Embed Size (px)
Citation preview

PERSPECTIVES IN PSYCHIATRIC CARE
Dear Judge K,
Per our verbal agreement, I will be attending Albany Police Court each Thursday from 1O:OO am to 12:OO pm beginning 2/8/79 to serve as a mental health consultant. A s we agreed, I will be available to assess any cases where the client’s emotional stability may be in question and make recommen dations on these cases. Listed below are my objectives for this program:
1. Psychiatric Center client facing Legal prosecution.
To identify treatment needs of any identified Capital District
2. To determine the extent to which such legal action may be imple- mented in accordance with treatment plans of CDPC clients.
3. To educate the court system to the special needs of psychiatric clients.
4. behavior, but it is, at times, illegal behavior.
To promote the concept that “acting out“ behavior is not “sick“
5 . To support court efforts toward clients seeking psychiatric treatment as part of the terms for probation when indicated.
6. To identify those people facing legal charges who may benefit from outpatient psychiatric treatment.
After a three-month period I would like to meet with you to assess the usefulness of this program both for you and Capital District Psychiatric Center.
I look forward to working with you.
Sincerely, Jean Moore, R.N., M . S .
204

Volume XVl l l No. 5 1980
1 was the writer of that letter, a community mental health nurse working on one of the Albany County Unit out- patient teams of Capital District Psychiatric Center.
I first became aware of the need for a consul- tative program with Albany Police Court at an in- ter-agency case conference at which Judge K, the Albany Court judge involved in the case, was pre- sent. As the conference progressed, Judge K commented on the lack of professional support between the Albany Police Court and the Albany County Unit of the Capital District Psychiatric Center. Judge K was seeing a number ofthe Cen- ter’s problematic clients regularly in Police Court and suggested that the Albany County Unit could assist the court by providing psychia- tric evaluation of these clients. Previously, when I had consulted with Judge K about a client fac- ing legal charges, I had found him receptive to further cooperative efforts in providing more ap- propriate treatment for psychiatric clients in the legal system. Thus, both Judge K and I shared a similar perception of need.
The next step involved obtaining support from the administration of Albany County Unit on the implementation of a mental health consultation program with Albany Police Court. Since such a program was well within the scope of the unit’s goals, approval was forthcoming,
Capital District Psychiatric Center is a state psychiatric facility which provides a range of psychiatric services to a nine-county area of New York State. The Albany County Unit of Capital District Psychiatric Center is composed of two inpatient units and three multi-disciplinary out- patient teams serving the county. The Albany County Unit is committed to the community mental health model of treatment. Its 1979 state- ment of goals states:
0 To work directly with community-based agen- cies in planning, coordinating and sharing mental health services within the County of Albany.
0 T o provide community treatment services and programs which will assure support for those cli- ents residing in the community and will minimize inpatient treatment. 0 T o maintain and promote healthy interpersonal functioning in all clients. 0 To establish and maintain a system of coor- dinated services which will assure continuity be- tween inpatient and outpatient care. 0 To provide short term emergency services to persons in acute emotional distress.
To train health and mental health students in community mental health. 0 To provide educational and consultative ser- vices to those community agencies relating to the population served by the Albany County Unit. 0 To provide direct counseling and psycho- therapy services to individuals and families who re- quire such help.
Point of Entry The first phase of the consultative process in-
volves building a relationship between the con- sultant and consultee. (Busser, 1972; Caplan, 1970; DeLoughery, Gebbie and Newman, 197 1) One of the most important aspects of the entry phase is that both consultant and consultee are congruent on perception of need (Glidewell, 1956). In fact, Grossman and Quinlan (1972) cite lack of this congruence as one probable cause for the failure of a consultative program attempted in a small community hospital.
Judge K identified his problem as his lack of knowledge about the psychological factors that can affect behavior - especially illegal behavior. He asked for input from a mental health profes- sional every week to help him understand the in- fluence of the psychological factors affecting per- sons facing legal charges and recommendations as to the most appropriate course of action.
The next step in building a relationship with an agency comes with defining the consultants’ role (Glidewell, 1956). According to Gibb (1956), this is the diagnostic stage of the entry phase in which the specifics of the problem are clearly identified
205

PERSPECTIVES IN PSYCHIATRIC CARE
and, based on this, the role of; the consultant is readily perceived. For me this entailed one brief meeting with Judge K, at which time we estab- lished the time for the consultation process to begin. It was following that meeting that my let- ter, defining the boundaries of my role, was formalized.
The first stage of the entry phase entails the ini- tial development of a coordinate relationship, i.e., one based on competence, respect, and inter- dependence. (Busser, 1972) As I initiated consul- tative services, such a relationship emerged. After the first three sessions, it became apparent that not only did Judge K require consultative help, but others also. As I demonstrated my skill as a consultant each week, I received requests for assistance from the District Attorney’s Office and the Public Defender’s Office. Thus, as my in- volvement increased and the reliability of my judgment became established, a trusting relation- ship developed.
Problem-Solving Phase Mental health consultation has been defined as
“a provision for technical assistance by an expert to individuals and agency care givers related to the mental health dimensions of their work.” (Mannino, Maclennan and Shore, 1975) Three types of consultation are identified by Schwab (1 968): 1) patient-oriented; 2) consultee-oriented; and 3 ) situation oriented. As the community mental health nurse consultant, I provided pa- tient-oriented, “technical assistance” to the Albany Police Court. Consultation sessions usu- ally began with an initial request by Judge K for me to speak with apprehended individuals- anywhere from two to six- whose behavior dur- ing or after an alleged crime indicated acute or chronic emotional distress. I would introduce myself, speak with each person briefly-any- where from 10 to 20 minutes-to determine the presence of emotional distress and its impact on the individual’s behavior. I would also try to es- tablish whether the person was currently receiv-
ing outpatient psychiatric treatment. Once the evaluation was completed, I would discuss my findings with Judge K and make recommenda- tions for the most appropriate course of action for each person evaluated. The staff from the Dis- trict Attorney’s Office and the Public Defender’s Office made similar requests which I handled in the same way. In addition to problem solving, I endeavored to share with the court staff the rea- soning behind my recommendations.
Consultative experience with the Albany Police Court entailed my building a strong, trusting relationship with an agency whose philo- sophical tenets were diametrically opposed to my own. While a court system is concerned with maintaining an ordered society, as a psychiatric nurse specialist I was concerned with a human- istic respect for individuals, and their capacity to assume responsibility for their actions. This philosophical divergence greatly affected my role as a consultative change agent. I had to plan my interventions carefully and devise appropriate strategies for presenting my theoretical frame- work to the court staff. I learned that effec- tive strategies were as important as good timing.
The mental health consultative experience is, in some ways, similar to psychotherapy. Both re- quire a specialist in a mental health profession to develop a strong, positive alliance with a person or a system of people, and to use this relationship in promotion of change and growth in each other toward the goal of mental health.
An Example of Consultation Louis, a 22-year-old single man, was arrested
two days before his arraignment for provoking an altercation in a restaurant. He had eaten a meal there, was unable to pay for it, argued with the manager, and subsequently ripped a pay phone off a wall of the restaurant. After his arrest, Louis talked “strangely.” I was asked to speak with him before his arraignment. Both Judge K and a law- yer from the Public Defender’s Office commented on how “crazy” this man was.
206

Volume XVl l l No. 5 1980
When asked to explain his current circum- stances, Louis explained he had extra sensory powers which enabled him to read minds. He had been reading minds since he was 14, and enjoyed relating at a “cosmic level,” but sometimes “got lost.” He also said he received public assistance and food stamps, but ate at the restaurant on a day he had no money or food stamps. But he in- tended to repay the restaurant as soon as he re- ceived his monthly food stamp allocation. When asked why he thought he could eat in a restaurant without paying right away, Louis replied that his extra sensory powers gave him‘ extra privileges. When asked what he was doing in jail if this were so, he said that now he realized he was wrong.
Louis had moved to Albany from Florida six months before. He had his own apartment, and was a maintenance worker in the work relief pro- gram. While in Florida, he had completed two years of college, had two brief psychiatric hospi- talizations, and about three years ago had been ar- rested under circumstances identical to those which led to his current arrest. He stated that one week before the arrest he had voluntarily sought outpatient psychiatric services and was sche- duled to be seen for an initial evaluation that day.
My assessment ofthis client was that despite an on-going, chronic thought disorder, he managed extremely well. Louis’s description of his power to read minds, and his tendency to sometimes get lost in “cosmic communication” could be inter- preted to mean he had weak ego boundaries and feared losing the boundaries completely under the stress of close interpersonal contact. He, therefore, tended to “distance” himself from others as a defense. His current situation, that is, establishing himself in Albany, indicated a capa- city to care for himself. Another indication of Louis’s high functional capacity was his plan to seek psychiatric help one week before the acting- out episode occurred; i.e., just before his arrest, he was seeking an appropriate resource to help him maintain emotional control and support his efforts to function independently.
Louis’s acting-out behavior did appear to be re- lated to his thinking disorder; therefore, his men- tal state seemed to contribute to his criminal be- havior. Based on this assessment, I thought the most appropriate course of action would be for this client to be probated, conditional on his con- tinued involvement in outpatient psychiatric treatment.
In explaining my assessment and recommenda- tion to Judge K and the Public Defender, I did not refute their position that Louis was “crazy,” but merely pointed out that despite his “crazi- ness” he was capable of functioning in a relative- ly stable fashion. Judge K and the Public De- fender both spoke with Louis, reviewing his past history and examining his current situation. Both concurred with my recommendation for action. Louis was sentenced to three-years probation on the condition that he engage in outpatient psy- chiatric treatment during that time.
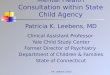
According to Busser( 1972), the process of con- sultation has three distinct goals: 1) provide new accurate information, 2) assist the consultee to fulfill his responsibility, and 3) help the consultee with attitudinal blocks. Transactions such as the one I have described facilitate achievement of the goals of consultation.
The diagram on p. 208 illustrates how lack of knowledge of psychological factors led to a com- munication breakdown between the court staff and Louis. Similar to the diagram devised by De- Loughery, Gebbie, and Newman( 1971), it illu- strates how the consultative process provided new information which assisted the consultee- and Judge K and the Public Defender - toward a better understanding of the mental health aspects of their case.
Evaluation I attempted to build in a mechanism for evalua- tion in the program design. My letter to Judge K, in which the boundaries of the program were de- fined, included a plan to evaluate the impact of the mental health consultation program after
207

PERSPECTIVES IN PSYCHIATRIC CARE
I
CLIENT
Intervention
Louis is arrested I
CON SU LTE E
Uses Intervention
stress of jail increases and enhances disorganized thinking
-----------
CO NSU LTANT
Confuses Data Due to Lack of Information
Louis is viewed
Sends More Data
makes grandiose delusional statements in jail as “crazy”
--_-----
Louis
Sends Data
‘IHe crazy”
Judge K Public Defender
+m Matches Data to
Before ’
Consultation: Synthesizes Data with Theory -------- Unstructured Data
-------- restaurant behavior in restaurant
Intervention -
I
Theory ------- data seen as vague and unclear
Evaluates Accuracy Uses Intervention of Data
no stress; able to participate Sends More Data appropriately in interview 9 sees need to educate
_--_------- --------
Louis reveals more of himself i
court staff; assesses level of trust; selects message
CI Utilizes New Intervention
New Intervention -
I
Re-evaluates Position in Intervention Light of New Information < Louis is considered crazy
presents a more complete picture
- - - - - - - - - but functional of Louis conditional probation
I J L I
I Sends Data
“That was helpful” >
208
Evaluates

Volume XVl l l No. 5 1980
three months. Thus, both consultant and consul- tee could evaluate the effects of the program.
Program evaluation is an essential component of consultation. The first step in the process is to examine the goals and objectives of the program and compare them to actual outcome. Caplan states that the two major goals of consultation are “to help the consultee improve his handling or understanding of the current work difficulty and through this to increase his capacity to master future problems of a similar type.”( 1970, p. 29) Based on these goals and the more specific objec- tives of the consultative program, I have identi- fied three major areas of outcome for evaluation: 1) effect on the mental health of clients; 2) effect on consultee performance, and 3) effect on con- sultee attitude. (Mannino and Shore, 1972; Cap- lan, 1970)
Researchers agree that the optimal method of program evaluation entails the use of experimen- tal design,(Caplan, 1970; Mannino and Shore, 1972) Currently, I have neither the time nor the resources to implement a program evaluation based on experimental design; therefore, I must focus on subjective evaluation. The program was evaluated in May, 1979, and was found to be useful to both the Albany Police Court staff and the Albany County Unit of Capital District Psy- chiatric Center. Because of the positive feedback, the program continues to operate. In fact, plans are currently underway to expand the con- sultant’s role in the Albany Police Court as the program’s effectiveness receives increasing attention.
Conclusions The trend toward community mental health
within the psychiatric field has meant a broader role for mental health professionals in promoting emotional well being within the community. One such emergent role is that of the mental health consultant who functions to support and educate community care-giving agencies. With the ulti- mate goals of enhancing the competence of such
agencies in more clearly recognizing emotional distress in clients, the mental health consultant assists clients, as indicated, in receiving the ne- cessary help to restore emotional well being, and consequently, reduces the incidence of emotional distress in clients.
References Altrocchi, J., “Mental Health Consultation,” Handbook of
Community Mental Health, Galann and Eisdorfer (eds.) New York: Appleton-Century-Crofts, 1972.
Busser, A., Mental Health Consultation and Education, Paio Alto, California: National Press Books, 1972.
Caplan, G., The Theory and Practice of Mental Health Con- sultation, New York: Basic Books, 1970.
Caplan, G., “Types of Mental Health Consultation,” Am- erican Journal of Orthopsychiatry, 1963, 33, pp. 470-481.
DeLoughery, G., K. Gebbie and B. Newman, Communi- ty Mental Health Nursing: Consultation and Community Organization, Baltimore: Williams and Wilkins, 197 1.
Gibb, J., “The Role of the Consultant,” The Journal of So- cial Issues, 1956, 15, pp. 1-4.
Glidewell, J., “The Entry Problem in Consultation,” The Journal of Social Issues, 1959, 15, pp. 51-59.
Grossman, F. and D. Quinlan, “Mental Health Consul- tation to Community Settings: a Case Study of a Failure to Achieve Goals,” Handbook of Community Mental Healrh, Golann and Eisdorfer (eds.), New York: Apple- ton-Century-Crofts, 1972.
Hallock, A. and W. Vaughn, “Community Organization- a Dynamic Component of Community Mental Health Practice, Journal of Orthopsychiatry, 1956, 26, pp.
Joint Commission on Mental Illness and Health, Action f o r Mental Health, New York: Basic Books, 1961.
Lippitt, R., “Dimensions of a Consultant’s Job,” The Jour- nal ofsocial Issues, 1959, 15, pp. 5-12.
Mannino, F., B. Maclennan and M. Shore, The Practice of Mental Health Consultation, New York: Gardiner Press, Inc., 1975.
Mannino, F. and M. Shore, “Research in Mental Health Consultation,” Handbook of Community Mental Health, Golann and Eisdorfer (eds.), New York: Appleton-Cen- tury-Crofts, 1972.
Mendel, W. and P. Solomon (eds.), The Psychiatric Consul- tant, New York: Grune and Stratton, 1968.
Parker, B., Mental Health Inservice Training: Some Practical Guidelines for the Psychiatric Consultant, New York: In- ternational Universities Press, 1968.
Schwab, J., Handbook of Psychiatric Consultation, New York: Appleton-Century-Crofts, 1968.
691-706.
209