Embed Size (px)
Citation preview
www.elsevier.com/locate/jad
Journal of Affective Disorders 80 (2004) 163–171
Research report
Comorbidity of generalized social anxiety disorder and depression
in a pediatric primary care sample
Denise A. Chaviraa,*, Murray B. Steina, Kelly Baileyb, Martin T. Steinc
aDepartment of Psychiatry, University of California San Diego, 8950 Villa La Jolla Drive, Suite 2243, La Jolla, CA 92037, USAbDepartment of Psychology, San Diego State University, San Diego, CA, USA
cDepartment of Pediatrics, University of California San Diego, La Jolla, CA, USA
Received 29 August 2002; accepted 5 March 2003
Abstract
Background: Comorbidity between adult social anxiety disorder and major depression is extensive. Considerably less
information about this relationship is available among youth. Methods: A randomly selected (from enrollees in a pediatric
primary care clinic) sample of 190 families with children between the ages of 8 and 17 responded by mail to questionnaires
assessing social anxiety, depression, and social functioning. Parents also completed a semi-structured telephone diagnostic
interview about their child. Results: The generalized type of social anxiety disorder was highly comorbid with major depression,
generalized anxiety disorder, specific phobias, and ADHD, while little comorbidity was present for the nongeneralized subtype
of social anxiety disorder. Logistic regression analyses indicated that generalized social anxiety disorder was the only anxiety
disorder associated with an increased likelihood of major depression (OR=5.1). In all cases, social anxiety disorder had a
significantly earlier age of onset than major depression. Limitations: This study relies on cross-sectional data and diagnoses are
based on parent reporting of child behavior. Conclusions: Generalized social anxiety disorder is strongly associated with
depressive illness in youth. Screening and treatment approaches that consider both social anxiety and depressive symptoms are
necessary. Early intervention to treat social anxiety disorder may prevent later depressive disorders.
D 2003 Elsevier B.V. All rights reserved.
Keywords: Social anxiety disorder; Subtypes; Children; Major depression; Primary care
1. Introduction
Considerable research has documented that child-
hood anxiety and depressive disorders are highly
comorbid. In a review of 21 population-based studies
that used DSM criteria, approximately 11–69%
0165-0327/$ - see front matter D 2003 Elsevier B.V. All rights reserved.
doi:10.1016/S0165-0327(03)00103-4
* Corresponding author. Tel.: +1-858-622-6124; fax: +1-858-
450-1491.
E-mail address: [email protected] (D.A. Chavira).
(median=17%) of anxious youth had a comorbid
depressive disorder while 15–75% (median=39%)
of depressed youth had a comorbid anxiety disorder
(Angold et al., 1999). Social anxiety disorder, one of
the more prevalent anxiety disorders of childhood
(Verhulst et al., 1997; Wittchen et al., 1999), fre-
quently co-occurs with depression. Data from epide-
miological studies indicate that approximately 25–
31% of adolescents and young adults with social
anxiety disorder have a comorbid depressive disorder
(Essau et al., 1999; Wittchen et al., 1999) while rates

D.A. Chavira et al. / Journal of Affective Disorders 80 (2004) 163–171164
from clinical studies are higher, ranging from 17 to
52% (Last et al., 1992; Albano et al., 1996; Chavira
and Stein, 2002). Social anxiety disorder has an age
of onset in the early teens and usually precedes the
onset of depressive disorders (Schneier et al., 1992;
Wittchen et al., 1999).
High rates of comorbidity and the temporal pri-
macy of many anxiety disorders have prompted
interest in the role of anxiety as a risk factor for
depression. In a longitudinal study, overanxious dis-
order (using DSM-III-R criteria, some cases of which
would likely be classified as social anxiety disorder
using DSM-IV) during adolescence was associated
with an increased odds ratio (OR=2.92) for major
depression during early adulthood (Pine et al., 1998).
In another longitudinal study of adolescents and
young adults, social anxiety disorder at initial assess-
ment was associated with an increased risk for major
depression at follow-up (34–50 months later)
(Wittchen et al., 1998). Data from the same study
also provided information regarding social anxiety
disorder subtypes. Adolescents and young adults
(ages 14–24) with the generalized subtype (i.e., fear
and avoidance of three out of six social situations)
had more co-occurring diagnoses, especially specific
phobia, post-traumatic stress disorder and dysthymia,
and experienced greater impairment than individuals
with the nongeneralized subtype. In contrast, Hof-
mann et al. (1999) did not find that adolescents being
treated for GSAD had more frequent depression
diagnoses or overall comorbidity than the nongener-
alized subtype. Their findings did indicate, however,
that GSAD was associated with greater self-reported
anxiety symptoms and a trend for elevated levels of
self-reported depressive symptoms. Differences in
subtyping schema, as well as age differences in the
samples, may account for differences in findings
across these studies.
1.1. Study aims
In the current study we were interested in evaluat-
ing rates of comorbidity between social anxiety dis-
order and major depression in a representative sample
of children and adolescents (ages 8–17) who were not
seeking mental health treatment. We were particularly
interested in how comorbidities, age of onset, and
social impairment might vary across subtypes. We
hypothesized that the presence of social anxiety dis-
order, particularly GSAD, would be associated with
an increased likelihood of major depression when
compared to other anxiety disorders. In addition, we
expected that GSAD would be associated with greater
comorbidity, more impairment, and an earlier age of
onset.
2. Methods
2.1. Participants and procedure
The current report is part of a larger project where
1173 families with children between the ages of 8 and
17 were selected from among enrollees in a pediatric
primary care clinic to participate in a study about
social anxiety. Initially, 2681 families were catego-
rized into two groups based on age of a randomly
selected index child from within the family (8–12 and
13–17 years old) and thereafter approximately 700
families from each age group were randomly selected.
Brief questionnaire packets were mailed to all selected
residences for both the child and parent to complete,
resulting in an eligible sample of 1173 families. Of
those families, 714 parents and children completed
paper and pencil measures of social anxiety in the first
phase of this study and 359 families also expressed
interest in completing the second phase that included a
questionnaire and a telephone interview with the
parent about the target child. Complete data were
received from 190 families (i.e., parental consent
and child or adolescent assent, questionnaires, and
parent telephone interview). A postdoctoral level
psychologist and an advanced masters student in
psychology conducted the interviews. The Human
Research Protection Program at our University ap-
proved this research.
The mean age of the parents completing the second
phase of the study was 43.9 (S.D.=6.0). Most parent
participants had a college education (75%) and were
Caucasian American (71%). The ethnic composition
of the non-Caucasian parent sample included Latinos/
Hispanic Americans (8%), African Americans (6%),
Filipino/Asian Americans (7%) and individuals who
identified as multicultural (8%). Approximately 53%
of the child participants were between the ages of
8 and 12 and 47% were between the ages of 13 and

D.A. Chavira et al. / Journal of Affective Disorders 80 (2004) 163–171 165
17. An equivalent number of boys (49%) and girls
(51%) participated in the study.
3. Assessments
3.1. Semi-structured interview
3.1.1. Anxiety disorders interview schedule for
children
The Anxiety Disorders Interview Schedule for
Children–Parent Version (Silverman and Albano,
1996) is a semi-structured diagnostic interview
designed to assess DSM-IV childhood anxiety disor-
ders as well as depressive and behavioral disorders.
Published j coefficients for the ADIS-C/P are 0.88 for
separation anxiety, 0.86 for social anxiety disorder,
0.65 for specific phobia, 0.72 for generalized anxiety
disorder, and 1.00 for ADHD (Silverman et al., 2001).
In the current study, the following modules were
included: separation anxiety disorder, social anxiety
disorder, specific phobia, generalized anxiety disor-
der, obsessive compulsive disorder, dysthymia, major
depression, eating disorders, selective mutism, and
ADHD. A generalized social anxiety disorder
(GSAD) diagnosis was applied if significant fear
and avoidance were endorsed for at least four of the
21 social situations queried and at least two situations
were interactional. In addition, an impairment rating
of 4 or greater (‘some’, ‘a lot’, ‘very very much’) was
necessary for a social anxiety disorder diagnosis.
Individuals who had fewer than four fears or only
performance-related fears were assigned to the non-
generalized social anxiety disorder (NSAD) group.
3.2. Parent and child self-report measures
3.2.1. Social Competence-Parent and Child Report
The social competence questionnaire (Spence,
1995) has both a parent (nine items) and child version
(10 items). Item content focuses on how effective a
child may be in social situations (e.g., ‘has stable
friendships with other kids his/her age,’ ‘finds it easy
to make friends,’ ‘gets invited to parties,’ ‘is popular
among others his/her age’, etc.). A three-point Likert
scale is used. Internal reliability is adequate and total
scores differentiate popular, average, and rejected
children.
3.2.2. The Social Skills Questionnaire
The social skills questionnaire (SSQ-P; Spence,
1995) is a 30-item scale that assesses a parent’s
perception of their child’s social skills. A three-point
Likert scale is used. The SSQ-P has good internal
consistent and split half reliability (Spence, 1995).
3.2.3. The Social Anxiety Scales
The Social Anxiety Scale-Children Revised
(SASC-R; La Greca et al., 1988) and Social Anxiety
Scale-Adolescents (SAS-A; La Greca and Lopez,
1998) were used to assess levels of social anxiety
with regard to peer relations. A five-point Likert scale
is used and there are 18 social anxiety items. Scores in
the range of 50–54 or greater are indicative of clinical
levels of social anxiety (La Greca and Lopez, 1998).
Adequate psychometric properties have been estab-
lished in both clinical and non-clinical samples (La
Greca and Stone, 1993; Ginsburg et al., 1998).
3.2.4. Child Depression Inventory
The Child Depression Inventory-Short Form (CDI-
S) is a 10-item abbreviated form of the Children’s
Depression Inventory (Kovacs, 1992). The short form
was developed by eliminating items from the long
form with the least reduction in alpha reliability. Items
assessing suicidality are not included in this version.
3.2.5. Asher’s Loneliness Scale
Asher’s loneliness scale (Asher and Wheeler,
1985) scale consists of 16 items assessing feelings
of loneliness and dissatisfaction as well as and eight
filler items. In this study, a three-point Likert scale
was used; total scores range from 0 to 32. The scale
has good internal consistency and is able to differen-
tiate rejected children from other sociometric groups.
4. Results
4.1. Participants versus non-participants
There were no significant differences in child’s
gender, age group, parental level of education, or
child- or parent-reporting of social anxiety severity
between participants who did and did not choose to
participate in the various phases of the study. There
was a trend for more Caucasians than ‘‘non-cauca-

D.A. Chavira et al. / Journal of Affective Disorders 80 (2004) 163–171166
sians’’ to respond to both phases of the study ðv2ð1;n ¼ 676Þ ¼ 3:04;P ¼ 0:08Þ: These findings suggest
that our results in the interviewed sample should be
broadly representative of the pediatric primary care
population from which it was selected.
4.2. Interview reliability
Interviews were audiotaped and reliability data
were gathered on 42 ADIS-C/P interviews. Interrater
reliability was estimated by having the second rater
listen to the audiotaped interviews. The j coefficients
were as follows: specific phobia=0.77, generalized
anxiety disorder=0.90, attention deficit hyperactivity
disorder=0.93, generalized social anxiety disor-
der=1.00, nongeneralized social anxiety disor-
der=1.00, and major depression=1.00. Kappa
coefficients were not calculated for the remaining
disorders due to small sample sizes.
4.3. Social anxiety disorder subtypes: a descriptive
overview
One-way analyses of variance (ANOVAs) were
used to examine differences in level of impairment
Table 1
Proportion of social fears endorsed across social anxiety disorder subtype
Social fears Nongeneralized
(%) (n=15)
Answering questions 20
Reading aloud/reports 47
Asking teacher a question 27
Taking tests 13
Writing on board 13
Interacting in groups 0
Going to gym class 3
Walking in hallways 0
Initiating conversation 8
Using public bathroom 0
Eating in front of others 0
Going to meetings 0
Using telephone 0
Performance 67
Inviting a friend over 0
Talking to adults 13
Speaking to unfamiliar people 20
Going to school activities 20
Having picture taken 0
Asserting self 6
Dealing with confrontation 20
and severity across subtypes. Where non-normal dis-
tributions were found, a nonparametric test was ap-
plied (e.g., Mann–Whitney, Kruskal–Wallis). Youth
with generalized social anxiety disorder (GSAD) had
greater interference ratings when compared to youth
with nongeneralized social anxiety disorder (NSAD)
(MWU=80.5, P=0.01). Using our subtyping criteria,
those with a GSAD diagnosis had approximately 10.5
(S.D.=2.7) social fears and those with NSAD had 3.3
(S.D.=1.8) social fears, F(1,24)=78.83, P<0.001. On
the parent version of the SASC-R/SAS-A, children
and adolescents with GSAD reported higher levels of
social anxiety than those with NSAD; F(1,34)=4.39,
P<0.05 (GSAD Mean=54.8 (S.D.=12.92) versus
NSAD Mean=46.8 (S.D.=8.50)). This difference was
not present when the child versions of the SASC-R
and SAS-A were used, F(1,34)=0.36, P>0.05. There
was an equal distribution of boys and girls as well as
age groups (i.e., 8–12 and 13–17 years old) across
subtypes (v2(1, n=36)=1.15, P=0.14, and v2(1,n=36)=1.15, P=0.14, respectively). Chi-square analy-
ses comparing the differential endorsement of 21
social fears across individuals with GSAD and NSAD
are presented in Table 1. After controlling for multiple
comparisons (P=0.002), social fears including writing
s
Generalized X2 df P
(%) (n=21)
62 4.64 1 0.03
76 2.15 1 0.14
62 3.06 1 0.08
24 0.13 1 0.72
81 13.45 1 0.001
62 11.98 1 0.001
14 0.82 1 0.36
14 2.40 1 0.12
53 15.44 1 0.001
8.3 0.84 1 0.36
8.3 0.84 1 0.36
22 5.31 1 0.02
14 2.40 1 0.12
67 0.00 1 1.00
14 2.40 1 0.12
57 5.34 1 0.02
81 10.81 1 0.001
48 1.82 1 0.18
22 5.31 1 0.02
33 5.34 1 0.02
62 4.64 1 0.03
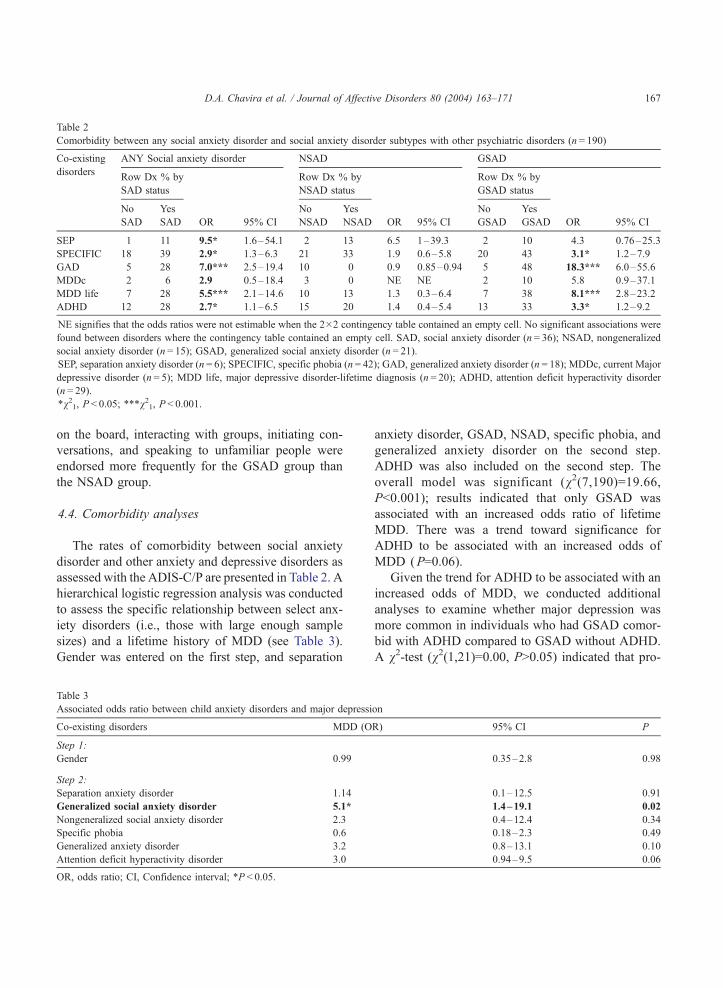
Table 2
Comorbidity between any social anxiety disorder and social anxiety disorder subtypes with other psychiatric disorders (n = 190)
Co-existing ANY Social anxiety disorder NSAD GSAD
disordersRow Dx % by Row Dx % by Row Dx % by
SAD status NSAD status GSAD status
No Yes No Yes No Yes
SAD SAD OR 95% CI NSAD NSAD OR 95% CI GSAD GSAD OR 95% CI
SEP 1 11 9.5* 1.6–54.1 2 13 6.5 1–39.3 2 10 4.3 0.76–25.3
SPECIFIC 18 39 2.9* 1.3–6.3 21 33 1.9 0.6–5.8 20 43 3.1* 1.2–7.9
GAD 5 28 7.0*** 2.5–19.4 10 0 0.9 0.85–0.94 5 48 18.3*** 6.0–55.6
MDDc 2 6 2.9 0.5–18.4 3 0 NE NE 2 10 5.8 0.9–37.1
MDD life 7 28 5.5*** 2.1–14.6 10 13 1.3 0.3–6.4 7 38 8.1*** 2.8–23.2
ADHD 12 28 2.7* 1.1–6.5 15 20 1.4 0.4–5.4 13 33 3.3* 1.2–9.2
NE signifies that the odds ratios were not estimable when the 2�2 contingency table contained an empty cell. No significant associations were
found between disorders where the contingency table contained an empty cell. SAD, social anxiety disorder (n = 36); NSAD, nongeneralized
social anxiety disorder (n = 15); GSAD, generalized social anxiety disorder (n = 21).
SEP, separation anxiety disorder (n = 6); SPECIFIC, specific phobia (n = 42); GAD, generalized anxiety disorder (n = 18); MDDc, current Major
depressive disorder (n = 5); MDD life, major depressive disorder-lifetime diagnosis (n = 20); ADHD, attention deficit hyperactivity disorder
(n = 29).
*v21, P < 0.05; ***v21, P < 0.001.
D.A. Chavira et al. / Journal of Affective Disorders 80 (2004) 163–171 167
on the board, interacting with groups, initiating con-
versations, and speaking to unfamiliar people were
endorsed more frequently for the GSAD group than
the NSAD group.
4.4. Comorbidity analyses
The rates of comorbidity between social anxiety
disorder and other anxiety and depressive disorders as
assessed with the ADIS-C/P are presented in Table 2. A
hierarchical logistic regression analysis was conducted
to assess the specific relationship between select anx-
iety disorders (i.e., those with large enough sample
sizes) and a lifetime history of MDD (see Table 3).
Gender was entered on the first step, and separation
Table 3
Associated odds ratio between child anxiety disorders and major depressi
Co-existing disorders MDD (O
Step 1:
Gender 0.99
Step 2:
Separation anxiety disorder 1.14
Generalized social anxiety disorder 5.1*
Nongeneralized social anxiety disorder 2.3
Specific phobia 0.6
Generalized anxiety disorder 3.2
Attention deficit hyperactivity disorder 3.0
OR, odds ratio; CI, Confidence interval; *P < 0.05.
anxiety disorder, GSAD, NSAD, specific phobia, and
generalized anxiety disorder on the second step.
ADHD was also included on the second step. The
overall model was significant (v2(7,190)=19.66,P<0.001); results indicated that only GSAD was
associated with an increased odds ratio of lifetime
MDD. There was a trend toward significance for
ADHD to be associated with an increased odds of
MDD (P=0.06).
Given the trend for ADHD to be associated with an
increased odds of MDD, we conducted additional
analyses to examine whether major depression was
more common in individuals who had GSAD comor-
bid with ADHD compared to GSAD without ADHD.
A v2-test (v2(1,21)=0.00, P>0.05) indicated that pro-
on
R) 95% CI P
0.35–2.8 0.98
0.1–12.5 0.91
1.4–19.1 0.02
0.4–12.4 0.34
0.18–2.3 0.49
0.8–13.1 0.10
0.94–9.5 0.06

D.A. Chavira et al. / Journal of Affective Disorders 80 (2004) 163–171168
portions of individuals with MDD were similar across
these groups.
4.5. Age and order of onset
All social anxiety disorder diagnoses (100%) pre-
ceded the onset of major depression. The mean age of
onset for social anxiety disorder was 7.1 years old
(S.D.=2.6) and for major depression, 13.2 years old
(S.D.=3.4). Children and adolescents with GSAD had
an earlier age of social anxiety disorder onset than
those with NSAD (M=5.1 (S.D.=2.2) vs. M=8.0
(S.D.=3.1), respectively), F(1,30)=8.19, P<0.01.
4.6. Social functioning outcomes across subtypes
Separate MANCOVAs were performed on parent
and child self-report measures of social functioning
and social outcomes; number of comorbid disorders
(which ranged from 0 to 4) was entered as a
covariate. Multivariate analyses revealed a main
effect of social phobia subtype on parental report of
child’s social functioning; Wilk’s F(2,31)=4.90,
P < 0.01. Children with a GSAD diagnosis were less
socially skilled than children with a NSAD diagnosis
(M=37.5 vs. M=48.9), respectively; F(2,32)=6.47,
P < 0.001. There were no significant differences on
parent’s report of social competence between sub-
types. The MANCOVA for child reports of social
competence, loneliness and depression was not sig-
nificant Wilk’s F(3,28)=0.59, P>0.05.
5. Discussion
The relationship between social anxiety disorder
and major depression is well documented in both the
adolescent and adult literatures but few studies have
looked at this relationship in younger children who
are not being recruited from a mental health clinic.
Using a representative sample is particularly impor-
tant given that comorbid conditions such as major
depression may prompt treatment-seeking behavior
(Schneier et al., 1992; Last et al., 1997), thereby
inflating comorbidity estimates in psychiatric sam-
ples. Furthermore, the topic of differences in social
anxiety subtypes has received little attention in the
child literature.
Findings from the current study confirm that the
comorbidity between social anxiety disorder and ma-
jor depression is significant even in a sample of
children and adolescents not seeking care for a mental
disorder. Approximately 28% of children with any
type of social anxiety disorder reported a lifetime
history of major depression, a rate consistent with
epidemiological studies (Essau et al., 1999; Wittchen
et al., 1999). A higher comorbidity rate (38%), similar
to those found in psychiatric samples, emerged among
children with the generalized subtype of social anxiety
disorder. When four of the most common anxiety
disorders were evaluated, generalized social anxiety
disorder was the only anxiety disorder associated with
an increased likelihood of lifetime major depression.
The presence of comorbid social anxiety disorder and
depression is particularly important given that such
children frequently report more severe depressive
symptoms and suicidality over time when compared
to children with depression only (Stein et al., 2001).
Furthermore, children with comorbid anxiety and
depression are more likely than anxious children
without lifetime depression to utilize mental health
services and to report functional impairment during
adulthood (Last et al., 1997).
Consistent with findings from longitudinal studies
of anxiety and depression (Breslau et al., 1995; Lew-
insohn et al., 1995), the age of onset of social anxiety
disorder predated major depression. An understanding
of the temporal primacy of social anxiety disorder
requires further investigation, but it may be that etio-
logical variables (including temperament, family influ-
ences, and cognitive biases) foster skills deficits and
avoidant behaviors that contribute to social isolation,
demoralization and subsequent depression (Brady and
Kendall, 1992; Stein et al., 2001). In general, the
presence of anxiety may overwhelm a child’s coping
resources in stressful situations, either physically or
cognitively, thereby creating a liability for depression.
It is plausible that early intervention for anxiety dis-
orders may reduce the risk for subsequent problems
such as substance abuse, depression, and suicidality.
Significant comorbidity between ADHD and major
depression has been found in previous studies (Mil-
berger et al., 1995; Biederman et al., 1996) and it has
been suggested that ADHD may be associated with
depressive risk factors including interpersonal deficits
and self-esteem problems (Slomkowski et al., 1995;

D.A. Chavira et al. / Journal of Affective Disorders 80 (2004) 163–171 169
Greene et al., 2001). Given this relationship, and the
fact that ADHD and social anxiety disorder were
highly comorbid in this study, we examined rates of
major depression among children who had general-
ized social anxiety disorder with and without ADHD.
Rates of depression were comparable across the
groups, suggesting that the presence of a comorbid
ADHD diagnosis did not explain the relationship
between generalized social anxiety disorder and de-
pression. The substantial comorbidity between ADHD
and anxiety disorders remains an important issue
given that comorbid disorders may influence baseline
characteristics, functional impairment and treatment
outcome (Greene et al., 2001; Jensen et al., 2001).
A second aim of this study was to assess differ-
ences in comorbidity, severity, impairment, and social
functioning across social anxiety subtypes. Social
fears that seemed to distinguish the generalized and
nongeneralized subtypes were mostly interactional in
nature, including interacting in groups, initiating con-
versation, speaking to unfamiliar people and to a
lesser extent, going to meetings, talking to adults,
asserting oneself, and dealing with confrontation.
Children with nongeneralized social anxiety disorder
had fears that could best be characterized as ‘public
speaking’ or ‘performance anxiety’. Participants with
the generalized subtype more often had comorbid
depression, anxiety (i.e., GAD and specific phobias)
and ADHD, whereas significant comorbidity was not
present in the nongeneralized subtype. Greater sever-
ity, more impairment, and an earlier age of onset were
also present in the generalized subgroup. Paralleling
findings from the adult literature, GSAD in youth
appears to be a more pervasive and disabling condi-
tion than NSAD (Stein and Chavira, 1998; Wittchen
et al., 1999).
Using self-report paper and pencil measures, sub-
type differences emerged on parents’ report of social
skills; a finding that is consistent with studies from
clinical samples of children with social anxiety disor-
der where social skills deficits are pronounced (Beidel
et al., 1999; Spence et al., 1999). The GSAD and
NSAD groups did not differ, however, on measures of
social competence, or on child’s self-report of loneli-
ness and depression. It is possible that children in the
GSAD group, while impaired, may not be avoiding
social situations to the same degree as those seen in
mental health settings. The absence of differences
between subtypes on the child depression scale may
be due to the fact that this measure was based on
child’s report and used a 2-week time frame. The
ADIS diagnoses, on the other hand, were derived
from parent report and queried a lifetime history of
major depression.
6. Limitations
The study is limited by its cross-sectional nature
and the use of telephone interviews that were only
conducted with parents about the target child. In a
study of the comparability of telephone and face-to-
face interviews, Rohde et al. (1997) found that the
reliability was excellent for anxiety disorders and very
good for major depressive disorder and substance use
disorders. The discrepancy between child and parent
report remains a topic of debate with little consensus.
Research shows that whenever parents and children
are independently assessed, reports are rarely over-
lapping (Verhulst et al., 1997; Grills and Ollendick,
2003); this seems to be true for both internalizing and
externalizing disorders although agreement seems to
be greater for behaviors that are more observable (i.e.,
externalizing behaviors) (Silverman and Eisen, 1992).
To date, a data-driven argument for weighing one
informant’s report more heavily is not available.
Due to time constraints, all childhood psychiatric
disorders were not assessed; for example, we did not
include conduct disorder and oppositional defiant
disorder. Additionally, developmental disorders that
might predispose individuals to be socially anxious,
including autistic spectrum disorders and communi-
cation/language disorders were not formally assessed,
although screening questions about pervasive devel-
opmental disorders and communication delays were
administered.
The sample was predominantly Caucasian and
well-educated; therefore the generalizability of our
results is somewhat limited. Generalizability may also
be limited by possible biases among those who chose
to participate at various junctures in the study. Find-
ings did indicate, however, that demographic charac-
teristics and social anxiety scores of those who
completed various phases of the study were similar
across individuals who chose to participate and those
who did not participate.

D.A. Chavira et al. / Journal of Affective Disorders 80 (2004) 163–171170
7. Conclusion
Findings from this study suggest that social anxiety
disorder is associated with considerable psychosocial
burden in a representative pediatric primary care (i.e.,
non mental-healthcare seeking) sample. Children who
present with the generalized subtype of social anxiety
disorder are more likely to require treatment than
individuals with the nongeneralized subtype and
may also benefit from treatment that addresses con-
current anxiety and depressive symptoms. Also, social
skills deficits are likely to perpetuate the anxiety and
avoidance found in GSAD; for some children, these
should become a primary focus of therapy. Many of
our current screening instruments and psychosocial
treatments may need to be modified to meet the time
and cost constraints of today’s tightly managed care
health system. It is hypothesized that early detection
and treatment may alter the chronic and frequently
disabling course of both anxiety and depressive dis-
orders, and that the pediatric primary care setting may
provide an ideal clinical venue in which to test such
interventions.
Acknowledgements
Funded in part by NIMH grant K24 MH64122-01
to MBS.
References
Albano, A.M., Chorpita, B., Barlow, D., 1996. Childhood anxiety
disorders. In: Mash, E.J., Barkley, R.A. (Eds.), Child Psychopa-
thology. Guilford Press, New York, pp. 196–241.
Angold, A., Costello, J.E., Erkanli, A., 1999. Comorbidity. J. Child
Psychol. Psychiatry 40, 57–87.
Asher, S.R., Wheeler, V.A., 1985. Children’s loneliness: a compar-
ison of rejected and neglected peer status. J. Cons. Clin. Psy-
chol. 53, 500–505.
Beidel, D.C., Turner, S.M., Morris, T.L., 1999. Psychopathology of
childhood social phobia. J. Am. Acad. Child Adolesc. Psychia-
try 28, 643–650.
Biederman, J., Faraone, S., Milberger, S., Guite, J., Mick, E.,
Chen, L., Mennin, D., Marrs, A., Ouellette, C., Moore, P.,
Spencer, T., Norman, D., Wilens, T., Kraus, I., Perrin, J.,
1996. A prospective 4-year follow-up study of attention-def-
icit hyperactivity and related disorders. Arch. Gen. Psychiatry
53, 437–446.
Brady, E.U., Kendall, P.C., 1992. Comorbidity of anxiety and
depression in children and adolescents. Psychol. Bull. 111,
244–255.
Breslau, N., Schultz, L., Peterson, E., 1995. Sex differences in
depression: A role for preexisting anxiety. J. Psychiatr. Res.
58, 1–12.
Chavira, D.A., Stein, M.B., 2002. Combined psychoeducation and
treatment with selective serotonin reuptake inhibitors for youth
with generalized social anxiety disorder. J. Child Adolesc. Psy-
chopharmacol. 12, 47–54.
Essau, C.A., Conradt, J., Petermann, F., 1999. Frequency of comor-
bidity of social phobia and social fears in adolescents. Behav.
Res. Ther. 37, 831–843.
Ginsburg, G.S., La Greca, A.M., Silverman, W.K., 1998. Social anx-
iety in children with anxiety disorders: relation with social and
emotional functioning. J. Abnorm. Child Psychol. 26, 175–186.
Greene, R.W., Biederman, J., Faraone, S.V., Monuteaux, M.C.,
Mick, E., DuPre, E.P., Fine, C.S., Goring, J.C., 2001. Social
impairment in girls with ADHD: patterns, gender comparisons,
and correlates. J. Am. Acad. Child Adolesc. Psychiatry 40,
704–710.
Grills, A.E., Ollendick, T.H., 2003. Multiple informant agreement
and the anxiety disorders interview schedule for parents and
children. J. Am. Acad. Child Adolesc. Psychiatry 42, 30–40.
Hofmann, S.G., Albano, A.M., Heimberg, R.G., Tracey, S., Chor-
pita, B.F., Barlow, D.H., 1999. Subtypes of social phobia in
adolescents. Depression Anxiety 9, 15–18.
Jensen, P.S., Hinshaw, S.P., Kraemer, H.C. et al., 2001. ADHD
comorbidity findings from the MTA study: comparing comor-
bid subgroups. J. Am. Acad. Child Adolesc. Psychiatry 40,
147–158.
Kovacs, M., 1992. In: Children’s Depression Inventory: Manual
Multi-Health Systems, North Tonawanda, NY.
La Greca, A.M., Lopez, N., 1998. Social anxiety among adoles-
cents: linkages with peer relations and friendships. J. Abnorm.
Child Psychol. 26, 83–95.
La Greca, A.M., Stone, W.L., 1993. Social Anxiety Scale for Chil-
dren-Revised: Factor structure and concurrent validity. J. Clin.
Child Psychol. 22, 17–27.
La Greca, A.M., Dandes, S.K., Wick, P., Shaw, K., Stone, W.L.,
1988. The development of the Social Anxiety Scale for Children
(SASC): Reliability and concurrent validity. J. Clin. Child Psy-
chol. 17, 84–91.
Last, C.G., Perrin, S., Hersen, M., Kazdin, A.E., 1992. DSM-III-R
anxiety disorders in children: sociodemographic and clinical
characteristics. J. Am. Acad. Child Adolesc. Psychiatry 31,
1070–1076.
Last, C.G., Hansen, C., Franco, N., 1997. Anxious children in
adulthood: a prospective study of adjustment. J. Am. Acad.
Child Adolesc. Psychiatry 26, 645–652.
Lewinsohn, P.M., Rohde, P., Seeley, J.R., 1995. Adolescent psy-
chopathology, III: the clinical consequences of comorbidity. J.
Am. Acad. Child Adolesc. Psychiatry 34, 510–519.
Milberger, S., Biederman, J., Faraone, S.V., Murphy, J., Tsuang,
M.T., 1995. Comorbidity within attention deficit hyperactivity
disorder is not an artifact of overlapping symptomatology.
Am. J. Psychiatry 152, 1793–1800.

D.A. Chavira et al. / Journal of Affective Disorders 80 (2004) 163–171 171
Pine, D.S., Cohen, P., Gurley, D., Brook, J., Ma, Y., 1998. The risk
for early-adulthood anxiety and depressive disorders in adoles-
cents with anxiety and depressive disorders. Arch. Gen. Psychi-
atry 55, 56–64.
Rohde, P., Lewinsohn, P.M., Seeley, J.R., 1997. Comparability of
telephone and face-to-face interviews in assessing axis I and II
disorders. Am. J. Psychiatry 154, 1593–1598.
Schneier, F.R., Johnson, J., Hornig, C.D., Liebowitz, M.R., Weiss-
man, M.M., 1992. Social phobia: Comorbidity and morbidity in
an epidemiologic sample. Arch. Gen. Psychiatry 49, 282–288.
Silverman, W., Albano, A.M., 1996. In: Anxiety Disorders Inter-
view Schedule For Children Using DSM-IV Psychological Cor-
poration, San Antonio, TX.
Silverman, W.K., Eisen, A.R., 1992. Age differences in the reliabil-
ity of parent and child reports of child anxious symptomatology
using a structured interview. J. Am. Acad. Child Adolesc. Psy-
chiatry 31, 117–124.
Silverman, W.K., Saavedra, L.M., Pina, A.A., 2001. Test-retest
reliability of anxiety symptoms and diagnoses with the anxiety
disorders interview schedule for DSM-IV: child and parent ver-
sions. J. Am. Acad. Child Adolesc. Psychiatry 40, 937–944.
Slomkowski, C., Klein, R.G., Mannuzza, S., 1995. Is self-esteem an
important outcome in hyperactive children? J. Abnorm. Child
Psychol. 23, 303–315.
Spence, S., 1995. In: Social Skills Training: Enhancing social com-
petence with children and adolescents NFER-NELSON Publish-
ing Company, Windsor, UK.
Spence, S., Donovan, C., Brechman-Toussaint, M., 1999. Social
skills, social outcomes, and cognitive features of childhood so-
cial phobia. J. Abnorm. Psychol. 108, 211–221.
Stein, M.B., Chavira, D.A., 1998. Subtypes of social phobias and
comorbidity with depression and other anxiety disorders. J. Af-
fect Disord. 50, 11–16.
Stein, M.B., Fuetsch, M., Muller, N., Hofler, M., Lieb, R.,
Wittchen, H.-U., 2001. Social anxiety disorder and the risk of
depression. Arch. Gen. Psychiatry 58, 251–256.
Verhulst, F.C., van der Ende, J., Ferdinand, R.F., Kasius, M.C.,
1997. The prevalence of DSM-III-R diagnoses in a national
sample of Dutch adolescents. Arch. Gen. Psychiatry 54,
329–336.
Wittchen, H.-U., Nelson, C.B., Lachner, G., 1998. Prevalence of
mental disorders and psychosocial impairments in adolescents
and young adults. Psychol. Med. 28, 109–126.
Wittchen, H.-U., Stein, M.B., Kessler, R.C., 1999. Social fears and
social phobia in a community sample of adolescents and young
adults: prevalence, risk factors and co-morbidity. Psychol. Med.
29, 309–323.