Embed Size (px)
Citation preview

Community-Based Prematurity Prevention
The Kentucky Experience
HRSA Regional Infant Mortality Summit January 12-13, 2012

Preterm Births, Low Birthweight ,Infant MortalityUnited States, 1981 - 2009
Percent
Source: National Center for Health Statistics, final natality and mortality data
Prepared by March of Dimes Perinatal Data Center, 2007
Rate per 1,000 live births

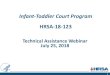
Three Leading Causes of Infant Mortality
United States, 1990 and 2007*
57
112.7
134.9
130.3
96.5
198.1
0 50 100 150 200 250
SIDS
Preterm / LBW
Birth Defects
1990
2007
Rate per 100,000 live births
Source: National Center for Health Statistics
Adapted from a slide Prepared by March of Dimes Perinatal Data Center, 2007

PREMATURITY FOCUS FOR INFANT MORTALITY EFFORTS
Prematurity is a prototypical public health problem- can happen to anyone- known risk factors- not just about medical interventions- high prevalence- short and long term consequences- high cost to multiple systems- prevention pays- evidence based policy and practice not well
established
Prematurity more common and more engaging- everyone knows someone who has had a premature baby
Improving systems of care and support for prematurity will also lead to Infant Mortality reduction

www.healthypeople.gov

Healthy Babies are Worth the Wait
Psychosocial Risk Factors: Perinatal Screening and Intervention
ACOG Committe Opinion # 343
“Biomedical risks, such as complications of pregnancy, concomitant maternal disease, infection, nutritional deficiencies, and exposure to teratogens, are estimated to account for approximately one half of the incidence of low-birth-weight infants and of prematurity and their postnatal sequellae. An important portion of the remaining cases of these adverse pregnancy outcomes may be attributable to psychosocial stress even after controlling for the effects of recognized sociodemographic, obstetric, and behavioral risk factors.”

• Social Ecological Model
7

The Life Course Perspective of Health Development
Lu MC, Halfon N. Racial and ethnic disparities in birth outcomes: a life-course perspective.Maternal Child Health J. 2003;7:13-30. 8
Critical Periods
Cumulative Effects
Interaction with
Environment
Health Equity
TIMING
TIMELINE
ENVIRONMENT
EQUITY

Birth Weight and Coronary Heart Disease
Barker Hypothesis
1.5
1.251.15
10.9
0.7
0
0.25
0.5
0.75
1
1.25
1.5
1.75
<5.0 5.0-5.5 5.6-7.0 7.1-8.5 8.6-10.0 >10.0
Ag
e A
dju
sted
Rel
ativ
e R
isk
Rich-Edwards 1997
Birthweight (lbs)

Birth Weight and Insulin Resistance Syndrome
Barker Hypothesis
18
8.4 8.5
4.9
2.21
0
5
10
15
20
<5.5 5.6-6.5 6.6-7.5 7.6-8.5 8.6-9.5 >9.5
Od
ds
rat i
o a
dj u
s ted
fo
r B
MI
Barker 1993Birthweight (lbs)

• The Brain is the last major organ system to develop
• Lower functions mature first, cortex last
Brain at 35 wks weighs only 2/3 what it will weigh at term
Development of the Human Brain
through Gestation
Cowan WM. Sci Am 241:113, 1979

Late Preterm Outcomes: Childhood
• Increased risk of ADHD and other clinically significant behavior problems– Linnet KM et al Arch Dis Child 2006; 91:655-60– Gray RF et al Pediatrics 2004; 114:736-43– McCormick et al Pediatrics 1996; 97:18-25
• Increased cognitive dysfunction and learning problems– VanBaar AL. Pediatrics 2009; 124:251-7– Chyi LJ et. al. J Pediatr 2008: 153:25-31– Saigal S, et al. Lancet 2008;371:261-69– Pietz et al early Hum Dev 2004;79:131-43

Late Preterm Outcomes: Childhood
• Increased risk Cerebral Palsy and Mental Retardation
– Petrini et al. J Peds, 2008– Moster et al. NEJM 2008; 359:262-73– Himmelman et al. Acta Paediatr; 2005;94:287-94– Moster et al. JAMA 2010; 304(9):976-982 (relative risk of CP 3.7 at 37 weeks)– Talge NM et al Pediatrics 2010; 124:1124-1131 (2-3X incr risk IQ<85)

Late Preterm Infants:Outcomes as Young Adults
Compared to infants born at term, Late Preterm have:
• Increased risk Schizophrenia and mental disorders (RR1.6)
• 40% increased risk for medical disability that severely limits working capacity as an adult
• Long-term neurologic handicap due to prematurity measured in young adults (age 23-29)
Moster et al. NEJM 2008; 359:262-73
Lindstrom K et al. Pediatr 120:70, 2007

Life Course Health Development
Poor NutritionStressAbuseTobacco, Alcohol, DrugsPovertyLack of Access to Health CareExposure to Toxins
Poor Birth Outcome
0 5 Puberty PregnancyAge

How Risk Reduction and Health Promotion Strategies influence Health Development
FIGURE 4: This figure illustrates how risk reduction strategies can mitigate the influence of risk factors on the developmental trajectory, and how health promotion strategies can simultaneously support and optimize the developmental trajectory. In the absence of effective risk reduction and health promotion, the developmental trajectory will be sub-optimal (dotted curve). From: Halfon, N., M. Inkelas, and M. Hochstein. 2000. The Health Development Organization: An Organizational Approach to Achieving Child Health Development. The Milbank Quarterly 78(3):447-497.
Trajectory Without RR and HP Strategies
0 20
Hea
lth
Dev
elo
pm
ent
40 60 80Age (Years)
HP
RR Risk Reduction Strategies
Health Promotion Strategies
Optimal Trajectory
Protective Factors
HP HPHP
RR
RR
RR
Risk Factors
16
HANDS – strengths-based; builds resilience; hardwires social-emotional pathways; improves family functioning; intervenes early in life course; long term payoff in outcomes

• Data driven decisions• Research to practice• Standards of care• Evidence-based
practice• Continuous quality
improvement• Late preterm brain
Development• Outcomes• Fetal Origins of disease
• Life course perspective– Critical periods– Cumulative effects– Interactions with
Environment– Protective factors, build
resilience
• Social determinants of health
• Ecological approach• Community-based
interventions (real world)• Prevention pays

• Implement Health Promotion and Education efforts to Improve Birth Outcomes and Reduce Infant Mortality
• Ensure Quality of Care for all Women and Infants• Enhance Service Integration and Supports for Women and
Infants• Improve Maternal Risk Screening for all Pregnant women• Improve Access to Health Care for Women before, during,
and after pregnancy• Use Data to Understand and Inform Efforts to Promote
Healthy Birth Outcomes and reduce adverse birth outcomes• Eliminate Health Disparities and Promote Health Equity to
improve birth outcomes and reduce Infant MortalityAMCHP Infant Mortality Compendium Draft 1-2012

The Prematurity Problem The Kentucky Data
For the Kentucky Prematurity Steering CommitteeNovember 14th, 2005Louisville, KY
Prepared by the Kentucky Department for Public Health, Division of Adult and Child Health Improvement

543,000
520,000
508,356
499,008
480,812
476,250467,201
450,000
500,000
550,000
2000 2001 2002 2003 2004 2005 2006
*2006 preliminary birth data provided by the National Center for Health Statistics; Source: National Center for Health Statistics
March of Dimes Prematurity Campaign
Prematurity Rates in U.S.
U.S. Babies Born Preterm, 2000-2006

21
Premature Birth Report Card
3

Percent of Live Births that were Preterm*; Kentucky and U.S.
*Preterm birth is defined as any live birth occurring <37 completed weeks gestation
Data Source: March of Dimes Peristats & National Center for Health Statistics
11.6 11.7 11.812.5 12.7 12.7
13.613.3
1414.4
15
12.712.512.312.111.911.611.811.611.41111
0
2
4
6
8
10
12
14
16
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
Per
cen
t
KY U.S.

Percent of Live Births that were Preterm* Among Southern Contiguous States
11 1
1.6
11
.9
12
.1
12
.3
12
.5
12
.7
11
.3
12
.7 13
.3
13
.6
14 1
4.4 15
10
.7
12
.7 13
.2
13
.4
13
.3 14 1
4.4
11
.6
11
.7
11
.7
11
.8
12
.1
12
.1
12
.313
.4
13
.5 14
13
.8
14
.1
14
.5
14
.7
0
2
4
6
8
10
12
14
16
1993 2000 2001 2002 2003 2004 2005
Per
cen
t
U.S.
KY
WV
VA
TN
*Preterm birth is defined as any live birth occurring <37 completed weeks gestation
Data Source: March of Dimes Peristats & National Center for Health Statistics

KY singleton Preterm Births Delivered Vaginally
0
500
1000
1500
2000
2500
3000
3500
1993 2000 2001 2002 2003 2004 2005
Nu
mb
er
<=26 wks.
27-28 wks.
29-30 wks.
31-32 wks.
33-34 wks.
35-36 wks.
*Preterm birth is defined as any live birth occurring <37 completed weeks gestationData Source: Kentucky Vital Statistics Files, Live Birth Certificate Files, 1993, & 2000-2005

KY Singleton Preterm Births by Cesarean Delivery
0
500
1000
1500
2000
2500
1993 2000 2001 2002 2003 2004 2005
Nu
mb
er
<=26 wks.
27-28 wks.
29-30 wks.
31-32 wks.
33-34 wks.
35-36 wks.
*Preterm birth is defined as any live birth occurring <37 completed weeks gestationData Source: Kentucky Vital Statistics Files, Live Birth Certificate Files, 1993, & 2000-2005

Singleton Preterm Birth RatesUS and Kentucky, 1994-2004
Singleton Preterm Births (<37wk)
Late Preterm Births (34-36 wks)

What is HANDS?
Health Access Nurturing Development Services
Voluntary, intensive weekly home visitation
First time moms or first time dads
Regardless of income
Prenatal to two years of age
Designed to improve both health & social outcomes 27

31% less Prematurity33% less LBW55% less VLBW70% less Infant Mortality50% less ER Usage29-40% less Child Abuse and
Neglect26% improved/increased EducationLess developmental delays
Outside Evaluator
OUTCOMES
28

0
2
4
6
8
10
12
Number of Prenatal Hands Visits
Per
cent
of B
abie
s B
orn
Pre
mat
urel
y
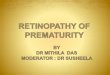
Series1 10.7 10.7 8.9 8.4 4.2
No pre-natal HANDS visits* 1-5 6-10 11-15 16+
Prematurity and Number of Prenatal HANDS Home Visits (based on 2000-2003 data for all teen mothers with no prior pregnancies, n=19,369)
The likelihood of having a child born prematurely decreases for mothers
w ho receive at least 6 prenatal HANDS home visits. Higher numbers of prenatal HANDS visits appear to contribute to a furthur reduction in the rate of premature births.
Note: May include families w ho received subsequent post-natal
HANDS visits.
Data sources: Kentucky Vital Statistcs Data and
HANDS participant database
PREMATURITY in HANDS Participants

Mothers who participated in at least 6 prenatal home visits were less likely to deliver a baby prematurely (before 37 weeks of gestation), as compared to HANDS eligible women who received no prenatal HANDS visits.
Prematurity – 31% less
30

0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
Per
cen
t o
f V
LB
W N
ewb
orn
s
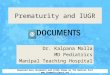
Series1 1.61 1.33 0.85 0.66 0.32
No pre-natal HANDS visits* 1-5 6-10 11-15 16+
Very Low Birth Weight (<1500 grams) by Prenatal HANDS Home Visits (based on 2000-2003 data for all teen mothers with no prior pregnancies, n=19,369)
The rate of very low birth w eight (VLBW) of new borns to teen mothers w as
positively correlated w ith the number of pre-natal HANDS home visits received by the mother. This data provides further evidence that HANDS visits contribute to improved birthw eight outcomes.
Note: May include families w ho received
subsequent post-natal HANDS visits.
Data sources: Kentucky Vital Statistcs Data and
HANDS participant database
VLBW


The BeginningsJoy Marini, M.S.P.A-C

An Initiative to Prevent Preterm Birth
• A ‘real world’, ecological design using evidence-based interventions in different health care settings (academic, private, clinic-based)
• An innovative, multi-dimensional intervention program designed to prevent “preventable” preterm birth in subgroups of the population where interventions have a likelihood of success in a reasonable period of time

Why Kentucky? State Selection for the first HBWW Primary Criteria (screening states):• Minimum of 40,000 births a year• 2003 state preterm birth rate of 13% or higher• PTB rate that has increased by at least 20% total (10%
singleton) in the past decadeSecondary Criteria:• DPH committed to reducing PTB rates (with focus on the LPTB)• Medical/nursing communities support and commitment• Related professional and state organizations support• High rates of modifiable risk factors• Control site availability• Number of hospitals – centralization of care considerations • NICU financial considerations

Kentucky Site Selection High rate of singleton preterm births, especially late
preterm births (34-36 weeks), that has risen steeply over the past decade
High prevalence of preventable/reversible risk factors including smoking, inadequate prenatal care, inappropriate weight gain during pregnancy, and unnecessary obstetrical/medical interventions prior to term/39 weeks.
Delivery volume contributing sufficiently to an overall sample size of 6000 live births in a 3 year period for a total project sample size of 12,000 live births (6000 each in the intervention and comparison sites)
Health community with interest to embrace HBWW, including a strong and functional clinical/public health community with high potential for collaboration


Local Partnerships:Varied Practice Models
• King’s Daughters, Ashland • Private practice physicians who deliver at the local hospital• Local health department• Rural community
• Trover, Madisonville • Hospital-based clinic practice; docs, midwives• Centering for low risk patients• Local health department • Rural community
• University of Kentucky, Lexington• University-based clinic practice; residents• Centering for Hispanic Patients• Local health department • Urban community

Five Core Components of HBWW:The 5 P’s
Partnership and
Collaboration
Provider Initiatives
Patient Support
Public Engagement
Progress Measures

National Partners:Johnson & JohnsonNational March of Dimes
Chapter March of DimesState Department of HealthHospitalsLocal Health DepartmentsLocal MediaKentucky Folic Acid
PartnershipKentucky Perinatal
AssociationKentucky Public Health
Association
Partnerships: The first “P”
Partners
Strategic PlanningImplementation (broadly)Provide ResourcesConvene Local PartnersCommunicationsEvaluation
State/NationalPartners’ Roles

Partnership Structure
•Organizational and financial oversight
Steering Committee
•Primary responsibility for program design and execution
Program Board
•Advise on all aspects of program planning and implementation
•Comprised of state (KY) experts in obstetrics, pediatrics, family medicine, nursing, oral health, public health, epidemiology
Site Council
•Technical assistance in specialized areas of the Program Board•Co
mmunications (CWG), Intervention (IWG), Evaluation (EWG)
Work Groups
•Local organizer to provide on-the-ground support and synchronize program activities in the field
Program Coordinator

Site-specific GrantsHealth Dept. Intervention Sites
Year 1 Year 2 Year 3 (6 mos)
Eval (6 mos)
TOTALS
Community Setting A
25K 25K 12.5K 12.5K 75K
Community Setting B
29K 29K 14.5K 14.5K 86K
University Urban Setting
75K 75K 37.5K 37.5K 225K
Other budget items for the Kentucky HBWW included:• Program coordinator for 6 sites• Consultants (e.g. evaluation, web)• Materials• Meetings

ImplementationKatrina Thompson, M.S.W.

Five Core Components:The 5 P’s
Partnership and
Collaboration
Provider Initiatives
Patient Support
Public Engagement
Progress Measures

Healthy Babies are Worth the WaitP2 – Provider Initiatives * Grand Rounds (state of art in PTB prevention)
* Brain Growth in Late Preterm Babies * ACOG Guidelines (induction, elective C/S,
progesterone, antenatal steroids, LPTB, etc.) * Aggressive Treatment of Infections, STI
* Resource centers with Cutting edge journal articles and latest research
* Patient Safety (Steve Clark, Kathleen Simpson)* Quality Improvement, provider feedback
* Oral Health Screening & referral* Psychosocial screening & referral* Smoking Cessation (5A’s)* Breastfeeding

Healthy Babies are Worth the WaitP2. Provider Initiatives
Physicians (OB, FP, Peds), Midwives, APRN’sResidentsNursesDentistsPharmacistsHealth educatorsHome visitorsAdministratorsCommunications staffRisk Management staffQuality Assurance staff

Healthy Babies are Worth the Wait
P3. PATIENT SUPPORT* “Every Week Counts” – emphasizing a healthy pregnancy should last to about 40 weeks (term)* Brain Development in the late preterm period* Early referral to public health programs – WIC, home visiting (HANDS), smoking cessation, QUIT line, etc.* Health Literacy- pregnancy diaries on line and hard copy* Promoting pre/interconception care* HBWW Information Items; totes, brochures, posters,
toothbrushes, magnets, picture frames, pregnancy due date wheels, fans, t-shirts, bookmarks, etc. * Text-4- Baby* same messages used in a variety of ways at each of the sites

Patient
Brochures

HBWW Consumer Surveys• Provided up-to-date, locally relevant KAB information from pregnant women, the target of the
HBWW Initiative• Based on findings, able to tailor educational materials and communication efforts of Initiative
to community needs• Results will be important for evaluation of the Initiative • (baseline vs. 3 year follow-up)
Materials
for
Professiona
ls

Healthy Babies are Worth the Wait
Materials

Healthy Babies are Worth the WaitP4. PUBLIC ENGAGEMENT• Governor’s Announcement at kickoff• Kentucky Toolkit for Community-Based
Prematurity Prevention activities• “Ask me” buttons, T-shirts for staff• “Born too Soon” Documentary by KY PBS• Media stories• Web site• Facebook, Twitter• Professional meetings

52www.prematurityprevention.org

Healthy Babies are Worth the Wait
“Real World” ecological model
Bundled interventionsDesigned to be adaptable to each community’s assets and resourcesCovered all aspects of best practices in prematurity prevention
Goal to Build better systems of care, support, and awareness within each community

Healthy Babies are Worth the Wait
Reducing elective induction and cesarean delivery before 39 weeks gestation.
• ISW – ACOG practice review (risk management initiatied)• Admitting patients not in labor• Inducing patients with unripe cervix• Standardized criteria for dating
• ISC – Attending review of all elective deliveries• Resident education• Nursing empowerment
• ISE – Quality review and provider report cards• Competition and education• Progressive reduction in rate of elective
& late preterm deliveries every year of project

Provider Interventions
Summary of Inductions and Scheduled C/S of Infants prior to 39 wks GA
PHYSICIANS TotalMedical
Indication
Medical Indication
Rate
Infants Admitted to NICU Who Were
Induced or Sectioned Without Medical
Indication
Doc A 5 5 100% 0
Doc B 3 1 33% 0
Doc C 2 2 100% 0
Doc D 3 2 66% 0
Grade Card for Physicians

Late Preterm BirthMonthly Comparisons
(percent of deliveries)
Jan
Feb Mar Apr May
Jun Jul Aug Sep Oct Nov Dec YR Avg
2006 11 10 10 11 18 13 11 20 13 8 16 10 13
2007 14 21 13 launch
12 10 11 12 11 7 9 8 13 12
2008 12 12 12 11 14 13 10 8 10 10 10 11 11
2009 6 7 7 13 19 7 6 9 8 11 6 11 9
Before implementation of an official dept policy
Provider Interventions

Healthy Babies are Worth the Wait
Oral Health• ISW - Dental hygenist regular presenter in Centering
• Dental Chair in Women’s Center at hospital– When moved to Health Dept a block away, patients did not
go
• ISC - Improved coordination with dental school clinics • increased emphasis with residents and nurses on oral
screening and care for patients• ISE - No dentists in area would treat pregnant
women• Hosted regional meeting with area dentists and OB’s,
nationally known dentist as speaker• Several local dentists then agreed to see pregnant
women referred by their obstetrician

Healthy Babies are Worth the Wait
Substance abuse prevention and management.• ISW - Improved local access to substance-abuse
treatment for pregnant women
– began universal screening for substance abuse as part of prenatal care; non-stigmatizing, non-punative
• ISC - Improved coordination with in-house detox unit for managing substance abuse in pregnancy
– Implemented universal psychosocial screening• ISE - Grand rounds on use of subutex by addiction
specialist for substance abuse in pregnancy– Hospital social worker went to OB offices to see
and do brief intervention with substance-abusing patients

Healthy Babies are Worth the Wait
Co-location of services/ Access• ISW –
• Dental chair in Women’s Center• WIC coordinator presented at Centering
• ISC • Hospital OB nurse educator attended health dept
clinics• Health Dept educator attending hospital OB clinics
• ISE • Hospital social worker goes to OB offices• Health dept staff integrated with pre-admission
teaching

Healthy Babies are Worth the Wait
Psychosocial Screening• ISW –
• Covered depression and mental health in Centering• Initiated substance abuse screening
• ISC • Implemented psychosocial screening in OB EMR• Made questions required fields that could not be
skipped• ISE
• Hospital social worker able to do more screening, brief intervention and referral in OB offices and in hospital

Healthy Babies are Worth the Wait
P 4. PUBLIC ENGAGEMENT ISW – Hospital used for Branding – billboards,
newsletters, T-shirts - Health dept utilized HBWW toolkit with all pregnant women in all programs- Presentations provided HBWW messages to civic groups, faith-based groups, schools, health fairs, home visitation programs, prisons
ISC – Newspaper articles- featured at large March of Dimes events- Community health magazines (hosp & health dept)
ISE – Internal marketing – daily team huddles, paycheck stuffers, staff newsletters- community health fairs, businesses- Local Television stories, Radio PSA’s

Communication Samples
Billboard
Billboard
Newspaper

Community Toolkit
MESSAGES:• Full Term is about 40 weeks
• Unless there are medical complications, women should try to take pregnancy to a full 40 weeks, because….
• Much of the brain development happens in those last 4-6 weeks of pregnancy
• Preventing prematurity improves the lives of families and communities
• Available at www.kfap.org (The KY Folic Acid Partnership)

Measuring Progress and Lessons Learned

Five Core Components:The 5 P’s
Partnership and
Collaboration
Provider Initiatives
Patient Support
Public Engagement
Progress Measures

Healthy Babies are Worth the Wait5. PERFORMANCE/PROGRESS Measures• Evaluation (pre & post surveys, focus groups,
both formative and summative)• Environmental and Policy Changes• Methods to Measure Progress at Site Level• Utilizing Potential Data Sources• Establishing Baseline Measures• Methods to measure community-wide outcomes• Perinatal Outcomes• Quality Improvement Activities • Using Data to Create Change

Percent Change in Preterm and Late Preterm Birth Rates US, KY and Selected Contiguous States, 2006-2008
67
Preterm (<37 wks) Late preterm (34-36 wks)
2006 2007 2008
% Chng 06-07
% Chng 07-08 2006 2007 2008
% Chng 06-07
% Chng 07-08
United States 12.8 12.7 12.3 -0.8 -3.1 9.1 9.0 8.8 -1.1 -2.2
Kentucky 15.1 15.2 14 0.7 -7.9 10.9 11.0 10.2 0.9 -7.3
Tennessee 14.8 14.2 13.5 -4.1 -4.9 10.3 10.0 9.7 -2.9 -3.0
Virginia 12 12.1 11.3 0.8 -6.6 8.6 8.6 8.1 0.0 -5.8
West Virginia 14 13.9 13.7 -0.7 -1.4 10.3 9.9 10 -3.9 1.0
Indiana 13.2 12.9 12.4 -2.3 -3.9 9.5 9.3 8.9 -2.1 -4.3
Ohio 13.3 13.2 12.6 -0.8 -4.5 9.4 9.2 8.7 -2.1 -5.4
Source: NCHS 2010

Percent Change in Program Eligible Preterm Birth Rates at HBWW Sites2006-2010
68
Preterm (<37 wks)
2006 2007* 2008* 2009* 2010**% Chng
07-08% Chng
08-09% Chng
09-10
Intervention East 15.6 15.4 14.4 13.6 13.6 -6.5 -5.6 0
Intervention West 14.8 16.9 15.5 14.0 13.9 -8.3 -9.7 -0.7
Intervention Central 13.3 14.4 13.9 15.1 11.7 -3.5 8.6 -22.5Combined Intervention 14.4 15.3 14.4 14.3 12.9 -5.9 -0.7 -9.8Comparison East 14.4 10.1 9.5 14.4 11.4** -5.9 51.6 -20.8**Comparison Central 21.3 19.4 17.4 18.2 17.0** -10.3 4.6 -6.6**Comparison West 12.5 11.6 10.2 13.3 10.6** -12.1 30.4 -20.3**Combined Comparison 16.6 14.4 13.1 15.9 13.8 -9.0 +21.4 -13.2**
*Program Intervention March 2007 thru Dec 2009** Comparison sites began HBWW interventions in January 2010Data Source: Healthy Babies are Worth the Wait program data; singleton, inborn deliveries only
Sustained effect

Percent Change in Program Eligible Late Preterm Birth Rates HBWW Sites 2006-2010
69
LATE PRETERM (34-36 wks)
2006 2007* 2008* 2009* 2010**% Chng
07-08% Chng
08-09% Chng
09-10
Intervention East 13.3 12.1 11.4 10.8 10.2 -5.8 -5.3 -5.6
Intervention West 11.0 12.2 12.5 11.3 11.7 2.5 -9.6 3.5
Intervention Central 9.1 9.8 8.6 10.9 8.0 -12.2 26.7 -26.6Combined Intervention 10.9 11.1 10.5 10.9 9.6 -5.4 +3.8 -11.9
Comparison East 11.7 8.3 8.3 12.3 9.2** 0 48.2 -25.2**
Comparison Central 14.9 13.1 12.5 12.3 11.2** -4.6 -1.6 -8.9**
Comparison West 10.8 9.0 9.0 11.1 9.2** 0 23.3 -17.1**
Combined Comparison 12.7 10.5 10.3 12.0 10.2** -1.9 +16.5 -15.0**
*Program Intervention March 2007 thru Dec 2009** Comparison sites began HBWW interventions in January 2010Data Source: Healthy Babies are Worth the Wait program data; singleton, inborn deliveries only
Sustained effect
Rest of KY had slight increase LPTB

Healthy Babies are Worth the WaitWHAT WENT WELL?:• Building Relationships and partnerships at all
levels• Accepting that the integrated concept required
different measurement and evaluation than linear cause-> effect
• Systems-building by seeking to identify gaps and fill them according to each community’s needs
• Engagement – people can identify and invest in prematurity prevention
• Motivation to keep it going despite competing priorities through networking and peer to peer learning
• Speeding the time from Research to Practice• KY was able to move the needle on reducing
preterm birth• Gains have been sustained in participating
sites

Healthy Babies are Worth the WaitWHAT MIGHT WE DO DIFFERENTLY?:• Have a dedicated project coordinator at each site• Must have a Physician Champion for improving
quality of clinical care.• Involve the community right from the start – more
community engagement• From the beginning, have an evaluation plan and
data collection plan with timelines so that everyone will know the expectations and be able to see successes.
• Celebrate more and increase project visibility with rewards and recognition

Community Based Prematurity Prevention
ARRA PUTTING COMMUNITIES TO WORK GRANTS – promoting policy and environmental change thru MAPPS:
• MEDIA – social marketing for importance of going to term, late preterm brain development, oral health s, etc.
• ACCESS – coverage, co-location, availability• POINT OF DECISION – Education on avoiding <39
week elective deliveries, Late preterm brain development
• PRICE – costs of prematurity – financial, emotional, and other for families, the health care system, and communities
• SYSTEMS & SUPPORT – identifying and filling gaps in the community systems of perinatal care and support services

Consumer & Public Awareness• Goldenberg et al, 2009. Women’s Perceptions Regarding the Safety of
Birth at Various Gestational Ages. Obstet Gynecol 2009. 114:1254-8
• Survey of 650 women enrolled in an insurance plan who had recently had a baby
“At what gestational age do you believe a baby is considered full term:
– Responses of </=37 weeks 45.7%
– 38 weeks 29.1%
– 39-40 weeks (correct response) 25.2%
• 92% thought that giving birth before 39 wks was safe

Community Based Prematurity Prevention
COMMUNITY TRANSFORMATION GRANTS:• Integrating High Quality Clinical services with
Community resources to create a comprehensive system of [perinatal] care
• Community or state level Policy and Environmental Changes for Chronic Disease prevention
Current CTG Future CTG??
Physical Activity Prematurity reduction
Nutrition Pre/Interconception care
Tobacco Safe Sleep

Questions for discussionWhat has your state done to implement community
based projects for reducing prematurity and infant mortality?
What interventions can/have been taken to scale in your state?
(e.g. state-wide maternal screening, any-door entry to services)
How are these being paid for?
What ideas might be applied in all states as a regional effort?