Embed Size (px)
Citation preview
690
of the population must concentrate on altering the taste for salt ofthat population--otherwise, people will add salt at home to foodsprocessed without salt.
James and colleagues imply that dietary salt restriction is anestablished means of limiting the usual rise in blood pressurewith age, and thus the development of coronary artery andcerebrovascular disease. However, in the references they cite, notone provides any evidence that dietary salt restriction actually limitsthe genesis of hypertension in normotensive subjects; indeed, themajority are reviews and some are reviews of reviews. Only onepaper reports the effects of a controlled trial of sodium restriction inessential hypertension.To point out as justification for dietary salt restriction that
current intake in affluent communities exceeds the physiologicalrequirement is nonsense. Do they propose limiting the intake ofother minerals or vitamins to the physiological requirement (whereknown), or indeed would they limit water, protein, carbohydrate,and fat-all consumed in excess of requirement? Our diet hasevolved on the principle of excess consumption of all essentialnutrients. What we need is used or stored, and any left is eliminated.If we are serious about controlling hypertension, then what isneeded is wider use of the sphygmomanometer and not another dietsheet.
20 Wimpole Street,London W1M 7AD ALEXANDER L. MACNAIR
COMMUNITY CAMPAIGN FOR IRON DEFICIENCY
SIR,-Your editorial (Jan 17, p 141) draws attention to therelation between iron deficiency and psychomotor development inchildren. There is much evidence for an association between iron
deficiency and delayed or impaired development.l However, thedifferences between iron-deficient and iron-replete children,though statistically significant, are small and within the normalrange. It should not be assumed that children with iron deficiencyare suffering from a major impairment of intellectual development.Furthermore, similar changes have been shown in adolescents2 andadults.3 If iron deficiency needs investigation and treatment, ourefforts should not be directed solely towards toddlers.
Royal Manchester Children’s Hospital,Pendlebury,Manchester M27 1HA D. I. K. EVANS
1. Evans DIK. Cerebral function in iron deficiency: A review. Child Care Health Dev1985; 11: 105-12.
2. Webb TE, Oski FA. J Special Ed 1974; 8: 153-56.3. Tucker DM, Sandstead HH, Penland JG, Dawson SL, Milne DB. Iron status and
brain function: Serum ferritin levels associated with asymmetries of corticalelectrophysiology and cognitive performance. Am J Clin Nutrition 1984; 39:105-13.
EARLY-ONSET AND LATE-ONSET PNEUMONIAS ININTENSIVE CARE UNITS
SIR,-We have a different interpretation for the data of DrMandelli and colleagues (Nov 8, p 1094) and we also have new dataon the pathogenic mechanisms of nosocomial pneumonias inintensive care units (ICU). Mandelli and colleagues suggest thatpatients with early-onset pneumonia (EOP) constitute a specificsubgroup of patients in an ICU whose pneumonia may differ inpathogenesis, prevention, and treatment from those with later-onsetpneumonia (LOP). The evidence included the consistent
proportion (about 55%) of EOP in all pneumonias in ICUs from1978 to 1984, and an unchanged case-fatality rate of about 35%during this period.However, we think that most cases of EOP (clinically present
before the fourth day in an ICU) are acquired in hospital wardsbefore entry to the ICU where the clinical debut occurs. The reasonthat the stay in the ICU of EOP cases is usually shorter than theexpected incubation period for pneumonia.
Despite a different place of infection EOP and LOP may sharethe same pathogenic mechanisms of aspiration of bacilli-contaminated pharyngeal secretions in debilitated patients. Thefrequency of EOP has decreased in the same proportion as all
pneumonias have decreased from 1978 to 1984 (see table in originalletter). This consistency is explained if the prevention measures that
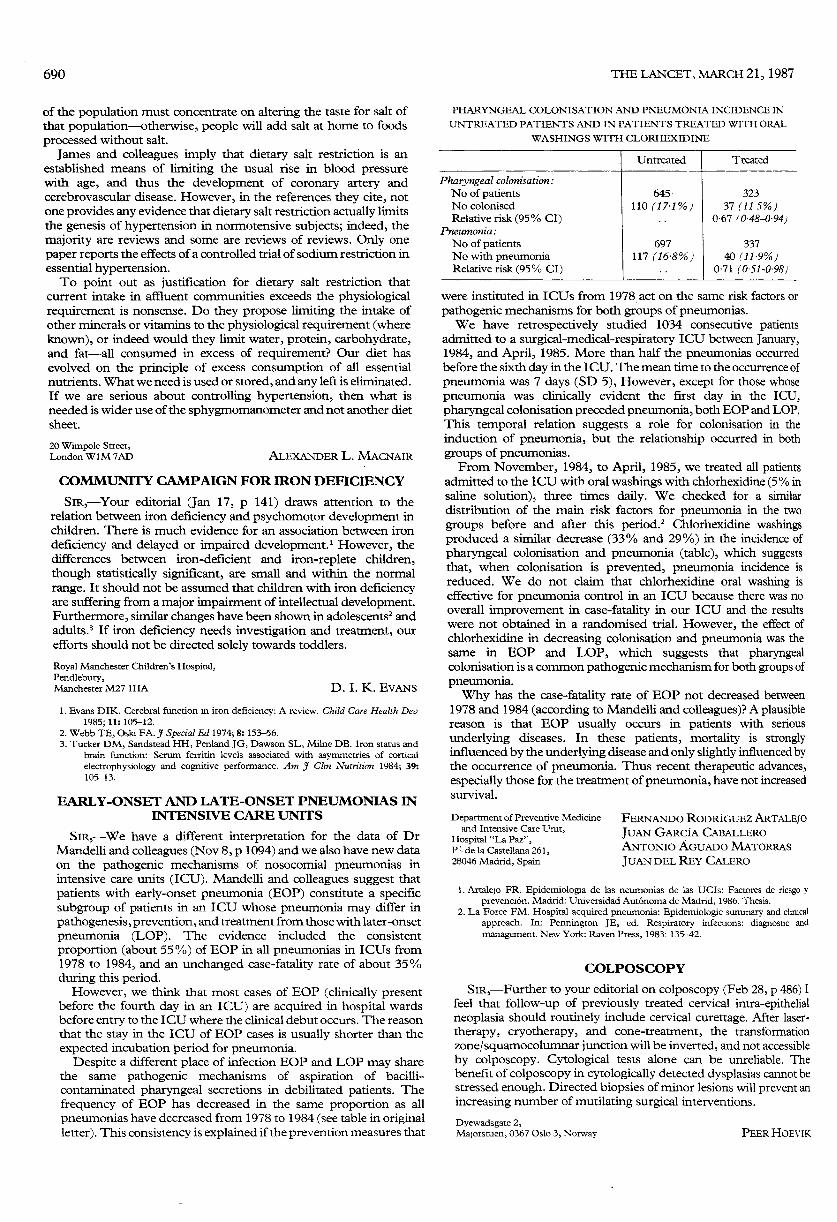
PHARYNGEAL COLONISATION AND PNEUMONIA INCIDENCE IN
UNTREATED PATIENTS AND IN PATIENTS TREATED WITH ORAL
WASHINGS WITH CLORHEXIDINE
I I
were instituted in ICUs from 1978 act on the same risk factors orpathogenic mechanisms for both groups of pneumonias.We have retrospectively studied 1034 consecutive patients
admitted to a surgical-medical-respiratory ICU between January,1984, and April, 1985. More than half the pneumonias occurredbefore the sixth day in the ICU. The mean time to the occurrence ofpneumonia was 7 days (SD 5), However, except for those whosepneumonia was clinically evident the first day in the ICU,pharyngeal colonisation preceded pneumonia, both EOP and LOP.This temporal relation suggests a role for colonisation in theinduction of pneumonia, but the relationship occurred in bothgroups of pneumonias.From November, 1984, to April, 1985, we treated all patients
admitted to the ICU with oral washings with chlorhexidine (5 % insaline solution), three times daily. We checked for a similardistribution of the main risk factors for pneumonia in the twogroups before and after this period.2 Chlorhexidine washingsproduced a similar decrease (33% and 29%) in the incidence ofpharyngeal colonisation and pneumonia (table), which suggeststhat, when colonisation is prevented, pneumonia incidence isreduced. We do not claim that chlorhexidine oral washing iseffective for pneumonia control in an ICU because there was nooverall improvement in case-fatality in our ICU and the resultswere not obtained in a randomised trial. However, the effect ofchlorhexidine in decreasing colonisation and pneumonia was thesame in EOP and LOP, which suggests that pharyngealcolonisation is a common pathogenic mechanism for both groups ofpneumonia.Why has the case-fatality rate of EOP not decreased between
1978 and 1984 (according to Mandelli and colleagues)? A plausiblereason is that EOP usually occurs in patients with serious
underlying diseases. In these patients, mortality is stronglyinfluenced by the underlying disease and only slightly influenced bythe occurrence of pneumonia. Thus recent therapeutic advances,especially those for the treatment of pneumonia, have not increasedsurvival.
Department of Preventive Medicineand Intensive Care Unit,
Hospital "La Paz",P- de la Castellana 261,28046 Madrid, Spain
FERNANDO RODRÍGUEZ ARTALEJOJUAN GARCÍA CABALLEROANTONIO AGUADO MATORRAS
JUAN DEL REY CALERO
1. Artalejo FR. Epidemiologia de las neumonias de las UCIs: Factores de riesgo yprevención. Madrid: Universidad Autónoma de Madrid, 1986. Thesis.
2. La Force FM. Hospital acquired pneumonia: Epidemiologic summary and clinicalapproach. In: Pennington JE, ed. Respiratory infections: diagnostic and
management. New York: Raven Press, 1983: 135-42.
COLPOSCOPY
SIR,-Further to your editorial on colposcopy (Feb 28, p 486) Ifeel that follow-up of previously treated cervical intra-epithelialneoplasia should routinely include cervical curettage. After laser-therapy, cryotherapy, and cone-treatment, the transformation
zone/squamocolumnar junction will be inverted, and not accessibleby colposcopy. Cytological tests alone can be unreliable. Thebenefit of colposcopy in cytologically detected dysplasias cannot bestressed enough. Directed biopsies of minor lesions will prevent anincreasing number of mutilating surgical interventions.
Dyewadsgate 2,Majorstuen, 0367 Oslo 3, Norway PEER HOEVIK