Embed Size (px)
Citation preview

emmuv
lp
tsc
tfetctatse
tpaf
Clinical Therapeutics/Volume 33, Number 2, 2011
Brief Report
Comparative Effectiveness of a Prenatal Medical Food toPrenatal Vitamins on Hemoglobin Levels and AdverseOutcomes: A Retrospective Analysis
Susan Bentley, WHNP-BC1; Amy Hermes, RN, WHNP-BC2; Diane Phillips, RNC3;Yahya A. Daoud, MS4; and Sylvia Hanna, MD5
1Women’s Clinic Shoals, Sheffield, Alabama; 2Gainesville Obstetrics and Gynecology, Gainesville, Texas;3Women’s Health Associates, Flowood, Mississippi; 4Quantitative Sciences Department, Baylor HealthCare System, Dallas, Texas; and 5Writing Assistance, Inc, Plymouth, Minnesota
03t(Ag(obat1[a
ABSTRACTBackground: The role of folate in pregnancy is well
stablished, with most prenatal vitamins (PNVs) on thearket containing at least 800 �g of folic acid. Folic acidust be converted in the body to L-methylfolate, the nat-ral and biologically active form of folate. The role ofitamin B12 in pregnancy is less characterized, and most
PNV formulations contain only 0 to 12 �g. The presentstudy was undertaken to evaluate whether taking a pre-natal medical food containing L-methylfolate and muchhigher doses of vitamin B12 results in higher hemoglobinevels and thus, a lower incidence of anemia duringregnancy.
Objective: The objective of this exploratory study waso evaluate the effects of the prenatal medical food versustandard PNVs on hemoglobin levels and adverse out-omes throughout pregnancy.
Methods: For this retrospective analysis, we reviewedhe charts of female patients taking either a prenatal medicalood or standard PNV during pregnancy. Hemoglobin lev-ls measured at initiation of prenatal care, end of secondrimester, and delivery were recorded. Patients who had re-eived additional iron supplementation, beyond that con-ained in theprenatalmedical foodorPNVtheywere takingnd before anemia screening at the end of the second trimes-er, were excluded from the study. Fisher exact test, �2 test,tudent t test, and ANOVA were used to evaluate differ-nces between the treatment groups.
Results: Data were analyzed from 112 charts: 58 pa-ients (51.8%) were taking the prenatal medical food; 54atients (48.2%) were taking standard PNVs. Mean (SD)ge at first prenatal visit was 27 (4.6) years in the medical
ood group and 28.8 (3.5) years in the PNV group (P �204
.024). Mean (SD) body mass indices were 29.1 (6.5) and1.7 (8.9) in the medical food and PNV groups, respec-ively (P � NS). In the medical food group, 35 women60.3%) were white/Caucasian, 17 (29.3%) were Africanmerican, and 6 (10.4%) were of other races. In the PNVroup, 24 women (44.4%) were white/Caucasian, 2546.3%) were African American, and 5 (9.3%) were ofther races. However, race was not significantly differentetween the two groups. At end of second trimester andt delivery, mean (SD) hemoglobin levels were higher inhe prenatal medical food group (11.8 [1.1] g/dL and1.8 [1.3] g/dL, respectively) than in the PNV group (11.31.2] g/dL and 10.7 [1.2] g/dL, respectively) (P � 0.011nd P � 0.001, respectively). Significantly fewer cases of
anemia were reported at end of second trimester in theprenatal medical food group than in the PNV group(39.7% vs 74.1%; P � 0.001).
Conclusions: In the present study, supplementationwith a prenatal medical food containing L-methylfolate andhigh-dose vitamin B12 may maintain hemoglobin levels anddecrease rates of anemia in pregnancy more effectively thanstandard prenatal vitamins; however, prospective, con-trolled studies are warranted. ClinicalTrials.gov identifier:NCT01193192. (Clin Ther. 2011;33:204–210) © 2011Elsevier HS Journals, Inc. All rights reserved.
This material was presented as a poster at the 67th Annual Meeting ofthe American Society of Reproductive Medicine in Denver, Colorado,October 23�27, 2010.
Accepted for publication February 22, 2011.doi:10.1016/j.clinthera.2011.02.0100149-2918/$ - see front matter
© 2011 Elsevier HS Journals, Inc. All rights reserved.
Volume 33 Number 2

p5fsadia
dq
rl
1prtcfcdt
vPm
f((mscB
S. Bentley et al.
Key words: anemia, folate, hemoglobin, medicalfood, Neevo, Neevo DHA, pregnancy, prenatal, pre-natal vitamin, vitamin B12.
INTRODUCTIONThe World Health Organization estimates that 35% to75% of pregnant women in developing countries and18% of women in industrialized countries developanemia.1 During a singleton pregnancy, maternallasma volume gradually expands by approximately0% (1000 mL), 2 and anemia can prevent the fetusrom receiving adequate oxygen and nutrition neces-ary for normal development. Multiple studies havelso shown a correlation between maternal anemiauring the first and second trimester of pregnancy and
ncreased rates of both preterm (�37 weeks’ gestation)nd low-birth-weight deliveries.3,4
The most common cause of anemia during preg-nancy is decreased red blood cell production due toiron deficiency. Iron supplementation has beenshown to decrease the prevalence of maternal ane-mia at delivery.5 However, the gastrointestinal sideeffects (eg, nausea, vomiting, constipation) of ironsupplements often lead to poor compliance.6 In ad-
ition to iron, folate and vitamin B12 also are re-uired for erythropoiesis.7
During pregnancy, the daily folate requirement isincreased by fetal demands, while simultaneously thereis a decrease in gastrointestinal absorption of folate.Older age and obesity in conjunction with pregnancymay also increase folate needs.8,9 Folate deficiency isthe most common cause of megaloblastic anemia dur-ing pregnancy.10 For decades, folic acid has been rec-ognized as an essential periconceptional supplementfor the prevention of neural tube defects.11 There isincreasing evidence that decreased maternal folate lev-els during pregnancy may also lead to intrauterinegrowth retardation and low infant birth weight.12,13
Additionally, various pregnancy complications, suchas miscarriage, placental abruption, and preeclampsia,have been associated with folate deficiency.8
Folate deficiency may be the result of genetic errorsof folate metabolism. L-methylfolate is the biologicallyactive isomer of folate and the primary form of folatein circulation. It is the only form of folate to cross theblood-brain barrier. Synthetic folic acid and dietarydihydrofolate must be converted to L-methylfolate in a
multistep process in which the methylenetetrahydrofo-February 2011
late reductase (MTHFR) enzyme is responsible for thefinal conversion to L-methylfolate. A common geneticvariant of the MTHFR enzyme significantly reducesthe amount of available L-methylfolate and can lead topreterm delivery and birth defects.8,14
The role of vitamin B12 in pregnancy is less charac-terized. Vitamin B12 deficiency has been shown to be aisk factor for neural tube defects, independent of fo-ate status.15 Vitamin B12 deficiency has also beenlinked to early pregnancy loss16,17 and preterm deliv-ery,18 although more research is needed.
Defined by the Orphan Drug Act Amendments in988, a medical food is a “specially formulated androcessed” product “(as opposed to a naturally occur-ing foodstuff used in a natural state)” and is in-ended for a patient who “has a limited or impairedapacity to ingest, absorb, or metabolize ordinaryoodstuffs or certain nutrients, or who has other spe-ial medically determined nutrient requirements, theietary management of which cannot be achieved byhe modification of the normal diet alone.”19,20 The
prenatal medical food with or without docosa-hexaenoic acid (DHA)* in the present study is indi-cated for “the dietary management of impaired meta-bolic processes in women under a doctor’s care whoface high to intermediate risk pregnancies and are un-able to fully metabolize or absorb folic acid.”21,22 Themajor differences between the prenatal medical foodand PNVs are in folate and vitamin B12 content (TableI). The prenatal medical food with or without DHAcontains 1.13 mg of L-methylfolate in addition to0.4 mg folic acid, whereas PNVs contain 0.8 to 1.0mg of folic acid alone. The prenatal medical foodwith and without DHA contain 1000 and 500 �g ofitamin B12, respectively, versus only 0 to 12 �g inNVs. The recommended daily allowance for vita-in B12 in pregnancy is only 2.6 �g (or 2.8 �g during
lactation).23 So whereas the vitamin B12 content dif-ers between the prenatal medical food with DHA1000 �g) and prenatal medical food without DHA500 �g), both are in vast excess of the recom-ended daily allowance and thus are treated as a
ingle treatment (high folate and high vitamin B12) inomparison to PNVs (low folate and low vitamin
12).
*Trademark: Néevo® or NéevoDHA® (Pamlab, LLC, Coving-
ton, Louisiana).205

3mdttlftnulpae
as
Clinical Therapeutics
The primary objective of this study was to evaluatethe effects of prenatal medical food with or withoutDHA on hemoglobin levels throughout pregnancycompared with PNV formulations containing 400 to1000 �g folic acid, 0 to 12 �g of vitamin B12, and 27 to5 mg of iron. Patients were prescribed the prenataledical food (with or without DHA) when they had aocumented MTHFR gene polymorphism. However,he genotype is rarely known and most commonly pa-ients are provided samples of multiple prenatal formu-ations (including PNVs and the prenatal medicaloods) and are instructed to choose one that is wellolerated to continue taking throughout the preg-ancy. Because the patient’s MTHFR genotype is notsually known, the potential for bias in treatment se-
ection by the prescriber is minimal and the type ofatients in each study group should be similar and suit-ble for comparison. Secondary objectives in the pres-
Table I. Comparison of nutritional content in prenaprenatal food with DHA, and prenatal vitam
ContentPrenatal Medical Food
Without DHA
L-Methylfolate, mg 1.13Folic acid, mg 0.4Vitamin A, IU –Vitamin B1, mg 3Vitamin B2, mg 3.4Vitamin B3, mg 20Vitamin B5, mg 7Vitamin B6, mg 2.6Vitamin B12, �g 500Biotin, �g 0.003Vitamin C, mg 80Vitamin D, IU 400Vitamin E, IU 30Calcium, mg 200Iron, mg 29Copper, mg 2.0Iodine, mg –Magnesium, mg 40Selenium, �g –Zinc, mg 15
*Nutritional content for prenatal vitamins was taken from: Pr
nt study compared the incidence of anemia diagnosed
206
t end of second trimester and incidence of preeclamp-ia between the study groups.
PATIENTS AND METHODS
This was a multicenter, retrospective, observationalstudy of pregnant women between the ages of 21 and39 years who were prescribed either prenatal medicalfood (with or without DHA) or a standard PNV.Charts were reviewed by nurse practitioners at 3 pri-vate practice obstetrics and gynecology clinics: Wom-en’s Clinic Shoals (Sheffield, Alabama), GainesvilleObstetrics and Gynecology (Gainesville, Texas), andWomen’s Health Associates (Flowood, Mississippi).The research was deemed exempt from full review byan Institutional Review Board because it involved onlythe review of de-identified patient data.
The PNV was required to contain no more than 1.2
edical food without docosahexaenoic acid (DHA),
Prenatal Medical FoodWith DHA Prenatal Vitamins*
1.130.4 0.4�1.0– 0�4000– 1.5�3.0– 1.6�4.0– 15�20– 0�10
25 2.5�50.01000 0�12
– 0�3040 28�120
– 200�40030 10�3075 100�23027 20�35
– 0�2– 0�0.175– 0�40– 0�65– 15�26
l vitamins. MPR (Monthly Prescribing Reference). 2010;21:121.
tal mins.
enata
mg of folic acid, between 27 and 35 mg of iron, and no
Volume 33 Number 2

engtba
S. Bentley et al.
more than 12 �g of vitamin B12. These requirementsapply to most prenatal vitamins on the market butexclude those with much higher iron content thanfound in the prenatal medical food. Pregnant womenwith successful birth delivery between January 1, 2008and December 31, 2009 were considered for inclusion.At each site, charts were screened for eligibility begin-ning with the most recent delivery on or before Decem-ber 31, 2009 and continuing in reverse chronologicalorder until 100 charts had been selected for analysis.Clinical diagnosis of pregnancy must have been made(and thus prenatal supplementation started) in the first12 weeks of pregnancy and on or after January 1,2008.
Women were excluded if they had undergone ablood transfusion in the 4 months before diagnosis ofpregnancy. Other exclusion criteria included takingany supplements containing �10 mg of vitamin B6,
�35 mg of iron, or �1.2 mg of folate or receivingvitamin B12 injections within 2 months of diagnosis ofpregnancy. Additionally, women taking an L-methyl-folate product such as Life Extension methylfolate(Life Extension Foundation, Ft. Lauderdale, Florida),ProThera methylfolate (ProThera, Inc, Reno, Nevada),Thorne 5-MTHF (Thorne Research, Dover, Idaho), orcertain medical food brands* within 2 months of diag-nosis of pregnancy were also excluded.
A total of 189 charts were screened: 16 were ex-cluded for age �21 years; 6 were excluded for age �39years; 17 were excluded because the diagnosis of preg-nancy was made at �12 weeks’ gestation; 6 were ex-cluded for the PNV iron content �35 mg; 3 were ex-cluded for having taken additional iron supplementsbefore the anemia screening at the end of the secondtrimester; and 29 were excluded for inadequate chartdocumentation, including no record of what prenatalformulation the patient was taking or missing hemo-globin values. The number of eligible charts across all 3sites was monitored biweekly by the sponsor until atleast 100 charts had been found to be eligible for in-clusion in the analysis. When this occurred, 112 chartshad been deemed eligible.
Hemoglobin blood levels were recorded at the 3time points usually measured during pregnancy: initi-ation of prenatal care (weeks 1�12), the end of thesecond trimester (weeks 22�28), and at or near the
*Trademarks: Metanx®, Deplin®, Cerefolin®, or CerefolinNAC®
(Pamlab, LLC, Covington, Louisiana).
February 2011
time of delivery. For the purposes of this study, “ane-mia” was confirmed by the documentation of addi-tional iron supplementation prescribed for a hemoglo-bin level �11 g/dL measured at the end of secondtrimester (weeks 22�28). Patient demographics andbody mass index were also recorded. All data collectedfrom the patient charts were de-identified and codedaccording to treatment group.
Fisher exact test and �2 test analysis were used tovaluate the differences between the patients in the pre-atal medical food group and the patients in the PNVroup for categorical variables, such as race. Student test and ANOVA were used to evaluate the differenceetween the 2 groups for continuous variables, such asge and hemoglobin values.
RESULTSA total of 112 charts were analyzed. Of the sample, 58patients (51.8%) had taken the prenatal medical foodand 54 patients (48.2%) had taken standard PNVs. Ofthe patients taking the medical food, 42 (72.4%) hadtaken the medical food without DHA and 16 (27.6%)had taken the medical food with DHA. The demo-graphic characteristics of the pregnant women werenot significantly different, with the exception of age,between the 2 treatment groups (Table II). The agedifference between groups was statistically significant;however, the difference of 1.8 years is perhaps not clin-ically significant. Additionally, no significant differ-ences were found between the 2 treatment groups inthe mean number of weeks pregnant when the 3 hemo-globin measurements were performed.
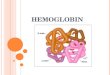
The effects of the prenatal medical food on hemo-globin levels, anemia, and preeclampsia in pregnantwomen throughout the course of pregnancy are foundin Table III. At the initiation of prenatal care (weeks1�12), no significant difference was found in mean(SD) hemoglobin between the prenatal medical foodgroup (12.4 [12] g/dL) and the PNV group (12.1 [12]g/dL). Mean (SD) hemoglobin levels were significantlyhigher in the prenatal medical food group at the end ofthe second trimester and at the time of delivery (11.8[1.1] g/dL and 11.8 [1.3] g/dL, respectively) when com-pared with the PNV group (11.3 [1.2] g/dL and 10.7[12] g/dL, respectively) (P � 0.011 and P � 0.001,respectively) (Figure). There was no significant differ-ence between the groups in the mean change in hemo-globin from the initiation of prenatal care to the end of
the second trimester. However, the mean (SD) change207

Clinical Therapeutics
in hemoglobin significantly dropped less in the prena-tal medical food group (�0.6 [1.6]) compared withPNV group (�1.3 [0.9]) from the initiation of prenatalcare to delivery (P � 0.003); this represents a relativechange of �4.0% and �10.9% in the prenatal medicalfood group and PNV group, respectively (P � 0.001).
Significantly fewer patients in the prenatal medicalfood group developed anemias requiring additionaliron supplements than in the PNV group (39.7% vs74.1%; P � 0.001). There was no significant differencebetween groups in the number of patients developingpreeclampsia (9/54 [16.7%] in the PNV group vs 6/58[10.3%] in the prenatal medical food group).
Table II. Summary of patient characteristics.
CharacteristicPr
Age, mean (SD), yBody mass index, mean (SD)Race, n (%)
WhiteBlackOther*
Gestational age at initiation of prenatal care,mean (SD), wkGestational age at delivery, mean (SD), wk
*Includes Asian, Hawaiian/Pacific Islander, and American In
Table III. Effects of prenatal medical food versus stan
Effect
Hgb at initiation of prenatal care, mean (SD), g/dLHgb at end of second trimester, mean (SD), g/dLHgb at delivery, mean (SD), g/dLRelative Hgb changes from initial to end of secondtrimester, mean (SD), %Relative Hgb changes from initial to delivery, mean (SIncidence of anemia, no. (%)Incidence of preeclampsia, no. (%)
Hgb � hemoglobin.
208
Adherence to prenatal regimen was assessedthrough a self-report interview throughout pregnancyand was extremely high; 100% of patients taking theprenatal medical food reported being compliant. Twopatients (3.7%) were not compliant in the PNV group,but the differences between the groups were notsignificant.
DISCUSSIONAlthough the study groups were not matched on a pa-tient-to-patient basis, the baseline demographics andcharacteristics of the groups were similar, consideringthat the small but statistically significant age difference
l Medical Foodn � 58)
Prenatal Vitamins(n � 54) P
.0 (4.6) 28.8 (3.5) 0.024
.1 (6.5) 31.7 (8.9) 0.091
35 (60.3) 24 (44.4) 0.30417 (29.3) 25 (46.3)
6 (10.4) 5 (9.3)
.0 (1.9) 7.9 (1.9) 0.690
.6 (1.2) 37.6 (1.1) 0.969
Alaska Native.
prenatal vitamins.
Prenatal Medical Food(n � 58)
Prenatal Vitamins(n � 54) P
12.4 (1.2) 12.1 (1.2) 0.12411.8 (1.1) 11.3 (1.2) 0.01111.8 (1.3) 10.7 (1.2) 0.001
�4.5 (10) �6.6 (6.2) 0.174�4.0 (12.8) �10.9 (7.4) 0.001
23 (39.7) 40 (74.1) 0.0016 (10.3) 9 (16.7) 0.409
enata(
2729
837
dian/
dard
D), %
Volume 33 Number 2

mit
gPioTipss
rtasvtstanssrsimhwc
mtr
S. Bentley et al.
between the groups is perhaps not clinically significant.The present study found that mean hemoglobin valuesin the prenatal medical food group were significantlyhigher at the end of the second trimester and at deliverycompared with the standard PNV group (P � 0.011and P � 0.001, respectively) (Figure). There were alsofewer incidences of anemia in the prenatal medicalfood group. These findings suggest that the prenatalmedical food formulation containing L-methylfolateand high-dose vitamin B12 may support erythropoiesis
ore effectively and reduce the need for additionalron supplements, but controlled studies are warrantedo test this hypothesis.
Fewer pregnant women in the prenatal medical foodroup developed preeclampsia compared with theNV group, but the results were not statistically signif-
cant, precluding any conclusions regarding the effectf prenatal medical food on preventing preeclampsia.he potential effect of the prenatal medical food on
ncidence of preeclampsia should be studied in a largeratient group. High compliance rates in both groupsuggest that the prenatal medical food caplets and cap-
Figure. Mean hemoglobin levels throughout preg-nancy in this retrospective study of the ef-fectiveness of prenatal medical food versusstandard prenatal vitamins (PNVs) on he-moglobin levels and adverse outcomes.ACOG � American College of Obstetri-cians and Gynecologists.
ules and PNVs are well tolerated.
February 2011
The present study is limited by its open-label, non-andomized, retrospective design. There is likely selec-ion bias due to different prenatal prescribing practicest each site, as well as due to the inclusion and exclu-ion criteria for age, gestational age at first prenatalisit, and additional iron supplementation. Because pa-ients were excluded for having taken additional ironupplements before hemoglobin screening at the end ofhe second trimester, selection may have been biasedgainst patients with a history of anemia during preg-ancy, which may have influenced the results of thetudy. Although charts were reviewed from multipleites and states, the study population may not be rep-esentative of the general population of pregnant per-ons. To confirm these results, more research is neededn a larger population. Minor differences in iron, vita-in B6, zinc, and other ingredients were assumed toave a negligible effect on study outcome. However,e acknowledge that these differences in formulation
ould not be fully controlled for in the present study.
CONCLUSIONThe results of this study suggest that beginning prena-tal care with a prenatal medical food containing L-methylfolate (the active form of folate) and high-dosevitamin B12 may be more effective in maintaining he-
oglobin levels and reducing the risk of anemiahroughout pregnancy; however, further study isequired.
ACKNOWLEDGMENTSThis research was funded by Pamlab, LLC, whichhad noncontrolling involvement in the study designbut not in the collection, analysis, or interpretationof data. The authors have indicated that they haveno other conflicts of interest regarding the content ofthis article.
Ms. Bentley proposed the overall design, includ-ing study groups and assessment of hemoglobin lev-els and anemia incidence; Pamlab, LLC, added theassessment of preeclampsia incidence. Ms. Bentley,Ms. Hermes, and Ms. Phillips reviewed charts attheir respective practices and submitted the recordeddata for statistical analysis, which was performed byMr. Daoud. Dr. Hanna authored significant portionsof the manuscript, in addition to Ms. Bentley. Pam-lab, LLC, did not restrict publication or dissemina-tion of the results of this study but reviewed the
manuscript before submission. Ms. Bentley, the pri-209

1
1
1
1
1
1
12
2
2
2
Clinical Therapeutics
mary author, had final approval of the manuscriptand publication.
REFERENCES1. World Health Organization. The Prevalence of Anaemia in
Women: A Tabulation of Available Information. 2nd ed. Geneva,Switzerland: World Health Organization 1992.
2. Pitkin RM. Nutritional influences during pregnancy. MedClin North Am. 1977;61:3–15.
3. Scanlon KS, Yip R, Schieve LA, Cogswell ME. High and lowhemoglobin levels during pregnancy: Differential risks forpreterm birth and small for gestational age. Obstet Gynecol.2000;96(5 Pt 1):741–748.
4. Xiong X, Buekens P, Alexander S, et al. Anemia duringpregnancy and birth outcome: A meta-analysis. Am JPerinatol. 2000;17:137–146.
5. Pena-Rosas JP, Viteri FE. Effects of routine oral ironsupplementation with or without folic acid for womenduring pregnancy. Cochrane Database Syst Rev. 2006;3:CD004736.
6. Hyder SM, Persson LA, Chowdhury AM, Ekström EC. Doside-effects reduce compliance to iron supplementation? Astudy of daily- and weekly-dose regimens in pregnancy.J Health Popul Nutr. 2002;20:175–179.
7. Koury MJ, Ponka P. New insights into erythropoiesis: Theroles of folate, vitamin B12, and iron. Annu Rev Nutr.2004;24:105–131.
8. Tamura T, Picciano MF. Folate and human reproduction.Am J Clin Nutr. 2006;83:993–1016.
9. Molloy AM, Daly S, Mills JL, et al. Thermolabile variantof 5,10-methylenetetrahydrofolate reductase associatedwith low red-cell folates: Implications for folate intakerecommendations. Lancet. 1997;349:1591–1593.
10. Philip S. Hematological complications of pregnancy. In:Gabbe SG, Niebyl JR, Simpson JL, eds. Obstetrics: Normal andProblem Pregnancies. 4th ed. New York, NY: Churchill Living-stone; 2002:1176–1179.
11. Lumley J, Watson L, Watson M, Bower C. Periconceptional
supplementation with folate and/or multivitamins forbellsouth.net
210
preventing neural tube defects. Cochrane Database Syst Rev.2001;3:CD001056.
12. Lindblad B, Zaman S, Malik A, et al. Folate, vitamin B12, andhomocysteinelevels inSouthAsianwomenwithgrowth-retardedfetuses.ActaObstetGynecolScand.2005;84:1055–1061.
3. Molloy AM, Kirke PN, Brody LC, et al. Effects of folate andvitamin B12 deficiencies during pregnancy on fetal, infant,and child development. Food Nutr Bull. 2008;29(Suppl2):S101–S111.
4. Zetterberg H. Methylenetetrahydrofolate reductase andtranscobalamin genetic polymorphisms in human sponta-neous abortion: Biological and clinical implications. Re-prod Biol Endocrinol. 2004;2:7.
5. Kirke PN, Molloy AM, Daly LE, et al. Maternal plasmafolate and vitamin B12 are independent risk factors forneural tube defects. Q J Med. 1993; 86:703–708.
6. Bennett M. Vitamin B12 deficiency, infertility and recurrentfetal loss. J Reprod Med. 2001;46:209–212.
7. Reznikoff-Etiévant MF, Zittoun J, Vaylet C, et al. Lowvitamin B(12) level as a risk factor for very early recurrentabortion. Eur J Obstet Gynecol Reprod Biol. 2002;104:156–159.
8. Ronnenberg AG, Goldman MB, Chen D, et al. Preconcep-tion homocysteine and B vitamin status and birth out-comes in Chinese women. Am J Clin Nutr. 2002;76:1385–1391.
9. Orphan Drug Act §5(b), 21 USC §360ee(b)(3) (1988).0. 56 Federal Register 60366 at 60377 (November 27, 1991);
Guidance for Industry: Frequently Asked Questions Ab-out Medical Foods, May 2007. http://www.fda.gov/Food/GuidanceComplianceRegulatoryInformation/GuidanceDocuments/MedicalFoods/ucm054048.htm.Accessed February 22, 2011.
1. Néevo [package insert]. Covington, La: Pamlab, LLC;2010.
2. NéevoDHA [package insert]. Covington, La: Pamlab, LLC;2010.
3. Office of Dietary Supplements, National Institutes ofHealth. Dietary Supplement Fact Sheet: Vitamin B12.http://ods.od.nih.gov/factsheets/vitaminb12/. Access-
ed January 31, 2010.Address correspondence to: Susan Bentley, WHNP-BC, Women’s ClinicShoals, 1100 S Jackson Highway, Sheffield, AL 35660. E-mail: subent@
Volume 33 Number 2