis): Evidence of active extrahepaticsite of HAV replication. Int J Exp Pathol 91: 87–97.
Andzhaparidze AG, Kazachkov Iu A, Balaian MS, Kusov I,Poleshchuk VF. 1987. Hepatitis A in Macaca fascicularisandM. arctoides infected by the Java monkey-55 strain ofhepatitis A virus. Vopr Virusol 32: 440–448.
Arankalle VA, GoverdhanMK, Banerjee K. 1994. Antibodiesagainst hepatitis E virus in Old World monkeys. J ViralHepat 1: 125–129.
Asher LV, Binn LN, Mensing TL, Marchwicki RH, VassellRA, YoungGD. 1995. Pathogenesis of hepatitis A in orallyinoculated owl monkeys (Aotus trivirgatus). J Med Virol47: 260–268.
BalayanMS. 1992. Natural hosts of hepatitis Avirus.Vaccine10: S27–S31.
Baptista ML, Marchevsky RS, Oliveira AV, Yoshida CF,Schatzmayr HG. 1993. Histopathological and immuno-histochemical studies of hepatitis A virus infection inmarmosetCallithrix jacchus. Exp Toxicol Pathol 45: 7–13.
BenensonMW, Takafuji ET, Bancroft WH, Lemon SM, Cal-lahan MC, Leach DA. 1980. A military community out-break of hepatitis type A related to transmission in a childcare facility. Am J Epidemiol 112: 471–481.
Bennett AJ, Sibley SD, Lauck M, Weny G, Hyeroba D, Tu-mukunde A, Friedrich TC, O’Connor DH, Johnson CA,Rothman JM, et al. 2016. Naturally circulating hepatitis Avirus in olive baboons, Uganda. Emerg Infect Dis 22:1308–1310.
Billam P, Huang FF, Sun ZF, Pierson FW, Duncan RB, El-vinger F, Guenette DK, Toth TE, Meng XJ. 2005. System-atic pathogenesis and replication of avian hepatitis E virusin specific-pathogen-free adult chickens. J Virol 79: 3429–3437.
Billam P, LeRoith T, Pudupakam RS, Pierson FW, DuncanRB,MengXJ. 2009. Comparative pathogenesis in specific-pathogen-free chickens of two strains of avian hepatitis Evirus recovered from a chicken with hepatitis–splenome-galy syndrome and from a clinically healthy chicken. VetMicrobiol 139: 253–261.
BradleyDW,Gravelle CR, Cook EH, Fields RM,Maynard JE.1977. Cyclic excretion of hepatitis A virus in experimen-tally infected chimpanzees: Biophysical characterizationof the associated HAV particles. J Med Virol 1: 133–138.
Bradley DW, Krawczynski K, Cook EH Jr, McCaustland KA,HumphreyCD, Spelbring JE,MyintH,Maynard JE. 1987.Enterically transmitted non-A, non-B hepatitis: Serialpassage of disease in cynomolgus macaques and tamarinsand recovery of disease-associated 27- to 34-nm viruslikeparticles. Proc Natl Acad Sci 84: 6277–6281.
Burke DS, Heisey GB. 1984. Wild Malaysian cynomolgusmonkeys are exposed to hepatitis A virus. Am J TropMed Hyg 33: 940–944.
Cossaboom CM, Cordoba L, Dryman BA, Meng XJ. 2011.Hepatitis E virus in rabbits, Virginia, USA. Emerg InfectDis 17: 2047–2049.
J.M. Cullen and S.M. Lemon
16 Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a033456
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org

Cossaboom CM, Cordoba L, Sanford BJ, Pineyro P, KenneySP, Dryman BA, Wang Y, Meng XJ. 2012. Cross-speciesinfection of pigs with a novel rabbit, but not rat, strain ofhepatitis E virus isolated in the United States. J Gen Virol93: 1687–1695.
Coursaget P, Levesque B, Gretillat E, Eyraud M, Ferrara L,Germain M. 1981. Hepatitis A virus in primates outsidecaptivity. Lancet 2: 929–929.
Deinhardt F, Courtois G, Dherte P, Osterrieth P, Ninane G,Henle G, Henle W. 1962. Studies of liver function tests inchimpanzees after inoculation with human infectious ha-patitis virus. Am J Hyg 75: 311–321.
Deinhardt F, Holmes AW, Capps RB, Popper H. 1967. Stud-ies on the transmission of human viral hepatitis to mar-moset monkeys. I: Transmission of disease, serial pas-sages, and description of liver lesions. J Exp Med 125:673–688.
Deinhardt F, Peterson D, Cross G, Wolfe L, Holmes AW.1975. Hepatitis in marmosets. Am J Med Sci 270: 73–80.
Dienstag JL, Feinstone SM, Purcell RH, Hoofnagle JH, Bar-ker LF, London WT, Popper H, Peterson JM, KapikianAZ. 1975. Experimental infection of chimpanzees withhepatitis A virus. J Infect Dis 132: 532–545.
Dienstag JL, Davenport FM, McCollum RW, Hennessy AV,Klatskin G, Purcell RH. 1976. Nonhuman primate-asso-ciated viral hepatitis type A. Serologic evidence of hepa-titis A virus infection. JAMA 236: 462–464.
Drexler JF, Corman VM, Lukashev AN, van den Brand JM,Gmyl AP, Brunink S, Rasche A, Seggewibeta N, Feng H,Leijten LM, et al. 2015. Evolutionary origins of hepatitis Avirus in small mammals. Proc Natl Acad Sci 112: 15190–15195.
Ebert JW,Maynard JE, BradleyDW, LorenzD, KrushakDH.1978. Experimental infection of marmosets with hepatitisA virus. Primates Med 10: 295–299.
Emerson SU, Tsarev SA, Purcell RH. 1991. Biological andmolecular comparisons of human (HM-175) and simian(AGM-27) hepatitis A viruses. J Hepatol 13: S144–S145.
Feinstone SM, Alter HJ, Dienes HP, Shimizu Y, Popper H,Blackmore D, Sly D, LondonWT, Purcell RH. 1981. Non-A, non-B hepatitis in chimpanzees and marmosets. J In-fect Dis 144: 588–598.
Fujiwara K, Yokosuka O, Ehata T, Saisho H, Saotome N,Suzuki K, Okita K, Kiyosawa K, Omata M. 2002. Associ-ation between severity of type A hepatitis and nucleotidevariations in the 50 non-translated region of hepatitis Avirus RNA: Strains from fulminant hepatitis have fewernucleotide substitutions. Gut 51: 82–88.
Gordon SC, Reddy KR, Schiff L, Schiff ER. 1984. Prolongedintrahepatic cholestasis secondary to acute hepatitis A.Ann Int Med 101: 635–637.
Gupta H, Tandon BN, Sriramachari S, Joshi YK, Iyenger B.1990. Animal transmission of enteric non-A, non-B hep-atitis infection to Macaca mulatta by faeco-oral route.Indian J Med Res 91: 87–90.
Halbur PG, Kasorndorkbua C, Gilbert C, Guenette D, Pot-ters MB, Purcell RH, Emerson SU, Toth TE, Meng XJ.2001. Comparative pathogenesis of infection of pigs withhepatitis E viruses recovered from a pig and a human. JClin Microbiol 39: 918–923.
Hirai-Yuki A, Hensley L, McGivern DR, Gonzalez-Lopez O,Das A, FengH, Sun L,Wilson JE, Hu F, Feng Z, et al. 2016.MAVS-dependent host species range and pathogenicityofhuman hepatitis A virus. Science 353: 1541–1545.
� Hirai-Yuki A, Whitmire JK, Joyce M, Tyrrell DL, LemonSM. 2018. Murine models of hepatitis A virus (HAV)infection. Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a031674.
Hirano M, Ding X, Tran HT, Li TC, Takeda N, Sata T, Na-kamura S, Abe K. 2003. Prevalence of antibody againsthepatitis E virus in various species of non-human pri-mates: Evidence of widespread infection in Japanesemonkeys (Macaca fuscata). Jpn J Infect Dis 56: 8–11.
Holmes AW, Wolfe L, Rosenblate H, Deinhardt F. 1969.Hepatitis in marmosets: Induction of disease with codedspecimens from a human volunteer study. Science 165:816–817.
Hornei B, Kammerer R,Moubayed P, FringsW, Gauss-Mul-ler V, Dotzauer A. 2001. Experimental hepatitis A virusinfection in guinea pigs. J Med Virol 64: 402–409.
Huang FF, Haqshenas G, Shivaprasad HL, Guenette DK,Woolcock PR, Larsen CT, Pierson FW, Elvinger F, TothTE, Meng XJ. 2002. Heterogeneity and seroprevalence ofa newly identified avian hepatitis E virus from chickens inthe United States. J Clin Microbiol 40: 4197–4202.
Inoue O, Nagataki S, Itakura H, Iida F, Shimizu Y, Yano M,Shikata T, Tandon BN. 1986. Liver morphology in mar-mosets infected with epidemic non-A, non-B hepatitis inIndia. Liver 6: 178–183.
Johne R, Heckel G, Plenge-Bonig A, Kindler E, Maresch C,Reetz J, Schielke A, Ulrich RG. 2010. Novel hepatitis Evirus genotype inNorway rats, Germany.Emerg InfectDis16: 1452–1455.
Jung YM, Park SJ, Kim JS, Jang JH, Lee SH, Kim JW, ParkYM, Hwang SG, Rim KS, Kang SK, et al. 2010. Atypicalmanifestations of hepatitis A infection: A prospective,multicenter study in Korea. J Med Virol 82: 1318–1326.
Kabrane-Lazizi Y, Fine JB, Elm J, Glass GE, Higa H, DiwanA, Gibbs CJ Jr, Meng XJ, Emerson SU, Purcell RH. 1999.Evidence for widespread infection of wild rats with hep-atitis E virus in the United States. Am J Trop Med Hyg 61:331–335.
Kamar N, Garrouste C, Haagsma EB, Garrigue V, Pischke S,Chauvet C, Dumortier J, Cannesson A, Cassuto-ViguierE, Thervet E, et al. 2011. Factors associated with chronichepatitis in patients with hepatitis E virus infection whohave received solid organ transplants. Gastroenterology140: 1481–1489.
Karayiannis P, Jowett T, Enticott M, Moore D, Pignatelli M,Brenes F, Scheuer PJ, ThomasHC. 1986. Hepatitis Avirusreplication in tamarins and host immune response inrelation to pathogenesis of liver cell damage. J Med Virol18: 261–276.
Karayiannis P, Chitranukroh R, Fry M, Petrovic LM, MooreD, Scheuer PJ, ThomasHC. 1990. Protracted alanine ami-notransferase levels in tamarins infected with hepatitis Avirus. J Med Virol 30: 151–158.
Keenan CM, Lemon SM, LeDuc JW, McNamee GA, BinnLN. 1984. Pathology of hepatitis A infection in the owlmonkey (Aotus trivirgatus). Am J Pathol 115: 1–8.
Comparative Pathology of HAV and HEV Infections
Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a033456 17
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org

Krawczynski K, Meng XJ, Rybczynska J. 2011. Pathogeneticelements of hepatitis E and animal models of HEV infec-tion. Virus Res 161: 78–83.
Kryger P, Christoffersen P. 1983. Liver histopathology of thehepatitis A virus infection: A comparison with hepatitistype B and non-A, non-B. J Clin Pathol 36: 650–654.
Lanford RE, Feng Z, Chavez D, Guerra B, Brasky KM, ZhouY, YamaneD, PerelsonAS,Walker CM, Lemon SM. 2011.Acute hepatitis A virus infection is associated with a lim-ited type I interferon response and persistence of intra-hepatic viral RNA. Proc Natl Acad Sci 108: 11223–11228.
Lemon SM. 1994. The natural history of hepatitis A: Thepotential for transmission by transfusion of blood orblood products. Vox San 67: 19–23; discussion 24–16.
� Lemon SM, Walker CM. 2018. Hepatitis A virus and hepa-titis E virus: Emerging and re-emerging enterically trans-mitted hepatitis viruses. Cold Spring Harb Perspect Meddoi: 10.1101/cshperspect.a031823.
Lemon SM, LeDuc JW, Binn LN, Escajadillo A, Ishak KG.1982. Transmission of hepatitis A virus among recentlycaptured Panamanian owl monkeys. J Med Virol 10: 25–36.
Lemon SM, Chao SF, Jansen RW, Binn LN, LeDuc JW. 1987.Genomic heterogeneity among human and nonhumanstrains of hepatitis A virus. J Virol 61: 735–742.
� Li T-C, Wakita T. 2018. Small animal models of hepatitis Evirus infection. Cold Spring Harb Perspect Med doi:10.1101/cshperspect.a032581.
Li TC, Yoshizaki S, Ami Y, Suzaki Y, Yasuda SP, YoshimatsuK, Arikawa J, Takeda N, Wakita T. 2013. Susceptibility oflaboratory rats against genotypes 1, 3, 4, and rat hepatitisE viruses. Vet Microbiol 163: 54–61.
Ma H, Zheng L, Liu Y, Zhao C, Harrison TJ, Ma Y, Sun S,Zhang J, Wang Y. 2010. Experimental infection of rabbitswith rabbit and genotypes 1 and 4 hepatitis E viruses.PLoS ONE 5: e9160.
Malcolm P, Dalton H, Hussaini HS, Mathew J. 2007. Thehistology of acute autochthonous hepatitis E virus infec-tion. Histopathology 51: 190–194.
Mao JS, Guo XY, Huang HY, Yu PH, Huang BZ, Ding ZC,Chen NL, Yu JH, Xie RY. 1981. Studies on the transmis-sion of human hepatitis A virus to stump-tailed monkey.Sci Sin 24: 1590–1596.
Mathiesen LR, Moller AM, Purcell RH, London WT, Fein-stone SM. 1980. Hepatitis Avirus in the liver and intestineofmarmosets after oral inoculation. Infect Immun 28: 45–48.
Matsuda H, Okada K, Takahashi K, Mishiro S. 2003. Severehepatitis E virus infection after ingestion of uncookedliver from a wild boar. J Infect Dis 188: 944.
Maynard JE. 1975. Hepatitis A: Perspectives and recent ad-vances. Am J Pathol 81: 683–694.
Maynard JE, Bradley DW, Gravelle CR, Ebert JW, KrushakDH. 1975. Preliminary studies of hepatitis A in chimpan-zees. J Infect Dis 131: 194–197.
Meng XJ. 2010. Hepatitis E virus: Animal reservoirs andzoonotic risk. Vet Microbiol 140: 256–265.
Meng XJ, Purcell RH, Halbur PG, Lehman JR, Webb DM,Tsareva TS, Haynes JS, Thacker BJ, Emerson SU. 1997. Anovel virus in swine is closely related to the human hep-atitis E virus. Proc Natl Acad Sci 94: 9860–9865.
Nainan OV, Margolis HS, Robertson BH, Balayan M, Brin-ton MA. 1991. Sequence analysis of a new hepatitis Avirus naturally infecting cynomolgus macaques (Macacafascicularis). J Gen Virol 72: 1685–1689.
Peron JM, BureauC, PoirsonH,Mansuy JM,Alric L, Selves J,Dupuis E, Izopet J, Vinel JP. 2007a. Fulminant liver failurefrom acute autochthonous hepatitis E in France: Descrip-tion of seven patients with acute hepatitis E and enceph-alopathy. J Viral Hepat 14: 298–303.
Peron JM, Danjoux M, Kamar N, Missoury R, Poirson H,Vinel JP, Mansuy JM, Bureau C, Izopet J, Brousset P, et al.2007b. Liver histology in patients with sporadic acutehepatitis E: A study of 11 patients from South-WestFrance. Virchows Arch 450: 405–410.
Pfeifer U, Thomssen R, Legler K, Bottcher U, Gerlich W,Weinmann E, Klinge O. 1980. Experimental non-A,non-B hepatitis: Four types of cytoplasmic alteration inhepatocytes of infected chimpanzees. Virchows Arch BCell Pathol Incl Mol Pathol 33: 233–243.
Popper H, Dienstag JL, Feinstone SM, Alter HJ, Purcell RH.1980. The pathology of viral hepatitis in chimpanzees.Virchows Arch A Pathol Anat Histol 387: 91–106.
Purcell RH, Emerson SU. 2001. Animal models of hepatitisA and E. ILAR J 42: 161–177.
Purcell RH, Engle RE, Rood MP, Kabrane-Lazizi Y, NguyenHT, Govindarajan S, St Claire M, Emerson SU. 2011.Hepatitis E virus in rats, Los Angeles, California, USA.Emerg Infect Dis 17: 2216–2222.
Purcell RH, Engle RE, Govindarajan S, Herbert R, St ClaireM, Elkins WR, Cook A, Shaver C, Beauregard M, Swerc-zek J, et al. 2013. Pathobiology of hepatitis E: Lessonslearned from primate models. EmergMicrobe Infect 2: e9.
Rein DB, Stevens GA, Theaker J, Wittenborn JS, WiersmaST. 2012. The global burden of hepatitis E virus genotypes1 and 2 in 2005.Hepatology (Baltimore, Md) 55: 988–997.
� Sander A-L, Corman VM, Lukashev AN, Drexler JF. 2018.Evolutionary origins of enteric hepatitis viruses. ColdSpring Harb Perspect Med doi: 10.1101/cshperspect.a031690.
Shevtsova ZV, Lapin BA, Doroshenko NV, Krilova RI, Kor-zaja LI, Lomovskaya IB, Dzhelieva ZN, Zairov GK, Stak-hanova VM, Belova EG, et al. 1988. Spontaneous andexperimental hepatitis A in Old World monkeys. J MedPrimatol 17: 177–194.
� Shin E-C, Jeong S-K. 2018. Natural history, clinical manifes-tations, and pathogenesis of hepatitis A.Cold Spring HarbPerspect Med doi: 10.1101/cshperspect.a031708.
Siebert U, Rademaker M, Ulrich SA, Wohlsein P, Ronnen-berg K, Prenger-Berninghoff E. 2017. Bacterial micro-biota in harbor seals (Phoca vitulina) from the NorthSea of Schleswig-Holstein, Germany, around the time ofmorbillivirus and influenza epidemics. J Wildl Dis 53:201–214.
� Smith DB, Simmonds P. 2018. Classification and genomicdiversity of enterically transmitted hepatitis viruses. ColdSpring Harb Perspect Med doi: 10.1101/cshperspect.a031880.
Soe S, Uchida T, Suzuki K, Komatsu K, Azumi J, Okuda Y,Iida F, Shikata T, Rikihisa T,MizunoK, et al. 1989. Enteri-cally transmitted non-A, non-B hepatitis in cynomolgusmonkeys: Morphology and probable mechanism of hepa-tocellular necrosis. Liver 9: 135–145.
J.M. Cullen and S.M. Lemon
18 Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a033456
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org

Taylor RM,Davern T,Munoz S, Han SH,McGuire B, LarsonAM, Hynan L, Lee WM, Fontana RJ. 2006. Fulminanthepatitis Avirus infection in the United States: Incidence,prognosis, and outcomes. Hepatology 44: 1589–1597.
Teixeira MR Jr, Weller IV, Murray A, Bamber M, ThomasHC, Sherlock S, Scheuer PJ. 1982. The pathology of hep-atitis A in man. Liver 2: 53–60.
Theamboonlers A, Abe K, Thongmee C, Poovorawan Y.2012. Complete coding sequence and molecular analysisof hepatitis A virus from a chimpanzee with fulminanthepatitis. J Med Primatol 41: 11–17.
Ticehurst J, Rhodes LL Jr, Krawczynski K, Asher LV, EnglerWF, Mensing TL, Caudill JD, Sjogren MH, Hoke CH Jr,LeDuc JW, et al. 1992. Infection of owl monkeys (Aotustrivirgatus) and cynomolgus monkeys (Macaca fascicula-ris) with hepatitis E virus from Mexico. J Infect Dis 165:835–845.
Tsarev SA, Emerson SU, Balayan MS, Ticehurst J, PurcellRH. 1991. Simian hepatitis A virus (HAV) strain AGM-27: Comparison of genome structure and growth in cellculture with other HAV strains. J Gen Virol 72: 1677–1683.
Tsarev SA, Emerson SU, Tsareva TS, YarboughPO, LewisM,Govindarajan S, Reyes GR, Shapiro M, Purcell RH. 1993.Variation in course of hepatitis E in experimentally in-fected cynomolgus monkeys. J Infect Dis 167: 1302–1306.
Tsarev SA, Tsareva TS, Emerson SU, Yarbough PO, LegtersLJ, Moskal T, Purcell RH. 1994. Infectivity titration of aprototype strain of hepatitis E virus in cynomolgus mon-keys. J Med Virol 43: 135–142.
Tsarev SA, Tsareva TS, Emerson SU, Rippy MK, Zack P,Shapiro M, Purcell RH. 1995. Experimental hepatitis E
in pregnant rhesus monkeys: Failure to transmit hepatitisE virus (HEV) to offspring and evidence of naturally ac-quired antibodies to HEV. J Infect Dis 172: 31–37.
Uchida T, Win KM, Suzuki K, Komatsu K, Iida F, Shikata T,Rikihisa T, Mizuno K, Soe S, Myint H, et al. 1990. Serialtransmission of a putative causative virus of entericallytransmitted non-A, non-B hepatitis to Macaca fascicula-ris and Macaca mulatta. Jpn J Exp Med 60: 13–21.
Wang L, Wang L. 2016. Animal models for hepatitis E virus.Adv Exp Med Biol 948: 161–173.
Watanabe T, Katagiri J, Kojima H, Kamimura T, Ichida F,Ashida M, Hamada C, Shibayama T. 1987. Studies ontransmission of human non-A, non-B hepatitis to mar-mosets. J Med Virol 22: 143–156.
Wendum D, Nachury M, Yver M, Lemann M, Flejou JF,Janin A, Bertheau P. 2005. Acute hepatitis E: A cause oflymphocytic destructive cholangitis. Hum Pathol 36:436–438.
Werzberger A, Mensch B, Kuter B, Brown L, Lewis J, SitrinR, Miller W, Shouval D, Wiens B, Calandra G, et al.1992. A controlled trial of a formalin-inactivated hepa-titis A vaccine in healthy children. N Engl J Med 327:453–457.
Yu C, Boon D, McDonald SL, Myers TG, Tomioka K,Nguyen H, Engle RE, Govindarajan S, Emerson SU, Pur-cell RH. 2010. Pathogenesis of hepatitis E virus and hep-atitis C virus in chimpanzees: Similarities and differences.J Virol 84: 11264–11278.
Yugo DM, Cossaboom CM, Meng XJ. 2014. Naturally oc-curring animal models of human hepatitis E virus infec-tion. ILAR J 55: 187–199.
Comparative Pathology of HAV and HEV Infections
Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a033456 19
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org






![Hepatitis B virus and hepatitis C virus play different ... · alcoholic cirrhosis, hepatitis viruses, tobacco and metabolic diseases[4]. Hepatitis viruses, including hepatitis B virus](https://img.pdfslide.us/doc/110x75/60e46cab5bd9101a6f539e91/hepatitis-b-virus-and-hepatitis-c-virus-play-different-alcoholic-cirrhosis.jpg)