Embed Size (px)
DESCRIPTION
bsava revista
Citation preview

The essential publication for BSAVA members
Clinical ConundrumLabrador with acute pelvic limb lamenessP10
How To……approach a smelly earP14
The essential publication for BSAVA members
companionSEPTEMBER 2010
Physio in practiceApproach to rehabilitationP21
Open wide – dental extraction in practice

2 | companion
companion
3 Association NewsLatest news from BSAVA
4–5 The Big PictureCongress gets a brand new look
6–9 Dental ExtractionAlexander Reiter describes what tooth extraction entails
10–13 Clinical ConundrumConsider a case of traumatic hind limb lameness
14–18 How To…Approach the smelly ear
19–20 An Exotic WinterA look at BSAVA’s forthcoming Exotics Mini Modular Course
21–23 PublicationsPhysical therapies in practice
24–25 PetsaversLatest fundraising news
26–28 WSAVA NewsThe World Small Animal Veterinary Association
29–30 The companion InterviewJohn Tandy
31 CPD DiaryWhat’s on in your area
Additional stock photography Dreamstime.com© Amwu; © Emprise; © Jocic; © Ragnarock; © Serdar Tibet; © Willeecole; © Yobro10; © Zts
companion is published monthly by the British Small Animal Veterinary Association, Woodrow House, 1 Telford Way, Waterwells Business Park, Quedgeley, Gloucester GL2 2AB. This magazine is a member only benefit and is not available on subscription. We welcome all comments and ideas for future articles.
Tel: 01452 726700Email: [email protected]
Web: www.bsava.com
ISSN: 2041-2487
Editorial BoardEditor – Mark Goodfellow MA VetMB CertVR DSAM DipECVIM-CA MRCVSSenior Vice-President – Richard Dixon BVMS PhD CertVR MRCVS FRSE
■ CPD Editorial TeamIan Battersby BVSc DSAM DipECVIM-CA MRCVSEsther Barrett MA VetMB DVDI DipECVDI MRCVSSimon Tappin MA VetMB CertSAM DipECVIM-CA MRCVS
■ Features Editorial TeamCaroline Bower BVM&S MRCVSAndrew Fullerton BVSc (Hons) MRCVS
■ Design and ProductionBSAVA Headquarters, Woodrow House
No part of this publication may be reproduced in any form without written permission of the publisher. Views expressed within this publication do not necessarily represent those of the Editor or the British Small Animal Veterinary Association.
For future issues, unsolicited features, particularly Clinical Conundrums, are welcomed and guidelines for authors are available on request; while the publishers will take every care of material received no responsibility can be accepted for any loss or damage incurred.
BSAVA is committed to reducing the environmental impact of its publications wherever possible and companion is printed on paper made from sustainable resources and can be recycled. When you have finished with this edition please recycle it in your kerbside collection or local recycling point. Members can access the online archive of companion at www.bsava.com .
All BSAVA memberships run from January to December, so it will soon be time to renew your membership for 2011. If you’ve not already set up a Direct Debit for your
membership, this is a great time to arrange it and save yourself some money at the same time.
Annual Direct Debit (DD) payments receive a £10 discount from the annual subscription fee – so not only is this the easiest way to make sure your membership is renewed promptly, it is also the most cost-effective.
As well as the annual DD option, there is also another Direct Debit payment plan being offered for the first time – you can pay monthly to spread the cost throughout the year. Conditions do apply, so see the website for more details.
We recently sent out Direct Debit forms to all members not currently using this easy option to renew their membership. As it isn’t possible to submit a DD application online, you should return these forms immediately. If you have not received them you can download them from www.bsava.com, or request them from [email protected]. If you have any questions our membership team will be happy to help – call 01452 726700, 9–5 Monday to Friday.
IMPORTANT DEADLINE: You only have until 29 October to change your membership payment to one of these Direct Debit plans. ■
Easiest membership renewalYou will soon need to renew your membership – set up an annual Direct Debit before 29 October to save £10…
PRACTICE NEWSLETTER – DID YOU GET YOURS?BSAVA recently sent their first newsletter for practices – principally a way of talking to practice managers and those principal people in your team who might otherwise not hear from us in other ways. We want to make sure that everyone is aware of what we can do for the whole practice and how we can help nurses and managers too. Did your practice manager get their copy? If so – make sure they return the reply slip as we might be able to help streamline some things for you – like membership renewal and Congress registrations. Email [email protected] if you have any questions. ■
Let us make life easierAs a busy practice manager you will have a lot of people to keep happy and your own busy workload to maintain. BSAVA would like to help, and this newsletter is the fi rst in a series designed purely for the practice manager. We hope that you will feel that the information is useful and perhaps will pin it on your notice board to highlight CPD courses, manuals, Congress, online resources and the range of benefi ts available to vets and nurses in your practice.
We appreciate that booking events for members of the practice team may be a task that falls to you and are keen to help where we can. For example, comments on the online booking process for Congress 2010 have been taken on board and we will be launching an improved group booking process this year. It would help us if we could link you as the practice manager to your practice within our database. If you are happy for us to do this, please complete the reply slip included within this newsletter and return it in the enclosed envelope. The reply slip contains a few quick questions concerning you and how much input your practice has in relation to buying services for vets within your practice; this will help us to understand how we may expand our services to help you. If you have any other ideas about how we can help your practice, there is a space for additional comments. All completed reply slips sent in by 17 September 2010 will be entered into a draw to win a copy of the new BSAVA Manual of Canine and Feline Rehabilitation, Supportive and Palliative Care; 10 runners up will each receive a free copy of the BSAVA Manual of Practical Animal Care.
If you need any further information please contact the Membership and Customer Services Team on 01452 726717 or via email on [email protected].
from BSAVA
for·the·practiceIssue 1 • Summer 2010
Get more involvedBSAVA is an association run by members for members. We have 12 regions throughout the UK and each is run by a local team of professionals who know the needs of the people working in that area. We are also run by Standing Committees that infl uence all areas of the association, including manuals, courses, Congress and member benefi ts. Find out more about getting involved – email Carole Haile at [email protected] or talk to the volunteers in your region.
Members do bestThe practice budget goes further and the right support is more accessible when you are a member of the BSAVA. There are discounts of at least a third on manuals, CPD and Congress, plus online resources and benefi ts to make professional life easier and more rewarding.
From the complimentary copy of each edition of the invaluable BSAVA Small Animal Formulary and subscriptions to JSAP and companion, to the cost-effective day and evening CPD courses made available locally through our network of regions, BSAVA fi nds practical, useful ways to fulfi l its remit to promote excellence in small animal practice through education and science.Membership runs from January to December and it couldn’t be easier to join. You can join online at www.bsava.com, request an application form by emailing us at [email protected], or call us on 01452 726700 – if you have any questions then a member of our team is waiting to talk to you.
Benefi ts in focus ■ Great reduction on BSAVA Congress
registration ■ Free Congress MP3 podcasts ■ Exceptional discounts on BSAVA courses ■ Unbeatable savings on BSAVA manuals ■ Complimentary copy of the BSAVA Guide to
Procedures in Small Animal Practice ■ Complimentary copy of the BSAVA Small
Animal Formulary ■ Complimentary subscription to JSAP and companion
■ Cost-effective, accessible regional CPD ■ Exclusive online resources ■ Health and Safety advice ■ Free room hire at BSAVA HQ ■ Ancillary benefi ts – insurance, stationery,
car hire

companion | 3
ASSOCIATION NEWS
Frances is a European Specialist in Veterinary Diagnostic Imaging, and a double diplomate of the Royal College of Veterinary Surgeons and
the European College of Veterinary Diagnostic Imaging. She has worked both in practice and as an academic, with 26 years working in Higher Education, and has a rich and long history of working as a BSAVA volunteer, culminating in her taking on the presidential mantle in 2007.
The BSAVA postgraduate programme provides both Frances and the Association with a huge challenge – one that aims to provide the best possible educational offering to the profession, particularly to
both of which carry a higher risk of contracting rabies. Children are often unaware of the danger that dogs transmit rabies and may not tell their parents when a bite, lick, or scratch has occurred from an infected animal”, says Briggs.
The good news of course is that rabies is easily preventable. “Vaccination prior to possible exposure is a crucial part of health management of domestic animals, and is the single most important factor in rabies prevention”, said Peter Costa, Global Communications Coordinator for the Alliance for Rabies Control.
The World Rabies Day initiative also raises money towards local rabies prevention and control programmes, with eight projects funded since 2008. “Through the World Rabies Day campaign we continue to engage all the major stakeholders associated with rabies to take action”, says Costa. “We invite everyone to join the team that is Making Rabies History!” More information on World Rabies Day can be found at the official web site, www.worldrabiesday.org. ■
World Rabies Day28 September will mark the World Rabies Day initiative, when partners will be working together to make rabies history
To most of us the figures will be shocking, especially for a disease that is entirely preventable – more than 55,000 people, mostly
in Africa and Asia, die from rabies every year – that’s one person every ten minutes. Children are often the most at risk.
World Rabies Day is led by the Alliance for Rabies Control and supported by numerous human and animal health organisations worldwide. “Rabies is primarily a disease of children, who are particularly at risk from this terrible disease, due to their close contact with dogs, the major global source”, said Dr Debbie Briggs, Executive Director of the Alliance for Rabies Control. “Children are more likely to suffer multiple bites and scratches to the face and head,
The good news of course is that rabies is easily
New Academic Director for Postgrad QualificationIn July BSAVA announced the appointment of Dr Frances Barr as Academic Director with the task of launching the new BSAVA Postgraduate Qualification in association with the Open University in 2012
those in practice. Grant Petrie, BSAVA President, says “Producing a postgraduate qualification is a natural progression to BSAVA’s current CPD offering – there is clearly a need for it and we have a strong legacy as a provider of quality CPD. We want to make sure that the profession is served well – with a programme designed by vets for vets. As a charity with education at the core of our remit, BSAVA is best positioned to create something that will keep investing in the knowledge and talent of the profession. However, we always knew that we would need an exceptional individual to oversee the programme, and, in Frances Barr, we know we have that person.”
The BSAVA postgraduate programme will launch in 2012, with more information about registration available at Congress 2011 and online from April next year. Frances Barr will begin working with the Open University and the BSAVA team from November. For more information about the BSAVA postgraduate course email [email protected] or visit the CPD section at www.bsava.com. ■

4 | companion
Congress Chair, thinks this new look does that job well, “We want people everywhere, from all over the globe, to know when they see these images they are looking at something relating to the world’s largest and leading small animal congress – and that they need to stop and find out more.”
So – this is what you need to be looking out for in the coming months – from thepreview out now, to the registration forms that will be landing on your mat in October – keep an eye out to make sure you are the first to benefit from the information and offers contained inside. n
Congress make over
Being the biggest and most established small animal Congress in the world has never meant that the Congress Committee rest on their laurels. There are a number of new initiatives once again this year – and they have come up with a new look too
The 2011 event will see the start of a whole new image for Congress – something fresh and contemporary to
represent the scale and excellence of the conference and provide a way of everyone being able to identify with the material easily and quickly.
Until now BSAVA has used a completely different image each year for the event – something that the President has selected to represent the culmination of their presidential year. And that tradition will still continue in part. This year Grant Petrie is launching the new-look Congress design by incorporating the unique commissioned artwork of Will Shakspeare, who has made a series of handmade glass animals from his studio in Taunton, and we will be using abstracts of his beautifully blown glass on the covers for 2011. See www.shakspeareglass.co.uk.
Creating an identityCongress committee have worked with a team to create what those in the know call a new ‘brand identity’. But whatever it’s called, it has now given BSAVA a representative image for Congress that is strong, professional and recognisable – all over the world.
Leading veterinary excellence
54th Annual Congress 31 March – 3 AprilThe ICC / NIA – Birmingham – UK
thepreview
Leading veterinary excellence
Leading veterinary excellence
There are four colours in the new scheme, with blue being the primary one we’ll use across most of the printed material. Then there’s the unique, bold animal graphics – clearly not realistic portrayals, but clever representative graphics that highlight the range and variety of species the companion animal vet might see on any given day.
BSAVA Congress is all about leading veterinary science alongside opportunities to socialise, as well as getting a unique view of what’s going on in industry. Combining all that into a single identity was never going to be easy but John Williams,

companion | 5
Congress make over
COUNTDOWN TO
n Book online to save 5% on your registration – available in October 2010
n Early Bird Deadline – 3 January 2011
n Practice Badge Deadline – 10 March 2011
Visit www.bsava.com or email [email protected] for more details
2011 HIGHLIGHTSThere are 40 lecture streams, more than 100 expert speakers, and over 250 individual lectures – a totally peerless scientific programme. You can fulfil your entire annual CPD requirement by attending Congress and listening to some of the lectures you missed online afterwards at your leisure.
Can’t come for the whole four days? For the first time you will be able to take
advantage of the weekend pass – which for a member booking before the Early Bird Deadline means just £227 for top quality science, as well as access to the exhibition and the chance to have a fun weekend with friends and colleagues. You can find out more online or from your registration pack.
2011 will also see additional interactive lectures so you can participate in votes and answer questions using the easy-to-use key pads. There are new management
and communication streams too, with the return of the popular lectures from recent years and most cutting edge topics. For the first time some streams will have simultaneous translation into Spanish and Polish, which is going to add to the international flavour of our event.
Discover Congress highlights and download the Scientific Programme online at www.bsava.com or email [email protected] if you have any questions.

6 | companion
DENTISTRY
Tooth extraction is required where a disease process is too advanced for the teeth to be saved. In addition, financial and other
considerations may lead an owner to request it. The most common indications for tooth extraction are:
■■ In dogs – periodontal disease; endodontic disease from tooth fracture (Figure 1); and the presence of persistent deciduous teeth
■■ In cats – tooth resorption; retained root remnants; and stomatitis.
PreparationThe client’s approval must be obtained for the extent of treatment to avoid the potential for future litigation.
The patient needs to be of reasonable health to undergo general anaesthesia. An endotracheal tube with inflated cuff and an oropharyngeal pack will prevent fluid and debris from entering the trachea or
Dental extractionTooth extraction is a frequently performed procedure in small animal practice. Alexander Reiter, a contributor to the BSAVA Manual of Canine and Feline Dentistry, describes what is entailed
Figure 1: Left maxillary fourth premolar tooth in a dog with a complicated crown–root fracture. The detached ‘slab’ (asterisked) is being raised with a periodontal probe (© Alexander M Reiter)
DENTISTRY

companion | 7
DENTISTRY
oesophagus. The jaws are securely propped open without unnecessary strain on the temporomandibular joints. Additional pain control is achieved with regional anaesthesia (nerve blocks).
Professional dental cleaning followed by rinsing with chlorhexidine gluconate (0.12%) aids in reducing bacteraemia and prevents debris from contaminating the extraction site. Tooth extraction is a surgical procedure, and sterile instruments should be used. Perioperative antibiotics are given in patients that are debilitated and immunocompromised, in those with endocrine disorders, cardiovascular disease, severely contaminated wounds or systemic infections and to patients receiving permanent implants and transplants.
Dental radiographs are obtained prior to tooth extraction to evaluate alveolar bone health and variations in root anatomy, and to determine the presence of dentoalveolar ankylosis or resorption of roots that could complicate the extraction procedure.
Safety measures during the extraction procedure include wearing safety glasses, masks and gloves. The patient’s head is cradled over the bridge of the maxilla with the palm of the free hand during maxillary tooth extractions. During mandibular tooth extractions, the lower jaw can be cradled in the palm of the free hand, or the individual side can be grasped between the thumb and forefinger.
The size of dental elevators should closely fit the size of the tooth or root segment being elevated. Elevators are grasped with the butt of the handle seated in the palm and the index finger extended along the blade of the instrument to act as a stop should the instrument slip.
TechniquesTeeth are anchored to alveolar bone of the mandible, incisive bone and maxilla by the gingiva and periodontal ligament. These tissues must be severed, stretched or torn to allow delivery of the tooth to be extracted. In the dog the incisors, canines, first premolars and mandibular third molars are single-rooted teeth; in the cat, the incisors, canines and, commonly, the maxillary second premolars are single-rooted. The cat’s maxillary first molar may be
treated as a single-rooted tooth even though it may have two roots that are usually fused together. Tooth extraction is performed using the closed technique (without mucoperiosteal flap) or open technique (with mucoperiosteal flap to expose alveolar bone).
Closed extractionClosed extraction begins with incising the gingival attachment around the tooth with a scalpel blade. Then the tip of a dental elevator is inserted into the space between the tooth and the alveolar bone. A well controlled rotational motion on the shank’s long axis between the root and a fulcrum point is performed to create a slow, gentle and steady pressure on the tooth, which is held for 10 seconds to break down the periodontal ligament fibres. The elevator can also be placed perpendicular to the tooth or crown–root segment to lever it out of the alveolus through the line of least resistance, with a fulcrum point preferably on alveolar bone (horizontal rotation) and not on adjacent teeth, unless the tooth used as a fulcrum is to be extracted as well. Multi-rooted teeth must be sectioned to provide multiple single-rooted segments. Extraction forceps should only be applied when the tooth is very loose. The extracted tooth or crown–root segment is examined, ensuring that the entire root has been removed (obtain a radiograph if uncertain). The alveolus is debrided, sharp bony edges are smoothed with a diamond-coated round bur and water irrigation (alveoloplasty), the extraction site is rinsed, and the wound is closed with synthetic absorbable monofilament suture material (such as poliglecaprone 25).
Open extractionOpen extraction is performed when raising a mucoperiosteal flap with a periosteal elevator after creation of one or two releasing incisions that extend from gingiva into alveolar mucosa. Removal of alveolar bone overlying the root(s) (alveolectomy) by as much as one to two thirds of the length of the root(s) is accomplished with a round bur and water irrigation (Figure 2), and multi-rooted teeth are sectioned (Figure 3).

8 | companion
DENTISTRY
Dental extraction
This is followed by elevation of the tooth or crown–root segments (Figure 4), debridement of the alveolus, alveoloplasty (Figure 5), and rinsing of the extraction site.
The periosteum at the connective tissue side of the flap base is incised with a scalpel blade in a distomesial direction. Metzenbaum scissors are used to bluntly undermine the flap (Figure 6) before it is apposed in a tension-free manner to the palatal/lingual gingiva by means of simple interrupted sutures (Figure 7).
Figure 2: Mesial and distal releasing incisions are made, and a mucoperiosteal flap is raised. Alveolectomy is performed over the mesiobuccal and distal roots with a round bur and water irrigation (© Alexander M Reiter)
Figure 3: The mesiobuccal (MB) root and distal (D) root are separated, followed by separation of the mesiobuccal root from the mesiopalatal (MP) root (© Alexander M Reiter)
Figure 4: The mesiobuccal root is elevated and extracted, and its apex is inspected to ensure removal of the entire root (© Alexander M Reiter)
Figure 5: The slab (S) and all crown–root segments are extracted and on display. Alveoloplasty is performed with a round diamond-coated bur and water irrigation. (© Alexander M Reiter)
Figure 6: The periosteum at the flap base is incised with a scalpel blade, and the flap is further released by blunt dissection with Metzenbaum scissors (© Alexander M Reiter)

companion | 9
DENTISTRY
Utilizing good instrumentation and applying proper
techniques will help to avoid complications…
DENTISTRY
AVAILABLE FROM BSAVAThe BSAVA Manual of Canine and Feline Dentistry, 3rd edition, is designed for vets in practice, concentrating on common conditions and procedures. Full-colour photos and specially drawn illustrations illuminate the text throughout.
ContentsOrodental anatomy and physiology; Oral and dental diagnostics; Anaesthesia and analgesia; Operator safety and health considerations; Dental instrumentation and equipment; Developmental oral and dental conditions; Canine infectious, inflammatory and immune-mediated oral conditions; Feline inflammatory, infectious and other oral conditions; Physical orodental conditions; Other oral and dental conditions; Dental surgical procedures; Index.
Download a sample chapter online at www.bsava.com
Member price: £45Non-member price £69
Figure 7: The extraction site is closed with simple interrupted sutures (© Alexander M Reiter)
Postoperative managementOpioids and non-steroidal anti-inflammatory drugs are used for pain control and to reduce tissue swelling associated with open extractions. Chlorhexidine digluconate (0.12 %) gel is applied to the extraction site twice daily for 2 weeks. Unless there is a well founded reason for antibiotic administration, antibiotics should not be used.
Water is offered once the animal has recovered sufficiently from anaesthesia. Soft food is offered 8–24 hours after anaesthesia and maintained for about 2 weeks. Hard treats and chew toys are withheld while the oral tissues heal.
Possible complications of tooth extraction include: fractured roots; haemorrhage; trauma to adjacent teeth, permanent tooth buds and soft tissue; sublingual oedema and salivary mucocele; orbital trauma; fracture of the alveolus or jaw; oronasal communication; trauma from opposing teeth; tongue hanging out of the mouth; emphysema and air embolism; and local and systemic infection. Utilizing good instrumentation and applying proper techniques will help to avoid these complications. ■
companion readers wishing to know more regarding surgical extractions are reminded that “How to perform a surgical extraction” featured in companion March 2009 and can be downloaded from www.bsava.com.

10 | companion
CLINICAL CONUNDRUM
Clinical conundrumconundrumGareth Arthurs of the Royal Veterinary College and the British Veterinary Orthopaedic Association considers a case of traumatic hind limb lameness
Case presentationA 4-year-old male black Labrador presents with acute onset right pelvic limb lameness. Two days previously, the dog jumped out the back of a Land Rover and got his right hind foot caught in the tow bar of the vehicle. Physical examination shows that the dog is clinically stable. Orthopaedic examination shows grade 3 of 5 lameness of the right pelvic limb with visible instability of the right hind pes. Examination of the pes of the pelvic limb is very well tolerated and does not seem to cause the dog discomfort or pain but there is valgus instability originating in the region of the mid pes. No other abnormalities are observed.
4. Haematology and biochemistry prior to sedation or general anaesthesia. Assessment of the dog’s haematological and biochemical status is a sensible consideration prior to any chemical restraint. This patient was a young healthy dog with no indication of a metabolic problem, and trauma was localised to only the right pes; therefore haematology and biochemistry were not performed. However, arguably a haematocrit, total solids, electrolytes and urea/creatinine could have been measured for a minimum baseline.
Because of the benefits of radiography, the dog was anaesthetised and the right pes was radiographed. The radiographs are shown in Figures 1 and 2.
What steps are you considering for further investigation in this case?1. Radiograph the pes under sedation or general
anaesthesia. This is the simplest diagnostic test most likely to give useful further information.
2. Further palpation under sedation or general anaesthesia. This is a sensible consideration as many orthopaedic patients are too stressed or in pain to allow detailed physical examination whilst conscious. However, this patient tolerated conscious examination very well. Repeat examination under sedation was performed that showed dorsal and medial instability of the mid pes.
3. CT examination of the pes. The numerous tarsal bones and their complex shapes and 3-dimensional overlapping relationship can make interpretation of tarsal bone pathology challenging from the 2-dimensional images of radiographs. Generally, radiographs are sufficient for gross pathology such as luxations or simple fractures but CT is invaluable for more complex fractures. However, CT imaging is significantly more expensive than radiography and life-sized images that can be used for pre-operative templating and intra-operative reference are not produced. For these reasons CT was not performed in this patient.
Figure 1: Dorsoplantar radiograph of the right pes
Figure 2: Mediolateral radiograph of the right pes

companion | 11
CLINICAL CONUNDRUM
Describe the radiographs and the abnormalities you can seeThe mediolateral view of the pes shows no abnormality. The dorsoplantar view of the right pes shows subtle enlargement of the centrodistal tarsal joint and the lateral aspect of the tarso-metatarsal joint. In addition, mild lateral malalignment of the metatarsal bones relative to the proximal tarsal bones is visible.
If you can’t see these abnormalities or you’re unconvinced, what could you do to clarify this?Radiograph the contralateral limb – comparing radiographs of the normal to the affected limb can help to highlight subtle abnormalities that might otherwise not have been noticed. In this case, radiographs of the contralateral (left) pes were taken and compared: see Figures 3 and 4. Comparison of the dorsoplantar views of the left and right sides highlights the widened centrodistal and lateral tarso-metatarsal joints of the right pes. In addition, the position of the 3rd tarsal bone relative to the 4th is abnormal on the right side.
What is the diagnosis so far?Instability and subluxation of the centro-distal tarsal and lateral tarso-metatarsal joints with mild lateral malalignment of the distal pes.
Is this the final diagnosis? Is this sufficient information to plan treatment for the dog?No, it is not – although the problem has been localised based on static radiographs, the dynamic component is unknown. In other words, what is the impact of this instability during weight bearing? In what planes is the pes stable or unstable? These are important questions to answer as they will influence the treatment options.
What is the next diagnostic step?Take stress radiographs of the affected pes and if necessary, compare them with stress radiographs of the normal limb. The pes should be stressed in all four planes, i.e. dorsal, plantar, medial and lateral. Stress radiographs of this dog are shown in Figures 5 to 8. The red arrow indicates the direction of the applied stress.
Figure 3: Dorsoplantar radiograph of the left pes2 = 2nd tarsal bone, 3 = 3rd tarsal bone, 4 = 4th tarsal bone, C = central tarsal bone.
Figure 4: Mediolateral radiograph of the left pes
Figure 5: Dorsoplantar radiograph of the right pes with laterally applied stress
Figure 6: Dorsoplantar radiograph of the right pes with medially applied stress

12 | companion
CLINICAL CONUNDRUM
Clinical conundrum
What is your interpretation of these radiographs?The stress radiographs show that the pes is stable to dorsal and medial directed forces. However, plantar and laterally directed forces demonstrate gross instability of the pes with centrodistal luxation and lateral tarso-metatarsal subluxation with secondary lateral and plantar malalignment of the metatarsal bones. The dorsoplantar view shows that the metatarsal bones, 3rd and 2nd tarsal bones are united and mechanically stable as one unit, and the central, 4th and more proximal tarsal bones are mechanically stable as one unit. In addition, the first tarsal bone has fractured.
The primary instability is loss of dorsomedial support and subsequent luxation of the centrodistal joint. The subluxation of the lateral aspect of the tarso-metatarsal joint is secondary and much less severe, as it is constrained by the intact lateral collateral ligaments; these are demonstrated to be intact, as the pes is stable to medially applied stress.
What are the treatment options for this dog?1. Partial tarsal arthrodesis – standard lateral
approach. This is a procedure that fuses most of
Figure 7: Mediolateral radiograph of the right pes with dorsally applied stress
Figure 8: Mediolateral radiograph of the right pes with plantar applied stress
the joints of the weight bearing axis of the pes/tarsus, i.e. the calcaneo-quartral joint and the lateral aspect of the tarso-metatarsal joint. It is typically performed by application of a plate to the lateral aspect of the tarsus from calcaneus to the 4th metatarsal bone. This is an option for this dog, as it would stabilise the pes and give good results longer term. The disadvantage is that it involves arthrodesing two joints that are effectively normal and the affected centrodistal is not directly addressed. To address these limitations, a medial approach could be considered.
2. Atypical partial tarsal arthrodesis – medial approach. The surgical approach is made on the medial aspect of the pes and the plate applied to the medial aspect; thus the centro-distal joint is arthrodesed directly. However, application of the plate to the medial aspect is much more challenging because of the irregular medial surface contour of the tarsal bones. A medial approach would also necessitate fusion of two unaffected joints – the talocentral and medial tarso-metarsal joints.
3. Selective arthrodesis of only the centrodistal joint. As this is the location of the primary instability, this seems a logical approach. However, can this be achieved and, if so, how? A relatively small dorsomedial incision is made, only the affected joint is treated surgically and surgical dissection is much reduced. Far fewer implants are placed as a simple 2 screw and tension band wire is sufficient to effect the arthrodesis. However, is such a simple surgical solution strong enough? The critical fact is that plantar support of the pes/tarsus is intact – confirmed radiographically as application of dorsal stress caused no plantar instability. As plantar support is intact, the surgical reconstruction is protected from, and does need to withstand, the main forces of weight bearing, as these are borne by the reconstructed tarsus and not the implants.
4. Surgical repair of the fractured first tarsal bone. Theoretically this is appropriate but in reality the fractured bone is so small that reliable purchase of any implant in the bone would be very challenging and there would be a high risk of further fracture during implant placement
5. Conservative management by external coaptation. As previously discussed, plantar support of the pes is intact; therefore conservative management could be effective if it would reliably maintain the pes/tarsus in reduction. However, as the subluxated tarsal bones are imperfectly reduced in the neutral radiograph (see Figure 1), this would not be improved with a dressing. Imperfect reduction means that residual instability of the joint may persist, which could result in persistent instability or development of degenerative joint disease.

companion | 13
CLINICAL CONUNDRUM
BVOA AUTUMN MEETINGBVOA’s annual autumn meeting will this year will be held in Dublin, 12–14 November. The scientific programme promises the usual stimulating mix of UK and international speakers with small animal veterinary and human orthopaedic backgrounds. The provisional scientific programme includes:
■■ Imaging of the shoulder joint, including advanced imaging and with an emphasis on comparative aspects between canine and human shoulder joint imaging
■■ Shoulder joint arthroscopy and the management of ligamentous injuries of the shoulder■■ Developmental conditions of the shoulder joint■■ Miscellaneous condition of the shoulder joint, such as mineralization of the tendons of the peri-scapular
muscles, and caudal glenoid fragmentation.■■ Management of soft tissue injuries of the human shoulder – a physiotherapist’s perspective■■ Imaging and management of skeletal neoplasia of the forelimb
For more information www.bsava.org.uk/bvoa/ or email [email protected]
Given these options what would you do?In this case, a selective centrodistal joint arthrodesis was performed. A dorsomedial approach was made to the centrodistal joint and the incision was situated so as not to be directly over the implants in order to avoiding problems of skin healing directly over the implants. The subluxated centrodistal joint was identified, and further exposed. The pes was manipulated to increase exposure and the articular cartilage was removed using a high speed bur. Cancellous bone graft was harvested from the proximal right tibia and packed into the centrodistal joint. The subluxated joint was reduced and immobilised using pointed reduction forceps. A laterally directed 2.7 mm cortical screw was placed in the central tarsal bone, and another in the 2nd tarsal bone, which also engaged the 4th tarsal bone laterally.
An orthopaedic washer was placed beneath the head of each screw and narrow gauge orthopaedic wire was placed in a figure-of-eight pattern between each screw head to apply compression and stability across the arthrodesis site. After placement of the implants, tarsal alignment and stability were checked, and were normal. The surgical site was flushed thoroughly and closed in a routine manner. The post-operative radiographs are shown in Figures 9 and 10.
How would you manage this case post-operatively?In this case, the right pes was placed in a cast for 6 weeks post-operatively; a splinted dressing or modified Robert Jones support dressing would have been good alternatives. The dog was confined to lead walks only and re-radiographed at 6 weeks post-operatively: the radiographs showed no evidence of implant loosening, and early evidence of union of the
centrodistal joint. The dressing was removed and the dog remained confined to lead exercise only. The dog was re-examined and the pes was re-radiographed at 12 weeks post-operatively; these showed mature union of the talo-central arthrodesis site with no evidence of implant related problems. The dog was returned to normal activity over the next 6 weeks and recovered uneventfully. ■
Figure 9: Dorsoplantar post-operative radiograph of the right pes
Figure 10: Mediolateral post-operative radiograph of the right pes
14 | companion
HOW TO…
How to…
Approach the smelly ear
Janet Littlewood of Veterinary Dermatology Referrals, Cambridge, guides us through this often frustrating problem
Ear disease is a common reason for the presentation of small animals in general veterinary practice. After
preventive health care, dermatological conditions are the most common reason for pet owners seeking veterinary attention. Otitis is the third most common dermatological presentation for dogs, and second commonest for cats, accounting for 22% and 19% of dermatological cases, respectively 1.
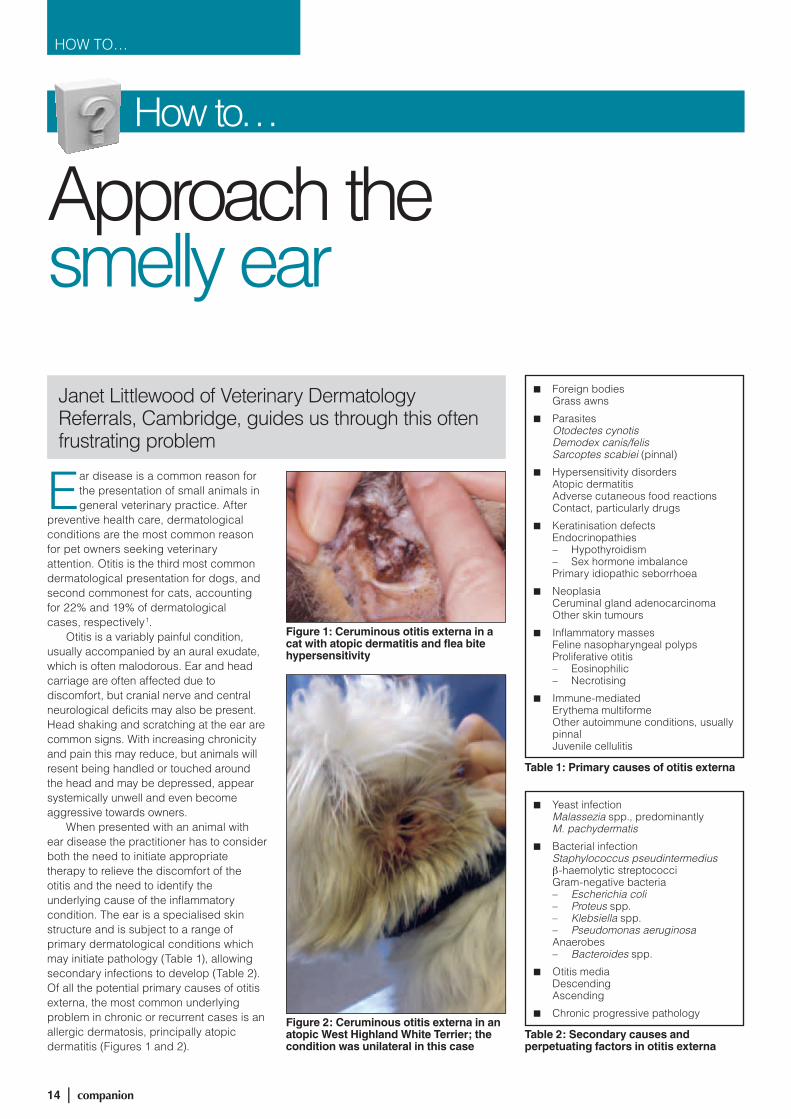
Otitis is a variably painful condition, usually accompanied by an aural exudate, which is often malodorous. Ear and head carriage are often affected due to discomfort, but cranial nerve and central neurological deficits may also be present. Head shaking and scratching at the ear are common signs. With increasing chronicity and pain this may reduce, but animals will resent being handled or touched around the head and may be depressed, appear systemically unwell and even become aggressive towards owners.
When presented with an animal with ear disease the practitioner has to consider both the need to initiate appropriate therapy to relieve the discomfort of the otitis and the need to identify the underlying cause of the inflammatory condition. The ear is a specialised skin structure and is subject to a range of primary dermatological conditions which may initiate pathology (Table 1), allowing secondary infections to develop (Table 2). Of all the potential primary causes of otitis externa, the most common underlying problem in chronic or recurrent cases is an allergic dermatosis, principally atopic dermatitis (Figures 1 and 2).
Figure 1: Ceruminous otitis externa in a cat with atopic dermatitis and flea bite hypersensitivity
Figure 2: Ceruminous otitis externa in an atopic West Highland White Terrier; the condition was unilateral in this case
■■ Foreign bodiesGrass awns
■■ ParasitesOtodectes cynotisDemodex canis/felisSarcoptes scabiei (pinnal)
■■ Hypersensitivity disordersAtopic dermatitisAdverse cutaneous food reactionsContact, particularly drugs
■■ Keratinisation defectsEndocrinopathies – Hypothyroidism – Sex hormone imbalance
Primary idiopathic seborrhoea
■■ NeoplasiaCeruminal gland adenocarcinomaOther skin tumours
■■ Inflammatory massesFeline nasopharyngeal polypsProliferative otitis – Eosinophilic – Necrotising
■■ Immune-mediatedErythema multiformeOther autoimmune conditions, usually pinnalJuvenile cellulitis
Table 1: Primary causes of otitis externa
■■ Yeast infectionMalassezia spp., predominantly M. pachydermatis
■■ Bacterial infectionStaphylococcus pseudintermediusβ-haemolytic streptococciGram-negative bacteria – Escherichia coli – Proteus spp. – Klebsiella spp. – Pseudomonas aeruginosa
Anaerobes – Bacteroides spp.
■■ Otitis mediaDescendingAscending
■■ Chronic progressive pathology
Table 2: Secondary causes and perpetuating factors in otitis externa

companion | 15
HOW TO…
Aetiology and pathogenesisThe normal healthy ear canal produces minimal secretions from the sebaceous and modified apocrine (ceruminous) glands. The secretions are carried upwards and distally, with the upward migration of the epithelial cells of the stratum corneum, and out of the external auditory meatus. Inflammation results in an increase and alterations in glandular secretions, overcoming the normal upward escalatory cleaning mechanism, which in turn enhances the growth of microbes.
Malassezia organisms are part of the normal flora of the canine and feline ear and are found in small numbers in up to 36% of normal dogs 2. Increased humidity, from both secretions and water in the ear canals, enhances the growth of yeast organisms 3 and Malassezia organisms are present in up to 76% of cases of otitis externa 4, often in combination with Staphylococcus pseudintermedius.
With increasing chronicity bacterial infection tends to supersede yeast infection. A range of opportunistic organisms may be implicated. This picture may then be further modified by the use of antimicrobial preparations which may select for resistant organisms, resulting in the therapeutically challenging clinical presentation of Pseudomonas otitis. This progression of disease is accompanied by a change in the gross nature of the aural exudate, initially ceruminous brownish and waxy or more yellow-orange in colour, to a purulent off-white to greenish exudate which may be obviously slimy or mucoid and often with an offensive odour (Figure 3).
Inflammation of the external ear canal results in hyperplasia of the integument lining the canal and of the glands. The resulting narrowing of the lumen of the canal, further impairs the normal drainage function of the ear and enhancing the microenvironment for
microbial multiplication (Figure 4). Chronic inflammation is accompanied by fibrosis, progressive stenosis and calcification of the cartilage structures of the external ear canal. Ears that have been previously affected by otitis externa are more at risk from future episodes of infection if the inflammatory changes are not fully reversible.
Otitis media is a common complication of chronic otitis externa. Middle ear involvement was noted in 52% of cases of chronic otitis in dogs, compared with 16% of acute cases 5. In 82.6% of ears with
chronic otitis concurrent otitis media was present, with the tympanum intact in 71% of cases. Bacterial isolates from the horizontal ear canal and tympanic bulla were different in terms of organisms and/or antibiotic sensitivity profile in 89.5% of cases. Neurological complications may accompany otitis media (Table 3 and Figure 5) and the anatomical structure of the middle ear means that progressive pathology (granulation tissue formation, osteomyelitis) and chronic irreversible changes may ensue.
Figure 3: Purulent otitis externa due to Pseudomonas aeruginosa infection in an atopic Basset Hound
Figure 4: Chronic otitis externa with ceruminous exudate in an atopic German Shepherd Dog, showing hyperplasia, thickening and lichenification of the pinnal integument and stenosis of the external auditory meatus
Figure 5: Otitis media in a Weimaraner secondary to chronic otitis externa due to atopic dermatitis, with left-sided facial paralysis
DeafnessHorner’s syndromeFacial paralysisGlossopharyngeal damageVestibular diseaseMeningoencephalitis
Table 3: Neurological complications of otitis

16 | companion
HOW TO…
Approach the smelly ear
Approach to the caseHistory – Effective client communication is of paramount importance. History relating to the current ear problem is obviously important, but the clinician must not forget to gather information pertaining to the presence of concurrent clinical signs or previous manifestations relating to a more generalised dermatosis (Table 4). Owners often ignore or misinterpret signs of mild pruritus in dogs, such as regular foot-licking, an itch-scratch reflex (ticklish spot) and excessive perineal or preputial attention.
cotton bud will collect material for microscopical examination.
Exudate should be spread on to two microscope slides:
■■ The first mixed with either liquid paraffin or potassium hydroxide for examination for external parasites
■■ The second heat fixed and stained with a rapid cytological stain for identification of microbes and cells.
Ceruminous otitis externa is characterised by increased numbers of squames (some of which may be nucleated) increased numbers of yeast organisms (>10 per high power field), a few bacterial cocci and occasional to a few inflammatory cells (Figures 6 and 7).
Cases of purulent otitis may have mainly coccoid bacteria or a mixture of cocci and bacilli, with many neutrophils (both degenerate and band neutrophils) as well as increased squames (Figure 8).
The cytological findings in cases of parasitic otitis, foreign bodies and neoplasia are variable, depending on duration of disease and secondary opportunistic infection.
Significance of bacteria – If bacterial cocci are identified, a presumptive diagnosis of S. pseudintermedius infection is justified and empirical selection of antibiotics is appropriate unless the case is long-standing and has failed to respond to appropriate antibiotics previously. All cases in which bacterial rods are identified should have swabs submitted for bacterial culture and sensitivity, preferably by minimum inhibitory concentration techniques rather than by disc diffusion methodology.
Otoscopic examination is likely to need sedation or general anaesthesia. In cases of acute onset of signs of otitis, this should be undertaken at the first presentation in case of the presence of a foreign body, but in cases of chronic or recurrent otitis it may be more appropriate to instigate some initial therapy prior to scheduling this procedure.
Otoscopic examination allows an assessment of the patency of the vertical and horizontal canals and the nature and extent of the inflammatory process, and may allow visualisation of the ear drum. Video-otoscopy allows excellent and detailed visualisation of the ear canal and
■■ SignalmentAge – Parasites and allergies often
young animals – Tumours and endocrinopathies
often older animalsBreed – Predispositions to atopic disease – Predispositions to hypothyroidism
■■ Acute onset or gradual, progressive
■■ Unilateral or bilateral
■■ RecurrencesTime of year, seasonality
■■ Other dermatological signsPruritus, especially pedalPyodermaScaling/seborrhoea
Table 4: History in cases of otitis
Clinical examination of the patient should include general examination, in case of systemic abnormalities and the likelihood of needing sedation or general anaesthesia to assess the ear problem fully, and a complete dermatological examination.
Examination of the ear in the conscious patient may be limited to: an assessment of the pinnae and external auditory meatus, noting the presence and nature of any exudate; and external palpation of the vertical ear canal, to assess rigidity and pain. Difficulty or pain on opening the mouth often accompanies middle ear pathology and an assessment of cranial nerve function should be conducted.
Cytological examination of aural exudate should be undertaken in all cases where discharge is evident at the external auditory meatus. Sometimes the outer ear may appear relatively clean, but considerable exudate is present in the ear canal and gentle introduction of a
Figure 6: Cytology of ceruminous exudate, showing large numbers of yeast organisms, squames and occasional bacterial cocci, but no inflammatory cells
Figure 7: Cytology of aural exudate from a case with mixed yeast and bacterial infection, showing several nucleated squames and moderate numbers of yeast organisms and bacterial cocci, with streaks of chromatin from degenerate neutrophils and clumps of inflammatory debris and some intact neutrophils
Figure 8: Cytology of purulent aural exudate showing many neutrophils, mostly degenerate, with streaks of chromatin, clumps of inflammatory debris and bacterial rods
even the middle ear in larger animals, with accompanying specialised instrumentation. However, a good quality hand-held otoscope is adequate in the majority of cases. If the ear drum cannot be seen, it should be assumed to be ruptured and

companion | 17
HOW TO…
cleansing agents chosen appropriately. If visible, the tympanum may show evidence of pathology in the middle ear, with loss of transparency, thickening and bulging.
A full assessment of middle ear involvement may require imaging by radiography or magnetic resonance imaging, which should be conducted without any attempts to clean the ear canal(s) so that the presence of fluid /soft tissue densities can be evaluated without the prior introduction of cleaning solutions. Considerable information can be obtained by performing myringotomy; the author’s preferred instrument is a Spreull’s needle rather than a soft catheter, since the rigidity of the needle allows for more accurate manipulation in the middle ear, avoiding the auditory ossicles and round and oval windows, and an assessment of the nature of the lining of the bulla (bony or soft, suggesting the presence of granulation tissue).
In chronic or recurrent cases, where flushing under general anaesthesia is planned as part of the therapeutic protocol, and particularly cases where placement of ear wicks is intended, anti-inflammatory therapy should be initiated prior to otoscopy. High anti-inflammatory doses of steroids are indicated (prednisolone 1–2 mg/kg daily). This will give some immediate relief to the animal and controlling the inflammation will enable more effective cleansing both by the clinician and subsequently by the owners. Otoscopic examination can be scheduled for a few days to a week later, depending on whether bacteriology samples have been submitted.
Medical management of otitisThe recent trend in the management of otitis has been towards topical therapy without use of systemic antibiotics. Much higher concentrations of drugs can be achieved by medicating the ear directly rather than by systemic administration of drugs. Some clinicians will still employ systemic medication in some cases of Malassezia otitis, particularly when concurrent Malassezia hypersensitivity is present, and for cases of streptococcal bacterial otitis. Opinion in the veterinary dermatology field appears to be divided in respect of the use of systemic drugs in cases of otitis media.
A) Thorough initial and repeated ongoing cleaning of the ear canal(s)This is an essential prerequisite to allow effective specific topical therapy. Inspissated deposits of wax may require the use of ear curettes or forceps to remove material from the ear canal, but in most cases the exudate can be softened by use of light oils or lubricants (liquid paraffin or propylene glycol), or ceruminolytics (sulphosuccinates, lactic acid or acetic acid). The ear canals can then be flushed and cleansed.
Choosing an ear cleaner – There are many ear cleaners available on the veterinary market and factors to be considered in selecting a suitable cleaner should include irritancy, safety in the middle ear in case the ear drum is ruptured, efficacy at cleaning and antimicrobial effect. Cleaners containing organic acids tend to have better antimicrobial effects, but are more astringent and may not be well tolerated by some patients, particularly in the presence of significant inflammation.
For cleaning under general anaesthesia some clinicians prefer to use water or sterile saline, in order to avoid damage to the middle ear and associated structures, but dilute chlorhexidine (<0.05%) and acetic acid at low concentrations (2.5%) are safe in the middle ear and have antimicrobial properties. TrizEDTA solution is also safe in the middle ear and can be used after an acidic cleanser to neutralise the solution, as well as having a potentiating effect on some antibiotics. However, use of TrizEDTA alone as a cleaner may enhance or encourage the growth of yeast organisms; this can be avoided by using solution with added chlorhexidine or ketoconazole.
Whilst ear flushing under sedation or general anaesthesia is usually without complications, neurological disturbances may ensue in a small number of cases and owners should be warned of the risk at the time of obtaining consent for the procedure.
B) Treatment of infectionsChoosing a medication – Most medicated ear preparations authorised for veterinary use in the UK include:
■■ An antifungal agent (nystatin, tiabendazole, monosulfiram, clotrimazole, miconazole)
■■ An analgesic or anti-inflammatory agent: most include a glucocorticoid, such as prednisolone, betamethasone or dexamethasone
■■ An antibiotic: the antibiotics included in ear drops effective against Gram-positive organisms include fusidic acid, framycetin, neomycin, gentamicin and marbofloxacin. Some of these are also effective against some Gram-negative organisms, with polymixin B another good first choice antibiotic.
In cases of Pseudomonas infection, bacterial resistance is a very significant problem, which may arise due to intermittent or incomplete treatment of otitis externa. Some isolates may be sensitive to veterinary labelled drugs, but often the clinician will have to use a drug ‘off-label’, such as silver sulphadiazine 1%, enrofloxacin solution, ceftazidime, piperacillin, tobramycin or ticarcillin. Whilst some of these drugs are potentially ototoxic and are not recommended for use if the ear drum is ruptured, the risks of ongoing infection and potential extension of pathology into the cranial vault may necessitate the use of one of these drugs. Interestingly for some of these, particularly the aminoglycosides, there may be less ototoxicity with local use in the ear than with systemic use. The toxicity of agents in the middle ear may relate more to the vehicle carrying the drug than to the drug itself. Drugs in aqueous solution are far safer in the middle ear than those in an oily vehicle.
C) Daily owner careCleaning – Where the owner is able to, and the dog permits, the ear canals should be cleaned daily with an appropriate cleaner until there is no further discharge evident. It is vitally important that the client is given suitable instruction in how to clean their pet’s ears properly.
Medicating – Medicated drops should be applied at least 15–20 minutes after cleaning, allowing time for the dog to shake out residual cleaner and exudate that cannot be wiped away. This ensures that when the medication is applied it can contact the surface of the integument rather than sit in a puddle of exudate and

18 | companion
HOW TO…
Approach the smelly ear
cleaning solution. In most cases medicated drops should be applied twice daily.
The duration of treatment will depend on the chronicity of the condition, but should continue until beyond cure of infection and will usually be of the order of 1–3 weeks. Response to treatment should be assessed at appropriately scheduled re-examinations. Failure to follow up cases of otitis externa is a clear factor in the development of chronic resistant infections
D) Use of ear wicks in case of poor patient compliance or resistant infectionWhere patient compliance is poor, or resistant infections are present, the placement of polyvinyl A ear wicks followed by impregnation with antibiotic solution to give a high local concentration of drug is often effective in securing bacteriological cure. The ear wicks are left in place for 7–10 days, with the owner maintaining hydration of the wicks by introduction of antibiotic solution every other day. Ear wicks are usually well tolerated if the dog is on adequate anti-inflammatory doses of glucocorticoid at the same time. At the time of wick removal further cytological assessment and bacterial culture should be undertaken.
Management of otitis mediaSurgical intervention is indicated if there are chronic inflammatory changes in the middle ear; in such cases medical management is inappropriate. Those cases amenable to medical therapy may need to have the middle ear flushed on several occasions. A cuffed endotracheal tube is essential to prevent aspiration of material entering the nasopharynx via the auditory (Eustachian) tube.
The tympanic bulla should be flushed with 5–10 ml of warm sterile saline gently introduced in a ventral direction via a Spreull’s needle and solution and debris aspirated. The procedure is repeated until the aspirate is clear. Topical antibiotics in aqueous solution chosen on the basis of culture and sensitivity testing and systemic steroid therapy should be employed.
Brainstem auditory evoked response (BAER) studies in patients with otitis media have shown improved hearing in those successfully treated with topical marbofloxacin, gentamicin, clotrimazole
NeoplasiaStenosis of ear canalProliferative/nodular hyperplasiaCalcification of ear cartilagesBony changes to bullaGranulation tissue in middle earNeurological deficits, deafnessFailure to respond to medical therapy
Table 5: Indications for ear surgery
and silver sulphadiazine. A profound reduction in BAER was documented after treatment with ticarcillin and tobramycin, more severe with the latter drug. However, if successful treatment obviates the need for total ear canal ablation (TECA), the residual auditory function may be better than after surgery.
Diagnosis and management of underlying diseaseMany of the manifestations of otitis observed are secondary; the primary causes of otitis externa will require appropriate investigations in order to reach a definitive diagnosis and enable specific therapy to be initiated. The therapeutic requirements of the ear pathology may delay some diagnostic procedures, particularly where steroid therapy would interfere with tests and interpretation of results. However, it may be appropriate to initiate an elimination diet whilst appropriate therapy for the ear disease is conducted. When other diseases have been ruled out, allergen-specific IgE testing can be undertaken at a later date when steroid therapy has been withdrawn.
Managing recurrence – Recurrent episodes of otitis externa are a risk even when the underlying disease process is correctly identified and appropriate treatment regimes initiated. Many cases will require ongoing prophylactic aural care. The atopic Labrador Retriever who enjoys a regular swim is an example of a dog at risk of Malassezia overgrowth. The aim of routine treatment is to maintain normal aural health, with a normal, non-inflamed integument over the whole of the external ear and a normal population of microbial flora (i.e. a few yeast organisms and no bacteria). This can be achieved by regular use of an ear cleaner that has antimicrobial and astringent properties, the frequency of use depending on the individual patient’s needs, but usually between 1–2 x weekly to 1–2 x monthly.
Some authors advocate the use of topical medicated ear drops on an intermittent, pulse-treatment basis, but this author considers that this may enhance the risk of selecting for resistant bacterial strains and the benefits of this treatment probably lie in the regular use of a topical glucocorticoid.
Since the majority of cases of recurrent otitis externa are due to underlying atopic dermatitis, the primary pathological event in these cases is cutaneous inflammation, often starting on the pinnal surface and then extending down the ear canal. If this allergic inflammation can be kept under control, then episodes of otitis and secondary infection will be minimised. Suitable agents to achieve this include prednisolone succinate or phosphate drops applied to the ear canal(s) and hydrocortisone aceponate spray for the pinnal surfaces 2–3 times weekly. More chronic, lichenified changes may require the use of more potent steroids such as dexamethasone or betamethasone in solution for the ear canals or in gel formulation for the pinnae.
Indications for surgerySome cases will require surgical intervention because of the primary disease process, such as neoplasia or inflammatory polyps. Whilst many cases of otitis externa are suffering from primary medical rather than surgical disease processes, repeated episodes of otitis may result in chronic progressive pathology, sometimes termed “end-stage” otitis and TECA surgery is indicated in such cases (Table 5). Occasionally the difficulties of ongoing management in uncooperative patients not amenable to regular treatment may indicate the need for surgical intervention even when irreversible pathology is not present, since removal of the ear canal removes the source of pain and inflammation, albeit at the cost of significant hearing loss. ■
References 1–5 and further reading list available to download from www.bsava.com

companion | 19
CPD
FEESFull SeriesBSAVA Member: £597.83 inc. VATNon-member: £869.73 inc. VAT
Individual courseBSAVA Member: £203.28 inc. VATNon-member: £304.91 inc. VAT
CPD
FEESFEESFull SeriesBSAVA Member: £597.83 inc. VATNon-member: £869.73 inc. VAT
Individual courseBSAVA Member: £203.28 inc. VATNon-member: £304.91 inc. VAT
During three days of exotics lectures, presentations, videos and interactive case studies with video presentations, delegates will
discover a new breadth of knowledge and be able to focus on the most current issues, latest therapies and surgical techniques.
Tuesday 5 October: Medicine, surgery and emergency careThe first course will cover small exotic pet mammals (rabbits, rodents and small marsupials) and consider the latest medical and surgical approaches to exotic pets. There will be particular emphasis on:
■ Critical care and emergency medicine of small mammals;
■ Surgery and anaesthesia, diagnosis and management of renal failure, hepatic lipidosis in rabbits and rodents;
■ Hormonal disease and control of reproduction in ferrets;
■ An approach to neoplasia and surgical and chemotherapeutic options in ferrets and rabbits.
An exotic winter
Tuesday 2 November: Medicine, surgery and emergency care of cage birds and raptorsThe second course will look at cage birds and raptors. The main focus will be on:
■ Critical care and emergency medicine for birds; ■ Techniques for safe anaesthesia of the sick bird; ■ How to manage avian fractures; ■ Common soft tissue surgical techniques; ■ An approach to interpreting haematology,
biochemistry and cytology tests. And how to get the most out of them;
■ A logical approach to the feather plucking parrot;
■ Management of the persistent bumblefoot case.
Tuesday 7 December: Medicine, surgery and emergency care of reptilesThe final session will cover reptiles and amphibians, exploring:
■ How to approach the anorexic snake; ■ Interpreting haematology and getting the most
from biochemistry and cytology tests; ■ Techniques for safe anaesthesia of the
compromised reptile patient; ■ Common soft tissue surgical techniques;
■ Managing venomous reptiles in the practice.
BSAVA’s Exotics Mini Modular Course starts in October with specialists Simon Girling and Romain Pizzi at Mottram Hall in Cheshire
20 | companion
CPD
An exotic winter
ROADSHOW: A PRACTICAL APPROACH TO WOUND MANAGEMENTSpeakers: Geraldine Hunt & Ronan Doyle
■ 13 October – Novotel, Newcastle ■ 15 October – Holiday Inn, Cambridge ■ 18 October – Chilworth Manor, Southampton ■ 20 October – Thistle, Brands Hatch
BSAVA Members: £203.28 inc. VATNon-members: £304.91 inc. VAT
BSAVA MANUAL OF EXOTIC PETS, 5TH EDITIONEdited by: Anna Meredith and Cathy Johnson-Delaney
This edition is the Foundation Manual for information across the range of exotic pets, from small mammals, through birds, reptiles and amphibians, to invertebrates. Commoner pets such as rabbits, rodents and budgies retain their place. However, the ever-increasing range of non-traditional pets encountered by the veterinary surgeon in practice is reflected in coverage of new groups such as marsupials, ratites and crocodilians.
■ Biology, husbandry, handling and restraint ■ Diagnostic approach to common conditions ■ Supportive care ■ Anaesthesia and analgesia ■ Common surgical procedures ■ Euthanasia ■ Drug formulary
Member price: £49.00Non-member price: £75.00
SIMON GIRLING BVMS (Hons) DZooMed CBiol MSB MRCVSRCVS Recognised Specialist in Zoo & Wildlife MedicineSimon has worked in first opinion and referral exotic species practice for the last 16 years. He gained his RCVS Diploma in Zoological Medicine in 2002 and his RCVS Specialist status in Zoo & Wildlife Medicine in 2003. He is Senior Vice President of the British Veterinary Zoological Society and has acted as chief examiner for both the RCVS Certificate and Diploma exams in Zoological Medicine. Simon has contributed to several books on exotic species, including acting as co-editor for the BSAVA Manual of Reptiles, 2nd edition and as an author in the BSAVA Manual of Psittacine Birds, 2nd edition. He is currently the Head of Veterinary Services to the Royal Zoological Society of Scotland’s Edinburgh Zoo and also co-owns a first opinion and referral exotics and small animal practice in Perth. Simon is also an Honorary Senior Lecturer in Zoological Medicine at Glasgow University Vet School.
ROMAIN PIZZI BVSc DZooMed FRES MACVSc (Surg) MRCVSRCVS Recognised Specialist in Zoo & Wildlife MedicineRomain has performed wildlife, zoo, and exotic animal veterinary work on five continents, holds an MSc in Wild Animal Health, the RCVS Certificate and Diploma in Zoological Medicine, and Membership of the Australian College of Veterinary Scientists by examination in Small Animal Surgery. Former pathologist at the Zoological Society of London, he is currently veterinary surgeon at Edinburgh Zoo and lectures in Zoo and Wildlife Medicine at the University of Nottingham. He is responsible for veterinary care to the more than 3000 annual wildlife cases at the Scottish SPCA Wildlife rescue centre. His particular interest is in endoscopy and minimally invasive surgery.
BVMS (Hons) DZooMed CBiol MSB MRCVS
companion | 21
PUBLICATIONS
Ask people about physiotherapy and most will be aware of human physiotherapists and what they can do. They will have a reasonable idea of the
importance of their role in the rehabilitation of the human patient, even if they do not have personal experience. Ask the same question in a veterinary context, however, and many would say they were unaware even of the existence of veterinary physiotherapists, let alone be able to suggest how one could help their pet.
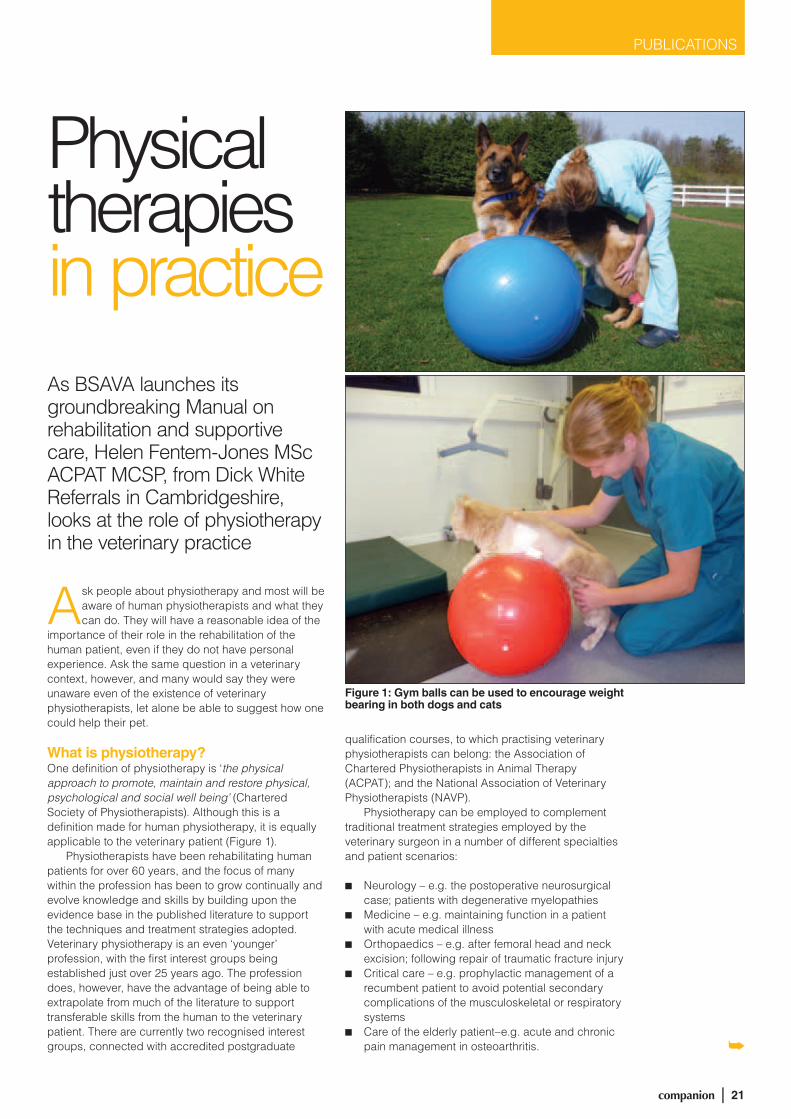
What is physiotherapy?One definition of physiotherapy is ‘the physical approach to promote, maintain and restore physical, psychological and social well being’ (Chartered Society of Physiotherapists). Although this is a definition made for human physiotherapy, it is equally applicable to the veterinary patient (Figure 1).
Physiotherapists have been rehabilitating human patients for over 60 years, and the focus of many within the profession has been to grow continually and evolve knowledge and skills by building upon the evidence base in the published literature to support the techniques and treatment strategies adopted. Veterinary physiotherapy is an even ‘younger’ profession, with the first interest groups being established just over 25 years ago. The profession does, however, have the advantage of being able to extrapolate from much of the literature to support transferable skills from the human to the veterinary patient. There are currently two recognised interest groups, connected with accredited postgraduate
qualification courses, to which practising veterinary physiotherapists can belong: the Association of Chartered Physiotherapists in Animal Therapy (ACPAT); and the National Association of Veterinary Physiotherapists (NAVP).
Physiotherapy can be employed to complement traditional treatment strategies employed by the veterinary surgeon in a number of different specialties and patient scenarios:
■■ Neurology – e.g. the postoperative neurosurgical case; patients with degenerative myelopathies
■■ Medicine – e.g. maintaining function in a patient with acute medical illness
■■ Orthopaedics – e.g. after femoral head and neck excision; following repair of traumatic fracture injury
■■ Critical care – e.g. prophylactic management of a recumbent patient to avoid potential secondary complications of the musculoskeletal or respiratory systems
■■ Care of the elderly patient–e.g. acute and chronic pain management in osteoarthritis.
Physical therapies in practiceAs BSAVA launches its groundbreaking Manual on rehabilitation and supportive care, Helen Fentem-Jones MSc ACPAT MCSP, from Dick White Referrals in Cambridgeshire, looks at the role of physiotherapy in the veterinary practice
PUBLICATIONS
Figure 1: Gym balls can be used to encourage weight bearing in both dogs and cats

22 | companion
PUBLICATIONS
The Veterinary Surgeons Act (1966) requires that physiotherapists work following referral by a veterinary surgeon. This close collaboration between physiotherapists and veterinary surgeons can only work for the better for the patient outcome.
Working togetherCurrently the majority of veterinary surgeons will refer animals requiring physiotherapy to an outpatient physiotherapist. These therapists may work in a number of ways, such as offering outpatient clinics from local veterinary practices, or from their own facilities, or even visiting the patient in their own home.
Once seen by the physiotherapist, the owner will be given a structured home exercise plan, designed on an individual basis to tackle their pet’s specific functional deficits. This will be carried out at home with their pet and the patient’s progress reassessed at regular intervals until the desired goal has been achieved. At the same time the therapist will keep in regular contact with the veterinary surgeon, providing them with updates as to the patient’s progress, as well as highlighting any areas of concern.
At present, inpatient physiotherapists are few and far between, and tend to work predominantly in secondary referral centres. Inpatient physiotherapy has the advantage of being delivered by the therapist much more intensely in the acute stages. This can provide very rapid recovery times in certain patient groups (potentially shortening length of hospital stay) as well as having a prophylactic effect with regard to complications such as respiratory infections. Other advantages include direct face-to-face contact with the vet in charge of the case.
No-one can predict what the future holds; however, the acknowledgment by vets that one method of continuing to advance and improve patient care involves the transposition of treatment strategies employed in the human field, would lead to the more prevalent use of physiotherapy and hydrotherapy, on both an inpatient and an outpatient basis.
TechniquesPhysiotherapists use a number of different treatment strategies to achieve restoration of function, including: movement and rehabilitation therapies; manual
techniques; soft tissue techniques; electrophysical modalities; hydrotherapy; and expert advice.
Movement therapies incorporate a very broad spectrum – from passive range of movement exercises to the obstacle course. Multiple benefits include the nourishment of synovial joints, maintenance of soft tissue length, progressive strengthening of weakened muscle groups (Figure 2), proprioceptive re-education, resorption of oedema, optimising the healing process, analgesic effects and optimising respiratory function.
Physical therapies in practice
Figure 2: Using a Cavaletti pole to encourage strengthening of the flexor muscle groups through greater range
Manual techniques include mobilisations and manipulations of the joints, predominantly for relief of stiffness and/or pain relief. Mobilisations may be physiological (movements done in the same pattern as would be produced voluntarily by the muscles) or accessory (movements that cannot be produced voluntarily, e.g. glides). These techniques can have immediate positive effects in increasing range of movement of a previously limited joint 1. Manual techniques also includes those used to treat the respiratory patient, such as coupage, percussion, ‘rib springing’ and vibrations. When used in combination with positioning for postural drainage and ventilation/perfusion matching, these have been shown to be effective at aiding secretion clearance and improving ventilation.

companion | 23
PUBLICATIONS
Soft tissue techniques include massage, myofascial release, trigger point deactivation and sustained stretches. Massage can be defined as manipulation of the soft tissues to affect a desired system. The systems that can be influenced include muscular, skeletal, digestive, respiratory, circulatory, lymphatic, endocrine, emotional, mental and nervous. The technique can be used to aid lymphatic drainage (resolving oedema), to loosen restricted soft tissue (e.g. muscle spasm of irregular scar tissue) and to aid restoration of normal movement. It can also be used to aid pain relief and to relieve stress 2.
Electrophysical modalities encompass the application of a number of different types of ‘energy’ including therapeutic ultrasound (different wavelengths to diagnostic ultrasound), light energy (lasers), electromagnetic energy (pulsed electromagnetic therapy, PEMT), thermal energy (hot and cold packs) and pulsed electrical impulses (transcutaneous electrical nerve stimulation, TENS; neuromuscular electrical stimulation, NEMS). When prescribed appropriately, these can create multiple positive results. For example, lasers have been show to improve wound healing significantly 3 and PEMT can assist the healing of multiple tissues including soft tissues, bone 4 and nerve. Even something as simple as cold can create profound physiological effects and, when used in combination with compression, has been shown to reduce oedema significantly 5 (Figure 4).
Hydrotherapy is the use of water for therapeutic benefit. It involves the use of properties such as buoyancy, hydrostatic pressure, viscosity, resistance and surface tension, to assist or resist movement according to the desired therapeutic effect. Hydrotherapy can either be done on a water treadmill or within a pool. It can exercise similar muscle groups to land-based exercise but in a more supported environment. If the water depth is to the level of the lateral epicondyle, 15% of the animal’s weight is supported by buoyancy; the exercise can then be progressed by reducing water depth (support) and so strengthening antigravity/extensor muscle groups. Advantages of hydrotherapy include increasing range of movement (so strengthening
Figure 4: Using the principle of ice, elevation and compression to resolve oedema in the limb of a recumbent dog
■■ The NEW Manual for the whole veterinary team■■ Pain management■■ Clinical nutrition■■ Physiotherapy, hydrotherapy, acupuncture■■ Evidence-based and patient-centred■■ Unique case study approach■■ Fully illustrated throughout
Member price £49Available September 2010
…the majority of veterinary surgeons will refer animals
requiring physiotherapy to an outpatient physiotherapist…
PUBLICATIONS
flexor muscle groups through greater range), general cardiovascular fitness, and mental stimulation when on restricted exercise regimes. It is recommended that the hydrotherapist is registered with the Canine Hydrotherapy Association and thus is adequately trained to monitor the patients throughout the course. ■
References 1–5 available to download from www.bsava.com

24 | companion
PETSAVERS
Improving the health of the nation’s pets
London 10KOn 11 July, the World Cup final was not the only sporting event to take place;
over 25,000 runners gathered in London to take part in the British 10K London Run. The Petsavers team had a great day out and despite the hot
weather everyone managed to complete the race. So far this has raised an estimated £2300 for Petsavers, with more sponsorship money to come. If you would like to sponsor this year’s team in retrospect, please visit www.petsavers.org.uk to donate.
If you would like to take part in next year’s 10K then please get in touch early to ensure you get a place as these are limited. If you would like to take part in any other sponsored run or event on behalf of Petsavers, let us know and we can help and support you. ■
Christmas CardsPetsavers produces Christmas cards each
year and this year they are available for a bargain price of £3 for a pack of ten,
including postage and VAT. Petsavers cards are a great way to spread the festive cheer to your friends and colleagues, or you may like to send to cards to your valued clients.
Order forms are available from the BSAVA on request, or cards can be purchased online at www.petsavers.org.uk. If you work in practice and would like to make these available to your clients we can send order forms to you to display in your reception. ■
Photography competitionThe annual Petsavers photography competition is now open, so visit
www.petsavers.org.uk for full details on how to enter. There have been some really creative entries in the past, so this year we’ve
decided to let your imaginations run wild and not limit photos to a particular theme. This means you can send in any picture of your pet you like! The judges will be looking for qualities like humour and character in the photos, as well as photographic skill. The Petsavers website shows the winners of the previous year’s competitions, so take a look to see what has caught the judges’ eyes in the past to give you some ideas. ■
Which bact eria are associated with feline chronic gingivostomatitis?A study undertaken by David Bennett and David Taylor at the Faculty of Veterinary Medicine at the University of Glasgow and Marcello P. Riggio of the Infection & Immunity Research Group at the University of Glasgow Dental School
Inflammatory diseases of the mouth of the cat are very common. Feline chronic gingivostomatitis (FCGS) is
characterised by inflammation of the surfaces of the mouth that extends beyond the tooth region and reaches as far as the back of the throat. It remains the most challenging inflammatory oral disease to treat.
Many different bacterial species, including several previously linked with human periodontal disease, have been implicated in FCGS. Viruses may also play a critical role, with feline herpesvirus (FHV), feline calicivirus, feline immunodeficiency virus (FIV) and feline leukaemia vius (FeLV) the centre of much attention.
The treatment of FCGS is problematic. Simple oral hygiene may be successful in mild cases although extractions are often
Order forms are available from the BSAVA on request, or cards can be purchased
for full details on how to enter. There have been some really creative entries in the past, so this year we’ve
decided to let your imaginations run wild and not limit photos to a particular theme. This means you can send in any picture of your pet you like! The judges will be looking for qualities like humour and character in the photos, as well as photographic skill. The Petsavers website shows the winners of the previous year’s competitions, so take a look to see what has caught the judges’ eyes in the past to give you some ideas. ■
human periodontal disease, have been implicated in FCGS. Viruses may also play a critical role, with feline herpesvirus (FHV), feline calicivirus, feline immunodeficiency virus (FIV) and feline leukaemia vius (FeLV) the centre of much attention.
The treatment of FCGS is problematic. Simple oral hygiene may be successful in mild cases although extractions are often

companion | 25
PETSAVERSPETSAVERS
Which bact eria are associated with feline chronic gingivostomatitis?
necessary, and indeed the most successful treatment for FCGS is extensive (all pre-molar/molar teeth) or full mouth extraction. Antimicrobial treatment is often used but with poor results. Some evidence exists as to the efficacy of interferon-omega in the treatment of this disease, although large-scale controlled studies have not been carried out.
In our study funded by Petsavers we investigated the types of bacteria associated with both FCGS and a healthy oral cavity, using both conventional culture methods, which grow bacteria under laboratory conditions, and also DNA-based methods for identifying bacteria. The advantage of DNA-based identification methods is that, as well as detecting bacteria that can be readily grown in the laboratory, they can also be used to identify bacteria which cannot be grown under laboratory conditions and also bacteria which have never previously been identified.
Three healthy samples were analysed for the presence of bacteria by culture methods and the most frequently found species were Pasteurella pneumotropica (10.3%) and previously uncultured bacteria (10.3%). In the nine FCGS samples analysed, the most frequently found bacteria were Pasteurella multocida subsp. multocida (14.1%), previously uncultured bacteria (14.1%) and Pasteurella multocida subsp. septica (10.6%).
In the same samples, more different types of bacteria were detected using
DNA-based methods. In the healthy samples, the most frequently found bacterium was Capnocytophaga canimorsus (10.8%). For the FCGS samples, the most frequently found bacteria were Pasteurella multocida subsp. multocida (33.1%) and Tannerella forsythensis (13.2%). Overall, fewer types of bacteria were found in the FCGS samples compared to the healthy samples. Bacteria that had not previously been grown in the laboratory were found in both the healthy samples (8.2%) and the FCGS samples (8.4%). Of particular note was the finding that a much larger proportion of novel bacteria that had not previously been identified were found in the healthy
samples (43.7%) compared to the FCGS samples (8.8%).
Two healthy and nine FCGS samples were tested for the presence of FeLV, FIV, FCV and FHV. FeLV and FHV were not detected in any samples. Both healthy samples were positive for the presence of FIV antibodies. FCV was isolated from one of two healthy samples and from seven of nine FCGS samples. We concluded that fewer types of bacteria are found in cats with FCGS than in healthy cats. However, Pasteurella multocida subsp. multocida is found to be significantly more prevalent in FCGS than in healthy cats and, consequently, may play an important role in the disease. ■

26 | companion
World Congress highlightsSome 2,000 people visited Geneva to make the 2010 congress a success
Close to 2,000 attendees from all over the world came together in the international yet intimate, historical and culturally diverse city of Geneva
in Switzerland to learn and to celebrate the collegiality of veterinary medicine. Hosted by the Swiss Association for Small Animal Medicine (SVK-ASMPA), the 35th WSAVA World Congress was held in conjunction with the 16th FECAVA, the 41st SVK-ASMPA, and 5th FAFVAC Congresses. The scientific programme featured 79 world-renowned veterinary lecturers covering over 25 disciplines in 207 lectures with English, French, and German translations, including six State-of-the-Art Lectures (SOTALs). Furthermore, there was WSAVA Human–Animal Interaction, WSAVA Hereditary Diseases, a FECAVA Symposium and a North American Veterinary Conference “How I Treat” stream, as well a Pre-Congress Forum sponsored by the International Veterinary Ear Nose and Throat Association. This was complemented by a range of Short Communications featuring abstracts that highlighted veterinary research from around the globe.
The international appeal of the WSAVA World Congress was reflected in the diversity of the attendees, with 72 countries represented and people from every
continent but Antarctica. The five countries supplying the most delegates were Switzerland, France, United Kingdom, Germany and the United States.
Evenings were spent meeting old friends and making new ones at a variety of lively social events. The Opening Ceremony saw the presentation of the prestigious WSAVA Awards and the evening closed with cocktails served in the Exhibition area. Guests at the Gala evening watched a gorgeous sunset over Lake Geneva and the surrounding mountains, while enjoying an hour-long cruise followed by an elegant dinner aboard the cruise boat. The following night hosted the Swiss Evening Party, which took place at the historic Bâtiment des Forces Motrices, a former hydroelectric plant on the Rhône River, where guests were treated to a variety of Swiss foods, local wine and Swiss music.
As the saying goes “all good things must come to an end”. At the Closing Ceremonies the hard work of the many volunteers was recognized and a presentation was given by next year’s Congress host featuring several traditional Korean dances, which no doubt ensured that many of those present will join their colleagues again for the 36th WSAVA Congress to be held from 14–17 October 2011 on the exotic island of Jeju, Korea.
The Congress was supported by WSAVA Prime Partner Hill’s Pet Nutrition, and partners Nestlé Purina, Novartis and Pfizer Animal Health. They joined the 87 exhibitors in the Exhibition Hall.
For more information and photos from the 2010 WSAVA Congress, visit the WSAVA homepage at www.wsava.org.

companion | 27
WSAVA NEWS
WSAVA Assembly MeetingWSAVA President David Wadsworth provided assembly members with updates from a very active WSAVA leadership, including the Executive Board and various committees. The months since the last meeting at the 2009 WSAVA Congress have seen the WSAVA become an incorporated, not-for-profit entity in Canada, with the WSAVA Charitable Foundation to follow shortly.
The Congress Steering Committee proposed the following motions that will see the vibrant WSAVA Congress enhanced while providing for the future financial sustainability of the WSAVA:
■ The CSC had implemented the Assembly-adopted motion to enter into a preferred partner relationship with a Professional Congress Organizer (PCO) through a Request for Proposal. This narrowed the field to two international PCOs, with final selection of the partner to be based on a case study of the 2014 WSAVA World Congress
■ The WSAVA World Congress will rotate through three global regions, comprised of the Americas; Europe, Africa, and the Middle East; and Oceania/Asia.
The newly elected WSAVA Executive Board (from left to right): Walt Ingwersen, Honorary Secretary (Canada); Di Sheehan, Vice President (Australia); Veronica Leong, Board Member (Hong Kong); Shane Ryan, Honorary Treasurer (Singapore); Jolle Kirpensteijn, President (Netherlands); Peter Ihrke, President Elect (USA); David Wadsworth, Past President (UK)
© Kongressfotos and Karin Degasperi

28 | companion
WSAVA NEWS
These were adopted by a majority vote of 2010 Assembly participants.
WSAVA Officer elections were held, which saw Prof. Jolle Kirpensteijn (Netherlands) assume the WSAVA Presidency. Prof. Peter Ihrke (USA) became President-Elect, Dr Di Sheehan (Australia) moved from Treasurer to Vice President, Dr Veronica Leong (Hong Kong) retained her seat as seventh Board Member, and Dr Shane Ryan (Singapore) joined the Board as Honorary Treasurer. Dr David Wadsworth (UK) assumed the Past Presidency and Dr Walt Ingwersen (Canada) remained as Honorary Secretary.
In addition, the past and ongoing contributions of Prof. Ellen Bjerkås to the WSAVA and international veterinary community were recognized through her receipt of the 2010 WSAVA President’s Award. For more information on this and other WSAVA award winners, please see the July issue or visit the Awards page at www.wsava.org.
The assembly members also voted in favour of accepting one new affiliate member association, the Academy of Veterinary Dentistry. Finally Cape Town, South Africa was voted as the host of the 2014 WSAVA Congress.
More details will be provided in the Assembly Minutes which will be available at www.wsava.org.
Proceedings available onlineProceedings from the WSAVA 2010 World Congress are available online via the WSAVA website (link on the right-hand column of the home page). The WSAVA World Congress proceedings are also available online in a partnership with IVIS (International Veterinary Information Service), a New York-based not-for-profit organization. ■
With a mysterious and unique landscape designated as a World Heritage site by UNESCO, a relaxing atmosphere and a
fascinating traditional culture, Jeju will provide an inspiring and unforgettable backdrop to the WSAVA World Congress being held from 14–17 October 2011.
The Korean Organizing Committee will develop a structured and high-level scientific programme, bringing vets, their families and companies from around the world together to encourage one another and build friendships. Top quality lectures by world-renowned scholars will enable participants to share and expand specialized knowledge and experience. State of the art information will be provided at the exhibition.
An opportunity to experience a truly memorable event awaits you in Jeju, Korea, in 2011. We look forward to meeting and welcoming you. Visit www.wsava2011.com for more information. ■
FUTURE CONGRESSES ■ Jeju, South Korea: 14–17 October 2011 ■ Birmingham, UK: 12–15 April 2012 ■ Christchurch, New Zealand: 6–9 March 2013 ■ Cape Town, South Africa: 15–19 September 2014
Welcome from Jeju!
The Organizing Committee of the 2011 WSAVA World Congress and the 3rd FASAVA Congress welcome you wholeheartedly to Jeju Island, South Korea
© G
abrie
l Pen
t | D
ream
stim
e.co
m

companion | 29
THE companion INTERVIEW
John Tandy
John Tandy was born and grew up in St Helens. His father worked 16-hour days as a railway porter, allotment holder and poultry keeper, while his mother looked after the home and family. He was educated at Cowley High School and was accepted at Liverpool Veterinary School at 17. On qualifying in 1957 he spent three years in large animal practice (two years in Bristol and one in Malton). He then set up his own practice back in his home town at a time when the surge in pedigree dog ownership was taking place. This became one of the earliest registered veterinary hospitals in the UK. He became involved in professional politics, the pharmaceutical industry, producing veterinary educational material, communication training, veterinary journals, recruitment, university activity, animal welfare and conservation charities, and a variety of local organisations. He is a happily married, and very proud father and grandfather. John was the first president of the BVHA, the president of SPVS and the president of the BVA.
QWho has been the most inspiring influence on your professional career?
AThis is an extremely difficult question to answer – there have been so many inspiring people in my life that have had influence on my career. I
must mention the maths master at my school who said “Tandy, one day you will either be Prime Minister or a bandit chief – but which ever it is you will finish up being hanged.” So far all his predictions are wrong! Then there is Professor John George Wright; he was a remarkable influence on me and many other students that he taught. Alf Wight (James Herriott) worked in a neighbouring practice during the time I was in Malton. This man, who had a most remarkable talent, which for a time was not fully appreciated, became a good friend. Lord Soulsby is another inspiring friend and mentor. Nobody has worked so hard on matters relating to the profession, sometimes under very difficult circumstances, than this man. I met Jane Goodall over 30 years ago in the forest of Gombe
Stream in Tanzania, where she was studying her chimpanzees. She is now a world leader in educating mankind in the need to protect our environment and to conserve our wild animal populations.
What is the most frustrating aspect of your work?I have been involved with animal welfare and conservation groups for many years, including 10 years as chairman of the Jane Goodall Institute. I have become frustrated by the fact that I have not been more successful in my efforts to raise sufficient income and improve front line services to make the impact that I would have wished.
What do you regard as the most important decision that you have made in your life?One important decision was to invite Ian Hughes to join me as a partner in the practice. Another was the trip I made a trip to the USA in the mid 1960s to visit veterinary practices. The secretary of the American Animal Hospital Association, Frank Booth, helped

30 | companion
THE companion INTERVIEW
organise the trip. I looked in depth at the construction, design and management of over 30 veterinary practices in all parts of the country. I learned so much. It was life changing. Before I went a senior member of the profession said, “Don’t go John. They have nothing to teach us!” But, thank goodness, I did it my way!
What has been your main interest outside work?Rugby Union has been one of my main interests outside work. When I began my sporting life at grammar school, the rugby master asked what position I played. I confessed that I had never played in any position. He said, “Right, you are a hooker”. That is the position that I played for the next 35 years. I went on to play for the school, the University and St Helens (now Liverpool St Helens) and Malton. My last game was representing past players of the Malton club against the current side. At that time I was president of SPVS and a fellow member of our team was Norman Chandler, then president of BEVA. There’s a challenge for current presidents!
When and where were you the happiest?I thoroughly enjoy travelling the world. I am at my happiest when in the company of my wife, family and friends. It follows that I am at my happiest when viewing the Andes or watching wildebeest migrating across the Mara River, or sipping a glass of wine in their company.
What is the most significant lesson that you have learned so far in life?Frank Sinatra sang “I did it my way” with passion, and then there was the song from South Pacific “You’ve got to have a dream”. Combine the two songs and that is the basis of the lesson that I learned.
If you were given unlimited political power what would you do with it?I would first become Schools Secretary and restore the grammar school system, which allowed people from poorer families to make progress based on ability rather than some contrived political process. Once this had been achieved, I would then become responsible for health services. I would change the current NHS inefficient bureaucratic system to one that involved
more competition for services with patient choice and insurance payments. The premiums of those that could not afford full payment would be subsidised from the vast amounts of savings that would be made. My new system would be based on the prevailing veterinary health system. I realise that there would be some political skirmishing to deal with but then I do have unlimited power, do I not?
Which historical or literary figure do you most identify with – and why?I suppose that I must change the question to “who would I wish to identify with” and then I can say Winston Churchill is the man. It is my view that nobody, at least in my lifetime, has been dealt a challenge of such magnitude as the Second World War. Winston sorted it out with unbelievable courage, clarity of thought, decisive action, leadership skills and eloquence.
If you could change one thing about your appearance or personality, what would it be?My only thought for this was “well you are a bit loud. Maybe you should quieten down a bit”. I sought help from my wife; she suggested that, “You should listen a little more to what other people have to say before you offer your own opinion”. So there you have it!!
What is your most important possession?I first thought that I should say my 22-year-old rusting Mercedes was my most important possession. However, with a little more thought I must declare that it is Ty Mawr, my 300-year-old cottage in the hills of North Wales. This is the place where I have been able to spend so much time relaxing and sharing the odd glass of wine with my family and friends for over 40 years.
What would you have done if you hadn’t chosen to work in the veterinary sphere?Despite the recent bad press over the expenses scandal, I know, personally, MPs who show remarkable dedication. They work long hours, are completely honest and do an important job for their constituents and the country. I have enjoyed every minute of being a veterinary surgeon but my second choice of career would be that of a Member of Parliament. ■
I have enjoyed every minute of being a veterinary surgeon but my second choice of career would be
that of a Member of Parliament.
THE companion INTERVIEW

companion | 31
CPD diaryA broad network of regional branches gives you the potential to meet like-minded colleagues in your area and delivers high-quality CPD on your doorstep. Visit the CPD section at www.bsava.com to find dates for local courses and details for your regional committee.
All dates were correct at time of going to print; however, we would suggest that you contact the organisers for confirmation.
EXCLUSIVE FOR MEMBERSExtra 10% discount on all BSAVA publications for members attending any BSAVA CPD event.
EVENING MEETING – SOUTHERN REGION
Thursday 16 SeptemberOphthalmology: getting the most from your diagnostic instrumentsSpeaker Peter RenwickPotters Heron Hotel, Romsey SO51 9ZFDetails from [email protected]
EVENING MEETING – SOUTH WEST REGION
Wednesday 15 SeptemberCommon feline surgical techniquesSpeaker Colin WhitingJunction 24, Sedgemoor Auction Centre, North Petherton TA6 6DFSponsors NovartisDetail from Rachel Sekules, [email protected], 07791628635
DAY MEETING – NORTH WEST REGION
Wednesday 15 SeptemberDermatological RoadshowSpeakers Andrew Hillier & Sue PatersonMottram Hall, Cheshire SK10 4QTDetails from [email protected]
DAY MEETING – NORTH EAST REGION
Sunday 12 SeptemberAbdominal surgery versus laparoscopyNovotel Hotel, Ponteland Road, Newcastle Upon Tyne NE3 3HZDetails from [email protected]
EVENING MEETING – MIDLANDS REGION
Thursday 23 SeptemberEndocrinology update with case studiesSpeaker Grant PetrieYew Tree, Kegworth, Derby DE74 2DFDetails from [email protected]
DAY MEETING – SOUTH WEST REGION
Monday 20 SeptemberDermatological RoadshowSpeakers Andrew Hillier & Sue PatersonWoodbury Park, Exeter EX5 1JJDetails from [email protected]
DAY MEETING – SOUTHERN REGION
Tuesday 21 SeptemberDermatological RoadshowSpeakers Andrew Hillier & Sue PatersonHampshire Court Hotel, Basingstoke RG24 8FYDetails from [email protected]
EVENING MEETING – KENT REGION
Wednesday 22 SeptemberTop tips for oncological surgerySpeaker Terry EmmersonRussel Hotel, 136 Boxley Road, Maidstone, Kent ME14 2AEDetails from Hannah Perrin, 01304 206989, [email protected]
DAY MEETING – MIDLANDS REGION
Friday 17 SeptemberDermatological RoadshowSpeakers Andrew Hillier & Sue PatersonYew Lodge, Kegworth DE74 2DFDetails from [email protected]
EVENING MEETING – SURREY AND SUSSEX REGION
Wednesday 29 SeptemberSurgery of the upper respiratory tractSpeaker Benito de la PuertaLeatherhead Golf Club, Kingston Road, Leatherhead KT22 0EEDetails from Jo Arthur, 01243 841111, [email protected]
DAY MEETING – SOUTH WEST REGION
Tuesday 28 SeptemberGIT II: oesophagus, stomach and intestinesSpeaker Alex GermanBSAVA, Woodrow House, 1 Telford Way, Gloucester GL2 2ABDetails from Membership and Customer Services Team, 01452 726700, [email protected]
DAY MEETING – NORTH EAST REGION
Sunday 26 SeptemberThrough the keyhole or open doors? – open sesame!Speakers Romain Pizzi & Liz WelshNovotel Hotel, Ponteland Road, Newcastle Upon Tyne NE3 3HZDetails from [email protected]

British Small Animal Veterinary AssociationWoodrow House, 1 Telford Way, Waterwells Business Park,
Quedgeley, Gloucester GL2 2ABTel: 01452 726700 Fax: 01452 726701
Email: [email protected]: www.bsava.com
For more information or to order visit www.bsava.com, email [email protected] or call 01452 726700.Order online to save on Postage & Packing
Special offers on BSAVA Manuals
BSAVA Manual of Small Animal
Dermatology, 2nd editionEdited by Aiden Foster and Carol Foil
■ Practical information ■ Problem-oriented ■ Clinical approach algorithms ■ Boxes highlight clinical entities
HALF PRICE WHILE STOCKS LAST
Member price £55
Non-member price £85
£27
£45
BSAVA Manual of Canine and Feline
Endocrinology, 3rd editionEdited by Carmel Mooney and Mark Peterson
■ Sampling and assays ■ Common laboratory abnormalities ■ Common and uncommon conditions ■ Practical standard chapter format to aid information retrieval
‘…I would thoroughly recommend the manual as an excellent addition to the practice bookshelf...’ Veterinary Record
‘…I would recommend that you have this book in your clinic, and that you set aside a period of time when the book arrives to familiarize yourself with the contents, so you will appear to be a true genius when your next derm case walks in the door…’ Veterinary Information Network
HALF PRICE WHILE STOCKS LAST
Member price £49
Non-member price £75
£25
£40
New editions of both manuals will be published in 2011



















![September2010 Clinical Guidelines[1]](https://img.pdfslide.us/doc/110x75/577c7cc31a28abe0549bee3e/september2010-clinical-guidelines1.jpg)









