Embed Size (px)
Citation preview

Comorbidity between personality disorders anddepressive symptomatology in women: A cross-sectional study of three different transitionallife stages
AURORE ENFOUX1, ROBERT COURTOIS1,2, INGE DUIJSENS3,4, CHRISTIAN REVEILLERE2,JEAN LOUIS SENON5, GUILLAUME MAGNIN6, MELANIE VOYER5, HELENE MONTMASSON7,VINCENT CAMUS1,8 AND WISSAM EL-HAGE1,8, 1Clinique Psychiatrique Universitaire, Pôlede Psychiatrie, CHRU de Tours, France; 2Département de psychologie, EA2114 ‘Psychologie des âgesde la vie’, Université François Rabelais de Tours PRES Centre-Val de Loire; 3Department of ClinicalHealth andNeuropsychology, LeidenUniversity, Leiden, TheNetherlands; 4Datec Psychological Tests,Leiderdorp, The Netherlands; 5SHU Psychiatrie et Psychologie Médicale, CH Henri Laborit, Poitiers,France; 6Service Gynécologie-Obstétrique, CHU La Milétrie, Poitiers, France; 7Pôle de PsychiatrieGénérale, CH de Blois, France; 8Inserm U930 ERL, Université François Rabelais de Tours, France
ABSTRACTThis study assessed the prevalence of personality disorders (PDs), according to DSM-IV criteria, in relation todepressive symptomatology at three different periods of life in female subjects.Depressive symptoms and personality disorders were assessed in a sample of 568 women from three differenttransitional stages: 134 students, 314 primiparous women after childbirth and 120 women diagnosed with breastcancer. Depressive symptoms were assessed by the Hospital Depression and Anxiety Scale in the first and thirdgroups and by the Edinburgh Post-natal Depression Scale in the second group, whereas PDs were assessed by theFrench version of the Vragenlijst voor Kenmerken van de Persoonlijkheid.Depressive symptomatology and rates of PD (20.4% and 6.3%) were equivalent in the three groups. Theprevalence of PD was higher in the depressed group compared with the non-depressed group, with more paranoid,borderline, avoidant, obsessive–compulsive, schizotypal, antisocial, dependent and histrionic PD.Our findings support the hypothesis that PDs are more frequently associated with depressive symptoms. Borderlineand avoidant PDs were more prevalent among young women. All cluster C PD (dependent, avoidant andobsessive–compulsive) co-occurred significantly with depressive symptoms. Copyright © 2013 JohnWiley& Sons, Ltd.
Introduction
Susceptibility to depression has been linked toheterogeneous aetiology, e.g., environmental and
genetic factors (Caspi et al., 2003; El-Hage, Powell,& Surguladze, 2009), female sex (Kessler et al.,1994) and comorbidity with other mental disorders.The relationship between depression and personality
Copyright © 2013 John Wiley & Sons, Ltd. 7: 233–241 (2013)DOI: 10.1002/pmh
Personality and Mental Health7: 233–241 (2013)Published online 25 March 2013 in Wiley Online Library(wileyonlinelibrary.com) DOI 10.1002/pmh.1228

disorders (PDs) is one of the most commoncomorbidities in psychiatry (Hirschfeld, 1999;Oldham et al., 1995). There is growing evidenceabout the influence of PD on outcome in depressivedisorders, showing for instance that patients with PDare less responsive to therapeutic strategies, but theconclusions are not definitive. Considering the effectof PD on treatment response, relevant reviewsshowed mixed results (Kool et al., 2005; Mulder,2002; Newton-Howes, Tyrer, & Johnson, 2006),with differential efficacy between the different typesof treatments. Thus, PDs seem to have no adverseimpact on treatment response to Cognitive–Behavioural Therapy (Joyce et al., 2007) or Electro-Convulsive Therapy (Mulder, 2002; Newton-Howes,Tyrer, & Johnson, 2006), but negatively affecttreatment response to interpersonal psychotherapy(Joyce et al., 2007). The results remain inconsistentconcerning the antidepressant treatments, withstudies reporting little or no difference in short-termoutcome (Kool et al., 2005; Mulder, 2002).
Approximately two-thirds of patients withPD have suffered from at least one comorbiddepressive episode (Morey et al., 2010), anddepression is frequently associated with PDs suchas avoidant, borderline, dependent, obsessive–compulsive (Skodol et al., 1999) and self-defeating PDs (Hirschfeld, 1999). For Iacovielloet al. (2007), cluster B personality disturbanceconfers a risk for depressions of longer durationand greater severity, whereas cluster C signifi-cantly predicts symptomatic chronicity. For Moreyet al. (2010), the validity of a PD diagnosis is inde-pendent of the local depressive mood, with diag-nosis of the PD remaining stable after remissionfrom depression. Nevertheless, PDs are more prev-alent in depressed patients and appear to be both apredisposing and a prognostic factor for depres-sion. Comorbid PDs predicted higher rates ofdepression recurrence and a shorter time to recur-rence (Cyranowski et al., 2004). Subjects sufferingfrom PD may lack the required resources tocope with stressful or demanding interpersonalsituations, which in turn may worsen their depres-sive symptomatology.
The aim of this study was to evaluate cross-sectionally the prevalence of PD and of depressivesymptoms in women, according to DSM-IV criteria(American Psychiatric Association, 2000), at threedifferent transitional periods: during student life,after childbirth and during sickness (in breastcancer patients). We hypothesized higher rates ofdepressive symptoms in women suffering from PDcompared with women without PD, as well as moredepressive symptoms during sickness.
Methods
Participants
Clinical data from 568 women (32.3� 14.1,16–81 years) were evaluated from three differentgroups pooled from ongoing studies. The firstgroup consisted of 158 female students (21.2� 2.8,18–41 years) randomly approached and recruitedfrom the Psychology department of the university;134 fully completed the questionnaires. In thesecond group, 456 primiparous women were consec-utively approached, and 314 women (27.6� 4.6,16–44 years) were enrolled while in the hospitalfollowing delivery. The third group consisted of141 women diagnosed with breast cancer withoutmetastasis. Twenty-one questionnaires were notfully completed, and 120 women (56.1� 10.7,33–81 years) were enrolled at the end of the first stageof treatment. The exclusion criteria were metastasis,cancer recurrence, other comorbid cancer or historyof cancer, or impaired cognition. Personality, moodand anxiety states were assessed to identify theeffects of these various risk factors on the level ofemotional distress. Mood and anxiety symptoms wereassessed before and after surgery. Personality wasassessed after surgery but before radiotherapy.
Procedure
All tests were performed for clinical purposes usingroutine techniques; thus, ethical approval was notrequired according to relevant regulations in
234 Enfoux et al.
Copyright © 2013 John Wiley & Sons, Ltd. 7: 233–241 (2013)DOI: 10.1002/pmh

France. The participants were given the full detailsabout the experimental protocol, and they gavetheir written informed consent before the begin-ning of the experiments. This study conforms tothe Code of Ethics of the World Medical Associa-tion (Declaration of Helsinki). Mood symptomsand PDs were assessed in each sample. In the firstgroup, questionnaires were given at the universityby the research team and had to be sent backwithin 1week. In the second group, personalitywas assessed by medical practitioners during themother’s stay in the maternity ward. In the thirdgroup, personality was assessed by medical practi-tioners 3months after enrolment in the initialtreatment phase.
Personality assessment
We assessed personality using the French versionof the Vragenlijst voor Kenmerken van dePersoonlijkheid (VKP-4) or the Questionnaire onPersonality Traits Duijsens, Eurelings-Bontekoe, &Diekstra, 1996; Camus, de Mendonça Lima,Gaillard, Simeone, & Wertheimer, 1997). TheVKP-4 questions provide a uniform approach forassessing PD for both the DSM-IV and ICD-10classification systems. The assessment of PDs ishampered by the difficulty of using currentlyavailable tools (e.g. International Personality Disor-der Examination (IPDE), structured interviews suchas SCID), which are time consuming and/or needtrained interviewers to be properly administered.The VKP is a self-report questionnaire of 197items derived from the IPDE (Loranger et al.,1994), and it requires only 30 to 40min tocomplete. Like the IPDE, the VKP is scored on athree-point rating scale. ‘True; (?); or False’responses are, respectively, rated 2, 1 and 0. Somequestions have a fourth answer possibility, NA(Not applicable). Most of the VKP questions areformulated positively. Some items are negativelyformulated to reduce the risk of repetitiveanswering. The VKP yields dimensional scores aswell as diagnoses. The dimensional score iscalculated by counting the number of criteria
met (True) for each disorder, and it thus containsmore information than just the diagnosis, which isonly given when a minimum number of criteriahave been met.
Depressive symptoms assessment
In the first and third groups, depressive symptom-atology was assessed using the French version ofthe Hospital Anxiety and Depression Scale(HADS) (Zigmond & Snaith, 1983; Razavi,Delvaux, Farvacques, & Robaye, 1990). TheEdinburgh Post-natal Depression Scale (EPDS)(Cox, Holden, & Sagovsky, 1987; Guedeney &Fermanian, 1998) was used in the primiparousgroup, as it is adapted for pregnant women.
The HADS is a 14-item self-questionnaire,rated on a four-point scale (from 0 to 3), and itis designed to assess the levels of anxiety anddepression using two subscales of seven itemseach. The possible scores range from 0 to 21 foranxiety and 0 to 21 for depression. It is a simple,sensitive and specific tool for screening for psychi-atric disorders in an oncology inpatient population(Razavi et al., 1990). For the screening for depres-sion only, a cut-off score of 19 gave 70% sensitiv-ity and 75% specificity. For the screening foradjustment disorders and depression taken together,a cut-off score of 13 gave 75% sensitivity and 75%specificity. Here, we chose a cut-off score of 19 toinclude only women in the depression group.
The EPDS is a 10-item, self-rating scaledesigned to identify post-natal depression. It is asimple, well-accepted assessment tool and is easyto fill in. The mother underlines one of the fourpossible responses that are closest to how she hasbeen feeling during the past week. A cut-off of12.5 is usually recommended, but according tovarious studies, the best cut-off scores range from9.5 to 12.5 (Cox et al., 1987; Murray & Carothers,1990; Harris, Huckle, Thomas, Johns, & Fung,1989), with variable sensibility and specificity. Inour study, we chose a cut-off score of 11.5, whichobtained both good sensitivity (0.73) and highspecificity (0.95) in the French version.
235Depression and personality disorders
Copyright © 2013 John Wiley & Sons, Ltd. 7: 233–241 (2013)DOI: 10.1002/pmh

Data analysis
We performed non-parametric tests (Kruskal–Wallis ANOVA or Mann–Whitney U test) forbetween-group comparisons of the followingvariables: age, graduate level education, meansymptoms of PD and prevalence of depressivesymptoms. Comparison of the prevalence of PD(as determined by the VKP) according to depres-sive status was accomplished using the Chi2 test,or the Fisher test (exact p) when the number ofsubjects was less than five in one cell. An alphalevel of less than 5% was considered to be statisti-cally significant. The statistical analyses wereperformed with the aid of SPSS software 18.0 forWindows (SPSS Inc., Chicago, IL, USA).
Results
Personality disorders
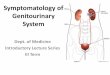
Among the 568 subjects, 6.3% were diagnosed witha PD, with no significant differences (p=0.77) inthe rates between the three groups of participantsas follows: students (6.9%), primiparous women(6.0%) and breast cancer survivors (6.7%). Themost frequent diagnoses were as follows: 15.8%paranoid (95% CI= 12.8–18.9), 15.3% avoidant
(95% CI= 12.3–18.9), 9.5% obsessive–compulsive(95% CI= 7.0–11.9) and 8.5% borderline (95%CI= 6.2–10.7) PDs. These four PDs were found tobe the most prevalent in each of the groups.Other PDs were less prevalent: 3.3% schizoid(95% CI = 1.9–4.8), 2.8% schizotypal (95%CI= 1.5–4.2), 1.6% antisocial (95% CI= 0.6–2.6),1.2% histrionic (95% CI= 0.3–2.1), 1.2% narcis-sistic (95% CI= 0.3–2.1) and 0.4% dependent(95% CI= 0.2–0.6) PD. The three groups werecomparable in terms of their prevalence of PD,except that the students had significantly increasedrates of borderline (14.2%, p=0.02) and avoidantPDs (21.6%, p=0.02) (Figure 1).
Depressive symptoms
We found a high prevalence of depressive symptomsin the whole sample (20.4%, n=116), with no sig-nificant differences (H=2.36, p=0.31) betweenthe students (16.4%), primiparous (22.6%) and on-cology (19.2%) groups. Subjects with depressivesymptoms had significantly lower graduate educa-tional levels (z=2.51, p< 0.02) compared withsubjects with no depressive symptoms (12.5� 0.2vs. 13.0� 0.1). There was no age effect for thewhole sample, although the primiparous women
Figure 1: Prevalence of personality disorders in the whole sample and in each of the groups of students (n=134), primiparouswomen (n=314) and cancer survivors (n= 120). *p=0.02
236 Enfoux et al.
Copyright © 2013 John Wiley & Sons, Ltd. 7: 233–241 (2013)DOI: 10.1002/pmh

with depressive symptoms were significantly(z=2.84, p< 0.005) younger than the women withno depressive symptoms (26.3� 0.5 vs. 28.0� 0.3).
Depressive symptoms and personality disorders
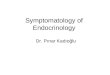
Table 1 and Figure 2 show the prevalence of PDs di-agnosed with the VKP-4 in relation to depressivesymptomatology. We found significantly higherprevalence of PD in the depressed group (12.8%)compared with the non-depressed group (4.7%)(z=�5.5, p< 0.001). Compared with the non-depressed subjects, the depressed subjects had signif-icantly more paranoid (31.0% vs. 11.9%, p< 0.001),borderline (21.6% vs. 5.1%, p< 0.001), avoidant(27.6% vs. 12.2%, p< 0.001), obsessive–compulsive(17.2% vs. 7.5%, p< 0.01), schizotypal (7.8% vs.1.5%, p=0.001), antisocial (5.2% vs. 0.7%,p< 0.01), dependent (7.8% vs. 3.1%, p< 0.05)and histrionic (3.4% vs. 0.7%, p< 0.05) PDs.Differences in narcissistic and schizoid PD were notsignificant.
We calculated the odds ratios (ORs), whichsuggested that borderline (OR= 5.12), schizotypal(OR=5.35) and histrionic (OR= 5.35) PDs wereat least five times more prevalent in females withdepressive symptoms. Avoidant (OR= 2.75), de-pendent (OR= 2.63) and obsessive–compulsive(OR=2.56) PDs were nearly three times moreprevalent. Paranoid (OR= 3.32) PDs were at least
three times more prevalent, and antisocial PDswere (OR= 8.16) eight times more likely to beassociated with depressive symptoms.
Discussion
This study evaluated the prevalence of PD in rela-tion to depressive symptoms in female subjects. Theprevalence rate for PD (6.3%) in our study replicatesthe findings from the literature (Paris, 2010; Huanget al., 2009). The prevalence of paranoid andavoidant PDs is higher than in previous studies. Thiscould be explained, in part, by the use of the VKP,which appears to overestimate the prevalence ofsome PD, particularly paranoid and avoidantPDs (Duijsens, Eurelings-Bontekoe et al., 1996).Our three groups of female participants were ofdifferent life stages and different ages, yet theywere comparable in terms of the prevalenceof PD. Our result suggests that there is not a hugeeffect of age on the courses of PD. An age effect issupported by some studies (Engels, Duijsens,Haringsma, & Van Putten, 2003) but rejected byothers (Stevenson, Datyner, Boyce, & Brodaty,2011; Ames & Molinari, 1994). Only borderlineand avoidant PDs were found to be moreprevalent in the student group. This is concordantwith previous studies (Huang, Ling, Yang, & Dou,2007; Chabrol, Montovany, Chouicha, Callahan,& Mullet, 2001) showing higher rates of
Table 1: Comparison of the prevalence (%� SD [CI]) of personality disorders (PDs) between women with (Depressed;n= 116) or without (Non-depressed; n=452) significant depressive symptoms
Depressed Non-depressed Odds ratio p
Paranoid 31.0� 0.46 [22.5–39.6] 11.9� 0.32 [8.9–14.9] 3.32 [2.05–5.39] 0.001Schizoid 5.2� 0.22 [1.1–9.3] 2.9� 0.17 [1.3–4.4] 1.84 [0.69–4.96] nsSchizotypal 7.8� 0.27 [2.8–12.7] 1.5� 0.12 [0.4–2.7] 5.35 [1.95–14.68] 0.001Antisocial 5.2� 0.22 [1.1–9.3] 0.7� 0.08 [0.0–1.4] 8.16 [2.01–33.16] 0.01Borderline 21.6� 0.41 [14.0–29.1] 5.1� 0.22 [3.1–7.1] 5.12 [2.79–9.43] 0.001Histrionic 3.4� 0.18 [0.1–6.8] 0.7� 0.08 [0.0–1.4] 5.35 [1.18–24.23] 0.05Narcissistic 0.9� 0.09 [0.0–2.6] 1.3� 0.11 [0.3–2.4] 0.65 [0.08–5.42] nsAvoidant 27.6� 0.45 [19.3–35.8] 12.2� 0.33 [9.1–15.2] 2.75 [1.68–4.51] 0.001Dependent 7.8� 0.27 [2.8–12.7] 3.1� 0.17 [1.5–4.7] 2.63 [1.11–6.24] 0.05Obsessive–compulsive 17.2� 0.38 [10.3–24.2] 7.5� 0.26 [5.1–10.0] 2.56 [1.41–4.65] 0.01
237Depression and personality disorders
Copyright © 2013 John Wiley & Sons, Ltd. 7: 233–241 (2013)DOI: 10.1002/pmh

borderline PD in young adults, particularly inwomen compared with men.
Prevalence of depressive symptoms in our sam-ple (20.4%) is slightly higher than rates from epi-demiological studies (Kessler et al., 1994). Thismay be due to a group effect; our sample is com-posed only of women who are at greater risk fordepression. In particular, postpartum is a high-riskperiod for the occurrence of depressive episodes(Teissedre & Chabrol, 2004; Halbreich &Karkun, 2006), as are periods of illness, such asexperienced by our women suffering from breastcancer (Aapro & Cull, 1999). However, depressivesymptoms were equally prevalent among the threegroups. Nevertheless, our estimates of depressionrates are not conclusive because our study is notprospective and compared three different groups.
Our results confirm that most PDs are morefrequent when associated with depressive symp-toms. Cluster C PDs are more than three timesmore likely to be present in women with depres-sive symptoms. There is a strong associationbetween borderline PD and depressive symptom-atology, a frequent result in studies of thecomorbidity between PD and depression (Skodolet al., 1999). However, while previous studieshave found associations between antisocial PD
and depression (Lenzenweger, Lane, Loranger,& Kessler, 2007), we found a significantly greatereffect in our all-female population. Supported byrecent literature, the DSM-V highlights theutility of dimensional approaches to diagnosis.Thus, a recent study (Xia et al., 2011) conductedin women found that neuroticism scores werehigher in women with a Mood Depressive Disorder(MDD) compared with women without MDD.Moreover, there are strongly positive correlationsbetween neuroticism and most PDs (Duijsens &Diekstra, 1996; Saulsman & Page, 2004). Ourresults also suggest that, in comparison withother PDs, paranoid (31.2%), avoidant (27.6%),borderline (21.6%) and obsessive–compulsive(17.2%) PDs are more frequently associatedwith depressive symptoms. These rates are lowerthan the rates found in clinical samples (Skodolet al., 1999), except for those for paranoid PD.These results have often been replicated in recentstudies, showing that borderline, avoidant andparanoid PDs were independently and significantlyassociated with an increased risk for MDD(Reichborn-Kjennerud et al., 2010). The associa-tions measured by ORs were the same as for border-line PD, but they were higher than the ones wefound for paranoid and avoidant PDs and similar
Figure 2: Comparison of the prevalence of personality disorders (PDs) between women with (Depressed; n=116) or without(Non-depressed; n= 452) significant depressive symptoms. *Significant difference: Depressed>Non-depressed
238 Enfoux et al.
Copyright © 2013 John Wiley & Sons, Ltd. 7: 233–241 (2013)DOI: 10.1002/pmh

to those found by Skodol et al. (1999) for borderlineand avoidant PDs. In particular, according to previ-ous studies, subjects with a lifetime (Reichborn-Kjennerud et al., 2010) or a current depressionepisode have significantly more co-occurrences ofavoidant and borderline PDs (Oldham et al.,1995), although they have less obsessive–compulsive and dependent PDs (Skodol et al.,1999). Moreover, individuals with borderline,avoidant, dependent, schizotypal and histrionicPDs or antisocial, borderline, dependent, depressive,schizotypal and histrionic PDs traits had a greaterrisk for depression than individuals without anyPD (Johnson, Cohen, Kasen, & Brook, 2005).
This raises the question of comorbidity or inter-actions between PD and depression. It is oftenquite difficult to disentangle when a diagnosis ofeither type of disorder is sufficient for describingand understanding a patient’s psychopathology orwhen a diagnosis of each type is more informative.Some PDs may contribute to an increased vulner-ability to depression and precede such episodes.On the contrary, depression can precede the PDand foster its development. Common aetiologicalfactors have been hypothesized to underlie thedevelopment of certain PDs (Koenigsberg et al.,1999) and depressive disorders. Another hypothe-sis is that some PDs and mood disorders mayoccupy different points along a common affectivespectrum (Johnson et al., 2005). Some associa-tions between PD and depressive symptoms couldbe attributable, in part, to overlapping diagnosticcriteria.
Limitations
The main limitation of this study is the lack ofhomogeneity of our sample, which included onlywomen in three different subsamples with differ-ent ages/pathologies. The sample is not represen-tative of the general population, as pregnancyand cancer could modify personality and inducedepressive symptoms. However, our sample ismore representative of the female population.
Our study did not show a reduction in theprevalence of PD with increasing age. Thisresult may be partly explained by our cross-sectional design and by the need to include afourth sample of elderly women (more than70–80 years) to assess the effect of increasingage on the prevalence of PD. Indeed, our studyexamined only cross-sectionally the prevalenceof PD and depression; a prospective cohortdesign is more appropriate and can indicatemore clearly the temporal sequence betweenlongitudinal changes in personality traits anddepression or symptoms of depression. However,the originality of our design relies upon thecomparison of female groups at different majorstages of a woman’s life.
The VKP, designed as a self-report question-naire, is most likely more sensitive than a structuredclinical interview. It may overestimate the rates ofPD when compared with the IPDE (Duijsens,Bruinsma, Jansen, Eurelings-Bontekoe, & Diekstra,1996). The VKP tends to diagnose several disordersbecause its diagnostic algorithm cannot prioritizediagnoses. However, the VKP remains a very usefultool because it is simple to use, is a self-reportquestionnaire and appears to be a potentially usefulscreening instrument for PD.
Conclusion
Our findings confirm that there is a greater prev-alence of PD among subjects suffering from signif-icant depressive symptoms, and they show thestability of this association at three differenttransitional periods. Because the presence ofcomorbid personality pathology can complicatethe course and treatment of depression, cliniciansand researchers need to evaluate prominentpersonality traits in any patient suffering from aMDD.
Conflict of interest
I. J. Duijsens has the worldwide copyrights of theVKP questionnaire and sells the VKP on a
239Depression and personality disorders
Copyright © 2013 John Wiley & Sons, Ltd. 7: 233–241 (2013)DOI: 10.1002/pmh

commercial basis. The other authors have notdeclared any conflicts of interest.
Acknowledgements
This work was supported in part by a grantfrom the French Ministry of Health AOINCA/SHS 2005 and by the INCa (InstitutNational du Cancer).
References
Aapro, M., & Cull, A. (1999). Depression in breast cancerpatients: The need for treatment. Annals of Oncology,10, 627–636.
American Psychiatric Association. (2000). Diagnostic andstatistical manual of mental disorders. Washington, DC:American Psychiatric Association.
Ames, A., & Molinari, V. (1994). Prevalence of personalitydisorders in community-living elderly. Journal of GeriatricPsychiatry and Neurology, 7, 189–194.
Camus, V., de Mendonça Lima, C. A., Gaillard, M.,Simeone, I., & Wertheimer, J. (1997). Are personalitydisorders more frequent in early onset geriatric depres-sion? Journal of Affective Disorders, 46, 297–302.
Caspi, A., Sugden, K., Moffitt, T. E., Taylor, A., Craig, I. W.,Harrington, H., McCmay, J., Mill, J., Martin, J.,Braithwaite, A., & Poulton, R. (2003). Influence of lifestress on depression: Moderation by a polymorphism inthe 5-HTT gene. Science, 301, 386–389.
Chabrol, H., Montovany, A., Chouicha, K., Callahan, S., &Mullet, E. (2001). Frequency of borderline personalitydisorder in a sample of French high school students.Canadian Journal of Psychiatry, 46, 847–849.
Cox, J. L., Holden, J. M., & Sagovsky, R. (1987). Detectionof postnatal depression. Development of the 10-itemEdinburgh Postnatal Depression Scale. The British Journalof Psychiatry, 150, 782–786.
Cyranowski, J. M., Frank, E., Winter, E., Rucci, P., Novick, D.,Pilkonis, P., Fagiolini, A., Swartz, H. A., Houck, P., &Kupfer, D. J. (2004). Personality pathology and outcomein recurrently depressed women over 2 years of mainte-nance interpersonal psychotherapy. Psychological Medicine,34, 659–669. DOI:10.1017/S0033291703001661
Duijsens, I. J., & Diekstra, R. F. W. (1996). DSM-III-R andICD-10 personality disorders and their relationship withthe big five dimensions of personality. Personality andIndividual Differences, 21, 119–133.
Duijsens, I. J., Eurelings-Bontekoe, E. H. M., & Diekstra,R. F. W. (1996). The VKP, a self-report instrument
for DSM-III-R and ICD-10 personality disorders:Construction and psychometric properties. Personalityand Individual Differences, 20, 171–182.
Duijsens, I. J., Bruinsma, M., Jansen, S. J. T., Eurelings-Bontekoe, E. H. M., & Diekstra, R. F. W. (1996).Agreement between self-report and semi-structuredinterviewing in the assessment of personality disorders.Personality and Individual Differences, 21, 261–270.
El-Hage, W., Powell, J. F., & Surguladze, S. A. (2009). Vul-nerability to depression: What is the role of stress genesin gene x environment interaction? Psychological Medicine,39, 1407–1411. DOI:10.1017/S0033291709005236
Engels, G. I., Duijsens, I. J., Haringsma, R., & Van Putten, C. M.(2003). Personality disorders in the elderly compared tofour younger age groups: A cross-sectional study ofcommunity residents and mental health patients. Journalof Personality Disorders, 17, 447–459. DOI:10.1521/pedi.17.5.447.22971
Guedeney, N., & Fermanian, J. (1998). Validation study ofthe French version of the Edinburgh Postnatal DepressionScale (EPDS): New results about use and psychometricproperties. European Psychiatry, 13, 83–89.
Halbreich, U., & Karkun, S. (2006). Cross-cultural and socialdiversity of prevalence of post partum depression anddepressive symptoms. Journal of Affective Disorders, 91,97–111. DOI:10.1016/j.jad.2005.12.051
Harris, B., Huckle, P., Thomas, R., Johns, S., & Fung, H.(1989). The use of rating scales to identify post-nataldepression. The British Journal of Psychiatry, 154, 813–817.
Hirschfeld, M. A. (1999). Personality disorders and depres-sion: Comorbidity. Depression and Anxiety, 10, 142–146.
Huang, Y., Kotov, R., De Girolamo, G., Preti, A.,Angermeyer, M., Benjet, C., Demyttenaere, K., De Graaf,R., Gureje, O., Karam, A. N., Lee, S., Lepine, J. P.,Matschinger, H., Posada-Villa, J., Sulinam, S., Vilagut,G., & Kessler, R. C. (2009). DSM-IV personalitydisorders in the WHO world mental health surveys. TheBritish Journal of Psychiatry, 195, 46–53. DOI:10.1192/bjp.bp.108.058552
Huang, X., Ling, H., Yang, B., & Dou, G. (2007). Screeningof personality disorders among Chinese collegestudents by personality diagnostic questionnaire-4+. Jour-nal of Personality Disorders, 21, 448–454. DOI:10.1521/pedi.2007.21.4.448
Iacoviello, B. M., Alloy, L. B., Abramson, L. Y., Whitehouse,W. G., & Hogan, M. E. (2007). The role of cluster B andC personality disturbance in the course of depression: Aprospective study. Journal of Personality Disorders, 21,371–383. DOI:10.1521/pedi.2007.21.4.371
Johnson, J. G., Cohen, P., Kasen, S., Brook, J. S., 2005.Personality disorder traits associated with risk for unipolardepression during middle adulthood. Psychiatry Research,136, 113–1121.
240 Enfoux et al.
Copyright © 2013 John Wiley & Sons, Ltd. 7: 233–241 (2013)DOI: 10.1002/pmh

Joyce, P. R.,McKenzie, J.M., Carter, J. D., Rae, A.M., Luty, S. E.,Frampton, C. M. A., & Mulder, R. T. (2007). Tempera-ment, character and personality disorders as predictors ofresponse to interpersonal psychotherapy and cognitive–behavioural therapy for depression. The British Journal ofPsychiatry, 190, 503–508. DOI:10.1192/bjp.bp.106.024737
Kessler, R. C., McGonagle, K. A., Zhao, S., Nelson, C. B.,Hughes, M., Eshleman, S., Wittchen, H. U., & Kendler,K. S. (1994). Lifetime and 12-month prevalence ofDSM-III-R psychiatric disorders in the United States:Results from the national co-morbidity survey. Archivesof General Psychiatry, 51, 8–19.
Koenigsberg, H. W., Anwunah, I., New, A. S., Mitropoulou,V., Schopick, F., & Siever, L. J. (1999). Relationshipbetween depression and borderline personality disorder.Depression and Anxiety, 10, 158–167.
Kool, S., Schoevers, R., De Maat, S., Van, R., Molenaar, P.,Vinke, A., &Dekker, J. (2005). Efficacy of pharmacotherapyin depressed patients with and without personality disorders:A systematic review and meta-analysis. Journal of AffectiveDisorders, 88, 269–278. DOI:10.1016/j.jad.2005.05.017
Lenzenweger, F. L., Lane, M. C., Loranger, A. W., & Kessler,R. C. (2007). DSM-IV personality disorders in theNational Comorbidity Survey Replication. Biological Psy-chiatry, 62, 553–564. DOI:10.1016/j.biopsych.2006.09.019
Loranger, A. W., Sartorius, N., Andreoli, A., Berger, P.,Buchheim, P., Channabasavanna, S. M., Coid, B., Dahl,A., Diekstra, R. F. W., & Ferguson, B. (1994). The Inter-national Personality Disorder Examination, IPDE. TheWHO/ADAMHA international pilot study of personalitydisorders. Archives of General Psychiatry, 51, 215–224.
Morey, L. C., Shea, M. T., Markowitz, J. C., Stout, R. L.,Hopwood, C. J., Gunderson, J. G., Grilo, C. M.,McGlashan, T. H., Yen, S., Sanislow, C. A., & Skodol,A. E. (2010). State effects of major depression onthe assessment of personality and personality disorder.The American Journal of Psychiatry, 167, 528–535.DOI:10.1176/appi.ajp.2009.09071023
Mulder, R. T. (2002). Personality pathology and treatmentoutcome in major depression: A review. The AmericanJournal of Psychiatry, 159, 359–371.
Murray, L., & Carothers, A. D. (1990). The validation of theEdinburgh Post-natal Depression Scale on a communitysample. The British Journal of Psychiatry, 157, 288–290.
Newton-Howes, G., Tyrer, P., & Johnson, T. (2006). Personal-ity disorder and the outcome of depression: Meta-analysisof published studies. The British Journal of Psychiatry, 188,13–20. DOI:10.1192/bjp.188.1.13
Oldham, J. M., Skodol, A. E., Kellman, H. D., Hyler, S. E.,Doidge, N., Rosnick, L., & Gallaher, P. E. (1995).Comorbidity of axis I and axis II disorders. The AmericanJournal of Psychiatry, 152, 571–578.
Paris, J. (2010). Estimating the prevalence of personalitydisorders in the community. Journal of Personality Disor-ders, 24, 405–411. DOI:10.1521/pedi.2010.24.4.405
Razavi, D., Delvaux, N., Farvacques, C., & Robaye, E.(1990). Screening for adjustment disorders and majordepressive disorders in cancer in-patients. The BritishJournal of Psychiatry, 156, 79–83.
Reichborn-Kjennerud, T., Czajkowski, N., Røysamb, E.,�rstavik, R. E., Neale, M. C., Torgersen, S., & Kendler,K. S. (2010). Major depression and dimensional represen-tations of DSM-IV personality disorders: A population-based twin study. Psychological Medicine, 40, 1475–1484.DOI:10.1017/S0033291709991954
Saulsman, L. M., & Page, A. C. (2004). The five-factormodel and personality disorder empirical literature: Ameta-analytic review. Clinical Psychology Review, 23,1055–1085. DOI:10.1016/j.cpr.2002.09.001
Skodol, A. E., Stout, R. L., McGlashan, T. H., Grilo, C. M.,Gunderson, J. G., Shea, M. T., Morey, L. C., Zanarini, M. C.,Dyck, I. R., & Oldham, J. M. (1999). Co-occurrenceof mood and personality disorders: A report from thecollaborative longitudinal personality disorders study(CLPS). Depression and Anxiety, 10, 175–182.
Stevenson, J., Datyner, A., Boyce, P., & Brodaty, H. (2011).The effect of age on prevalence, type and diagnosis ofpersonality disorder in psychiatric inpatients. InternationalJournal of Geriatric Psychiatry, 26, 981–987. DOI:10.1002/gps.2645
Teissedre, F., & Chabrol, H. (2004). A study of theEdinburgh Postnatal Depression Scale (EPDS) on 859mothers: Detection of mothers at risk for postpartumdepression. Encephale, 30, 376–381.
Xia, J., He, Q., Li, Y., Xie, D., Zhu, S., Chen, J., Shen, Y.,Zhang, N., Wei, Y., Chen, C., Shen, J., Zhang, Y., Gao,C., Li, Y., Ding, J., Shen, W., Wang, Q., Cao, M., Liu,T., Zhang, J., Duan, H., Bao, C., Ma, P., Zhou, C., Luo,Y., Zhang, F., Liu, Y., Li, Y., Jin, G., Zhang, Y., Liang,W., Chen, Y., Zhao, C., Li, H., Chen, Y., Shi, S., Kendler,K. S., Flint, J., & Wang, X. (2011). The relationshipbetween neuroticism, major depressive disorder and co-morbid disorders in Chinese women. Journal of AffectiveDisorders, 135, 100–105. DOI:10.1016/j.jad.2011.06.053
Zigmond, A. S., & Snaith, R. P. (1983). The HospitalAnxiety and Depression Scale. Acta PsychiatricaScandinavica, 67, 361–370.
Address correspondence to: Dr Robert Courtois,Clinique Psychiatrique Universitaire, CHRU deTours, 37044 Tours Cedex 9, France. Email:[email protected]
241Depression and personality disorders
Copyright © 2013 John Wiley & Sons, Ltd. 7: 233–241 (2013)DOI: 10.1002/pmh