Embed Size (px)
Citation preview
Note: Not all wounds are Pressure Ulcers. Only stage Pressure Ulcers!!!
We own all Pressure Ulcers that develop at our facility or that we did not find and document properly upon admission!!!
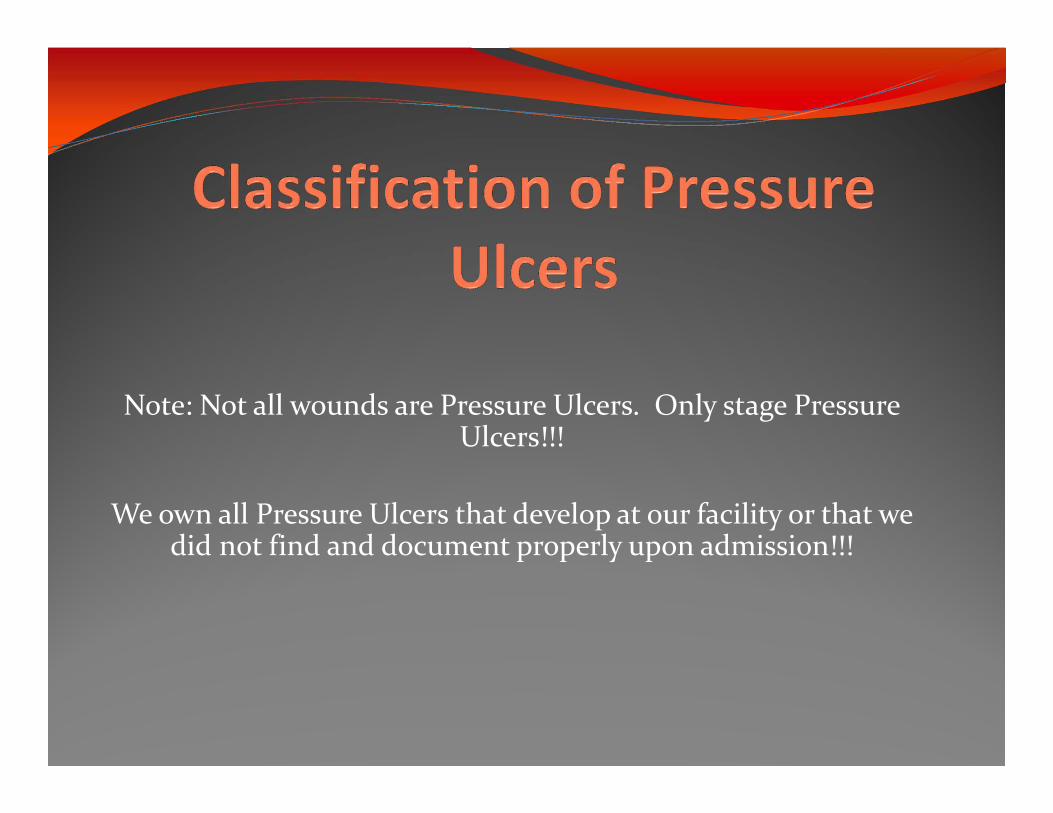
Common Sites for Pressure Ulcers

Wound ClassificationAll wounds are either:
Partial Thickness
Full Thickness
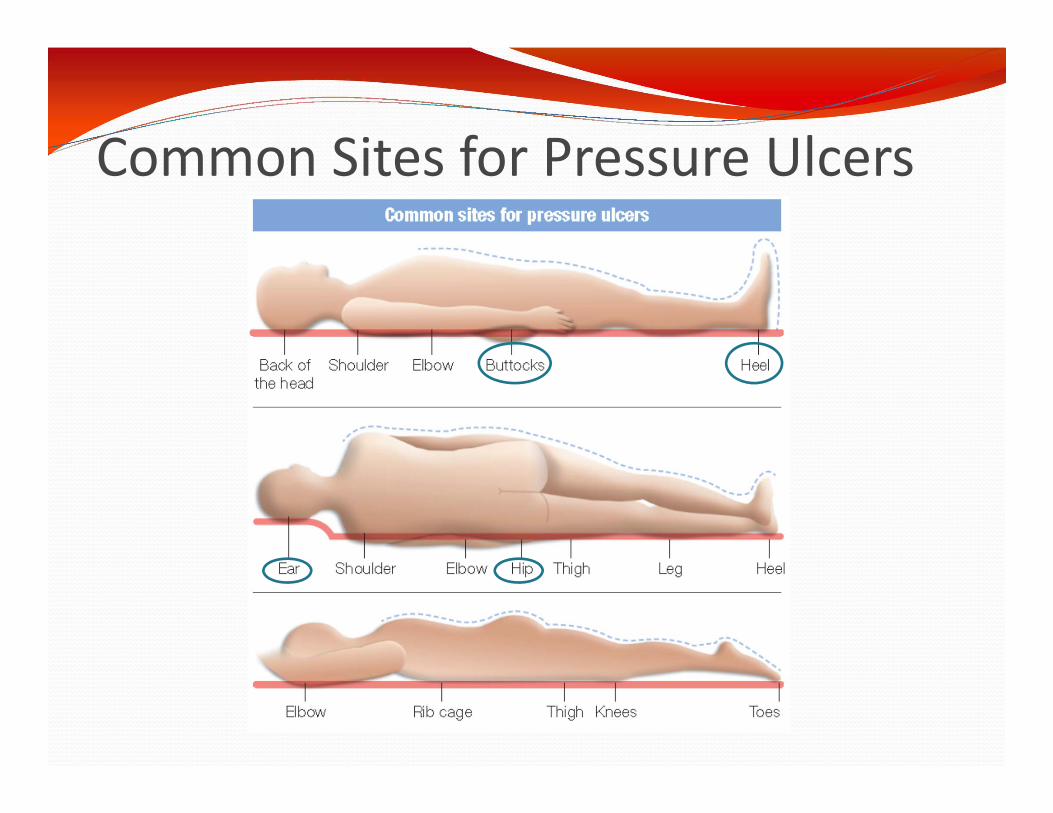
Partial ThicknessDestruction of epidermis and dermis

Partial Thickness
Pink Painful NO Yellow tissue
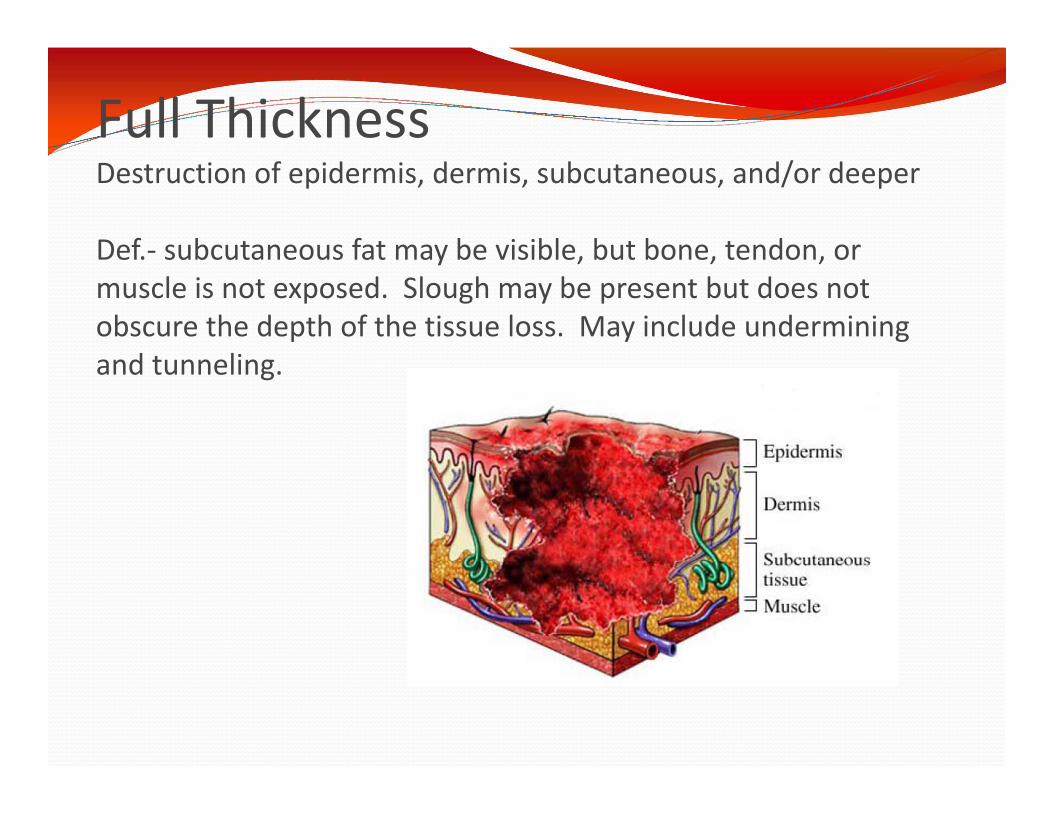
Full ThicknessDestruction of epidermis, dermis, subcutaneous, and/or deeper
Def.‐ subcutaneous fat may be visible, but bone, tendon, or muscle is not exposed. Slough may be present but does not obscure the depth of the tissue loss. May include undermining and tunneling.

Full Thickness
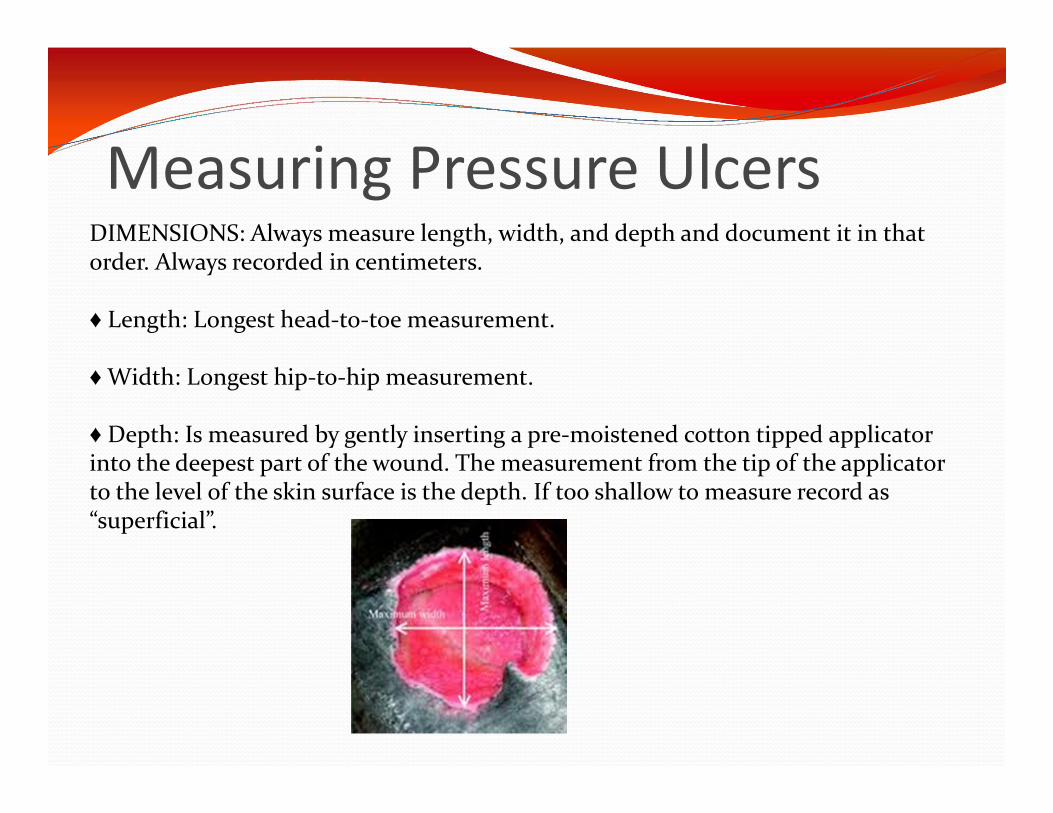
DIMENSIONS: Always measure length, width, and depth and document it in that order. Always recorded in centimeters.
♦ Length: Longest head‐to‐toe measurement.
♦Width: Longest hip‐to‐hip measurement.
♦ Depth: Is measured by gently inserting a pre‐moistened cotton tipped applicator into the deepest part of the wound. The measurement from the tip of the applicator to the level of the skin surface is the depth. If too shallow to measure record as “superficial”.
Measuring Pressure Ulcers
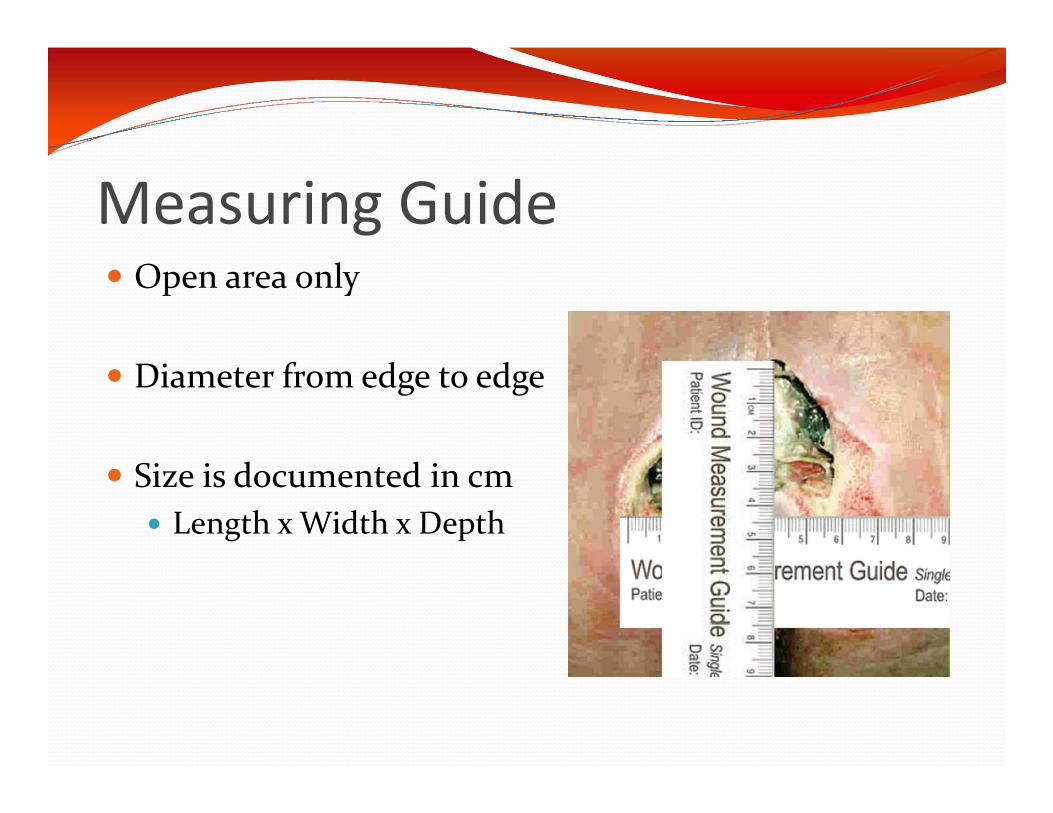
Measuring Guide Open area only
Diameter from edge to edge
Size is documented in cm Length x Width x Depth
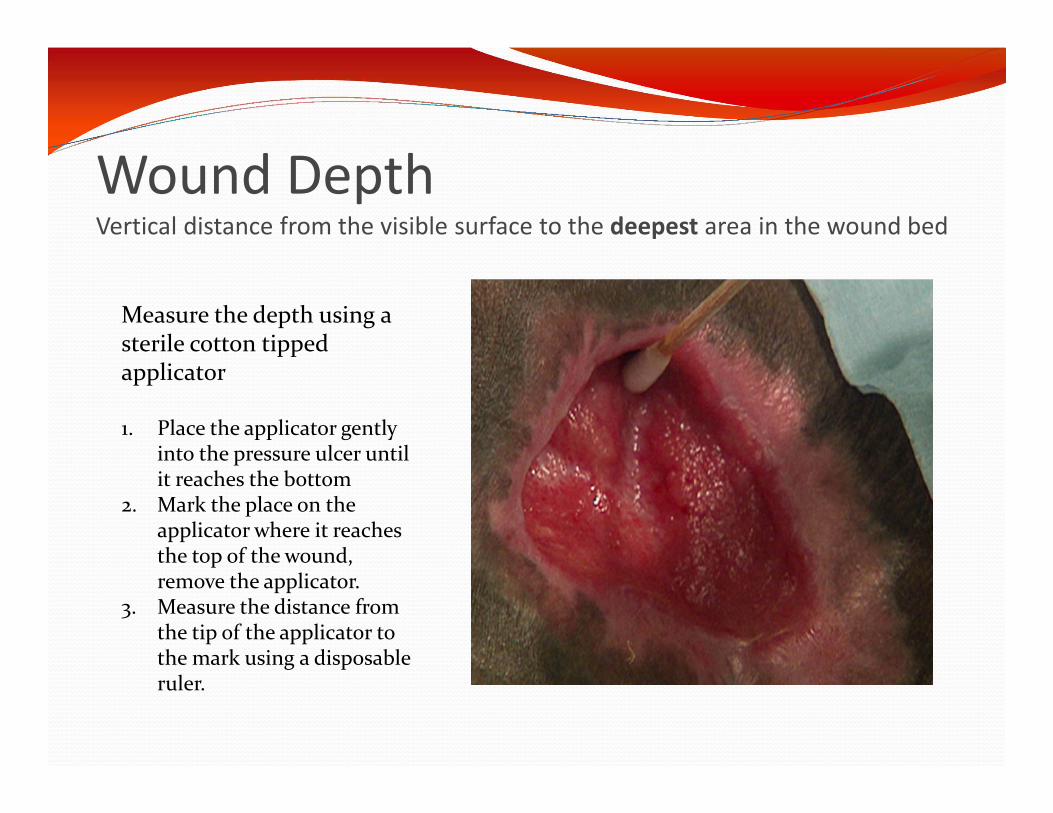
Wound DepthVertical distance from the visible surface to the deepest area in the wound bed
Measure the depth using a sterile cotton tipped applicator
1. Place the applicator gently into the pressure ulcer until it reaches the bottom
2. Mark the place on the applicator where it reaches the top of the wound, remove the applicator.
3. Measure the distance from the tip of the applicator to the mark using a disposable ruler.
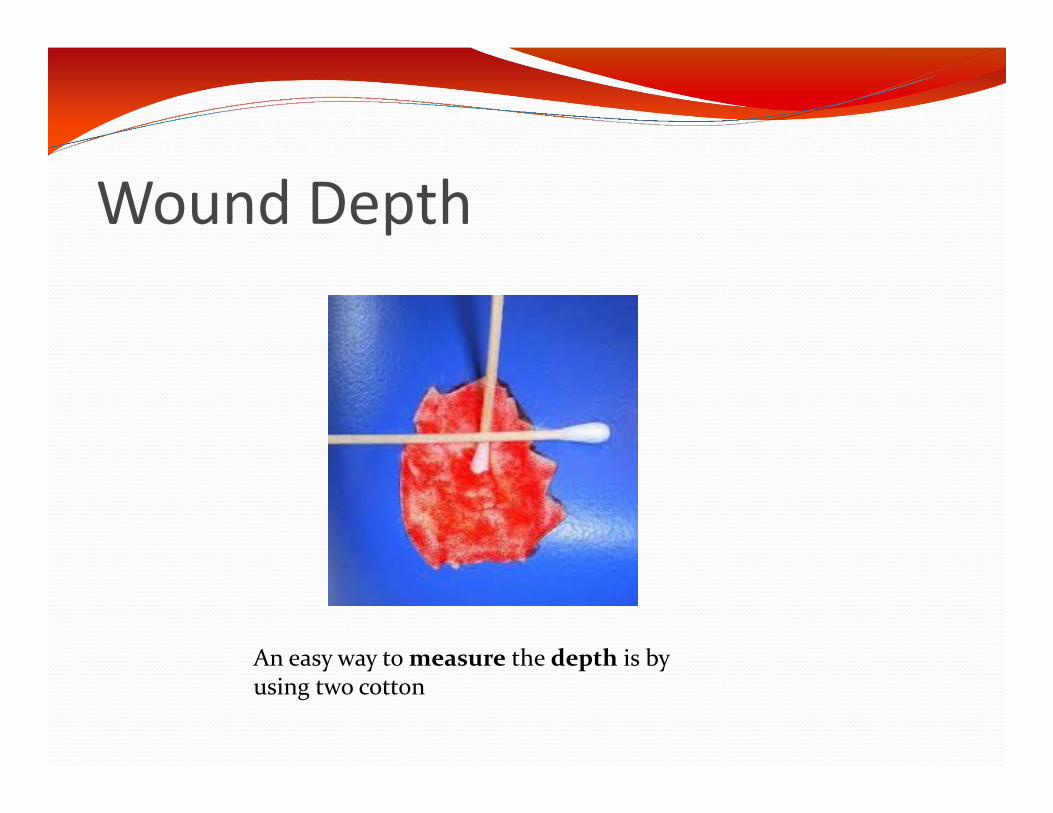
Wound Depth
An easy way to measure the depth is by using two cotton
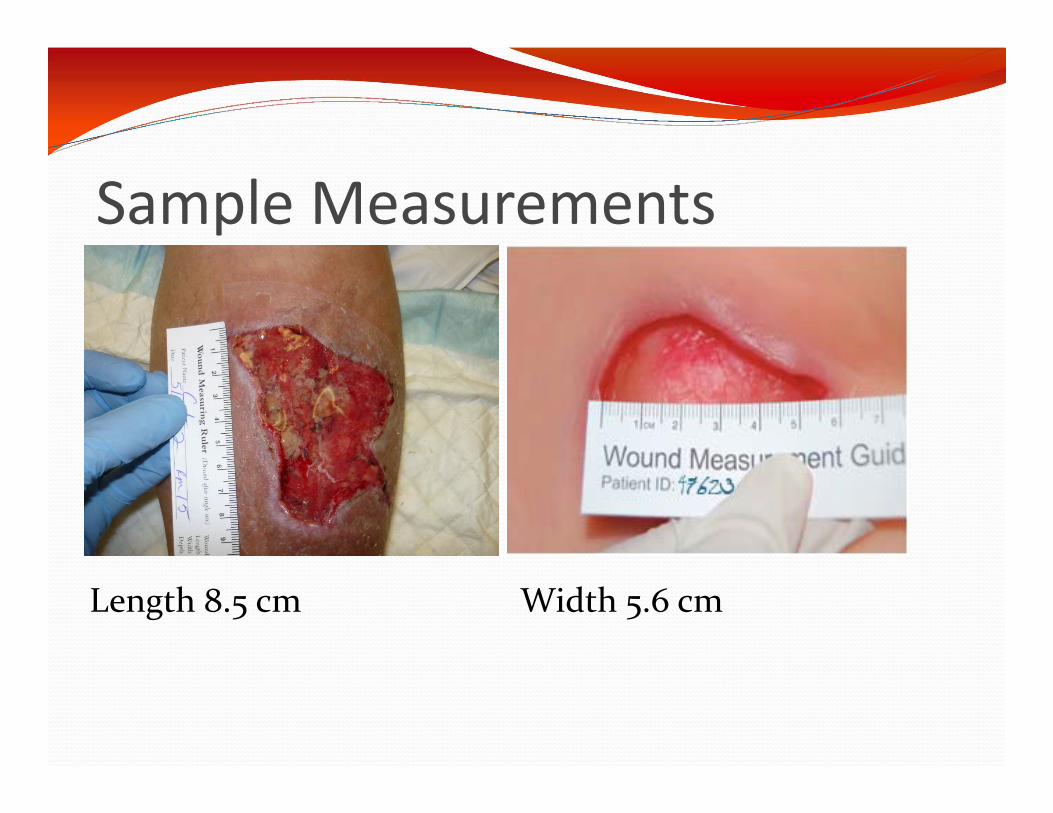
Sample Measurements
Width 5.6 cmLength 8.5 cm
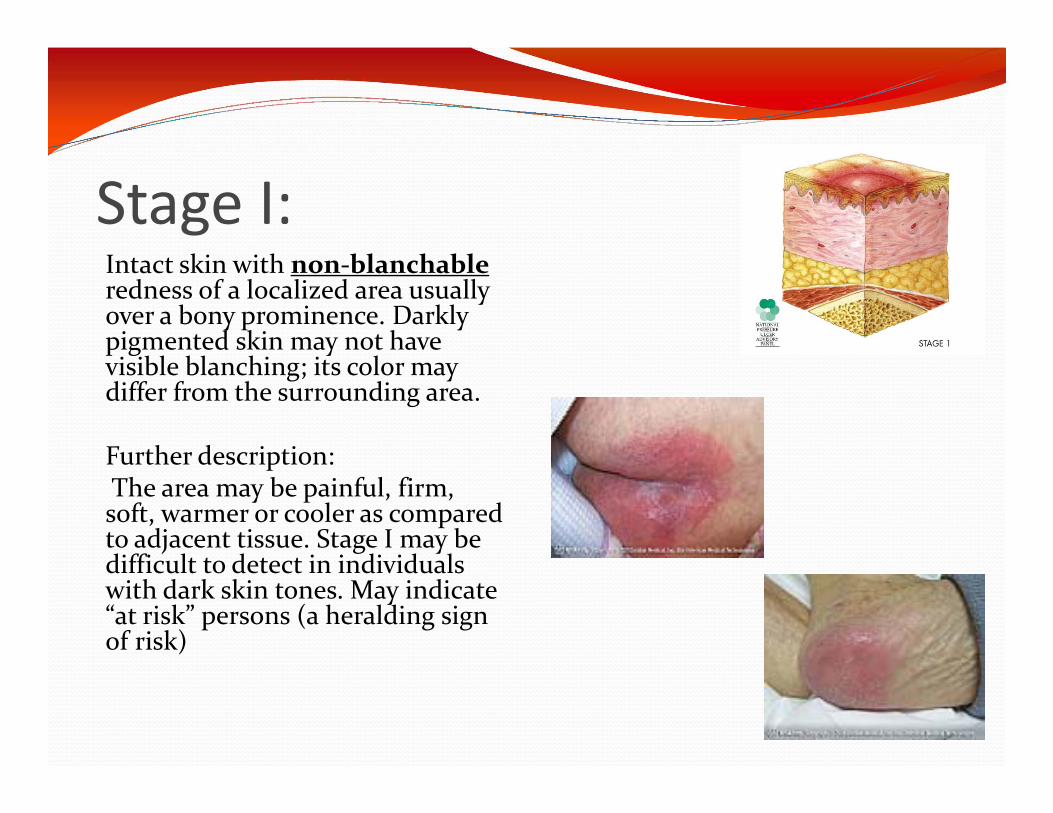
Stage I:Intact skin with non‐blanchableredness of a localized area usually over a bony prominence. Darkly pigmented skin may not have visible blanching; its color may differ from the surrounding area.
Further description:The area may be painful, firm, soft, warmer or cooler as compared to adjacent tissue. Stage I may be difficult to detect in individuals with dark skin tones. May indicate “at risk” persons (a heralding sign of risk)

Stage II:Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed, without slough. May also present as an intact or open/ruptured serum‐filled blister.
Further description:Presents as a shiny or dry shallow ulcer without slough or bruising.* This stage should not be used todescribe skin tears, tape burns, perineal dermatitis, maceration or excoriation.*Bruising indicates suspected deep tissue injury
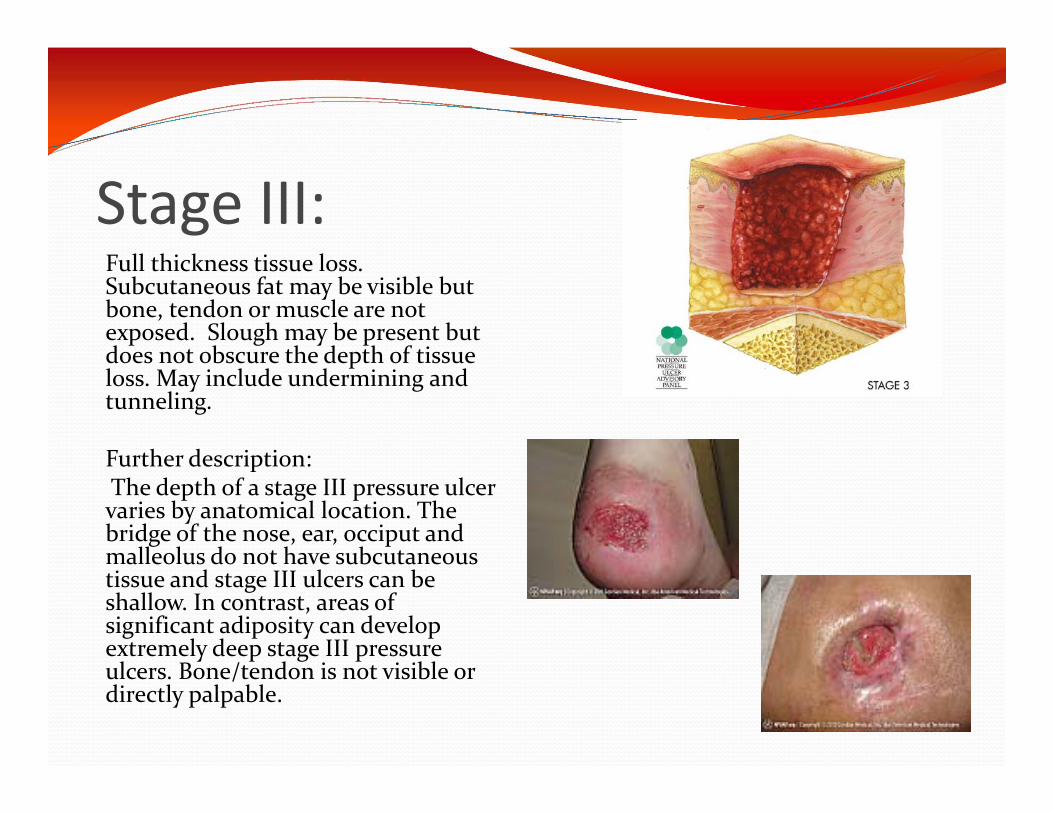
Stage III:Full thickness tissue loss. Subcutaneous fat may be visible but bone, tendon or muscle are not exposed. Slough may be present but does not obscure the depth of tissue loss. May include undermining and tunneling.
Further description:The depth of a stage III pressure ulcer varies by anatomical location. The bridge of the nose, ear, occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow. In contrast, areas of significant adiposity can develop extremely deep stage III pressure ulcers. Bone/tendon is not visible or directly palpable.
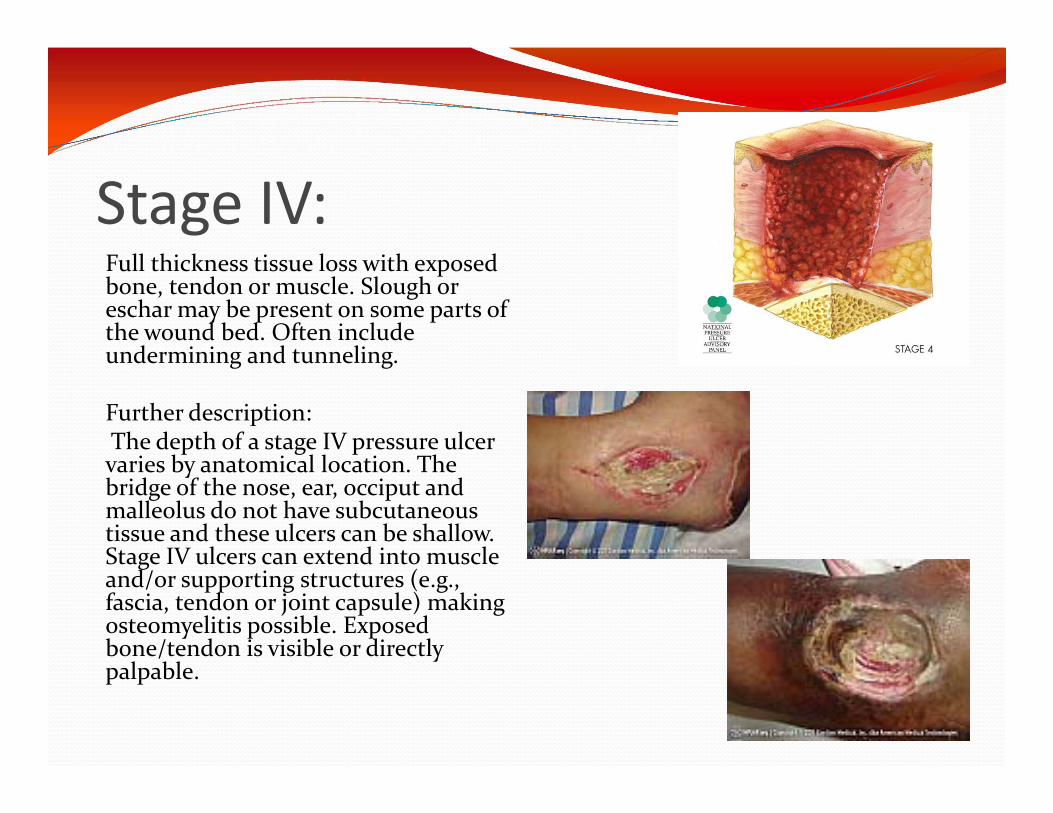
Stage IV:Full thickness tissue loss with exposed bone, tendon or muscle. Slough or eschar may be present on some parts of the wound bed. Often include undermining and tunneling.
Further description:The depth of a stage IV pressure ulcer varies by anatomical location. The bridge of the nose, ear, occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow. Stage IV ulcers can extend into muscle and/or supporting structures (e.g., fascia, tendon or joint capsule) making osteomyelitis possible. Exposed bone/tendon is visible or directly palpable.
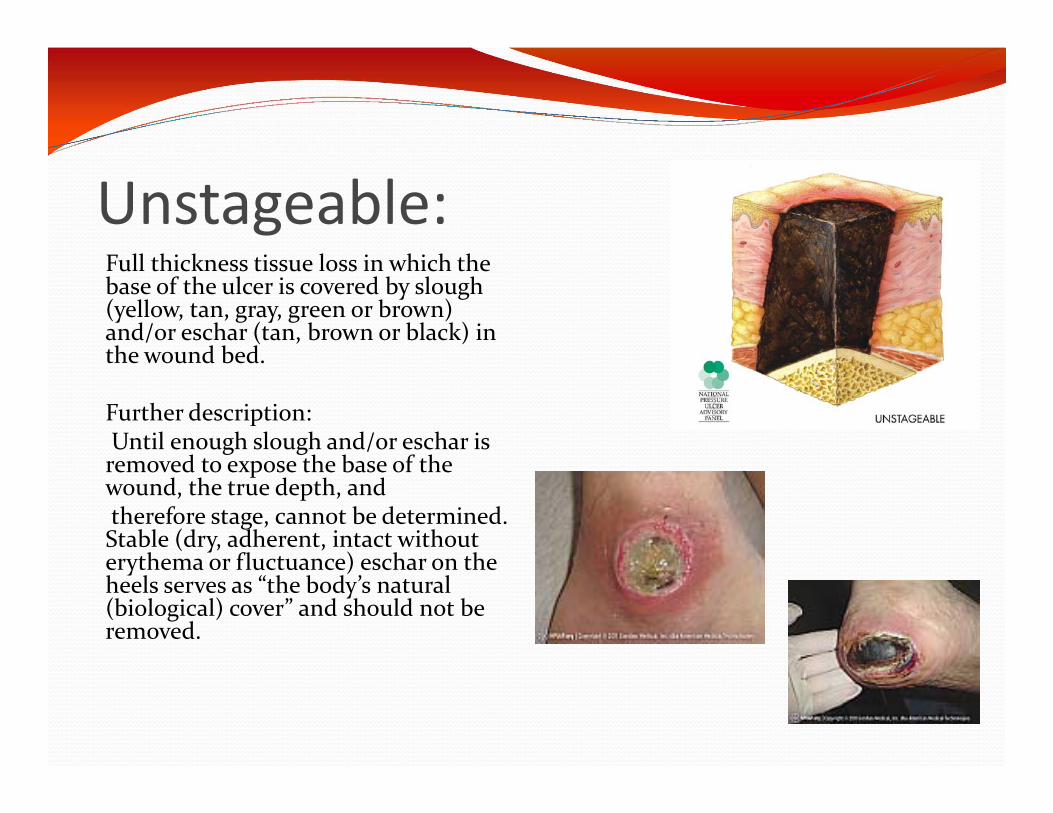
Unstageable:Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow, tan, gray, green or brown) and/or eschar (tan, brown or black) in the wound bed.
Further description:Until enough slough and/or eschar is removed to expose the base of the wound, the true depth, andtherefore stage, cannot be determined. Stable (dry, adherent, intact without erythema or fluctuance) eschar on the heels serves as “the body’s natural (biological) cover” and should not be removed.
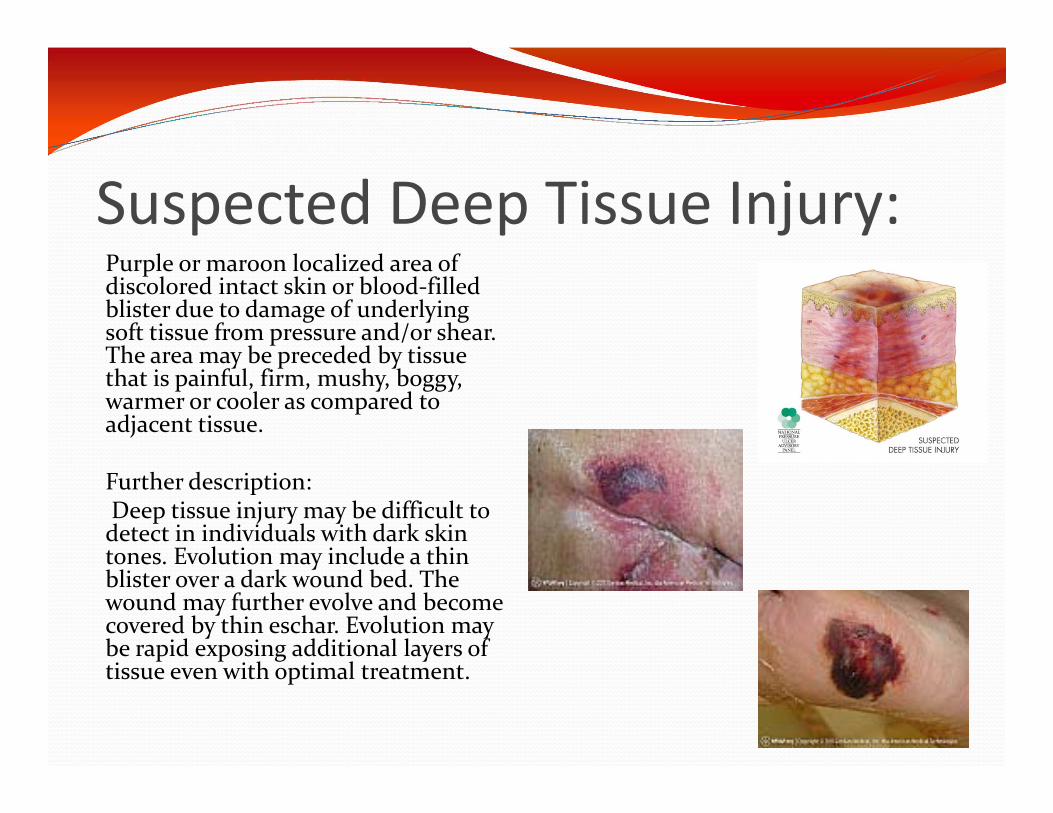
Suspected Deep Tissue Injury:Purple or maroon localized area of discolored intact skin or blood‐filled blister due to damage of underlying soft tissue from pressure and/or shear. The area may be preceded by tissue that is painful, firm, mushy, boggy, warmer or cooler as compared to adjacent tissue.
Further description:Deep tissue injury may be difficult to detect in individuals with dark skin tones. Evolution may include a thin blister over a dark wound bed. The wound may further evolve and become covered by thin eschar. Evolution may be rapid exposing additional layers of tissue even with optimal treatment.
Most SevereTissue Type
Granulation Tissue
Eschar
New skin growing in superficial ulcer
Outer most layer of skin Deep pink to pearly pink, shiny Close the wound
Black, brown, grey, or tan tissue that adheres firmly to the wound bed or edges
Darker, thicker Harder than surrounding tissue
Epithelial Tissue‐
Slough Yellow, green, grey, or white
tissue that adheres to the ulcer bed
Lighter, thin, wet stringy
New tissue that replaces dead tissue
Pink or beefy red with shiny, moist, granular appearance
Grows from base of wound

Slough

Eschar

Epithelial Tissue

Granulation Tissue
Post Test Name:_________________Date:_____________
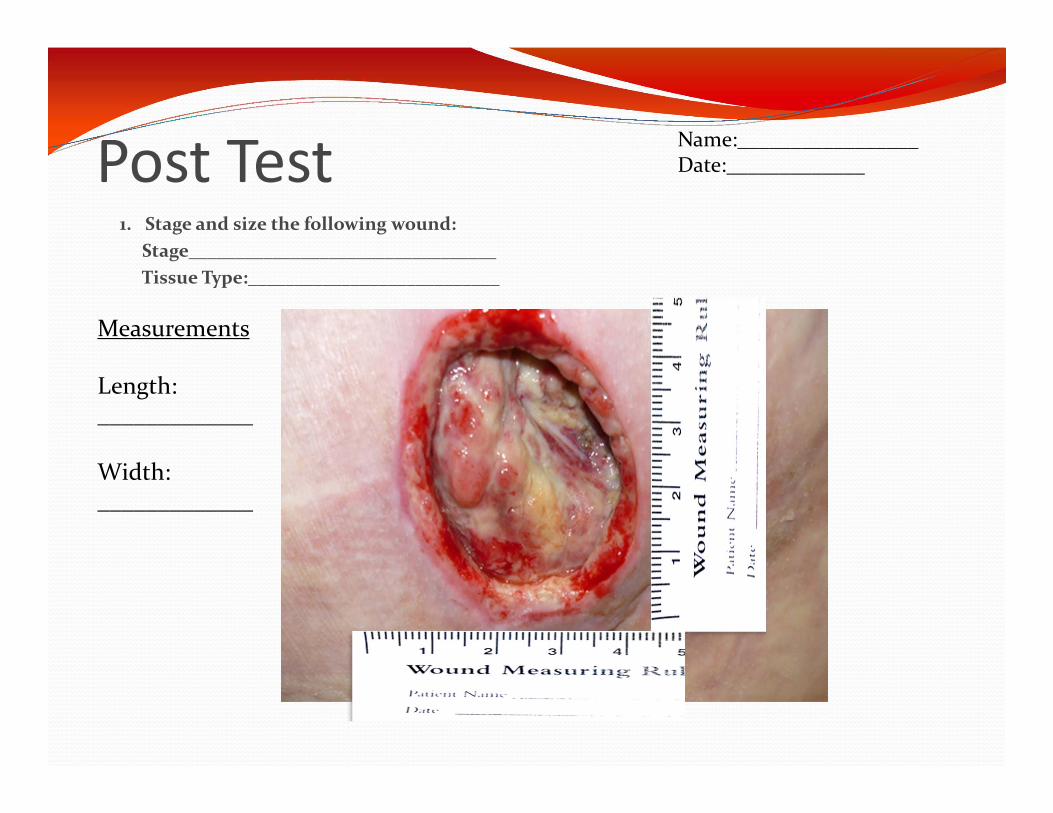
1. Stage and size the following wound:Stage_________________________________Tissue Type:___________________________
Measurements
Length:_____________
Width:_____________
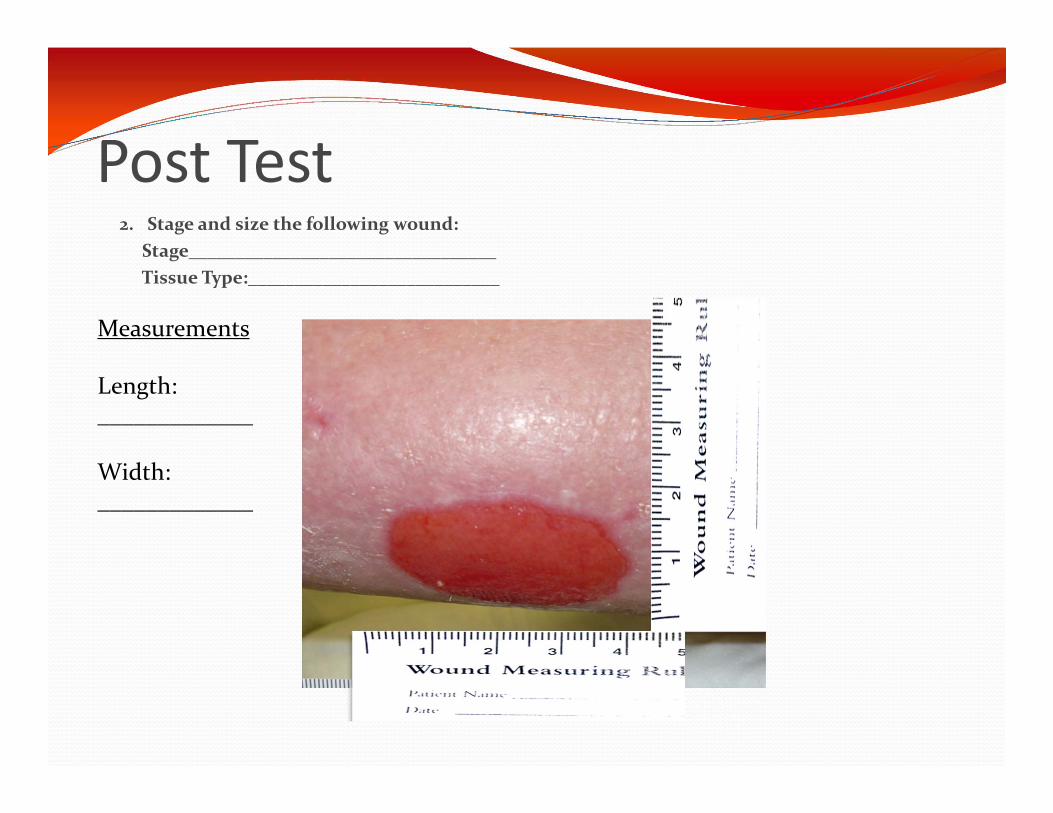
Post Test2. Stage and size the following wound:
Stage_________________________________Tissue Type:___________________________
Measurements
Length:_____________
Width:_____________
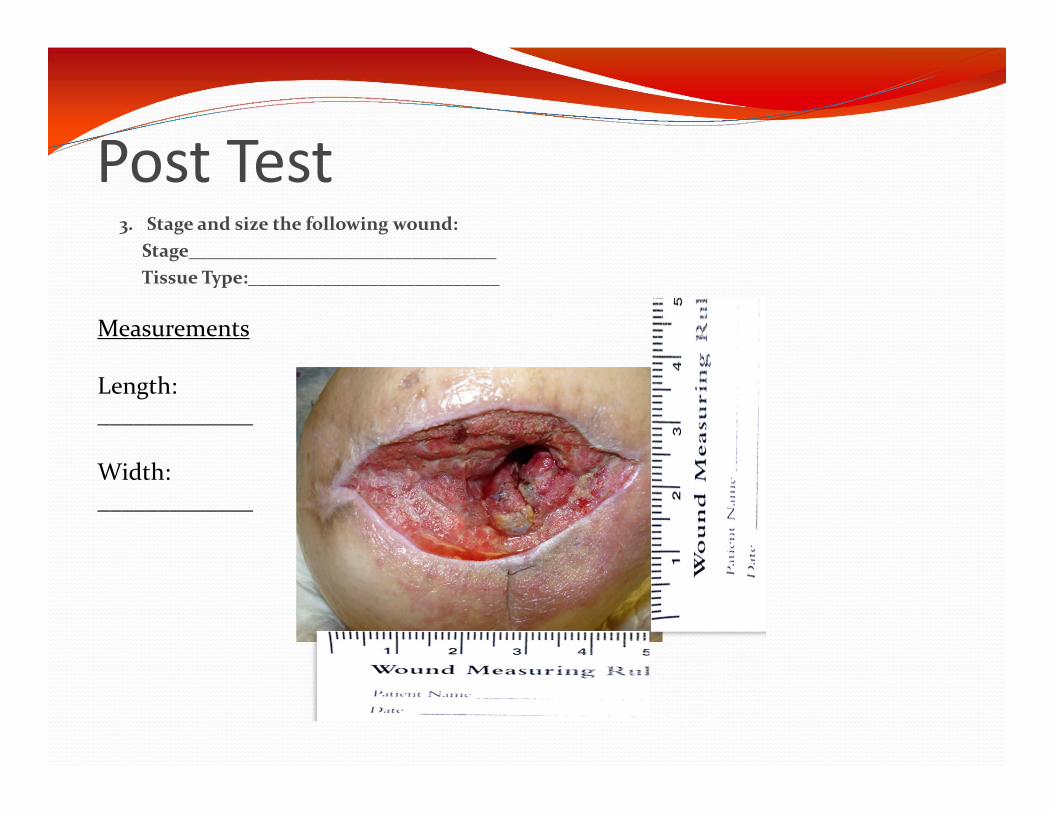
Post Test3. Stage and size the following wound:
Stage_________________________________Tissue Type:___________________________
Measurements
Length:_____________
Width:_____________
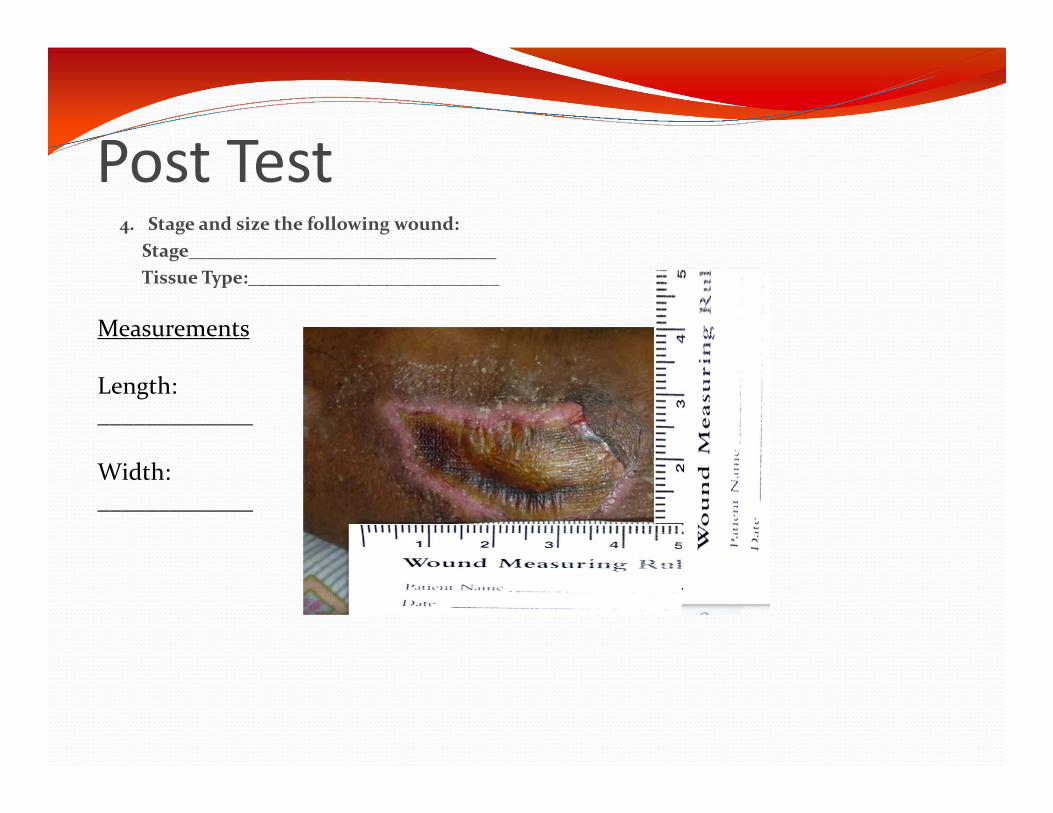
Post Test4. Stage and size the following wound:
Stage_________________________________Tissue Type:___________________________
Measurements
Length:_____________
Width:_____________
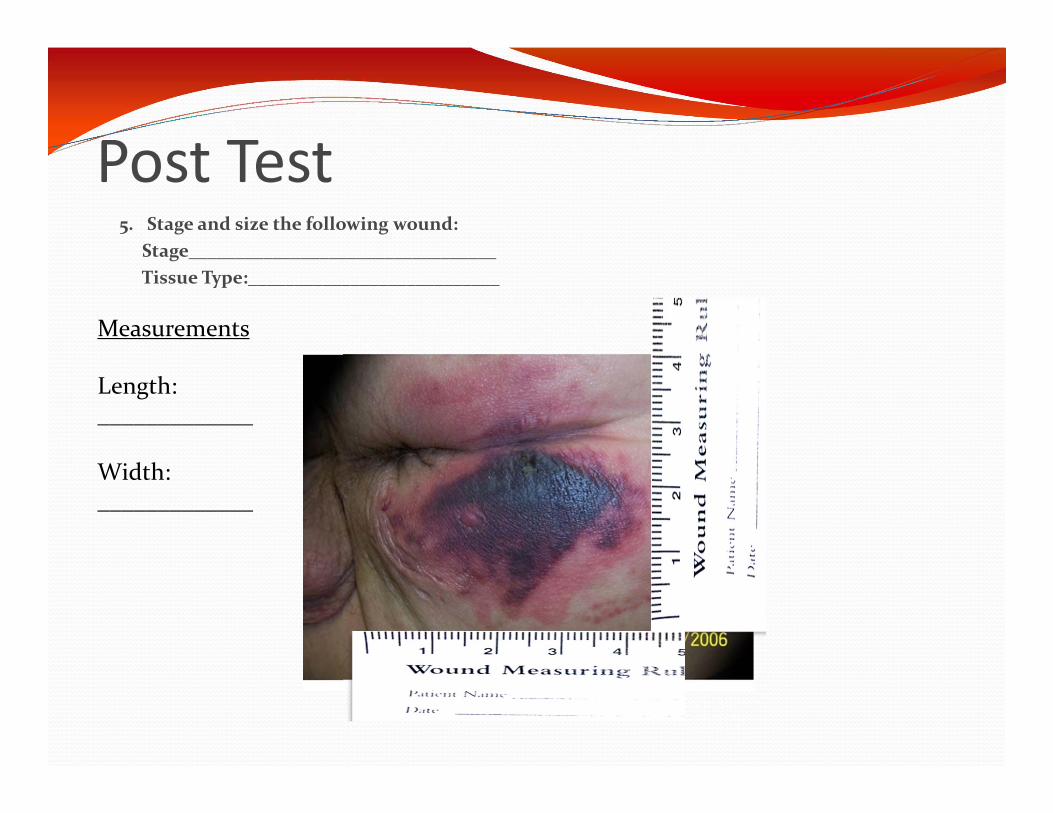
Post Test5. Stage and size the following wound:
Stage_________________________________Tissue Type:___________________________
Measurements
Length:_____________
Width:_____________
Post Test Questions:6. When measuring the depth of a wound, you should use:
A. Disposable Wound Measuring RulerB. Your FingerC. Sterile Q‐tip applicatorD. Your pen after it has been cleansed with alcohol
7. List 4 common areas pressure ulcers occur1.2.3.4.
8. The following is indication of a Stage_______ Pressure Ulcer:Full thickness tissue loss. Subcutaneous fat may be visible but bone, tendon or muscle are not exposed.
Slough may be present but does not obscure the depth of tissue loss. May include undermining and tunneling.
9. The following Tissue Type would be considered ________________________.Black, brown, grey, darker, thicker, harder
10. What is the procedure for measuring the depth of a would?1.2.3.
11. Wounds are always measured in:A. mmB. cmd. Inchesc. It does not matter, just be consistent