Embed Size (px)
Citation preview

Communication Decisions and Services
Online Presentation forDeaf Education - Parent InfantMichigan State UniversityMarilyn Sass-Lehrer, Ph.D.Gallaudet University

Goals• What Decisions?
– Identify the decisions families face; Understand the challenges• Roles and Responsibilities
– Understand the professional’s role using “Informed Choice”– Understand how child and family characteristics influence decisions
• ASL and English Bilingual Approach– Describe what it is– Identify features of an Effective Program– Identify FAQs about a Bilingual Approach
• Information and Resources– Identify strategies for promoting decision making – Identify the “evidence base” and resources

Decisions, Decisions, Decisions

Decision Making: A Difficult Process
• Perceived Urgency • Strong Opinions • Professional Bias • Not all Options
Presented• Resources Not Available• Insufficient Information

Misinformation– All children with hearing loss should sign
– If children sign then they won’t talk– Children who are deaf cannot learn to talk
– You have to choose signing or talking– Depends on the extent of the hearing loss
– All children should try speech first– ASL is not a “real” language
– Children who speak don’t need signs– Children with cochlear implants should not
sign

Questions to Consider:
• What is bias? • Should professionals be “neutral”?• What does informed choice mean?• Can/Should families make decisions?• What do families need to make decisions?• Do all families want to decide for themselves?• How can professionals be most helpful?

What is Bias?• A bias is a prejudice in a general or specific sense, usually in
the sense for having a preference to one particular point of view or ideological perspective. However, one is generally only said to be biased if one's powers of judgment are influenced by the biases one holds, to the extent that one's views could not be taken as being neutral or objective, but instead as subjective.
• wikipedia.org/wiki/Bias

In the Words of the14th Dalai Lama
A biased mind never sees the complete picture, and any action that results will not be in tune with reality…I often say that while one can adhere to the principle of “one truth, one religion” at the level of one’s personal faith, we should embrace at the same time the principle of “many truths, many religions” in the context of wider society. (The Washington Post, Oct. 21, 2007).

What is the Evidence?

Is one Technology, Communication Approach, or Program More Effective
than Another? • Research Methodology Difficulties:
– Quality and quantity of studies; – Size of samples, – Generalizability; – Diversity of population; – Lack of long term outcomes; – Lack of studies with children who were identified early

Younger is better for ease in typical progression of spoken language development
No age limit for “some” benefit (older children, teens, senior citizens)
Children with implants have diverse spoken language outcomes related to a variety of factors.
Children with additional special needs can benefit
Importance of early language in any modality for improved spoken language outcomes with implant
What is the research suggesting on CI?
Cochlear Implant Education Center, Gallaudet University

What is the Research Suggesting about Communication Approaches?• No evidence that one communication approach is best for all• Language growth is the critical measure of effectiveness• Services must support Communication Approach • Exposure to dual communication modes does not impede
progress across developmental domains• Individual child characteristics and overall development
inform decisions • Multi-sensory communication options should be based on
individual characteristics and environmental conditions• Bilingualism (ASL and English) does not impede language
growth and may provide a supportive benefit to both languages

What is the research suggesting regarding Programming?• Programs should be comprehensive• Family-Centered• Relationship-Based• Emphasizing Family Involvement/Parent-Child
Communication • How much, when, where has little impact on outcomes
– hours per week – public vs private – home vs center
• Evidence suggests that “specialists” make a difference

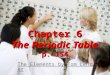
FullyVisual
Communicator
MostlyAuditory
Communicator
MostlyVisual
Communicator
FullyAuditory
Communicator
VV VVAA VAVA AAvv AA
Receptive Communication Continuum
Continuum concept: Bettie Waddy-Smith
Laurent Clerc National Deaf Education Center

Receptive Communication• V Depends on visual information ASL/Signs
• VA Depends on ASL/signs; obtains some benefit from auditory information
• VA Equally depends on and able to use ASL/signs and auditory information via Spoken English
• Av Depends on Spoken English, sometimes needs Sign to clarify Spoken English
• A Depends on auditory information via Spoken English

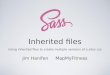
FullySign
Communicator
MostlyOral
Communicator
MostlySign
Communicator
FullyOral
Communicator
SS SSOO SOSO OOss OO
Expressive Communication Continuum
Continuum concept: Bettie Waddy-Smith
Laurent Clerc National Deaf Education Center

Expressive Communication
• S Uses Signs/ASL Only
• So Uses Signs/ASL; some oral communication
• SO Equally able to use sign and oral communication
• Os Uses oral communication; signs for clarification
• O Uses oral communication only

Where a child fits on the continuum depends on the coming together of many impacting factors
(and may change over time)
Cochlear Implant Education Center, Gallaudet University

ASL English Bilingual Approach
• Philosophy:– Deaf and hard of hearing children should acquire,
learn and use two languages (their native sign language and the spoken language(s) of their country)
• Goal:– Children to become academically and
linguistically competent in both ASL and English

Principles• Based on principles of 2nd language acquisition• Supports language and literacy development as well
as cognitive and social development• “Best of both worlds”• Language acquired through meaningful interactions
with fluent users of the languages• ASL is foundation (and/or bridge) to English• Both languages continue to develop

Acquisition
• Watching/Attending• Signing• Fingerspelling
• Fingerreading• Fingerspelling• Reading• Writing/Typing• Lipreading• Speaking & Listening

Educational Implications• ASL and English are languages of instruction and interaction• Children have full access to both languages• Visually rich environment• Which language? Codeswitching
– Rules for when and where to use which language– Communication and Language Plan
• Bilingual Approach – ASL is dominant language with early exposure to English
• English as 2nd Language – ASL first – then English

ASL Programs for Families
• Sign Language Programs – Needs/Interests of Parents– Times, Places Convenient
• Visual Communication Strategies (Mohay, 2000)
• FAQs (See ASDC website)

Informed Choice and Information– Comprehensive, meaningful, relevant, un-biased– Accurate, up to date, evidence-based– Evaluative information is essential (risks and
benefits)– Convey unpredictability or range of outcomes– Information should promote involvement– Promote knowledge and understanding
• Young, Carr, Hunt, Skipp, Tattersall, 2006

Assessment-Based Process• F.A.M.I.L.Y. Assessment
Approach – Auditory Skills
– Language and Communication Skills
– Play Skills– Motor Skills
– Family Needs• Stredler-Brown (2003). • www.csdb.org/chip/build
blocks.html

What Professionals Should Tell Families
• Communication is not always “either/or”• Decisions take time and may change over time• No evidence that signs impede speech• Evidence that signs facilitate language acquisition• Better Language means better speech • Focus must be language access and use – not
form• Language delays are difficult to overcome

Language is the “Holy Grail”

High Expectations: Benchmarks
• EI by 6 months• Maintain language
commensurate with hearing peers
• One year’s growth in one year time
Adapted from Stredler-Brown, 2005

How Families Make Decisions• Families use a variety of strategies to gain
information • Families give a lot of thought to decisions• Decisions made are frequently changed• Level of hearing loss influences approach selected• Deaf/HH adults and families influence decisions• Families want knoweldgable professionals• Perceptions of what professionals should do varies
• Wainscott & Sass-Lehrer (In preparation)

Decision Making Model • Professional Decision
– Professional is responsible for making decisions for child• Guided Decision
– Professional guides and directs families to the “right” decisions
• Collaborative Decision– Professionals and family are partners in making decisions
• Informed Decision– Families have the information they need to make the right
decisions Wainscott, In Preparation

What Families Want: Advice for Professionals
• Comprehensive, accurate, up to date, evidence-based Information
• Honesty, Patience• Open-Minded Flexible• Cultural Sensitivity• Resources (Families/Deaf-HH
Adults)• Monitoring Progress • Support Families’ decisions
Meadow-Orlans, Mertens& Sass-Lehrer, 2003; Wainscott, Croyle & Sass-Lehrer, 2006; Young, et al.; 2006

Additional ReferencesMcLaughlin, L., Small, A., Spink-Mitchell, C. Cripps, J. (2004). A Parent Guidebook: ASL and Early Literacy. Mississaugua, Ontrario: Ontario Society for the Deaf.
Meadow-Orlans, K.P., Mertens, D., Sass-Lehrer, M. (2003). Parents and their deaf children: The early years. Washington, DC: Gallaudet University Press.
Schwartz, S. (2007) Second Ed. Choices in Deafness. Bethesda, MD: Woodbine.
Young, A., Carr, G., Hunt, R., McCracken, W., Skipp, A., Tattersall, H. Informed choice and deaf children: Underpinnings, concepts and enduring challenges. Journal of Deaf Studies and Deaf Education 2006: 11: 322-336

So…..
• What did you learn or find interesting in this session?
• How could you connect something you learned with your work with children and families