Embed Size (px)
Citation preview

1
Community Reaction to Persons with HIV/AIDS and their Parents in Thailand
Mark VanLandingham, Ph.D. Tulane University
School of Public Health and Tropical Medicine 1440 Canal Street, Suite 2200
New Orleans, LA 70112
Wassana Im-em, Ph.D. Institute for Population and Social Research
Mahidol University Salaya, Nakorn Pathom 73170
Thailand
Chanpen Saengtienchai, M.A. University of Michigan
Population Studies Center Ann Arbor, MI 48106
PSC Research Report 05-577
Acknowledgement: The research described in this paper is part of a larger ongoing study of the impacts of the AIDS epidemic in Thailand, and is supported by grants from the National Institutes of Aging (grants AG18648 and AG15983). Laura Andrews provided expert research assistance on the qualitative data analysis. Charlotte Colvin and Fumihiko Yokota provided helpful comments on an earlier draft. John Knodel and Jiraporn Kespichayawattana have provided valuable input and assistance at all stages of the research upon which this paper is based. An earlier version of this paper was presented at the Population Association of America meetings, May 9, 2002, in Atlanta, Ga.
2
Abstract We systematically examine community reaction to persons with HIV/AIDS (PHAs) and their families in Thailand from multiple perspectives using several types of data. We explore these community reactions during the time of the PHAs’ illness and after their deaths. Quantitative data sources include a survey of young adult PHAs (n=425); a survey of parents who suffered the death of an adult child to AIDS (n=394 cases); a KAP study of AIDS that includes both older and young adults (n=1174); and quantitative data from local key informants about cases in their area (n=286 cases). This extensive quantitative information is supplemented with several sources of qualitative data. Data were collected during 1999 – 2001 from a wide range of settings throughout Thailand. We find community reaction to PHAs and their families to vary by features of the case, social group, and type of observer, but overall these reactions are much more positive than is widely assumed. The overwhelming majority of key informants’ assessments and of PHA parents’ reports indicate either a generally positive community response or a neutral one. Results from our sample of PHAs, who are recruited from PHA support groups, are more mixed. For those who were treated poorly, it is suggested by at least some of our data sources that living in the city, living in an area without an NGO working on AIDS, being described as having problematic character, or being at either extreme of the socioeconomic spectrum may elevate the risk of experiencing negative community reaction. We conclude that much existing research on community reaction to AIDS neglects both a rich body of social theory on stigma and a strong tradition of population-based empirical research. Much existing research also fails to adequately distinguish between key aspects of the social settings where most AIDS cases occur and the social settings where most of the stereotypes surrounding AIDS-related stigma have originated. Sociologists have much to offer to further investigations of this critically important dimension of the AIDS epidemic.
3
Introduction
Stigma and discrimination against persons with HIV and AIDS (PHAs) are unfortunate and in some cases tragic consequences of infection that compound the suffering of some PHAs and their families. Whether such consequences are rare or common, they should serve to draw attention and response to the special burdens such families face. But from a sociological and public health point of view, the dimensions, degree, extent, and cofactors of these phenomena matter profoundly. Sociologically, it is important to understand which factors are causally linked with stigma so that we can better understand how stigma interacts with other social processes and anticipate its antecedents and consequences. Stigma is very unlikely to occur independently of other social phenomena. From a public health point of view, it is important to know which social groups are most likely to experience stigma and its adverse consequences so that limited public resources can be targeted in the most effective way possible.
Unfortunately, the empirical literature on stigma is not well developed and this deficiency leads to widespread assumptions about its extent and distribution, the validity of which are unknown. Systematic investigations of variations across time, place, and social position are rare. In their place, sweeping generalizations unsupported by empirical evidence are issued even by reputable organizations (e.g., UNAIDS 2000), which profoundly limit our ability to target our efforts accurately.
The lack of systematic research on stigma results in part from the difficulties of obtaining data on a potentially sensitive issue from a reasonably unbiased and sufficiently large sample to warrant meaningful conclusions. Some families may be reluctant to disclose their situation for fear of being stigmatized. Other families who are willing to discuss their situation may be much more vocal and/or otherwise dissimilar from typical families, which make them poor representatives of the general situation. Some organizations, such as ministries of health, may have a vested interest in portraying a social situation as more supportive than it is; others, such as nongovernment organizations who wish to publicize the plight of affected individuals and subpopulations, have an interest in portraying the situation as more negative than it really is.
Our study of how AIDS affects older persons in Thailand provides an unusual opportunity to explore the extent, distribution, manifestation, and consequences of stigma from a variety of perspectives, including those of the PHAs themselves, parents who live with and care for them, health workers who treat them, and local volunteers who share a community with them. We also analyze data from a general survey of AIDS knowledge and attitudes that taps into more general perspectives of this population on AIDS and the persons who are stricken by it. Our data are collected from a wide range of communities and include a substantial number of cases. They incorporate observations from those who are affected by stigma as well as from local observers who are not, but who are in a good position to assess reactions towards PHAs and their families within their communities. Background
Perspectives on stigma Goffman (1964) provides an excellent entry point into the concept of stigma. Describing the term
as “an attribute that is deeply discrediting,” he introduces several key dimensions of this complicated phenomenon that have been further developed by subsequent scholars. First, stigmatized and normal are not discrete categories but rather ends of a continuum, and by implication, much of actual experience lies in the gray areas in between. Such a perspective belies the view of those who see some communities as harboring stigma but others not. The empirical reality, if Goffman is correct, is likely to be much more complicated. Second, Goffman’s concepts of discredited and discreditable persons also initiated a theoretical distinction between actual experienced stigma (by a “discredited” person) and anticipated stigma (by a “discreditable” person). Subsequent authors have further developed this concept into a productive distinction between felt (or anticipated) stigma and enacted stigma (e.g., Jacoby 1994; Malcolm et al. 1998), and how perceptions and experiences of stigma may vary over the course of the
4
illness (Brashers et al. 1998; Alonzo et al. 1995). While both felt and enacted stigma may lead to negative consequences, some persons suffering from HIV may anticipate negative reactions from their communities and therefore have a more negative interpretation of community reaction than members of the community may have. Thus, in order to gain a full appreciation of this complicated phenomenon, it is important to be able to contrast the views of PHAs and their families with the views of others, and to explore how stigma towards the PHA and the family may change over the course of the illness. Our data allow for such comparisons.
A third distinction to result from Goffman’s seminal work is expressive (symbolic) versus evaluative (instrumental) reactions regarding stigma (Herek and Capitanio 1998). Observers may feel negatively based on prejudice, e.g., regarding homosexuals; but may act only on instrumental criteria, e.g., fear of infection. Indeed, in the U.S., Sowell et al. (1997) find that stigma encompasses both dimensions for various groups, but that symbolic stigma towards PHAs is much more common than instrumental stigma.
Mechanic (1995) has highlighted the importance of the social and cultural context for how stigma manifests itself, and Link and Phelan (2001) have recently emphasized the important links among stigma, power, and discrimination. Indeed, we anticipate that the relative levels of symbolic and instrumental stigma should be quite different in Thailand compared to the U.S., since the Thai epidemic is not so closely associated with socially stigmatized behaviors as is the U.S. epidemic. Stigma, especially symbolic stigma, towards PHAs in the U.S. is likely to be driven by negative feelings about male homosexual behavior and injecting drug use. These issues are not as relevant in Thailand since most infections have occurred via behaviors that are less or not-at-all socially problematic. Related to this, less powerful groups or individuals may be more vulnerable to stigma and its consequences than the more powerful. Many authors have asserted that in developing countries stigma and its consequences affect women much more than men (e.g., De Bruyn 1992; Warwick et al. 1998; Nyblade et al. 2003). Unfortunately, empirical evidence to support this contention is often omitted, anecdotal, based upon small samples, and/or produced by women’s advocacy groups. Given this lack of adequate empirical data, our contention is that not enough is known to predict interactions between gender and AIDS-related social stigma; rather, we anticipate that other factors will have more explanatory power. Moreover, the relative status of women compared to men in Thailand is better than in many other developing countries (Keyes 1984; Keyes 1989; Knodel 1997). Potential impacts of stigma
Stigma could have a variety of potential impacts on persons, families, and societies affected by AIDS. Incidents of stigma and AIDS discrimination have been found to adversely affect the life satisfaction of PHAs in the U.S. (Heckman et al. 1997). In Thailand, anecdotal evidence suggests that stigma towards a PHA may delay treatment seeking, and reduce access to care and other assistance programs (Buzra 2001). Stigma and discrimination could affect the parents and other members of the PHA household through isolation, by creating or exacerbating intrahousehold conflict and anxiety, or through courtesy stigma – a sort of "guilt by association" (Mullan 1998; Paul 2001; Songwathana 2001; Stein 1997; Palloni and Lee 1992; Goffman 1964). Stigma could potentially adversely affect public health efforts to stem the spread of the virus if it reduces incentives for testing and/or prevents open discussion of the disease (Takahashi et al. 1999). On the bright side, where AIDS related discrimination and stigma do occur, a review by Brown et al. (2003) concludes that the available evidence suggests that they can be reduced by interventions that include information, counseling, and coping skills acquisition. However, a common shortcoming of the reviewed studies that is noted in the Brown et al. (2003) report is that both the definitions and measures of stigma are typically vague. A second generalization to be made regarding the empirical research on this topic is that existing studies often focus more on the potential and/or extreme impacts of stigma and discrimination rather than the distribution of impacts (e.g., see Parker and Aggleton 2002). Much remains to be learned about the dimensions, distribution, and cofactors of this complicated social phenomenon.
5
AIDS in Thailand
Thailand currently faces a moderately severe AIDS epidemic. Prevalence levels are much higher than those found in the U.S. and western Europe, but much lower than those found in the hardest hit African countries, such as Botswana and Malawi. By the early 1990s HIV had established itself firmly within the population of sex workers and the men who patronize them (Brown et al. 1994). Participation in commercial sex was until very recently generally considered to be a normal part of growing up for many young men; very few Thais would consider the behavior to be morally problematic for unmarried men (VanLandingham et al. 1998; MacQueen et al. 1996; Im-em 1999; Maticka-Tyndale et al.1997).
Both the providers and purchasers of sex services are concentrated in the late adolescent and young adult ages. Reported AIDS cases are heavily concentrated among 20-39 year olds, accounting for almost four-fifths of all cases through 1998 (Thailand Ministry of Public Health web site 1999). The fact that -- until very recently -- a large number of Thai men engaged in commercial sex with a relatively small number of female sex workers is reflected in the substantially greater number of reported AIDS cases among males than among females, since current cases roughly reflect incidence levels approximately 5-10 years ago. AIDS is now spreading in the population of married Thai women, many of whom have become infected due to their husbands’ prior contact with sex workers (World Bank 2000). The sex ratio of infection (male/female) is expected to decline to 1.6 by 2010 as more women become infected over the next decade (Thai Working Group on HIV/AIDS Projection 2001).
Infection rates vary widely by region, and are highest in the northern part of the country. HIV prevalence rates among pregnant women range from over 10% in some northern provinces to less than 1% in some central, northeastern, and southern provinces. Military recruit data also indicate much higher levels among soldiers in the north (Mason et al. 1995).
Cumulatively, by the end of 2001 approximately 1 million cases of HIV infection or AIDS is estimated to have occurred within a Thai population of about 64 million (Thai Working Group on HIV/AIDS Projection 2001). While exact numbers and projection trends are subject to contention, it is generally agreed that incidence has peaked and will continue to decline for the foreseeable future. This is due in large part to the success of Thailand’s efforts to slow the spread of HIV by encouraging brothel owners to implement a 100% condom policy with clients (Chamratrithirong et al. 1998), and by aggressive treatment of other sexually transmitted diseases that facilitate the spread of HIV (Hanenberg et al. 1994). Increasing fears among young men about the dangers of commercial sex patronage has also undoubtedly played a major role (VanLandingham and Trujillo 2002; UNAIDS 1998).
We are aware of no large or medium scale systematic empirical investigations of stigma in Thailand. Journalistic and academic accounts rely primarily on case studies and non-systematic samples and analyses. Such reports highlight and emphasize instances of negative community reaction (e.g., Assavanonda 2001; Kornsirilak 2001; Songwathana and Manderson 2001) and give little attention to issues of generalizability and variability, although Buzra (2001) notes that positive community reactions to AIDS afflicted families sometimes occur, and Songwathana and Manderson (2001) mention some mitigating cultural features.
This sparseness of systematic research on stigma in Thailand is unfortunate, since the country has excellent data on epidemiological trends and differentials, and has a history of documented success in its public health campaigns against the epidemic. The Thai situation, while unique in many ways, has much in common with many of the other medium to high prevalence countries of the developing world. The epidemic is spread primarily by behaviors that are quite normative; rapid decline and death usually occur soon after the onset of symptoms (World Bank 2000); intensive care giving is provided to PHAs by their families, especially their parents (Knodel et al. 2001; Kespichayawattana and VanLandingham 2002), who live in tight knit communities in close proximity to other families, and where information travels quickly and easily; and many Thais know individuals who are suffering from or who have died from AIDS (Im-em et al. 2002). In contrast, one could scarcely imagine a more different scenario than the U.S., the country that provides the setting for the much of the research and advocacy, as well as many of the existing stereotypes, on AIDS-related stigma.

6
Data and Methods
Key features of our data and procedures are briefly described here; more details are provided in the appendix. In part to protect against a wide range of potential biases that could result from any one approach, we chose to pursue our study of stigma using information from a variety of perspectives: the parents of PHAs; key informants, who were local level health professionals living and working in the subdistricts we studied; the general population of young and older age adults as participants in our KAP study of AIDS; PHAs themselves; and village (or community) health volunteers (VHVs), who live and work in our communities of interest. Our five surveys are supplemented by several sources and types of qualitative data. We purposely select a wide range of settings for our data collection: Urban and rural areas of Chiang Mai, Chiang Rai, and Lampang provinces in the upper-north, where the HIV prevalence levels are high relative to the rest of the country and the epidemic is of longest duration; Rayong and Trat on the southeastern seaboard, where prevalence levels have recently also become high; Petchburi and Prachuap in the central part of the country, where prevalence levels are moderate; Khon Kaen and Ubon in the northeast, where prevalence levels have remained low; Phichit in the lower north, also with low prevalence rates; Phuket in the south, with moderate levels; and Bangkok, with moderate levels relative to the rest of the country. See Table 1 for an overview of data sources.
Our analytical approach is to first show the range and distribution of community reaction to PHAs and their families. Second, we show the variability (or consistency) by place, by perspective, and over time, presenting data on specific reactions to individual families and broader community reactions to PHAs and their families generally. Third, we explore a number of factors that may explain variability where we find it. Finally, we discuss some of the consequences of community reaction and stigma. Results
Level of awareness and interest about AIDS among Thai adults
Thai adults are generally quite familiar with and interested in the topic of AIDS. Table 2 shows that awareness is nearly universal for both young adults and older Thais. Among young adults, the proportion expressing interest in the topic approaches 90%, with over a third reporting ever attending a lecture, ever having been tested for the virus, and worrying at least some about contracting it. Over two thirds of each age group report ever having known a PHA. Almost everyone in the sample understood the most prominent means of transmission, i.e., unprotected sexual relations, while substantial minorities seem overly concerned about the risks of casual contact. For example, over a quarter of young adults worry unnecessarily about the chances of contracting the virus through living or working near a PHA, sharing a meal with a PHA, sharing a household with a PHA, sharing a glass with a PHA, or eating a meal prepared by a PHA – the proportion answering correctly is even less for the older respondents. So, while overall awareness of AIDS is extremely high among Thai young and older adults, undue concern about the risks of casual contact with PHAs present at least the potential for negative community reaction towards PHAs living in close proximity to their neighbors. Indeed, most of the instances of negative community reaction reported in our in-depth interviews with older parents of PHAs and our focus group discussions with community health providers were related to neighbors’ fears of contagion through casual contact.
Reactions to PHAs and their families are explored more directly with community level data in Table 3. The top half of the table presents the distribution of community reactions as assessed by our key informants (KIs), who are local public health professionals working (and in most cases living) in the communities they report on. Just over seventy percent of the KIs report that most people in their communities are neutral towards PHAs and their families, i.e., neither positive nor negative. Altogether, over 4/5 of the KIs assess the overall reaction in their communities to be either neutral or positive, with only 10% characterizing the general community reaction as negative (i.e., avoiding contact with or criticizing the family). Differences in the distributions between urban and rural areas; between areas with epidemics of less than five years duration and those with longer durations; and between areas with low
7
prevalence and those with medium prevalence do not reach statistical significance. This is likely due to the small number of sites included in the study, as some of the comparisons are highly suggestive. KIs living in urban or peri-urban areas are much more likely to report a general reaction of avoidance to AIDS families – and much less likely to report general sympathetic reactions -- than are KIs in rural areas. In none of the areas with recent epidemics (less than five years) was the general reaction reported to be sympathetic, but this assessment was made by eleven percent of KIs from those areas with longer experience with the epidemic. Local communities in the provinces with the lowest levels of prevalence were judged by more KIs to have avoidance reactions than were communities in the provinces with more moderate prevalence.
Such a time trend towards more positive reaction is also suggested in the lower part of the top half of this table, which presents distributions of the KIs' assessments of trends in their communities. Eighty seven percent of the KIs judged their communities as becoming more tolerant to PHAs and their families over time; none saw a hardening of reactions over time. This view was essentially universal in the focus group discussions involving these types of community health officials as well.
R1: Before, people would stay away from the patients. Even the officials were afraid and didn't want to be near the patients. R2: People are now more educated… They know that they will not be infected when sitting next to the patients… R1: They now have more understanding… And it's also because these patients are now their relatives or their loved ones [Community health officials focus group discussion, Chiang Rai]. The bottom half of Table 3 also assesses general community reaction from a local observer's
viewpoint, but in this case it is the village health volunteer (VHV) who provides the assessment. Such volunteers serve in a quasi-official role as they advise the households under their jurisdiction on a wide range of issues. Once again, the overwhelming response is that community reaction towards households with PHAs is not in fact driven by the fact that a household member is infected - 82% feel that community reaction to those households is no different than it was before the family suffered this calamity. Ninety percent report that at least some residents will feel sympathy towards the AIDS household, and over three quarters report that at least some in the community will offer help. These positive assessments do not appear to be an attempt to deny the existence of negative community reaction, as about half report at least some negative reaction, disgust, and avoidance by some in the community. Two thirds report at least some gossip about these households. As is the case for the health officials, the vast majority of VHVs (84%) assess the trajectory of community response in their areas to be in a more supportive direction.
Such general assessments of community reaction may miss variation among how particular cases are treated where such variation exists. Thus in our next table we turn to the assessments of our key informants of community reaction towards specific families affected by AIDS. Table 4 provides an assessment from our local health professionals of how open the family was to the fact that a member had AIDS; how they were treated by the community during the illness; and how they were treated by the community after the death of the PHA. Among the 286 AIDS families for which we have detailed information, 57% were generally open to the community about the fact that a household member was suffering from HIV or AIDS. About a quarter were open to some, and almost a fifth were not open at all. A trend towards more openness over time is again suggested by the data in the next two columns, but this difference is not statistically significant. The presence of NGOs working in the area is associated with more openness, and this difference is significant (p < 0.01).1 PHAs judged by the KI to be of good or normal character appear more likely to be open than individuals who were judged to be of bad character, or whose assessment contained some qualification indicating that he or she may not have been highly regarded in the community. This difference is not statistically significant, nor is the difference suggesting 1 This test is a Pearson’s chi-square, our test of choice for bivariate associations unless otherwise specified.
8
women to be more open than men. Differences in degree of openness by socioeconomic status are illustrated in the final three columns (p < 0.05) and suggest an inverse association between these two variables.
As shown in the middle section of this table, the degree to which AIDS families are treated either positively or neutrally by their neighbors, as assessed by our KIs, is remarkable – a full 73% were believed to have experienced no negative reaction due to the illness (38% plus 35%) and less than a fifth were believed to have experienced only negative reactions by these local observers. This overwhelmingly positive reaction towards the family became even more pronounced after the PHA died. After the death, 91% of the AIDS households were believed to have experienced no negative community reaction.
As in the previous table, a longer duration of the epidemic in the local area appears to make community reaction slightly more supportive, but this difference again fails to reach statistical significance. But having an NGO working on AIDS in the area increases the likelihood that a family will be treated the same way during the illness as before (p < 0.05). The assessed character of the PHA has strong effects on how s/he and the family were treated during the illness (p < 0.001) but not afterwards. A family in which the PHA had bad or questionable character was more likely to be treated negatively and less likely to be treated positively by neighbors during their illness, but apparently after such a PHA dies, the family does not continue to carry the burden of the PHA’s poor reputation in the community. Sex differences are significant after the death of the PHA (p < 0.05), but these differences are difficult to interpret – female PHAs may evoke stronger community reactions on both ends of the continuum compared to males.
Table 5 provides more specific types of community reaction to AIDS families, as observed by our local health officials. Of the 278 families that were open to the community about the fact that a household member had AIDS, 78% experienced no specific negative community reaction, according to reports by our KIs. Avoidance or criticism were experienced by a fifth of the families. The proportion of families experiencing no specific negative reactions after the death of the PHA rises to 93%. So few cases of specific negative community reactions were reported that further analysis by selected cofactors was not possible.
Specific positive reactions were more commonly reported. Over a third of the families received either visits or expressions of sympathy from neighbors during the illness of the PHA, but this declined to 10% after the death of the PHA. VHVs (see the bottom panel) also report primarily positive or neutral community reaction to the specific AIDS families in their areas, with almost 90% of the families reported to either have received help from neighbors or, at the very least, to have experienced no avoidance.
In spite of the fact that our key informants work for or have an association with the government-- which may have an interest in portraying community reaction in a favorable light -- we believe our KIs to be reliable observers of how their communities respond to individuals and families stricken by AIDS. Interviews were conducted or observed by the main investigators on the project, and our impressions have been that the KIs were generally well informed and candid in their assessments. They spoke at length, for example, of cases that experienced problems. Moreover, there are some clear advantages of employing key informants over interviewing families directly. First, we obtain a more complete census of cases in the area, since we do not have to recruit families to participate. Second, KIs may in some cases be in a better position to judge the overall community reaction to a case than an AIDS family would, since some comments might be made that the KI hears about but not the family.
On the other hand, interviewing families directly also presents a number of advantages. First, their experience with community reaction is direct and does not have to be filtered through the lens of another. Second, some forms of community reaction, both positive and negative, may be too subtle for a secondary observer to note.
In Table 6, we present the reported experiences of community reaction by parents who had experienced the death of an adult son or daughter to AIDS during the previous 3 years. Substantially more families reported themselves to be at least open to some in the community (98%) than the proportion of cases reported by our KIs (82% from Table 4). We believe that this difference is more likely due to differences in the sample than in perspective. Even though we did not ask about AIDS specifically in our
9
interviews with parents unless the respondent mentioned it first (we asked only about deaths), we knew beforehand that these families had experienced a recent AIDS death, and these cases were screened by our intermediaries as likely to be willing to talk with us. This sample of parents is therefore is weighted towards families who are open to the community about the death in their household, and in most cases, the reasons underlying this death.2 Our in-depth interviews with parents will also miss those who are least open about the cause of the death of their adult child, but even among those we did interview, some made clear their concerns about how they would be treated by the community should they be open with this information. If fact, this anticipation of negative community reaction should the family be open about their calamity may be in some cases worse than the actual community reaction, or may even become self-fulfilling.
I told (my son) to look at himself. I didn't feel repelled by him but other people might. He was skinny then. His feet and his arms were so dark. It's like his skin was burnt. I told him not to go out but he said he didn't feel embarrassed. I told him to at least think about me. Other people would say how could he go out like this. I told him not to go out; so he didn't go. [51-year-old mother, in-depth interview, Bangkok]. I wanted to talk to other people but I was afraid that they would feel disgusted. [60-year-old mother, in-depth interview, Chiang Mai] (In one case I know) the mother cannot handle the truth. She told a health official that her child is infected but insisted that he not tell anybody else. However, people have already found out about it and had no problem with it [Community health official, focus group discussion, Petchburi].
The well-off in our parents survey were less likely to report themselves open to the community about the serious illness in their household (the illness that resulted in an AIDS-related death) compared to the other two SES groups (p < 0.05). This is also the case for urban compared to rural dwellers (p < 0.001) and for residents of Phichit province compared to Chiang Mai and Rayong (p < 0.01; results not shown). Given the fact that social ties are often looser and more transient in urban compared to rural communities, and that AIDS in Phichit is much more rare than in the other two provinces, these results are as expected. We did not anticipate SES differences in a particular direction, but suspect that the well off may have more at stake in terms of their reputation in the community compared to the other two SES groups.3 Families in which the character of the PHA is judged by the parents to be bad (only six percent of these families) appear to be less willing to disclose, similar to the pattern that exists in the KI reports, but again the difference does not reach statistical significance.
The proportion of AIDS households that were open to the community and who report some demonstration of positive community reaction during the illness is remarkable at 94%. Nearly all of the families who were open report visits by neighbors,4 many of whom did not come empty-handed or without some advice or service to offer (see Table 6).
2 When asked the cause of death of their deceased son or daughter, in two-thirds of the AIDS parents’ interviews, the respondent explicitly stated AIDS. A substantial share of those who did not state AIDS as the cause of death were open about the fact that their child had AIDS but gave as the cause of death an AIDS-related symptom or illness. 3 No time trends are apparent, which is not surprising since all of the cases for this survey were selected on the basis of having occurred during the past 3 years. 4 The fact that the proportion who report visits is slightly higher than those who report any positive community reaction is due to the fact that the respondents were prompted for each type of specific reaction if they did not mention it spontaneously. Prompted responses for these specific positive (and negative) reactions were much higher than the unprompted responses.
10
(Neighbors) came to visit (my son). I don't know what they thought but they came to visit him and bought a lot of things for him... They bought food and we ate together. Some people came a long way... I don't think (the neighbors changed any) because when he had to stay at the hospital, a lot of them came over to visit him. There were a lot of people at his funeral. [54-year-old mother and 59 year old father, in-depth interview, Phetchaburi]
Urbanites in the parents’ survey were significantly less likely to report offers by neighbors to
watch over the sick PHA or to receive advice compared to rural villagers; parents of PHAs deemed (by the parents) to be of bad character were less likely to receive visits or food compared to parents of PHAs of good or qualified character; and parents in Chiang Mai, where the epidemic is of longest duration and highest intensity, were more likely to receive offers to look after the ill child, gifts of medicine, and advice compared to parents in Phichit and Rayong (p < 0.05 for all comparisons).
A quarter of the families who were open report some negative reaction during the illness, gossip being the most common but isolation (not having neighbors come to visit) reported by a fifth (30% when the PHA was female versus 18% when the PHA was male; p < 0.05) of the parental households. Several of the PHAs’ parents in our in-depth interviews reported such reactions.
Those who did not hate us came and told us who did. How they talked about us. [59-year-old mother, in-depth interview, Rayong]
Negative reactions appear more common among families in the parents’ survey in which the PHA was deemed (by the parent) to be of bad character compared to the reference groups, but these differences are not significant.
Among the families whose situation was known to the community, more than 7 in 10 assessed the net community reaction to their misfortune to be sympathetic during the time of the illness; about a fifth reported both sympathetic and negative reactions; only three percent reported negative reactions only; and only four percent reported no reaction. Differences of these net reactions by a number of other factors explored are not significant but are suggestive of more positive experiences among the families with male PHAs, the non-poor, those deemed to be of at least qualified good character, and living in areas with epidemics of at least moderate seriousness (results not shown for seriousness of epidemic).
Among families reporting at least some negative community reaction, over half reported durations of at least a month; almost a fifth continue to suffer the consequences of negative community reaction (deaths occurred at least six months prior to the survey). Parents of PHAs who were male suffered shorter durations of negative community reaction than parents of female PHAs (p < 0.05). Other differences are not significant; sample sizes become quite small here due to the small number of households reporting negative community reaction.
Positive community reactions as reported by the AIDS parents continue in the vast majority of cases after the death of the PHA child (see Table 7). Over 90% of these parents report many or a normal number of persons attending the funeral of their child; at least some sympathy or offers to help; visits; and help with funeral arrangements by neighbors after the death of their child. Important differentials also exist. The minority of parents who describe their child to be of bad character are much less likely to report normal attendance at the funeral compared to the reference groups; as are parents in Phichit compared to the other two provinces (p < 0.001 for both comparisons). Parents in Phichit are also significantly less likely to report visits or help with funeral arrangements from neighbors than parents in the other two provinces, as do parents in urban relative to rural areas (p < 0.01 for both comparisons). Urban parents are in fact significantly less likely to report at least some supportive or helpful community reaction compared to parents in rural areas on all four dimensions measured (p < 0.05 for all). The poor fare worse than middle and high SES groups on having neighbors visit and on funeral attendance (p < 0.05 for both). Specific negative community reactions after death are more rare, but much more likely to be reported by Phichit parents compared to parents from the other two provinces (p < 0.05 for all five specific measures).
11
Parents of female and widowed (not shown) PHAs who died are more likely to report neighbors refusing to eat and drink at the funeral compared to the reference groups (p < 0.05 for both comparisons).
These significantly higher proportions of some groups suffering negative community reaction compared to others warrant attention, but it is also important to keep in mind that, according to these parents of PHAs who died, overall community reaction to the families was usually either positive or neutral (84% of the cases), and in cases where negative reaction does occur, in almost half of the cases it is quite short-lived – less than a month for 45% of the cases. This was noted by several of our community observers as well.
Interviewer: Was there any criticism (of this case)? | VHV: Yes, at first there was some talk, some criticism. But it disappeared after a couple of weeks, then things were back to normal [Village health volunteer interview, Petchburi]. Next, we turn to assessments of community reaction from the PHAs themselves. While a
reasonably representative sample of households experiencing the death of a young adult to AIDS presents formidable challenges, obtaining a reasonably representative sample of PHAs is even more difficult. This is because many PHAs are likely to be less willing to speak frankly about their current situation and experience than are their parents after a period of grieving has passed. Also, PHAs who participate in such a study will not only need to be quite open about their situation but also healthy enough to participate. Thus, our sample of PHAs is more likely to be weighted towards cases who are open than are the parents in our AIDS parents survey, and certainly more so than the cases identified by our key informants. Nevertheless, we were able to recruit 425 PHAs for our survey, mostly through their participation in local support groups for PHAs.
Perceptions of community reactions among this group of PHAs, both to PHAs generally and to themselves (if they are open to the community) are presented in Table 8 by the sex, education level, residence, and province of the PHA. PHAs report a wide range of both positive and negative reactions within their communities. Only about a fifth report no reaction at all, either to PHAs generally or to themselves. This is a substantially lower percentage than reported by the KIs in Table 4, who report this neutral community response for 38% of the cases they know about. More PHAs report positive community reactions than negative ones, and all reactions except for general talk are slightly more likely to be reported by a PHA speaking about himself than about PHAs generally.5 Women PHAs in this sample are significantly more likely to be open to their communities than men (p < 0.001), but this is likely due in part to the fact that over half of the women were widowed (and presumably infected by their husbands) whereas only 10% of the men were (results not shown). On the other hand, the pattern is similar to that reported by the KIs in Table 4.
Women are more likely to report responses of sympathy, support, and help (both for PHAs generally and for themselves) than men (p < 0.05 for all comparisons). Men are significantly more likely to report reactions of disgust or fear towards them than are women (p < 0.05).6 PHAs with intermediate levels of education (a proxy for SES here) fare better than those at either extreme for experiencing community sympathy and support, either for themselves or for PHAs generally (p < 0.001 for all comparisons). They are also the least likely to report experiencing fear or disgust (p < 0.05), while it is those with the least amount of education who are most likely to report being looked down upon (p < 0.01). Persons with the highest levels of education (more than six years) are the least likely to be open to their communities (p < 0.001). Areal differences in community reaction as assessed by these PHAs are
5 This is reasonable since those who are not open would be likely left out of the numerator in both panels and out of the denominator in the lower one. 6 When the above comparisons are limited to non-widows and to the PHAs’ personal experience, they continue to consistently show worse outcomes for men than women but are no longer statistically significant because of the reduced cell sizes.
12
profound. Urban dwellers, especially those from Bangkok (see the far right panel), are much less likely to be open to their communities than rural dwellers (p < 0.001), and apparently with good reason: urban PHAs are much less likely to report receiving expressions of sympathy or support from their communities than are rural PHAs (p < 0.001 for both comparisons). And in the far right panel, Bangkok is the clear outlier in the proportions of PHAs experiencing expressions of sympathy, support, disgust or fear, and condescension from their communities – PHAs in the other three provinces fare much better (p < 0.01 for all comparisons).
In the final sections of the paper, we explore some of the implications and consequences of community reaction for PHAs and their families. In Table 9, we show how the parents of PHAs who have died assess the reactions and responses of community officials towards them during their child's illness and after their death. Approximately half report helpful or sympathetic reactions from local health center staff and from community health volunteers. Positive reactions from village headmen were more common, at 62%. Reported negative reactions from all three types of community leaders were very rare. Parents of female PHA were less likely to report positive interactions with community health volunteers than were parents of men (p < 0.05), and parents of PHAs living in urban areas were less likely to report positive interactions with all three types of community leaders than their rural counterparts (p < 0.001 for all three comparisons). AIDS parents in Rayong were less likely than parents in Chiang Mai and Phichit to report support or sympathy from health center staff and community health volunteers.
Table 10 presents results from bivariate analyses of whether experience of negative community reaction either during the illness of the PHA or after their death was predictive of a deterioration of the parental respondent's relations with neighbors, overall level of happiness, or health. We focus on any experience of negative community reaction (as opposed to a net negative reaction, which is very uncommon) in order to include as many cases in our cells of interest as possible, i.e., to increase the power of these tests. Experience of any negative community reaction by the parental respondent was significantly related to a decline in community relations, whether the negative reaction occurred during the illness or after the death of the PHA (p < 0.05 for both comparisons). Also, the proportion reporting a very difficult care-giving experience was significantly higher for those parental respondents who experienced negative community reaction compared to those who did not, again, this is true no matter when the negative reaction occurred (p < 0.05 for both comparisons). To explore whether the experience of negative community reaction was predictive of a difficult care-giving experience in the presence of potentially confounding variables, we estimated a multivariate logistic regression model that included controls for urban versus rural residence, time spent on care-giving (a great deal versus the other categories), sex of the respondent, and sex of the PHA. Any experience of negative community reaction more than doubled the odds of the parental respondent reporting a very difficult care-giving experience, even in the presence of the aforementioned controls (p < 0.01 - results not shown). Discussion and Conclusions
We employ recently-collected data from a wide range of sources and perspectives to assess community reaction towards PHAs and their parents in Thailand. These data were collected during the period 1999-2001; include five surveys, one set of focus groups, one set of group interviews, and two sets of in-depth interviews; and address community reaction from the perspective of the PHAs themselves, their parents, health care providers, local community observers, and a general sample of young and older age adults. Our study sites include a wide range of circumstances in Thailand, including rural and urban locations, and areas with varying levels of HIV and AIDS prevalence. These unusually comprehensive and systematic data place us in an excellent position to make a number of conclusions about the manifestation of AIDS-related stigma in a medium-prevalence country; to discuss the implications of our findings for more general theory regarding community reaction and AID-related stigma; and to discuss the implications of these empirical findings for programs that address the plight of families and societies suffering the consequences of AIDS.
13
The experience of AIDS-related stigma in Thailand
Our KAP survey shows generally high levels of interest and understanding about AIDS among Thai young and older age adults. We also find evidence of some over-concern about the risks of non-intimate contact with a PHA or his family, concern that could be the basis for avoidance of and/or stigma towards PHAs. However, while this set of surveys does reveal a fair degree of variation in community reaction among and within the communities we studied, these data generally indicate that quite neutral or positive responses towards PHAs and their families is the norm in Thailand. Data collected from local level health professionals provide the basis for much optimism regarding the treatment of PHAs and their families. Among the 85 sites in the survey, 82% of the respondents report either positive or neutral overall community reaction, and 87% report that the trend is towards more tolerance. Community health volunteers reporting from 49 sub-communities are similarly sanguine, and both types of observers' reports for reactions towards specific families (as opposed to general assessments of their communities) indicate widespread community acceptance for most families affected by this disease.
Differentials are also apparent, with stigma varying with features of the social environment, the affluence of the household, the reputation of the affected individual, and the stage of illness. Areas without NGOs actively working on AIDS have fewer AIDS families treated the same way they were before their misfortune – a finding similar to results reported by Kongsin et al. (2001), conducting related research on the impacts of AIDS on households in a northern Thai province. Households in which the PHA had bad or questionable character were more likely to be treated negatively and less likely to be treated positively by neighbors during the illness (but not afterwards). Negative community reactions towards affected families were more common during the illness than after the death of the PHA, according to our local health officials and the AIDS parents we surveyed. In a substantial proportion of the instances where negative reactions did occur, they were quite transitory. Data gathered from local observers do not indicate significant socioeconomic differentials in community reaction, but the data from our parents and PHA surveys do. Poor parents were much less likely than the other SES groups to report receiving help looking after their sick child during the illness and receiving visits after the death of their child than did the well off or those of moderate means. PHAs of moderate levels of education reported receiving sympathy and support more frequently than did PHAs in the high and low education categories and were least likely to report experiencing reactions of fear or disgust. Community response in rural areas was judged to be more positive than in urban areas on a wide range of variables in both the AIDS parents survey and in the PHA survey. As predicted, gender is not a consistent predictor of AIDS-related stigma; community reaction to women with AIDS relative to men varies with the source of information. Results from community observer data are ambiguous; reports from the parents’ survey indicate better community reactions towards men; and results from the PHA survey indicate better community reactions towards women. Point of view is clearly an important factor to consider when interpreting sex-based differences in AIDS-related stigma, and our results clearly contradict the widely reported notion that women PHAs are treated much worse by their communities than are men; the reality is much more complicated. More generally, more attention should be given to how point-of-view influences not only an individual’s perception of stigma, but also the relationships among social position, social roles, and social sanctions. Implications for theoretical perspectives on AIDS-related stigma and community reaction
We find evidence to support our hypothesis that the relative magnitudes of symbolic versus instrumental stigma will be the reverse of what has been found in the U.S., although our evidence here is only suggestive. That so few PHAs, parents, or observers report fear or disgust, condescension, and avoiding conversation, we take to imply that symbolic stigma is not especially widespread in the Thai context. This was anticipated because the behaviors most associated with HIV in Thailand have not been as stigmatized as the behaviors most closely linked with HIV infection in the U.S. It is instrumental stigma, related to fears of becoming infected, that warrants the most attention in Thailand -- many Thais overestimate the risks of contracting HIV through casual contact.

14
As anticipated by earlier theoretical work by Goffman and Mechanic, we find community reaction to PHAs to be complex, dynamic, and dependent upon both the context and the observer. Many of our PHAs, parents, and observers report both positive and negative reactions to PHAs and their families. Also, reports of specific forms of negative community reaction among the PHAs, while still a minority, are more frequent than specific negative reports by AIDS parents and much more frequent than those reported by the health officials. One interpretation of this finding is consistent with one of our hypotheses: some PHAs may anticipate negative community reaction more than they are actually the target of it, à la Goffman. Some of our in-depth interviews with the parents of PHAs also strongly suggest that it is the anticipation of negative community reaction that may cause some affected families to withdraw from their communities. We note that observed differences in perceptions of stigma among the types of respondents could also be due to differences in the specific questions asked of each source (although the proportion of parents and observers reporting any negative reactions are still less than the PHAs' reports of specific forms of negative reaction); the way the samples were drawn; more sensitivity on the part of PHAs because of a focus on stigma in PHA group activities; or the possibility that one type of observer may be in a better position to observe and judge community reaction than another.
Also, given our wide range of data sources and large number of statistical tests conducted, the possibility of reporting a significant effect when none in fact exists (a Type I error) is not trivial. However, what we find most remarkable is that no such odd or unexplainable findings appear to occur; rather, the consistency of the story told by this wide range of data sources is remarkable. Why don’t we find more stigma? It is possible that Thailand is a special case – after all, it has had one of the most effective responses to the epidemic to date – but this strikes us as unlikely to be a major factor. Most reports on community reaction to AIDS in Thailand in the popular press and in the research literature have emphasized negative reaction, as have reports elsewhere. We believe that this emphasis is due in large part to the propensity of many journalistic accounts to sample on the dependent variable, i.e., to focus attention on unfortunate cases and then to generalize their experience to broader groups. Much qualitative research makes this same mistake. Related to this is the fact that an instance of stigma is more salient than is an instance of no stigma and thus is much more likely to result in a story to tell (Songwathana and Manderson 2001). While case studies are essential for helping us to interpret the experience of stigma where it occurs, population based studies are essential for assessing the prevalence and distribution of community reaction. A second reason for finding less negative community reaction than is often reported is related to the anticipated stigma versus actual stigma distinction. Curiosity is sometimes mistaken for stigma. An AIDS case is a remarkable event in village life -- only four percent of the families in our parents survey reported no reaction from the community to their plight -- and a misinterpretation of curiosity and interest for malice is probably fairly common. We did try to distinguish between gossip (ninta) and general talk (kui) in the PHA survey, but in practice, in Thai as in English, such distinctions often lie in the eye of the beholder. This is in fact an observation made frequently by several of our various types of community observers.
Such a misinterpretation becomes more likely if community reaction is viewed with a western lens rather than with a culturally specific one (Goldin 1994). If we consider that much of the attention given to community reaction arises from an activist tradition, and that often research on stigma is conducted by western-trained scholars who value privacy and the rights of the individual over openness and the interests of the community,7 the emphasis of negative over positive community reaction in the AIDS literature makes sense.
Other dynamics working at the local level may also serve to perpetuate the idea of negative community reaction as the norm. Our fear that high-level health officials might try to portray the situation as more positive than it really is did not materialize. To the contrary, some high-level Thai government officials may over-generalize from the negative cases that they hear about. One high-level provincial 7 Many western-trained scholars also incorrectly assume that many of the key behaviors that put one at risk of contracting HIV in developing countries are themselves highly stigmatized, as they are in their home countries.

15
health official we interviewed stated categorically that most people in the province did not accept PHAs, a point of view that is contradicted by the data we subsequently collected there.8 Without the extensive and community based data we collected as part of this study, such a strongly stated point of view that could have been extremely misleading to a researcher investigating community reaction to AIDS in provincial Thailand. Implications for programs
Research and advocacy that may exaggerate the distribution and effects of stigma surely has the well-being of affected individuals and families as its goal, but such exaggerations are not without costs. Resources that are directed towards stigma reduction cannot be put towards other goals that may have greater payoff. For example, Uthis (1999) finds social stigma to be the least consequential of a variety of potential impacts of living with and caring for PHAs in Thailand; economic hardships were the most severe. Kespichayawattana and VanLandingham (2003), in work related to the results reported here, find that less than 1% of the over 300 care givers (mothers, fathers, or parents) to an adult child who died from AIDS felt that negative community reaction was the most difficult dimension of the experience; rather it was the strains of care giving itself that was most commonly cited. Where negative community reaction exists it appears to be of consequence to some. Thirteen percent of parents who experienced negative community reaction considered leaving their communities. A small number report negative experiences with local officials, which could affect their well-being and standing in their communities. Parents who experienced negative community reaction were more likely to report a decline in their relations with neighbors over time than those parents who had not experienced these negative reactions. And parents who experienced negative community reactions were also more likely to report a very difficult care taking experience than those who did not, a result that holds up in multivariate analysis.
Community reaction towards individuals and families suffering the consequences of AIDS in Thailand appears to be quite positive or neutral for most but not all. For that minority whose suffering from this terrible disease is compounded by the indifference or hostility of their neighbors, we recommend an aggressive and rapid response both to help change the social environment in which these negative reactions occur, and to help these unfortunate individuals and families cope with these occasionally unsupportive environments.
8 The general community reaction as assessed by our community health workers in 6 of the 9 communities surveyed in that province was either neutral or sympathetic; and all reported that the trend was towards more acceptance -- results from our survey of VHVs were similarly optimistic.
16
References Alonzo AA, Reynolds NR. Stigma, HIV and AIDS: an exploration and elaboration of a stigma trajectory.
1995. Social Science and Medicine 41: 303-15. Assavanonda, Anjira. 2001. Infected people still face discrimination: Forum pinpoints problems in
society. Bangkok Post. Bharat S and P Aggleton. 1999. Facing the challenge: household responses to HIV/AIDS in Mumbai, India.
AIDS Care 11: 31-44. Brashers DE, Neidig JL, Reynolds NR, Haas SM. 1998. Uncertainty in illness across the HIV/AIDS trajectory.
Journal of the Association of Nurses in AIDS Care. 9: 66-77. Brown, Lisanne, Kate Macintyre and Lea Trujillo. 2003. Interventions to reduce HIV/AIDS stigma: What have
we learned? AIDS Education and Prevention 15(1). Brown, Tim, Werasit Sittitrai, Suphak Vanichseni, & Usa Thisyakorn. 1994. The recent epidemiology of HIV
and AIDS in Thailand. AIDS 8(Supplement 2): S131-S141. Busza, JR. 2001. Promoting the positive: responses to stigma and discrimination in Southeast Asia. AIDS Care
13: 441-56. Chamratrithirong, Aphichat, Varachai Thongthai, Wathinee Boonchalaksi, Philip Guest, Churnrurtai
Kanchananchitra & Anchalee Varangrat. 1998. The Success of the 100% Condom Promotion Programme in Thailand: Evaluation of the 100% Condom Promotion Programme and the Validation of the Decline in Trends for Selected STDs. Manuscript.
De Bruyn D. 1992. Women and AIDS in Developing Countries. Social Science and Medicine 34: 249-262. Goffman, Erving. 1964. Stigma: Notes on the management of spoiled identity. Englewood Cliffs, NJ:
Prentice-Hall, Inc. Goldin C. 1994. Stigmatization and AIDS: Critical Issues in Public Health. Social Science and Medicine 39:
1359-1366. Hanenberg, Robert, Wiwat Rojanapithayokorn, Prayura Kunasol, & David C. Sokal. 1994. Impact of
Thailand's HIV-control programme as indicated by the decline of sexually transmitted diseases. Lancet 344 (July 23, 1994): 243-245.
Heckman, T. G., A. M. Somlai, K. J. Sikkema, J. A. Kelly, and S. L. Franzoi. 1997. Psychosocial predictors of life satisfaction among persons living with HIV infection and AIDS. Journal of the Association of Nurses in AIDS Care. 8(5): 21-30.
Herek, Gregory M., and John P. Capitanio. 1998. Symbolic Prejudice or Fear of Infection? A Functional Analysis of AIDS-Related Stigma Among Heterosexual Adults. Basic and Applied Social Psychology 20: 230–241.
Im-em, Wassana, Mark VanLandingham, John Knodel, and Chanpen Saengtienchai. 2002. HIV/AIDS-related Knowledge and Attitudes: A Comparison of Older Persons and Young Adults in Thailand. AIDS Education and Prevention 14(3): 246-260.
Im-em, Wassana, Mark VanLandingham, John Knodel, and Chanpen Saengtienchai. 2001. Knowledge and Attitudes of Older People about HIV/AIDS in Thailand: A Comparison with Young Adults. PSC Research Report No. 01-464, 2001. Published as Publication No. 257, Institute for Population and Social Research, Mahidol University, Thailand. http://aidseld.psc.isr.umich.edu
Im-em Wassana. Changing partner relations in the era of AIDS in Upper-north Thailand. 1999. In Caldwell J, et al. (eds). Resistances to Behavioural Change to Reduce HIV/AIDS Infection in Predominantly Heterosexual Epidemics in Third World Countries. Canberra, Australia: Health Transition Center.
Jacoby, Ann. 1994. Felt Versus Enacted Stigma: A Concept revisited. Social Science and Medicine 38: 269-274.
Kespichayawattana Jiraporn and Mark VanLandingham. 2003. Health impacts of co-residence with and care giving to persons with HIV/AIDS (PHAs) on older parents in Thailand. Journal of Nursing Scholarship 35(3): 217-224.
Keyes CF. 1989. Thailand: Buddhist Kingdom as Modern Nation-state. Boulder: Westview Press. Keyes CF. 1984. Mother or mistress but never a monk: Buddhist notions of female gender in rural Thailand.
American Ethnologist 11(2):223-241.
17
Knodel, John, Mark VanLandingham, Chanpen Saengtienchai, and Wassana Im-em. 2000. Older People and AIDS: Quantitative Evidence of the Impact in Thailand. PSC Research Report 00-443. http://www.psc.isr.umich.edu/pubs/> - click on “Search for PSC publications.
Knodel John, et al. 2002. The Impact of an Adult Child’s Death due to AIDS on Older-aged Parents: Results from a Direct Interview Survey. PSC Research Report. http://www.psc.isr.umich.edu/pubs/> - click on “Search for PSC publications.
Knodel, John, Chanpen Saengtienchai, Wassana Im-em and Mark VanLandingham, “The Impact of Thailand’s Aids Epidemic on Older Persons: Quantitative Evidence from a Survey of Key Informants.” PSC Research Report 00-448. July 2000. Published as Publication No. 252, Institute for Population and Social Research, Mahidol University, Thailand (2000). http://www.psc.isr.umich.edu/pubs/> - click on “Search for PSC publications.
Knodel, John, Chanpen Saengtienchai, Wassana Im-em and Mark VanLandingham. 2001. The Impact of AIDS on Parents and Families in Thailand: A Key Informant Approach. Research on Aging 23(6): 633-670
Knodel, John. 1997. The closing of the gender gap in schooling: the case of Thailand. Journal of Comparative Education 33: 61-86.
Kongsin Sukhontah, Sukhum Jiamton, Charlotte H Watts, and Angsana Boonthum. 2001. Conducting a household survey on the economic impact of chronic HIV/AIDS morbidity in rural Thailand: Methodological issues. Journal of Health Sciences 10: 276-289.
Kornsirilak, Swat. 2001. Interactions of community in providing care to PHA in the dimension of community people and of PWA in a border area in the South. Abstract, National AIDS Conference.
Link, B, and JC Phelan. 2001. Conceptualizing stigma. Annual Review of Sociology. 27: 363-385. Macqueen, K, et al. 1996. Alcohol consumption, brothel attendance, and condom use: normative expectations
among Thai military conscripts. Medical Anthropology Quarterly 10(3): 402-423 Malcolm, Anne, Peter Aggleton, Mario Bronfman, Jane Galvao, Purnima Mane, and JaneVerrall. 1998. HIV-
related stigmatization and discrimination: its forms and contexts. Critical Public Health 8: 347. Mason, Carl J., Lauri E. Markowitz, Suchai Kitsiripornchai, Achara Jugsudee, Narongrid Sirisopana, Kalyanee
Torugsa, Jean K. Carr, Rodney A. Michael, Sorachai Nitayaphan, & John G. McNeil. 1995. Declining prevalence of HIV-1 infection in young Thai men. AIDS 9: 1061-1065.
Maticka-Tyndale E, et al. 1997. Contexts and patterns of men’s commercial sexual partnerships in northeastern Thailand: Implication for AIDS prevention. Social Science & Medicine 44: 199-213
Mechanic, David. 1995. Sociological dimensions of illness behavior. Social Science and Medicine 41:1207-1216.
Mullan, Joseph T. 1998. Aging and informal caregiving to people with HIV/AIDS. Research on Aging, Special Issue: HIV/AIDS and Aging, ed. Marcia Ory, Diane Zablotsky, and Stephen Crystal. Thousand Oaks: Sage.
Nyblade, Laura, Rohini Pande, Sanyukta Mathur, Kerry MacQuarrie, Ross Kidd, Hailom Banteyerga, Aklilu Kidanu, Gad Kilonzo, Jessie Mbwambo, Virginia Bond. 2003. Addressing HIV-Related Stigma and Resulting Discrimination in Africa: A Three-Country Study in Ethiopia, Tanzania, and Zambia. Manuscript. International Center for Research on Women.
Palloni, Alberto, and Yean Ju Lee. 1992. Some Aspects Of The Social Context of HIV And Its Effects on Women, Children and Families. Population Bulletin of the United Nations No 33-1992.
Parker R and P Aggleton. 2002. HIV/AIDS-related stigma and discrimination: a conceptual framework and agenda for action. Manuscript - The Population Council’s Horizons Program.
Paul Godfred. 2001. When the Boomerang Returns: A Qualitative Study of the Socio-Economic Impact of HIV/AIDS on Older People in Northern Thailand. Manuscript.
Saengtienchai Chanpen and J Knodel. 2001. Parents providing care to adult sons and daughters with HIV/AIDS in Thailand. Geneva: UNAIDS.
Chanpen Saengtienchai and John Knodel. Parents providing care to adult sons and daughters with HIV/AIDS in Thailand. UNAIDS Case Study, Best Practice Collection, Geneva: UNAIDS, November 2001. Also issued as “Parental Caregiving to Adult Children with AIDS: A Qualitative Analysis of Circumstances and Consequences in Thailand.” Population Studies Center, University of Michigan, Research Report 01-481, July 2001

18
Songwathana Praneed, and Lenore Manderson. 2001. Stigma and rejection: living with AIDS in villages in southern Thailand. Medical Anthropology 20(1): 1-23.
Songwathana, Praneed. 2001. Situation analysis of home and community based care for people living with HIV/AIDS in Southern Thailand. Abstract, National AIDS Conference.
Sowell, RL, Lowenstein A, Moneyham L, Demi A, Mizuno Y, and BF Seals. 1997. Resources, stigma, and patterns of disclosure in rural women with HIV infection. Public Health Nursing 14: 302-12.
Stein, J. 1997. The impact of HIV/AIDS on the household. AIDS Bulletin. 6:20-3. Takahashi, S., Y. Yamazaki, and C. Kawata. 1999. Client anxiety from awareness of personal HIV
risk and relation to taking HIV test at public health centers in Japan. Nippon Koshu Eisei Zasshi 46(4):275-88.
Thai Working Group on HIV/AIDS Projection. 2001. Projections for HIV/AIDS in Thailand: 2000-2020. Bangkok, Thai Ministry of Public Health.
Thailand Ministry of Public Health Web Site 1999. UNAIDS. 2000. Report on the global HIV/AIDS epidemic. Geneva, Switzerland: UNAIDS. UNAIDS. 1998. Connecting Lower HIV Infection Rates with Changes in Sexual Behaviour in Thailand: Data
Collection and Comparison. UNAIDS Case Study. Geneva, UNAIDS Best Practice Collection, UNAIDS/98.15.
Uthis P. 1999. The effects of commitment to care giving role, stressors, appraisal of stress, coping resources, and coping responses on emotional well-being among HIV/AIDS family caregivers in Thailand. Ph.D. dissertation. Case Western Reserve University.
VanLandingham Mark and Lea Trujillo. 2002. Recent changes in sexual attitudes, norms, and behaviors among unmarried Thai men: A qualitative analysis. International Family Planning Perspectives 28(1):6-15.
VanLandingham, Mark and Wassana Im-em. 2001. Living with HIV/AIDS in Thailand: Results from a Self-administered Survey. PSC Research Report No. 01-488, http://aidseld.psc.isr.umich.edu
VanLandingham Mark, Knodel John, Chanpen Saengtienchai, and Anthony Pramualratana. 1998. In the company of friends: Peer influence on Thai male extramarital sex. Social Science and Medicine 47(12): 1993-2011.
Warwick, Ian, Shalini Bharat, Roberto Castro, Rafael Garcia, Melkizedeck Teshabari, Anchalee Singhanetra-Renard, and Peter Aggleton. 1998. Household and community responses to HIV and AIDS in developing countries. Critical Public Health 8(4): 311-328.
World Bank. 2000. Thailand's response to AIDS: building on success, confronting the future. Washington: The World Bank.

19
Appendix: More details on the data and methods used in the study. Potential biases
Any empirical study of community reaction to AIDS faces formidable methodological challenges. The first set involves potential selection biases – individuals who are most susceptible to stigma or most likely to engage in it may be least likely to participate in such a study. While these potential biases are of concern in the current study, we benefit from working in a society with an extensive public health clinic system in local areas, staffed by local health workers who are knowledgeable of and usually live in close contact with the local population. Also, Thais are generally cooperative in social science surveys, and only in fairly rare instances will refuse to participate if approached in a culturally appropriate manner. Finally, our triangulation of data from a variety of sources allows for some built-in checks against biases that might severely compromise a study based upon a single survey.
A second set of potential biases could be labeled reputation and political biases. Individuals who engage in, experience, or witness stigma or discrimination may not wish to report this behavior if it is seen to impugn the character of the local population. Similarly, it is often in the interest of the government to portray a situation as perhaps more uplifting than it is; the interests of nongovernment organizations are often the opposite. Fortunately, our interviews of PHAs and their parents, and our general KAP study of AIDS knowledge and attitudes in the general population will provide some important checks on the reports from government officials who might have a vested interest in portraying the situation in a particular way. Since the officials we collect our data from are local practitioners at a low rank in the health bureaucracy (as opposed to higher level political appointees), they should be under less pressure to distort the situation in a way favorable to the interests of the government. In fact, we generally found them to be extremely candid in their descriptions of local cases, and found them quite willing to discuss difficult situations where they occurred.
A third set of challenges involves the power of anecdotes in forming impressions. A tragic case, even a rare one, can have powerful influences on how an observer may view the general situation. Families that experience no stigma will be far less salient to such an observer than a family that does, since if no stigma occurs there is no event to think about or attend to.
Data and sampling
Data from the AIDS parents study resulted from face-to-face structured interviews of the parents of 394 PHAs who died. At most sites, all parents of PHAs who died in our study sites during a specified period of time (six months to three years prior to the survey) were asked to participate by our local health contacts. Sites, chosen to reflect a broad range of circumstances, were selected from three provinces from three sub-regions of Thailand.9 These survey data are supplemented by qualitative data resulting from 18 in-depth interviews of parents who had lost an adult PHA child.10
Data from the Thai AIDS Cases Study (TACS) resulted from semi-structured face-to-face interviews of local health staff from eight provinces and Bangkok. The eight provinces include at least one province from each of the four regions of the country; there were a total of 85 local sites included in this component of the study. We included all cases occurring at the local site up to 20. These interviews generated individual and family level information for 963 cases of persons living with or who died of AIDS, and more extensive information for a subset of 286 adult AIDS cases – it is this latter subset upon which we base our analysis of community reaction here. This instrument also generated community level information for 85 communities (mostly village clusters).11 These survey data from our local key 9 For more information about this survey, please see our research report Knodel et al. 2002; downloadable from the website listed in the bibliography. 10 For more information about these in depth interviews, please see Saengtienchai and Knodel 2001. 11 For more information about this survey, please see our research report Knodel et al. 2000; downloadable from the website listed in the bibliography.
20
informants are supplemented with qualitative data from six group interviews with community hospital nurses (one to three nurses at each site), six focus group discussions of community level health officials, and 49 in-depth interviews with village health volunteers.
Data from the KAP study resulted from face-to-face structured interviews of 1170 adults from four provinces in three regions of Thailand, split fairly evenly among three age groups (20-39; 50-59; 60-74). Respondents were selected at systematic intervals from population registers where they existed; introductions were provided by local health staff and/or village health volunteers.12 Data from the PHA study resulted from assisted self-administered questionnaires from 425 PHAs from two provinces in the upper north and Bangkok. Most PHAs were recruited from local support groups; all were asked to participate.13 Village health volunteer (VHV) survey data resulted from semi-structured face-to-face interviews of 49 VHVs, each serving a subset of households in a village. VHVs were recruited by our professional contacts working in provinces of interest. These interviews generated contextual information on 49 sub-communities from six provinces representing three sub-regions of Thailand, and family level information for 64 AIDS affected households. Qualitative data were collected using semi-structured guidelines, and were systematically coded and analyzed using a standard text analysis program (The Ethnograph). Qualitative results are used here primarily to supplement and illustrate the survey findings.
12 For more information about this survey, please see our research report VanLandingham et al. 2001; downloadable from the website listed in the bibliography. 13 For more information about this survey, please see our research report Im-em et al. 2001; downloadable from the website listed in the bibliography.
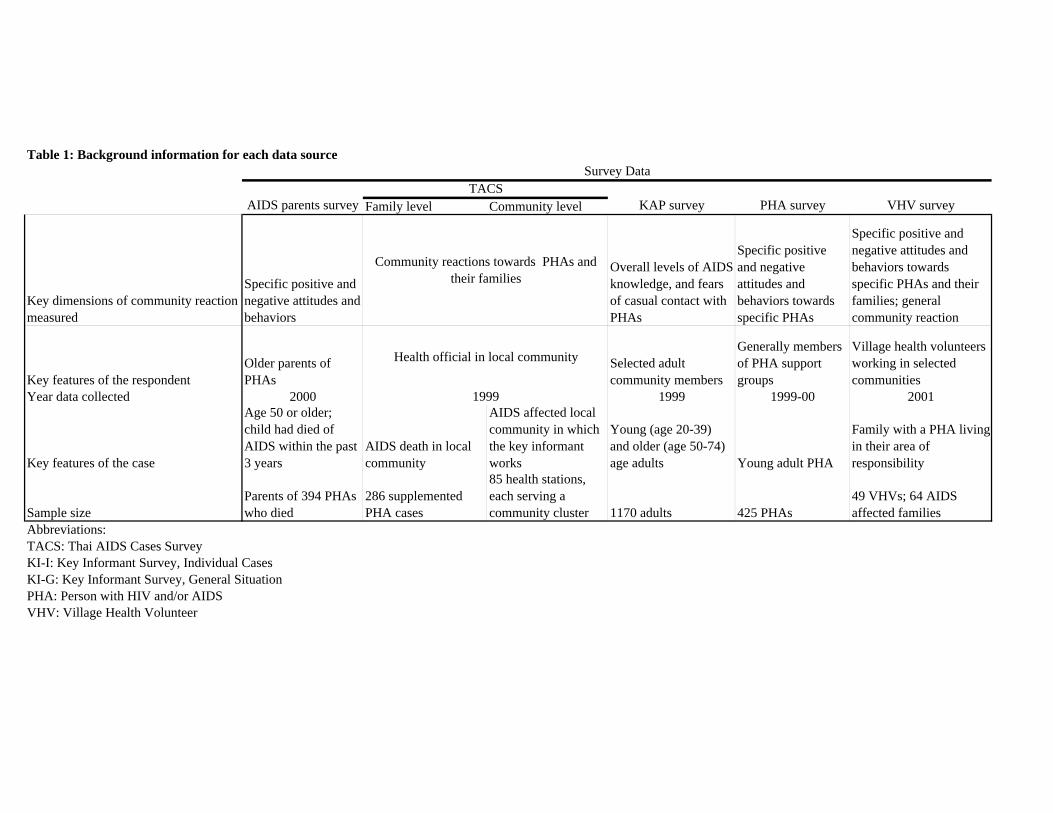
Table 1: Background information for each data source
Family level Community level
Key dimensions of community reaction measured
Specific positive and negative attitudes and behaviors
Overall levels of AIDS knowledge, and fears of casual contact with PHAs
Specific positive and negative attitudes and behaviors towards specific PHAs
Specific positive and negative attitudes and behaviors towards specific PHAs and their families; general community reaction
Key features of the respondentOlder parents of PHAs
Selected adult community members
Generally members of PHA support groups
Village health volunteers working in selected communities
Year data collected 2000 1999 1999-00 2001
Key features of the case
Age 50 or older; child had died of AIDS within the past 3 years
AIDS death in local community
AIDS affected local community in which the key informant works
Young (age 20-39) and older (age 50-74) age adults Young adult PHA
Family with a PHA living in their area of responsibility
Sample size Parents of 394 PHAs who died
286 supplemented PHA cases
85 health stations, each serving a community cluster 1170 adults 425 PHAs
49 VHVs; 64 AIDS affected families
Abbreviations: TACS: Thai AIDS Cases SurveyKI-I: Key Informant Survey, Individual CasesKI-G: Key Informant Survey, General SituationPHA: Person with HIV and/or AIDSVHV: Village Health Volunteer
Community reactions towards PHAs and their families
Health official in local community
1999
Survey Data
KAP survey PHA surveyTACS
VHV surveyAIDS parents survey
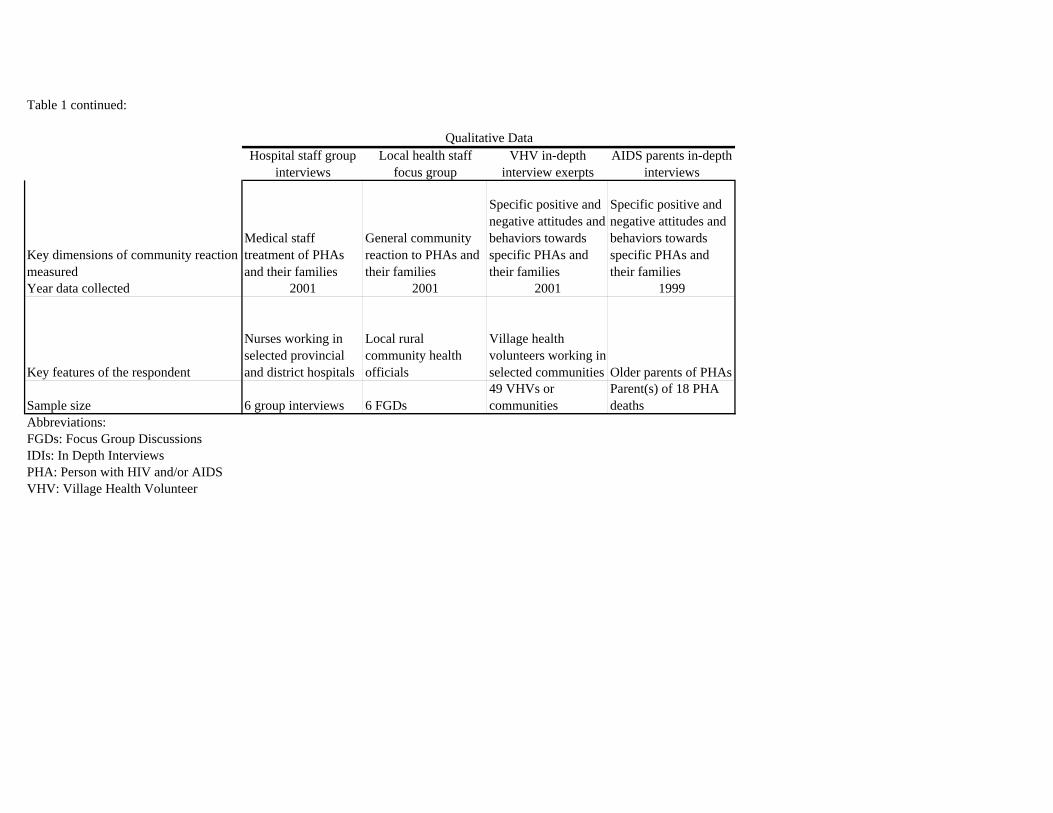
Table 1 continued:
Key dimensions of community reaction measured
Medical staff treatment of PHAs and their families
General community reaction to PHAs and their families
Specific positive and negative attitudes and behaviors towards specific PHAs and their families
Specific positive and negative attitudes and behaviors towards specific PHAs and their families
Year data collected 2001 2001 2001 1999
Key features of the respondent
Nurses working in selected provincial and district hospitals
Local rural community health officials
Village health volunteers working in selected communities Older parents of PHAs
Sample size 6 group interviews 6 FGDs49 VHVs or communities
Parent(s) of 18 PHA deaths
Abbreviations: FGDs: Focus Group DiscussionsIDIs: In Depth InterviewsPHA: Person with HIV and/or AIDSVHV: Village Health Volunteer
Qualitative DataHospital staff group
interviewsLocal health staff
focus group VHV in-depth
interview exerptsAIDS parents in-depth
interviews
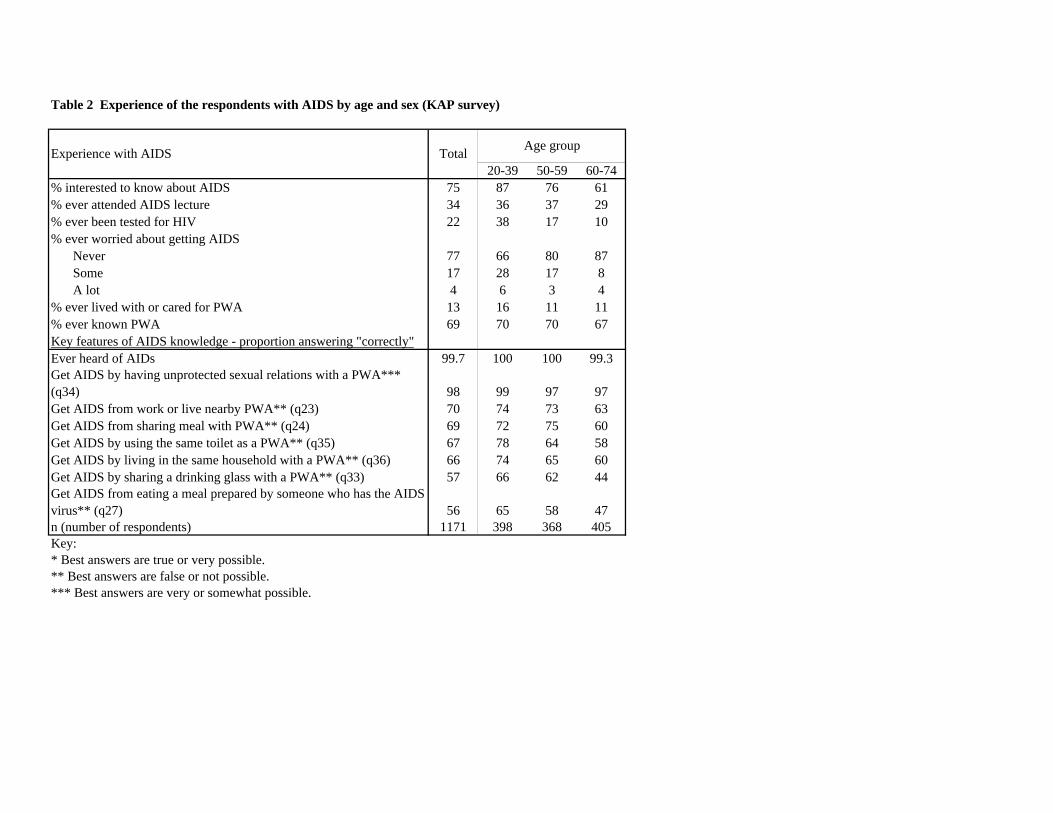
20-39 50-59 60-74% interested to know about AIDS 75 87 76 61% ever attended AIDS lecture 34 36 37 29% ever been tested for HIV 22 38 17 10% ever worried about getting AIDS
Never 77 66 80 87Some 17 28 17 8A lot 4 6 3 4
% ever lived with or cared for PWA 13 16 11 11% ever known PWA 69 70 70 67Key features of AIDS knowledge - proportion answering "correctly"Ever heard of AIDs 99.7 100 100 99.3Get AIDS by having unprotected sexual relations with a PWA*** (q34) 98 99 97 97Get AIDS from work or live nearby PWA** (q23) 70 74 73 63Get AIDS from sharing meal with PWA** (q24) 69 72 75 60Get AIDS by using the same toilet as a PWA** (q35) 67 78 64 58Get AIDS by living in the same household with a PWA** (q36) 66 74 65 60Get AIDS by sharing a drinking glass with a PWA** (q33) 57 66 62 44Get AIDS from eating a meal prepared by someone who has the AIDS virus** (q27) 56 65 58 47n (number of respondents) 1171 398 368 405Key: * Best answers are true or very possible.** Best answers are false or not possible. *** Best answers are very or somewhat possible.
Table 2 Experience of the respondents with AIDS by age and sex (KAP survey)
Experience with AIDS Total Age group
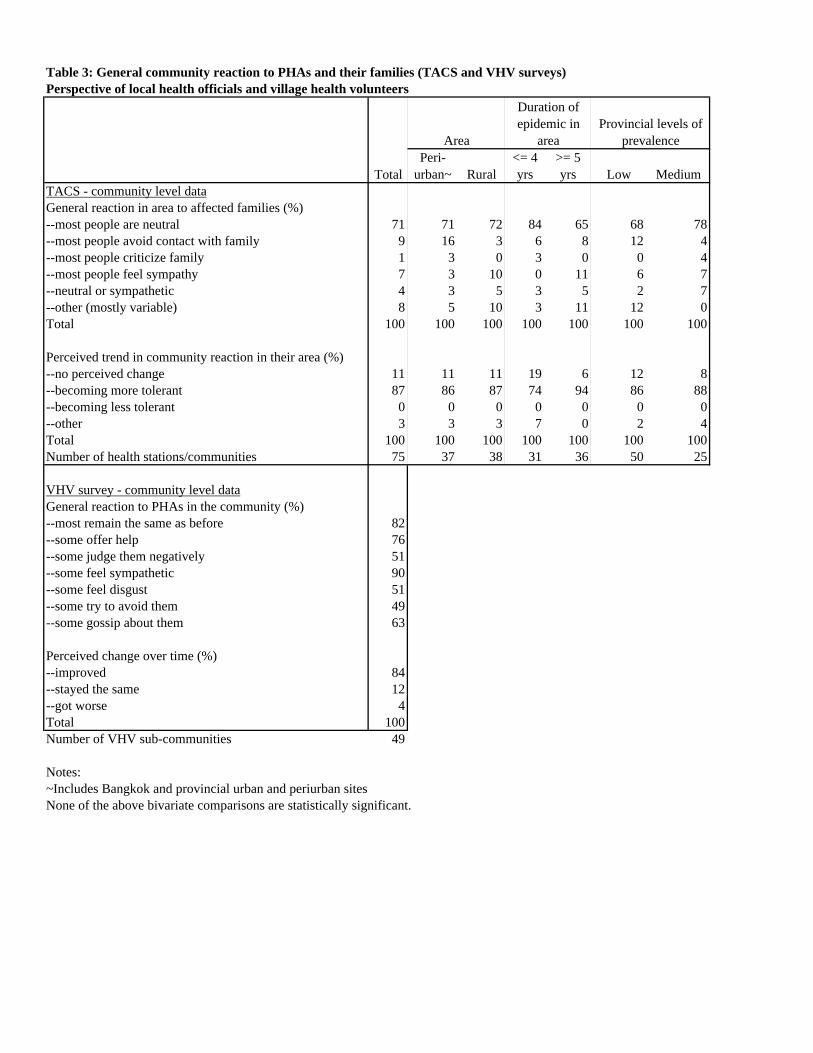
Perspective of local health officials and village health volunteers
Peri-urban~ Rural
<= 4 yrs
>= 5 yrs Low Medium
TACS - community level dataGeneral reaction in area to affected families (%)--most people are neutral 71 71 72 84 65 68 78--most people avoid contact with family 9 16 3 6 8 12 4--most people criticize family 1 3 0 3 0 0 4--most people feel sympathy 7 3 10 0 11 6 7--neutral or sympathetic 4 3 5 3 5 2 7--other (mostly variable) 8 5 10 3 11 12 0Total 100 100 100 100 100 100 100
Perceived trend in community reaction in their area (%)--no perceived change 11 11 11 19 6 12 8--becoming more tolerant 87 86 87 74 94 86 88--becoming less tolerant 0 0 0 0 0 0 0--other 3 3 3 7 0 2 4Total 100 100 100 100 100 100 100Number of health stations/communities 75 37 38 31 36 50 25 VHV survey - community level dataGeneral reaction to PHAs in the community (%) --most remain the same as before 82--some offer help 76--some judge them negatively 51--some feel sympathetic 90--some feel disgust 51--some try to avoid them 49--some gossip about them 63
Perceived change over time (%)--improved 84--stayed the same 12--got worse 4Total 100Number of VHV sub-communities 49
Notes: ~Includes Bangkok and provincial urban and periurban sitesNone of the above bivariate comparisons are statistically significant.
Table 3: General community reaction to PHAs and their families (TACS and VHV surveys)
Provincial levels of prevalence
Total
Area
Duration of epidemic in
area
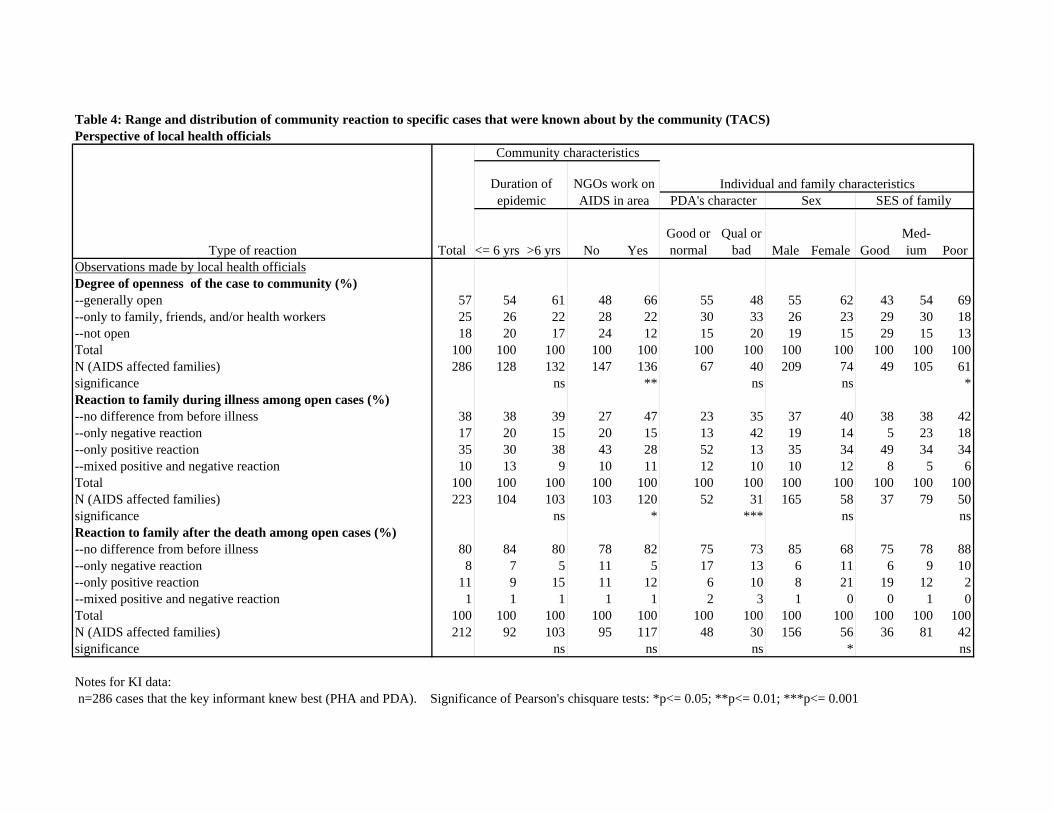
Perspective of local health officials
<= 6 yrs >6 yrs No YesGood or normal
Qual or bad Male Female Good
Med-ium Poor
Observations made by local health officialsDegree of openness of the case to community (%) --generally open 57 54 61 48 66 55 48 55 62 43 54 69--only to family, friends, and/or health workers 25 26 22 28 22 30 33 26 23 29 30 18--not open 18 20 17 24 12 15 20 19 15 29 15 13Total 100 100 100 100 100 100 100 100 100 100 100 100N (AIDS affected families) 286 128 132 147 136 67 40 209 74 49 105 61significance ns ** ns ns *Reaction to family during illness among open cases (%) --no difference from before illness 38 38 39 27 47 23 35 37 40 38 38 42--only negative reaction 17 20 15 20 15 13 42 19 14 5 23 18--only positive reaction 35 30 38 43 28 52 13 35 34 49 34 34--mixed positive and negative reaction 10 13 9 10 11 12 10 10 12 8 5 6Total 100 100 100 100 100 100 100 100 100 100 100 100N (AIDS affected families) 223 104 103 103 120 52 31 165 58 37 79 50significance ns * *** ns nsReaction to family after the death among open cases (%) --no difference from before illness 80 84 80 78 82 75 73 85 68 75 78 88--only negative reaction 8 7 5 11 5 17 13 6 11 6 9 10--only positive reaction 11 9 15 11 12 6 10 8 21 19 12 2--mixed positive and negative reaction 1 1 1 1 1 2 3 1 0 0 1 0Total 100 100 100 100 100 100 100 100 100 100 100 100N (AIDS affected families) 212 92 103 95 117 48 30 156 56 36 81 42significance ns ns ns * ns
Notes for KI data: n=286 cases that the key informant knew best (PHA and PDA). Significance of Pearson's chisquare tests: *p<= 0.05; **p<= 0.01; ***p<= 0.001
Table 4: Range and distribution of community reaction to specific cases that were known about by the community (TACS)
SES of family NGOs work on AIDS in area
Individual and family characteristics
Type of reaction
SexPDA's character
Community characteristics
Duration of epidemic
Total
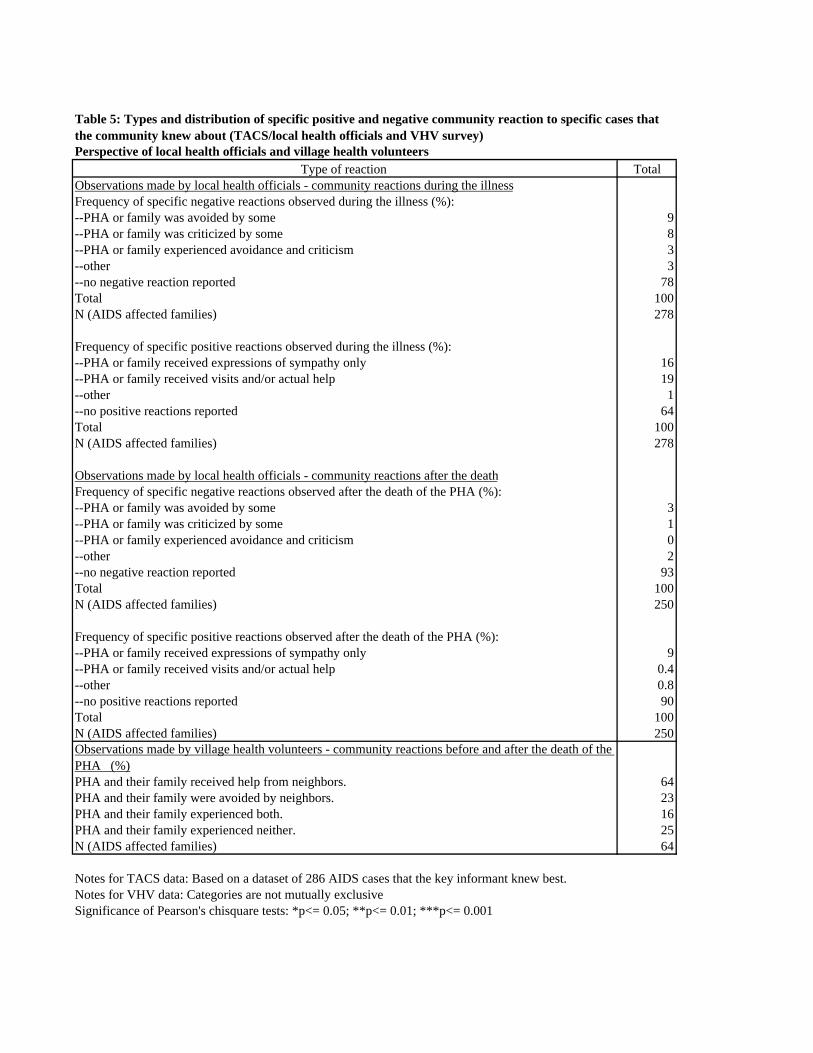
Perspective of local health officials and village health volunteersType of reaction Total
Observations made by local health officials - community reactions during the illnessFrequency of specific negative reactions observed during the illness (%):--PHA or family was avoided by some 9--PHA or family was criticized by some 8--PHA or family experienced avoidance and criticism 3--other 3--no negative reaction reported 78Total 100N (AIDS affected families) 278
Frequency of specific positive reactions observed during the illness (%):--PHA or family received expressions of sympathy only 16--PHA or family received visits and/or actual help 19--other 1--no positive reactions reported 64Total 100N (AIDS affected families) 278
Observations made by local health officials - community reactions after the deathFrequency of specific negative reactions observed after the death of the PHA (%):--PHA or family was avoided by some 3--PHA or family was criticized by some 1--PHA or family experienced avoidance and criticism 0--other 2--no negative reaction reported 93Total 100N (AIDS affected families) 250
Frequency of specific positive reactions observed after the death of the PHA (%):--PHA or family received expressions of sympathy only 9--PHA or family received visits and/or actual help 0.4--other 0.8--no positive reactions reported 90Total 100N (AIDS affected families) 250Observations made by village health volunteers - community reactions before and after the death of the PHA (%)PHA and their family received help from neighbors. 64PHA and their family were avoided by neighbors. 23PHA and their family experienced both. 16PHA and their family experienced neither. 25N (AIDS affected families) 64
Notes for TACS data: Based on a dataset of 286 AIDS cases that the key informant knew best. Notes for VHV data: Categories are not mutually exclusiveSignificance of Pearson's chisquare tests: *p<= 0.05; **p<= 0.01; ***p<= 0.001
Table 5: Types and distribution of specific positive and negative community reaction to specific cases that the community knew about (TACS/local health officials and VHV survey)
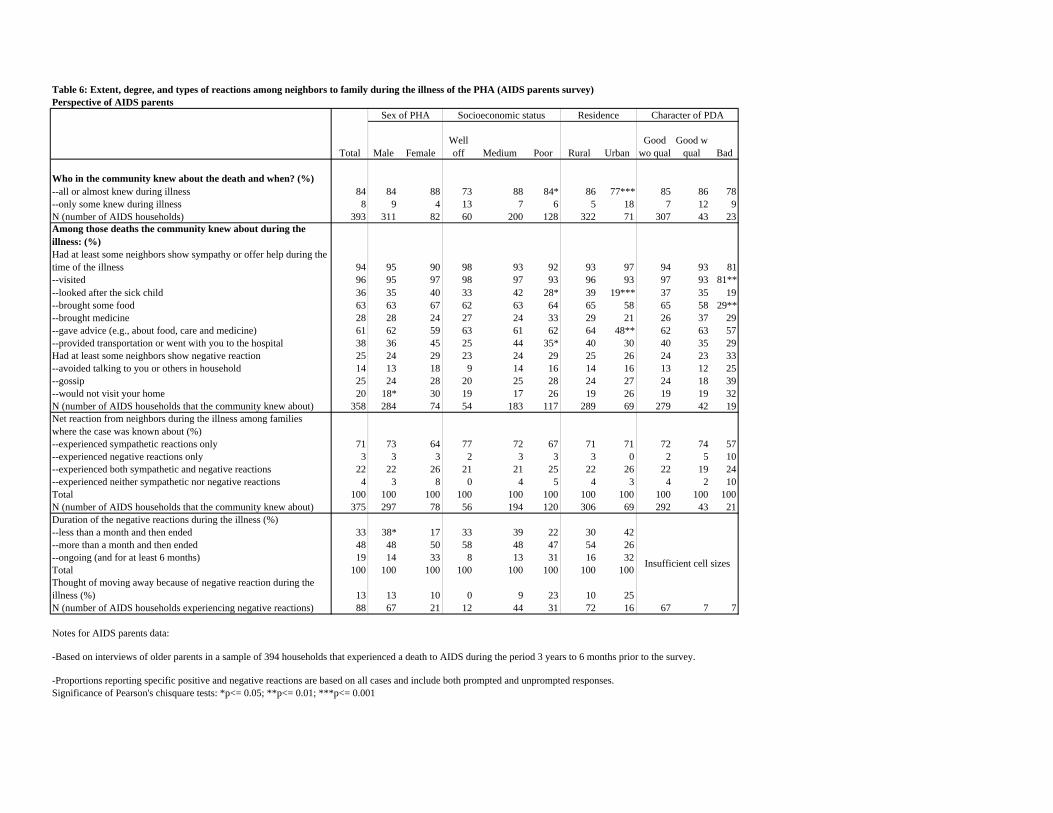
Perspective of AIDS parents
Male Female Well off Medium Poor Rural Urban
Good wo qual
Good w qual Bad
Who in the community knew about the death and when? (%)--all or almost knew during illness 84 84 88 73 88 84* 86 77*** 85 86 78--only some knew during illness 8 9 4 13 7 6 5 18 7 12 9N (number of AIDS households) 393 311 82 60 200 128 322 71 307 43 23Among those deaths the community knew about during the illness: (%)Had at least some neighbors show sympathy or offer help during the time of the illness 94 95 90 98 93 92 93 97 94 93 81--visited 96 95 97 98 97 93 96 93 97 93 81**--looked after the sick child 36 35 40 33 42 28* 39 19*** 37 35 19--brought some food 63 63 67 62 63 64 65 58 65 58 29**--brought medicine 28 28 24 27 24 33 29 21 26 37 29--gave advice (e.g., about food, care and medicine) 61 62 59 63 61 62 64 48** 62 63 57--provided transportation or went with you to the hospital 38 36 45 25 44 35* 40 30 40 35 29Had at least some neighbors show negative reaction 25 24 29 23 24 29 25 26 24 23 33--avoided talking to you or others in household 14 13 18 9 14 16 14 16 13 12 25--gossip 25 24 28 20 25 28 24 27 24 18 39--would not visit your home 20 18* 30 19 17 26 19 26 19 19 32N (number of AIDS households that the community knew about) 358 284 74 54 183 117 289 69 279 42 19Net reaction from neighbors during the illness among families where the case was known about (%) --experienced sympathetic reactions only 71 73 64 77 72 67 71 71 72 74 57--experienced negative reactions only 3 3 3 2 3 3 3 0 2 5 10--experienced both sympathetic and negative reactions 22 22 26 21 21 25 22 26 22 19 24--experienced neither sympathetic nor negative reactions 4 3 8 0 4 5 4 3 4 2 10Total 100 100 100 100 100 100 100 100 100 100 100N (number of AIDS households that the community knew about) 375 297 78 56 194 120 306 69 292 43 21Duration of the negative reactions during the illness (%) --less than a month and then ended 33 38* 17 33 39 22 30 42--more than a month and then ended 48 48 50 58 48 47 54 26--ongoing (and for at least 6 months) 19 14 33 8 13 31 16 32Total 100 100 100 100 100 100 100 100Thought of moving away because of negative reaction during the illness (%) 13 13 10 0 9 23 10 25N (number of AIDS households experiencing negative reactions) 88 67 21 12 44 31 72 16 67 7 7
Notes for AIDS parents data:
Significance of Pearson's chisquare tests: *p<= 0.05; **p<= 0.01; ***p<= 0.001
Table 6: Extent, degree, and types of reactions among neighbors to family during the illness of the PHA (AIDS parents survey)
-Based on interviews of older parents in a sample of 394 households that experienced a death to AIDS during the period 3 years to 6 months prior to the survey.
-Proportions reporting specific positive and negative reactions are based on all cases and include both prompted and unprompted responses.
Total
Insufficient cell sizes
Residence Character of PDASex of PHA Socioeconomic status
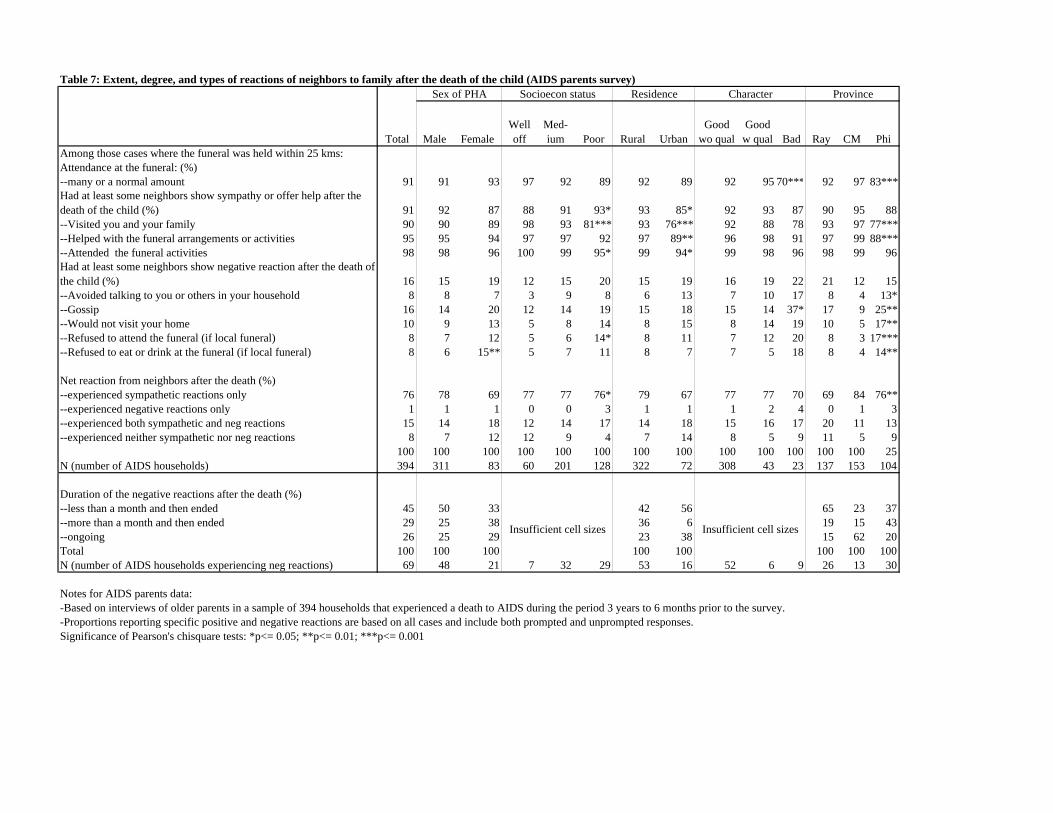
Table 7: Extent, degree, and types of reactions of neighbors to family after the death of the child (AIDS parents survey)
Male Female Well off
Med-ium Poor Rural Urban
Good wo qual
Good w qual Bad Ray CM Phi
Among those cases where the funeral was held within 25 kms:Attendance at the funeral: (%) --many or a normal amount 91 91 93 97 92 89 92 89 92 95 70*** 92 97 83***Had at least some neighbors show sympathy or offer help after the death of the child (%) 91 92 87 88 91 93* 93 85* 92 93 87 90 95 88--Visited you and your family 90 90 89 98 93 81*** 93 76*** 92 88 78 93 97 77***--Helped with the funeral arrangements or activities 95 95 94 97 97 92 97 89** 96 98 91 97 99 88***--Attended the funeral activities 98 98 96 100 99 95* 99 94* 99 98 96 98 99 96Had at least some neighbors show negative reaction after the death of the child (%) 16 15 19 12 15 20 15 19 16 19 22 21 12 15--Avoided talking to you or others in your household 8 8 7 3 9 8 6 13 7 10 17 8 4 13*--Gossip 16 14 20 12 14 19 15 18 15 14 37* 17 9 25**--Would not visit your home 10 9 13 5 8 14 8 15 8 14 19 10 5 17**--Refused to attend the funeral (if local funeral) 8 7 12 5 6 14* 8 11 7 12 20 8 3 17***--Refused to eat or drink at the funeral (if local funeral) 8 6 15** 5 7 11 8 7 7 5 18 8 4 14**
Net reaction from neighbors after the death (%) --experienced sympathetic reactions only 76 78 69 77 77 76* 79 67 77 77 70 69 84 76**--experienced negative reactions only 1 1 1 0 0 3 1 1 1 2 4 0 1 3--experienced both sympathetic and neg reactions 15 14 18 12 14 17 14 18 15 16 17 20 11 13--experienced neither sympathetic nor neg reactions 8 7 12 12 9 4 7 14 8 5 9 11 5 9
100 100 100 100 100 100 100 100 100 100 100 100 100 25N (number of AIDS households) 394 311 83 60 201 128 322 72 308 43 23 137 153 104
Duration of the negative reactions after the death (%) --less than a month and then ended 45 50 33 42 56 65 23 37--more than a month and then ended 29 25 38 36 6 19 15 43--ongoing 26 25 29 23 38 15 62 20Total 100 100 100 100 100 100 100 100N (number of AIDS households experiencing neg reactions) 69 48 21 7 32 29 53 16 52 6 9 26 13 30
Notes for AIDS parents data: -Based on interviews of older parents in a sample of 394 households that experienced a death to AIDS during the period 3 years to 6 months prior to the survey. -Proportions reporting specific positive and negative reactions are based on all cases and include both prompted and unprompted responses. Significance of Pearson's chisquare tests: *p<= 0.05; **p<= 0.01; ***p<= 0.001
Residence Character Province
Total
Insufficient cell sizes Insufficient cell sizes
Sex of PHA Socioecon status
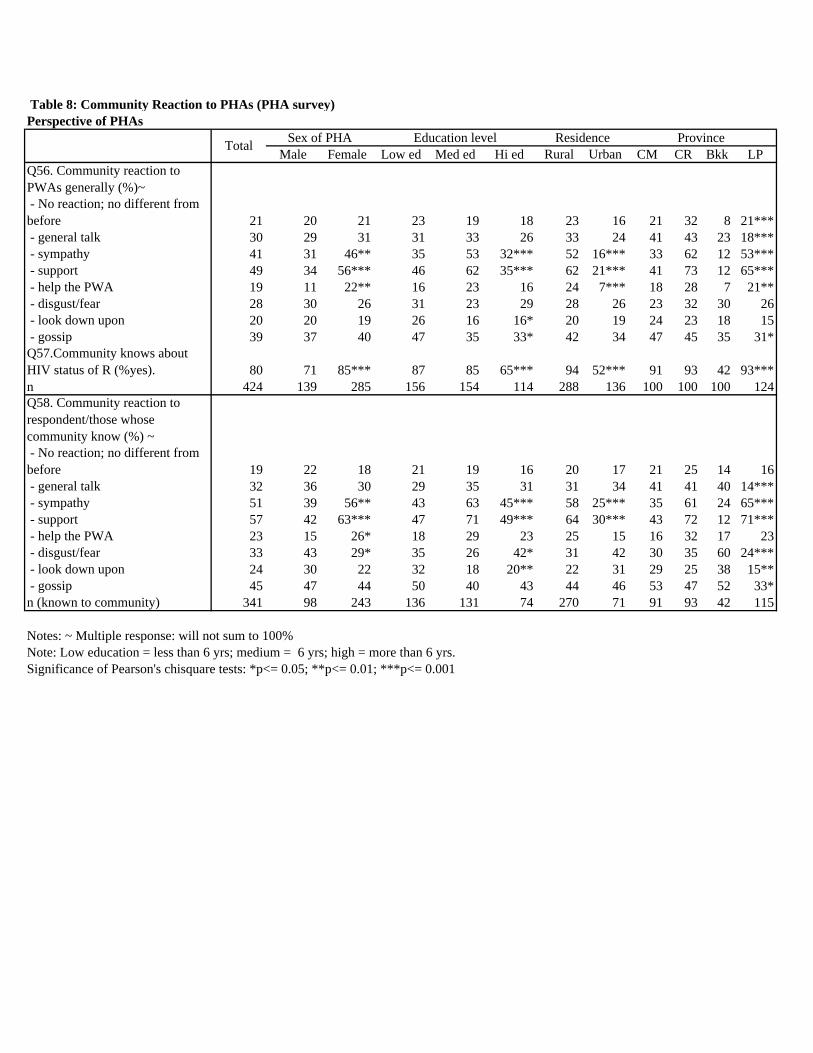
Table 8: Community Reaction to PHAs (PHA survey)Perspective of PHAs
Male Female Low ed Med ed Hi ed Rural Urban CM CR Bkk LPQ56. Community reaction to PWAs generally (%)~ - No reaction; no different from before 21 20 21 23 19 18 23 16 21 32 8 21*** - general talk 30 29 31 31 33 26 33 24 41 43 23 18*** - sympathy 41 31 46** 35 53 32*** 52 16*** 33 62 12 53*** - support 49 34 56*** 46 62 35*** 62 21*** 41 73 12 65*** - help the PWA 19 11 22** 16 23 16 24 7*** 18 28 7 21** - disgust/fear 28 30 26 31 23 29 28 26 23 32 30 26 - look down upon 20 20 19 26 16 16* 20 19 24 23 18 15 - gossip 39 37 40 47 35 33* 42 34 47 45 35 31*Q57.Community knows about HIV status of R (%yes). 80 71 85*** 87 85 65*** 94 52*** 91 93 42 93***n 424 139 285 156 154 114 288 136 100 100 100 124Q58. Community reaction to respondent/those whose community know (%) ~ - No reaction; no different from before 19 22 18 21 19 16 20 17 21 25 14 16 - general talk 32 36 30 29 35 31 31 34 41 41 40 14*** - sympathy 51 39 56** 43 63 45*** 58 25*** 35 61 24 65*** - support 57 42 63*** 47 71 49*** 64 30*** 43 72 12 71*** - help the PWA 23 15 26* 18 29 23 25 15 16 32 17 23 - disgust/fear 33 43 29* 35 26 42* 31 42 30 35 60 24*** - look down upon 24 30 22 32 18 20** 22 31 29 25 38 15** - gossip 45 47 44 50 40 43 44 46 53 47 52 33*n (known to community) 341 98 243 136 131 74 270 71 91 93 42 115
Notes: ~ Multiple response: will not sum to 100%Note: Low education = less than 6 yrs; medium = 6 yrs; high = more than 6 yrs. Significance of Pearson's chisquare tests: *p<= 0.05; **p<= 0.01; ***p<= 0.001
Sex of PHA Education level Province Total Residence
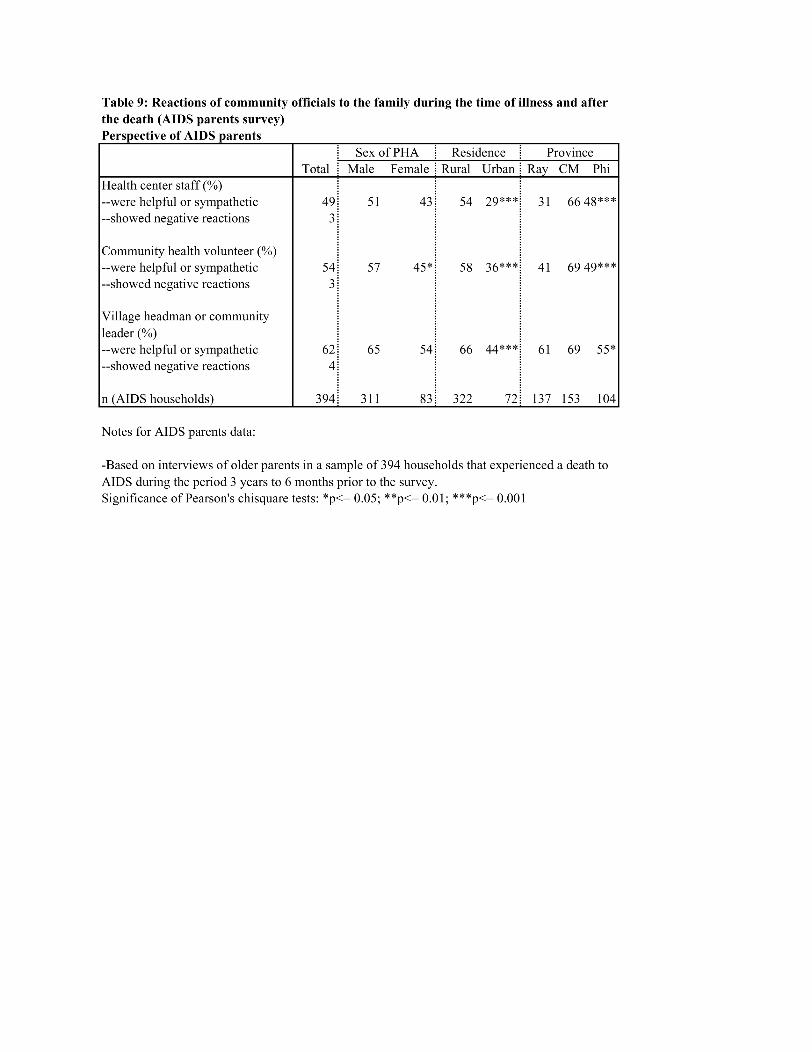
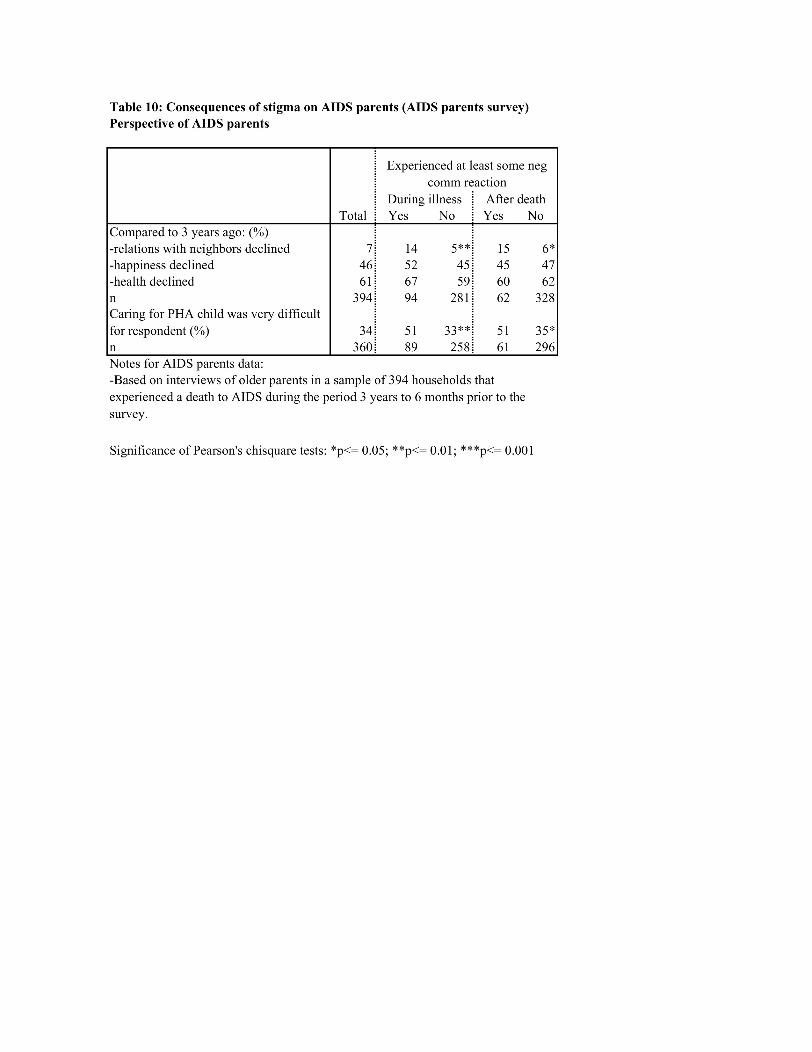





























![AIDS Research and Therapyquality of life of persons living with human immunodeficiency virus (HIV) infection [1]. Nevertheless, 17-32% of HIV infected persons living in countries with](https://img.pdfslide.us/doc/110x75/5e4c03c7b4174d2ec3675323/aids-research-and-therapy-quality-of-life-of-persons-living-with-human-immunodeficiency.jpg)