Embed Size (px)
Citation preview
Comparative Analysis of Renal Function afterTreatment of Infrarenal Abdominal AorticAneurysms with a Suprarenal FixationDevice as Opposed to Open Surgery
Jose Miguel Zaragoz�a Garcıa, Eduardo Ortiz Monzon, �Angel Plaza Martınez, Francisco Juli�an
Gomez Palones, Jose Ignacio Blanes Mompo, Johissy Lissethe Briones Estebanez, Carlos
Martınez Parreno, Bader Al-Raies Bolanos, Vicente Sala Almonacil, �Alvaro Torres Blanco,
Ignacio Crespo Moreno, and Inmaculada Martınez Perello, Valencia, Spain
We analyzed the repercussions on renal function between suprarenal endograft fixation andopen surgery in the treatment of infrarenal abdominal aortic aneurysms (IAAAs) and determinedthe influential factors. Between 1999 and 2005, 59 IAAAs were treated with elective OS and 56with SEF. The serum creatinine (Cr) level and its clearance were determined before the proce-dure, in the intensive care unit (ICU), on discharge, and after 1, 6, 12, and 24 months. A dete-rioration in renal function was considered to be a >30% increase in Cr or a Cr >2 mg/dL. Aunivariate statistical analysis and a logistical regression analysis were carried out to determinethe predictive factors for repercussions on renal function. There were no statistically significantdifferences in the rate of renal exacerbation between the groups either on discharge ( p ¼0.52) or after 1 month ( p ¼ 0.483), 6 months ( p ¼ 0.451), 12 months ( p ¼ 0.457), and 24 months( p ¼ 0.682). The only significant difference was that detected in the ICU ( p ¼ 0.033). Diabetesmellitus, time spent in the ICU, postoperative intubation time, intraoperative transfusion, andtransfusion in the ICU were factors that influenced the deterioration of renal function in the uni-variate analysis. The only significant factor in the multivariate analysis was the need for transfu-sion in the ICU. Exacerbation of renal function occurred in both groups independently oftreatment type. In the immediate postoperative period, hemodynamic deterioration is more fre-quent in the open surgery group. Renal exacerbation tended to disappear in both groups duringfollow-up.
INTRODUCTION
Since the first description of endovascular repair of
an infrarenal abdominal aortic aneurysm (IAAA)
in 1991 by Parodi et al.,1 the use of this technique
as a treatment option has spread in such a way
that it is currently more common than open surgery
(OS). Nevertheless, despite the enthusiasm it has
Vascular Surgery Department, Dr. Peset Hospital, Valencia, Spain.
Correspondence to: Jose Miguel Zaragoz�a Garcıa, MD, C/ Isabel deVillena 2,18. 46160 Llıria, Valencia, Spain, E-mail: [email protected]
Ann Vasc Surg 2008; 22: 513-519DOI: 10.1016/j.avsg.2008.02.013� Annals of Vascular Surgery Inc.Published online: May 27, 2008
generated, approximately one-third of patients con-
tinue to be considered unsuitable for endograft. The
limitations for endovascular treatment are deter-
mined by IAAA anatomy, including inadequate
proximal fixation of the graft and the small size of
the iliac.2 Although there have been important ad-
vances in release devices, as well as in the endograft
itself, the excessive angle on the proximal neck and
its length are still limiting factors.
Despite the fact that recent clinical trials have
suggested that the risks associated with endovascu-
lar repair of IAAA are less than those for OS, there
is still great concern regarding durability.3,4 The in-
cidence of endograft migration and/or endoleak is
>30% in some cases,5,6 and these are often respon-
sible for the continued risk of aneurysm rupture that
513

514 Garcıa et al. Annals of Vascular Surgery
occurs in >1% annually.5,7 Suprarenal fixation
with uncovered stent has been proposed as a method
that could improve proximal fixation, allowing the
repair of necks with complex morphology or that
are short, thereby reducing the risk of later compli-
cations (migration, endoleak formation, and rup-
ture of the aneurysm).
Fixing the endograft to the suprarenal aorta re-
quires the insertion of a transrenal stent. It has
been implied that the effect of the stent clamps pass-
ing through the ostium of the renal arteries is a factor
in potential renal function deterioration. At the
same time, patients who undergo this type of treat-
ment are already at high risk of developing renal
complications given that they are of advanced age
and therefore have associated increased risk factors
and comorbidity. Also, many of them are diabetics
or have a history of previous renal insufficiency
(RI), which carries a greater risk. Therefore, deterio-
ration in renal function after endovascular repair of
IAAA can reach>20%, and the causes are normally
multifactoral, including mechanical causes, the ad-
ministration of nephrotoxic contrast agents, and
renal atheroembolism.8
With regard to OS, RI is the third most common
complication after treatment,9 and its presence is
a strong predictor of poor life expectancy.10 The
only independent predictive factor that has been
related to RI after surgical treatment of an IAAA is
previous RI.11 Despite precaution in preoperative
administration of intravenous contrast, intraopera-
tive administration of diuretic agents, and special
care with the placement and timing of the aortic
clamp, the incidence of postoperative RI is still sig-
nificant at about 6%, with a mortality rate of
28%.9,12 The deterioration in renal function in OS
of the IAAA has been attributed to atheroembolism,
renal ischemia, intraoperative hypertension in the
context of a hemodynamic deterioration, and tech-
nical factors related to renal arteries.13,14
We analyzed the repercussions of suprarenal en-
dograft fixation (SEF) on renal function compared
with OS in the treatment of IAAA and determined
the influential factors.
METHODS
Between 1999 and 2005, 160 IAAAs were treated in
our center, of which 59 were treated with elective
OS and 101 endovascularly, 59 of the latter
(58.4%) with Zenith� (Cook, Bloomington, IN)
SEF. Demographic data of the patients were col-
lected retrospectively in both groups and are shown
in Table I. One hundred percent of the patients were
male. In the SEF group, three patients had terminal
RI with periodic hemodialysis and were therefore
excluded from the study.
The suprarenal component of the Zenith endog-
raft is made up of 0.018-inch stainless steel wires;
the uncovered part is 26 mm long and is made up
of 10 or 12 supports (10 supports for diameters
<28 mm 12 supports for diameters �28 mm).
Each support ends distally in a 5 cm- or 0.093
inch-long hook. The suprarenal component is fixed
to the polyester graft with a monofilament stitch.
Treatment techniques for IAAA through SEF or
OS have already been described in other stud-
ies.15,16 The study of renal function in both groups
included establishing the concentration of serum
creatinine (Cr) prior to treatment, in the intensive
care unit (ICU), on discharge, and after 1-, 6-, 12-,
and 24-month follow-up. A study of the permeabil-
ity of the renal arteries as well as the detection of re-
nal hemorrhage was carried out through computed
tomography (CT) on discharge and after 1, 6, 12,
and 24 months.
To adjust the Cr figures to the age and weight of
the patients, Cr clearing (CrC) was calculated using
the Cockgraft-Gault formula: (140 � age) x weight/
Cr x 72.17-20 Exacerbation of renal function was de-
fined in our study as an increase>30% of Cr prior to
treatment or a value of Cr>2 mg/dL. Permeability of
the renal arteries was defined as continuity of con-
trast flow in the CT between the aorta and the
main renal artery. Data were also collected on sec-
ondary treatment carried out during the follow-up
related to renal problems as well as the need for
hemodialysis in any of the patients.
Regarding statistical analysis, dispersion mea-
surements were expressed as the mean ± standard
deviation, and those variables with extreme values
that could compromise the mean (amount of bleed-
ing and postoperative intubation time) were ex-
pressed as the median. Contingency tables with
the c2 test and the difference of proportions test
compared category and nominal variables of two in-
dependent samples, respectively; and the Mann-
Whitney U-test was used to analyze nonparametric
variables. Analysis of variance was applied to com-
pare the means or medians. For factors predictive
of the effects on renal function, a univariate analysis
was conducted using the c2 test and the Fisher test
for category variables and the Mann-Whitney U-
test for continuous variables. Later, a multivariate
analysis was carried out using logistic regression, af-
ter cataloguing the variables that were significant in
the univariate study, in order to determine those
variables with more specific weight as risk factors
for renal function deterioration. All results were
Vol. 22, No. 4, 2008 Analysis of renal function after treatment of AAA 515
Table I. Demographic data for SEF and OS groups
SEF group (n ¼ 56) OS group (n ¼ 59) p
Age (years) 72 (range 51-83) 66 (range 56-81) 0.385
Smoking 21.4% (n ¼ 12) 34% (n ¼ 20) 0.279
Diabetes mellitus 7.1% (n ¼ 4) 11.8% (n ¼ 7) 0.349
Arterial hypertension 73.2% (n ¼ 41) 72.8% (n ¼ 43) 0.600
Dyslipidemia 32.1% (n ¼ 18) 25.4% (n ¼ 15) 0.269
Hyperuricemia 10.7% (n ¼ 6) 8.4% (n ¼ 5) 0.519
Ischemic heart disease 35.7% (n ¼ 20) 28.8% (n ¼ 17) 0.468
Coronary surgery/stent 8.9% (n ¼ 5) 10.2% (n ¼ 6) 0.537
Other heart diseases 21.4% (n ¼ 12) 8.4% (n ¼ 5) 0.044
Previous CVA 12.5% (n ¼ 7) 6.7% (n ¼ 4) 0.235
COPD 26.7% (n ¼ 15) 18.6% (n ¼ 11) 0.206
GDU 10.7% (n ¼ 6) 13.5% (n ¼ 8) 0.429
Previous RI 12.5% (n ¼ 7) 6.7% (n ¼ 4) 0.235
Single kidney 7.1% (n ¼ 4) 5.1% (n ¼ 3) 0.471
ASA IV 76.7% (n ¼ 43) 37.2% (n ¼ 22) 0.001
CVA, cerebrovascular accident; COPD, chronic obstructive pulmonary disease; GDU, gastroduodenal ulcer.
analyzed using SPSS statistical software (SPSS, Inc.,
Chicago, IL).
RESULTS
The two groups were compared in advance; there
were no significant statistical differences in age,
risk factors, or prevalence of comorbidities except
for the prevalence of other, nonischemic heart dis-
eases ( p ¼ 0.044) and the anesthetic risk value
(greater prevalence of American Society of Anes-
thesiologists [ASA] IV in the SEF group with p ¼0.001) (Table I). The mean follow-up was 20 ±
15.7 months for the SEF group and 36.2 ± 17.7
months for the OS group. There were 13 follow-
up losses (11.3%), all of which were from the SEF
group and 10 of which were patients from other
health-care areas who preferred to carry out
follow-up tests in their own hospitals, as well as
those we were not able to contact by telephone;
the other three patients refused the CT tests and
analysis. Mean time in surgery was 190 ± 51 min
in the SEF group and 204 ± 59 min in the OS group,
and there were no significant statistical differences
between the groups ( p¼ 0.193). The mean contrast
dose used in the SEF group was 222 ± 82 mL. There
was no association between the amount of contrast
used and the degree of renal function exacerbation
in the SEF group. The mean aortic clamp time was
61.3 ± 21.2 min in the OS group. The suprarenal
clamp was only necessary in two cases (3.3%). Su-
prarenal aortic clamping did not influence the de-
gree of renal function exacerbation. The median
volume of bleeding was 250 mL for the SEF group
and 1,000 mL for the OS group, which is a statisti-
cally significant difference ( p ¼ 0.01). Intraopera-
tive blood transfusion was necessary in 28.5% of
cases in the SEF group (n ¼ 16), while in the OS
group it was needed in 81.3% of cases (n ¼ 48) ( p
< 0.001). The mean packed red blood cells trans-
fused in surgery in the SEF group was 0.7 and
that in the OS group, 2.8 ( p < 0.001). The median
postoperative intubation time was 0 hr in the SEF
group (most of the patients who underwent general
anesthetic were extubated in the operating theater),
while in the OS group it was 5 hr ( p ¼ 0.097). The
mean stay in the ICU was 1.2 ± 0.7 days in the SEF
group and 3.4 ± 2.8 days in the OS group ( p ¼0.018). A blood transfusion in the ICU was neces-
sary in 23.2% of cases in the SEF group (n ¼ 13),
while in the OS group it was necessary in 23.7%
of cases (n ¼ 14) ( p ¼ 0.562). The mean packed
red blood cells transfused in surgery in the SEF
group was 0.7 and that in the OS group, 0.8 ( p ¼0.665). The mean stay in hospital was 6.9 ± 3.2
days in the SEF group and 10.5 ± 8 days in the OS
group ( p ¼ 0.024). Postoperative morbidity was
1.7% in the SEF group (n ¼ 1) and 1.6% in the
OS group (n ¼ 1) ( p ¼ 0.634).
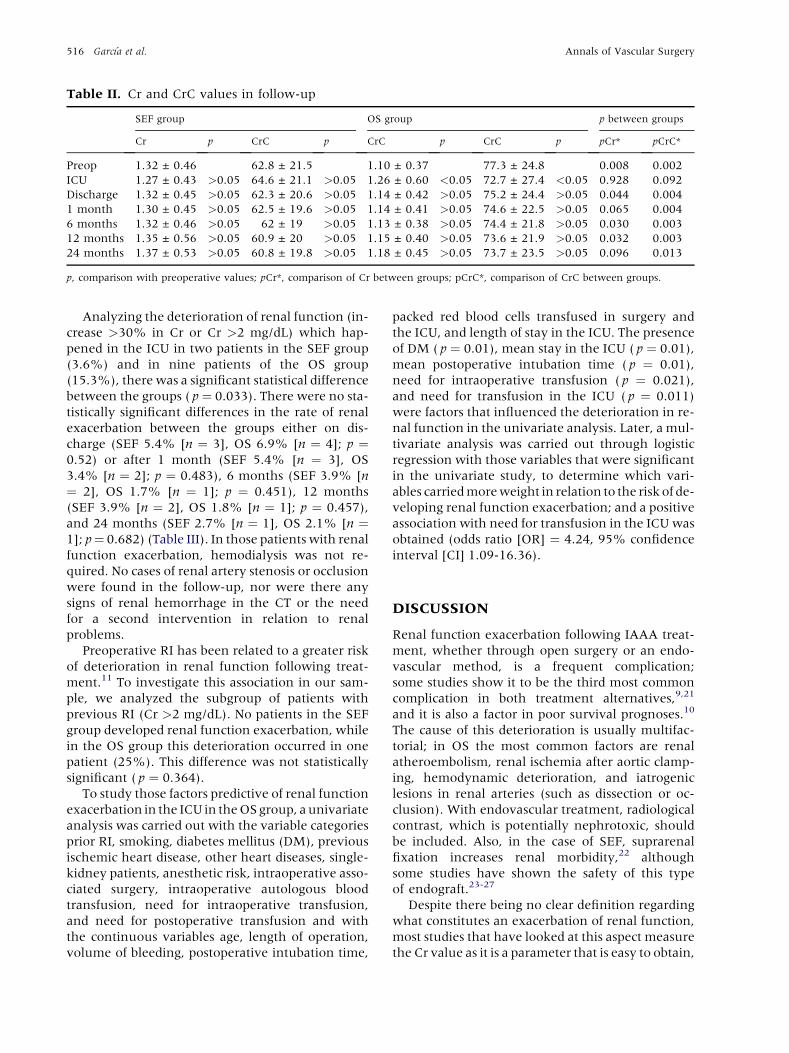
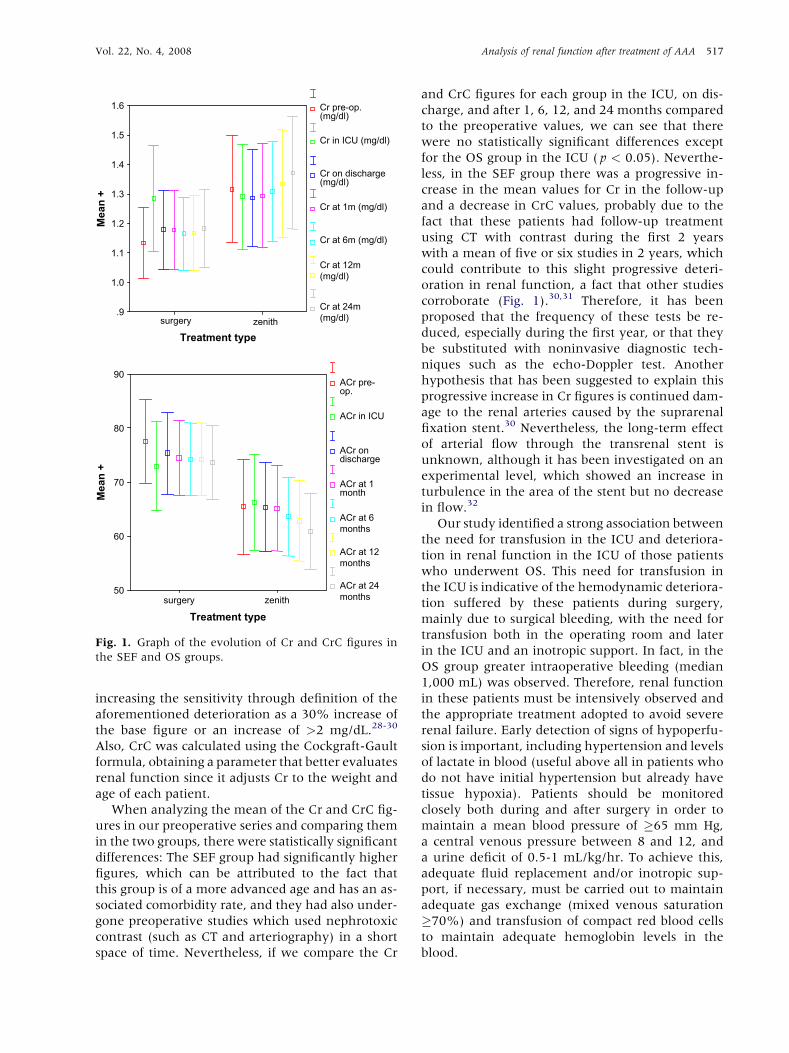
Table II shows the mean values for Cr and CrC.
Comparing Cr and CrC in the ICU and after 1, 6,
12, and 24 months with respect to the preoperative
Cr and CrC in each group, there were no significant
statistical differences, except in the Cr and CrC fig-
ures in the ICU of the OS group ( p < 0.05). Despite
the fact that there were no differences in the SEF
group, we observed an increasing tendency in Cr
and a decreasing tendency in CrC in the follow-
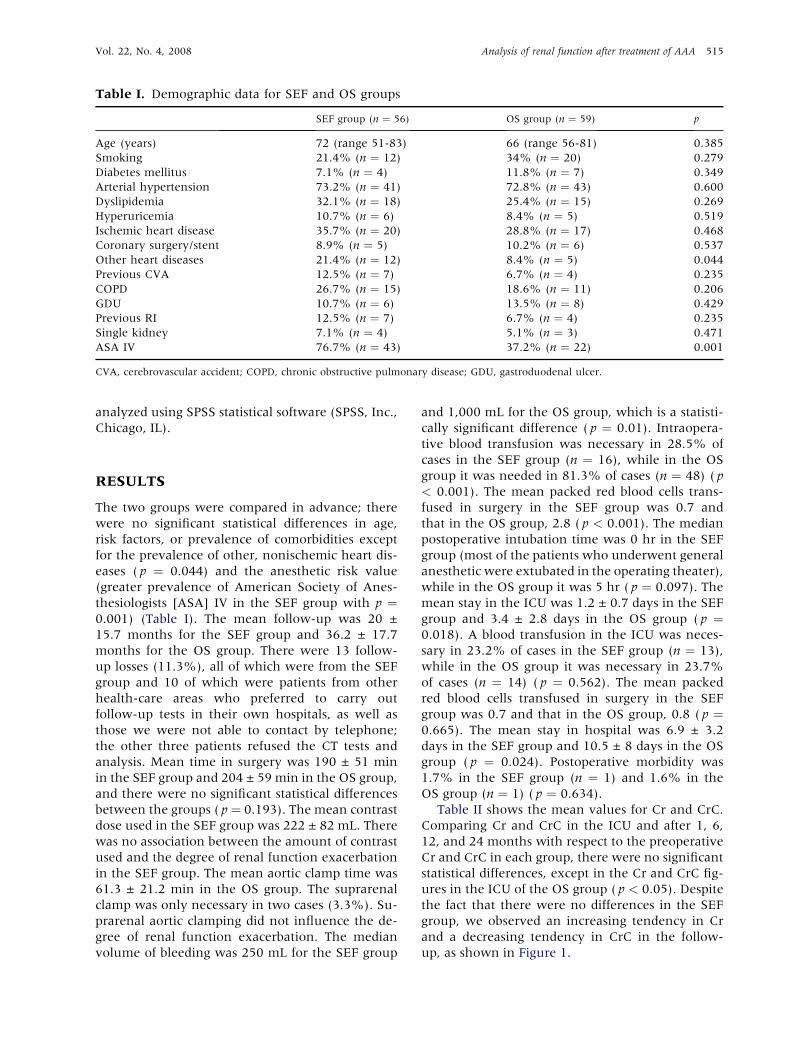
up, as shown in Figure 1.
516 Garcıa et al. Annals of Vascular Surgery
Table II. Cr and CrC values in follow-up
SEF group OS group p between groups
Cr p CrC p CrC p CrC p pCr* pCrC*
Preop 1.32 ± 0.46 62.8 ± 21.5 1.10 ± 0.37 77.3 ± 24.8 0.008 0.002
ICU 1.27 ± 0.43 >0.05 64.6 ± 21.1 >0.05 1.26 ± 0.60 <0.05 72.7 ± 27.4 <0.05 0.928 0.092
Discharge 1.32 ± 0.45 >0.05 62.3 ± 20.6 >0.05 1.14 ± 0.42 >0.05 75.2 ± 24.4 >0.05 0.044 0.004
1 month 1.30 ± 0.45 >0.05 62.5 ± 19.6 >0.05 1.14 ± 0.41 >0.05 74.6 ± 22.5 >0.05 0.065 0.004
6 months 1.32 ± 0.46 >0.05 62 ± 19 >0.05 1.13 ± 0.38 >0.05 74.4 ± 21.8 >0.05 0.030 0.003
12 months 1.35 ± 0.56 >0.05 60.9 ± 20 >0.05 1.15 ± 0.40 >0.05 73.6 ± 21.9 >0.05 0.032 0.003
24 months 1.37 ± 0.53 >0.05 60.8 ± 19.8 >0.05 1.18 ± 0.45 >0.05 73.7 ± 23.5 >0.05 0.096 0.013
p, comparison with preoperative values; pCr*, comparison of Cr between groups; pCrC*, comparison of CrC between groups.
Analyzing the deterioration of renal function (in-
crease >30% in Cr or Cr >2 mg/dL) which hap-
pened in the ICU in two patients in the SEF group
(3.6%) and in nine patients of the OS group
(15.3%), there was a significant statistical difference
between the groups ( p¼ 0.033). There were no sta-
tistically significant differences in the rate of renal
exacerbation between the groups either on dis-
charge (SEF 5.4% [n ¼ 3], OS 6.9% [n ¼ 4]; p ¼0.52) or after 1 month (SEF 5.4% [n ¼ 3], OS
3.4% [n ¼ 2]; p ¼ 0.483), 6 months (SEF 3.9% [n
¼ 2], OS 1.7% [n ¼ 1]; p ¼ 0.451), 12 months
(SEF 3.9% [n ¼ 2], OS 1.8% [n ¼ 1]; p ¼ 0.457),
and 24 months (SEF 2.7% [n ¼ 1], OS 2.1% [n ¼1]; p¼ 0.682) (Table III). In those patients with renal
function exacerbation, hemodialysis was not re-
quired. No cases of renal artery stenosis or occlusion
were found in the follow-up, nor were there any
signs of renal hemorrhage in the CT or the need
for a second intervention in relation to renal
problems.
Preoperative RI has been related to a greater risk
of deterioration in renal function following treat-
ment.11 To investigate this association in our sam-
ple, we analyzed the subgroup of patients with
previous RI (Cr >2 mg/dL). No patients in the SEF
group developed renal function exacerbation, while
in the OS group this deterioration occurred in one
patient (25%). This difference was not statistically
significant ( p ¼ 0.364).
To study those factors predictive of renal function
exacerbation in the ICU in the OS group, a univariate
analysis was carried out with the variable categories
prior RI, smoking, diabetes mellitus (DM), previous
ischemic heart disease, other heart diseases, single-
kidney patients, anesthetic risk, intraoperative asso-
ciated surgery, intraoperative autologous blood
transfusion, need for intraoperative transfusion,
and need for postoperative transfusion and with
the continuous variables age, length of operation,
volume of bleeding, postoperative intubation time,
packed red blood cells transfused in surgery and
the ICU, and length of stay in the ICU. The presence
of DM ( p ¼ 0.01), mean stay in the ICU ( p ¼ 0.01),
mean postoperative intubation time ( p ¼ 0.01),
need for intraoperative transfusion ( p ¼ 0.021),
and need for transfusion in the ICU ( p ¼ 0.011)
were factors that influenced the deterioration in re-
nal function in the univariate analysis. Later, a mul-
tivariate analysis was carried out through logistic
regression with those variables that were significant
in the univariate study, to determine which vari-
ables carried more weight in relation to the risk of de-
veloping renal function exacerbation; and a positive
association with need for transfusion in the ICU was
obtained (odds ratio [OR] ¼ 4.24, 95% confidence
interval [CI] 1.09-16.36).
DISCUSSION
Renal function exacerbation following IAAA treat-
ment, whether through open surgery or an endo-
vascular method, is a frequent complication;
some studies show it to be the third most common
complication in both treatment alternatives,9,21
and it is also a factor in poor survival prognoses.10
The cause of this deterioration is usually multifac-
torial; in OS the most common factors are renal
atheroembolism, renal ischemia after aortic clamp-
ing, hemodynamic deterioration, and iatrogenic
lesions in renal arteries (such as dissection or oc-
clusion). With endovascular treatment, radiological
contrast, which is potentially nephrotoxic, should
be included. Also, in the case of SEF, suprarenal
fixation increases renal morbidity,22 although
some studies have shown the safety of this type
of endograft.23-27
Despite there being no clear definition regarding
what constitutes an exacerbation of renal function,
most studies that have looked at this aspect measure
the Cr value as it is a parameter that is easy to obtain,
Vol. 22, No. 4, 2008 Analysis of renal function after treatment of AAA 517
increasing the sensitivity through definition of the
aforementioned deterioration as a 30% increase of
the base figure or an increase of >2 mg/dL.28-30
Also, CrC was calculated using the Cockgraft-Gault
formula, obtaining a parameter that better evaluates
renal function since it adjusts Cr to the weight and
age of each patient.
When analyzing the mean of the Cr and CrC fig-
ures in our preoperative series and comparing them
in the two groups, there were statistically significant
differences: The SEF group had significantly higher
figures, which can be attributed to the fact that
this group is of a more advanced age and has an as-
sociated comorbidity rate, and they had also under-
gone preoperative studies which used nephrotoxic
contrast (such as CT and arteriography) in a short
space of time. Nevertheless, if we compare the Cr
Treatment type
zenithsurgery
Mean
+
90
80
70
60
50
ACr pre-op.
ACr in ICU
ACr on discharge
ACr at 1month
ACr at 6 months
ACr at 12 months
ACr at 24 months
Treatment type
zenithsurgery
Mean
+
1.6
1.5
1.4
1.3
1.2
1.1
1.0
.9
Cr pre-op.(mg/dl)
Cr in ICU (mg/dl)
Cr on discharge (mg/dl)
Cr at 1m (mg/dl)
Cr at 6m (mg/dl)
Cr at 12m (mg/dl)
Cr at 24m(mg/dl)
Fig. 1. Graph of the evolution of Cr and CrC figures in
the SEF and OS groups.
and CrC figures for each group in the ICU, on dis-
charge, and after 1, 6, 12, and 24 months compared
to the preoperative values, we can see that there
were no statistically significant differences except
for the OS group in the ICU ( p < 0.05). Neverthe-
less, in the SEF group there was a progressive in-
crease in the mean values for Cr in the follow-up
and a decrease in CrC values, probably due to the
fact that these patients had follow-up treatment
using CT with contrast during the first 2 years
with a mean of five or six studies in 2 years, which
could contribute to this slight progressive deteri-
oration in renal function, a fact that other studies
corroborate (Fig. 1).30,31 Therefore, it has been
proposed that the frequency of these tests be re-
duced, especially during the first year, or that they
be substituted with noninvasive diagnostic tech-
niques such as the echo-Doppler test. Another
hypothesis that has been suggested to explain this
progressive increase in Cr figures is continued dam-
age to the renal arteries caused by the suprarenal
fixation stent.30 Nevertheless, the long-term effect
of arterial flow through the transrenal stent is
unknown, although it has been investigated on an
experimental level, which showed an increase in
turbulence in the area of the stent but no decrease
in flow.32
Our study identified a strong association between
the need for transfusion in the ICU and deteriora-
tion in renal function in the ICU of those patients
who underwent OS. This need for transfusion in
the ICU is indicative of the hemodynamic deteriora-
tion suffered by these patients during surgery,
mainly due to surgical bleeding, with the need for
transfusion both in the operating room and later
in the ICU and an inotropic support. In fact, in the
OS group greater intraoperative bleeding (median
1,000 mL) was observed. Therefore, renal function
in these patients must be intensively observed and
the appropriate treatment adopted to avoid severe
renal failure. Early detection of signs of hypoperfu-
sion is important, including hypertension and levels
of lactate in blood (useful above all in patients who
do not have initial hypertension but already have
tissue hypoxia). Patients should be monitored
closely both during and after surgery in order to
maintain a mean blood pressure of �65 mm Hg,
a central venous pressure between 8 and 12, and
a urine deficit of 0.5-1 mL/kg/hr. To achieve this,
adequate fluid replacement and/or inotropic sup-
port, if necessary, must be carried out to maintain
adequate gas exchange (mixed venous saturation
�70%) and transfusion of compact red blood cells
to maintain adequate hemoglobin levels in the
blood.

518 Garcıa et al. Annals of Vascular Surgery
Table III. Renal exacerbation rate in the two groups
Renal exacerbation rate
ICU Discharge 1 month 6 months 12 months 24 months
OS group 15.3% (n ¼ 9/59) 6.9% (n ¼ 4/58) 3.4% (n ¼ 2/58) 1.7% (n ¼ 1/58) 1.8% (n ¼ 1/56) 2.1% (n ¼ 1/47)
SEF group 3.6% (n ¼ 2/56) 5.4% (n ¼ 3/56) 5.4% (n ¼ 3/56) 3.9% (n ¼ 2/51) 3.9% (n ¼ 2/51) 2.7% (n ¼ 1/36)
p 0.033 0.52 0.483 0.451 0.457 0.682
CONCLUSIONS
Exacerbation of renal function occurred in both
groups independently of treatment type. In the im-
mediate postoperative period, this deterioration was
most frequent in the OS group, probably related to
the hemodynamic deterioration. In follow-up, this
deterioration tended to disappear in both groups, al-
though the Cr figures showed a constant increase in
the SEF group, probably due to the repeated diag-
nostic tests that use contrast and the effect of the
suprarenal fixation stent. Multicenter randomized
prospective studies would be needed to confirm
this hypothesis.
REFERENCES
1. Parodi JC, Palmaz JC, Barone HD. Transfemoral intralumi-
nal graft implantation for abdominal aortic aneurysms.
Ann Vasc Surg 1991;5:491-499.
2. Carpenter JP, Baum RA, Barker CF, et al. Impact of exclu-
sion criteria on patient selection for endovascular abdominal
aortic aneurysm repair. J Vasc Surg 2001;34:1050-1054.
3. Greenhalgh RM, Brown LC, Kwong GP, et al. Comparison of
endovascular aneurysm repair with open repair in patients
with abdominal aortic aneurysm (EVAR trial 1), 30-day op-
erative mortality results: randomised controlled trial. Lancet
2004;364:843-848.
4. Prinssen M, Verhoeven EL, Buth J, et al. A randomized trial
comparing conventional and endovascular repair of abdom-
inal aortic aneurysms. N Engl J Med 2004;351:1607-1608.
5. Zarins CK. The US AneuRx clinical trial: 6-year clinical up-
date 2002. J Vasc Surg 2003;37:904-908.
6. Carpenter JP. Midterm results of the multicenter trial of the
powerlink bifurcated system for endovascular aortic aneu-
rysm repair. J Vasc Surg 2004;40:849-859.
7. Harris PL, Vallabhaneni SR, Desgranges P, et al. Incidence
and risk factors of late rupture, conversion, and death after
endovascular repair of infrarenal aortic aneurysms: the
EUROSTAR experience. European Collaborators on Stent/
Graft Techniques for Aortic Aneurysm Repair. J Vasc Surg
2000;32:739-749.
8. Carpenter JP, Fairman RM, Barker CF, et al. Endovascular
AAA repair in patients with renal insufficiency: strategies
for reducing adverse renal events. Cardiovasc Surg 2001;9:
559-564.
9. Johnston K. Multicenter prospective study of nonruptured
abdominal aortic aneurysm. II: Variables in predicting mor-
bidity and mortality. J Vasc Surg 1989;9:437-447.
10. Hertzer NR, Mascha EJ, Karafa MT, et al. Open infrarenal ab-
dominal aortic aneurysm repair: the Cleveland Clinic experi-
ence from 1989 to 1998. J Vasc Surg 2002;35:1145-1154.
11. Miller D, Meyers B. Pathophysiology and prevention of re-
nal failure associated with thoracoabdominal or abdominal
aortic surgery. J Vasc Surg 1987;5:518-523.
12. Johnston K, Scobie T. Multicenter prospective study of non-
ruptured abdominal aortic aneurysms. I: Population and
operative management. J Vasc Surg 1988;7:69-81.
13. Moore WS. The EVT tube and bifurcated endograft systems:
technical considerations and clinical summary. EVI Investi-
gators. J Endovasc Surg 1997;4:182-194.
14. Matsumura J, Brewster D, Makaroun M, et al. A multicenter
controlled clinical trial of open versus endovascular treat-
ment of abdominal aortic aneurysm. J Vasc Surg 2003;37:
262-271.
15. Greenberg R. The Zenith AAA endovascular graft for ab-
dominal aortic aneurysms: clinical update. Semin Vasc
Surg 2003;16:151-157.
16. Lawrence-Brown M, Sieunarine K, Hartley D, et al. The
Perth HLB bifurcated endoluminal graft: a review of the ex-
perience and intermediate results. Cardiovasc Surg 1998;6:
225-229.
17. Levey AS, Bosch JP, Lewis JB, et al. A more accurate method
to estimate glomerular filtration rate from serum creatinine:
a new prediction equation. Modification of Diet in Renal Dis-
ease Study Group. Ann Intern Med 1999;130:461-470.
18. Kurnik BR, Allgren RL, Genter FC, et al. Prospective study of
atrial natriuretic peptide for the prevention of radiocontrast-
induced nephropathy. Am J Kidney Dis 1998;31:674-680.
19. Levy EM, Viscoli CM, Horwitz RI. The effect of acute renal
failure on mortality: a cohort analysis. JAMA 1996;275:
1489-1494.
20. Cockcraft D, Gault M. Prediction of creatinine clearance
from serum creatinine. Nephron 1976;16:31-41.
21. Greenberg R, Chuter T, Sternbergh WC, et al. Zenith endo-
vascular graft: intermediate-term results of the US multicen-
ter trial. J Vasc Surg 2002;39:1209-1218.
22. Bove PG, Long GW, Shanley CJ, et al. Transrenal fixation of
endovascular stent-grafts for infrarenal aortic aneurysm
repair: mid-term results. J Vasc Surg 2003;37:938-942.
23. Alric P, Hinchliffe RJ, Picot MC, et al. Long-term renal func-
tion following endovascular aneurysm repair with infrare-
nal and suprarenal aortic stent-grafts. J Endovasc Ther
2003;10:397-405.
24. Lau LL, Hakaim AG, Oldenburg WA, et al. Effect of suprare-
nal versus infrarenal aortic endograft fixation on renal func-
tion and renal artery patency: a comparative study with
intermediate follow-up. J Vasc Surg 2003;37:1162-1168.
25. Malina M, Lindh M, Ivancev K, et al. The effect of endovas-
cular aortic stents placed across the renal arteries. Eur J Vasc
Endovasc Surg 1997;13:207-213.
26. Marin ML, Parsons RE, Hollier LH, et al. Impact of trans-
renal aortic endograft placement on endovascular graft

Vol. 22, No. 4, 2008 Analysis of renal function after treatment of AAA 519
repair of abdominal aortic aneurysms. J Vasc Surg
1998;28:638-646.
27. Morrissey NJ, Faries PL, Teodorescu V, et al. Transrenal bare
stents in endovascular treatment of abdominal aortic aneu-
rysms. J Invasive Cardiol 2002;14:36-40.
28. Faries PL, Brener BJ, Connelly TL, et al. A multicenter experi-
ence with the Talent endovascular graft for the treatment of
abdominal aortic aneurysms. J Vasc Surg 2002;35:1123-1128.
29. Parmer SS, Carpenter JP. Endovascular aneurysm repair
with suprarenal vs. infrarenal fixation: a study of renal
effects. J Vasc Surg 2006;43:19-25.
30. Greenberg RK, Chuter TAM, Lawrence-Brown M, et al. Anal-
ysis of renal function after aneurysm repair with a device using
suprarenal fixation (Zenith AAA endovascular graft) in con-
trast to open surgical repair. J Vasc Surg 2004;39:1219-1228.
31. Kichikawa K, Uchida H, Maeda M, et al. Aortic stent-graft-
ing with transrenal fixation: use of newly designed spiral
Z-stent endograft. J Endovasc Ther 2000;7:184-191.
32. Liffman K, Lawrence-Brown MM, Semmens JB, et al. Su-
prarenal fixation: effect on blood flow of an endoluminal
stent wire across an arterial orifice. J Endovasc Ther
2003;10:260-274.