Embed Size (px)
DESCRIPTION
Â
Citation preview

Electronic copy available at: http://ssrn.com/abstract=2164353Electronic copy available at: http://ssrn.com/abstract=2164353
! Community Health Insurance
An alternative for extending financial protection to excluded populations
Amardeep S Bhatia Commissioner & Secretary Government of Nagaland

Electronic copy available at: http://ssrn.com/abstract=2164353Electronic copy available at: http://ssrn.com/abstract=2164353
Page%|%2
Table!of!Contents!Executive)Summary)........................................................................................................................)3
1 Introduction)........................................................................................................................)3
2 Community)Health)Insurance)and)Community)Health)Financing).......................................)4
3 Dissecting)Community)Health)Insurance)(CHI))schemes.)...................................................)5
Design)Characteristics).............................................................................................................)5
Revenue%Collection)................................................................................................................)5
Pooling)..................................................................................................................................)7
Purchase%of%Services)..............................................................................................................)7
Management)characteristics)..................................................................................................)7
4 Outcomes)from)CHI)schemes.)............................................................................................)8
Resource%Mobilisation)...........................................................................................................)8
Financial%Protection)..............................................................................................................)9
Social%Inclusion)......................................................................................................................)9
5 Building)on)the)experience)gained)–)Scaling)up.)................................................................)9
Pre;requisites)......................................................................................................................)10
Designing%CHI%Schemes).......................................................................................................)10
Managing%CHI%Schemes)......................................................................................................)12
Government%interventions)..................................................................................................)12
6 CHI)and)National)Rural)Health)Mission,)India)...................................................................)13
7 Conclusions).......................................................................................................................)14
References)....................................................................................................................................)16
Endnotes).......................................................................................................................................)18
!

Executive!Summary!
Community)Health)Insurance)(CHI))schemes)provide)an)alternative)to)resource)constrained)low)and)middle) income) countries) to) increase) financial) resources) available) to) the) health) sector) as)well) as)extend) financial) protection) to) excluded) populations,) comprising)mostly) the) rural) and) informal) sector)and)consisting)of)more) than)a)billion)of) the)world’s)poor.)CHI) schemes)have)had)modest) success)and)require) careful)designing) to)meet) the)needs)of) the) community)and) their)high) level)of) involvement) to)meet) the) health) objectives) of) providing) affordable) and) equitable) access) to) all.) There) are) unresolved)issues) with) regard) to) sustainability,) high) administrative) costs,) ability) to) include) the) poorest,) etc.)However,) it) is) a) viable) alternative) which) can) supplement) national) efforts) at) universal) financial)protection.) Drawing) on) the) abundant) literature) on) the) subject,) the) paper) examines) the) key)characteristics) of) the) CHI) schemes) and) drawing) on) the) successful) interventions,) suggests) the)requirements)for)scaling)up)CHI)initiatives.)Lastly,)the)paper)examines)how)CHI)initiatives)can)be)used)in)the) case) of) India) and) suggests) some) policy) recommendations) for) incorporation) in) the) national)framework.)
1 Introduction!)Financing)and)providing)healthcare)to)the)world’s)more)than)1.3)billion)poor)people)who)live)in)the)
low)and)middle) income)countries)and)who)do)not)have)equitable)and)affordable)access) to)healthcare)services)is)one)of)the)world’s)most)challenging)and)urgent)problems1.)Weaknesses)in)the)financing)and)delivery)of)healthcare) is)a)major)cause)for) lack)of)access)to)effective)and)affordable)health)services)to)the) poor) and) the) effects)may)manifest) in) the) nonZavailability) of)manpower,) inadequate) government)health) centers) and) hospitals) or) their) inefficient) functioning.) According) to) estimates) made) for)Commission)for)Macroeconomics)in)Health)(2001),)the)expenditure)gap)for)achieving)universal)access)to)health) services) at) low) income) levels) through) public) financing) mechanisms) like) social) insurance) and)general)revenues)range)from)US$)25–50)billion)to)over)US$)100)billion)(Ron)1999;)Preker)et)al.)2002).)))
High) and) middle) income) countries) have) been) able) to) put) in) place) systems) to) use) general)revenues) and) have) developed) the) instrument) of) universal) social) insurance) for) providing) affordable)access)to)healthcare)for)its)citizens.)Universal)Social)insurance,)which)combines)the)principles)of)pooling)and) preZpayment) to) equalize) inequities) by) crossZsubsidizing) for) health) risk,) income) level) and) from)productive) to) nonZproductive) part) of) the) life) cycle) is) a) desirable) objective) for) providing) adequate)healthcare) and) population) coverage.) Countries) who) have) achieved) universal) coverage) through) social)insurance)have)taken)long)transition)periods)to)do)so.)Large)informal)sectors)and)rural)populations)limit)the) extension) of) the) scheme) in) low) and) middle) income) countries.) Limited) tax) base) and) competing)demands)on)public) funds)have) limited)the)ability)of)the) low)income)countries)to) increase)government)spending)on)healthcare)also.)Looking)at)this)from)the)policy)perspective,)healthcare)financing)in)the)low) 1 Expenditure on health varies from a high of US$2636 per capita in the Americas to a very low of US$ 31 per capita in South East Asia (World Health Statistics 2009)

Page%|%4
and)middle)income)countries)can,)therefore,)typically)be)characterized)by)government)as)well)as)market)failure,)in)the)inability)of)governments)to)organize)public)finance)and)exercise)oversight)over)the)health)sector)as)well)as)market) failure) in) supplying)services)as)per) the)ability) to)pay) leading) to)an)unfulfilled)demand/need)gap)(Dror)and)Preker)2002;)Gottret)and)Schieber)2006).)
This) inability)to)provide)social) insurance)or)public)healthcare)facilities)has) led)to)a)high) ‘out)of)pocket’) expenditure) by) households) at) the) point) of) accessing) services,) which) can) be) stressful) during)catastrophic)events)and)drive)households)into)poverty.)As)per)the)World)Health)Statistics)2009,)share)of)government) in) health) spending) varies) from) 76%) in) Europe) to) 34%) in) SouthZEast) Asia) and) where)government)expenditure) in)health) is) low,) the) shortfall) is)made)up) in) lowZincome)countries)by)private)spending,)about)85%)of)which)is)out)of)pocket.))
) Recognizing) this,) other) methods) have) therefore) been) employed) by) governments,) using)communities)directly) in)health) financing.)Communities)have,) themselves,) led) initiatives) to)provide)risk)protection) against) cost) of) illness) using) the)principles) of) pooling) and)preZpayment.) These) subZnational!community!health!financing)schemes)have)been)particularly)used)in)subZSaharan)Africa,)Asia)and)Latin)America.) These) have) been) accompanied) by) or) followed) institution) of) decentralization) that) some) of)these)countries)undertook,)or)as)an)offshoot)of)the)success)of)microZcredit)schemes,)or)independently)as)a)part)of)income)protection)measures)or)to)fill)the)voids)created)by)missing)institutions)(Jütting 2004; Schneider 2004).)
2 Community!Health!Insurance!and!Community!Health!Financing!!)
The) term)community%health% financing) has)been)used)as) ‘a%generic%expression% to% cover%a% large%variety%of%health%financing%arrangements’,)describing)micro)health) insurance,)community)health)funds,)revolving) drug) funds,) community) involvement) in) user) fee) management,) rural) health) insurance) and)mutual)health)organizations)(Dror and Preker 2002).)All)of)these)instruments,)though)vary)in)the)extent)of) their) prepayment) and) risk) sharing,) in) their) resource) allocation) mechanisms,) organizational) and)institutional)characteristics,)exhibit)a)number)of)common)features)viz.)community)control)for)mobilizing,)pooling,) allocating,) managing) and/or) supervising) health) care) resources,) principles) of) voluntary)participation)and)builtZin)solidarity)mechanisms))and)generally)involve)those)who)do)not)have)access)to)general)tax)based)health)services)or)social)insurance)schemes(Hsiao 2001; Arhin-Tenkorang 2001).)The)term)community)is)used)here)in)its)broader)definition)to)describe)characteristics)of)‘social)fellowship’)or)‘people)organized) into) common)political,)municipal) or) social) unity’) (Oxford)definition)of) ‘community’) (Jakab 2001).) Community) based) health) funds) have) existed) for) centuries) and) some) of) the) nineteenth)century)schemes)in)Europe)and)Japan)were)a)preZcursor)to)the)modern)day)social)insurance)schemes1.)China)had)a)nationwide)community)based)and)managed)program)in)the)1950s)which)it)had)to)abandon)on)demise)of)the)cooperative)farms,)which)it)has)revived)again.)Recent)initiatives)were)spurred)by)the)Declaration)of)Alma)Ata,)Bamako)Initiative)and)the)Commission)for)Macroeconomics)in)Health)(Bennett)2004;) Ogawa) et) al.) 2003;) Carrin,) Waelkens,) and) Criel) 2005).) There) is) a) growing) interest) in) these)initiatives) in) the) recent) years) as) can) be) seen) from) the) growing) number) of) such) schemes) in) Asia) and)

Page%|%5
Africa)and)the)large)amount)of)literature)that)has)been)churned)out)on)the)subject)(Sara Bennett 2004; Molyneux et al. 2007; Ekman 2004)2.)
Though) ‘community) health) financing’) and) ‘community) health) insurance’) (CHI)) has) been) used)interchangeably)in)literature,)we)need)to)differentiate)between)the)two.)To)be)termed)as)an)insurance)scheme3,)an)activity)has)to)satisfy)the)requirements)of)pooling)risk)across)group)of)individuals)based)on)a)contract)between)the)insured)and)the)insurer.)The)contract)defines)contributions)(preZpayments))from)the)insured)for)covering)a)preZdefined)part)of)the)cost)of)care)by)the)insurer)with)regard)to)health)needs)(benefit)package))over)a)defined)period)in)the)future)(Dror and Preker 2002, Chapter 5).)In)addition)to)the)insured)(client))and)the)insurer,)in)order)to)be)operational,)a)health)insurance)scheme)also)requires)a)health)care)provider)to)provide)health)services.) )CHI)may,)therefore,)be)restricted) in) its)definition)to)those)‘schemes!managed!and!operated!by!an!organization,!other! than!a!government!or!private! for8profit! company,! that! provide! risk! pooling! to! cover! all! or! part! of! the! costs! of! health! care!services’(Bennett 2004)) or) alternatively) as) voluntary) health) insurance) schemes,) organized) at) the)community)level)and)having)the)common)characteristics)of)being)run)on)a)nonZprofit)basis)and)applying)the)basic)principle)of)‘risk)sharing’)(Carrin, Waelkens, and Criel 2005).))
The!rest!of!the!paper!deals!with!Community!Health!Insurance!(CHI)!schemes!as!defined!in!the!above!paragraph.!!
3 Dissecting!Community!Health!Insurance!(CHI)!schemes.!)
Community) Health) Insurance) (CHI)) uses) the) basic) health) insurance) principles) of) pooling) and)prepayment) to)purchase)health)services)and) involves)community) in) its)management.)The)basic)health)insurance) function) can)also)be) classified) (corresponding) to)health) financing) subZfunctions)) as) revenue)collection,)pooling)and)purchase)of)services)and)determine)the)design)of)a)scheme.)These)are,)therefore)called) the)design! characteristics) of) the) scheme.) The) configuration) in)which) the) communities)manage)these)functions)can)be)broadly)classified)as)the)management!characteristics)of)the)scheme.)In)view)of)the) flexibilities) and) adaptations) to) local) communities) needs,) there) are)many) different) configurations)available,) which) are) presented) in) this) section) under) the) above) two) broad) characteristics) of) the) CHI)schemes.)Elements)of)the)framework)in)Preker)et.)Al)(Preker)2001),)Jakab)and)Krishnan)(Jakab)2001))and)G.Carrin)(Carrin, Waelkens, and Criel 2005))have)been)used)in)the)analysis)that)follows.)
Design!Characteristics!
Revenue!Collection!Revenue) collection) is) dependent) on) the) extent) of) enrolment) of) the) community) and) the)contributions/collections)from)members)and)external)sources.)The)higher)the)collection,)the)greater) is)the)health)coverage)and)the)corresponding)financial)risk)mitigation.)))

Page%|%6
Contributions! and! collections! from! members) are) in) the) form) of) preZpayments,) coZpayments) and)deductibles.)PreZpayments)help) in)avoidance)of) financial) consequences)of) treatment)costs)and)secure)access) to) care) when) it) is) needed.) High) prepayments) may) protect) households) from) excessive) or)‘catastrophic’)healthcare)expenditure.)However,)high)prepayments)keep)the)poor)excluded)from)these)schemes)while)low)payments)make)their)sustainability)difficult)or)dependent)on)external)assistance.)CoZpayments)and)deductibles)are)out)of)pocket)expenditures)along)with)exclusions)and)limits)on)payments.)The)higher)the)‘out)of)pocket)expenditures’,)the)greater)is)the)disincentive)for)the)poor)to)be)included)in)these)schemes)and)the)limit)on)its)usefulness)(Carrin,)Waelkens,)and)Criel)2005;)Hong)et)al.)2005;)Preker)et)al.)2002).))The) schemes) also) receive) contributions! from! national,! provincial! governments,! NGOs! and! foreign!donors.)Greater)contribution)from)external)sources)has)the)potential)to)weaken)the)bonding)within)the)community) and) selfZreliance,) it) has) become) a) key) determinant) of) sustainability) (Jakab) 2001,)Supakankunti)1997,)Atim)1998;)Carrin,)Waelkens,)and)Criel)2005).)However,)as)demonstrated)in)the)case)of) the)China)CHI,)even)with)government)subsidies,)participation)rates)may)not)be)high) if)enrolment) is)only)voluntary)(Zhang)et)al.)2006).)))Enrolment) to) CHI) schemes) is) voluntary) in) nature,) have) largely) poor) members) and) is) determined) by)various) factors) viz.) ) affordable) premium) levels,) timing) of) collection,) cultural) aspects,) trust) in) the)healthcare)system,)distance)from)provider)and)quality)of)care.)The)larger)the)percentage)of)enrolment)from)the)participating)community,)the)greater)the)spread)of)the)risk)and)greater)the)revenue)collection)for)meeting) the)costs.)Affordability)of) the)contribution) is)an) important)consideration) in)a)household’s)decision) to) enroll,) which) depends) on) the) ability) to) pay) and) the) willingness) of) a) household) which) is)dependent)on)the)magnitude)of)poverty,)anticipated)benefits) from)the)scheme,)the) losses/costs) likely)due) to) ongoing) or) future) illZhealth) and) social) network/support.) Similarly,) collection) of) premiums)corresponding)to)the)income)patterns)of)the)members)play)an)important)role)in)promoting)enrolment)of)the)poorer)households.)On)the)one)hand,)annual)lump)sum)payments)corresponding)to)harvest)of)cash)crops)may)be)convenient)and)is)prevalent)in)many)schemes,)it)may)be)a)hindrance)for)others)who)may)find) smaller) monthly) or) quarterly) payments)more) suitable.) Good) geographical) accessibility) to) health)facilities) is) also) correlated) with) higher) enrolments.) However,) it) has) been) observed) that) in) case) of)enrolment) of) communities) from) afar) also,) utilization) of) insured) hospital) care) does) not) necessarily)increase)(Chankova,)Sulzbach,)and)Diop)2008;)Carrin,)Waelkens,)and)Criel)2005).)Whether)the)size)and)composition)of) the)CHI) benefit) package) corresponds) to) the)poor)household’s) needs) also) affects) their)enrolment)decision.))Communities) already) accustomed) to) riskZsharing,) solidarity) and) demonstrating) lower) levels) of)socioeconomic) inequality)may)have) a)higher) enrolment) rate) and) it)may)be)easier) to) introduce)CHI) in)these)communities.)Education)level)and)gender)of)the)head)of)the)household)also)affect)the)propensity)to)enroll)(Allegri)2006;)Chankova,)Sulzbach,)and)Diop)2008).)Further,)Most)CHI)schemes)operate)based)on)mutual,) nonZwritten) agreements.) Trust) of) the)members) on) CHI)managers) and) the) providers) is) of)extreme) importance) especially) as) most) of) the) CHI) schemes) operate) based) on) mutual,) non) written)

Page%|%7
agreements) and) in) many) cases) the) managers) do) not) have) the) technical) capacity) to) negotiate) with)providers) for) better) care.) Participation) in) the) design) of) the) schemes,) responsiveness) to) community’s)preferences,)inferior)quality)of)care)can)influence)trust)and)affect)enrolment/drop)outs.)In)addition,)the)provider)payment)mechanism)may)set)financial)incentives)to)providers)to)either)increase)the)number)of)services)and)related)costs)(which)may)lead)to)premium)increases)and)financial)instability))or)to)increase)the)use)of)preventive)care)and)provide)better)quality)care,)which)may)affect)the)level)of)trust)(Schneider)2004;)Carrin,)Waelkens,)and)Criel)2005).)
Pooling!Risk) pooling) is) at) the) core) of) a) health) insurance) scheme,) with) transfers) from) lowZrisk) to) highZrisk)members)and)wealthier)to)poorer)members)providing)financial)protection)to)those)most)in)need.)It)also)enables)providers)to)increase)efficiency)and)costZeffectiveness.)The)voluntary)nature)of)most)of)the)CHI)schemes,)however,)increases)the)risk)of)adverse)selection,)with)the)healthier)households)or)community)members) not) interested) while) the) less) healthier) will) be) interested.) Further,) communities) may) limit)membership)within)a)narrower)definition)of) the)community,)again) lowering)the)risk)pooling.)Also,) the)requirements)of) a)benefit)package)between) the)wealthier) and) the)poorer)may)differ) again) restricting)pooling.) For) a) risk) pool) to) be) successful,) sufficient) percentage) of) population) has) to) be) covered) and)adverse)selection)has)to)be)minimized.)))
Purchase!of!Services!The)CHI) is)dependent)on)outside)providers,)either)private,)nonZgovernmental)organizations) (NGOs))or)government) for) healthcare) provision.) In) some) cases,) the) CHIs) may) themselves,) employ) healthcare)providers.)In)general,)therefore,)the)CHI)is)concerned)about)the)best)providers)to)contract)with)from)the)limited)choice)available)to)provide)value)for)money)service)and)also)the)benefit)package)which)will)be)most)beneficial.)Benefit)packages)tend)to)be)as)per)the)available)services)at)the)facilities)participating)in)CHIs)and)not)necessarily)as)per)the)needs)of)the)community)and)in)many)cases,)benefit)packages)are)not)clearly)defined,)which)may)result)in)benefits)being)targeted)towards)the)chronically)ill.))Benefit)package)providing) ambulatory) care) at) primary) health) care) facilities) in) the) benefits) package) may) increase)enrolment)among)the)poor,)reduce)dropout)rates)and)costs)for)expensive)inZpatient)care.)Availability)of)government) or) nonZgovernmental) organizations) may) help) in) channelizing) subsidized) services) and)expanded) packages.) These) are) complex) decisions) requiring) dispelling) of) existent) ‘informational)asymmetries’)and)involve)trust)based)contracts)mostly.)
Cost) of) purchases) depend) on) the) size) of) pool,) economies) of) scale) achieved) and) benefit) package) and)determines)along)with)the)resource)mobilization,)including)from)governments)and)donors,)the)financial)performance)and)the)longZterm)sustainability)of)the)scheme.)
Management!characteristics!)
Community)involvement,)ownership)in)the)management)of)the)scheme)leads)to)improvement)in)revenue)collection,)cost)containment,)access)and)quality)of)services.)The)skills)necessary)to)design)the)

Page%|%8
scheme,)tackle)the)claims)settlement)process,)accounting,)bookkeeping,)etc.)are)not)available)and)the)scheme)does)not)have)the)capacity)to)bear)the)costs)for)a)trained)person.)These)skills)and)the)associated)costs,) therefore,) mostly) require) provider) or) government) assistance.) Strong) linkages) between) the)provider)and)the)scheme)improve)performance.))
Types!of!Community!Health!Insurance!CHI) management) models) involve) varying) degree) of) involvement) in) the) administration) of) the)
pooling) and) preZpayment) arrangements) of) the) community,) the) provider,) government,) nonZgovernmental) organizations) or) microZinsurance) agencies.) While) community) involvement) in)management) of) the) scheme) is) a) common) feature) in) all) these) schemes,) the) degree) of) involvement,)benefit)package)and)coverage)may)vary)depending)on) the) jurisdiction)of) the) community)and)also) the)providers.) Based) on) the) involvement,) these) can) be) broadly) categorized) as) first,) communityZbased)schemes) where) the) community) manages) and) administers) the) scheme) even) though) initiated) by)government)or)donors,) second,)providerZbased)community)health) insurance)where)provider,)usually)a)hospital,) plays) a) key) role) in)mobilizing) the) community) and) community’s) role) is)more) supervisory) and)third,) government) or) social) insuranceZsupported) communityZdriven) scheme)which) is) characterized) by)strong)involvement)of)governmental)supervision)or)involvement.)Most)of)the)earlier)CHI)schemes)have)either) been) initiated) by) the) health) providers) i.e.,)missionary) hospitals,) or) tend) to) be) set) around) the)providers)themselves)(Atim,)1998,)Jakab)2001),Musau,)1999).)There)are)variations)on)these)models)with)differing) degrees) of) collaborations) between) the) community) and) the) provider.) In) Africa,) third) party)insurance)has)not)been)a)feature)of)these)schemes)while)in)Asia,)in)certain)models,)NGOs)have)acted)as)a)link)between)communities,)providers)and)third)party)insurers.))
4 Outcomes!from!CHI!schemes.!)
There) has) been)mixed) experiences) of) CHI) schemes.) On) the) one) hand,) there) are) schemes)which)have)successfully)existed)for)many)years,)there)are)a)large)number)of)examples)which)have)folded)up)in)a)couple)of)years.)Large)scale)studies)have)been)conducted)by)ILO,)WHO)and)others)in)Africa)and)Asia)to)study) the) outcomes) of) CHI) schemes.) Empirical) evidence) from) these) studies) have) been) analyzed) in)literature.) However,) not) many) studies) have) been) consistent) in) terms) of) outcome)measurement) and)study)design.)Cost)effectiveness)data)has)also)been)lacking)(Ekman)2004).)Despite)these)inconsistencies)and) the)absence)of) systematic)evidence,) there) is)a)general)agreement) that) these)schemes)can,)under)proper) enabling) conditions,) improve) household’s) access) to) healthcare.) In) this) section,) some) of) the)successful) outcomes) are) analyzed.) Review) has) been)made) in) literature) of) these) schemes,) evaluating)them)against)the)objectives)for)setting)these)up)–)resource)mobilization)for)health,)financial)protection)of)households)and)social)inclusion.)
Resource!Mobilisation!CHI)schemes)mobilize)household)resources)which)would)otherwise)not)have)been)available) to)
the)health)system.)The)extent)of)this)mobilization,)as)compared)to)the)total)resources)made)available)to)

Page%|%9
the)local)health)systems)vary)and)may)not)be)sufficient)for)sustainable)financing)of)primary)healthcare)but) can) vary) from) 30) to) 100) percent) of) members’) healthcare) expenditures.) The) CHI) contributions)become)substantial)as)the)coverage)and)the)percentage)enrolment)increases.)Also,)taken)in)conjunction)with)other)community)or)health)financing)mechanisms)and)the)fact)that)governments)or)notZforZprofit)health)institutions)provide)care)to)the)members)of)the)CHI)schemes)and)there)is)a)shift)from)the)private)to)the)public)sector,)elements)of)sustainability)can)be)built) in)and)contributions)may)be)substantial)for))primary) care,) drugs) and) hospital) care) (Jakab) 2001;) ArhinZTenkorang) 2001;! Ekman) 2004;) Carrin,)Waelkens,)and)Criel)2005).)
Financial!Protection!CHI% schemes% substantially% reduce% financial% barriers% to% access% through% increased% utilization% by%
members% as% opposed% to% non;members% and% reduced% out;of% pocket% expenditure.) However,) the) poorest)may) still) be) excluded.) Success) depends) on) the) extent) of) community) involvement) in)management) to)ensure)member)compliance)with)revenue)collection,)capacity)building)of)the)community,)linkages)with)providers)and)the)government)support)for)sustainability.)))
Social!Inclusion!CHI)schemes)have)been)successful)at)increasing)the)reach)of)risk)protection)to)a)large)number)of)
people) who) would) otherwise) not) have) financial) protection.) However,) the) reach) to) the) poorest) and)socially) excluded) groups) has) not) been) very) encouraging.) Further,) limited) enrolment) of) high) income)individuals) also) mean) that) there) is) a) limited) redistribution) of) financial) risk) from) rich) to) poor(Jütting)2004;)Ekman)2004).))
In) nutshell,) CHI) schemes) have) the) potential) to) extend) coverage) of) financial) protection) for)healthcare) to) excluded) populations,) increase) resource) mobilization) for) healthcare,) supplement) the)national) level) schemes) for) universal) financial) protection) but) cannot) be) a) replacement) for) the) social)insurance)and)public)funded)healthcare)provisions)by)the)Government.))
5 Building!on!the!experience!gained!–!Scaling!up.!)
In)low)and)middle)income)countries,)CHI)is)a)relevant)instrument)to)leapfrog)the)systemic)rigidities)and)provide)risk)pooling)and)improved)healthcare)access)to)the)excluded)communities)–)those)who)are)not) covered) through) social) insurance) –) and) thus) reduce) the) chances) of) catastrophic) health) incidents)driving) households) into) poverty.) The) instrument) needs) to) be) used) with) care) as) these) schemes) are)generally) quite) fragile) and) do) not) possess) the) benefit) of) hindsight) and) experience2)and) the) evidence)base)for)successful) interventions)has)yet)to)reach)full)maturity.)National)guidelines)have)to)be)flexible)enough)and)carefully)implemented)on)smaller)levels)before)gradual)scale)up.))
)
2 ILO

Page%|%10
This) section)deals)with) the) lessons) learnt)and)knowledge)gained) for)designing)and)managing)CHI)schemes)that)can)be)applied)while)implementing)CHI)schemes.))))
Pre8requisites!)The)experience) in)CHI) schemes)has)been)mixed.) Success)has)not)been)universal) and,)wherever) it) has)been)achieved)required)active)community)participation)which)does)not)come)automatically.)NGO)and)governmental) interventions) to) successfully)mobilize) communities) are) also) dependent) on) the) existing)conditions) in) the) communities.) Mutually) beneficial) action) is) more) likely) to) succeed) in) communities)(villages)) that) have) a) reasonable) level) of) social) capital) and) capable) agencies) in) the) form)of) educated)village) leaders) (Krishna)2002).) In) communities) not) having) these) characteristics,) sufficient)mobilization)and)capacity)building)may)be)required)before)taking)up)these)schemes.))In)the)low)and)developing)countries,)absence)of)providers,)or)inefficient)and)ineffective)services)of)the)public)healthcare) system,)within)a) reasonable)geographic)distance) to)provide) service) to) the) rural) and)remote)communities)may)be)a)limiting)factor.)While)CHI)provides)a)collective)pool)and)creates)necessary)efficiencies) for) providers,) it) may) not) be) a) sufficient) demand) side) effort) for) deployment) of) sufficient)resources)by)private)providers,)in)which)case)government)will)have)to)intervene.))The)scheme)design)process)should)be)carried)out)in)a)consultative)manner,)involving)all)stakeholders)–)the) community) representatives) –) from) the)poorest) to) the) richest,) providers) –) health)workers,) facility)managers,)etc.,)the)governmental)and)other)representatives,)household)surveys)to)determine)the)needs)and) the) ability) to) pay,) health) facility) assessment) and) costing) studies.) This) participatory) exercise) will)ensure) that) the) design) and) modality) selected) is) appropriate,) ensure) greater) ownership) and) may)contribute)to)the)long)term)success)(ArhinZTenkorang)2001).))
Designing!CHI!Schemes!)A)successful)CHI)scheme)should)be)able)to)perform)financially,)match)its)resource)mobilization)with)the)cost)of)purchases,) though)cost) recovery) is)not)a)prime) indicator)of)performance)or)good)design)here.)The) process) of) design) involves) addressing) issues) of) adverse) selection,) supply) side) and) demand) side)moral) hazard,) expanding) the) risk) pool,) designing) benefit) packages) as) per) initial) willingness) to) pay,)ensuring) equitable) access) especially) for) the)poor,) using) existing) cooperative) structures) built) on) social)capital,) for) example,) self) help) groups,)microfinance) schemes) and)provider) payment)mechanisms.) The)design)has)also)to)match)with)the)overall)health)objectives)and)in)case)of)shortfalls,)alternative)ways)to)meet) the) shortfall,) for) example,) subsidies,) will) have) to) be) incorporated) in) the) overall) scheme.) For)example,) it) is) a) desirable) objective) of) health) insurance) to) reduce) adverse) selection,) but) at) the) same)time,)it)may)be)desirable)from)the)public)health)perspective)to)increase)utilization)of)health)facilities)and)
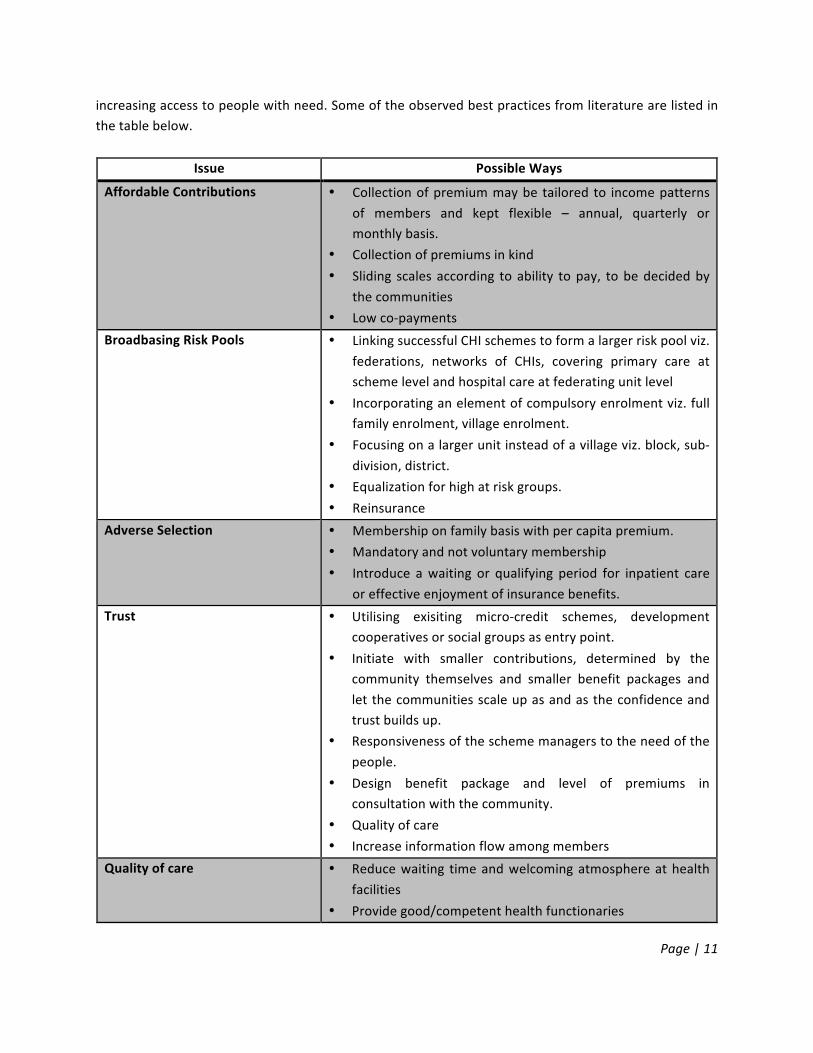
Page%|%11
increasing)access)to)people)with)need.)Some)of)the)observed)best)practices)from)literature)are)listed)in)the)table)below.))
Issue! Possible!Ways!
Affordable!Contributions! • Collection)of)premium)may)be) tailored)to) income)patterns)of) members) and) kept) flexible) –) annual,) quarterly) or)monthly)basis.)
• Collection)of)premiums)in)kind)• Sliding) scales) according) to)ability) to)pay,) to)be)decided)by)
the)communities)• Low)coZpayments)
Broadbasing!Risk!Pools! • Linking)successful)CHI)schemes)to)form)a)larger)risk)pool)viz.)federations,) networks) of) CHIs,) covering) primary) care) at)scheme)level)and)hospital)care)at)federating)unit)level)
• Incorporating)an)element)of)compulsory)enrolment)viz.)full)family)enrolment,)village)enrolment.)
• Focusing)on)a)larger)unit)instead)of)a)village)viz.)block,)subZdivision,)district.)
• Equalization)for)high)at)risk)groups.))• Reinsurance)
Adverse!Selection! • Membership)on)family)basis)with)per)capita)premium.)• Mandatory)and)not)voluntary)membership)• Introduce) a)waiting) or) qualifying) period) for) inpatient) care)
or)effective)enjoyment)of)insurance)benefits.)Trust! • Utilising) exisiting) microZcredit) schemes,) development)
cooperatives)or)social)groups)as)entry)point.)• Initiate) with) smaller) contributions,) determined) by) the)
community) themselves) and) smaller) benefit) packages) and)let)the)communities)scale)up)as)and)as)the)confidence)and)trust)builds)up.)
• Responsiveness)of)the)scheme)managers)to)the)need)of)the)people.)
• Design) benefit) package) and) level) of) premiums) in)consultation)with)the)community.)
• Quality)of)care)• Increase)information)flow)among)members)
Quality!of!care! • Reduce)waiting) time)and)welcoming)atmosphere)at)health)facilities)
• Provide)good/competent)health)functionaries)

Page%|%12
Issue! Possible!Ways!
• Availability)of)drugs)Referrals! • Gate)keeping)for)higher)level)of)care.)Primary)health)centre)
can)only)refer)for)hospital)care.)• Setting)referral)rules)
Moral! Hazard! –! Supply! side! and!Demand!side!!
• Clearly)defined)benefit)packages)• Strict)gateZkeeping)for)higher)level)of)care)• Clear)contracts)with)health)providers)• Capitation)payment)for)providers)instead)of)Fee)for)Service)
Equitable!Access! • Low)or)no)coZpayments)• Government)or)NGO)facilitation)• Exemptions)• Sliding) scale,) as) per) socio) economic) condition,) instead) of)
flat)contributions)• Access)to)facilities)geographically)close)to)communities)
(Jütting)2004;)Carrin,)Waelkens,)and)Criel)2005;)Dror)and)Preker)2002)and)others))
Managing!CHI!Schemes!)With)the)inherent)limitations)on)the)size)of)CHI)schemes)and)the)resultant)resource)pool,)remuneration)for)skills)to)manage)the)CHI)schemes)can)be)substantial)as)a)percentage)of)the)total)pool.)In)large)social)insurance)schemes,)the)average)administrative)expenditure) is)approximately)5)percent)whereas) in)CHI)schemes) it) reaches) upto) 40) percent) in) some) schemes.) Clearly) such) high) expenditures) are) not)sustainable.)The)alternatives)available)are) in)pooling)resources)with)either)other)CHI)schemes,)or)with)provider)facilities)–)government)owned)or)NGO)based)or)governments)providing)direct)subsidies)for)the)managerial) and) accountancy) skills.) Linkage) between) schemes) is) an) important) characteristic)demonstrated)by)successful)schemes.))Capacity)of)the)community)has)to)be)continuously)built)through)trainings)and)disseminations)to)enable)them)to)discharge)supervisory,)oversight)role)effectively)and)also)to)participate)in)the)CHI)design)and)its)continuous)evolution)meaningfully.)Absence)of)community)management)may) lead)to)provider)capture)and)unfavorable)pricing.)
Government!interventions!Government)support)to)CHI)schemes) is)a)requirement)for)their)sustenance.)Government) interventions)in)community)schemes)should,)however,)be)very)carefully)designed)to)ensure)that)these)do)not)make)CHI)schemes)into)another)government)scheme)taking)away)the)community)ownership.)Government)can)intervene) in) the) form) of) incentives) by) way) of) greater) services,) matching) cash) transfers) which) can)motivate)communities)to)perform)better.)Also,)in)some)cases,)government)interventions)to)improve)the)effectiveness)and)sustainability)of)existing)community)financing)schemes)can)be)in)the)following)form)of)

Page%|%13
increased) and) wellZtargeted) subsidies) to) pay) for) the) premiums) of) poor/lowZincome) populations;)insurance) to)protect)against)expenditure) fluctuations)and) reZinsurance) to)enlarge) the)effective) size)of)small) risk) pools;) effective) prevention) and) case) management) techniques) to) limit) expenditure)fluctuations;) technical) support) to) strengthen) the) management) capacity) of) local) schemes;) and)establishment)and)strengthening)of)links)with)the)formal)financing)and)provider)networks)(Preker)et)al.)2002;)ArhinZTenkorang)2001).))
)
6 CHI!and!National!Rural!Health!Mission,!India!)More) than)90)percent)of) Indian)population)and)almost)all) the)poor)are)not)covered)under)any)health)insurance)scheme.)Their)health)care)needs)are)met)primarily)through)direct)outZofZpocket)expenditure)on)services)provided)by)the)public)and)private)sectors.)Low)social)insurance)coverage)is)compounded)by)a) poorly) functioning) public) healthcare) system) leading) to) an) increasing) dependence) on) private)healthcare)(Gumber)2001).))Government)of)India)has)started)an)umbrella)health)system)program)under)the)nomenclature)National)Rural) Health) Mission) (NRHM)) since) April) 2005) with) the) objectives) of) providing) universal) access) to)equitable,)affordable)and)quality)health)care)which) is)accountable)at) the)same)time)responsive)to)the)needs)of)the)people.)The)scheme)envisages)strengthening)of)the)health)infrastructure,)especially)in)the)primary)and)secondary)health)sector)and)provides)the)much)needed)flexibility)to)the)states)to)operate)beyond)the)structural)confines)of)a)rule)bound)system)to)provide)manpower)and)other)requirements)of)a)fund)starved)health)sector.)New)organizational)structures)have)been)created)at)the)district)and)below)level.) Communities) are) represented) on) the) governing) societies) of) the) public) health) facilities,) with)responsibilities)delegated)to)them)along)with)some)untied)funds)and)powers)to) impose)user)fees.)The)Mission) recognizes) the) need) for) community) involvement) and) initiating) of) community) led) health)insurance)as)one)of)the)important)instruments)for)achieving)its)goal.))Establishing) CHI) schemes,) each) targeting) households) in) defined) poor) communities) such) as) villages) or)districts,) is) an) option) for) providing) immediate) financial) risk) protection) to) a) significant) number) of)households) in) the) absence) of) a) universal) social) insurance) arrangement.) Keeping) in) mind) the) weak)capacities)of)the)government)structures)to)implement)programs)effectively)and)also)the)fact)that)some)of) the)problems)have)become) institutionalized)and)organizational) changes)alone)may)not)bring)about)sustainable) changes) to) move) the) system) effectively) from) its) present) state) of) inertia,) it) may) be)appropriate)to)put)in)place)demand)side)pressures)through)CHI)like)initiatives.)))The)experience)of) India)has)been,) however,) in) the)provision)of)NGO) led) community)health) insurance)schemes) with) the) NGOs) acting) as) insurer) and) providers;) insurer) and) purchaser) of) care) for) the)community) from)a)private)provider)or) a) link)between)a) third)party) insurer) and)a)healthcare)provider)with) the) benefit) packages) including) primary) and) secondary) healthcare.)Most) of) the) schemes) require)

Page%|%14
external)resources)for)financial)sustainability.)The)SEWA)scheme)which)is)built)on)an)existing)women’s)cooperative)group)has)been)successful.)Successes)have)been)reported)for)provider)based)schemes)like)Yeshashwini.)However,)the)overall)impact)has)not)been)very)satisfactory.))In) order) to) systematically) implement) the) CHI) initiative,) a) survey) may) be) carried) out) to) identify)communities) and) excluded) communities,) which) satisfy) the) preZrequisites) identified) in) this) paper) and)having) high) level) of) social) capital,) available) and) successful) community) based) organizations,) self) help)groups,) cooperative) structures) who) have) won) the) trust) of) the) local) communities.) with) reasonable)success.) Simple) criteria) to) assess) trustworthiness) and) sustainability,) which) may) include) indicators) of)shared) norms) such) as) respect,) dignity,) fairness,) openness,) compromise) and) solidarity) and) evidence)around) cooperative) activities) and) handling) of) conflicts,) may) be) drawn) up) for) assessing) the) CBOs)(Molyneux)et)al.)2007).)))CHI)schemes)can)be)implemented)through)these)CBOs)and)will)require)government)support,)for)which)linkage) between) the) CBOs) and) the) newly) formed) Hospital) Management) Committees) (Rogi) Kalyan)Samities)) in) the) primary) level) facilities) providing) first) level) care) may) be) explored.) The) Hospital)Management)Committees)consist)of)elected)representatives,)have)their)own)bank)accounts)with)powers)to)retain)user)fees)and)reinvest)in)the)health)facilities.)Matching)cash)transfers)to)contributions)made)by)members)may)be)considered)as)incentive)and)also)as)a)means)of)providing)sustenance)funds)to)the)CHI)initiatives.) CHI) initiatives) can) supplement) and) considerably) boost) the) other) NRHM) initiatives) in)extending) affordable) and) equitable) access) to) healthcare) and)moving) it) closer) towards) achieving) the)avowed)goal)of)universal)access.)
7 Conclusions!)CHI) schemes) provide) low) and)middle) income) countries) with) an) alternative) to) reach) out) to) excluded)populations)and)seek)to)address)both)government)and)market)failure)in)reaching)formal)healthcare)to)these) communities.) CHI) is) not) a) replacement) of) universal) social) insurance) but) can) supplement) other)national) efforts) at) universal) financial) protection.) Success)of) a) CHI) scheme) is) highly) dependent)on) the)level) of) involvement) of) the) community) but) sustenance) requires) government) support) through) public)subsidy.)CHI)schemes)can)lead)to)substantial)reduction)in)out)of)pocket)expenditures)for)its)members)as)well) as) additional) resource) mobilization) for) the) health) sector.) Successful) implementation) not) only)requires) careful) design) involving) communities) but) also) involves) challenges) in) implementation.) Design)requirements)have)to)be)flexible)to)meet)the)diverse)requirements)of)the)communities,)especially)the)poor,) so) that) the) affordability,) trust,) equitable) access) and) increased) risk)pooling) criteria)are) satisfied.)The)challenge)in)many)of)the)countries)is)to)provide)alternatives)for)the)absent,)ineffective)or)inefficient)heathcare)services)in)the)geographical)areas)where)the)CHI)coverage)is)most)required)so)that)these)can)be)simultaneously) implemented.)The) issue)of)governance)and)management)of)CHI) schemes,) including)overseeing)contracting)arrangements)with)providers)is)another)challenge.)))

Page%|%15
India)has)embarked)on)an)ambitious)health)systems)reform)program)and)is)expanding)its)public)health)coverage.) CHI) provides) an) attractive) alternative) for) the) government) and) can) be) used) along)with) the)other) structures) being) established) under) the) program) and) involving) communities.) Successful) rollout)could) involve)community)based)organizations)and)other) initiatives) in)microcredit)and)self)help)groups,)development)cooperatives,)which)have)one)the)success)of)the)communities.)Success)would)also)require)capitalizing)on)the)considerable) level)of)social)capital)available)with) the)communities)by)building) local)capacities.) CHI) has) the) potential) to) reduce) the) high) out) of) pocket) expenditure) on) health) care) by) the)Indian)population,)improve)people’s)access)to)healthcare)and)reduce)the)risks)of)falling)into)poverty)due)to)catastrophic)health)expenditures.))

References!)
1. Allegri, Manuela De; Bocar Kouyaté; Heiko Becher; Adjima Gbangou; Subhash Pokhrel; Mamadou Sanon;Rainer Sauerborn. 2006. Understanding enrolment in community health insurance in sub-Saharan Africa: a population-based case–control study in rural Burkina Faso. Bulletin of the World Health Organization 84 (11).
2. Arhin-Tenkorang, Dyna. 2001. Health Insurance for the Informal Sector in Africa: Design Features, Risk Protection, and Resource Mobilization
3. Paper prepared for Working Group 3 Commission on Macroeconomics and Health. 4. Bennett, Sara. 2004. The role of community-based health insurance within the health care financing
system: a framework for analysis. Health Policy Plan. 19 (3):147-158. 5. Carrin, Guy, Maria-Pia Waelkens, and Bart Criel. 2005. Community-based health insurance in
developing countries: a study of its contribution to the performance of health financing systems. Tropical Medicine & International Health 10 (8):799-811.
6. Chankova, Slavea, Sara Sulzbach, and Francois Diop. 2008. Impact of mutual health organizations: evidence from West Africa. Health Policy Plan. 23 (4):264-276.
7. Dror, David M., and Alexander S. Preker. 2002. Social reinsurance : a new approach to sustainable community health financing: Washington, D.C. : World Bank, c2002.
8. Ekman, Bjorn. 2004. Community-based health insurance in low-income countries: a systematic review of the evidence. Health Policy Plan. 19 (5):249-270.
9. Gottret, Pablo E., and George Schieber. 2006. Health financing revisited : a practitioner's guide. Washington, DC: World Bank.
10. Gumber, Anil. 2001. Hedging the Health of the Poor: The Case for Community Financing in India.
11. Hong, Wang, Yip Winnie, Zhang Licheng, Wang Lusheng, and Hsiao William. 2005. Community-based health insurance in poor rural China: the distribution of net benefits. Health Policy & Planning 20 (6):366-374.
12. Hsiao, William. 2001. Unmet Needs of 2 Billion: Is Community Financing a Solution? 13. Jakab, Melitta; Krishnan, Chitra. 2001. Community Involvement in Health Care Financing: A Survey of
the Literature on the Impact, Strengths and Weaknesses. 14. Jütting, Johannes P. 2004. Do Community-based Health Insurance Schemes Improve Poor People's
Access to Health Care? Evidence From Rural Senegal. World Development 32 (2):273-288. 15. Krishna, Anirudh. 2002. Active social capital : tracing the roots of development and democracy. New
York: Columbia University Press. 16. Molyneux, Catherine, Beryl Hutchison, Jane Chuma, and Lucy Gilson. 2007. The role of community-
based organizations in household ability to pay for health care in Kilifi District, Kenya. Health Policy Plan. 22 (6):381-392.
17. Ogawa, Sumiko, Toshihiko Hasegawa, Guy Carrin, and Kei Kawabata. 2003. Scaling up community health insurance: Japan's experience with the 19th century Jyorei scheme. Health Policy Plan. 18 (3):270-278.
18. Preker, Alexander S., Guy Carrin, David Dror, Melitta Jakab, William Hsiao, and Dyna Arhin-Tenkorang. 2002. Effectiveness of community health financing in meeting the cost of illness. Bulletin of the World Health Organization 80 (2):143.

Page%|%17
19. Preker, Alexander S.; Guy Carrin, David M. Dror, Melitta Jakab, William Hsiao and Dyna Arhin. 2001. Role of Communities in Resource Mobilization and Risk Sharing.
20. Ron, Aviva. 1999. NGOs in community health insurance schemes: examples from Guatemala and the Philippines. Social Science & Medicine 48 (7):939-950.
21. Sara Bennett, Allison Gamble Kelley, Brant Silvers, Macqueen, Angus. 2004. 21 Questions on CBHF. PHRplus (March 2004).
22. Schneider, Pia. 2004. Why should the poor insure? Theories of decision-making in the context of health insurance. Health Policy Plan. 19 (6):349-355.
23. Zhang, Licheng, Hong Wang, Lushang Wang, and William Hsiao. 2006. Social capital and farmer's willingness-to-join a newly established community-based health insurance in rural China.(Report) Report. (cy0168-8510April 200):233.

Endnotes! 1 CommunityZbased)health)funds)have)existed)for)centuries.)The)earliest)ones)were)largely)sponsored)by)local) religious) organizations) such) as) churches) and) synagogues.) In) the) last) century,) community)cooperatives,) local) mutual) aid) societies,) and) local) funeral) funds) have) sponsored) and) managed) local)health)funds.)The)mutual)health)schemes)of)the)19th)century)in)Europe)were)a)preZcursor)to)the)national)health) insurance) schemes.)The)19th) century) Jyorei) community)health) scheme,)which)had) its)origins) in)village)populations)coming)together)to)ensure)continued)presence)of)community)based)doctors)in)their)villages)provided)the)base)for)the)National)Citizen’s)Health)insurance)Fund,)one)of)the)pillars)of)Japanese)social)health) insurance)system.) In) recent) times,) the% involvement%of% the%community% in%health% financing%was% spurred,% among%others,% by% the%Declaration% of%Alma%Ata% in% 1978.) The)Bamako) Imitative) for)Africa)(1987))also)encouraged)the)establishment)of)community)health)finance)initiatives)in)Africa)region.)More)recently,) the) Commission) for)Macroeconomics) in) Health) in) its) report) submitted) to) the)WHO) in) 2001)also,) while) recognizing) limitations) of) community) financing) mechanisms) had) recommended) for)conversion% of% current% out% of;pocket% expenditure% into% prepayment% schemes,% including% community%financing% programs% supported% by% public% funding,% where% feasible) in) the) low) income) countries) of) the)world.)) 2 Community)health)financing)initiative)has)again)picked)up)in)recent)years,)involving)national)and)local)governments,) civil) societies) and) international) donor) organizations) and) financers,)with) several) tens) of)millions) of) dollars) in) turnover.) There) is) also) a) growing) interest) in) developing) more) explicit) linkages)between) community) financing) initiatives) and) health) insurance) and) promotion.) As) an) example,) it) is)estimated)that)in)West)Africa)there)was)more)than)a)twoZfold)increase)in)the)number)of)CBHI)schemes)in)just)three)years,)from)199)schemes)in)2000)to)585)in)2003.)Developing)countries)in)Asia)and)Africa)are)exploring) community) health) financing) as) one) of) the) alternative) mechanisms) for) meeting) the) health)financing)needs)of)the)rural)populations)and)the)informal)sector)workers.)Renewed)interest)can)also)be)seen)in)the)large)amount)of)literature)that)has)been)churned)out)on)the)subject.) 3 Health) insurance) is)a) riskZsharing)mechanism)that) lowers) the)outZofZpocket)price) for)medical) care)at)the) time)of)purchase)by) smoothing)medical)payments)across) individuals) and) time.)Arhin)–)Tenkorang)defines)health) insurance)as) a)mechanism) for) spreading) the) risks)of) incurring)health) care) costs)over) a)group) of) individuals) or) households) constitutes) irrespective) of) the) administrative) arrangements)employed,) but) dependent) on) the) outcome) of) risk) sharing) and) subsequent) crossZsubsidization) of)healthcare)expenditures)among)the)participants.))





























