Embed Size (px)
Citation preview

COMMONLY ENCOUNTERED SHOULDER PATHOLOGIES IN ULTRASOUND
Teena AndersonStudent ID 09734007

BURSITIS & IMPINGEMENT
A bursa of is a small pocket of fluid surrounding muscles or tendons. Fluid within the bursa is synovium.
The subacromial-subdeltoid bursa is the largest bursa within the shoulder.
The role of the bursa is to reduce friction and allow smooth and free movement of the rotator cuff.
Bursitis can be caused by repetitive trauma to the bursa causing an increased production in collagen and synovium. The increased size of the bursa increases the friction which increases the pain (Ishii et al, 1997).
Ultrasound appearances can vary from a thickened hyperechoic region (which is the thickened walls) or a hypoechoic stripe within the bursal walls (which is the increase in synovial fluid).
A bursa with an increase in synovial fluid is indicative of a tear (due to communication with the joint), whereas a bursa with oedema is more likely a sign of impingement or bursitis (Rumack et al, 2005).

BURSITIS & IMPINGEMENT Impingement occurs when the rotator cuff tendons become
trapped beneath the acromion during movement.
This best assessed during dynamic scanning of the shoulder with ultrasound.
Impingement is present if during dynamic scanning the bursa or tendons bunch during abduction.
The bursa acts to reduce the friction to the rotator cuff during abduction. Impingement is present when the bursa or tendons are unable to move freely and smoothly during abduction (Ishii et al, 1997).

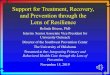
JOINT EFFUSIONS Joint fluid can be found in any of the shoulder
recesses. The most common for site to accumulate in a patient sitting upright is in the biceps tendon sheath.
When large fluid collections are found in the posterior joint recess inflammatory of infective causes should be considered (Rumack et al, 2005). The image to the right depicts a posterior joint recess collection. Aspiration of this collection indicated the cause to be inflammatory.
Effusions can have different ultrasonic appearances dependant on what they consist of. If the effusion is purely synovial fluid the appearance will be anechoic. Haemorrhage or debris within an effusion will produce more of a mixed echogenicity, but it will still be hypoechoic when compared to the surrounding tendons and musculature (Ishii et al, 1997).

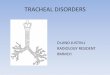
TENDINOPATHY Tendinopathy is a generalized term used for thickening
or changes within a tendon. It is a useful term as it does not imply an acute or chronic issue, rather just a general term of the tendons appearance.
Tendinopathy can be localized, but more often than not it is seen as more generalized (Rumack et al, 2005).
In acute tendinopathy ultrasound may show an increased vascularity. Light probe pressure is important when assessing for colour flow in the tendons.
The images on the left show a normal transverse supraspinatus tendon (top)
and a tendinopathic tendon.
The image on the right shows a normal longitudinal supraspinatus
tendon (top) and three images of the same tendinopathic tendon in its
entire width.

TENDON TEARS Tendon tears are named according to the amount of tendon that is
involved.
Partial Tendon Tear - these tears only involve one surface of the tendon. They are called bursal or articular tears.
Intrasubstance tears - do not form on either of the surfaces, rather they are found within the tendon fibrils.
Full Thickness Tears – involve both surfaces of the tendon (the bursal and articular), but not the entire width of the tendon. A small full thickness tear is <5mm and may not show retraction of the tendon.
Complete and Massive Tears – these have a greater extension than full thickness. Retraction will be seen as there are no intact tendons to hold the tendon in position. Herniation of the deltoid muscle over the retracted tendon may be evident. Further assessment of surrounding tendons is required to asses for extension (Bianchi and Martinoli, 2007).

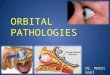
FULL THICKNESS TEAR Complete tear of the tendon fibres from bursal surface to the
articular surface. The complete width of the tendon may still be intact.
The most common site is in the anterior portion of the supraspinatus tendon at the level of the critical area. This often leave the posterior portion intact.
Ultrasound appearances vary dependent on how much joint effusion is present.
There may or may not be tendon fibre retraction, so use of probe pressure and angle is important (Bianchi and Martinoli, 2007).
A massive cuff tear can have several appearances:
When the humeral head is in direct contact with the acromion,
When the deltoid muscle is in direct contact with the humeral head, or
Only a thickened bursa and fat are seen between the deltoid muscle and humeral head (Rumack et al, 2005).
The images to the right are of a full thickness tear of the supraspinatus tendon.

PARTIAL TEAR Partial thickness tears make up ~18% of all rotator
cuff tears (Bianchi and Martinoli, 2007).
They are more common in younger patients.
They most commonly occur at the anterior third of the supraspinatus tendon.
The tears will often have a bursal or articular surface extension.
They can be difficult to visualise. It is important to look for any defects with hypoechoic fluid within them.
An intrasubstance tear does not extend to either the bursal of articular surface. It is quite subtle and will appear with hypoechoic fluid tracking along the tendon fibrils (Bianchi and Martinoli, 2007).
The image on the right is a articular partial thickness tear of the supraspinatus tendon.

CALCIFIC TENDONITIS Refers to the deposit of calcium within the
rotator cuff tendons.
Supraspinatus is the most common site of deposit (80%), then infraspinatus (15%) and subscapularis (5%). It should be noted that they can occur anywhere.
There are four stages: Precalcific;
Calcific
Resorptive; and
Post Calcific.
The example images show a Stage II deposit with posterior shadowing (Bianchi and Martinoli, 2007).

Calcific deposits have three types: Type I – hyperechoic deposit within the tendon with
well defined posterior shadowing.
Type II – A hyperechoic deposit within the tendon which has faint posterior shadowing.
Type III – may appear as hyperechoic deposit within the tendon with no posterior shadowing, or as an undefined hyperechoic/isoechoic structure within the tendon with mobile internal echoes. This is when the internal structure becomes liquefied.
Type I relate to the formative stage of the process.
Type II and III relate to the resorptive phase – where they may be aspirated (Bianchi and Martinoli, 2007).
Ultrasound is very useful in determining the internal structure of the calcific deposit (Rumack et al, 2005).

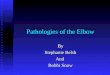
BICEP PATHOLOGY It is important to remember that the bicep tendon
sheath may have a small amount of fluid seen within the proximal section and be normal. This is due to its direct association with the shoulder joint.
Pathology that can be encountered include: Bicipital Tenosynovitis – usually due to impingement.
Bicep Tendon Tear – this results in the Popeye Deformity due to the retraction of the bicep muscle towards the elbow. This can be due to chronic overuse or an acute injury.
Subluxation/Dislocation – usually occurs in combination with a rotator cuff tear, compromising the structures holding the bicep within its bicipital groove (Crane, 2007).
The top and middle image on the right depict a subluxed bicep tendon. The bottom image shows biceps tenosynovitis.
(Figure 22: Biceps brachii tendon synovitis. Gaitini, 2012)

REFERENCESArend CF. Ultrasound of the Shoulder. Master Medical Books, 2013.
Bianchi S and Martinoli C. 2007. Ultrasound of the Musculoskeletal System. Springer, New York.
Crane, J. 2007. Shoulder:Biceps Tendon Pathology. Faculty of Health Sciences Stellenbosch Hospital. Tygerberg Hospital. http://www.capetownorthopaedic.co.za/shoulder-biceps-tendon-pathology.php
Gaitini D. Shoulder Ultrasonography: Performance and Common Findings. J Clin Imaging Sci 2012;2:38
Ishii H, Brunet JA, Welsh RP, Uhthoff HK (1997). ""Bursal reactions" in rotator cuff tearing, the impingement syndrome, and calcifying tendinitis". J Shoulder Elbow Surg 6 (2): 131–6.
Rumack et al. 2005. Diagnostic Ultrasound. 3rd edition. Elsevier Mosby, St Louis.
Wheeless, Clifford. "Subacromial Bursa". Accessed 5/07/2015.
All images, except one, used in this presentation have been produced by myself or a senior sonographer whilst I was training at Royal Perth Hospital. These images have been desensitised and had all identifying names and medical numbers removed.
The only borrowed imaged has been credited to the source.