Embed Size (px)
Citation preview
LISA ARCHIBALD—2013 WINSTON CHURCHILL FELLOW
”COMMUNITIES THAT WORK” CATEGORY
CHALLENGING PREJUDICE AND DISCRIMINATION DIRECTED TOWARDS
PEOPLE WITH MENTAL HEALTH CHALLENGES IN COMMUNITIES
“He aha te mea nui o te
Ao? He tangata, he
tangata, he tangata”
“Let me ask you, what is
the most important thing
in this world?
It is people, it is people, it
is people”
ACKNOWLEDGEMENTS:
I DEDICATE THIS REPORT TO MY KIND, INTELLIGENT, REFLECTIVE FATHER, ARCHIE, WHO PASSED AWAY FROM MOTOR NEURONE DISEASE 6 WEEKS BEFORE I BEGAN MY FELLOWSHIP. I FEEL THANKFUL TO HAVE BEEN
GIVEN THE OPPORTUNITY TO TRAVEL THE WORLD, A CHANCE HE NEVER HAD.
THANKS TO: WINSTON CHURCHILL MEMORIAL TRUST FOR THE LIFE CHANGING OPPORTUNITY.
THE AMAZING STAFF, COMMITTEE AND MEMBERSHIP OF NEW HORIZONS BORDERS, SIMON BRADSTREET AND THE SCOTTISH RECOVERY NETWORK TEAM, MEG ROPER AND BVCV, GRAHAM MORGAN AND ALL AT HUG, THE
INSPIRING LORRAINE NICHOLSON, HILARIOUSLY FUNNY AND POETIC EDINBURGH JO, RON COLEMAN AND KAREN TAYLOR, GLENN MERRILEES, HELEN GRAY, SUE BAKER, MENTAL HEALTH FOUNDATION (SCOTLAND), DR RACHEL
PERKINS, JOAN BREE AND SEE ME, JANETTE WESTHEAD, GROW, LIKE MINDS LIKE MINE, MARY O’HAGAN AND THE PEERZONE TEAM, MARGE JACKSON AND KITES, MAGDEL HAMMOND AND CONNECT, CASSANDRA LASKEY AND
EVERYONE AT MATARAKI, COUNTIES MANAKAU DISTRICT HEALTH BOARD, BLUEPRINT, MIND & BODY, FRANK BRISTOL AND BALANCE, FELLOW SCOT SHAUN MCNEIL AND THE CHATTY JOSHUA PALMER AT WELLINK, THE
BRILLIANT CHRISTCHURCH MENTAL HEALTH FOUNDATION TEAM AND THE ASTOUNDING ALL RIGHT CAMPAIGNERS, SUE RICKETTS AND MHAPS, MY IPS MENTOR DAWN HASTINGS, COMCARE, THE VERY FUNNY GAYLE BRISLANE AND THE DEPRESSION SUPPORT NETWORK, VAL DOCKERTY AND HER HOSPITABLE FAMILY,
GRANT COOPER AND EVERYONE AT OTAGO MENTAL HEALTH SUPPORT TRUST, TE ARA KOROWAI, MARY EASTON AT JOURNEYS TO WELLBEING, SUPPORTING FAMILIES IN WHANGANUI, THE VERY KIND AILSA FENTON AND
EVERYONE AT FOOTSTEPS, PACT, RAEWYN CLARKE AND SOUTHLAND DISTRICT HEALTH BOARD, DESLEY CASEY AND CAN MENTAL HEALTH NETWORK. ALSO THANKS TO JULIE REPPER, STEVEN MORGAN, SHERY MEAD (IPS)
FOR THEIR INSPIRATION.
THANKS ALSO TO MY FAMILY AND MY FRIENDS WHO HAVE FAITH IN MY ABILITIES EVEN WHEN I DON’T.
“NEARLY NINE OUT OF TEN PEOPLE WITH MENTAL ILL HEALTH SAY THAT STIGMA AND DISCRIMINATION HAVE A NEGATIVE EFFECT ON THEIR LIVES. SOCIETY IN GENERAL HAS STEREOTYPED VIEWS ABOUT MENTAL ILLNESS AND HOW IT AFFECTS PEOPLE. MANY
PEOPLE BELIEVE THAT THOSE WITH A MENTAL ILLNESS ARE VIOLENT AND DANGEROUS, WHEN IN FACT THEY ARE MORE AT RISK OF BEING ATTACKED OR HARMING THEMSELVES
THAN HARMING OTHER PEOPLE” (MENTAL HEALTH FOUNDATION).
“The stigma of mental ill-health is based on ill-
founded prejudices which have been with us for
a long time.
People in Scotland with mental ill health are
discriminated against in day to day life.
Stigma and discrimination due to mental ill-
health should not still be with us...[It] damages
people’s hopes, lives and relationships
(SEE ME)
AN EXTRACT FROM “BARRIERS” BY GLENN MERRILEES
THERE’S PEOPLE THROWING INSULTS
THERE’S PEOPLE THROWING STONES
YOU CANNOT SEE THIS ILLNESS
NO SIGN OF BROKEN BONES
SO MANY NASTY COMMENTS
REMARKS ARE SO UNKIND
YOU CANNOT SEE THIS DARKNESS
THIS POISON IN THE MIND.
HEY LOOK, THAT GUY IS MENTAL
A LOONEY, WHAT A WASTE
YOUR BITTER, TWISTED
COMMENTS
LEAVE AN ACRID TASTE.
JUST REMEMBER I’M A VICTIM
TO THIS PAIN YOU CANNOT SEE
DEPRESSIONS MADE A HOME IN
HELL
ESPECIALLY FOR ME.
DO NOT JUDGE THIS COVER
YOU SIMPLY HAVE TO LOOK
I’M DROWNING IN A SEA OF PAIN
PAGES MISSING FROM THIS BOOK.
WOULD YOU BERATE THE LOWLY
CRIPPLE
AND CALL POOR SOUL A NAME
MY ILLNESS NEEDS NO CRUTCHES
HANG YOUR HEAD IN SHAME.
PEOPLE’S EXPERIENCES OF DISCRIMINATION IN SCOTLAND
“BECAUSE I HAVE A
MENTAL HEALTH
DIFFICULTY, NOBODY
TRUSTS ME, THEY
DON'T LISTEN TO ME,
THEY DON'T BELIEVE
ME, THEY DON'T
ACTUALLY THINK THAT
I’VE GOT A BRAIN”
HUG MEMBER, STIGMA:
MARKED BY SOCIETY?
DVD
“I’VE BEEN VICTIMISED AND BULLIED FROM
TEACHERS, PUPILS, THE WHOLE SHEBANG. I WAS A
VICTIM AT HOME AND A VICTIM OUT IN THE
COMMUNITY.
I’VE ALWAYS BEEN PICKED ON. I WENT TO A
FESTIVAL ONE YEAR AND SOMEONE CAME UP AND
SAID I WAS A PSYCHO AND A WHOLE BUNCH OF
THEM STARTED JOINING IN. IT WAS HORRENDOUS.
I WENT HOME AND GOT VERY DRUNK. I WAS
VULNERABLE, I WAS ISOLATED. I WAS TERRIFIED
BUT NOW I’M NOT. FOR ME NOW, I TELL PEOPLE, I’M
NUTS AND PROUD BECAUSE FOR ME IT DOESN’T
MATTER WHAT DIAGNOSIS I’VE BEEN GIVEN IT
DOESN’T DEFINE WHO I AM ANYMORE. I HAVE MY
VULNERABILITIES BUT I DON’T LET IT RUN MY LIFE
ANYMORE. I’M HAPPY TO TALK ABOUT IT. I WANT TO
TALK ABOUT IT. “
HELEN, SCOTTISH BORDERS
I’VE BEEN STIGMATISED AND TRAUMATISED
FUR WHIT, I’VE DONE NO CRIME
LABELS THRUST UPON ME
NOO I’VE GOAT TAE SERVE THE TIME.
I’M A VICTIM, I’M A TARGET
DEPRESSIONS DEADLY CURSE
YER LOOKS, YER TWISTED WHISPERS
IT ONLY MAKES IT WORSE.
WE’VE GOAT TAE STOAP THIS STIGMA
WIPE IT OFF THE PLANETS FACE
WE’RE JUST PEOPLE WITH AN ILLNESS
PART OF THE HUMAN RACE.
FROM “STIGMA” BY GLENN MERRILEES
LORRAINE NICHOLSON, ARTIST AND POET FROM PERTH, UK, RECENTLY TOLD ME:
“I DIDN'T KNOW ANYONE WHO HAD DEPRESSION SO STIGMA KICKED IN EARLY. PEOPLE DON’T TALK ABOUT IT SO I FELT I WAS THE ONLY PERSON IN THE WORLD EXPERIENCING THESE SYMPTOMS. I DECIDED TO TACKLE STIGMA AND IT WAS ONE OF THE BEST THINGS
I DID, I WENT PUBLIC… CONSEQUENTLY I REALISED I WASN'T THE ONLY ONE, LOTS OF PEOPLE WERE AFFECTED BY DEPRESSION BUT STIGMA STOPPED THEM FROM TALKING
ABOUT IT“.
GRAHAM MORGAN OF HUG SPOKE OF AN INCIDENCE OF STIGMA HE HAD EXPERIENCED A FEW YEARS AGO:
“FLYING HOME FROM SPAIN, I GOT TO THE AIRPORT, ARRIVED REALLY EARLY AND
SOMEONE WAS ASKING WHAT I DID. I SAID I WORKED IN MENTAL HEALTH. HE SAID “WHY DO YOU DO THAT?”. I SAID “I HAVE A DIAGNOSIS OF SCHIZOPHRENIA”. HE TURNED
AROUND AND SAID “PEOPLE LIKE YOU ARE SCUM AND SHOULD BE WIPED OFF THE FACE OF THE EARTH AND DON’T DESERVE TO EXIST”. THAT’S THE BIGGEST THING AROUND
STIGMA THAT I HAVE EXPERIENCED. BUT THEN THERE ARE OTHER ONES THAT ARE MUCH MORE CONFUSING, I THINK, IS THIS STIGMA OR IS IT NOT?”
I AM LISA ARCHIBALD, SERVICE MANAGER OF A MEMBERS
LED CHARITY WHICH FACILITATES PEER SUPPORT SELF
HELP GROUPS AND COLLECTIVE ADVOCACY IN THE
SCOTTISH BORDERS.
THROUGH EXPERIENCE OF LIVING AND WORKING IN
SCOTTISH RURAL COMMUNITIES, I HAVE BEEN
INCREASINGLY AWARE THAT MANY PEOPLE, FEEL
“ASHAMED” OF TALKING ABOUT MENTAL HEALTH AND THAT
THEY HAVE “HAD TO HIDE IT” WHEN THEY ARE STRUGGLING.
PEOPLE HAVE DESCRIBED TO ME THE FEELING OF BEING “A
VICTIM IN THE COMMUNITY” AND OPENLY CALLED
OFFENSIVE TERMS LIKE “NUTTER” AND “PSYCHO”.
The language we use in the world of mental health has long been debated and the
opinions vary enormously!
However, it is important to recognise that language can reinforce stereotypes and can
increase discriminatory attitudes.
“The whole concept of ‘mental illness’ as an explanation of distressing human
behaviour has come into question. Calling something an illness does not make
it one, and psychiatrists have yet to demonstrate the existence of the illnesses
they have named and defined” (Chamberlin, 1987)
New Zealand is a country that benefits greatly from the beauty of the Maori language
and their models of health which are far more holistic and less clinical
In Maori, they talk about“Tangata Whaiora” – People Seeking Wellness
Traditional Māori health acknowledges the link between the mind, the spirit, the human
connection with whanau (family), and the physical world in a way that is seamless and
uncontrived.
Until the introduction of Western medicine there was no division between them.
The Māori philosophy towards health is based on a wellness or holistic health model.
For many Māori the major deficiency in modern health services is taha wairua (spiritual
dimension).
For Maori and Pacific people in particular, they generally see “mental illness” as a
pakeha (white European settlers) construct. They instead view mental well being as an
equal contributory part of our health along with family (whanau), physical well being
and spirituality. There are fantastic examples of Maori and Pacific models of health
which are used across mainstream health & education departments in New Zealand
not just within the cultural services.
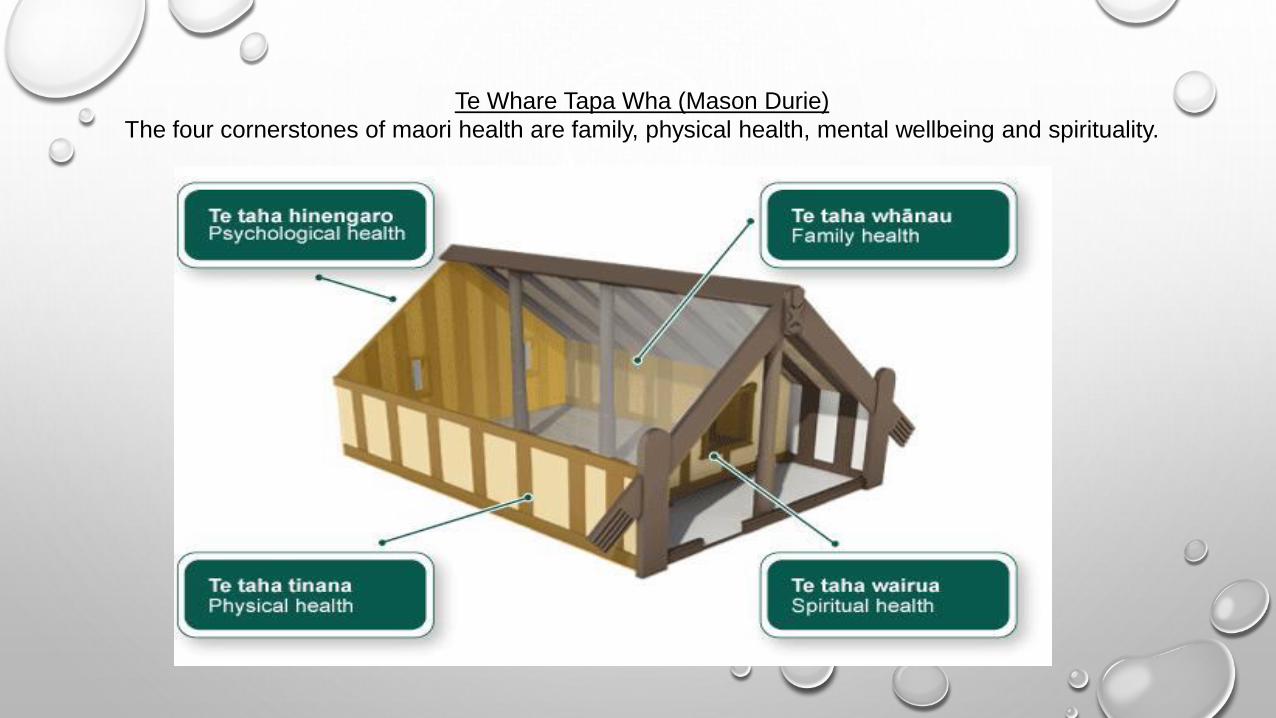
Te Whare Tapa Wha (Mason Durie)
The four cornerstones of maori health are family, physical health, mental wellbeing and spirituality.
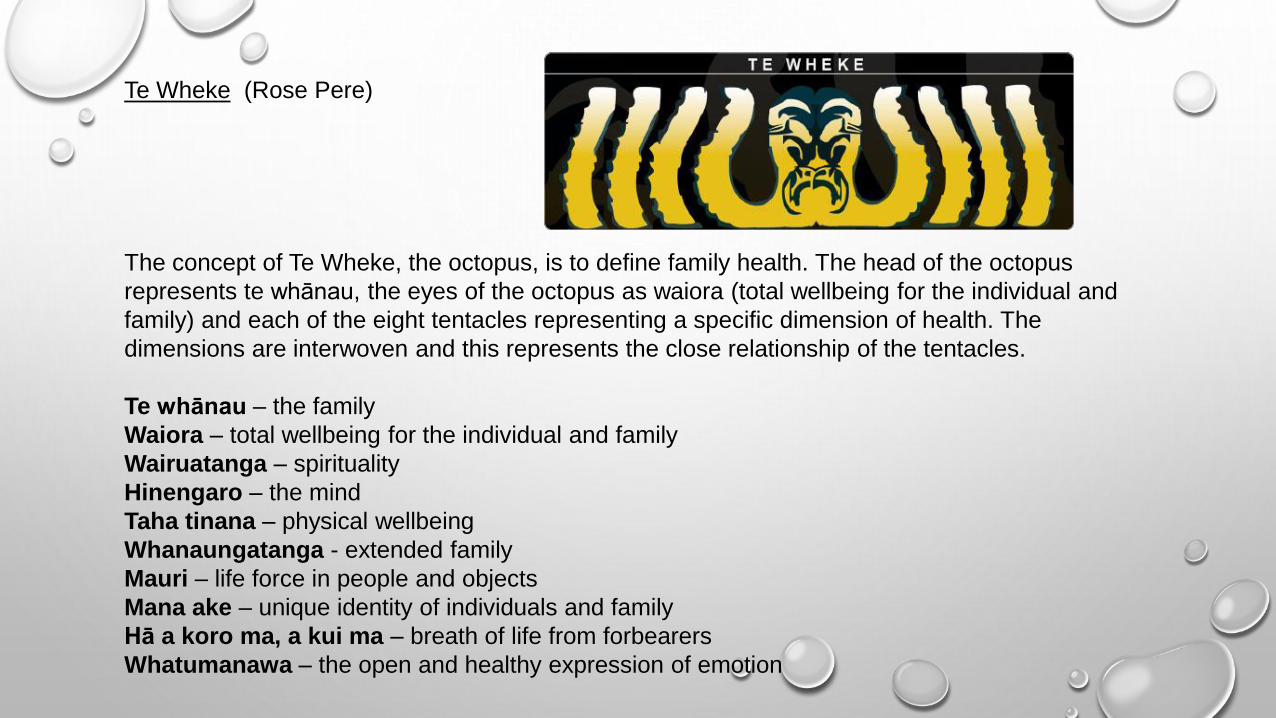
Te Wheke (Rose Pere)
The concept of Te Wheke, the octopus, is to define family health. The head of the octopus
represents te whānau, the eyes of the octopus as waiora (total wellbeing for the individual and
family) and each of the eight tentacles representing a specific dimension of health. The
dimensions are interwoven and this represents the close relationship of the tentacles.
Te whānau – the family
Waiora – total wellbeing for the individual and family
Wairuatanga – spirituality
Hinengaro – the mind
Taha tinana – physical wellbeing
Whanaungatanga - extended family
Mauri – life force in people and objects
Mana ake – unique identity of individuals and family
Hā a koro ma, a kui ma – breath of life from forbearers
Whatumanawa – the open and healthy expression of emotion
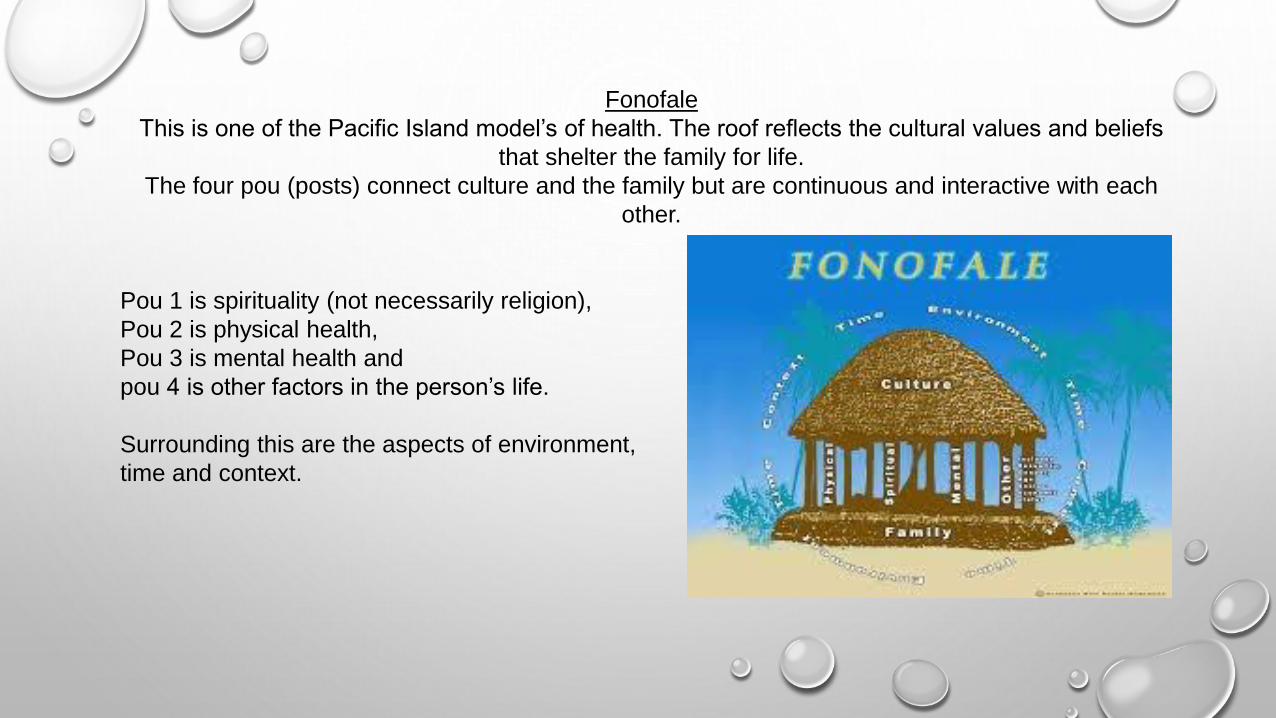
Fonofale
This is one of the Pacific Island model’s of health. The roof reflects the cultural values and beliefs
that shelter the family for life.
The four pou (posts) connect culture and the family but are continuous and interactive with each
other.
Pou 1 is spirituality (not necessarily religion),
Pou 2 is physical health,
Pou 3 is mental health and
pou 4 is other factors in the person’s life.
Surrounding this are the aspects of environment,
time and context.
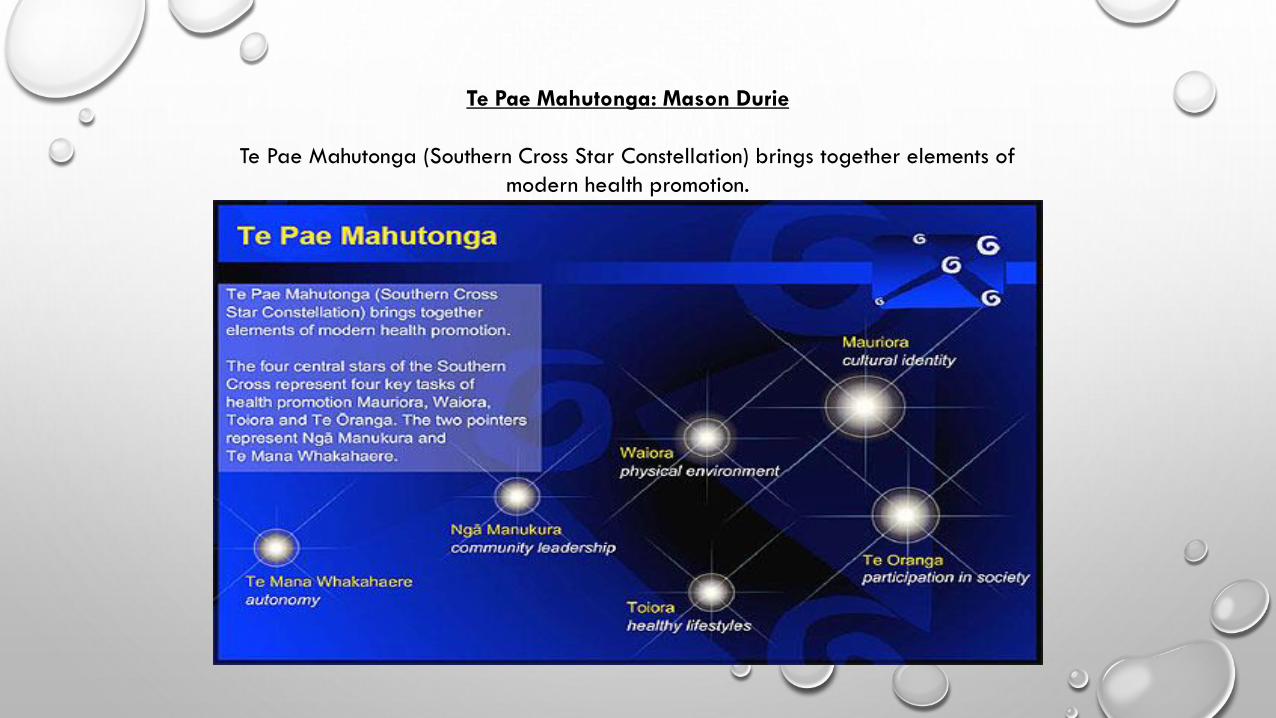
Te Pae Mahutonga: Mason Durie
Te Pae Mahutonga (Southern Cross Star Constellation) brings together elements of
modern health promotion.
These models of working are holistic, effective and view someone’s mental health as just
one part of their overall wellbeing, but they are all very culturally specific. They draw on the
beauty of the Maori and Pacific languages and spirituality, so are very appropriate for use
in New Zealand.
When spending time within some of the services in New Zealand who had a high
prevalence of consumers from the Maori communities, I was very aware that people would
draw similarities from their culture to mine as a Scot. For Maori people, ancestry and
genealogy is of huge importance. Many people I spoke with made comparisons between
the European settlers coming to New Zealand and the forced displacement of people
during the Scottish Highland clearances.
On a number of occasions, I was asked what clan I was from, referring to their Maori iwi
(tribes) and hapu (sub tribes/ clans). This made me very aware that as Scots, many of us
have experienced a loss of identity. However, as the move towards independence is taking
place it is becoming more apparent that Scottish people are re-embracing this aspect of
who they are. This could be an opportunity for a Scottish model of working to be introduced
that better meets the needs of our people using a language we can identify with.
The use of language and how people view mental health was a large topic of discussion
when I visited Mind and Body in Auckland.
Jim Burdett, Chief Executive:
“we are all on a continuum of human experience. We all experience wellbeing and
distress. It is an unsurprisingly appropriate human response to circumstances and
experiences, past and present”.
“you can reframe mental illness or create a new construct for mental illness.
Because it is something out there and the construct for a couple of hundred years
has been a scientific one that is to do with doctors, the health system and cured
with pills. But it is too universal to be anything other than a human problem”.
A fundamental human experience?
In the UK, most services are still constructed around scientific language, medication, care
plans, assessment and diagnosis.
New Zealand is instead generally viewing mental well health from a more holistic, human
experiential perspective. Therefore it is something we could all be affected by. Rather than
being seen a problem, challenge or something to “suffer from”, it is viewed more like a
journey therefore it is something we can move forwards from.
This approach is a key part of reducing stigma and discrimination.
After all, if it is reframed to be a “human experience” rather than about illness and deficit, it
reduces the likelihood that people will feel different which minimises the shame and guilt
people feel which often leads to self-stigma.
Dr Rachel Perkins is a UK psychiatrist (and former Winston Churchill fellow) who has lived experience of mental ill
health has written numerous papers on this subject. I was fortunate to interview her prior to beginning my
fellowship. Interestingly, Dr Perkins highlights the importance of the language used, preferring the terms
oppression, discrimination, exclusion or prejudice to stigma.
Dr Perkins believes that we need to create communities that can accommodate & provide opportunities for people
with mental ill health as equal citizens rather than medicating and treating individuals separately for their
"problems".
This viewpoint very much mirrors that of many of New Zealand’s services. It raises questions about whether the
current UK health system is meeting the needs of people by focussing mostly on medication and clinical input in
order to fix a problem seen to lie within the individual rather than addressing discrimination and prejudice that
happens in society.
Of huge concern is the observation that "People experience more discrimination in mental health services
than anywhere else“ (Dr Rachel Perkins).
This seems to be a common view shared by many people with experience of using UK mental health services.,
So how can we reduce this discrimination people are experiencing within the health service?
“Research shows that the best way to challenge stereotypes is through first hand contact
with people with lived experience of these challenges”. (Mental Health Foundation—
www.mentalhealthfoundation.org.uk).
However, first hand contact in itself is not enough, to be effective, the contact needs to “be on
equal terms with common goals in order to have a positive impact on attitudes and
beliefs” (Corrigan et al, 2011).
This is also called The Power of Contact and has been explored by Case Consultancy in 2005.
The Peer Worker and Consumer Advisor roles are valued and integrated in Australia and New
Zealand’s health services. These are roles which are reducing discrimination within the health service through the power of contact with people who have lived experience.
18
In 2005, Case Consulting Ltd published “The Power Of Contact”. This identifies the 3 fundamental
strategies for countering stigma and discrimination:
Education—replacing myths about mental distress with correct information
Contact—challenging discriminatory attitudes and behaviour through direct interactions with people
who experience mental distress
Protest—actions which suppress discriminatory attitudes and behaviours towards people who
experience mental distress.
The most important aspect of “The Power of Contact” is that it is not based on a one off interaction
but instead is about on going relationships.
The contact has to be:
• Based on equal status
• An ongoing developing of a relationship
• With mutually agreed goals

Scottish Recovery Network has supported the creation of Peer Worker roles in Scotland and we are
seeing some progress in this being now recognised as a valuable model of support.
However, while the Peer Worker role is progressing in the UK we still continue to have “service user
representatives” who are often untrained volunteers given a fairly tokenistic role in strategic
meetings and forums.
If we introduce paid, trained, supported “Consumer Advisers” posts (I prefer the title “Advisers
with Experience”) to UK health boards as they have done in Australia and New Zealand, we would
see the views of people who have experience being of equal contributory value to those of clinicians.
This will start to reduce the discrimination that takes place within the health services as it creates a
shift in the power balance and sense of “us and them” that exists. It will also make clinicians more
aware of the language they use in strategic processes which can often be discriminatory and deficit
based.
“It changes things from ‘once a consumer always a consumer’ to ‘once a consumer,
now a colleague’.
This is a cultural shift that helps everyone.
The introduction of a peer workforce is potentially the most effective catalyst for
synergizing cultural change in the services.
People who are open about their experiences and willing to be vulnerable suddenly
discover that there is a huge strength in that vulnerability. It reframes it. We slowly
change the world one relationship at a time.
The more we start the peer movement off about who we are, where we come from and
what’s happened to us is a whole different conversation in the services that have
been set up to describe what’s wrong with us.”
Frank Bristol, Consumer Advisor, Balance

New Zealand and Australia are also delivering some excellent awareness raising and educational
courses in communities, with employers and in services funded by Like Minds Like Mine (their
anti-stigma programme).
The best example I came across was MH101 by Blueprint (www.blueprint.co.nz) which had
outstanding results in terms of leading to long-term behaviour and attitudinal change in
participants.
I am fortunate that they agreed to share their materials with me and are open to discussing the
design of a culturally specific version of MH101 for delivery in Scotland.
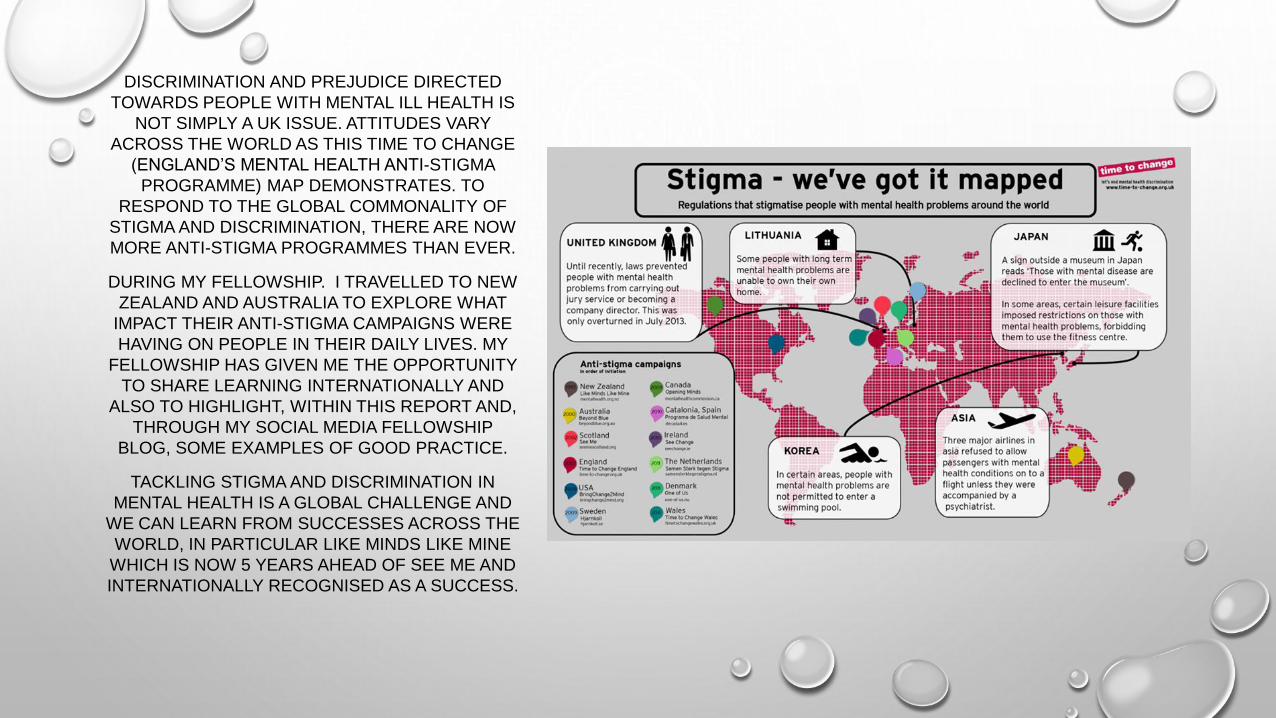
DISCRIMINATION AND PREJUDICE DIRECTED
TOWARDS PEOPLE WITH MENTAL ILL HEALTH IS
NOT SIMPLY A UK ISSUE. ATTITUDES VARY
ACROSS THE WORLD AS THIS TIME TO CHANGE
(ENGLAND’S MENTAL HEALTH ANTI-STIGMA
PROGRAMME) MAP DEMONSTRATES. TO
RESPOND TO THE GLOBAL COMMONALITY OF
STIGMA AND DISCRIMINATION, THERE ARE NOW
MORE ANTI-STIGMA PROGRAMMES THAN EVER.
DURING MY FELLOWSHIP. I TRAVELLED TO NEW
ZEALAND AND AUSTRALIA TO EXPLORE WHAT
IMPACT THEIR ANTI-STIGMA CAMPAIGNS WERE
HAVING ON PEOPLE IN THEIR DAILY LIVES. MY
FELLOWSHIP HAS GIVEN ME THE OPPORTUNITY
TO SHARE LEARNING INTERNATIONALLY AND
ALSO TO HIGHLIGHT, WITHIN THIS REPORT AND,
THROUGH MY SOCIAL MEDIA FELLOWSHIP
BLOG, SOME EXAMPLES OF GOOD PRACTICE.
TACKLING STIGMA AND DISCRIMINATION IN
MENTAL HEALTH IS A GLOBAL CHALLENGE AND
WE CAN LEARN FROM SUCCESSES ACROSS THE
WORLD, IN PARTICULAR LIKE MINDS LIKE MINE
WHICH IS NOW 5 YEARS AHEAD OF SEE ME AND
INTERNATIONALLY RECOGNISED AS A SUCCESS.
The Like Minds Like Mine anti-stigma movement has been delivering education and training to
communities throughout New Zealand since 1997. Internationally it has been recognised as a ground
breaking programme. The campaign has been led by and has focussed on the participation of people
with lived experience of mental distress since it’s inception.
This is recognised as the main reason behind it’s success
Like Minds Like Mine has two strategies.
• A national mass media and communications campaign.
• Regional programmes which meet the needs of communities led by local organisations who can
create innovative responses to specific issues of stigma and discrimination.
The programme has 3 outcomes:
Individual outcomes—for people experiencing mental distress to have the same opportunities as
everyone else to participate in society and in every day life of their communities.
Organisational outcomes—to have practices and policies that ensure people are not discriminated
against
Societal outcomes—nationally valuing and including people who experience mental distress.
Like Minds Like Mine achieves these outcomes in 3 ways:
• By providing opportunities for direct contact with people who experience mental distress.
• By promoting people’s rights and challenging the organisations and communities who discriminate.
• By delivering evidence based education and training facilitated by people with lived experience.
Local services are funded to facilitate training, awareness raising sessions and educational opportunities
to groups of people who are in a position to influence the life decisions of people who experience mental
distress.
Specific audiences are targeted in order to meet the outcomes of the programme and make the biggest
impact on communities.
Targeted groups include employers, family, housing providers, the media, community leaders, criminal
justice and government agencies such as work and income (the NZ employability and welfare benefits
services).
The Mental Health Strategy for Scotland 2012—15 prioritises “extending the anti-stigma agenda
forward to include further work on discrimination” and to “focus on the rights of those with a
mental illness”.
A reassuring recent development has been the 2013 announcement from the Scottish Government
that together with Comic Relief it will invest £4.5 million into a 3 year anti-stigma and discrimination
national programme.
This new investment is therefore an ideal opportunity to direct additional resources into localised,
targeted education programmes led by people with lived experience in order to lead to attitudinal and
behavioural change. This approach has proven to be successful with the Like Minds Like Mine
campaign in New Zealand. This is the most effective way Scotland can challenge prejudice and
discrimination which will in turn improve the lives of people with mental ill health in communities.
Public education through people “speaking out” locally can help change the perceptions of what
someone with a mental illness looks like or acts like. Training in communities and with employers
such as Blueprint’s MH101 would also be helpful.
Scottish Recovery Network has developed a new nationally recognised award for peer workers.
Whilst it is no doubt vital that Peer Workers should access training which will enhance their practice
and confidence in their role, adopting a structured model of working or using a values framework such
as the one SRN have developed (Smith and Bradstreet, 2011; Scottish Recovery Network, 2012) is of
more value than accredited qualifications. It also allows workers to “stay peer” (Perkins) and retains
that their experience is what makes them experts, not a qualification.
In the United States where peer-involved services have existed for some time, leading commentator
and trainer Shery Mead has defined peer-support as a ‘system of giving and receiving help
founded on the key principles of respect, shared responsibility, and a mutual agreement of
what is helpful’” (Mead et al, 2001).
Most of the services I visited in New Zealand and Australia that were offering a Peer Worker service
had opted to work within the Intentional Peer Support model (IPS) which has its roots in the USA
with Shery Mead, a peer consultant.
Intentional Peer Support (IPS) focuses on the connection between two people in a peer relationship
concentrating on learning and growing. IPS is about two way relationships which differs greatly from
the traditional power imbalanced relationship of clinician-client.
The model sees the person, not the clinical diagnosis or label they are given and is about well being
not illness. The relationships are not friendships and have a specific purpose. However there is
compassion and emotional safety as the person accessing peer support feels encouraged, heard
and not judged.
There are some examples of services in England, such as Chard Intentional Peer Support group in
Somerset, who are using the IPS model successfully following training from Shery Mead.
Currently the Intentional Peer Support model is not being offered within services in Scotland. Having
this model available would provide a structure to the fantastic work already being carried out which
is primarily informal and based within the voluntary sector.
In March, I will travel to Vermont in the USA on a scholarship to complete the Intentional Peer
Support training with the view to becoming an IPS Facilitator so this model can be available to peer
services in Scotland.
During my fellowship, I visited a number of outstanding services. Too
many to be able to explore in detail. The full list of services I visited
are at the end of this report.
I have chosen a few of the more memorable visits which are
examples of good practice that we can learn from in Scotland and in
the UK.
In Auckland, I visited a number of peer run acute residential respite services with Magdel
Hammond, General Manager of Connect. I was fortunate to chat with one of the guests at the
newly opened peer led residential Rodney service, Piri Pono, who, after a 10 day stay was getting
ready to go home
“For the first time ever I am able to properly communicate. Having just a few people here
means you get to know each other well, we really care about each other. In hospital, there
are too many people. The staff work 12 hour shifts and just don't care. Here you have time,
people care. I have learned so much about my own needs and my own healing. It's homely
and the colours are neutral, it's like a home but better. It feels calm.“
Guest, Piri Pono.
Having access to a welcoming home run by peers that used non-clinical language was a very
effective an alternative to hospital. Instead of being referred to as service users, consumers, clients
or patients, people are “guests”. They receive biographies of the peer workers and can select who
they feel they would like to be matched with. Through my discussions with the staff and the guests,
it was obvious that Connect created an environment of healing.
Balance, Whanganui
Balance in Whanganui is a peer run mental health charitable trust that makes a huge difference in the lives of
those affected by mental health and addiction issues in that area.
The kaupapa (mission) of Balance is “to provide high quality peer support, education, advocacy and training to
people (tangata whai ora) affected by mental health and addiction issues” Balance does this by providing
intentional self care (WRAP) and purposeful relationships (Intentional Peer Support).
When talking about his own recovery journey, David, a Like Minds Like Mine co-facilitator and advocacy
worker with Balance described it using the Japanese proverb “fall down 7 times, get up 8”.
“I think [the peer work force] could be a huge part of driving the change” Frank Bristol
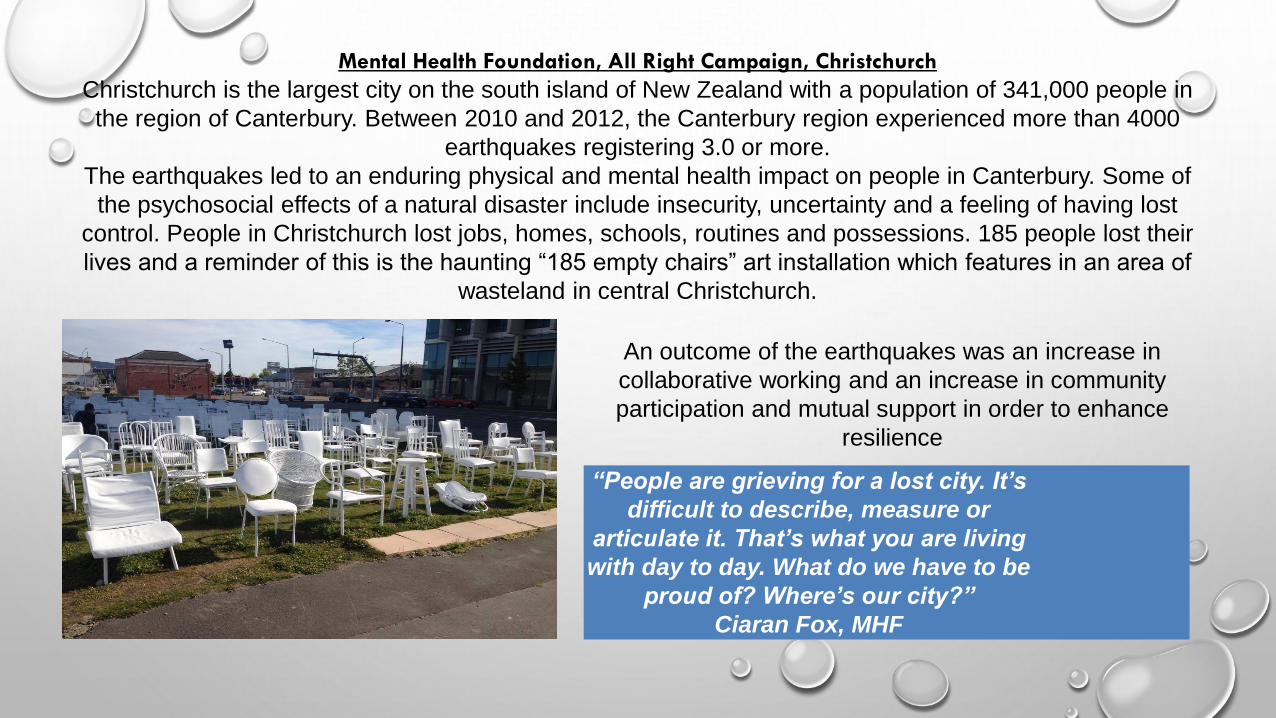
Mental Health Foundation, All Right Campaign, Christchurch
Christchurch is the largest city on the south island of New Zealand with a population of 341,000 people in
the region of Canterbury. Between 2010 and 2012, the Canterbury region experienced more than 4000
earthquakes registering 3.0 or more.
The earthquakes led to an enduring physical and mental health impact on people in Canterbury. Some of
the psychosocial effects of a natural disaster include insecurity, uncertainty and a feeling of having lost
control. People in Christchurch lost jobs, homes, schools, routines and possessions. 185 people lost their
lives and a reminder of this is the haunting “185 empty chairs” art installation which features in an area of
wasteland in central Christchurch.
An outcome of the earthquakes was an increase in
collaborative working and an increase in community
participation and mutual support in order to enhance
resilience
“People are grieving for a lost city. It’s
difficult to describe, measure or
articulate it. That’s what you are living
with day to day. What do we have to be
proud of? Where’s our city?”
Ciaran Fox, MHF
The Mental Health Foundation in Christchurch developed the All Right? Campaign which aims to
maintain and increase the mental health and well being of the people of Canterbury.
All Right? Is pitched at articulating to people how they can check in with themselves and others. “When
a crisis happens, people automatically check on each other – sharing water, running generators,
making soup. Humans have evolved that way, we are designed that way” Ciaran Fox, MHF
The most successful aspect of the All Right?
Campaign is that the messages are fun, upbeat and
positive. They are also placed where people are
affected. They have not presented it as an earnest
public health campaign but instead it is marketed
“like a coke ad”.
In addition to the positive messages that are presented across Christchurch to inspire hope, they
have also created “short bursts of all right”. These short video clips are present on social media
and you tube and are events/ stunts that catch the viewers’ attention instantly. The message is to
encourage people to think about how they are feeling but in a warm, empathic and gentle way.
The videos are funny, uplifting and inspiring.
Blueprint, Wellington
Blueprint have developed a one day workshop called MH101 which is aimed at giving people confidence to recognise,
relate and respond to people experiencing mental ill health. It focusses on the wellbeing of people and communities.
This resource can be used with employers, communities, families and services such as housing or welfare to give an
understanding of mental health and the importance of managing well being. As the training is co-facilitated by a person
with lived experience, it is successful in achieving that most important aspect of the “power of contact” when educating
people
“We educate people from a service user’s point of view, we challenge people within the training… A reason a
lot of clinicians don’t understand recovery is because no-one’s ever explained it to them and when you go to
medical school, you don’t get recovery training – it’s all D.S.M. and counselling” Sonja Goldsack, Blueprint
MH101 has been running for 5 years. Prior to it’s development, mental health literacy in the Department of Work &
Pensions, housing and A&E was really low as people had no access to training. The results are impressive – at the
start of the training, most people have a confidence level of 15-20% but by the end it is 70-80%. An important
measurement is that when the 3 month follow up takes place, there has been no reduction.
Facilitating MH101 sessions within services, communities and with employers is a really effective way of creating
attitudinal and behavioural change among people who previously had little understanding of mental health. This is
therefore one method that could reduce stigma and discrimination.
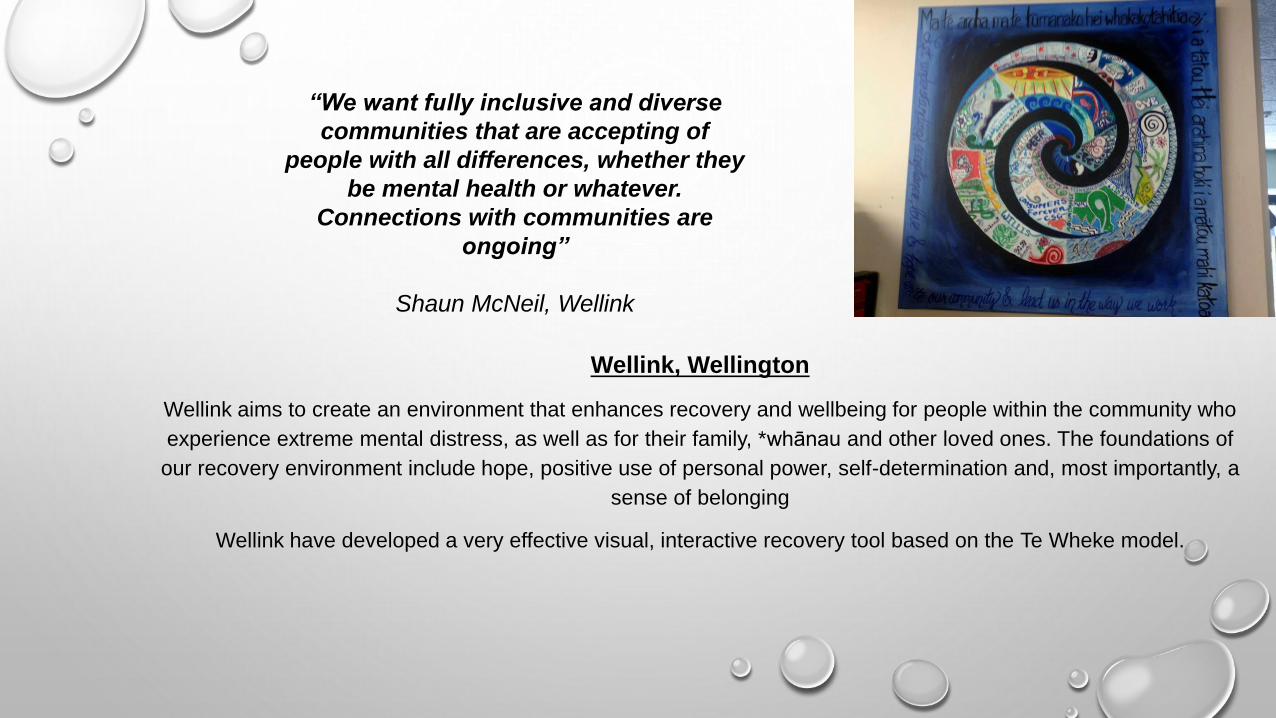
Wellink, Wellington
Wellink aims to create an environment that enhances recovery and wellbeing for people within the community who
experience extreme mental distress, as well as for their family, *whānau and other loved ones. The foundations of
our recovery environment include hope, positive use of personal power, self-determination and, most importantly, a
sense of belonging
Wellink have developed a very effective visual, interactive recovery tool based on the Te Wheke model.
“We want fully inclusive and diverse
communities that are accepting of
people with all differences, whether they
be mental health or whatever.
Connections with communities are
ongoing”
Shaun McNeil, Wellink
Peerzone, Wellington
Peerzone was created by Mary O’Hagan and Sara McCook Weir who have developed eighteen
workshops for people to explore their recovery and wellbeing in a fun, safe, peer group setting.
They currently run Peerzone programmes in New Zealand and Australia. This service offers an
intentional practice tool for peer workers who can facilitate PeerZone as part of their work.
In her paper “Peer Support in Mental Health and Addictions: A background paper” (2011), Mary
O’Hagan reinforces that the two key values most unique to peer support are “reciprocity” and
“experiential knowledge”. She refers to some of the oldest examples of peer support taking
place in the indigenous traditions such as Maori healing rituals and Aboriginal sharing circles.
However, it is now becoming more recognised with the best known examples being the Alcoholics
Anonymous 12 steps programme, Mary Ellen Copeland’s WRAP and Shery Mead’s Intentional
Peer Support. Within the report, it is cited that “peer respondents said the best type of
agencies to ‘house’ peer support services are small, non-profit, community or peer-driven
with a flat hierarchy and consensus decision making” (O’Hagan et al, 2010)
Kites, Wellington
The Kites service empowers consumers to take part in decision making processes. They offer a fantastic “buddies”
service which is a peer support programme which increases community participation for people who have been in
hospital.
They are also developing Toka Tu which is an evaluative tool for NGO’s (voluntary sector organisations) providing peer
support. Tōka Tu is about understanding what resources and support peer support providers need to evaluate their
effectiveness and so evidence their value
Kites are Like Minds Like Mine providers. They facilitate local, targeted training and education in order to reduce stigma
and discrimination associated with mental distress.
Toka Tu is the name chosen for this project, and comes from the whakatauki:
“Ahakoa akina a tai, akina a hau, he toka tu toka ahuru tatou”
“Although the tides and winds may come crashing down on us, like a rock we stand resilient and
comfortable in the face of adversity”
Conclusion
Referring back to the 3 ways of challenging discrimination according to Case Consultancy’s Power of
Contact, we can break the priorities down into the categories of education, contact and protest.
Education—replacing myths about mental distress with correct information
How can we do this?
• We should develop local, targeted educational programmes like MH101 which will provide
communities, employers and services with correct information and will challenge discriminatory
attitudes. These should not be one off sessions but should be part of a programme of delivery in order
to build relationships. The programme should be facilitated by people with lived experience.
• We should work with the media to include positive recovery stories in their publications in order to
counter balance the negative stereotyping tabloid stories that often link mental ill health to criminality.
We should consider introducing local stigma-watch groups to challenge this issue as they have done
in New Zealand.
Contact—challenging discriminatory attitudes and behaviour through direct interactions with people
who experience mental distress
How can we do this?
• We should continue to grow a peer work force which is independent, trained, supported and
working within a structured, intentional model (such as IPS) and with a values framework. A more
holistic model specific to Scottish culture should be developed but drawing on the importance of
spirituality, culture and physical wellbeing as with the Maori and Pacific models (Appendix 1)
• We should introduce the posts of “Advisors with Experience” within each local authority area who
can advise and guide health boards and clinicians on best practice. This will encourage
practitioners to be recovery focussed and consider their use of discriminatory language.
Protest—actions which suppress discriminatory attitudes and behaviours towards people who
experience mental distress.
How can we do this?
• We should have local, targeted anti-stigma campaigns which are based in grassroots services.
This will allow the work in each service to be tailored to the identified needs of each geographical
area. This has been effective in New Zealand who have accepted that the needs of one area in the
country may vary greatly from the needs of another due to cultural diversity, population, rurality
and attitudes.
• We should be discouraging the use of negative, deficit based language which reinforces
discrimination by creating distance between people who are perceived as “well” and people
perceived as “ill”. This is particularly relevant to the health sector. The challenges of emotional
distress are experienced by not 1 in 4 but 1 in 1. Everyone at some point in their life will
understand what it feels like to be struggle to the point that they are not sure how to cope. That is a
natural human response to the challenges of life, a “human experience”. By talking about the
spectrum of emotional wellbeing to emotional distress, we can make the subject less taboo and
people are likely to ask for help sooner and therefore less likely to reach crisis. It will also help
address the issue of self-stigma.
“Madness can cause terror, confusion and despair. But so can grief or dying in
pain for a just cause; so can the path towards spiritual enlightenment or being
falsely accused. The difference between these states and madness is that society
legitimises them and allows for the possibility of growth or recovery”
(Mary O’Hagan, Peerzone).
References:
Well? What do you think? (2008) The Fourth National Scottish Survey of Public Attitudes to Mental
Wellbeing and Mental Health Problems, Davidson et al, 2009. www.scotland.gov.uk
Perkins, R & Repper, J (2013) Prejudice, discrimination and social exclusion: reducing the barriers to recovery for people diagnosed with mental health problems in the UK. Neuropsychiatry, p377-384.
Consultation on the involvement of people with a mental health problem in See Me and Challenging Stigma, HUG, 2013
Policy Into Practice, National Mental Health Development Unit, Public attitudes: annual national survey pf attitudes to mental health in England.
TNS (UK) for CSIP, 2008, Attitudes to Mental Illness research report, London Dept of Health. The Mental Health Strategy for Scotland 2012—15 Opening doors, Kites (2006)
O’Hagan, M (2011) Peer Support in mental health and addictions. Like Minds Like Mine Best Practice Guidelines: For delivering education and training to counter
stigma and discrimination associated with mental distress. Kites, 2012
Like Minds Like Mine National Plan 2007-2013
“Stigma: Marked by Society?” HUG DVD
The Power of Contact, Case Consulting Ltd, 2005
Corrigan (2011) Best Practices: Strategic Stigma Change: Five Principles for Social Marketing Campaigns to Reduce Stigma.”
Huxley, P. (1993) Location and stigma: a survey of community attitudes to mental illness: enlightenment and stigma. Journal of Mental Health UK, 2, 73–80.
Peterson et al (2009) Stepping out of the shadows: Insights into self-stigma and madness, CASE Consulting Ltd
Repper, J and Perkins, R (2003) Social Inclusion and Recovery: A Model for Mental Health Practice, Bailliere Tindall
Chamberlin, J (1988) On our own, MIND
Kirwen, J (2010) All Blacks Don’t Cry: A story of hope, Penguin
Woodhouse A & Vincent A (2006) Development of Peer Specialist Roles: A literature scoping exercise: SRN & Scottish Development Centre for Mental Health.

Media coverage following my fellowship
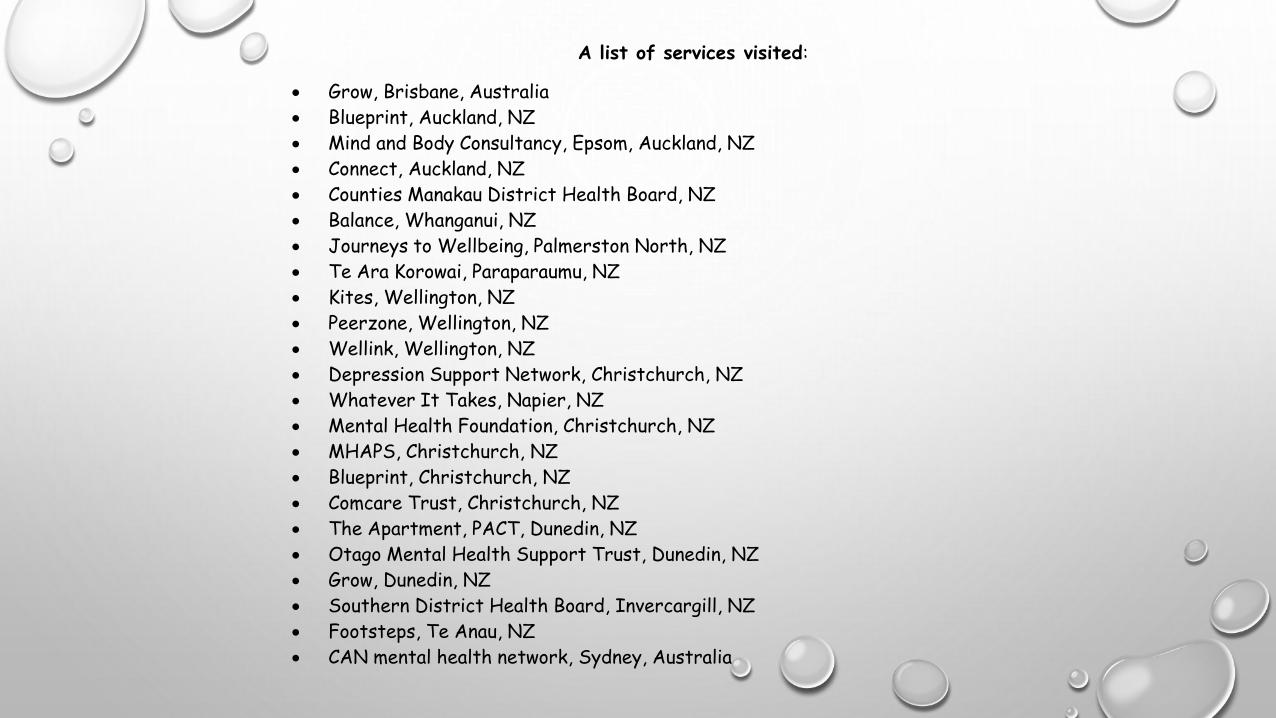
A list of services visited:
Grow, Brisbane, Australia
Blueprint, Auckland, NZ
Mind and Body Consultancy, Epsom, Auckland, NZ
Connect, Auckland, NZ
Counties Manakau District Health Board, NZ
Balance, Whanganui, NZ
Journeys to Wellbeing, Palmerston North, NZ
Te Ara Korowai, Paraparaumu, NZ
Kites, Wellington, NZ
Peerzone, Wellington, NZ
Wellink, Wellington, NZ
Depression Support Network, Christchurch, NZ
Whatever It Takes, Napier, NZ
Mental Health Foundation, Christchurch, NZ
MHAPS, Christchurch, NZ
Blueprint, Christchurch, NZ
Comcare Trust, Christchurch, NZ
The Apartment, PACT, Dunedin, NZ
Otago Mental Health Support Trust, Dunedin, NZ
Grow, Dunedin, NZ
Southern District Health Board, Invercargill, NZ
Footsteps, Te Anau, NZ
CAN mental health network, Sydney, Australia