Embed Size (px)
Citation preview

Atopic Dermatitis and Ichthyosis
Amy S. Paller, M.D.Walter J. Hamlin Professor and
Chair of Dermatology Professor of Pediatrics
Northwestern University Feinberg School of Medicine
Chicago, Illinois
Atopic Dermatitis = Eczema • Very itchy inflammatory skin disorder that
affects 17% of US children
• Onset in 1st year in 60%; by 5 years in 90%
• Increased prevalence, esp. in industrialized countries; parallels increase in asthma
…and AD can be miserable!
AD persists in >80% of US children to 2nd decade
1-year prevalence of AD in US adults is 7-10%
‐ Not too different from 10.7% prevalence found in US children
Silverberg and Hanifin. JACI 2013;132:1132
Margolis et al. JAMA Dermatol. 2014 Apr 2
Shaw et al. JID 2011;131:57
Percentage of children with mod severe AD
Silverberg, Simpson. Pedi Allergy Immunol. 2013;24:476
with mod-severe AD increases with age, esp. after 3 years (p<.0002)
Silverberg, Simpson. Dermatitis. 2014;25:107
Comorbidities of AD• Asthma• Hay fever/respiratory allergies• Food and digestive allergy
• Itch• Poor sleep efficiency
i
• Keratoconus• Cataracts/ Glaucoma• Dental health problems
• Impetigo/cellulitis/furuncles• Viral warts
i• Insomnia
• Depression• Anxiety• ADD / ADHD• Epilepsy/seizures
• Accidental/traumatic injury
• Eczema herpeticum
• Urinary tract infections• Upper respiratory infections• Pneumonia• Influenza• Recurrent ear infections
What causes AD?
• Genetics: Runs in families with eczema, dry skin, allergic disorders
Proksch E. J Derm Sci 2006; 43:159
• Immune issues in the skin: abnormal reactivity to triggers
• Poor skin barrier: Impairedwater retention; easier ingress of bacteria/certain viruses and allergy triggers
• Formation of tightly stacked outer skin cells
Role of filaggrin in barrier integrity
Precursor to natural moisturizing factor (NMF): breakdown products urocanicacid and pyrrolidonecarboxylic acid – retain water, lower pH, reduce bacteria
Miajlovic et al. JACI 2010;126:1184

• Semi-dominant• Fine scaling• Mild-moderate PPK
with hyperlinear
Filaggrin deficiency: Ichthyosis vulgaris
with hyperlinear palms and soles
Smith et al. Nat Genet. 2006;38:337
Ichthyosis vulgaris• Most prominent and
larger scales on lower extremities: worst in cold, dry weatherFl l• Flexural areas characteristically spared
• Generally improves with age, in summer, and in warm moist environments
F.I.R.S.T. (www.firstskinfoundation.org)
• 1:10 persons (N. European) carry mutation in FLG (profilaggrin): different mutations in different ethnic/racial populations
• Leads to dry skin (water loss) and easier ingress or triggering of immune reactivity by external agents ( i i i i b )
Ichthyosis vulgaris and risk of eczema
(antigens, irritants, microbes)
Ichthyosis vulgaris: Polygonal scaling on legs and hyperlinear palms
Meta-analyses: Strong genetic association between eczema and ichthyosis vulgaris/ FLG mutations
Greatest known risk factor
Ichthyosis vulgaris• 20-30% with FLG mutation have AD• 14-56% with AD have FLG mutation
• Fewer filaggrin repeats correlates with dry skinSandilands et al. J Cell Sci 2009;122:1285
Ginger et al. Arch Derm Res 2005;297:235
Ichthyosis vulgaris and eczema• Higher risk of asthma, hay fever, food and
other allergies if filaggrin mutations and eczema (“atopic march”)
Osawa et al. Allergol Int 2011;60:1

How do we manage atopic dermatitis?
• Section 1. Diagnosis and assessment of atopic dermatitis.
• Section 2. Management and treatment of atopic dermatitis with topical therapies.
• Section 3. Management and treatment with phototherapy d t i t
Guidelines of Care for the Management of Atopic Dermatitis
and systemic agents.
• Section 4. Prevention of disease flares and use of adjunctive therapies and approaches.
JAAD 4-part series, 2014
Standard Therapies for Pediatric Atopic Dermatitis
• Irritant and allergen avoidance• Moisturization a few times daily/ barrier repair• Bathe at least once daily
W d f l t h d t ki– Wonderful way to hydrate skin– Important for parent-baby bonding– Clears dead skin cells– Decreases bacteria– Water softeners make no difference
• Moisturize immediately after bath with good emollient
Standard Therapies for Pediatric Atopic Dermatitis
• Anti-inflammatories as main therapy
• Managing infection
• Sedating antihistamines to help with sleep (child• Sedating antihistamines to help with sleep (child and parents)
• *Education: Chronicity, flare factors hard to find
– Patient understanding is critical for compliance
Improve the barrier
- Avoid irritants and potential allergic triggers
- Bathing to hydrate
Moisturizing several times daily- Moisturizing several times daily, esp. after bath
- Opportunity to deliver: alter pH, ceramides, natural moisturizing factors/ missing proteins
Can prophylactic barrier repair prevent AD and sensitization
Simpson et al. JACI 2014;134:818

Barrier therapy to decrease AD risk• Randomized controlled trial (US and UK) in
infants at high risk for AD (1o family with atopy)• Intervention arm: Full-body emollient therapy at
least once per day starting within 3 weeks of birth; Control arm: No emollients
• Cream formulation (67%)>sunflower oil (23%)>ointment ; 85% used at least 5x/wk
• Reduced AD incidence of AD by 50% (relative risk, 0.50; 95% CI, 0.28-0.9; p=0.017)
Simpson et al. JACI 2014;134:818
Horimukai et al. JACI 2014;134:824
• 32% fewer infants with AD in active treatment group (p = 0.012); had better skin hydration
Anti-inflammatory Therapy• Anti-inflammatory medications are key for
suppressing inflammation and pruritus• Topical steroids have been mainstay
• In general, ointments are more potent, better emollients, and with fewer additives than creams
• Patient and parental preference should be heeded
Anti-inflammatory Therapy
• Various successful techniques of steroid use– Discontinuation leads to flare– Burst therapy vs. maintenance– Dial down to lower strength steroid or
calcineurin inhibitors- Proactive therapy
• Be familiar with strengths of topical steroids– Superpotent steroids are inappropriate – Potent steroids for older children at
recalcitrant sites, intermittent as needed– Do not use halogenated steroids on face, groin,
intertriginous areas
• Salicylic acid (2-6%) with topical steroid (e.g., triamcinolone) and can put in emollient base (Aquaphor); sometimes add tar as anti-inflammatory
Recalcitrant lichenified dermatitis: Compounded steroids
- Compounding adds expense; 1 lb.- Monitor carefully – more side effects
and systemic absorption- Taper dosing and substitute as patient
improves
Limitations of Topical Corticosteroid Therapy
• Side effects– Unusual unless inappropriate use– Atrophy/ striae– Potential for systemic absorption
• Efficacy– Tachyphylaxis: Resistance and
requirement for stronger steroids– Limited by steroid phobia: 36% are non-
adherent to treatment because of phobia– Latest issue: Phobia about “steroid addiction”
“Steroid Addiction”?
• Growing media attention and public concern
• Uncommon side effect: occurs after TCS withdrawal (esp 2-3 wks after), usually after use for AD
• Particularly rare in children (7% <18 y/o; 0.3% <3 y/o)
• Follows prolonged, inappropriate and frequent use
Systematic review of ~300 articles: Hajar et al. JAAD 2015;72:541

What is “steroid addiction”?- 81% are women; 97% use on face (can affect
genitalia); 86% use mid to high-potency steroids - 92% showed persistent erythema, often
with sharp demarcation; may spare nose and ears (“headlight sign”); sometimes papules/nodules
Hajar et al. JAAD 2015;72:541
p p
- Frequent burning/stinging (65%), itch
- Recognize, provide supportive therapy
- Should not discourage from appropriate use of TCS for AD
Compliance is a major issue Microprocessor in cap for stealth monitoring32% compliance to AD regimen during 8 weeks; most compliant before visits
Krejci-Manwaring et al. JAAD 2007;56:211
Explore reasons for noncompliance and address them creatively (steroid phobia; timing; vehicle)Heed patient and parental preferenceConsider shorter duration before 1st followup
Written action plans
Shah et al. Cutis 2013;91:105
• Calcineurin inhibitors and “medical devices” as “steroid-sparing agents”
• Topical calcineurin inhibitors (tacrolimus ointment and pimecrolimus cream) do not lead to
Other anti-inflammatories?
ointment and pimecrolimus cream) do not lead to skin thinning or eye risks: safe for face
– Off-label use for 0.1% tacrolimus ointment
– Off-label use for <2 years of age
• Topical calcineurin inhibitors may allow repair of steroid-induced side effects/ barrier issues
Proactive maintenance therapy
173 9
200
• Regular use to clear/almost clear areas– Decreased potential risk, increased compliance
• Intermittent fluticasone cream to maintain
• Intermittent tacrolimus ointment Hanifin. BJD 2002;147:528; Schmitt t al. BJD 2011;164:415
• 3x/wk once clear-almost clearBreneman JAAD 2008;58:990173.9
106.7
0
50
100
150 p = 0.0008
Flar
e-fr
ee d
ays
(Mea
n)
TCL (n=67) Vehicle (n=36)
• 2x/wk: indication in Europe
• 1x/wk as good as 3x/wk
• Fluticasone slightly more effective
Breneman. JAAD 2008;58:990 Paller. Pediatrics 2008;122:e1210
Reitamo and Allsopp. J Derm Treat 2010;21:34 Thaci et al. JEADV 2010;24:1040
Schmitt al. BJD 2011;164:415
Chung. BJD 2013;168:908
• Risk of non-melanoma skin cancer decreased with TCI use and potency
No signal to date in adults or children
What about the Black Box warning?
• Increased lymphoma risk with AD, esp. severe – No correlation with use of TCIs
Margolis. JAMA Derm 2015 Feb 18; Arellano. JACI 2009;127:808; Arellano. JID 2007;127:808; Siegfried. Am J Clin Derm 2013;14:163
• 10-year study of tacrolimus in 8000 children worldwide, 6 year U.S. study in ~7500 infants and toddlers and PEER study of pimecrolimus (6000) as well as FDA’s adverse event reporting system
– No increased risk of skin cancer, lymphoma through 2014 data
Consider contact allergic reactionsEspecially with face or hand dermatitis
• Up to 22% with AD react to non-nickel allergens – Emollient ingredient 50% (esp. avena extract, wheat
protein, calendula, lanolin)– Topical antiseptic (chlorhexidine), cleanser– Topical steroid
• Extensive dermatitis may reflect airborne allergens (exposed areas) or systematized reactions
Reaction to baby wipes (broponol preservative, fragrance))
• 19% react to balsam of Peru, 20% to fragrance mix
Courtesy, Dr. S. Jacobs

• 80-90% of patients with AD harbor S. aureus• Decreased innate immune responses
- Poor barrier (filaggrin down, proteases up)- Decreased antimicrobial peptides
• Microbiome studies: reduction in normal flora with flares and increased S. aureus
What about Infection? Staph worsens AD
- What is role of normal flora?- Factors secreted by S. epi kill S. aureus;
nonpathogenic bacteria reduce inflammation in NC/NgA mice
• MRSA is a growing concern
Volz et al. JID 2014;134:96
Bacterial swabs from rims, nozzles, container content; preserved and unpreserved ointments - 53% of containers were contaminated‐ 25% with S. aureus
‐ Nasal carriage of same S. aureus strain in 65% of parents
‐ Pets can carry same microbiota incl MRSA
Carr and Cork, ISAD 2008
Chiu et al. Arch Derm 2010;146:748; Bonness et al. J Clin Microbiol 2008;46:456
Reducing environmental S. aureus
‐ Pets can carry same microbiota, incl MRSA
Recommendations:– Keep open moisturizers in refrigerator– Pumps or pour bottles rather than jars– Avoid direct contact with hands; decant– Avoid sharing personal hygiene items– Consider decolonizing household members, incl pets
Misic et al. Presented at SID, 2014
• Bleach baths (sodium hypochlorite) .005% at least 2x weekly (1/2 cup per full tub; 4cc tsp/gallon; 1 cc/L)
• Moderate to severe AD with history of infection
How can we decrease S. aureus levels?Can we decrease the severity of AD?
Huang et al. Pediatrics 2009;123:e808; Huang et al. Arch Derm 2011;147:246
-25
-20
-15
-10
-5
00 1 2 3
Time
Cha
nge
in %
BSA
(-)
Placebo Treatment
-18-16-14-12-10-8-6-4-20
0 1 2 3
Time
Cha
nge
in E
ASI
scor
e
PlaceboTreatment
p=0.004 p=0.004
Eczema severity Body surface area
“Exposed” sites: Head and NeckMean change: Baseline to 1 month: p=.32Mean change: Baseline to 3 months: p= 62
Baths or the mupirocin combo?“Bath Submerged” sites: Limbs, Trunk
Mean change: Baseline to 1 month: p=.03Mean change: Baseline to 3 months: p=.0005
Mean change: Baseline to 3 months: p=.62
• Did not fully clear S. aureus– Maintenance use up to daily (if severe) now
standard of care; don’t need for mild, <3 mos.– Marketing of new bleach-based antiseptics
Huang et al. Pediatrics 2009;123:e808; Huang et al. Arch Derm 2011;147:246
Na hypochlorite 0.006% cleanser for showers
• 12 wk open-label trial of 18 children with moderate to severe AD
• Positive lesional cultures for S. aureus• At least 3x/wk with shower; no other changes• Significant reduction in IGA by 2 wks (p=.01) and
SA 1 ( 0 00 )BSA by 1 month (p=0.005)
Ryan et al. Pediatr Derm 2013;30:308
Day 0 Day 11
Week 8Week 10
• Is there more than anti-bacterial action?• Reversibly inhibits NF-κB signaling in cultured KCs
Sodium hypochlorite may be anti-inflammatory
• Reduces disease severity d l i i ith
Leung et al. JCI 2013;123:5361
and ulcers in mice with acute radiation dermatitis
• In aged mice, enhanced epidermal thickness and proliferation
H2O
HOCl
Not improving on topicals?
Some pearls to consider
Have you tried? Wet wraps• Traditional: wrap with wet gauze after bathing
and topical medication or moisturizer
• Modified: Damp PJ’s (cotton long underwear-Dabade et al. JAAD 10/4/11 Epub
like) and socks; top with dry PJ’s or sweat suit and socks to avoid chilling
• Modify for hand dermatitis by wet cotton gloves topped with vinyl glove
Wet wrap management
• Decreases pruritus and discomfort
• Best applied for severely affected infants and toddlers (compliance)and toddlers (compliance)
• May increase absorption of topically applied medication
Have you considered Allergy?
• Dietary manipulation controversial
• Consider allergy testing, challenge testing and dietary avoidance in infants or toddlers with ysevere, resistant AD
– Referral to an allergist with experience
– Maintain good nutrition (risk kwashiorkor, rickets)
• Rarely necessary• Virtually all children improve in a few days…
maintenance is tricky
O t it t t h ti t d t b t
Hospitalization to “cool down”
• Opportunity to teach patient and parents about proper use of medication
• Opportunity for consultation (beyond derm)• Gives family a “break”
• Balance with risk of exposure/ acquisition of resistant microorganisms
Narrow band UVB• Retrospective review of 50 children with severe
AD with > 10 exposures– Complete clearance in 40%; good
improvement in 23%; moderate in 26%– Median length of remission 3 months
Clayton et al. Clin Exp Derm 2007;32:28
• Problems:– Requires cooperation– Can’t start when too inflamed– Potential risk of skin cancer and premature
aging– Busy schedules if school-aged (Home nUVB)
y p ;

• Is the quality of life for the patient and family impacted enough to justify?
• Weighing risks and benefits with family
Systemic Immunosuppressants
g g y
• Families need to be advised about risks (infections, neoplasia)
• No comparative trials or detailed treatment guidelines, esp for use in children
• Cyclosporine (short-term)• Methotrexate• Mycophenolate mofetil• Azathioprine
– 1-2 years max on immunosuppressant
Systemic Immunosuppressants
y pp– Side effects are unusual
• Corticosteroids– Typically avoided because of effects of
continued use– Rebound is major problem: slow taper
• Continue “rotational” topicals
What’s on the horizon?
– AN2728: Unique boron-based anti-inflammatory• Increases cAMP
Topical Therapy in Trials:Phosphodiesterase 4 inhibition
Reduces inflammatory cytokines, incl. IL-31
Well tolerated across 16 completed clinical studies
No clinically important safety signals; most AEs mild (esp. application site reactions) and considered unlikely to be related to study drug
cytokines, incl. IL 31
Atopic ExperienceThree phase 2 studies completed in mild-moderate AD: 2 in adolescents
- Double-blind, randomized, dose-ranging ().5% vs 2%) in 86 adolescents with 35% BSA: twice daily for 28 d
Confidential
daily for 28 d- Open label pK study at 2% dosing in 23
adolescents (10-35% BSA): twice daily for 4 wks
Safety and pK study in children as young as 2 years: No safety signals; most AE’s mild (application site); no blood levels
>70% Clear or Almost Clear (IGA) after 4 >70% Clear or Almost Clear (IGA) after 4 Wks of twice daily therapyWks of twice daily therapy
ISGA Scale:0 Clear1 Almost Clear2 Mild
Proportion of Subjects Achieving Clear or Almost Clear on ISGA
2 Mild3 Moderate4 Severe
Confidential AN2728-AD-203
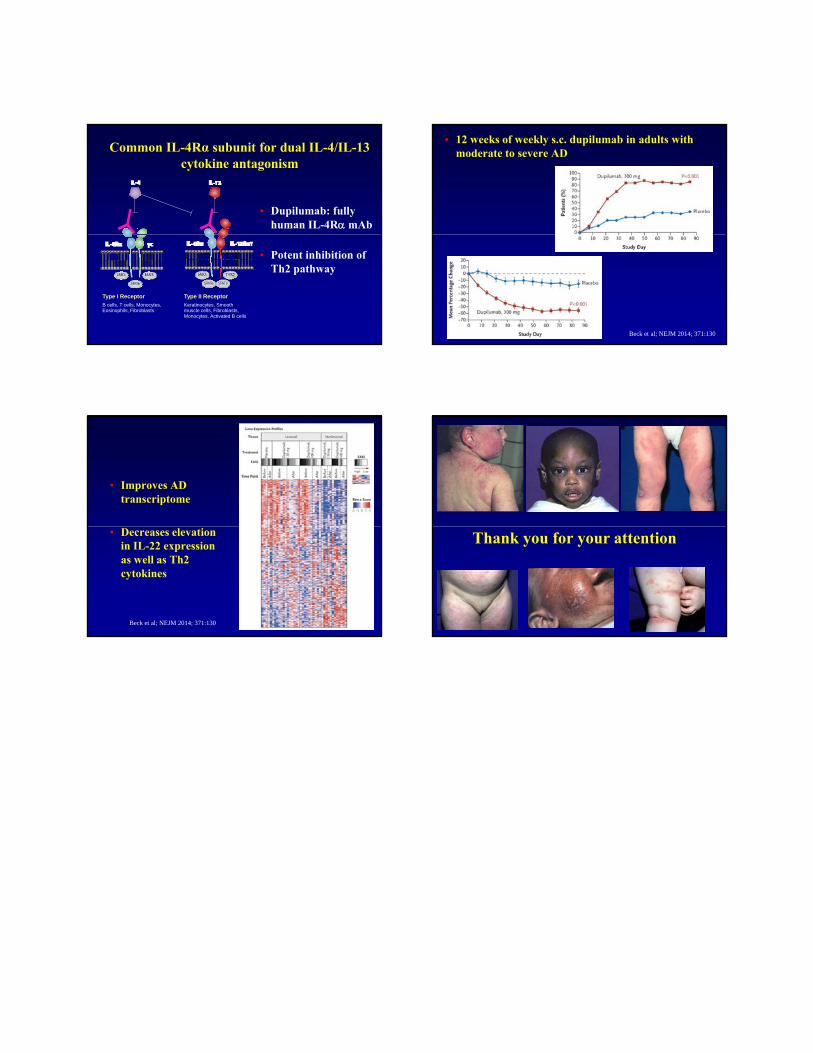
Common IL-4Rα subunit for dual IL-4/IL-13 cytokine antagonism
• Dupilumab: fully human IL-4Rα mAb
Type I ReceptorB cells, T cells, Monocytes, Eosinophils, Fibroblasts
Type II ReceptorKeratinocytes, Smooth muscle cells, Fibroblasts, Monocytes, Activated B cells
• Potent inhibition of Th2 pathway
• 12 weeks of weekly s.c. dupilumab in adults with moderate to severe AD
Beck et al; NEJM 2014; 371:130
• Improves AD transcriptome
Beck et al; NEJM 2014; 371:130
• Decreases elevation in IL-22 expression as well as Th2 cytokines
Thank you for your attention





























