Embed Size (px)
DESCRIPTION
bsava revista
Citation preview
The essential publication for BSAVA membersThe essential publication for BSAVA members
companionNOVEMBER 2011
READ DogsLiteracy the canine wayP4
How To…Manage seizures
P14
Congress 2012How to pick your talksP20
A case of epistaxis in a DLH
01 OFC November.indd 1 20/10/2011 08:43
2 | companion
companion
companion is published monthly by the British Small Animal Veterinary Association, Woodrow House, 1 Telford Way, Waterwells Business Park, Quedgeley, Gloucester GL2 2AB. This magazine is a member only benefit and is not available on subscription. We welcome all comments and ideas for future articles.
Tel: 01452 726700Email: [email protected]
Web: www.bsava.com
ISSN: 2041-2487
Editorial BoardEditor – Mark Goodfellow MA VetMB CertVR DSAM DipECVIM-CA MRCVSSenior Vice-President – Grant Petrie MA VetMB CertSAC CertSAM MRCVS
■■ CPD Editorial TeamIan Battersby BVSc DSAM DipECVIM-CA MRCVSEsther Barrett MA VetMB DVDI DipECVDI MRCVSSimon Tappin MA VetMB CertSAM DipECVIM-CA MRCVSPatricia Ibarrola DVM DSAM DipECVIM-CA MRCVS
■■ Features Editorial TeamCaroline Bower BVM&S MRCVSAndrew Fullerton BVSc (Hons) MRCVS
■■ Design and ProductionBSAVA Headquarters, Woodrow House
No part of this publication may be reproduced in any form without written permission of the publisher. Views expressed within this publication do not necessarily represent those of the Editor or the British Small Animal Veterinary Association.
For future issues, unsolicited features, particularly Clinical Conundrums, are welcomed and guidelines for authors are available on request; while the publishers will take every care of material received no responsibility can be accepted for any loss or damage incurred.
BSAVA is committed to reducing the environmental impact of its publications wherever possible and companion is printed on paper made from sustainable resources and can be recycled. When you have finished with this edition please recycle it in your kerbside collection or local recycling point. Members can access the online archive of companion at www.bsava.com .
3 Association News Latest news from BSAVA
4–7 READ Dogs Can reading to dogs aid learning?
8–11 Clinical Conundrum Consider a case of epistaxis in a middle-aged cat
12–13 Publications Helping vets around the world
14–18 How To… Manage seizures
19 CPD Knowledge for nurses
20–22 World Congress Lectures types explained and an extra day of social fun
23 Petsavers Latest fundraising news
24–25 Pet Loss Support in Veterinary Practice A look at how both the profession and pet owners manage grief
26–27 Blood Typing: Positive and Negative Encourage practitioners to blood test
28–29 WSAVA News The World Small Animal Veterinary Association
30–31 The companion Interview Nathalie Wissink-Argilaga
32 CPD Challenge at BVA Congress A report on the BSAVA sessions held at BVA Congress
33 Meet Your Region Spotlight on Surrey & Sussex Region
34–35 CPD Diary What’s on in your area
Additional stock photography Dreamstime.com© Daniel Rajszczak; © Dmccale; © Edite Artmann; © Isselee; © Karen Roach; © Lyn Baxter; © Simon Howden; © Steve Allen; © Toxawww; © Vinicius Tupinamba
Small Animal Medicine Society (SAMSoc) and BSAVA recently produced the first version of the PROTECT poster highlighting the need for appropriate antibacterial use and
providing some suggestions for the empirical therapy of several common medical situations.
It is inevitable that some of these suggestions will be refined as new material comes to light, new research is published, and available products and current practices change. As such the list of suggestions in no way excludes other authorised products should veterinary surgeons believe that they are in their patient’s best interest.
It is SAMSoc and BSAVA’s intention to update this poster when needed. Later editions may differ in content and style. All suggestions for improvements are very welcome; please send them to [email protected].
Already some refinements have been made to the section dealing with ophthalmology and dermatology, thanks to feedback, and we suggest that companion readers might like to update their copies of the poster accordingly. ■
poster notesThank you to those who sent in praise and comments about the special antibiotics edition and the PROTECT poster that came with your October companion. This will be an ongoing project with SAMSoc and updates will appear online at www.bsava.com
Eye infectionsSuspected Chlamydophila:■■ Systemic: doxycycline OR enrofloxacin. Topical fusidic
acid may be added if desired.
Skin infectionsPyoderma:Empirical choice of antibacterials suitable for surface and superficial pyoderma (if no resistance or treatment failure) but culture required for deep pyodermas.■■ Topical: chlorhexidine AND/OR fusidic acid OR silver
sulfadiazine*. (Antifungals for concurrent Malassezia often useful.)
■■ Systemic: recommendations unchanged.
PROTECT
02 Page 02 November.indd 2 20/10/2011 08:42

companion | 3
ASSOCIATION NEWS
Hundreds of members are already enjoying using the Formulary App on their smart phones, and now you can
keep the Procedures to hand too with the latest in the free member-only iPhone and Android Apps from BSAVA. The Association had always planned to extend the number of these digital member benefits, and were particularly spurred on by the comment about the Formulary left by ‘talland’ on the iTunes store – “Absolutely fantastic App – in some ways even easier to use than the book itself. Well done BSAVA. (It’d be great if the Guide to Procedures in Small Animal Practice could be an App too).” Visit www.bsava.com for more details. ■
The British Small Animal Veterinary Association is
delighted to announce the appointment of Dr Sally Everitt as Scientific Policy Officer.
This new post adds to the in-house expertise within the core staff at BSAVA, and Sally joins Dr Frances Barr as one of two highly qualified veterinary surgeons working at the Gloucester HQ. This reinforces the invaluable contribution that the Association’s volunteers provide, as well as making us even more effective in the delivery of timely and relevant material for our members.
Sally qualified from Bristol Vet School in 1981 and spent most of her working life in small animal practice. She also undertook PhD research at the University of Nottingham, looking at the factors which influence clinical decision making in veterinary practice. She says; “I am aware of the constraints of first opinion practice, so I hope that by developing evidence-based resources I can help our members make even more informed decisions about the care of their animal patients.” ■
MRSA WEBINARThe Bella Moss Foundation is holding a CPD webinar entitled Recent advances in the treatment and control of meticillin-resistant staphylococci on 8 December at 9pm. All funds received from sales of this webinar will go directly to the Bella Moss Foundation to help with educational projects for vets and nurses. For more information email [email protected]. ■
New Scientific Policy Officer
On Monday 3 October, demand for places on the 2012 BSAVA postgraduate certificates far outstripped the limited
number of places available on the first year’s intake for the courses in small animal medicine and surgery, with both programmes filling just 20 minutes after the website opened for booking. There is now a waiting list and pre-registration for 2013.
This followed the great success of a debate about postgraduate education hosted by BSAVA in London on 22 September. ‘The future of veterinary postgraduate education – what do we want and what do we need?’ was hosted by BSAVA Director of Education, Dr Frances Barr. She was joined by: Bradley Viner, founder of the Blythwood Veterinary Group and a member of RCVS Council with a doctorate for his studies on the introduction of clinical audit in veterinary practice; Neil Forbes, principal of Great Western Referrals, holder of UK and European diplomas in avian medicine, and president of the European Board of Veterinary Specialisation; and Stephen May, deputy principal with specific responsibilities for teaching at the Royal Veterinary College.
With members of the profession and the attending press considering it a worthwhile debate, BSAVA was pleased to have hosted a successful discussion around the future of postgraduate study. The event was also an opportunity for Education Chair, Sue Paterson, to introduce the guests to BSAVA’s latest initiative, the Nursing Merit Awards, due for launch at BSAVA Congress in 2012, and a way of offering comprehensive and accessible training for key nursing staff. Email [email protected] for more information. ■
Postgrad promise
New Procedures App
She was joined by: Bradley Viner, founder of the
the introduction of clinical audit in veterinary
avian medicine, and president of the European
for teaching at the Royal Veterinary College.
attending press considering it a worthwhile
03 Page 03 November.indd 3 20/10/2011 08:41

4 | companion
READ DOGS
READ dogsIs the READ (Reading Education Assistance Dogs) concept likely to produce real and lasting improvements in a child’s comprehension or does it simply make the act of reading a book more fun? John Bonner talks to the US veterinary surgeon who is looking at the role of canine classroom assistants in helping children to read
There was consistency – though perhaps not a great deal of imagination – in the comments made by children at a South Coast primary
school about a scheme in which dogs are brought into their class every week to sit with them as they read stories. “I really liked it,” said Lewis… “I really liked it,” echoed Cameron… “I liked reading with my dog,” Honey confirmed.
The scheme is targeted at children who are struggling to read, some of whom can be embarrassed to let their teachers and classmates see the difficulties that they are experiencing and may even develop a lasting unwillingness to consider picking up a book for pleasure. However, it seems that if they are allowed to sit alone with a dog, they will start to enjoy the experience of reading, overcome their problems and develop a skill which will be essential for their later success in school and at work.
04-07 READ Dogs.indd 4 20/10/2011 08:41
companion | 5
READ DOGS
That is the theory behind the READ dogs concept which was developed in the late 1990s by Intermountain Therapy Animals, a non-profit organisation based in Salt Lake City, Utah. It originally organised groups of volunteers to take their dogs into hospitals and daycare centres, so the literacy programme was an extension of an existing therapy dog service. “We currently have 1,926 active READ members. There are teams in 49 states, three provinces of Canada, Ireland, Slovenia, Italy, Spain, and England – and the list is growing all the time,” says Lesley Pulsipher, the organisation’s national READ coordinator.
Meeting resistance with evidenceChildren that have taken part in these exercises have clearly enjoyed themselves and their teachers have reported improvements in their reading ability. But those responsible for organising local READ schemes can still face opposition from school authorities who are unconvinced that bringing dogs into primary schools will genuinely improve educational standards and there are fears that the animals could transmit disease or even bite a child.
Dr Lisa Freeman is a lecturer at the Tufts University School of Veterinary Medicine in Grafton, Massachusetts, and an advisor to a local pet therapy group. In August she published a paper on the first study looking to measure accurately the impact of dogs on reading ability. “We are involved in a couple of READ programmes at local libraries. Everybody who participates sees the benefits; it is very obvious how much this helps the children learn to read. But the problem is that there is very little data behind it and for people who aren’t involved it is very easy for them to not believe it works. So as an academic institution we wanted to put some science behind it.”
With her undergraduate student Dawn Lenihan, Lisa set up a small pilot study comparing the reading performance of two groups of 7- or 8-year-old children in the ‘second grade’ of a local elementary school. They went to the library once a week for five weeks during the summer vacation and read aloud either to a READ dog or to an adult. The children’s reading ability was examined at the beginning and end of the trial using a standard academic test, the CBM (Curriculum Based Measurement) test, and their attitude to
reading assessed using another standard procedure, ERAS (Elementary Reading Attitude Survey).
All the children in the READ group enjoyed the process enough to want to continue going to every session but three out of nine children in the control group dropped out at some stage during the five week period. In children of this age, teachers will often notice some deterioration in reading skills during the long summer holiday when the child’s attention is fixed elsewhere. “Those children that just read to people did show this drop off in reading skills which is typically seen over the summer. But in those that read to dogs, not only were they more likely to stay in the group, they stayed more interested in reading and they didn’t show that drop off.”
Positive outcomesThe fact that children in the READ group had higher scores in the ERAS test indicated a more positive attitude to reading, irrespective of whether there is a dog around to hear the story. “This suggests that the READ programme may not only affect the reading ability of children during the programme, but may also make them more receptive to reading programmes in school. This could lead to further differences in the two groups once the school year
04-07 READ Dogs.indd 5 20/10/2011 08:41
6 | companion
READ DOGS
READ dogs
begins, which have not been accounted for in this study,” she explains.
Dr Freeman notes that because of the small size of their study there wasn’t enough statistical power to show significance in all of the parameters being measured. “But it was certainly very encouraging for us to go on to the next step with a larger study.” The children who took part in the pilot had average reading skills but further studies could assess the effects in specific groups, such as slow readers or those learning to read in English as a second language, which is another application of the READ dogs concept in the US.
Further studies could also look more closely at the reasons why the presence of a canine reading partner can help to improve reading skills. Lisa suspects that one factor may be the positive impact that it has on the child’s self esteem. “When they are struggling with confidence or skills these children are often pulled out of class. That can be traumatic for them but when they get to participate in the READ programme they are actually quite proud that they get to go read to a dog – so it is very exciting and reading becomes much more of a fun thing to do.”
Children much older than those in this study may still find reading a chore but it isn’t known whether the same approach will succeed with different age groups.
Lisa suspects that the innocence of children in the 7 and 8 years age group may be an important factor. At this age they still genuinely believe that the dog is listening to everything they say and that it likes looking at the pictures with them, she points out.
Another issue that cannot be ignored is the role of the dog’s owner who will sit in on each reading session. These people are trained by the scheme’s organisers and can play a subtle role in directing the process. “They are trained in teaching the child through the dog. So if a child reads a word incorrectly they won’t say ‘Honey, you read that word wrong’, they will say ‘Hey, my dog didn’t understand that last word you said – could you say it again?’,” Lisa explains.
Dr Freeman’s main research interest is in small animal nutrition but she is keen to carry out more studies on this rather surprising collision between veterinary science and human psychology. “As with all academic studies exploring a new area, this small study raises more questions than it creates answers,” she says. “But if we can show that there are indeed some measurable benefits it will do a great deal to advance the cause of these programmes – to help get more funding and allow them to expand.”
UK involvementAcquiring the information they need to convince the sceptics in schools and local authorities will do a great deal to help READ-based organisations in countries like the UK, where the concept is still in its infancy. One of the first groups to introduce READ-style learning in British schools is Caring Canines, a voluntary body which organises visits by dogs and their handlers to institutions in the Bournemouth area.
Run by Sue Dennett and Julie Lankshear, the organisation was set up in 2006 and has the owners of dogs ranging in size from Yorkshire Terriers to Newfoundlands on its books. The pair have to be very careful about who they take on, so any volunteer wanting to work on their ‘Book Buddy’ scheme has to undergo a Criminal Records Bureau check and must have proved themselves by taking part in visits to other institutions, like hospitals and nursing homes, before they will be allowed to work with children.
Sue says that they have no problems in attracting suitable volunteers and there are plenty of schools and
04-07 READ Dogs.indd 6 20/10/2011 08:41

companion | 7
READ DOGS
...we visit a stroke rehabilitation ward... some of the people there have difficulty
in communicating because their speech is impaired... when there is a
dog... it doesn’t matter how they sound, the dog will always pay attention...
READ DOGS
other institutions that appreciate the benefits of having regular visits by members of the team. However, greater recognition of the value of therapy dogs could help them fight their way through the bureaucratic obstacles that are often put in their way – such as the conflicting demands of adjoining local authorities, and the fact that permission to visit a particular institution may be given or withheld according to the whim of whoever is currently on duty there.
As with their colleagues in Utah, Sue and Julie are promoting the wider benefits of contact with animals for other vulnerable groups, such as the elderly and
infirm. As with the children in the literacy projects, these older people also value the dogs’ attention, affectionate nature and non-judgemental attitude.
“One place that we visit regularly is a stroke rehabilitation ward at one of the local hospitals,” Sue explains. “Some of the people there have difficulty in communicating because their speech is impaired. It is very embarrassing for them to have to repeat everything they say and still not be understood. But when there is a dog there, it doesn’t matter how they sound, the dog will always pay attention and so it encourages them to talk.” ■
companion | 7
04-07 READ Dogs.indd 7 20/10/2011 08:41
8 | companion
CLINICAL CONUNDRUM
Clinical conundrumconundrum
Create a problem list for this patient
n Bilateral epistaxis n Pale mucous membranes n Lethargy n Poor appetite
What are your differentials and can you narrow them based on the information available?It is likely that the pale mucous membranes are a result of anaemia and linked to the epistaxis, given its severity. Lethargy and inappetence are likely to be secondary.
Differential diagnoses for epistaxis can be subdivided into intranasal and extranasal processes.
IntranasalV VascularI IdiopathicT Toxic/Traumatic: Trauma is an uncommon
cause of epistaxis and is unlikely in this case given the duration of the clinical signs and incompatible history.
A Anomalous: A foreign body is a possible differential diagnosis for epistaxis, but less likely in this case given the absence of a mucopurulent discharge prior to the epistaxis. Also, a unilateral discharge would be more likely than bilateral.
M MetabolicI Inflammatory (immune-mediated and
infectious): Fungal infection (e.g. Cryptococcus neoformans and Aspergillus fumigatus) is a possible but uncommon cause of epistaxis in cats.
N Neoplastic/Nutritional: Neoplasia is a possible differential (lymphoma, adenocarcinoma and, less commonly, fibrosarcoma). Most commonly, nasal neoplastic lesions lead to a unilateral discharge and often facial deformity or exophthalmos. These were not noted in this case. However, it is possible for a mass to invade both sides of the nasal cavity, so neoplasia cannot be excluded on this basis alone.
D Degenerative
ExtranasalDifferential diagnoses for extranasal causes of epistaxis can be split into primary (e.g. thrombo-cytopenia) and secondary (e.g. to rodenticide toxicity) coagulation anomalies, and hypertension. Although no other sites of haemorrhage have been detected, a bleeding disorder should be considered in this case because the discharge is bilateral, there is no mucopurulent component, no signs of swelling or pain, and no history of sneezing.
What would be your first diagnostic steps and why?Haematology should be performed to assess platelet number and degree of anaemia, as well as to search for evidence of regeneration as the cat has been showing clinical signs for 1 week. A biochemistry profile should also be run as the patient has had a poor appetite for 1 week, to assess electrolytes and particularly to evaluate any changes suggestive of hepatic lipidosis. Coagulation profiles should be obtained to evaluate both intrinsic and extrinsic pathways, and blood pressure should be measured to investigate possible hypertension. If the blood pressure is elevated, a retinal examination should be performed. FeLV/FIV snap tests should be performed because retroviruses can cause thrombocytopenia, and the
Laura Thornton, intern at Davies Veterinary Specialists, invites companion readers to consider a case of epistaxis in a middle-aged cat
Case presentationA 14-year-old male neutered DLH cat was presented with a week-long history of very severe bilateral epistaxis and poor appetite. The cat had been in a cattery for the preceding week. He was slightly lethargic and pale mucous membranes were noted on physical examination as well as a crusty bloody discharge around both nares. Body condition score was good and the rest of the physical examination was unremarkable.
08-11 Clinical Conundrum.indd 8 20/10/2011 08:40
companion | 9
CLINICAL CONUNDRUM
patient’s blood should be typed in case of the need for transfusion in the future.
Initial results
n For haematology and biochemistry results, see Tables 1 and 2
n APTT = 118 seconds (65–119 seconds) n PT = 21 seconds (15–22 seconds) n Blood type = A n Blood pressure = 155 mmHg n FeLV/FIV negative
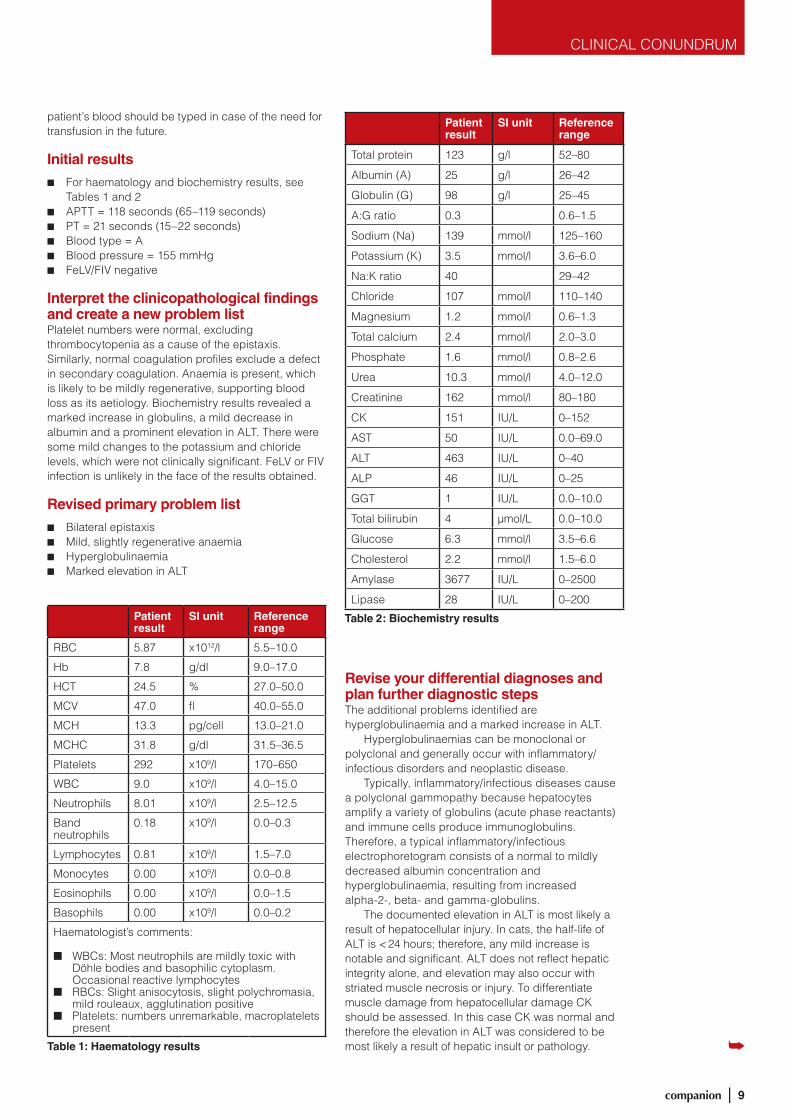
Interpret the clinicopathological findings and create a new problem listPlatelet numbers were normal, excluding thrombocytopenia as a cause of the epistaxis. Similarly, normal coagulation profiles exclude a defect in secondary coagulation. Anaemia is present, which is likely to be mildly regenerative, supporting blood loss as its aetiology. Biochemistry results revealed a marked increase in globulins, a mild decrease in albumin and a prominent elevation in ALT. There were some mild changes to the potassium and chloride levels, which were not clinically significant. FeLV or FIV infection is unlikely in the face of the results obtained.
Revised primary problem list
n Bilateral epistaxis n Mild, slightly regenerative anaemia n Hyperglobulinaemia n Marked elevation in ALT
Revise your differential diagnoses and plan further diagnostic stepsThe additional problems identified are hyperglobulinaemia and a marked increase in ALT.
Hyperglobulinaemias can be monoclonal or polyclonal and generally occur with inflammatory/infectious disorders and neoplastic disease.
Typically, inflammatory/infectious diseases cause a polyclonal gammopathy because hepatocytes amplify a variety of globulins (acute phase reactants) and immune cells produce immunoglobulins. Therefore, a typical inflammatory/infectious electrophoretogram consists of a normal to mildly decreased albumin concentration and hyperglobulinaemia, resulting from increased alpha-2-, beta- and gamma-globulins.
The documented elevation in ALT is most likely a result of hepatocellular injury. In cats, the half-life of ALT is < 24 hours; therefore, any mild increase is notable and significant. ALT does not reflect hepatic integrity alone, and elevation may also occur with striated muscle necrosis or injury. To differentiate muscle damage from hepatocellular damage CK should be assessed. In this case CK was normal and therefore the elevation in ALT was considered to be most likely a result of hepatic insult or pathology.
Patient result
SI unit Reference range
RBC 5.87 x1012/l 5.5–10.0
Hb 7.8 g/dl 9.0–17.0
HCT 24.5 % 27.0–50.0
MCV 47.0 fl 40.0–55.0
MCH 13.3 pg/cell 13.0–21.0
MCHC 31.8 g/dl 31.5–36.5
Platelets 292 x109/l 170–650
WBC 9.0 x109/l 4.0–15.0
Neutrophils 8.01 x109/l 2.5–12.5
Band neutrophils
0.18 x109/l 0.0–0.3
Lymphocytes 0.81 x109/l 1.5–7.0
Monocytes 0.00 x109/l 0.0–0.8
Eosinophils 0.00 x109/l 0.0–1.5
Basophils 0.00 x109/l 0.0–0.2
Haematologist’s comments:
n WBCs: Most neutrophils are mildly toxic with Döhle bodies and basophilic cytoplasm. Occasional reactive lymphocytes
n RBCs: Slight anisocytosis, slight polychromasia, mild rouleaux, agglutination positive
n Platelets: numbers unremarkable, macroplatelets present
Table 1: Haematology results
Patient result
SI unit Reference range
Total protein 123 g/l 52–80
Albumin (A) 25 g/l 26–42
Globulin (G) 98 g/l 25–45
A:G ratio 0.3 0.6–1.5
Sodium (Na) 139 mmol/l 125–160
Potassium (K) 3.5 mmol/l 3.6–6.0
Na:K ratio 40 29–42
Chloride 107 mmol/l 110–140
Magnesium 1.2 mmol/l 0.6–1.3
Total calcium 2.4 mmol/l 2.0–3.0
Phosphate 1.6 mmol/l 0.8–2.6
Urea 10.3 mmol/l 4.0–12.0
Creatinine 162 mmol/l 80–180
CK 151 IU/L 0–152
AST 50 IU/L 0.0–69.0
ALT 463 IU/L 0–40
ALP 46 IU/L 0–25
GGT 1 IU/L 0.0–10.0
Total bilirubin 4 µmol/L 0.0–10.0
Glucose 6.3 mmol/l 3.5–6.6
Cholesterol 2.2 mmol/l 1.5–6.0
Amylase 3677 IU/L 0–2500
Lipase 28 IU/L 0–200
Table 2: Biochemistry results
08-11 Clinical Conundrum.indd 9 20/10/2011 08:40
10 | companion
CLINICAL CONUNDRUM
Clinical conundrum
Differentials for a polyclonal gammopathy
1. Infectious disease. Chronic suppurative processes (e.g. pyometra, pyoderma) can cause polyclonal gammopathies, although these are not compatible with the history or physical examination in this case. FIP and Mycoplasma haemofelis can also cause a polyclonal gammopathy; and, of these, FIP is to be considered the more likely given the magnitude of the gammopathy.
2. Immune-mediated diseases such as polyarthritis and systemic lupus erythematosus. These are unlikely in this patient.
3. Neoplasia. Rarely, mast cell tumours, lymphomas and some necrotic masses can cause a polyclonal gammopathy.
Differentials for monoclonal gammopathiesWhen one clone of immune cells produces an identical type and subtype of immunoglobulin, a monoclonal gammopathy occurs. In cats, these gammopathies are most commonly due to neoplasia (particularly multiple myeloma or lymphoma) but rarely they do occur with FIP.
What is the next diagnostic step?At this stage, a unifying diagnosis which explains the clinical signs (principally epistaxis) and the clinicopathological findings (hyperglobulinaemia and elevated ALT) has not been reached. Whilst coagulation times and platelet numbers were normal, platelet function has not been evaluated as a cause of the epistaxis. A buccal mucosal bleeding time (BMBT) test should ideally be performed to assess platelet function; however, in this patient it proved impossible to perform the test. Determining whether the hyperglobulinaemia is polyclonal or monoclonal, using serum electrophoresis, will narrow the differential diagnosis list. In addition, an ultrasound examination of the abdomen should be performed, specifically concentrating on the liver.
ResultsElectrophoresis revealed a monoclonal hyperglobulinaemia (Table 3) and the ultrasound examination of the abdomen revealed a hyperechogenic hepatic parenchyma.
Revised differential diagnoses and diagnostic planThe finding of a monoclonal gammopathy narrows the differential list to lymphoproliferative neoplasia
(multiple myeloma, lymphoma, plasma cell neoplasia) and, although less likely, FIP. In addition, the epistaxis can be explained by platelet dysfunction caused by the monoclonal gammopathy.
Although the clinicopathological findings are not typical for FIP, further information is required to differentiate these conditions.
Thoracic radiographs (two laterals & DV) are required to screen for, and to evaluate the vertebrae and long bones for any evidence of, neoplasia. If unremarkable, a liver biopsy and bone marrow biopsy (to evaluate for occult neoplasia) should be considered. At this stage and whilst the cat is under general anaesthetic, an oesophagostomy tube should be placed to provide nutrition. In this case a naso-oesophageal tube was contraindicated due to the epistaxis. Although placement of an oesophageal tube is associated with a risk of bleeding given this cat’s bleeding tendency, it was felt that the need for nutrition was of greater concern.
Further test resultsRadiographs of the thorax, abdomen and axial skeleton were unremarkable. At this point it was unclear whether hepatic or bone marrow sampling would provide more information. It was considered possible that the hepatic changes were related to the hyperglobulinaemia, but given the cat’s history these changes could also represent hepatic lipidosis. Given that the patient was under general anaesthetic it was elected to perform bone marrow aspiration before obtaining an aspirate from the liver, as this would be the safer of the two diagnostic techniques given the platelet dysfunction.
Bone marrow aspirates were normal with no evidence of neoplasia so, following discussion of the
Patient result
SI unit Reference range
Total protein
95 g/l 54.0–77.0
Albumin 23.10 g/l 20.0–40.0
Alpha-1 globulin
2.29 g/l 2.0–5.0
Alpha-2 globulin
7.51 g/l 3.5–11.5
Beta globulin
8.80 g/l 10.0–18.0
Gamma globulin
53.30 g/l 5.0–12.0
Table 3: Electrophoresis results
08-11 Clinical Conundrum.indd 10 20/10/2011 08:40
companion | 11
CLINICAL CONUNDRUM
risks involved with the owner, ultrasound-guided FNA of the liver was performed.
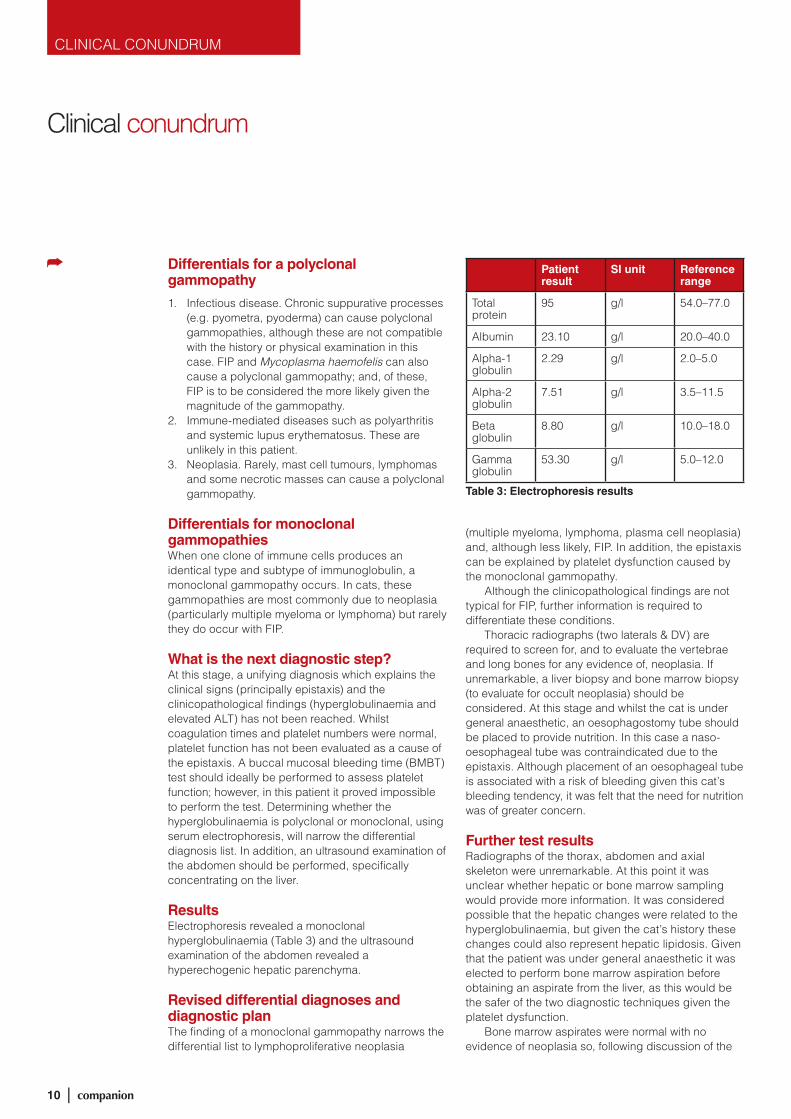
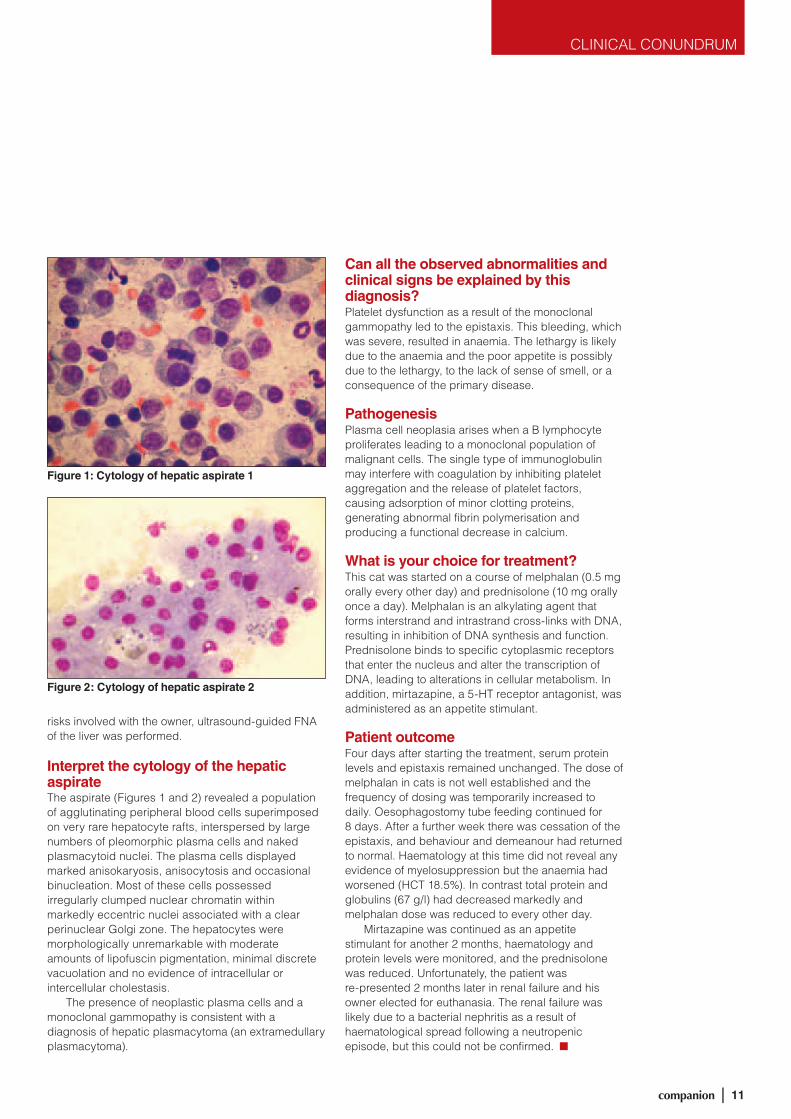
Interpret the cytology of the hepatic aspirateThe aspirate (Figures 1 and 2) revealed a population of agglutinating peripheral blood cells superimposed on very rare hepatocyte rafts, interspersed by large numbers of pleomorphic plasma cells and naked plasmacytoid nuclei. The plasma cells displayed marked anisokaryosis, anisocytosis and occasional binucleation. Most of these cells possessed irregularly clumped nuclear chromatin within markedly eccentric nuclei associated with a clear perinuclear Golgi zone. The hepatocytes were morphologically unremarkable with moderate amounts of lipofuscin pigmentation, minimal discrete vacuolation and no evidence of intracellular or intercellular cholestasis.
The presence of neoplastic plasma cells and a monoclonal gammopathy is consistent with a diagnosis of hepatic plasmacytoma (an extramedullary plasmacytoma).
Can all the observed abnormalities and clinical signs be explained by this diagnosis?Platelet dysfunction as a result of the monoclonal gammopathy led to the epistaxis. This bleeding, which was severe, resulted in anaemia. The lethargy is likely due to the anaemia and the poor appetite is possibly due to the lethargy, to the lack of sense of smell, or a consequence of the primary disease.
PathogenesisPlasma cell neoplasia arises when a B lymphocyte proliferates leading to a monoclonal population of malignant cells. The single type of immunoglobulin may interfere with coagulation by inhibiting platelet aggregation and the release of platelet factors, causing adsorption of minor clotting proteins, generating abnormal fibrin polymerisation and producing a functional decrease in calcium.
What is your choice for treatment?This cat was started on a course of melphalan (0.5 mg orally every other day) and prednisolone (10 mg orally once a day). Melphalan is an alkylating agent that forms interstrand and intrastrand cross-links with DNA, resulting in inhibition of DNA synthesis and function. Prednisolone binds to specific cytoplasmic receptors that enter the nucleus and alter the transcription of DNA, leading to alterations in cellular metabolism. In addition, mirtazapine, a 5-HT receptor antagonist, was administered as an appetite stimulant.
Patient outcomeFour days after starting the treatment, serum protein levels and epistaxis remained unchanged. The dose of melphalan in cats is not well established and the frequency of dosing was temporarily increased to daily. Oesophagostomy tube feeding continued for 8 days. After a further week there was cessation of the epistaxis, and behaviour and demeanour had returned to normal. Haematology at this time did not reveal any evidence of myelosuppression but the anaemia had worsened (HCT 18.5%). In contrast total protein and globulins (67 g/l) had decreased markedly and melphalan dose was reduced to every other day.
Mirtazapine was continued as an appetite stimulant for another 2 months, haematology and protein levels were monitored, and the prednisolone was reduced. Unfortunately, the patient was re-presented 2 months later in renal failure and his owner elected for euthanasia. The renal failure was likely due to a bacterial nephritis as a result of haematological spread following a neutropenic episode, but this could not be confirmed. n
Figure 1: Cytology of hepatic aspirate 1
Figure 2: Cytology of hepatic aspirate 2
08-11 Clinical Conundrum.indd 11 20/10/2011 08:40

12 | companion
PUBLICATIONS
report on her time in the South Pacific.“The Esther Honey Foundation is a
registered non-profit organisation based on Rarotonga, the largest of the Cook Islands. Established in 1994 by Sue Ragan-Anusen, the Esther Honey Foundation is the sole provider of veterinary care to the thousands of companion animals in the Cook Islands. The day-to-day activities of the clinic are managed by volunteers (Figure 1) and funded entirely by donations. A basic veterinary clinic, temporary animal shelter and rehoming service are run by the Foundation.
Activities at the clinic cover the full spectrum of small animal practice, although a large number of the cases seen are as a result of trauma. These are especially interesting as without a functional X-ray machine, you are very reliant on your fingers to detect fractures. A lot of time is also devoted to nursing animals back to health, that have been poisoned by fish – caused by a neurotoxin found in the lagoon fish on Rarotonga and
Aitutaki; clinical signs range from mild ataxia to recumbency and opisthotonus. Many of these cases require intensive nursing for weeks, not to mention diazepam and methocarbamol.
The activities of the Foundation are by no means restricted solely to Rarotonga with Vet Treks® to various other South Pacific Islands forming an important aspect of their programme. To date the Foundation has run over 100 Vet Treks® to the remote outer Cook and South Pacific Islands, including Atiu, Aitutaki and Mangaia, allowing local animals access to veterinary care (Figure 2). Treks only occur once or twice a year to each island, so the cases that present are both varied and challenging and range from inappetent cats with a significant dermatology complaint to scouring goats. Vet Treks® also play an important role in stabilising the local animal population, aiming to neuter 70% of canine and feline populations. This goal has been achieved on two islands so far, including Rarotonga.
Helping vets around the worldMany veterinary surgeons around the world are doing a great job under difficult conditions and with limited resources. Penny Watson, Chair of the Publications Committee, highlights some of the donations of BSAVA Manuals made this year
Figure 1: Volunteers working at the Esther
Honey Foundation clinic in April this year
BSAVA Publications has made a number of donations to worthy causes during 2011, including the
Esther Honey Foundation in the Cook Islands and the Watamu Turtle Centre in Kenya. The donation of BSAVA Manuals helps provide study books to veterinary surgeons who have difficulty in accessing good sources of information for their continuing professional development. The Publications Committee feels that this is a rewarding and important contribution to small animal veterinary medicine worldwide.
The Esther Honey Foundation – Cook IslandsAt the beginning of the year Eilidh Hawkins from Glasgow approached BSAVA to ask whether we would be able to donate a copy of the BSAVA Guide to Procedures in Small Animal Practice to the Esther Honey Foundation where she was volunteering for the next few months – we were happy to oblige – and Eilidh sent us the following
12-13 Publications.indd 12 20/10/2011 08:39
companion | 13
PUBLICATIONS
Figure 4: Ian Mellor presenting Dr Demirkan with a copy of the latest BSAVA Manual of Oncology
Figure 3: Professor Cooper presenting Ms Parazzi and Dr Faisal with a copy of the BSAVA Manual of Reptiles
Figure 2: Patients being seen during a recent Vet Trek®
As a vet, this is about as close to working in paradise as you can get; however, it does present its own set of challenges: spaying dogs in a bar on a picnic table, whilst you kneel on the floor, with lots of spectators asking questions is a long way from your average operating room.” For further information regarding donations or how to volunteer, visit www.estherhoney.org.
IVSA Denmark – BelgradeAt BSAVA Congress this year, Michelle Christensen from the Danish chapter of the International Veterinary Students Association (IVSA) approached BSAVA with a request for assistance. The goals of the IVSA include providing benefit to the animals and people of the world by harnessing the potential and dedication of veterinary students to promote the international application of veterinary skills, education and knowledge. Ms Christensen explained that at the recent IVSA Symposium, ISVA Denmark were approached by the chapter from Belgrade to help update their small outdated library, which was preventing the students from gaining the knowledge and skills they would like to in the course of their academic studies. BSAVA was happy to donate a number of Manuals covering anaesthesia and analgesia, oncology, reproduction and veterinary care to the ‘Books for Belgrade’ project.
Helping vets around the world
Watamu Turtle Centre – KenyaIn May, Professor John Cooper and Mrs Margaret Cooper participated in a two-day course on the health, welfare and conservation of sea turtles held jointly at Watamu Turtle Centre and Bio-Ken (a research centre dealing with reptiles) in Kenya. The course consisted of both lectures and practical workshops, covering the following areas:
■■ Lectures: turtle conservation, biology, health, law, ethics, examination and diagnosis of samples, and disease control
■■ Practical workshops: handling, sampling, health monitoring, basic veterinary techniques, and investigation of clinical cases.
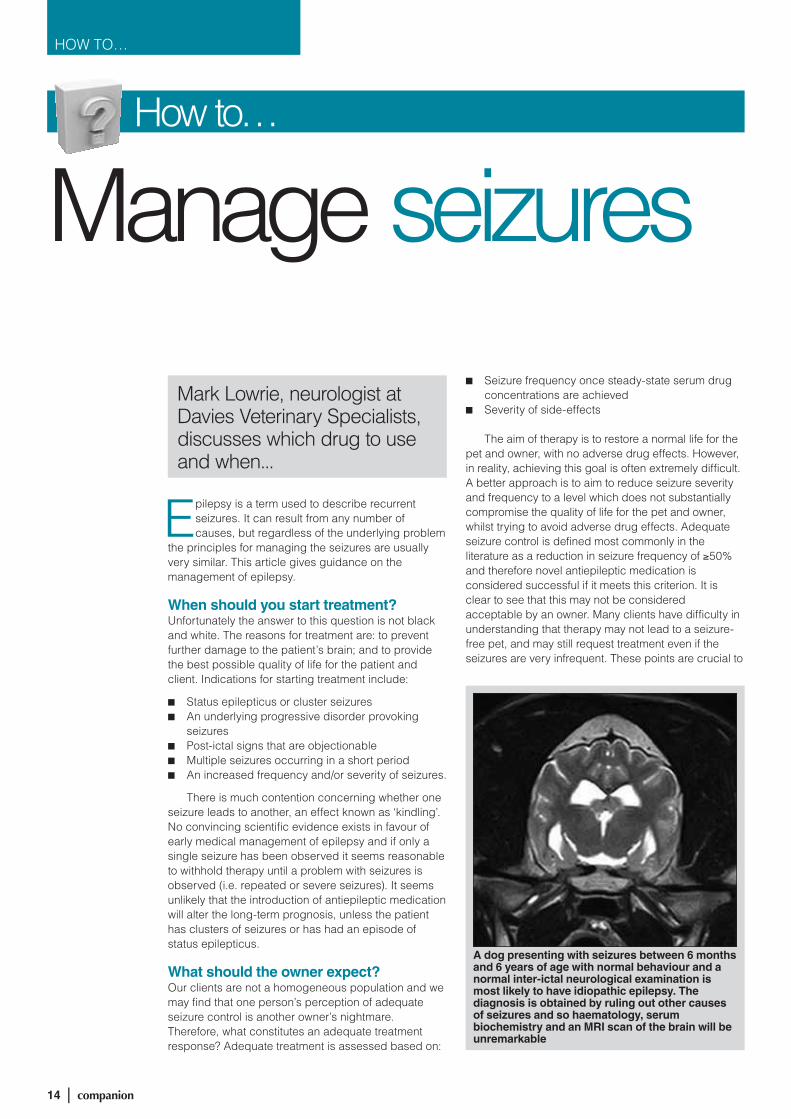
During their visit, Professor Cooper presented a copy of the BSAVA Manual of Reptiles, 2nd edition to Nicky Parazzi, Trustee of the Watamu Turtle Centre and Dr Faraj Faisal, veterinary surgeon at the Centre (Figure 3).
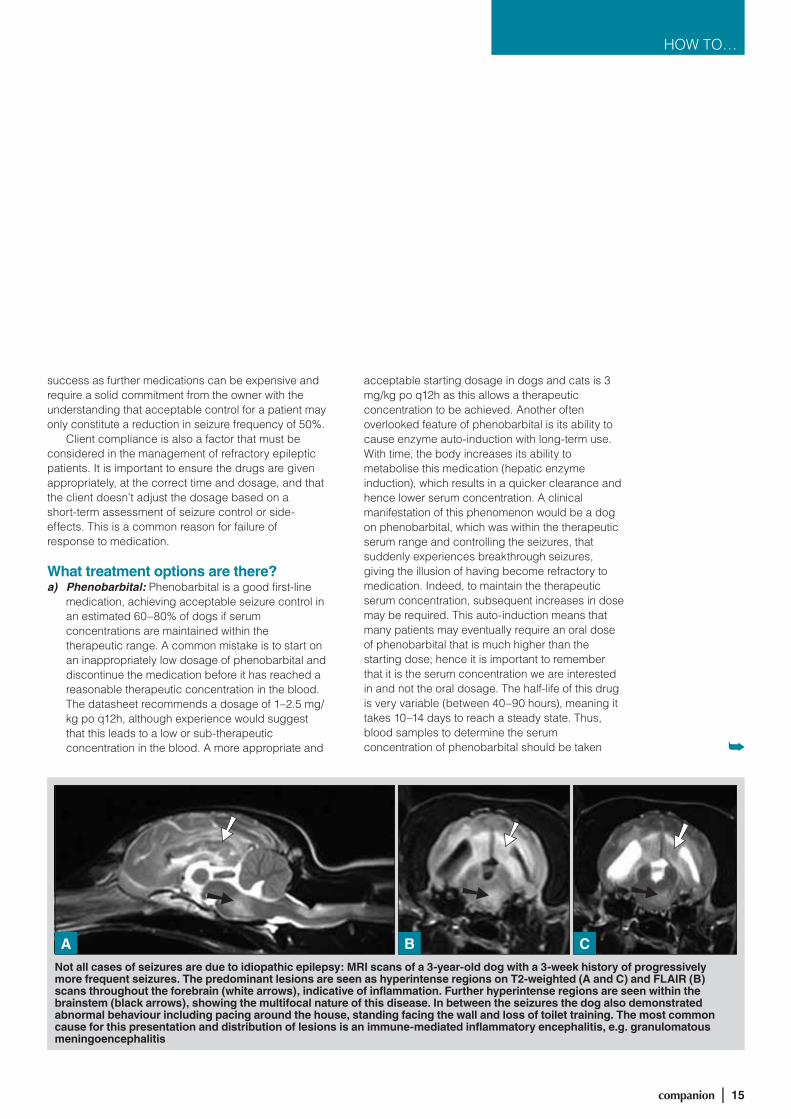
Oncological Society – TurkeyAt the FECAVA Conference held in Istanbul during September, Ian Mellor (BSAVA’s Publications Manager) presented Professor Dr Ibrahim Demirkan, President of the Turkish Oncological Society (Figure 4), with a copy of the BSAVA Manual of Canine and Feline Oncology, 3rd edition. ■
BREATHE NEW LIFE INTO yOUR OLD BOOKSBSAVA will be inviting you to bring your older Manuals and textbooks to BSAVA Congress in support of Worldwide Veterinary Service. Luke Gamble, the founder and chief executive of WVS, graduated from Bristol in 1999 and established this charity in 2003 to provide a sustainable veterinary resource to help animal organisations around the world. There will be more information and a reminder nearer the time, but if you could set aside your older material now, we will work with WVS to give them a new and useful life elsewhere.
Visit www.wvs.org.uk or email [email protected] for more details.
12-13 Publications.indd 13 20/10/2011 08:39
14 | companion
HOW TO…
Mark Lowrie, neurologist at Davies Veterinary Specialists, discusses which drug to use and when...
How to…
Manage seizures
Epilepsy is a term used to describe recurrent seizures. It can result from any number of causes, but regardless of the underlying problem
the principles for managing the seizures are usually very similar. This article gives guidance on the management of epilepsy.
When should you start treatment?Unfortunately the answer to this question is not black and white. The reasons for treatment are: to prevent further damage to the patient’s brain; and to provide the best possible quality of life for the patient and client. Indications for starting treatment include:
■■ Status epilepticus or cluster seizures■■ An underlying progressive disorder provoking
seizures■■ Post-ictal signs that are objectionable■■ Multiple seizures occurring in a short period■■ An increased frequency and/or severity of seizures.
There is much contention concerning whether one seizure leads to another, an effect known as ‘kindling’. No convincing scientific evidence exists in favour of early medical management of epilepsy and if only a single seizure has been observed it seems reasonable to withhold therapy until a problem with seizures is observed (i.e. repeated or severe seizures). It seems unlikely that the introduction of antiepileptic medication will alter the long-term prognosis, unless the patient has clusters of seizures or has had an episode of status epilepticus.
What should the owner expect?Our clients are not a homogeneous population and we may find that one person’s perception of adequate seizure control is another owner’s nightmare. Therefore, what constitutes an adequate treatment response? Adequate treatment is assessed based on:
■■ Seizure frequency once steady-state serum drug concentrations are achieved
■■ Severity of side-effects
The aim of therapy is to restore a normal life for the pet and owner, with no adverse drug effects. However, in reality, achieving this goal is often extremely difficult. A better approach is to aim to reduce seizure severity and frequency to a level which does not substantially compromise the quality of life for the pet and owner, whilst trying to avoid adverse drug effects. Adequate seizure control is defined most commonly in the literature as a reduction in seizure frequency of ≥50% and therefore novel antiepileptic medication is considered successful if it meets this criterion. It is clear to see that this may not be considered acceptable by an owner. Many clients have difficulty in understanding that therapy may not lead to a seizure-free pet, and may still request treatment even if the seizures are very infrequent. These points are crucial to
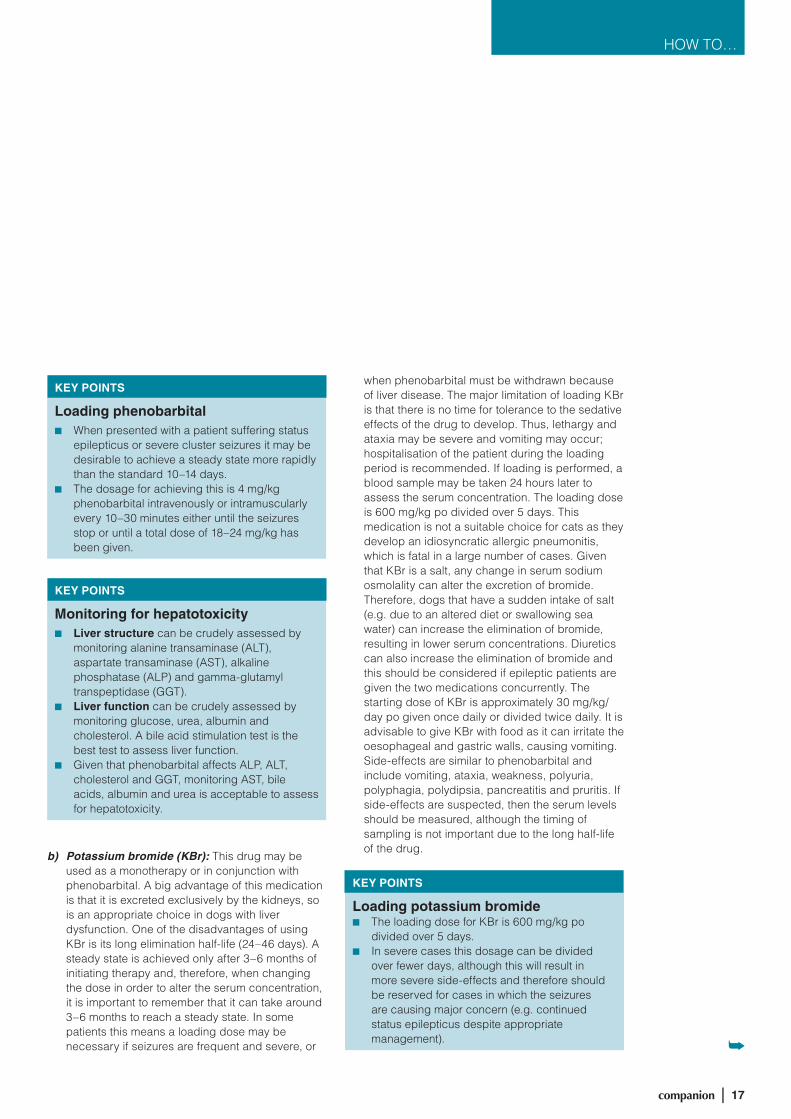
A dog presenting with seizures between 6 months and 6 years of age with normal behaviour and a normal inter-ictal neurological examination is most likely to have idiopathic epilepsy. The diagnosis is obtained by ruling out other causes of seizures and so haematology, serum biochemistry and an MRI scan of the brain will be unremarkable
14-18 How To.indd 14 20/10/2011 08:38
companion | 15
HOW TO…
success as further medications can be expensive and require a solid commitment from the owner with the understanding that acceptable control for a patient may only constitute a reduction in seizure frequency of 50%.
Client compliance is also a factor that must be considered in the management of refractory epileptic patients. It is important to ensure the drugs are given appropriately, at the correct time and dosage, and that the client doesn’t adjust the dosage based on a short-term assessment of seizure control or side-effects. This is a common reason for failure of response to medication.
What treatment options are there?a) Phenobarbital: Phenobarbital is a good first-line
medication, achieving acceptable seizure control in an estimated 60–80% of dogs if serum concentrations are maintained within the therapeutic range. A common mistake is to start on an inappropriately low dosage of phenobarbital and discontinue the medication before it has reached a reasonable therapeutic concentration in the blood. The datasheet recommends a dosage of 1–2.5 mg/kg po q12h, although experience would suggest that this leads to a low or sub-therapeutic concentration in the blood. A more appropriate and
acceptable starting dosage in dogs and cats is 3 mg/kg po q12h as this allows a therapeutic concentration to be achieved. Another often overlooked feature of phenobarbital is its ability to cause enzyme auto-induction with long-term use. With time, the body increases its ability to metabolise this medication (hepatic enzyme induction), which results in a quicker clearance and hence lower serum concentration. A clinical manifestation of this phenomenon would be a dog on phenobarbital, which was within the therapeutic serum range and controlling the seizures, that suddenly experiences breakthrough seizures, giving the illusion of having become refractory to medication. Indeed, to maintain the therapeutic serum concentration, subsequent increases in dose may be required. This auto-induction means that many patients may eventually require an oral dose of phenobarbital that is much higher than the starting dose; hence it is important to remember that it is the serum concentration we are interested in and not the oral dosage. The half-life of this drug is very variable (between 40–90 hours), meaning it takes 10–14 days to reach a steady state. Thus, blood samples to determine the serum concentration of phenobarbital should be taken
Not all cases of seizures are due to idiopathic epilepsy: MRI scans of a 3-year-old dog with a 3-week history of progressively more frequent seizures. The predominant lesions are seen as hyperintense regions on T2-weighted (A and C) and FLAIR (B) scans throughout the forebrain (white arrows), indicative of inflammation. Further hyperintense regions are seen within the brainstem (black arrows), showing the multifocal nature of this disease. In between the seizures the dog also demonstrated abnormal behaviour including pacing around the house, standing facing the wall and loss of toilet training. The most common cause for this presentation and distribution of lesions is an immune-mediated inflammatory encephalitis, e.g. granulomatous meningoencephalitis
A B C
14-18 How To.indd 15 20/10/2011 08:38

16 | companion
HOW TO…
Manage seizures
2 weeks after any dose change. The main factor to consider when obtaining these samples is to ensure that the specimen is always collected at the same time of day, to avoid comparing peak and trough serum levels within the same individual. In summary serum concentrations should be measured approximately 10–14 days after starting treatment. Additionally, they should be repeated every 3–6 months to monitor for auto-induction. Further indications for monitoring serum concentrations include poorly controlled seizures, following any dose change or suspected drug-related adverse effects. Sedation and ataxia are common adverse effects seen with this medication, although, they are usually transient and only persists in some cases. Polyphagia, polydipsia and polyuria are also frequently encountered and are usually dose-related. Other side-effects that occur
with phenobarbital are classified as idiosyncratic, as they seem to be related to neither dose nor prolonged administration. These include hyperexcitability, acute hepatotoxicity, blood dyscrasias (e.g. thrombocytopenia, anaemia or leucopenia) and superficial necrolytic dermatitis. Hepatic toxicity is one of the more serious side-effects and can be difficult to detect. Given that phenobarbital induces hepatic enzymes, it is not unexpected to see elevations in liver enzymes suggesting that the hepatic structure has been altered. However, hepatic function is more important in a patient on phenobarbital therapy and should be assessed by monitoring albumin, urea, cholesterol and glucose levels as well as performing a bile acid stimulation test. It is recommended that these tests are performed every 6 months as routine.
Not all cases of seizures are due to idiopathic epilepsy: MRI of a 13-year-old dog that had suffered only three seizures in the last 6 weeks and had a normal neurological examination and was normal inter-ictally. A dog that first presents with seizures over the age of 6 years is more likely to have an identifiable underlying cause for the seizures. T2-weighted (A), FLAIR (B), and pre- (C) and post-contrast (D) T1-weighted transverse images are presented. The images reveal an ill-defined high signal intraparenchymal lesion of the left parietal lobe on T2-weighted and FLAIR images (black arrows) likely to represent oedema. Following administration of contrast (D) an extra-axial homogeneous hyperintense lesion becomes apparent, with a broad-based meningeal association (white arrows). In this case the imaging findings were compatible with an intracranial extra-axial neoplasm, with a meningioma seeming most likely.
A
DC
B
14-18 How To.indd 16 20/10/2011 08:38
companion | 17
HOW TO…
b) Potassium bromide (KBr): This drug may be used as a monotherapy or in conjunction with phenobarbital. A big advantage of this medication is that it is excreted exclusively by the kidneys, so is an appropriate choice in dogs with liver dysfunction. One of the disadvantages of using KBr is its long elimination half-life (24–46 days). A steady state is achieved only after 3–6 months of initiating therapy and, therefore, when changing the dose in order to alter the serum concentration, it is important to remember that it can take around 3–6 months to reach a steady state. In some patients this means a loading dose may be necessary if seizures are frequent and severe, or
KEY POINTS
Loading potassium bromide■■ The loading dose for KBr is 600 mg/kg po
divided over 5 days.■■ In severe cases this dosage can be divided
over fewer days, although this will result in more severe side-effects and therefore should be reserved for cases in which the seizures are causing major concern (e.g. continued status epilepticus despite appropriate management).
KEY POINTS
Loading phenobarbital■■ When presented with a patient suffering status
epilepticus or severe cluster seizures it may be desirable to achieve a steady state more rapidly than the standard 10–14 days.
■■ The dosage for achieving this is 4 mg/kg phenobarbital intravenously or intramuscularly every 10–30 minutes either until the seizures stop or until a total dose of 18–24 mg/kg has been given.
KEY POINTS
Monitoring for hepatotoxicity■■ Liver structure can be crudely assessed by
monitoring alanine transaminase (ALT), aspartate transaminase (AST), alkaline phosphatase (ALP) and gamma-glutamyl transpeptidase (GGT).
■■ Liver function can be crudely assessed by monitoring glucose, urea, albumin and cholesterol. A bile acid stimulation test is the best test to assess liver function.
■■ Given that phenobarbital affects ALP, ALT, cholesterol and GGT, monitoring AST, bile acids, albumin and urea is acceptable to assess for hepatotoxicity.
when phenobarbital must be withdrawn because of liver disease. The major limitation of loading KBr is that there is no time for tolerance to the sedative effects of the drug to develop. Thus, lethargy and ataxia may be severe and vomiting may occur; hospitalisation of the patient during the loading period is recommended. If loading is performed, a blood sample may be taken 24 hours later to assess the serum concentration. The loading dose is 600 mg/kg po divided over 5 days. This medication is not a suitable choice for cats as they develop an idiosyncratic allergic pneumonitis, which is fatal in a large number of cases. Given that KBr is a salt, any change in serum sodium osmolality can alter the excretion of bromide. Therefore, dogs that have a sudden intake of salt (e.g. due to an altered diet or swallowing sea water) can increase the elimination of bromide, resulting in lower serum concentrations. Diuretics can also increase the elimination of bromide and this should be considered if epileptic patients are given the two medications concurrently. The starting dose of KBr is approximately 30 mg/kg/day po given once daily or divided twice daily. It is advisable to give KBr with food as it can irritate the oesophageal and gastric walls, causing vomiting. Side-effects are similar to phenobarbital and include vomiting, ataxia, weakness, polyuria, polyphagia, polydipsia, pancreatitis and pruritis. If side-effects are suspected, then the serum levels should be measured, although the timing of sampling is not important due to the long half-life of the drug.
14-18 How To.indd 17 20/10/2011 08:38

18 | companion
HOW TO…
Manage seizures
c) Rectal diazepam: Rectal diazepam can be extremely useful, particularly in dogs with severe cluster seizures. Rectal absorption is comparatively faster than oral or intramuscular absorption, occurring within 10 minutes. The recommended dose is 0.5–2 mg/kg for a maximum of three treatments within 24 hours. This is usually used as an adjunct to the above medications as opposed to an alternative.
d) Levetiracetam (Keppra): This is a relatively new medication that is reserved for those patients who fail to respond to phenobarbital and KBr or, in the case of cats, phenobarbital alone. It has a unique mechanism of action, which is a potential advantage when the drug is used in combination with other antiepileptic medications. The half-life of this drug is 4–6 hours, meaning that a steady state is achieved within 48 hours, but also that frequent administration is necessary. It is primarily excreted by the kidneys, making it a suitable choice in patients with liver disease. Its efficacy is initially excellent and the recommended starting dosage is 20 mg/kg po q8h. In a study of 14 dogs with refractory idiopathic epilepsy, 9 dogs responded to the addition of levetiracetam to the drug regimen (i.e. seizure frequency decreased by >50% in these patients). The drug was well tolerated by all dogs in the study and sedation was the only side-effect reported in just one of the 14 dogs. However, of the 9 dogs that responded to levetiracetam, two-thirds experienced an increase in seizure frequency after 4–8 months. Therefore, some dogs that initially
improve on levetiracetam therapy may return to the baseline seizure frequency after 4–8 months (the so-called ‘honeymoon effect’). Thus, this drug may be useful for dogs demonstrating cluster seizures who have numerous seizure episodes within 24–72 hours but a relatively long inter-ictal period between clusters (usually weeks to months). The short-term addition of levetiracetam for the duration of the cluster can reduce the number of seizures during the episode. The drug can be used at a dose of 10–30 mg/kg po q8h for the duration of the cluster (usually 2–3 days) and then stopped again until the start of the next cluster. No study has proven the efficacy of ‘pulse-dosing’ but anecdotally it has been useful in patients and appears to offset the ‘honeymoon effect’. The main factor limiting the use of levetiracetam in dogs and cats is its expense, although it is slowly becoming more affordable, particularly in small dogs and cats.
PRACTICAL TIP
Using levetiracetamOccasionally a patient may present suffering from very severe clusters of seizures within a short period of time (e.g. 24–48 hours) followed by a long inter-ictal period of weeks or months. Levetiracetam may be given during these severe clusters to reduce the number and severity of the seizures. Following cessation of the seizures, the medication can be discontinued and restarted next time a severe cluster occurs. In this way, some of the high costs of the drug are avoided as well as reducing the possibility of tolerance. The drug can be used at a dose of 10–30 mg/kg po q8h for the duration of the cluster (usually 2–3 days) and then discontinued when the patient has been seizure-free for 24 hours.
Idiopathic epilepsy is less common in cats than in dogs. It is important to exclude some of the common metabolic causes for seizures in this species, including hepatic encephalopathy, renal encephalopathy, ionic imbalance, hypoglycaemia, polycythaemia, hypertensive encephalopathy and hyperthyroidism
In summary, phenobarbital remains a good first-line drug in the majority of patients. Potassium bromide is useful when phenobarbital alone does not control the seizures sufficiently or when hepatotoxicity is a problem. Levetiracetam is reserved for those patients where potassium bromide and phenobarbital are found to be inappropriate, either due to their side-effects or due to continued frequent and/or severe seizures. However, the owners of all patients should be provided with rectal diazepam regardless of the severity or frequency of the seizures. ■
Editor’s note: Readers are reminded to follow the cascade when considering use of medications not authorised for use in veterinary species.
14-18 How To.indd 18 20/10/2011 08:38

companion | 19
CPDCPD
NURSING REPTILES: KEEPING EVERYTHING TO SCALEExotic pets, and reptiles in particular, now make up a significant proportion of the practice caseload, and expectations of owners is often extremely high. However, whilst many will have excellent knowledge of the care that these animals need, not all owners of reptiles understand the complex housing and nutritional needs of their pets – as a result health problems can arise from poor husbandry. Also, it is unfortunate that a lot of these pets are bought on impulse with little planning for their living conditions. This day course will discuss these issues, as well as how to provide good nursing care for the sick reptile.
Details: Tuesday 2 October 2012, with Matthew Rendle in Blackpool, venue to be confirmed
Fees: BSAVA Nurse Member: £167.00 Non-member: £250.00
RABBIT NURSING… HOW TO DO IT RIGHTRabbits are being presented at veterinary practices more and more frequently, with owners willing to pay for and expecting the best of healthcare for their pets. Nurses are often at the forefront of this care and need to keep up to date on the latest thinking on rabbit nursing. Rabbits present different challenges in the care they require and often necessitate more in-depth care than dogs or cats. Topics to be covered will include: hospitalisation, nursing care plans, anaesthesia and analgesia, fluid therapy and nutritional support, and pre, peri and post operative care. There will also be case-led discussions.
Details: Wednesday 23 November 2011, with Richard Saunders and Claire King at Nottingham Belfry
Fees: £195.00
From 2012 BSAVA nurse members will begin to benefit from a discount on their CPD and will be able to consider taking their career forwards with
the BSAVA Nursing Merit Awards (more about the latter in a future issue of companion).
The Association has always sought to offer cost-effective courses to VNs and this move means stretched CPD budgets can go further, as well as have an option to really expand your skills. Here are the courses currently in the diary (dermatology and ophthalmology are also being planned, email [email protected] for more information).
Knowledge
BSAVA is expanding its CPD for nurses in order to offer more options to VNs and their practices
CARDIOLOGY FOR NURSES IN PRACTICEThis day course is targeted at nurses in first opinion or referral practice that are involved in nursing dogs and cats with heart disease. Topics will range from basic themes, such as understanding common cardiac diseases and heart failure, to more advanced themes, such as the nurse’s role in interventional cardiology. The meeting will be interactive and practically based, with tips on nursing patients with heart disease and diagnostic testing. An ECG and arrhythmia practical in the afternoon will allow small group training for those with no experience of ECG and those who wish to discuss challenging cases.
Details: Thursday 8 March 2012, with Simon Dennis and Charlotte Pace at Woodrow House, Gloucester
Fees: BSAVA Nurse Member: £167.00 Non-member: £250.00
for nurses
19 CE Nursing.indd 19 20/10/2011 08:38
20 | companion
Congress 11–15 April 2012
Nursing Master Series■■ A chance to cover a topic
in depth■■ Double lectures allow
plenty of time
Designed for veterinary nurses with more experience. These sessions may appeal to nurses working in specialist or referral practice, or with a particular interest in the topic.
Nursing Master SeriesA chance to cover a topic
Double lectures allow plenty of time
Designed for veterinary nurses with more experience. These sessions may appeal to nurses working in specialist or referral practice, or with a particular interest
How to pick your lecturesBSAVA Congress aims to cater for all, with a wide ranging scientific programme. How can you decide whether a particular scientific session will be at the right level for you? Here is a handy guide to indicate the level and format of the different sessions
Congress 11–15 April 2012
General lectures (Veterinary and Nursing)■■ Focus on common presentations■■ logical approaches to diagnosis
and management
ideal for new and recent graduates, those returning to work after a career break, those who don’t see small animals every day, or individuals who would like to refresh their knowledge on a topic.
Also useful for more experienced veterinary professionals who wish to learn about a subject new to them. Are there new technologies or procedures that you aren’t yet familiar with? Are there topics which weren’t considered when you were a student? A general lecture may provide the information you need.
Advanced lectures (Veterinary and Nursing)■■ Focus on improved decision
making■■ Dealing with difficult cases■■ Current controversies
Aimed at veterinary professionals who feel confident in their daily work, but who would like to improve their knowledge and skills, and make sure they remain up to date.
State of the Art lectures■■ Current concepts and ongoing
research in the field■■ up to date approaches to
diagnosis and treatment■■ Cutting-edge technologies
Aimed at all veterinary professionals interested in the “how”, “when” and “why” of the conditions they recognise and deal with.
Clinical research abstracts■■ Short presentations of current
clinical research■■ informal sessions with a small
audience■■ opportunity to ask questions
Clinical research abstracts are one of BSAVA Congress’s best kept secrets! ideal for those working in teaching and research, but also for experienced veterinary surgeons working in small animal practice.
The timetable of clinical research abstracts, with titles and speakers, will be available this year on the BSAVA website prior to Congress, to allow delegates to include these sessions in their planning.
20 | companion
Veterinary Masterclasses■■ An opportunity to explore a
subject in greater depth■■ Case-based discussion
ideal for more experienced veterinary surgeons. Baseline knowledge of the subject and familiarity with commonly used terms will be assumed – but delegates are not expected to have specialist knowledge. The small group format is relaxed and informal, and discussion is encouraged but is not enforced – you can just sit, listen and learn.
Each masterclass runs for 3 hours, and is restricted to a maximum of 40 delegates. To take part in a masterclass you need to purchase a ticket for that class in addition to registering for congress. Tickets for masterclasses may be purchased at Congress if spaces remain – but they have often sold out. To avoid disappointment therefore, we recommend that you purchase your masterclass ticket(s) at the same time as you register for Congress.
Avian ophthalmology: one of the 12 Veterinary Masterclasses on offer for World Congress 2012
lecture may provide the information you need.
20-22 Congress.indd 20 20/10/2011 08:37

11–15 April 2012 Congress
Interactive lectures (Veterinary and Nursing)■■ Case-based sessions with
interactive decision making■■ personal delegate keypads allow
anonymous voting
ideal for any veterinary surgeon or nurse working in small animal practice.
The speaker leads the audience through the presentation and work-up of a series of cases. The delegates become involved in the decision-making process for each case through their interactive voting keypads. The keypads, which are issued to each delegate as they enter the lecture hall, are simple to use – and completely anonymous. Questions are directed at the whole audience rather than at individuals, and only you know the decisions that you make. indeed there is no need to vote at all if you prefer just to think about your answers. The responses given by the audience are displayed graphically after each question, so you can see the spread of decisions. And the speaker can then explain why one or more of the options would be better than others. it really is the ideal way to practice clinical decision making without anyone knowing if you make a mistake!
interactive sessions can be very popular, so if you plan to attend one of these, make sure you arrive at the hall in good time.
Although the human–animal bond has existed for thousands of years, the formal study of Animal
Assisted Therapy (AAT) is a relatively new field. AAT is a therapy that involves animals as a form of treatment. The aim of AAT is to improve a patient’s social, emotional or cognitive functions, it can also be used for educational and motivational purposes. Companion animals commonly used for therapy include dogs, cats, horses, birds, rabbits, and other small animals.
Such animals make people feel safe and appreciated. They do not communicate with words and so patients afraid of approaching people can comfortably approach an animal. Also, a therapist with a companion animal is less intimidating and so an uncommunicative patient may be more willing to respond.
The contribution of companion animals in people’s lives is conducted using specialised intervention methods termed Animal Facilitated Activities. These interventions have taken place in different scientific fields including genetics, biology, developmental psychology, nursing and psychoanalysis. in medical and veterinary science, they are divided into two groups: animal assisted therapy; and animal assisted activities.
The involvement of veterinarians in these programmes from their inception is critical. They serve as: advocates for public health and welfare and for the health of animals participating in these programmes; experts in zoonotic disease transmission; experts about the wellbeing of the animals; and experts about the
FECAVA’s AAT SympoSium
kind, genetic profile, sex and age of the animals that participate. They can also provide answers to fundamental questions concerning animal husbandry and behaviour.
FECAVA recognizes that the human–animal bond is important to human and community health and has therefore organized a special Symposium with the title “Animal assisted facilities: companionship works its magic” during WSAVA/FECAVA/BSAVA Congress 2012.
Simon orr, FECAVA president, will give a brief introduction to the organisation’s policy about animal assisted facilities. The invited speakers are: Dr James Serpell, the director of the Center for the interaction of Animals and Society at the university of pennsylvania; Dr Elizabeth ormerod, the chair of the Society for Companion Animal Studies; and Dr Jane Fossey, a clinical psychologist and deputy chairman of the Society for Companion Animal Studies. ■
Trauma cases: one of the topics that will be discussed in the popular Interactive lectures
companion | 21
11–15 April 2012 Congress
20-22 Congress.indd 21 20/10/2011 08:37

22 | companion
Congress 11–15 April 2012
Congress has a reputation for offering four days of great fun, as well as the superb science. So how to top that
when you are hosting the WSAVA/FECAVA Congress? make it five days!
So whilst officially the dates have been advertised as 12–15 April 2012 – we are changing that from now on – because from Wednesday 11 April you can kick-start your Congress with a free Welcome Ceremony at 6.30pm and then move into the ticketed ‘Taste of Britain’ party at 7.30pm.
Free to allAnyone registered for Congress is encouraged to attend the World Congress opening Ceremony in Hall one on Wednesday. This will include the presentation of the prestigious WSAVA & FECAVA awards, and presidents of all participating organisations (Andrew Ash,
BSAVA; Jolle Kirpensteijn, WSAVA; Simon orr, FECAVA) will invite you to join them in launching the largest ever veterinary conference in Europe.
This event is also open to anyone attending any of the pre-Congress Affiliated Group meetings during the day on Wednesday, so let your friends in these specialists groups know they are welcome to join us.
Taste of BritainThe Welcome Ceremony will be followed by the best of British, as guests get to mingle at an informal evening of entertainment and tasty treats from across the uK. All four home countries will be represented in culinary form, with samples of the very best food and drink available from Scotland, England, Wales and Northern ireland. The musical treat of the evening comes in the form of 20 young men from South Wales.
only men Aloud have enjoyed a rollercoaster ride after winning the BBC show Last Choir Standing. They secured a five-album deal with universal, with their first selling over a quarter of a million copies, and they have collaborated with Josh Groban, russell Watson, Bonnie Tyler and Katherine Jenkins.
The choir creates a huge wall of sound and their repertoire is an eclectic mix, ranging from the 15th century to modern pop, proving that choirs can be fresh and funky. Their set can include traditional
Welsh hymns, such as Guide Me O Thou Great Jehovah and comedic folk songs like What Do You Do With A Drunken Sailor?, to pop anthems, like robbie Williams’ Angels.
Their sound is deeply rooted in the traditions of male voice choirs, yet they manage to make the traditional very current with their slick performances. This is not a choir that simply stands in militaristic rows to belt out standards – they make clever musical choices and put on a show.
And much more…Joining only men Aloud as part of Wednesday evening’s entertainment is a band that won’t have far to come – the Hot Jazz Biscuits hail from the North West midlands and have earned themselves a great reputation for enthusiastic and uplifting covers of a wide variety of musical styles, including jazz, motown, soul, disco and pop.
This is going to be a really lovely evening of fun, fabulous food, great entertainment and the chance to catch up with old friends and make new ones – potentially from all corners of the globe too. So join us to celebrate a ‘Taste of Britain’ in the international atmosphere of the World Congress Welcome Evening. Tickets cost just £20 for the whole evening, including food, and can be bought alongside your registration, or separately. Visit www.bsava.com/congress or email [email protected] for more information. ■
To welcome the world to Birmingham there will be a free Welcome Ceremony and a brilliant British-themed event on the Wednesday of Congress
Congress 11–15 April 2012
Come a day early formore social fun
20-22 Congress.indd 22 20/10/2011 08:37
PETSAVERS
companion | 23
Improving the health of the nation’s pets
PETSAVERS CHRISTMAS CARDSPetsavers Christmas cards are available for just £3 for a pack of ten, including postage and VAT. Order forms are available from the BSAVA on request, or the cards can be purchased online at www.petsavers.org.uk. If you work in practice and would like to make these available to your clients, we can send order forms to you to display in your reception. ■
Products that pay for PetsaversThe Petsavers range of products is designed to meet the needs of small animal practices – and raise funds for the charity at the same time. By choosing these products, you will know that all the profit goes directly to support the important research into the illnesses that affect our nation’s pets
Heated padsPetsavers heated pads are designed to keep small pets warm in hospital and are also effective in minimising perioperative hypothermia. The pads are cheaper than an incubator and are less hassle than hot water bottles. They are easy to clean and run on a low voltage so that they can be left on constantly. A plug-in lead means the pad can be easily passed through the bars of a cage.
To see the complete range of Petsavers products please visit our online shop at www.petsavers.org.uk. Alternatively, to order over the phone, please call 01452 726700. ■
Protective collarsPetsavers protective collars are easy to assemble and can be attached to regular collars. The protective collars come in packs of ten and are available in a range of sizes, starting at 7.5cm through to 40cm.
Recovery blanketsPetsavers recovery blankets are made of metalised polyester, which means that they are tough and also retain 95% of radiated body heat. The blankets are ideal for preventing hypothermia in the perianaesthetic period and are also radiolucent, which means that diagnostic radiographs can be taken while the animal remains in the blanket. They are especially useful for trauma patients or hypothermic cases. The blankets are 2.14m x 1.42m and can be cut to fit smaller animals.
Pet carriersPetsavers wire carriers are suitable for cats and small dogs. The hinged lid allows full access to the interior of the carrier, so it’s easy to get pets in and out. Petsavers also have inexpensive cardboard carriers that are very popular with clients and easy to store.
At the recent Scottish Congress Banquet a fantastic £969.10 was raised for Petsavers. Thank you to everyone who donated; your generous support is greatly appreciated by the charity. This money will go towards funding much needed clinical research projects which aim to improve the health of our pets by providing vets with a better understanding of the illnesses that affect animals. ■
money will go towards funding much
which aim to improve the health of our
SCOTTISH CONGRESS CHARITY SUCCESS
PETSAVERS CHRISTMAS CARDSPetsavers Christmas cards are available for just £3 for a pack of ten, including postage and VAT. Order forms are available from the BSAVA on request, or the cards can be purchased online at www.petsavers.org.ukIf you work in practice and would like to make these available to your clients, we can send order forms to you to display in your reception.
23 Petsavers.indd 23 20/10/2011 08:37
24 | companion
PET BEREAVEMENT
Those times when you get to see the happiness your work brings to the people around you are the moments you are glad that you chose your
profession. Working in a veterinary practice often gives you the opportunity to experience people’s joy when you have been instrumental in making their beloved pet well again.
However, the more challenging aspects of your week are likely to include the times when you are facing clients who are contemplating or experiencing the loss of their beloved pet. Grief and bereavement is something that, as a veterinary professional, you probably come across more often than most. It’s something that is rarely part of your training and yet something that forms so much of your professional life.
A bond-centred approachDeveloping a ‘bond-centred practice’ can help to provide a much better support strategy for your clients, your colleagues and yourself. It also makes good business sense as it can help clients to have a clearer understanding of what is going on, to follow medical instructions more accurately and to feel prepared to own another animal again after the loss of their pets. So it helps to maintain customer loyalty and retention.
So how do we adopt a more bond-centred approach to veterinary practice?
First, let us consider the human–companion animal bond: the connection that we humans have with our pets and the reciprocal connection they have with us. Acknowledging the significance of that bond for your clients and their pets is an important step.
How many of your clients (and colleagues, friends, family) call their pets their ‘babies’? It is often quite a few. This is because the human–companion animal bond is a relationship based on attachment and this is most often seen between parent and child. No matter how long the relationship with the pet, it can offer comfort and safety, provoke pleasure upon reunion and anxiety upon separation.
Most of us have seen a client so anxious about leaving their pet with the vet for treatment or surgery that they have made themselves ill, or so stressed that it affected everyone else around them, including their pet and the practice staff.
You might even recall a client who was so concerned for the health and well-being of their animal that they actually hindered its health and well-being? Perhaps they felt they knew better than you what medication to give their pet, and when they should give it, or not give it. Perhaps they felt they knew better than you what they should be feeding their pet and how much and how often. All with the best intentions but with often detrimental effect.
Non-judgemental approachUnderstanding why a person’s bond with their pet may be intensified by their environment or circumstances can help us to be non-judgemental when their behaviour challenges our professional and personal opinion.
For example: Has the client who gets so anxious about leaving her pet with you been living on her own with her animal companion since her husband passed away? That pet may now be the only regular company she has and without it, your client thinks she will be entirely alone in the world. She may not feel it possible to have another pet after this one, as she thinks it wouldn’t be fair as her recent loss is making her only too aware of her own mortality.
Taking time to get to know a little about your clients’ backgrounds and situations can help
Julia Dando, Training Manager for the Society for Companion Animal Studies which looks after the Pet Bereavement Support Service with The Blue Cross, looks at how both the profession and pet owners manage grief
Pet loss support in veterinary practice
24-25 Pet bereavement.indd 24 20/10/2011 08:36
companion | 25
tremendously in providing understanding, compassion and support. Be empathetic – put yourself in their position and think to yourself: “If I were them right now – what would I need from me?”
Active listeningAlso, you and your colleagues can learn active listening skills. This doesn’t just mean listening attentively; there are specific ways that we can offer emotional support to another. These are skills that can help when we enter the realm of “what can I say?”. Reflecting, restating, paraphrasing and summarising are all examples.
Asking ‘open’ questions that allow the person to tell you about their pet are useful, rather than ‘closed’ questions that only require a “yes” or “no”.
Whilst you are dealing with this on a regular basis, this event can be significant, emotional, and sometimes traumatic for the client, so take care not to fall into autopilot and use ‘standard responses’. Don’t be afraid of silence: sometimes you don’t need to say anything; sometimes you just need to listen.
Developing protocolsThink about developing the pet loss support protocols at your practice. For example, booking euthanasias at the end of the day in a longer time slot so the client will not be rushed, providing an exit that does not require walking through the waiting room, ensuring there are tissues available (the blue stuff on the big roll doesn’t count), providing pre-euthanasia consultations, giving the client the option to stay with their pet during euthanasia, sending sympathy cards, providing information sheets and referring people to the Pet Bereavement Support Service or other appropriate services.
You tooThis is very important: don’t forget to look after yourself. It isn’t something our profession is always that good at. Remember, you are not expected to become a counsellor – that is something very different, but you can offer emotional support, as can anyone. Recognise when it is time to refer your client on to another professional (such as a GP or qualified counsellor). ■
THERE IS HELPThe Pet Bereavement Support Service has been providing a free helpline since 1994 when it was launched at BSAVA Congress. It is now run jointly by the Society for Companion Animal Studies and the Blue Cross. It is not only available for your clients; when you have had a rough week dealing with pet loss, there is always someone there to listen to you too.
The Society for Companion Animal Studies offers a distance learning course specifically for those in veterinary practice. Covering many aspects of pet loss support, the course looks at:
■ Reflecting upon personal and professional experience ■ The human–companion animal bond (HCAB) and its relevance to
veterinary practice ■ The most frequently applied models of grief used to understand
reactions to pet loss, highlighting how these can be applied to practice ■ The special needs and considerations arising from euthanasia-
related grief ■ Core active listening skills and other practical strategies for supporting
clients through crisis and grief ■ How life stage and age may impact on experiences of pet loss,
highlighting considerations for providing emotional support ■ How pets and horses may grieve for lost companions and highlighting
supportive strategies ■ Options for after-death body care and ways of remembering pets ■ Developing pet loss support protocols for veterinary practice to
ensure good standards of client care.
This course can be booked directly through the SCAS website: www.scas.org.uk. BSAVA members qualify for a special discounted rate.
COPING WITH LOSS LEAFLETPetsavers has an excellent leaflet called Coping with the loss of your pet which you can make available to your clients. You can find out more online at www.petsavers.org.uk or email [email protected] or call 01452 726723.
...don’t be afraid of silence: sometimes you don’t need to say anything; sometimes you just need to listen...
24-25 Pet bereavement.indd 25 20/10/2011 08:36

26 | companion
BLOOD
If you are the owner of a dog with a DEA 1.1-negative blood type, then Wendy Barnett would like to hear from you. She is head of clinical services at the Pet
Blood Bank, the charity set up to provide blood for use by veterinary practices around the country.
DEA 1.1-negative dogs are the universal donors, in demand because their blood will not result in an adverse reaction when infused into another whose own red blood cells are positive for that particular antigen. It isn’t safe the other way round, and if a DEA 1.1-negative patient already primed with antibodies to the positive cells from an earlier transfusion is then given a second dose, the results are likely to be fatal.
So if all patients, both positive and negative for this key antigen are given the DEA 1.1-negative blood then there isn’t a problem, surely? Yes there is, says Wendy, because only 30 per cent of domestic dogs are negative and they cannot be expected to bear the burden of supplying the rest of the population with blood.
Blood typingThis is why practitioners are being urged to use one or other of the two widely available DEA 1.1 tests to identify positive dogs which can be given the more widely available blood type. This would save the more limited supplies of DEA 1.1-negative blood for those dogs that need blood of that same antigen type.
“Typing would take the pressure off us, as we could make better use of the positive blood. At the moment we have to ask their owners not to donate because if they gave more regularly – three or four times a year is feasible – we couldn’t fully utilise it,”
Wendy explains. While serum can be stored in a freezer for up to a year, whole blood has a limited shelf life of about six weeks. “It is a quite a see-saw, trying to balance the supplies of the available blood types. It costs us money to collect and store blood, so we don’t want to throw any away.”
Any patient needing exogenous blood is likely to be a genuine emergency and part of the reason why fewer practitioners than Wendy would like are testing their patient’s blood is that there are probably many other pressing issues on their minds. But the two tests available in Britain only take a few seconds to perform. They are an agglutination assay marketed in the UK by the Woodley Equipment and a newer monoclonal antibody-based test produced by the French company Alvedia.
These tests cost around £20 and the DEA 1.1-negative blood is sold at a premium of about £40 for a standard 450 ml unit. So blood typing can save the patient’s owners a few pounds, probably a small amount compared with the overall cost of a lengthy and complex course of treatment, but one still worth having.
Some small practices may question the need to buy a test that they are unlikely to use very often and has a finite shelf life. But there is no need to throw the product away; Wendy points out that it can be used to blood type a dog owned by a staff member or a sympathetic client which could then be used as a donor in any future emergency.
Improving standardsThere is another very good reason why practitioners should be using blood typing tests on their canine patients, as Dave McComas, Biomedical Technical Manager for Woodley Equipment explains. While using DEA 1.1-negative blood in a positive dog may not cause a life-threatening reaction, it is not an ideal combination. The half-life of the donated red cells is dramatically reduced, he says.
Until 5 years ago, Dave was working as a biomedical scientist in the National Blood Transfusion Service. “I was shocked to see how transfusions were handled in the veterinary industry compared with the way we did things in the NHS. In Britain, we are also a long way behind the way that US veterinary surgeons carry out these procedures.”
There are rapid tests available to ensure that canine emergencies do not experience catastrophic immune reactions after receiving donated blood. So why are practitioners so reluctant to use them?
Blood typing: positive and negative
26-27 Pet Blood Bank.indd 26 20/10/2011 08:32
companion | 27
BLOOD
Blood typing is actually the minimum that pet owners should expect for their animals. He insists that veterinary practices should also be carrying out cross-matching tests – mixing a small amount of donated blood with serum from the intended recipient. The blood typing test identifies the antigens carried on red blood cells but a further test is needed to show antibodies which could cause rare but potentially damaging responses to blood of the same DEA 1.1 tissue type.
McComas feels that veterinary practices have become complacent about their canine patients because they do not show the immediate and potentially lethal reactions seen in a human or a cat given the wrong blood type. “With dogs there is a feeling that it doesn’t matter as there won’t be a problem with the first transfusion. But the chances are that it may need another, and so why take the risk when with a test costing a few quid you can accurately blood type the patient?”
Reducing the numbers of dogs receiving the ‘wrong blood’ is only one way to ensure that there are plentiful supplies of each blood type, where and whenever they are needed. Pet owners could be encouraged to sign up their animals with the Animal Blood Register set up by the large referral practice Davies Veterinary Specialists (DVS), both a major user of donated blood and one of those sites around the country where regular donor sessions are held to provide the material needed by the charity.
Cats and dogsNat Whitley, a small animal medicine specialist and a director at DVS, points out that the register recruits both cat and dog owners around the country who will offer their pets’ services to a nearby practice in an emergency situation. For many reasons, maintaining a core of volunteer cat owners is a bigger issue. Not only is blood typing essential for safe transfusions in cats, there are a number of other practical problems. Cats have to be sedated before a procedure, the amount of blood that can be safely harvested is small (only about 60 ml) and the cat may need intravenous fluid therapy to support it after a donation.
Additionally, some cats cannot be bled as readily
as dogs and the volumes obtained are unpredictable so that the blood cannot be mixed with a standard amount of preservative in a pre-prepared bag. Traditionally, donor cats are bled using multiple fillings of syringes. The contents are then mixed together, and maintaining adequately sterile conditions can be a challenge, he says.
Indeed, the outlook for those performing feline blood transfusions has actually deteriorated over the past couple of years. In 1999 the US biotechnology company Biopure launched Oxyglobin, a semi-synthetic blood substitute made from processed bovine blood for use by veterinarians. But in 2009 the company filed for bankruptcy, dragged down by the costs involved in developing a safe product for human use. Although the veterinary product had a long shelf life, the last stocks have now been used and there is no sign of a new company entering the market in the near future, Nat explains.
Making the best of itWith no technological fix on the horizon, the Pet Blood Bank, the Animal Blood Register and the broader veterinary profession will have to rely on the goodwill and public spiritedness of the nation’s pet owners to ensure that supplies of this life-saving fluid will keep flowing.
On the canine side, Wendy, Nat and their colleagues would be particularly keen to recruit owners of those large breeds that have been shown to have a higher than normal prevalence of the valuable DEA 1.1-negative blood type. These include Airedales, Dobermanns, German Shepherds and especially Greyhounds in which about 75% of individuals carry the necessary gene.
For the profession to reap the benefits of a successful donor service, it must also show this same benevolence in helping its own members. Wendy hopes that the readiness shown by many of the more regular users of the blood service to assist their colleagues will continue to grow. There have been many occasions when practices holding stocks of blood have let their neighbouring practices use some in an emergency. This very much reflects the spirit in which the charity was first established, she says. ■
26-27 Pet Blood Bank.indd 27 20/10/2011 08:32

28 | companion
From 12–23 September 2011, I was privileged to be able to deliver the WSAVA Continuing Education
programme in China, thanks to the kind sponsorship of Hill’s, Bayer Animal Health and MSD Animal Health. The subject of my lectures in China was interpretation of haematological data and evaluation of the blood smear, and these topics were very well received by each audience.
The visit began in Beijing, where I represented the WSAVA at the official opening ceremony then delivered a full-day stream at the 7th Congress of the Beijing Small Animal Veterinary Association (BJSAVA). The BJSAVA and this congress have grown rapidly and
there were approaching 2,000 delegates at the congress, participating in parallel lecture streams, a large exhibition and congress banquet.
In Shanghai the lectures in the Shanghai Science Institute were attended by around 150 veterinarians.
The lectures in Guangzhou were held at the campus of the South China Agricultural University, where some 200 veterinarians listened attentively despite the 35°C heat and very high humidity. Some of this audience had travelled long distances from remote cities and there was a particularly active question and answer session at this seminar.
My Chinese hosts were incredibly hospitable and the arrangements in each location were flawless. In Beijing and Shanghai I was fortunate to have some time to visit some amazing historical and cultural highlights, accompanied by young English-speaking vets Sarah (Beijing) and Vivian (Shanghai). My thanks go to my hosts: Dr Louis Liu (President BJSAVA),
CE in China
Professor Michael Day reports on a fascinating lecture tour
Dr Geoffrey Chen (President Shanghai Small Animal Veterinary Association) and Professor Huijun Xiong (South China Agricultural University). I would like particularly to acknowledge the unsurpassed efforts of Dr Shu Dai (Hill’s Pet Nutrition Asia-Pacific) who acted as my translator for each of the three presentations, having previously translated my written notes and powerpoint slides.
From Guangzhou, I travelled by train to Hong Kong to speak on immune-mediated cytopenias to an audience of 60 veterinarians from the Hong Kong Veterinary Association (HKVA) at an evening seminar. In Hong Kong, I was looked after superbly by Drs Tint Naing and Tom Mangan (NKVA) and by Dr Veronica Leong (WSAVA Executive Board), with special thanks to Dr Olivia Chan for my guided tour of local landmarks.
It was an honour to represent the WSAVA at these events and to have the opportunity to visit a fascinating country at a time of rapid change and development. ■
28-29 WSAVA News.indd 28 20/10/2011 08:31

companion | 29
WSAVA NEWS
The WSAVA presented its annual Awards and its inaugural One Health Award at the World Congress in Jeju,
Korea, in October. Highly regarded in global companion animal care, the WSAVA Awards recognise ground-breaking research and achievement in the clinical care of companion animals. This year’s winners are as follows:
WSAVA International Award for Service to the ProfessionThis award is made to a vet judged to have made an outstanding contribution to the fostering and exchange of scientific and professional ideas throughout the world. It has been given to Boyd Jones, Professor of Companion Animal Medicine at Massey University in New Zealand.
American College of Veterinary Internal Medicine, is President of the American College of Veterinary Internal Medicine in Oncology. He is also chair of the Children’s Oncology Groups Bone Biology Subcommittee and a founding member of the Canine Comparative Oncology and Genomics Consortium.
WSAVA International Award for Scientific AchievementThis award, which recognises the work of a vet in advancing the profession’s knowledge of companion animal disorders, has been made to Dr Stephen Withrow, Founder and Associate Director of the Animal Care Centre (ACC) at Colorado State University. The ACC’s mission is to improve the prevention, diagnosis and treatment of cancer in companion animals and translates its research and knowledge to benefit people with cancer.
Dr Withrow’s pioneering work in cancer treatment for animals was judged an outstanding achievement, which will advance the profession’s understanding of the disease as it affects companion animals.
WSAVA Hill’s Pet Mobility AwardThis award, recognising the outstanding work of a clinical researcher in the field of canine and feline orthopaedics, has been made to Professor Steven Budsberg, Director of Clinical Research at the College of Veterinary Medicine at the University of Georgia. Professor Budsberg has been widely published in his areas of particular interest, which include canine gait analysis, non-steroidal anti-inflammatory drugs and evidence-based medicine applications in orthopaedics.
Commenting on the 2011 WSAVA Awards, Jolle Kirpensteijn, said: “It is thanks to the pioneering work of individuals and organisations such as those we are recognising this year that the profession as a whole continues to move forward. We are again grateful to Dr John Holt and his wife Mary for sponsoring our award for Service to the Profession.” Dr Holt is a long-term supporter of the WSAVA, a Past President (1986–88) and past Service to the Profession Award winner (1998). ■
And the winners are...The WSAVA awards recognise outstanding contributions to the clinical care of companion animals – we congratulate the 2011 recipients
Professor Jones has made a particular contribution to global veterinary development and learning, speaking regularly at events around the world. He is also an editorial board member, a referee for a range of clinical journals and an examiner for degrees and specialist college qualifications. He has published 170 refereed papers and book chapters in areas including working dogs and veterinary education.
Rau Benavente was the owner and Director of the Veterinary Clinic Javier Prado in Lima, Peru. In his numerous roles as a lecturer and speaker and representative on many veterinary bodies, he played a vital role in the development of the profession throughout Latin America.
WSAVA Global One Health AwardThis new award has been created to recognise the outstanding contribution made by an individual or an organisation in promoting the One Health concept globally. The OIE (World Organisation for Animal Health) is the recipient of the inaugural award in recognition of its efforts to promote One Health and, in particular, for its acknowledgement of the importance of including small animals in the One Health programme.
WSAVA Hill’s Excellence in Veterinary Healthcare AwardThis award, which recognises outstanding work in promoting companion animal health care, has been made to Dr Chand Khanna, Head of the Pediatric Oncology Branch’s Tumor and Metastasis Biology Section and Director of the Center for Cancer Research, Comparative Oncology Program at the National Cancer Institute of the USA.
Dr Khanna, a Diplomate of the
Further news from the WSAVA World Congress in Jeju, Korea, will follow in the next issue of companion.
WSAVA President’s AwardThis award is made periodically by the President of the WSAVA to a member judged to have made an outstanding contribution to the association. This year the award has been made posthumously to Rau Benavente, who died in August 2010.
28-29 WSAVA News.indd 29 20/10/2011 08:31

30 | companion
THE companion INTERVIEW
Nathalie Wissink-Argilaga was born in Apeldoorn in The Netherlands, but grew up and went to school in Rosas in Spain. Her mother is an estate agent and her father is a businessman. Nathalie graduated from the Universitat Autonoma de Barcelona in 2004. After working in several exotic practices and zoos around the world, she completed a one-year Small Animal internship at Davies Veterinary Specialists. Nathalie started work at The Scott Veterinary Clinic in May 2006. In 2008 she passed her GP certificate in Exotic Animal Practice. Her special interest is in exotic pets, particularly birds and reptiles, and she holds the RCVS certificate in Zoological Medicine.
Nathalie Wissink-Argilaga
THE companion INTERVIEW
Nathalie Wissink-ArgilagaLic.Vet CertAVP (ZooMed) MRCVS
QWhat made you want to be a vet?
AI have wanted to be a vet for as long as I can remember but it suddenly became very real when my horse had to be referred to the vet
school. I have always been surrounded by animals from a very early age. I became very involved in equestrian sports as a child and unfortunately my horse developed colic and had to be referred. It was an extremely difficult time to see him so poorly. The work of the vets and techs was amazing and he fully recovered. This made me realize that I wanted to spend the rest of my life helping people and their pets get through these difficult times.
Has the job lived up to what you hoped it would be?The job has definitely lived up to all my expectations, and more. I really enjoy my job and find that being an exotic animal vet is extremely rewarding because I feel that I help the more unusual pet species get the care they deserve. It also makes it extremely varied as on a normal working day I can see so many different species: from an axolotl to a skunk or a bird of prey.
How did you decide to take the veterinary career path you chose?I became involved in a student association for wildlife and exotic veterinary medicine in my first year at university. I soon realized that there was still a lot of work to do in that area and that it seemed to be
30-31 Interview.indd 30 20/10/2011 08:30

companion | 31
THE companion INTERVIEW
...on a normal working day I can see so many different species: from
an axolotl to a skunk or a bird of prey...
THE companion INTERVIEW
forgotten in the curriculum. It made me realise that I really wanted to help all of these ignored species.
What do you consider your greatest achievement career wise?Passing my RCVS Certificate in Zoological Medicine.
What are the highs and lows of practice life for you?The highs are all the difficult and challenging cases that we resolve successfully, as well as all the times we help to improve the quality of life of the more unusual patients. The lows are the loss of some patients despite all our best efforts and, in my line of work, especially the cases that could have been prevented with better husbandry and care.
What makes you unhappy?Rain.
What single thing would improve the quality of your life?Having a bit more sunshine in the UK.
What is your guiltiest pleasure?Chocolate, no doubt.
What do you owe your parents?Apart from large amounts of money, I owe my mum everything. She has always been there for me, supporting me and believing in me, no matter what crazy idea got into my mind. She also provided me with the opportunity to travel and see practice all over the world, which really helped me to develop my career in exotic animal medicine. Without her all my dreams would not have come true.
Who has been the biggest influence on your career?My good friend and great vet David Sanchez Migallon-Guzman. He really encouraged me to pursue my career in exotic animal medicine and taught me that nothing was impossible as long as you worked hard enough for it.
What or who is the greatest love of your life?My husband and my two cats, Mr Fish and Mr Chips.
Which words or phrases do you most overuse?‘Awesome’ and ‘cool’.
Is there a song that will always get you on the dance floor?Hips Don’t Lie by Shakira. There is nothing like a bit of booty shakin’ to relieve stress! ■
INTERVIEW WHO?The companion Interview profiles people in our profession of influence and interest. If there is someone you’d like to see feature on this page then let us know. Email [email protected] or call Kay Pringle on 01452 726718.
...on a normal working day I can see so many different species: from
an axolotl to a skunk or a bird of prey...
THE companioncompanion INTERVIEW
30-31 Interview.indd 31 20/10/2011 08:31

32 | companion
BVA CONGRESS
This year’s BVA meeting seemed to attract a larger and noticeably younger audience than is usual for
what has become known as the main forum for political debate for veterinary professionals. They came, in part, to benefit from the quality companion animal CPD sessions, provided by the BSAVA, as an alternative attraction for those wanting a more balanced diet of science and politics.
Truly interactiveAnother key difference between the meeting and a conventional CPD event was interactive sessions at the end of both days, when the audience had an opportunity to interrogate the experts about their likely approach to managing an unusual case.
The idea, according to Ian Ramsay from the Glasgow Veterinary School who devised the CPD programme, is that the quiz is not just a little light relief at the end of the day. Those sessions are also intended to help embed the information acquired earlier in the minds of the attending practitioners, so that they will be able to apply the newly absorbed information in their next consult session.
Top speakersThe speakers, all highly respected figures in their chosen disciplines, drew from their experience to devise a particularly challenging scenario. In one case described by Liverpool University lecturer Alex German, the story illustrated the importance of asking the key questions at the beginning of a diagnostic work-up.
He outlined the case of dog that was referred with diarrhoea and progressive weight loss and which had already been examined by several colleagues. The clinical and laboratory findings gave no explanation for the dog’s deteriorating condition until Alex went back to the
beginning and asked the owner to describe in detail how they were feeding the animal.
It turned out that they were sticking rigidly to the instructions in the table given by the first practitioner to have seen the animal on how much food a dog should receive for its bodyweight. As the animal’s condition deteriorated it was being given progressively smaller rations by the well-meaning but slightly misguided owners, and this could not sustain a dog of its size. Once the animal started to receive sufficient nutrition it immediately started to regain condition and showed no signs of the gastrointestinal problems which were the initial reason why the owners had sought veterinary help.
Good reviewsWhat did those involved think of the format of the day and the quality of the CPD provided at the meeting?
“I thought it was excellent – all three Saturday speakers on liver, pancreas and GI were highly respected in their fields and good speakers. The lectures were pitched at a general practitioner standard, with glimpses of reasoning from a referral perspective on each topic,” said Stephen Barabas, a BVA Council member who had used the occasion to brush up on his clinical knowledge.
“I think that previously people have been put off as they interpret BVA Congress as a purely political meeting, whereas with the clinical lecture streams now it is a very diverse meeting with a lot of interesting topics covered on a local, UK, regional and International level, as well as providing high quality CPD.”
So did the organisers get the response that they had hoped for from the audience? “ Definitely,” says soft tissue surgery specialist John Williams, who gave a presentation on surgical treatment of liver and gall bladder conditions and who devised one of the challenging cases scenarios. “We were pleased with the attendance in the lecture hall, which was generally half to two thirds full. Even so it was still quite an intimate setting and people were perhaps less reluctant to voice their opinions than they might have been in one of the larger halls with hundreds of people at the main BSAVA Congress.”
As the Chairman of BSAVA’s Congress Committee, John is keen to explore different approaches for the Association to provide CPD. “I’d guess that the nearest we get to this sort of interactive approach at BSAVA Congress is those sessions where members get to vote on the various possibilities in a clinical situation using a push button key pad. That is another good way of getting people to think about the clinical options and we have now invested in this technology so that we can use the same format at our regional meetings.” ■
CPD challengeat BVA Congress
John Bonner reports on the BSAVA sessions held at BVA’s London Congress 23–24 September
DOWNLOAD ALL BVA CONGRESS LECTURES ANYTIMEThe Congress podcasts are one of the most popular BSAVA member benefits – and so we arranged to have all the BVA talks recorded and have added these to your MP3 library available online at www.bsava.com (go to Congress – Scientific – Podcasts). You must be registered with the website and logged in to access any exclusive online material, so if you have yet to do so email [email protected] to get your login details.
32 BVA Report.indd 32 20/10/2011 08:30
companion | 33
REGIONS
MeetYourRegionSurrey & SussexAs part of a continuing series, this month companion features BSAVA Surrey & Sussex Committee
BSAVA Surrey & Sussex Committee Members
■■ Olive O’Leary MVB MRCVS – Chair
Olive graduated from University College Dublin in 2003 and has spent most of her working life in small animal practice in West Sussex. Olive joined BSAVA three years ago and has enjoyed every minute. “It has been a very interesting and informative three years. I have
benefited from great CPD, made new friends and acquired many new skills. It is also great to be involved in a charitable organisation and to promote veterinary education both at home and abroad.”
■■ Louise Smith BVSc CertSAM MRCVS – Treasurer
Louise graduated from Bristol in 2006 and initially worked in mixed practice in Horsham. She recently moved to another first opinion practice in Guildford and gained the RCVS Certificate in Small Animal Medicine. In her spare time Louise enjoys long pub walks and agility with her dog Fizz.
■■ Muna Roberts BVetMed DipAS(CABC) MRCVS – Secretary
Muna qualified in 1991 from the RVC and has worked in small animal practice since then, obtaining her Diploma in Companion Animal Behaviour Counselling from Southampton University in 2005. She is currently in a sole-charge practice in Godalming, where she is studying for her certificate in Small Animal Medicine (feline).
■■ Alissa Cooper BSc BVetMed MRCVS – Petsavers Rep
Alissa graduated from the RVC in 2002 after her first a degree in Animal Science from Cornell University in America. After 18 months in equine practice, she entered small animal practice in Surrey. She is currently taking time off to spend with her two young children. She enjoys being a BSAVA committee member and is hoping to return to practice in the future.
Other Committee Members
■■ Wolfgang Dohne DrMedVet MRCVS
Wolfgang studied veterinary medicine in Hanover and Oslo before starting to working in the UK. In 1999 he established the Virginia Water Veterinary Clinic. In 1996 he joined the regional BSAVA committee and he became a member of BSAVA’s International Affairs Committee in 2007. Two years later he was appointed FECAVA director for BSAVA.
■■ Gerry Polton MA VetMB MSc(Clin Onc) DipECVIM(Onc) MRCVS
Gerry has been a volunteer for BSAVA since 2006. Before joining the Surrey and Sussex Region he acted as Chair for the East Anglia Region; he also volunteers for the Journals Management Committee, with current responsibility for commissioning interesting reviews for JSAP. Gerry is an oncology specialist working for North Downs Specialist Referrals in Bletchingley, Surrey.
■■ Julian Hoad BSc (Hons) BVetMed MRCVS
Julian qualified from the RVC in 1996 and after gaining experience in mixed practice in Kent made the move to small animal practice. He is now a partner at Crossways Veterinary Group in Storrington, West Sussex. He joined Surrey and Sussex in 1998, and served on the BSAVA education committee for four years. When not working in the practice, Julian likes to do extra work such as nurse lecturing or ultrasound training. “I first joined the committee so that I could have a say in what CPD was provided. I never thought I’d still be doing it all these years on – and still loving it.”
MEETINGSAn essential date for your diary in 2012: Wednesday 22 February, when Adrian Boswood will present Emergency Management of Canine and Feline Cardiac Arrhythmias in First Opinion Practice, at Leatherhead Golf Club, Kingston Road, Surrey. Visit www.bsava.com for further information on 2012 courses. If you’d like to receive email updates on upcoming events, submit suggestions for upcoming CPD, offer comments on the service, or even volunteer for the region, please email [email protected].
The Surrey & Sussex Committee is made up of both recent and
established volunteers, which makes for an interesting mix. We are always interested in recruiting new committee members and getting feedback (constructive criticism only!) from our members. Special thanks to Jo and Jackie who helped run the region for many years and to Janine who has only recently left to return to South Africa. Anyone interested in helping out can contact us at surreyandsussexregion @bsava.com. We are particularly keen to hear from our East Sussex members and any nurses interested in joining our committee.
33 Meet Your Region.indd 33 20/10/2011 08:29

34 | companion
CpD diary
evening Meeting – Surrey anD SuSSeX region
Wednesday 9 novemberrepairing the damage: old and new tricks of reconstructive surgerySpeaker: Pierre BarreauLeatherhead Golf Club, Kingston Road, Surrey KT22 0EEDetails from [email protected]
evening Meeting – South WeSt region
Monday 14 novemberorthopaedics: decision making in cat pelvic traumaSpeaker: Michael HamiltonLyngford House Conference Centre, Selworthy Road, Priorswood, Taunton TA2 8HDDetails from [email protected]
Day Meeting – north WeSt region
Sunday 20 novemberanaesthesiaSpeaker: Derek FlahertySwallow Hotel, PrestonDetails from [email protected]
evening Meeting – MiDlanD region
Wednesday 16 novemberpractical reading of chest radiographs (interactive)Speaker: Richard EwersYew Lodge Hotel, 33 Packington Hill, Kegworth, Derby DE74 2DFDetails from [email protected]
evening Meeting – South WaleS region
Wednesday 23 novemberhips without hops: management of pelvic fracturesSpeaker: Bill OxleyThe International Legacy Hotel (formerly the Quality Hotel), Cardiff CF15 7LDDetails from [email protected]
evening Meeting – SCottiSh region
thursday 24 novembereCgsSpeaker: Dr Paul WottonGlasgow University Vet SchoolDetails from [email protected]
evening Meeting – Southern region
Wednesday 23 novemberurogenital surgerySpeaker: Tony RyanBournemouth Marriott Hotel, Bournemouth BH2 5DUDetails from [email protected]
WeeKenD Meeting – eaSt anglia region
Saturday 12 and Sunday 13 novemberDentistry: theory and practical (with the BvDa)Speakers: Lisa Milella, Gerhard Putter and Annalize IdeAnimal Health Trust, Newmarket, Suffolk CB8 7UUDetails from [email protected]
Day Meeting – north eaSt region
Sunday 13 novemberi’d like to try this technique but… a step-by-step guide to practical medical and emergency techniquesSpeakers: Nick Bexfield and Karen HummThe Bridge, Walshford, Wetherby, North Yorkshire LS22 5HSDetails from [email protected]
evening Meeting – Kent region
Wednesday 9 novemberneurological examination in the cat: should you really bother?Speaker: Laurent GarosiBest Western Russell Hotel, 136 Boxley Road, Maidstone ME14 2AEDetails from [email protected]
Day Meeting
tuesday 15 novemberthe challenges of old age: optimising veterinary care of the geriatric catSpeakers: Angie Hibbert and Jo MurrellKettering Park Hotel & Spa, NorthantsDetails from [email protected]
Day Meeting
tuesday 22 novemberMedical neurology of the dog and cat: how to make sense of the wobbly, weak or collapsing patientSpeaker: Jacques PenderisBSAVA Headquarters, GloucesterDetails from [email protected]
Day Meeting
Wednesday 23 novemberrabbit nursing: how to do it rightSpeakers: Richard Saunders and Claire KingNottingham BelfryDetails from [email protected]
Day Meeting
thursday 24 novemberClinical nutrition: let food be your first medicineSpeaker: Penny WatsonRadisson SAS, Manchester AirportDetails from [email protected]
Day Meeting
thursday 17 novembera stitch in time: all you need to know about small animal ophthalmic surgerySpeakers: Sue Manning and Jim CarterCrowne Plaza, Gatwick Airport RH11 7SXDetails from [email protected]
BSava roaD ShoW – Metropolitan region
Wednesday 9 novemberrabbit road Show: the essentials of rabbit medicine in 1 daySpeakers: Karen Rosenthal and Anna MeredithBellhouse, BeaconsfieldDetails from [email protected]
Wednesday 9 novemberWednesday 9 november
BSava roaD ShoW – north eaSt region
Monday 14 novemberrabbit road Show: the essentials of rabbit medicine in 1 daySpeakers: Karen Rosenthal and Anna MeredithThe Bridge Hotel, Walshford, Wetherby, North Yorkshire LS22 5HSDetails from [email protected]
Monday 14 novemberMonday 14 november
BSava roaD ShoW – MiDlanDS region
Friday 11 novemberrabbit road Show: the essentials of rabbit medicine in 1 daySpeakers: Karen Rosenthal and Anna MeredithYew Lodge, Kegworth, DerbyDetails from [email protected]
BSava roaD ShoW – Kent region
Wednesday 16 novemberrabbit road Show: the essentials of rabbit medicine in 1 daySpeakers: Karen Rosenthal and Anna MeredithBridgewood Manor Hotel, ChathamDetails from [email protected]
Wednesday 16 novemberWednesday 16 november
34-35 Diary.indd 34 20/10/2011 08:29
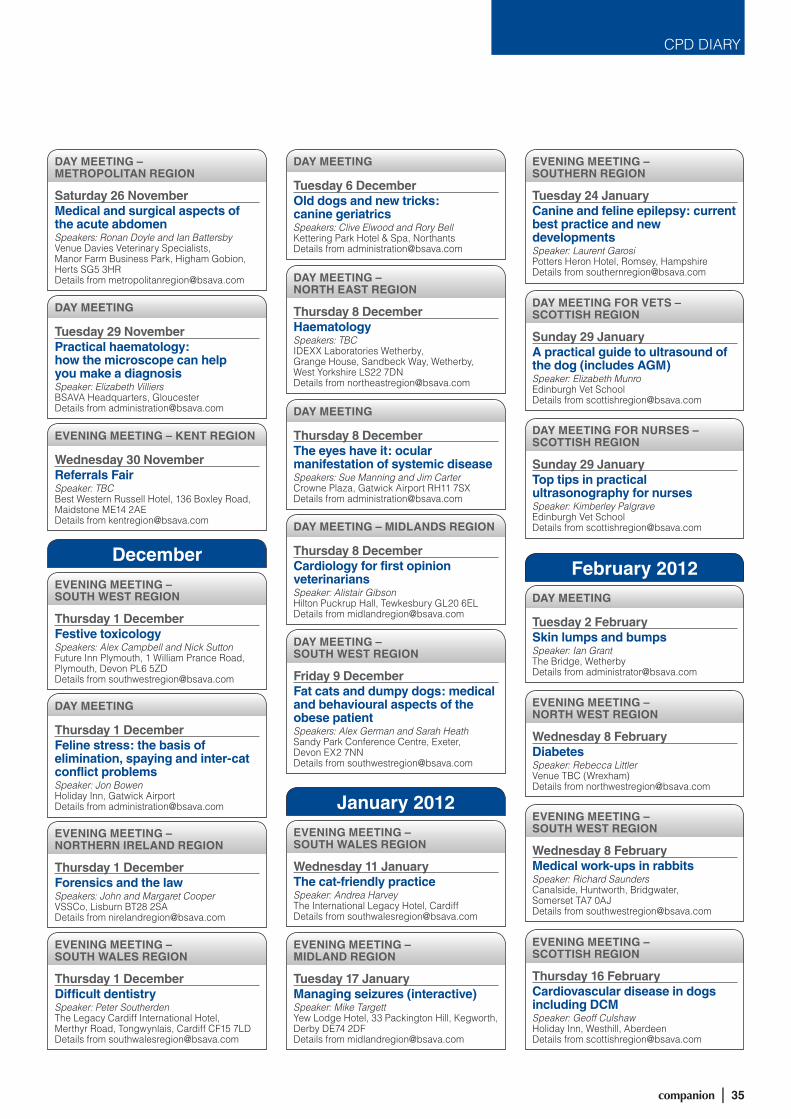
companion | 35
CPD DIARY
Day Meeting – Metropolitan region
Saturday 26 novemberMedical and surgical aspects of the acute abdomenSpeakers: Ronan Doyle and Ian BattersbyVenue Davies Veterinary Specialists, Manor Farm Business Park, Higham Gobion, Herts SG5 3HRDetails from [email protected]
evening Meeting – South WeSt region
thursday 1 DecemberFestive toxicologySpeakers: Alex Campbell and Nick SuttonFuture Inn Plymouth, 1 William Prance Road, Plymouth, Devon PL6 5ZDDetails from [email protected]
evening Meeting – northern irelanD region
thursday 1 DecemberForensics and the lawSpeakers: John and Margaret CooperVSSCo, Lisburn BT28 2SADetails from [email protected]
evening Meeting – South WaleS region
thursday 1 DecemberDifficult dentistrySpeaker: Peter SoutherdenThe Legacy Cardiff International Hotel, Merthyr Road, Tongwynlais, Cardiff CF15 7LDDetails from [email protected]
evening Meeting – MiDlanD region
tuesday 17 JanuaryManaging seizures (interactive)Speaker: Mike TargettYew Lodge Hotel, 33 Packington Hill, Kegworth, Derby DE74 2DFDetails from [email protected]
evening Meeting – Southern region
tuesday 24 JanuaryCanine and feline epilepsy: current best practice and new developmentsSpeaker: Laurent GarosiPotters Heron Hotel, Romsey, HampshireDetails from [email protected]
Day Meeting For vetS – SCottiSh region
Sunday 29 Januarya practical guide to ultrasound of the dog (includes agM)Speaker: Elizabeth MunroEdinburgh Vet SchoolDetails from [email protected]
Day Meeting For nurSeS – SCottiSh region
Sunday 29 Januarytop tips in practical ultrasonography for nursesSpeaker: Kimberley PalgraveEdinburgh Vet SchoolDetails from [email protected]
evening Meeting – north WeSt region
Wednesday 8 FebruaryDiabetesSpeaker: Rebecca LittlerVenue TBC (Wrexham)Details from [email protected]
evening Meeting – South WeSt region
Wednesday 8 FebruaryMedical work-ups in rabbitsSpeaker: Richard SaundersCanalside, Huntworth, Bridgwater, Somerset TA7 0AJDetails from [email protected]
evening Meeting – SCottiSh region
thursday 16 FebruaryCardiovascular disease in dogs including DCMSpeaker: Geoff CulshawHoliday Inn, Westhill, AberdeenDetails from [email protected]
evening Meeting – South WaleS region
Wednesday 11 Januarythe cat-friendly practiceSpeaker: Andrea HarveyThe International Legacy Hotel, CardiffDetails from [email protected]
Day Meeting – north eaSt region
thursday 8 DecemberhaematologySpeakers: TBCIDEXX Laboratories Wetherby, Grange House, Sandbeck Way, Wetherby, West Yorkshire LS22 7DNDetails from [email protected]
Day Meeting – South WeSt region
Friday 9 DecemberFat cats and dumpy dogs: medical and behavioural aspects of the obese patientSpeakers: Alex German and Sarah HeathSandy Park Conference Centre, Exeter, Devon EX2 7NNDetails from [email protected]
Day Meeting
tuesday 29 novemberpractical haematology: how the microscope can help you make a diagnosisSpeaker: Elizabeth VilliersBSAVA Headquarters, GloucesterDetails from [email protected]
Day Meeting
tuesday 6 Decemberold dogs and new tricks: canine geriatricsSpeakers: Clive Elwood and Rory BellKettering Park Hotel & Spa, NorthantsDetails from [email protected]
Day Meeting
thursday 8 Decemberthe eyes have it: ocular manifestation of systemic diseaseSpeakers: Sue Manning and Jim CarterCrowne Plaza, Gatwick Airport RH11 7SXDetails from [email protected]
Day Meeting – MiDlanDS region
thursday 8 DecemberCardiology for first opinion veterinariansSpeaker: Alistair GibsonHilton Puckrup Hall, Tewkesbury GL20 6ELDetails from [email protected]
Day Meeting
tuesday 2 FebruarySkin lumps and bumpsSpeaker: Ian GrantThe Bridge, WetherbyDetails from [email protected]
Day Meeting
thursday 1 DecemberFeline stress: the basis of elimination, spaying and inter-cat conflict problemsSpeaker: Jon BowenHoliday Inn, Gatwick AirportDetails from [email protected]
evening Meeting – Kent region
Wednesday 30 novemberreferrals FairSpeaker: TBCBest Western Russell Hotel, 136 Boxley Road, Maidstone ME14 2AEDetails from [email protected]
December
January 2012
February 2012
34-35 Diary.indd 35 20/10/2011 08:29
Evaluate signs of stress and causes of stress in cats■ Identify the causes of common behavioural problems■ Plan environmental modifi cation programmes to minimise
the impact of stress on cats■ Plan treatment programmes for behavioural problems
and to minimise stress
Thursday 1 December 2011Holiday Inn, Gatwick AirportBSAVA Member: £218.00 Non-member: £327.00
Felinestressthe basis of elimination, spraying and inter-cat confl ict problems
Visit www.bsava.com or call 01452 726700 to book your place.
Jon Bowen offers a wealth of information on this intermediate course for practitioners who want greater insight and more confi dence when tackling behavioural cases
36 OBC.indd 36 20/10/2011 08:28





























