Embed Size (px)
Citation preview
Common Bile Duct Exploration --Primary Closure of the Duct with Retrograde Transhepatic Biliary Drainagew
~[sukasa TSUNODA*, Toshiomi KUSANO**, Masato FURUKAWA**, Toshifumi ETO* and Ryoichi TSUCHIYA*
ABSTRACT: A new method of retrograde transhepatic biliary drainage (RTBD) using an RTBD tube with primary closure o f the common duct was investigated with special reference to the usefulness and feasibility of this procedure. At operation, an atraumatic vinyl chloride tube was inserted from a choledochotomy incision and in most cases advanced via the left hepatic duct to the liver surface, which was then penetrated. After the choledochotomy incision had been primarily sutured, the RTBD tube was fixed to the abdominal wall. This drainage method was applied to 71 patients as an alternative to the conventional T-tube drainage and its effect on bile drainage was prominent . The insertion of an RTBD tube did not influence liver function tests and an RTBD tube cholangiography revealed no sever e deformity at the primary closure site of the bile duct. The most common complication was movement of the optimal site for stenting of the bile duct, however, no serious complications were encountered. On average, the RTBD tube was removed on the 16th postoperative day, the mean postoperative stay in hospital being 22 days. These findings suggest the need for a prospective randomized clinical trial to prove the usefulness and feasibility of primary bile duct closure using our drainage method.
KEY WORDS: common duct stones, primary closure of the bile duct, retrograde transhepatic biliary drainage
INTRODUCTION
Most surgeons employ intraductal drainage after exploration of the bile duct, usually in the form of a T-tube, over which the choledochotomy incision is closed. This tube acts mainly as a safety valve to prevent the
*The Second Department of Surgery, Nagasaki University School of Medicine, Nagasaki, Japan, and * *the Department of Surgery, Nagasaki Chuo National Hospital, Nagasaki, Japan
Reprint requests to: Tsukasa Tsunoda, MD, The Second Department of Surgery, Nagasaki University School of Medicine, 7-2, Sakamoto, Nagasaki City 852, Japan
extravasation of bile through the choledo- chotomy incision and also to facilitate post- operative cholangiography. 1
However, early extubation of the T-tube is impossible until an adequate T-tube sinus tract is complete. Moreover, there have been reports of severe complications of T-tube drainage, such as tube dislocation or inade- quate fistulation, resulting in reoperation and prolonged hospitalization. ~
We conducted this study to determine whether or not the method o f retrograde transhepatic biliary drainage (RTBD) using an RTBD tube with primary closure of the duct could serve as an alternative for the conventional T-tube drainage.
JAPANESE JOURNAL OF SURGERY, VOL 21, No. 2 pp. 162-166, 1991
Volume 21 RTBD after bile duct exploration 163 Number 2
PATIENTS AND METHODS
Between April, 1986 and August, 1989, a new drainage method using an RTBD tube was applied to 71 patients requiring choledo- chotomy, accounting for 97.3 per cent of a total 73 patients with common bile duct stones treated during the same period.
There were 32 males and 39 females, with a mean age of 53.5 years, whose ages ranged from 28 to 86 years. The stones were located in both the gallbladder and common bile duct in 51 patients and the common bile duct alone in 20. ~A cholecystectomy was per- formed in all patients apart from 11 who had previously undergone a cholecystectomy. No other surgery was performed.
The RTBD tube used in this study was an atraumatic vinyl chloride tube with an outer diameter of 2.5-4.5 mm (SumitomoBakelite Medical Co., Ltd, Tokyo) (Fig. 1). There was a specific alminium needle at its tip, 15 cm in length and able to be bent to conform with the bile duct through which the tube was inserted.
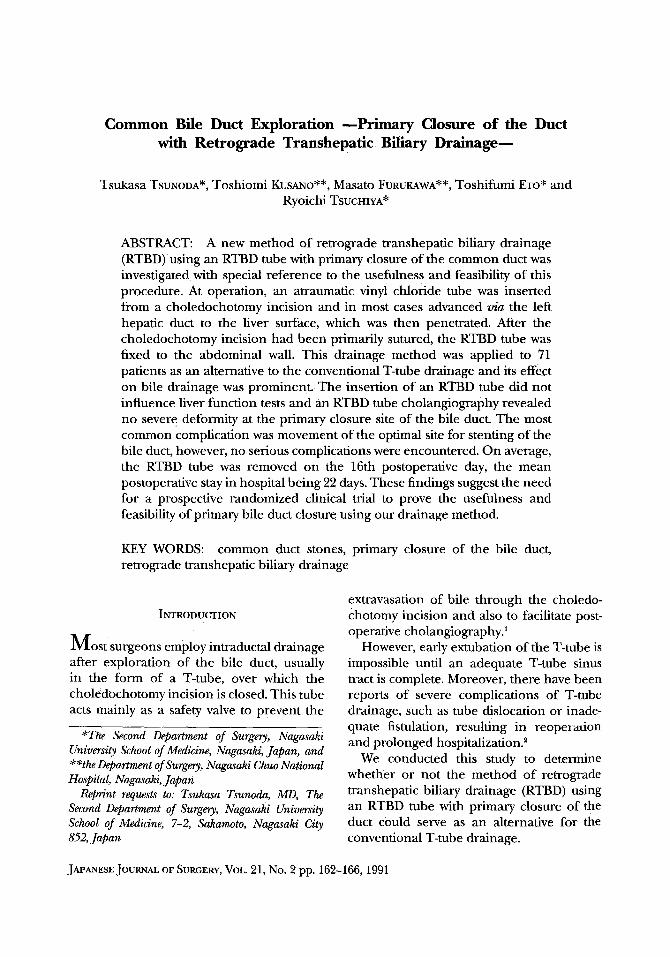
A schematic drawing of our drainage method is shown in Fig. 2. At the time of operation, the needle was inserted from a Choledochotom E incision and advanced as far along the designated intrahepatic duct as possible. An intraoperafive ultrasonography was per formed at this stage to avoid penetra- tion of the large vessels. The surgeon then placed the palm of the other hand on the liver surface, palpated resistance of the tip of the needle, penetrated the liver parenchyma, and then placed the other tip at the most preferable site in the common bile duct for drainage. The abdominal wall was then penetrated as close to the penetrated site o f the liver parenchyma as possible and t h e RTBD tube fixed to the abdominal wall. T h e common bile duct incision was closed with 3-0 or 4-0 atraumatic absorbable suture and a Penrose drain left in situ for 1-2 days at the Winslow's foramen. We found it preferable to insert the RTBD tube to the liver surface
Fig. 1. The RTBD tubes: the tip of these catheters can be bent according to the required purpose.
,,, ~,",, ,~v~:;
/77-%,"
I ~ --Primary closure site of y . . /L the common bile duet
~ Penrose drain Fig. 2. A schematic drawing of retrograde
transhepati e drainage.
via the left hepatic duct to p reven t disloca- tion or movement of the tube.
The patients in this study who underwent both RTBD and primary bile duct closure after common duct exploration were re- viewed with reference to the effect on bile drainage, liver function tests, deformity of the primarily sutured bile duct, complica- tions, and periods of tube drainage and hospital stay after RTBD.
RESULTS
The daily bile outflow and changes in liver function are shown in Table 1. The mean bile drainage through the RTBD tube was 488 ml per day on the 3rd postoperative day and 514 ml per day on the day before clamping of the tube. There were no signifi- cant differences in the values o f GOT, GPT, ALP or LAP between the preoperative period and the 3rd postoperative day, however, the
164
Table 1.
Tsunoda et al.
Daily Bile Outflow and Changes in Liver Function (n=70)
Jpn. J. Surg. March 1991
Preop 3POD Day before Clamping
Bile flow (ml) (--) 488-t-270 514_+73
LFTs I I
Bilirubin (mg/dl) 1.6___1.0 0.7+--1.3 1.1+-0.3
GOT (IU/1) 34+- 11 46+- 16 26-+ 8 I I
GPT (IU/1) 95_+ 83 98+_ 28 55+_37
ALP (IU/1) 381+_171 340-t-152 310-+74 I I
LAP (IU/1) 176+- 73 145+- 19 131-+23
Preop, preoperation; 3POD, 3rd postoperative day; Day before clamping, Day just before clamping of an RTBD tube; LFTs, liver function tests The data from a patient with inadvertent extubation of an RTBD was excluded., ,=95% confidence interval
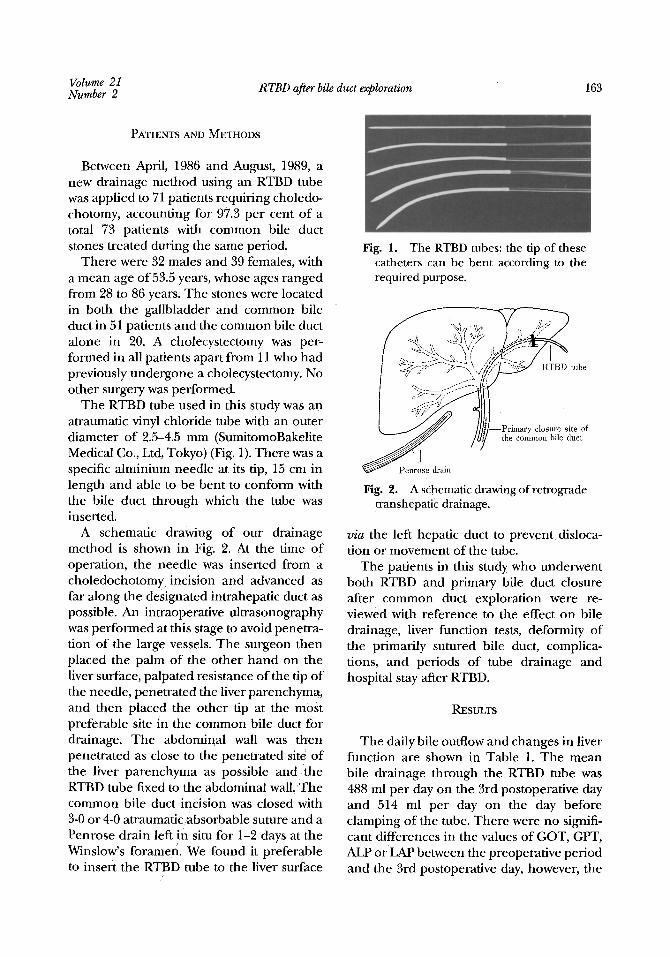
Fig. 3a. An example of no or mild de- formity seen on an RTBD tube cholan- giograpby.
values had improved by the day before removal o f the RTBD tube.
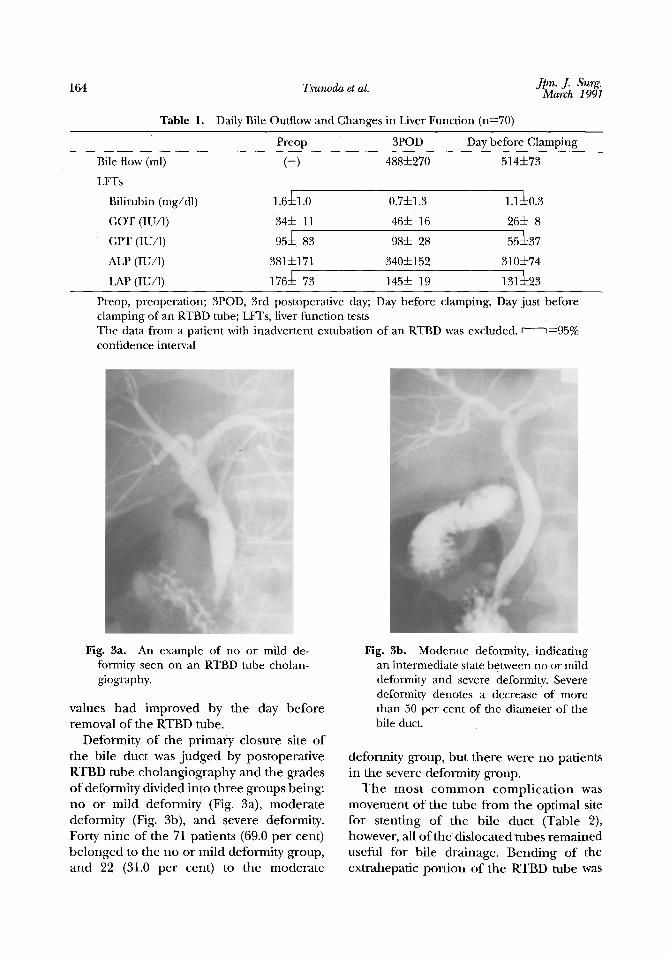
Deformity of the pr imary closure site of the bile duct was judged by postoperative RTBD tube cholangiography and the grades of deformity divided into three groups being: no or mild deformity (Fig. 3a), modera te deformity (Fig. 3b), and severe deformity. Forty nine of the 71 patients (69.0 per cent) be longed to the no or mild deformity group, and 22 (31.0 per cent) to the moderate
Fig. 3b. Moderate deformity, indicating an intermediate state between no or mild deformity and severe deformity. Severe deformity denotes a decrease of more than 50 per cent of the diameter of the bile duct.
deformity group, but there were no patients in the severe deformity group.
T h e mos t c o m m o n c o m p l i c a t i o n was movement of the tube f rom the optimal site for stenting of the bile duct (Table 2), however, all of the dislocated tubes remained useful for bile drainage. Bending of the extrahepatic port ion of the RTBD tube was

Volume 21 Number 2 RTBD after bile duct exploration
Table 2. Complications after RTBD Tube Insertion
Movement from the optimal site in the bile duct 19/71 (26.8%) Bending of the extrahepatic portion of the tube 6/71 (8.5%) Bleeding 2/71 (2.8%)
Total 27/71 (38.0%)
165
seen in 8.5 per cent of the patients. Two patients suffered bleeding from the tube af ter inser t ion, which was al leviated by moving the tube about 1 cm. No bile dis- charge from the Penrose drain, that is, no extravasation of bile through the choledo- chotomy incision, was noticed. No complica- tions necessitating reoperation or prolonga- tion of hospitalization arose.
The postoperative course was virtually un- eventful in all patients. The RTBD tube was removed between the 7th and 28th post- operative day, the mean being the 16th day, after 1 or 2 days' clamping of the tube. Before clamping, the RTBD tube was with- drawn just enough to remove it from the bile duct but to leave the tip in the liver paren- chyma. In one patient, the RTBD tube was inadvertently removed on the second post- operative day, but there were no resultant complications such as biliary peritonitis or bile discharge from the inserted penrose drain. The patients were discharged on the 12th to 28th postoperative day, the mean being the 22nd day and there have been no long term complications such as biliary stric- ture or gallstone recurrence thus far ob- served.
DISCUSSION
Although it may be possible in some cases to perform primary closure of the common bile duct without drainage, T-tube drainage has been routinely employed at many institu- tions all over the world. In fact, until our RTBD drainage method come into use, we had also performed T-tube drainage.
In addition to primary duct closure, the purpose o f our drainage method using an RTBD tube was/also to provide the advan-
tages of T-tube drainage, such as bile duct drainage and the facilitation of postoperative cholangiography, as well as to overcome the major complicat ions o f T-tube drainage, such as tube dislocation and inadequate fistulation, which may result in biliary peri- tonitis.
For biliary drainage, Smith reported in 1964 the excellence of the retrograde trans- hepatic route by which bile is guided from the. distal to proximal sites? Th e drainage effect of our method was prominent and thought to be sufficient because the liver function tests improved and there were no hazardous ,complications. Furthermore, the fact that n0,deter iorat ion had occurred in the liver function tests by the 3rd postopera- tive day prove d that the insertion of an RTBD tube had exerted no direct influence on liver function.
The postoperative cholangiographies in our series revealed no severe deformity of the primary closure site of the incised bile duct. Sawyers et aP reported 250 patients undergoing bile duct exploration with pri- mary closure of the duct and no stenosis of the sutured bile duct was reported on the basis of a follow-up study, al though no postoperative cholangiographies were per- formed. In patients with severe stenosis of the sutured site requiring correction, or in patients with retained stones, an RTBD route can give access for percutaneous bougieing of the stricutred bile duct or for percutane- ous endoscopic lithotomy after widening of the stricture by graduated dilatorsr
T h e most c o m m o n compl ica t ion was movement of the RTBD tube from the opti- mal site for stenting of the bile duct, al- though the dislocated RTBD tubes remained useful for bile drainage and caused no

Jpn. J. 166 Tsunoda et al. ~',~',~; March
serious complications. Accord ing to the re- por t o f Sawyer et al c o n c e r n i n g pr imary closure o f the duct, 4 it is no t always necessary to stent the bile duct after c o m m o n duct explorat ion. Bend ing o f the ex t rahepa t ic por t ion o f the tube was of ten seen w h e n a small caliber RTBD tube was used. Bleeding has b e e n a n o t h e r serious p rob lem in the past 3 but massive b leed ing is now avoidable because damage to large b lood vessels can be prevented by intraoperative ul t rasono- graphy.
I n this series, on average, the RTBD tube was r emoved on 16th postoperative day a nd the postoperative stay in hospital was 22 days. Extubat ion o f a T-tube can no t be d o n e until an adequate sinus tract is complete, however, an RTBD can be r e m ove d earlier because it is no t necessary to wait for comple t ion o f the sinus tract. At first, we withdrew the RTBD tube only e n o u g h to remove it f rom the bile duct and then left it in place for 1-2 days outside the bile duct in the liver pa renchyma , so that it acted as a drain for any possible bile leakage.
We did no t apply the above m e t h o d in 2 cases because o f adverse indications and bel ieve it shou ld no t be used w h e n there is a h igh possibility o f re ta ined stones.
Al though the n u m b e r o f patients t reated by this p rocedure is still small and the longest observat ion per iod has ,only b e e n 42 months , we have no t exper ienced any late complicat ions s ince discharge. These find- ings suggest the n e e d for a prospective r a n d o m i z e d clinical trial to prove the use- f u lne s s a n d feas ib i l i ty o f o u r d r a i n a g e method.
(Received for publicat ion on Jan . 29, 1990)
REFERENCES
1. Chassin JL. Common bile duct exploration. In: Operative strategy in general surgery (Vol. 2). New York: Springer-Verlag 1984; 83-100.
2. McKenzie G. Extravasation of bile after operations on the biliary tract. Aust New ZealJ Surg 1955; 24: 181-191.
3. Smith R. Hepaticojejunostomy with transhepatic intubation. A technique for very high strictures of the hepatic duct. BrJ Surg 1964; 51: 186-194.
4. Sawyers JL, Herrington JL, Edwards WH. Primary closure of the common bile duct. AmJ Surg 1965; 109: 107-112.
5. Kune GA, Sali A. Mechanical extraction through T- tube track. In: The practice 'of biliary surgery. Oxford: Blackwell Scientific Publications 1980; 173-176.