Embed Size (px)
Citation preview

Health Services Management Centre
Contents
1. Introduction and background
- this project- policy context- defining commissioning- levels of commissioning
2. Commissioning in the reformedNHS
- the commissioning challenge- the tasks and activities of
commissioning- PCT commissioning functions- practice based commissioning
functions
3. Governing commissioning
- the commissioning governance ‘web’- governing partnerships- governing markets- governing practice based
commissioning- involving patients and the public- securing clinical advice and leadership
4. Developing commissioningcapacity
- leadership- data capture, processing and analysis- procurement and contracting- external communications: public
relations and public engagement
5. Conclusion: putting policy intopractice
References
Appendices
Commissioning in the reformed NHS:policy into practiceElizabeth Wade, Judith Smith, Edward Peck and Tim Freeman
March 2006ISBN: 0 7044 2582 3
Executive summary
In 2006, PCTs and practice based commissioners face an expansion in their overallcommissioning function.
PCTs will need to become ‘NHS Local’, a strong, legitimate and recognised body thatpeople consider to be responsible for ‘their’ NHS.
The expanded commissioning task comprises three sets of functions that wedescribe as being the ‘conscience’, ‘eyes and ears’, and ‘brain’ - this reflects corefunctions of governance, data gathering and analysis, and procurement.
PCTs are responsible for deciding where to locate these functions - some will beaggregated upwards to supra-PCT bodies, others will be contained within the PCT,and others will be sub-contracted to practice based commissioners or others.
PCTs will be the overall guardian of local commissioning activities and hence will needto develop stronger and more sophisticated governance of the ‘web’ of accountabilityrelationships both within the local health system, and across wider civic society (e.g.Local Strategic Partnerships).
Specifically, PCTs will need to give consideration to how they will governpartnerships, markets, their relationship with patients and the public, and the securingof clinical advice and leadership. The model of a corporate board taking advice froma professional executive committee and patients’ forum is unlikely to be fit for purposein the reformed NHS.
Other models for securing public engagement in PCT governance need to be exploredas a matter of urgency, drawing on relevant experience within the wider publicsector and NHS foundation trusts.
There is a need for careful review of the role of professional executive committees,and for consideration to be given to additional and alternative models of gainingclinical advice and input.
Practice based commissioning calls for a more sophisticated approach to themonitoring and management of conflicts of interest at a practice level. It might behelpful to consider practice based commissioning as a form of extended serviceprovision in this regard.
NHS commissioning has been a largely under-developed function to date, with littleattention given to growing the next generation of commissioning specialists. In orderto deliver the extended range of commissioning functions in a manner that is properlygoverned, there is a need for PCTs to develop commissioning capacity and capabilityas an immediate priority.
To support this, PCTs should undertake a detailed skills audit to identify existingexpertise within PCT and practice teams, gaps in the skill base, and plans forensuring these are filled within the new commissioning arrangements.
The current process of commissioning reform presents significant challenges.However, it also offers unrivalled opportunities for detailed analysis of thecommissioning task, and for developing far-reaching plans to enhance the skills of thepeople charged with what is probably the most responsible of management activitieswith a health system.

2 Commissioning in the reformed NHS: policy into practice
1. Introduction and background
In March 2005, the NHS Alliance and HSMCpublished a briefing paper on ‘ReconfiguringPCTs: influences and options’ (Peck andFreeman, 2005). The report wascommissioned in the context of growingscepticism over the ability of individual PCTsto effectively and efficiently discharge theirexpanding range of responsibilities,particularly in relation to the commissioningof secondary care. Its purpose was toinform PCT boards and professionalexecutive committees (PECs) about theinfluences on, and options available forreconfiguring commissioning functions. Thereport identified a range of emerging modelsthat moved beyond PCTs operatingindependently as commissioners, but thatfell short of total merger. Options suggestedincluded managed practitioner networks,joint commissioning arrangements, jointpolicy units between PCTs and localauthorities, and PCT associations.
The 2005 report concluded that the choiceof appropriate options for PCTinterdependence would require judgement ata local level (taking account of relevanthistory and context), and would in manycases involve a combination of approaches.To assist local option-appraisal, the reportprovided some analysis of the differentemerging commissioning structures, and theextent to which each of these supported arange of different PCT functions.
This projectThe purpose of this second phase of theresearch is to build on the first, assessingmore specifically the particular policychallenges posed by Commissioning aPatient-Led NHS (CPLNHS) (Department ofHealth 2005a), exploring the ways in whichlocal health communities are responding tothese, and considering what this means forthe future role and configuration of PCTs.The current reforms clearly haveimplications for both the commissioning andproviding responsibilities of PCTs. However,this report focuses on the factorsinfluencing commissioning configuration andfunctions. The rationale for this focus isthat:
i) the complexity and scope of the issues tobe considered warrants a separate andspecific analysis;
ii) changes to commissioning structuresnow have a defined national frameworkand pressing timetable, while the policyapproach to provider options is one that isbeing left more to local determination; and
iii)Arguably, consideration of commissioningconfiguration should precede that of newprovider models, the pattern of whichshould be driven by the newcommissioning bodies once their ownfunctions and objectives are more clear.
This project has entailed a review of theliterature concerning: health commissioning;primary care-led commissioning; primarycare organisations; public sectorgovernance; and the development ofcommissioning and purchasing capacity.Interviews have been carried out with casestudy sites in the NHS, these being healthcommunities known to be pursuingdistinctive approaches to the organisationand development of their commissioningfunctions. Finally, a stakeholder workshopwas held in Birmingham in January 2006 asa means of testing out early themes andfindings from this study. The workshopdrew together managers, clinicians andresearchers who are closely involved in themanagement and governance ofcommissioning in health and social care. Afull list of workshop participants is set out atAppendix A.
Policy contextWith the implementation of ‘Shifting theBalance of Power’ in 2002, commissioningbecame a core responsibility of primary caretrusts (PCTs) in England, along with the dutyto improve health and develop primary care(Department of Health, 2001).Commentators observed that the successof Shifting the Balance of Power indelivering the objectives of the NHS Plan(Department of Health, 2000) would dependupon ‘… the ability of Primary Care Trusts todevelop robust commissioning systems thatcan ensure the delivery of better, moreaccessible and more cost effectiveservices’ (James et al, 2002, p.5).
Since then, the importance of commissioningfunctions has been reinforced, as PCTshave acquired additional responsibilities forcommissioning primary care services. In thecase of the new medical servicescontracts, this has required a shift from thetraditional ‘primary care development’function of PCTs to a more explicitrelationship between PCTs ascommissioners, and practices as providersof services, while the implementation of thenew dental and community pharmacycontracts has presented an entirely newchallenge to many PCTs. Devolution ofresponsibilities in areas such as prisonhealth has expanded further the scope ofPCTs’ commissioning functions, again
requiring the development of newknowledge, skills and processes.
The extent of the challenge facing PCTswas emphasised at the time of theirestablishment, along with the need to allowthem time and space to develop appropriatestructures, skills and relationships (Smithand Goodwin, 2002). There has been agrowing sense, however, that instead ofgradually rising to this challenge, PCTs havestruggled to fulfil their expanding range offunctions (Bramley-Harker and Lewis, 2005;Smith and Mays, 2005). As noted above, itwas in response to this fact, and theexpectation that some reconfiguration ofcommissioning functions would be requiredto address the situation, that the originalphase of the current research wascommissioned (Peck and Freeman 2005).
Since the initial report was published, thepolicy context has changed significantly,following the publication of ‘Commissioning aPatient-Led NHS’ in July 2005, andsubsequent supporting guidance. Thispolicy, designed to instigate ‘…a step-change in the way services arecommissioned by front-line staff…’(Department of Health, 2005a, p1) set outthe Government’s requirements for:
universal roll-out of practice basedcommissioning by December 2006;improved coordination with socialservices through greater congruence ofPCT and local government boundaries;divestment by PCTs of all responsibilitiesfor service provision (other than in caseswhere there is no alternative solution);a progressive move towards greater useof new providers, including those fromthe independent sector;development of PCT role in ensuringaccess to and choice of high qualityservices through the performancemanagement of contracts with providers;centralisation of ‘back-office’ functions(including payment) into regional ornational hubs; anddelivery of at least 15% reduction inmanagement and administrative costs.
While the policy document stated that thechanges required to deliver these outcomes‘… may or may not involve mergers andreconfigurations’ (Department of Health,2005a, p3), the direction of travel was madevery clear: ‘PCTs will become patient-led andcommissioning-led organisations with theirrole in provision reduced to a minimum’(Department of Health, 2005a, p4). CPLNHSasserted the Government’s expectation thatall these changes would be completed bythe end of 2008.

Level of Commissioning
Individual . . . Practitioner . . . Practice . . . Locality . . . Community . . . Region . . . Nation
Multi-practice orlocality
commissioning
Single practice-based
commissioning
Jointcommissioning
Primary CareOrganisation/PCT
commissioningNational
Commissioning
Lead PCT/LHB/HBcommissioning
PatientChoice
Commissioning in the reformed NHS: policy into practice 3
In response to major concerns raised byNHS staff, trades unions and professionalbodies, the Government has now steppedback from original statements regarding thecompulsory transfer of existing PCT-managed services to alternative providers,emphasising that the nature of managementof community and other PCT services will bedown to local determination (DoH 2006a,p.13). Nevertheless, a clear marker as tothe trend anticipated by the Government hasbeen set. At the very least, thecommissioning ‘arms’ of PCTs are expectedto separate themselves from in-houseservices, and to subject them to the sameperformance management and monitoringregime as any other provider. They are alsoexpected to consider the potential forgreater value for money and flexibility to bedelivered through alternative providermodels.
Since August 2005, all SHAs have thereforedeveloped options for local PCT(re)configuration, which collectivelypropose the number of organisations beingreduced to anything between 120 and 160(compared to the current 300). TheDepartment of Health has reviewed andapproved these proposals, which weresubject to a 14-week consultation(concluded on 22 March 2006). Whateverthe final outcome, at the time of writing it isclear that increasing interdependence andcollaboration between PCTs will be requiredin the future, both during the transition to thenew arrangements, and in the subsequenttask of delivering a ‘step-change’ in theeffectiveness and efficiency of NHScommissioning. Full guidance on the futurecommissioning framework for new PCTs isdue to be published in the summer of 2006.This report seeks to assist PCTs and otherstakeholders in determining what thefunctions of commissioning will look likepost-CPLNHS, and to analyse what thosefunctions will mean for the governance anddevelopment of commissioning.
Defining commissioning‘Commissioning’ is a function that applies tothe role of ‘third party payers’ in a healthsystem, namely organisations or individualswho have responsibility, on behalf oftaxpayers or insured persons, for spendingresource allocated for healthcare in waysthat will ensure the meeting of the healthobjectives of the health system, insuranceorganisation or patient. Woodin(forthcoming) has defined commissioning inthe NHS as follows:
‘Commissioning…tends to denote aproactive strategic role in planning,designing and implementing the rangeof services required, rather than amore passive purchasing role. Acommissioner decides whichservices or health care interventionsshould be provided, who shouldprovide them, and how they shouldbe paid for, and may work closelywith the provider in implementingchanges.’
She goes on to explain that a purchaserbuys what is on offer, or reimburses aprovider on the basis of usage, this being aless strategic and more operational activity.She considers procurement and contractingto be activities that focus on one specificpart of the wider commissioning process –the selection, negotiation and agreementwith the provider of the exact terms onwhich the service is to be supplied. Woodin
adds that procurement usually refers to theprocess of provider sourcing and selection,and contracting to the establishment andnegotiation of the contract documentation –her overall definitions of activities related tocommissioning are set out in box 1 below.The definition of commissioning used byWoodin is similar to that of John Ovretveit(1995) who extended the understanding ofcommissioning to include activities which donot directly involve payment for services,such as influencing other agencies topromote the health of the population.
In exploring the functions and tasksassociated with commissioning in the NHSfor 2006 and beyond, we are taking the term‘commissioning’ to embrace the variousactivities identified by Woodin under theheadings commissioning, purchasing,procurement and contracting (see box 1).
Box 1: definitions of activities associated with the commissioning function
Commissioning is the set of linked activities required to assess the health careneeds of a population, specify the services required to meet those needs within astrategic framework, secure those services, monitor and evaluate the outcomes.
Purchasing is the process of buying or funding services in response to demand orusage
Contracting is the technical process of selecting a provider, negotiating and agreeingthe terms of a contract for services, and ongoing management of the contract includingpayment, monitoring, variations.
Procurement is the process of identifying a supplier, and may involve for examplecompetitive tendering, competitive quotation, single sourcing. It may also involvestimulating the market through awareness raising and education
(Woodin, forthcoming)
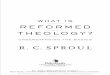
Figure 1: The Continuum of Commissioning Levels in the UK
Source: Smith et al, 2004, p6

4 Commissioning in the reformed NHS: policy into practice
Levels of commissioningInternational analysis of commissioning(Robinson et al, 2005) identifies three mainlevels at which this ‘strategic purchasing’takes place: macro-level (through a nationalsingle health insurance fund); meso-level(regional organisations with devolvedpurchasing responsibilities for populationsof 100,000 to 500,000); and micro-level(situations with a high degree of localdecision making and devolved purchasingbudgets). Within the NHS, these levelscould be categorised as follows:
macro-level – national commissioningarrangements and performance targets,pan-PCT specialised commissioningmeso-level – PCT commissioning, jointcommissioning with local authoritiesmicro-level – practice-basedcommissioning, direct payments, patientchoice
There are different benefits and risksassociated with locating commissioningactivities at each of these levels. Forexample, as it sits closest to the ‘end-user’of the commissioning process (the patient orclient), ‘micro-level’ commissioning might beexpected to improve sensitivity andresponsiveness to users’ needs. However,it is also likely to have increased ‘transactioncosts’, due to duplication of activities by alarge number of small commissioners.
In a review of the research evidenceconcerning effective primary care-ledcommissioning (Smith et al, 2004), theauthors concluded that rather than a single‘ideal’ location for commissioning, there wasa continuum of commissioning activity thatran across the different levels of a healthsystem. The challenge for managers andpolicy makers was how to decide at whichlevel of the system specific commissioningactivities should be located. The continuumdeveloped in Smith et al’s research is set outin figure 1.
This continuum provides a basis on whichpolicy makers and managers can decidetheir specific local commissioningconfiguration, namely where to allocate theresponsibility for carrying out the planning,purchasing and funding of a particularservice or health priority. It does nothowever elucidate the actual nature ofdifferent elements of the commissioningfunction – that is, what actually happenswithin this activity we are describing as‘commissioning’. The current researchtherefore extends this analysis, bydescribing in more detail the different tasks
and activities contained within thecommissioning function, and what thesemean for the configuration and managementof commissioning bodies.
This reportThis report focuses on a detailed analysis ofwhat the commissioning function post-CPLNHS will actually entail – the tasks andactivities that will need to be carried out byPCTs or their agents. This analysis is setout in section 2 of the report, and isintended to offer PCTs and practice basedcommissioners a ‘map’ of the territory thatlies ahead, along with some case studyexamples of how local organisations areresponding to the need to redesigncommissioning arrangements. Section 3considers what theory and experience tellus about the governance arrangements thatwill be established in the implementation ofthe current round of system reforms andreorganisation of the commissioningfunction. In section 4 of this report, weexplore the issue of how commissioningcapacity can be developed and thenecessary skills put in place to enablestrong and effective commissioning to becarried out in the NHS. In section 5, wedraw together the practical steps that arerequired if PCTs are to develop strong andeffective commissioning within the reformedNHS.
2. Commissioning in thereformed NHS
The timing and nature of the publication ofCPLNHS has been the cause of someconcern both within and beyond the NHS. Inits review of the policy, for example, TheHouse of Commons Health Committeeconcluded “the research evidence is clearthat this restructuring will set NHSorganisations back by 18 months, withpatient services likely to be affected in theinterim” (House of Commons 2006, p.6).
Consequently, the Department of Health hasbeen keen to demonstrate how this policyfits with, and is fundamental to the deliveryof, wider health system reform. In “Healthreform in England: update and next steps”(Department of Health 2005b) CPLNHS istherefore presented as one of themechanisms for strengthening the ‘demand’side of the health service market.Emphasising that there has been significantinvestment in modernising and increasingthe capacity of service providers (the‘supply side’) in recent years, the document
explains that maintaining theseachievements through a process ofcontinuous improvement now depends onestablishing a much stronger voice forpatients, and for the commissionerssecuring services on their behalf.
In combination, Patient Choice, Payment byResults, and Practice-Based Commissioning(PBC) are intended to provide new ‘stronger’PCTs with the tools required to deliver a‘patient-led NHS’.
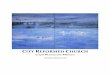
The overall commissioningframeworkTo some extent, the system reformscurrently being enacted in pursuit of this‘self-improving’ NHS involve a transfer ofexisting commissioning responsibilities andfunctions from one type of commissioner toanother at a different level in the system(e.g. some responsibilities for serviceredesign will be devolved from PCTs topractice based commissioners, and somedecisions about referral will move from theGP/practice based commissioner to thepatient). However, there are also a numberof new commissioning activities within thereformed system (e.g. supporting practicebased commissioning and patient choice),so that that the overall effect is anexpansion, rather than simply a re-alignment, of commissioning functions (seeFigure 2).
Figure 2 does not attempt to accuratelyrepresent the actual relative distribution(current or anticipated) of commissioningresponsibilities between the organisationsinvolved. Rather, it simply seeks to illustratethat the overall size and scope of thecommissioning framework appears likely toexpand under the proposed systemreforms. This is because all constituents ofthe system will be taking on new tasks thatare not required in the existing framework,without necessarily losing existingfunctions. This is true at all levels. Theindividual patient, for example, in gainingincreased choice, also now has more ‘work’to do in exploring the options for exercisingthat choice. At the other end of thespectrum, the role of national bodies suchas independent regulators will expandbeyond the inspection and assurance ofservice standards, to include the setting of aregulatory framework (the ‘rules’) for theexternal market.
As noted above in the case of PCTs andpractice based commissioners, the systemreforms theoretically involve shifting someexisting commissioning responsibilities and

Commissioning in the reformed NHS: policy into practice 5
functions from one to the other. It issuggested here, however, that the level ofsupport for PBC that practices will requirefrom PCTs, combined with the need for PCTsto review, monitor and administer PBCarrangements, means that PCTs’ totalworkload will not be reduced. Even if thiswere the case, any excess capacity wouldsoon be absorbed by taking on the newresponsibilities that PCTs now face, such aslocal market management, and supportingpatient choice (see Figure 2).
Similarly, it might be assumed that theaggregation of tasks such as data captureand analysis at the level of PCTcollaborations or alliances will allowrationalisation of information, contractingand finance functions. This may well be thecase in the medium to long term. However,this research suggests that collection andanalysis of data at the level required tosupport PBC and PbR is a relatively newtask for many PCTs, actually requiringadditional resources. In the short-term,therefore, any rationalisation may simplymitigate previously anticipated increases inthe level of resources required, rather thanactually reducing them.
Essentially, the increasing emphasis on thePCT as the body accountable forstewardship of local health care resourcessuggests an expansion in their overallactivities and probably of the resourcesthey themselves will require. At the sametime, the responsibilities of other agenciesinvolved in the ‘demand-side’ of the system(e.g practice based commissioners, PCTcollaborations) also appear to be expanding.
This is quite appropriate given the intentionto re-balance supply and demandrelationships in the NHS as part of theoverall intention to ‘strengthen’commissioning. However, this clearly hasimplications for the capacity and capabilityof the emerging organisations tasked withdelivery, particularly given that another majorobjective of CPLNHS is to reducemanagement costs in PCTs and strategichealth authorities (SHAs) by 15%. Thesubject of commissioning capability isexplored in detail in section 4.
Given this expansion in the overallcommissioning function in the NHS, we setout here an analysis of the nature of thetasks within this expanded function, beforegoing on to suggest the levels of the healthsystem at which these tasks and activitieswill take place, and how they will begoverned.
Figure 2: Expansion of the commissioning framework:
The tasks and activities ofcommissioningSmith and Mays (2005) have conceptualisedthe commissioning element of a healthsystem as its ‘conscience’ (thoseelements that relate to stewardship, qualityassurance, public protection) and ‘brain’(activities associated with resourceallocation decisions, system and servicedesign, planning). As a result of discussionand analysis carried out with NHSstakeholders as part of this research, wehave added to that metaphor a thirddimension of the ‘eyes and ears’ (thetasks that are related to keeping close to thepatient experience, receiving and analysingdetailed information, determining messagesfor subsequent action by the brain andconscience).
The responsibilities of these elements canbe summarised as follows:
Conscience - setting out “how thingsshould be” -what the system aims toachieve and how;Eyes and ears - observing and reportingon “how things are” - what the system iscurrently delivering;Brain (having processed information fromboth sources) - identifying andimplementing the optimal solutions fordelivering stated objectives.
The relationship between these componentsis of course dynamic, as the ‘eyes and ears’monitor and report back information on theoutcomes of the interventions designed by
the ‘brain’, and the ‘conscience’ reflects onthis, potentially adjusting the objectives orrules of engagement, in an attempt tomaintain the overall consonance of thesystem. The ‘eyes and ears’ will be presentin a number of different places in the system(patients, GPs, nurses, informationcollectors and analysts, regulators etc.) andhence the specific ways in which theyinteract with the brain and conscience willvary according to the local health system, itsconfiguration and governance. This issue isexplored further in section 3. Figure 3summarises the anticipated tasks of the‘conscience’, ‘eyes and ears’ and ‘brain’within the new commissioning framework.
This analysis demonstrates the extensiverange of responsibilities that accrue tocommissioners in the NHS post-CPLNHS. Italso highlights the fact that the differenttypes of commissioning functions andresponsibilities do not map directly toparticular levels of the health system (as setout in figure 1), but are instead distributedacross them. For example, within a nationalbut devolved system, responsibility for‘determining overall system objectives’ lieswith the government (for setting nationalpriorities and targets), with SHAs and,increasingly, PCT collaborations (foroverseeing the strategic, rationalconfiguration of services), and with PCTs(for identifying and prioritising local needs).Likewise, the assessment of servicecapacity and outcomes will require both‘hard’ data collected at a PCT or supra-PCTlevel, and more ‘qualitative’ data provided by
Examples of new tasks Pt: research re provider and treatment options Prac: supporting patient choice; service planning & re-design PCT: Perf mgt of primary care providers & PBCs; co-ordinating tendering & procurement; administering PBC; managing partnerships PCO+: data capture & processing. SHA: accreditation of providers; performance managing PCTs National: price setting; establishing and regulating competition policy
Pre-reform distribution of commissioning responsibilities
National Bodies
Individual Patient
Practice
PCT
PCO Collaboration
SHA

practice based commissioners on the basisof feedback from their own patients.
The Department of Health has stated that itdoes not expect commissioning to be theresponsibility of a single organisation in apatient-led NHS, but rather a partnershipbetween PCTs, general practice, local (andpresumably national) government. It hasalso given strong indications that it expectsthe independent sector to become moreinvolved in supporting commissioningfunctions particularly, though notexclusively, in the delivery of ‘backroom’ oradministrative tasks (2005b). Researchcarried out for this project indicates thatconsideration of this option is alreadyunderway in some areas.
Further guidance to clarify exactly how theDepartment of Health sees this matrix ofresponsibilities working in practice is duelater in 2006. However, certain things arealready very clear:
i) New PCTs will be held to account for theeffective use of taxpayers’ money in theinterests of their local communities
ii) There will be two major hubs ofcommissioning activity (and risk) – thePCT and the practice-based commissioner(PBC).
iii) The relationship between these hubs willbe critical to the success of the systemreforms.
We therefore focus on these two types ofcommissioner as the basis in our analysis ofwhat a local commissioning system mightlook like in 2006 and beyond.
PCT commissioning functions
Current health system reforms positioncommissioning bodies not simply as the ‘co-ordinators’ of a local NHS system but,potentially, as the only ‘pure’ NHS bodyexisting at a local level. The policyframework points to an eventual (althoughunlikely) possibility of a provider networkmade up largely (or even entirely) of non-NHS providers (recognising here that themajority of primary care practitioners - GPs,dentists, pharmacists, optometrists - are notmanaged by, but rather work under contractwith, public sector bodies as thingscurrently stand). The principles of publiclyfunded health services are not, however,being questioned. It is the PCT that will beaccountable for making sure that theseprinciples are upheld for the local population,and it is this responsibility that encapsulatesthe PCT’s core commissioning functions.In effect, the PCT becomes the ‘NHS Local’.This reflects the emphasis in CPLNHS on
strong and effective local commissioningbodies that are, where possible,coterminous with elected local authorities,and hence identifiable to citizens as ‘theNHS in our area’. In time, the terminologyitself might need to be changed to reflectthis idea, with “Our Town NHS”, being notonly more resonant for the local populationthan “Our Town Primary Care Trust”, butalso a more accurate description of thecomprehensive local health responsibilitiesof PCTs (which are clearly not only involvedin the delivery of primary care services asthe name perhaps suggests to the public).
If PCTs are the embodiment of the local NHS,it follows that all of the tasks set out infigure 3 will, to some extent, be part of theircommissioning (and wider governance)responsibilities. It does not mean, however,that they will all be actually undertaken byeach PCT. Certain functions might beaggregated upwards if they are moreeffectively or efficiently performed at asupra-PCT level, others might be delegateddownwards (for example to practice basedcommissioning clusters), and some might becontracted out of the NHS altogether.We explore here what their commissioningresponsibilities mean for a PCT, and thedegree to which each is appropriatelyshared with other parties. The areas ofresponsibility examined are: objective settingand decision making; the management ofpartnerships; supporting patient choice;information collection and analysis; servicespecification and resource allocation; andprocurement and contracting.
Objective setting and decision making
The ‘conscience’ functions set out in figure3 are clearly a core part of the role of thePCT as the local NHS body accountable forthe use of resource, assurance ofstandards, and improvement in health.These conscience functions will, in somecases, be governed by standards andframeworks designed elsewhere in thewider health system. For example, someservice standards will be determined by theHealthcare Commission, market rules will, inpart, be set by the Department of Health,and priority setting for healthcare resourceswill be influenced by the guidance anddecisions of the National Institute for Healthand Clinical Excellence.
Individual PCTs will, however, be held toaccount for the effective allocation ofresources and delivery of standards withinthese frameworks. For this level ofaccountability to be reasonable and
meaningful, PCTs must not only have accessto effective incentives and sanctionsthrough which to influence providerbehaviour (as is the intended outcome of thereform programme), but also recognition bythe wider system that they (rather than thestrategic health authority or Department ofHealth) are the main locus for decision-making regarding the local NHS.
This research thus highlights a need for astronger PCT, one that is enabled to standup for its decisions, both in relation to itslocal population and to the Department ofHealth. Given that this decision-makingresponsibility is the crux of theorganisation’s accountability to patients andtaxpayers, the function is not amenable to‘outsourcing’ or sub-contracting, whether toother NHS, or independent sector bodies.
All PCTs therefore need to establish robustdecision-making arrangements that enablethe organisation to be clear about itspriorities and objectives, and about howthese are to be met.
The management of partnerships
As the PCT increasingly takes on a role as‘NHS Local’, seeking to claim legitimacy forplanning and delivering services that willimprove the health of its local population, soit needs to demonstrate an effective andsophisticated ability to manage a wide rangeof partnerships. These partnerships willtake a variety of forms and will include: jointcommissioning arrangements with localauthority and voluntary sector bodies; leador joint commissioning schemes with otherNHS bodies; participation in formalpartnership structures such as localstrategic partnerships; and communityplanning arrangements emerging fromregeneration or other initiatives.
Supporting Patient Choice
Within the current health system reforms,‘Patient Choice’ is both a general policyobjective (to empower patients and thepublic by increasing their knowledge of andinfluence over service delivery) and aspecific initiative (which means that allpatients requiring hospital treatment shouldalready have the option to choose from atleast four different health care providersand, by 2008, will have the right to choosefrom any provider, as long as they meetclear NHS standards and are able to do sowithin the national maximum price that theNHS will pay for the intervention the patientneeds).
6 Commissioning in the reformed NHS: policy into practice

Figure 3: The ‘conscience’, ‘eyes and ears’ and ‘brain’ of NHS commissioning
Responsibilities of the conscience include: Responsibilities of the eyes and ears include: Responsibilities of the brain include:
likely to be undertaken fully or partly at a national/ regional level
indicates activities to be undertaken by PCTs
likely to be assumed either fully or in part by practice based commissioners
likely to be undertaken fully or partly at a national/ regional level
indicates activities to be undertaken by PCTs
likely to be assumed either fully or in part by practice based commissioners
likely to be undertaken fully or partly at a national/ regional level
indicates activities to be undertaken by PCTs
likely to be assumed either fully or in part by practice based commissioners
Establishing the overall objectives of and desired outputs from the system Setting minimum standards for services Evaluating and weighing the costs and benefits of different market models Assuring the quality of services commissioned Influencing patterns of demand at a macro level through public health activities Setting and regulating the ‘rules of engagement’ to assure the probity and ‘acceptability’ of the system (including developing nationally specified ‘core contracts’) Ensuring that the rules of engagement allow for sufficient contestability and choice within the local system Registering, regulating and arbitrating in conflicts of interest within the local health market
Ensuring that health system objectives dovetail with those of other local commissioners (e.g. those who are part of Local Strategic Partnerships) Ensuring appropriate and mature partnerships with other health and social care organisations and agencies are in place, and proactively managed Stewardship of public resources (including reporting and accounting for outcomes) Ensuring that there are robust and appropriate methods in place for making decisions about funding priorities, and on action to be taken when brain can not reconcile demands of national priorities with available resource Ensuring the system operates in a way that does not create or increase inequalities (e.g. ensuring Patient Choice does not threaten access for vulnerable individuals)
Establishing health objectives for individual patients and practice populations Supporting individuals in making choices
National collation of data and statistics for benchmarking (e.g. QOF data) External audit of local processes (e.g. Audit Commission ‘spot-checks’ of coding and reporting under PBR) Inspection of providers and commissioners against national standards (e.g. by Healthcare Commission, Monitor etc.)
Assessing needs of population and modelling demand for services (current and future) Monitoring and validating activity levels, costs and service outcomes Benchmarking need, demand, activity and outcomes Horizon scanning – identifying trends,/technologies/ evidence (e.g. as endorsed by NICE),/policies etc. likely to impact on patters of need, demand and costs Designing and implementing processes to ensure patients are effectively ‘tracked’ through the health care system.
Assessing and reporting on current capacity of system to meet needs and achieve objectives (including availability of services, and patients’ experiences of health and satisfaction with health services)
Establishing structures, processes and incentives required to ensure system objectives are achieved Supporting local application of processes (e.g. through designing ‘templates’ for contracts, PBC budgets, information packs etc.)
,Deciding what services will be commissioned at which level of the system Allocating purchasing budgets to individuals, commissioners and networks Designing incentive and payment systems that encourage providers to enter market and deliver desired service models and pathways (market development and management) Procuring, contracting with and allocating resources to providers Managing the performance of providers Removing resources from providers if service levels and standards are not achieved Designing and implementing local arrangements to assure patient choice, including designing and distributing information for patients and PBCs
Translating patient experience data into information to be used in commissioning Translating patient activity data from primary and secondary care into information to be used in commissioning Planning and designing efficient and effective protocols service models, and clinical pathways (and ensuring appropriate clinical advice and service user involvement in this process) Micro-level demand management Provision of extended primary care services Supporting individuals in making choices
Utilising ‘consumer power’ in this way toplace direct pressure on providers toimprove their responsiveness is animportant part of the drive to strengthen thedemand-side of the health care system.However, it is also poses a potentialchallenge to commissioners attempting tomanage demand and develop services inline with long-term, population-basedstrategic plans.
One particular concern that has beenidentified is that ‘choice’ might be exercisedless easily by more vulnerable anddisadvantaged service users, and that theultimate effect of the policy will, therefore,be to increase inequalities in health andaccess to healthcare (Farrington-Douglas
and Allen, 2005, p.18). There is also someevidence from international experience thatpublication of the type of data onperformance and outcomes that theGovernment envisages supporting PatentChoice, may have unintended effects onprovider behaviour (e.g. selection anddifferential treatment of patients accordingto the severity of their condition and risk oftreatment) (Dranove et al 2003).Farrington-Douglas and Allen (2005) argue,therefore, that PCTs have an obligation tomanage the Patient Choice agenda in a waythat ensures equity for disadvantagedpatients, and that protects against theinadvertent reduction of choice for morevulnerable individuals. They suggest, forexample, that Primary Care Organisations
should provide or commission informationsupport and advocacy services that targetparticular groups of patients most likely toneed such assistance.
Others may argue, of course, that one ofthe main motivations for introducing patientchoice is, in fact, to give differential benefitto the more affluent, thus securing theirongoing support for a publicly funded healthservice, to the ultimate benefit of all. That is,that the objective of Patient Choice is toachieve relatively short-term politicalobjectives, rather than being seen as amechanism for promoting long-term healthimprovements.
Commissioning in the reformed NHS: policy into practice 7

Whatever position is accepted here inprinciple, in practice, PCTs will need (to agreater or lesser extent) to ensure thatappropriate information is available topatients to enable them to make choices; toassess whether the professionalssupporting patients in those choices aredoing so effectively and equitably; and tomanage the complex interaction betweenindividual patient choice, population-basedstrategic commissioning, and politicalimperative.
The governance arrangements required toenable PCTs to fulfil these ‘conscience-related’ responsibilities are explored in moredetail in section 3.
Information collection and analysis
The key to a PCT’s ability to make robustdecisions about the allocation of resourceswill be the availability of accurate, timely andmeaningful information. The responsibilitiesof a PCT’s commissioning ‘eyes and ears’therefore include gathering and reportingdata on: the current and future needs of thelocal population (and associated patterns ofdemand for services); the capacity andperformance of the system (in terms of bothactivity and costs, and patient satisfactionand outcomes); and how this comparesacross and between localities.
The type of data that will be required includebut are not restricted to:
Demographic and epidemiological datarelating to the PCT populationDescriptions of the type, location andrange of local health servicesPrimary care (medical services)performance data (e.g. access targets,QOF achievement levels, referral rates,prescribing behaviour and costs)Other primary care (dental, communitypharmacy, optometry) performance andactivity dataInformation regarding the utilisation ofcommunity and mental health services;
Secondary care activity data:- elective activity – inpatient and day
case;- non-elective admissions, including
information on length of stay;- first outpatient appointments, and
follow up ratios;- use of diagnostic tests and
procedures;- consultant to consultant referrals; and- accident and emergency attendances.Service quality data, including results ofclinical audit, patient complaints, selfassessment and independent reviewsPatient satisfaction dataHorizon-scanning information about newtechnologies, treatments andinvestigations
This information will have to be madeavailable in aggregate form for decision-making at a PCT level (or supra-PCT wherejoint commissioning arrangement are inplace), and in the form of practice basedcommissioning ‘information packs’ at theindividual practice level. One example ofhow a PCT is developing a new approach tothe collection and analysis of data, is set outin the box below.
Guidance has made it very clear that PCTsmust avoid any increase in management andtransaction costs as they implement therecommendations in CPLNHS, and thatresponsibility for producing information toinform commissioning must remain with thePCT, and not be delegated to practice basedcommissioners.
This does not necessarily mean, however,that each PCT must actually undertake thiswork – these tasks are amenable to beingcontracted out to a third party agency, beingconcerned with stating ‘how things are’,rather they ‘how things should be’. Assuch, aggregating or subcontracting thesefunctions seems less problematic than in thecase of decision-making or ‘stewardship’tasks (see column to right for an example of
Case study – North Eastern Derbyshire PCT health numerics analysisNorth Eastern Derbyshire PCT has commissioned external expertise to develop detailedanalysis of health care activity in relation to use of resources. The resulting ‘resourcemaps’ will offer an in-depth insight into the pattern of service and resource use bypatients with specific clinical conditions within a practice population (for example,chronic obstructive pulmonary disease), and are considered to be an excellent basisupon which to start practice based commissioning discussions and plans. The intentionis that this mapping of resource, drawing on both secondary care and primary careactivity and financial data, will enable more meaningful co-design of services bypractice based commissioners and hospital providers.
Contact: Martin McShane, Chief Executive, NE Derbyshire [email protected]
Case study – a contractinginformation hubIn Birmingham and the Black CountrySHA area, PCTs are developingcommercially-based support for an‘information hub’ that will undertake thetransactional work supportingcontracting. This will include theprovision of timely, relevant data andanalysis to practices on populationfactors, activity levels, tariffs,spending, and activity and financialtrends. The hub will not have anyresponsibility for commissioningdecisions, which will remain theresponsibility of the (re-configured)PCTs. A project board has beenestablished, a service specificationagreed, and consensus reachedamong all the PCTs on the funding forthe service. The aim is to havecontracted for and established theservice by the time the new SHAarrangements are in place.
Contact: Steve Allen, 0121 695 2424 [email protected]
this approach). What is important, however,is that there are transparent processes inplace to demonstrate who is carrying outwhat function, and how the PCT is holdingits subcontractors to account.
In addition to processing and disseminatingthis type of (largely quantitative) ‘activity’data, PCTs will also need to havemechanisms for gathering ‘process’ related(perhaps more qualitative) informationregarding the implementation of the newcommissioning systems. For example, theymay wish to obtain feedback from practice-based commissioners on their experiencesof establishing new service models, in orderto share relevant learning with otherpractices. Similarly, they may wish to obtaininformal feedback on the responsivenessand behaviour of a particular provider, or onpatient experiences, to inform contractmonitoring and re-negotiations. This is thetype of ‘front-line’ intelligence that practice-based commissioners can add to thecommissioning process, but which PCTcommissioners will need to access andinterpret if they are to utilise it effectively intheir procurement role. PCTs may facilitatethis type of information collection andexchange by supporting (‘virtual’ and actual)practice-based commissioning networksand forums.
8 Commissioning in the reformed NHS: policy into practice

Service design and resourceallocation
In line with their responsibilities for makingstrategic resource allocation decisions,PCTs must be responsible for decidingwhich services will be commissioned atwhat level, and for allocating purchasingbudgets accordingly. In the context ofpractice based commissioning, this includesestablishing indicative practice levelbudgets, reviewing practice basedcommissioning business cases andensuring collective risk managementstrategies are in place across the PCT.
However, many of the ‘brain’ functions ofcommissioning will be carried out by bothPCTs and other partners, or ‘sub-contracted’commissioners. These include practice-based commissioners (single practices andclusters of practices), and also potentiallyother PCTs, a local authority commissioner, aprivate sector commissioner, and a third orvoluntary sector commissioner. In this way,the PCT acts as overall steward of localhealthcare resources, and designer of thewider health system, but passes resourceto specific bodies who undertake to design,purchase and deliver specific areas ofhealth service on behalf of the PCT.
A PCT may, for example, aggregateupwards with other PCTs in order to carryout some areas of specialised servicecommissioning and, in setting priorities fornew and emerging therapies, PCTs are likelyto seek to act as associations or consortiain order to gain critical mass for purchasing,and strength and credibility in relation todevelopment. Commissioning in suchconsortia is not new to the NHS, especially
Case study: North Derbyshire, South Yorkshire and BassetlawCommissioning Consortium (NORCOM)NORCOM comprises a joint sub-committee consortium of seven PCTs which has beenformed to enable the PCTs to make collective decisions on the planning, procurementand review of services provided for populations larger than an individual district. Theconsortium also seeks to develop networks for clinical services determined to be acommissioning responsibility. A further role is to ensure an appropriate co-ordinatedresponse to issues raised by specialised commissioning programmes and, asappropriate, to coordinate links with the South Yorkshire Strategic Health Authority. Theconsortium meetings are attended by PCT chief executives and senior clinicians, and isviewed as a crucial and senior commissioning forum. It has a particular role in co-ordinating priority-setting decisions for the group of PCTs, having the capacity toconvene at short notice to debate and reach decisions on emerging therapies, recentexamples having included Herceptin and the NICE guidance on fertility treatments.NORCOM is hosted by Barnsley PCT, and is currently carrying out a major piece of workon the strategic future of cancer services.
Contact: Ailsa Clare, [email protected]
in relation to specialised services, but it isnotable that PCTs have been establishingnew forms of governance for suchconsortia, seeking to engage senior levelPCT officers in direct decision making aboutconsortium services, rather than delegatingthis ‘up’ to an agency. An example of asupra-PCT commissioning consortium is setout in the box below.
As well as aggregating commissioningfunctions upwards to consortia, PCTs willdisaggregate functions out to practicebased commissioners. For example, a PCTmight devolve a budget for diabetes care toa locality group of primary careprofessionals who are acting as a practicebased commissioning cluster, having a clearagreement with this group in relation to whatservice and health outcomes are expectedto result from the service the group designsand commissions. It should be noted thatthe practice based commissioning groupmight actually provide some elements of thecare covered by the overall commissioningbudget and, as discussed below, sucharrangements will need to be carefullyconsidered and regulated by the PCT in its‘conscience’ role.
Another example of devolution of ‘brain’functions by the PCT might be the allocationof a budget to a private healthcare companyfor the planning, funding and management ofcare for a group of older people living withcomplex conditions. Likewise, the PCT mightdevelop a contract with a local providertrust for it to design, purchase and managea service such as unscheduled out-of-hours care for a local population.In all of these examples, the PCT remainsaccountable for the commissioning
decisions of their subcontractors, andneeds to have robust methods for assuringthe quality of commissioning that is carriedout on its behalf. This process ofaccountability for devolved commissioningwill also require clarity about what the PCTis to provide to the sub-contractedcommissioner by way of support. In relationto practice based commissioning, PCTs arerequired to offer support not only throughthe provision of information, but also throughassisting practice based commissioners ininterpreting these data, and in developingskills such as service redesign. With othersub-contractors, the PCT would need towork closely with them to clarify minimumrequirements and acceptable servicemodels, and to ensure appropriateintegration with other service providers.
At the level of sub-PCT commissioning,therefore, there is significant potential foroverlap between the commissioning orpurchasing role, and that of the provider.This is not unusual or necessarilyproblematic, for in all systems that rely on apurchaser-provider arrangement, there is aneed for providers to have a role in servicedesign, and for commissioners to engage in,and sometime manage, how services areactually delivered. Where longer termservice delivery arrangements are needed(as they typically are in the NHS) andsignificant competition to existing providersmay be constrained (as it is in the NHS giventhe political reality of needing to preservelarge elements of local health provision forthe benefit of the population), thedevelopment of more mature (and complex)commissioner-provider arrangements is bothlikely and desirable, as long as thenecessary governance framework is put inplace to mitigate against conflicts of interest.
However, there is a question mark here asto what this framework might look like in thecase of practice based commissioners. Inthe preceding paragraphs, we havereferred to them as ‘sub-contracted’commissioners, accountable to the PCT. Yettheir entitlement within current policy toinfluence the PCT’s commissioning decisionsmeans that they have in fact been given arole as commissioning decision-makerswithin the process to which they areaccountable as providers. This places themin a less clear position in comparison withother providers and sub-contractors, raisingimportant and complex questions ofgovernance, which are explored furtherbelow, and in section 3.
Commissioning in the reformed NHS: policy into practice 9

Procurement and Contracting
As in the case of information collection andanalysis, practice based commissioningguidelines require that responsibilities forprocurement and contracting (alsopresented here as ‘brain’ activities) must beretained at the PCT level, and should not becarried out directly by practices. Thesefunctions include developing servicespecifications, advertising contracts,deciding between different potentialproviders, and agreeing contractual andperformance management arrangements.With an increasingly pluralistic ‘supply side’that is likely to include a growing number ofnon-NHS providers, these more technicalaspects of commissioning will often involveformal competitive tendering procedures,and the negotiation and monitoring of legallybinding contracts (rather than serviceagreements).
Again, combining some of these functionsacross a number of PCTs will beappropriate, and potentially more efficient.In cases where PCTs have an establishedhistory of working in a collaborative mannerto support their commissioning activity, suchextended forms of aggregated arrangementare already being developed in the light ofCPLNHS. One such example is theAssociation of Greater Manchester PrimaryCare Trusts’ planned ‘commissioningbusiness service’, details of which are setout in the box below.
PCT commissioning functions –summary
In summary, it is clear is that the new PCT isthe overall accountable local body in respectof what international colleagues know asstrategic purchasing, and what is currentlyunderstood as ‘effective commissioning’ inthe English NHS. The extent to which anindividual PCT carries out ‘conscience’,‘eyes and ears’, and ‘brain’ functions itself,or delegates these upwards, outwards ordownwards to another agency is for thePCT to decide. The actual localcommissioning configuration will and shouldvary, but what is not negotiable is that a PCTshould stand to account for how citizens’health care resources are spent and thedegree to which local people’s healthoutcomes change as a result of thosecommissioning decision.
Case study: Greater Manchester Commissioning Business ServiceThe Commissioning Business Service (CBS) is a new venture developed by the 14Greater Manchester primary care trusts (PCTs). The CBS has as its mission thesourcing, procurement and contract-management of the delivery of quality and cost-effective services. It will provide a service to PCTs, practice based commissioners,local authorities, collaborative commissioners, and even providers who sub-contractservices. CBS services will include: the provision of off the shelf or bespoke servicespecifications; a detailed directory of providers and services; public health andcomparative clinical data and intelligence; and the full range of operational contractmanagement including contract compliance and resource utilisation analysis. The CBSis planned to become operational in April 2006 and is currently working on businessmodelling, the development of memoranda of information for each of its business areas,due diligence, the seeking of expressions of interest in providing CBS services, and thedetailed design of the organisational model.
Contact: Mike Asher, Project Director - [email protected] 07767-758353
Practice based commissioningfunctions
Practice based commissioning (PBC) is thesecond major plank of the government’spolicy focused on developing more effectivecommissioning in the NHS. It entails theallocation of an indicative budget to apractice or group of practices, this budgetbeing intended for the commissioning(design, planning, funding) of a specific setof services as agreed with the PCT. In thisway, practice based commissioning is asystem of devolved micro-purchasers,nested within the overall responsibility andaccountability of the PCT. As discussedabove, guidance makes it clear that the PCTis the ‘sovereign’ commissioner within localhealth systems, being the holder ofcontracts with providers and the ultimateaccountable body. In this way, practice-based commissioning differs markedly fromGP fundholding of the 1990s, where GPmicro-purchasers held budgets that theyused to place direct contracts withproviders. It is the governance of practicebased commissioning, and its clear locationwithin a statutory NHS commissioning body,that marks it out from GP fundholding, andthis dimension is thus reflected in ouranalysis of practice based commissioningfunctions. Practice based commissionersare largely responsible for assuming someof the ‘brain’ and many of the ‘eyes andears’ functions as set out in figure 3. Thus,the design of local services (with clinicaland user input), the implementation of patientchoice and the management of demand forservices are core functions for practicebased commissioning.
Service planning and design
As discussed above, while PCTs will retainresponsibility for collating and processingroutine data relating to population healthneeds, service utilisation and costs, a greatdeal of the information required to informeffective commissioning is obtained and heldat practice level. Such information includesclinical data stored within practices’ patientrecords, as well as evidence of servicequality and outcomes obtained from patients’accounts, and/or the practice team’s ownexperience of dealing with particular serviceproviders.
In addition to this ‘front-line’ feedbackmechanism, primary care professionals ofcourse bring their clinical experience andexpertise to assessments of theappropriateness, safety, and efficacy ofvarious service models. In many cases,they also bring the pragmatism,entrepreneurialism and ‘commercial’ acumengained through running their own smallbusinesses. Practice based commissionerstherefore have a crucial role in assessingpatients’ needs and experiences of care,and in analysing data about services costsand outcomes, in order to inform futureservice design and purchasing.
Practice-based commissioners caninfluence service models in several differentways:
i) through reviewing their own approach toprescribing and managing care
ii) through using their influence and‘purchasing power’ to encouragechanges in the pattern or quality ofservices offered by other providers
iii) through extending their own role inservice provision
10 Commissioning in the reformed NHS: policy into practice

Prescribing and managing care
Practice based commissioners are, first andforemost, primary care professionals. Assuch, their fundamental roles are those ofthe diagnostician, prescriber of care, andco-ordinator of services for patients. Theseroles have been traditionally regarded as thebedrock of NHS primary care, and a featureof the health system that is envied by manyinternational commentators (Starfield, 1998;Wilson et al, 2005). For PCTs facing apressing need to reduce unscheduledadmissions to hospital, deliver moreeffective management of chronic disease,and keep local health care budgets undercontrol, this care management and ‘gate-keeping’ role assumes even greaterimportance. PCTs require strong andeffective care managers who will assessneed and make appropriate decisions aboutthe care of individuals, but with reference towider system objectives and availableresources.
For practice-based commissioners theincentive to review approaches to gate-keeping and co-ordination now lies with thepotential to re-invest any resources savedthrough ‘tighter’ care management (forexample, through reducing avoidableadmissions by identifying and monitoringpatients who are heavy users of services,and proactively intervening to avoidpredictable deterioration of their condition).
Of course, GPs who choose not to respondto these incentives, and decline to take onan indicative budget, still make decisionsimpacting on the utilisation of resources inother parts of the health care system. Inthis sense, it could be argued that all GPsand their teams are involved in practice-based commissioning, whether explicitly ornot. This raises the question of whetherpractice-based commissioning shouldtherefore be treated as a core function ofgeneral practice, an issue which isdiscussed in more detail below, and insection 3. The point here is that thetraditional care-management andcoordination role of general practice is itselfone element of the practice-basedcommissioning process.
A new aspect of the care management roleis introduced by the principle and practice of‘patient choice.’ With patients requiring asecondary referral now having the rightboth to be offered a selection of possibleservice providers, and ultimately to book aconvenient appointment from the surgery,practices have a number of new (and/or
extended) roles. These include theadministrative tasks associated withappointment bookings, as well as theextension of the consultation process toinclude what is likely to be a more detaileddiscussion of the referral and treatmentoptions than has often taken place in thepast. This transition in the role of primarycare practitioner from ‘decision-maker’ to‘advisor’ may not be a dramatic revolution.Many practitioners already approach thetask in this way, of course, while manypatients are likely to continue to rely heavilyon professionals when exercising their rightto ‘choose’. However, forthcoming researchinto the patient choice commissioned by theDepartment of Health apparently suggeststhat patients do often make choices whichare opposed to what their GPsrecommended (Lloyd, 2006), and this is anexperience that seems likely to becomemore common as more people becomeaware of their rights and options. The roleof care management in the context of amore empowered and informed patientpopulation may well require newapproaches to consultation and decision-making at a practitioner and practice level.
The status of ‘patient choice’ also needs tobe considered carefully by PCTs in the caseof a practice based commissioner actingboth as care-manager and, potentially, asthe provider of ‘extended’ primary care (seebelow). As distinctions between secondarycare and ‘enhanced primary care’ becomeincreasingly blurred, it is not entirely clearwhether (and at what point) patients mustbe offered choice between their ownpractice and other alternative providers of‘specialist’ primary care services. Thissituation will need to be closely monitoredand reviewed by PCTs.
A final but critical point to note here is thatmany primary care professionals other thanGPs have care management and/or ‘gate-keeping’ roles and, according to the analysisabove, are therefore involved in some wayin the commissioning process. Manycommunity nurses, social workers,therapists and other allied healthprofessionals make decisions about thepackages of care required by patients, andabout access to secondary care services(e.g. in the case of physiotherapist triage oforthopaedic referrals). The currentresearch suggests that clarification of therelationships between these care managersand practice-based budget holders is at anearly stage. In some circumstances, therelationship may be seen as a partnershipwithin an ‘extended’ practice-based
commissioning team, while in others certaincare-management functions may be ‘sub-contracted’ to other professionals bypractice-based commissioners. Given theknowledge, skills and experience of theseprofessionals, and their potentialcontribution to demand management andservice redesign, this is clearly an issue thatrequires some further consideration anddevelopment.
Influencing other service providers
As well as reviewing their own role inmanaging demand, practice-basedcommissioners will also play a part inprompting other providers to improve thequality and responsiveness of theirservices. With their critical position insupporting (and undoubtedly influencing)patient choice, and increasing flexibility toidentify alternative providers if not satisfiedwith existing options, practice-basedcommissioners should be well placed innegotiations with NHS trusts, foundationtrusts and other providers over the qualityand range of services they wish to seeprovided. This function is likely to becarried out in partnerships with otherpractice-based commissioners, andsupported by PCT commissioning managers.
Extending service provision
In many situations, it is likely that in planningand redesigning services, practice-basedcommissioners will seek to identify elementsof care pathways that can be shifted out ofsecondary care and provided instead bythemselves, or by other primary care basedcolleagues. Indeed, anecdotal evidencesuggests that it is this aspect of the initiative(rather than opportunities to changepatterns of delivery of more specialistservices) that is proving most attractive tothose practices actively engaging in practicebased commissioning.
This trend supports the current policy todevelop care outside hospitals. However(as referred to on a number of occasionsabove), it all also creates certain theoreticaland practical problems for the operation andgovernance of practice basedcommissioning, due to the status of practicebased commissioners as bothcommissioners and providers.
In attempting to resolve this conflation, itcould be suggested that ‘practice basedcommissioning’ is not an accurate term forwhat is actually being expected of practicesas they assume a budget on behalf of their
Commissioning in the reformed NHS: policy into practice 11

local population. Instead, the requirementthat practices assess and review their ownprescribing, referral and activity data as aprerequisite to designing new forms of localservice delivered via a budget delegatedfrom the PCT, could be interpreted as anextension of the core primary care servicesthat PCTs commission from practices. Inother words, the PCT is in a sensecommissioning extended provision ofprimary and intermediate care frompractices and localities, within a frameworkof closer review and scrutiny of currentpractice, and with financial incentives todesign and deliver (directly or via otherproviders) new services.
This interpretation of practice basedcommissioning as a form of extendedprimary and intermediate care provision islent further weight by the emergence ofnew practice-led provider organisations thatare seeking to assume practice basedcommissioning budgets in tandem withsetting up new organisations for deliveringextended care to local people, and by theintroduction of a practice basedcommissioning Directed Enhanced Service(a provision whereby PBC is funded as aservice delivered by a practice to a PCT).
Regarding practice based commissioning asa form of extended care provision offersinsights into how this activity might beappropriately governed, and might be helpfulin encouraging GPs and other primary careprofessionals to assume a local budget.Arguably, the extension of primary careprovision is crucial to any subsequentredesign of intermediate and unscheduledcare, and the shift of services from hospitalto community settings. Thus the capacityfor PCTs to commission extended primarycare within a wider framework of serviceredesign, would seem to make sense.
Strategic Planning and objectivesetting
Our analysis of commissioning functionssuggests that the ‘conscience’ functions (asarticulated here) are much less amenable todelegation to practice based commissionersthan those of the ‘eyes and ears’ and the‘brain’. This reflects the tensions between‘population-based’ and ‘patient-focussed’commissioning identified under previousmodels of primary-care led commissioningand, again, is complicated by the dual role ofpractice based commissioners as providersof primary care and purchasers/designersof other care on behalf of the PCT. It ishowever likely that a PCT would involve
Case study – an extended practice provider organisationSmethwick Pathfinder operates under a legal joint venture agreement between twopractices in Smethwick (a town within Sandwell PCTs) covering a population of approx19,000. Since being established as a first wave personal wave medical services(PMS) pilot the Pathfinder has used their PMS plus contract to increase the servicesthey provide locally to their patients, transferring care from the acute sector into localsettings. This includes establishing pain relief clinics, developing a joint service withsecondary care specialists and primary care staff to implement a locally based carepathway for their diabetic patients, and developing on-site orthopaedic servicesproviding consultant input, osteopathy and physiotherapy. The organisation now wantsto extend its service redesign activity and is establishing a commissioning cluster oflocal practices with a responsibility for 70,000 patients. The cluster is currently workingwith its local PCT to identify the indicative global budget and has begun analysingreferral and activity data in order to identify priorities for a 3-year business plan. Thenew venture expects to develop services and facilities that allow patients to receivenon-acute care within a variety of local settings, working in partnership with secondarycare professionals to provide integrated pathways of care.
Contact: Stuart Tilsley, [email protected]
practice based commissioners indischarging their ‘collective conscience’functions. This might take the form ofengaging a locality or practice in theprocess of reviewing and setting overalllocal health system objectives, representingthe PCT in a commissioning network orpartnership, working on the process ofsetting minimum standards of care for aparticular service, or working with the PCTon public health activities aimed at changingoverall patterns of need.
Summary – practice basedcommissioning functions
In conclusion, practice based commissioningfunctions will be largely concerned withreview of current service provision andreferral patterns, design of appropriate carepathways and services to meet assessedneeds, and co-purchasing of such carepathways with PCT commissioners. Thepractice based commissioner brings‘brainpower’, closeness to the patientexperience, and clinical insight to theprocess of meso-level purchasing for alocal population. Its role rests fundamentallyon the role of the GP or other primary carepractitioner as care manager and allocatorof resource for people’s care. In exercisingthese functions, the practice basedcommissioner is likely to seek to extendprimary and intermediate care provision, andmay take on some of that extended rolewithin their own practice. Practice basedcommissioning cannot, in the current policyand governance frameworks, stand aloneor aside from the commissioning carried outby PCTs acting as ‘NHS Local’. Instead,
practice based commissioning offers anadditional dimension to the expanded PCTcommissioning framework, and requires amore sophisticated governancearrangement that can both assure publicaccountability for the use of resource andregulate potential conflicts of interest withincommissioning.
Conclusion – commissioningfunctionsIt is clear that the overall commissioning taskis greater than ever before, and that it isbeing relied upon by policy makers toimprove health and health services, assurequality, and deliver value for money in anNHS that is under significant public scrutiny.In this context, it is of crucial importance thateach PCT develops the appropriatearchitecture for carrying out itscommissioning functions. This section hasidentified the nature of the commissioningtask in relation to ‘conscience’, ‘brain’ and‘eyes and ears’ functions, and has exploredwhat activities will fall to PCTs and practicebased commissioners. In the next section,we consider the models of governanceneeded for the delivery of commissioning byPCTs beyond 2006, before going on toexplore what skills will be required in orderto make ‘stronger commissioning’ a reality asenvisaged in Commissioning a Patient-LedNHS.
12 Commissioning in the reformed NHS: policy into practice

3. Governing commissioning
We have discussed so far the objectivesand content of the current health systemreforms, and the functions or activities thatwill be involved in implementing them. Thethird element of the policy process is thegovernance of the system. Oneinterpretation of the nature of governance inhealth care organisations that this researchteam has found helpful is that set out byContandriopoulos et al (2004) who contendthat governance is related to problems:
of securing convergence or agreementon a programme of action among adiversity of actors and organisations;of redistributing power in anorganisational or social field that ischaracterised by a high level ofheterogeneity; andof gaining sufficient legitimacy to act in thename of the collectivity.
The above categorisation of governanceunderlines the importance of the threegroups of commissioning functions that weidentified earlier in the this report: the ‘brain’(redistributing power); ‘eyes and ears’(securing agreement from a range ofsources); and the ‘conscience’ (gaininglegitimacy in the name of the collectivity).
In the light of the White Paper on communityhealth services (Department of Health,2006a), there is clearly a need for PCTs todesign systems of governance that enablevarious forms of intelligence (as generatedby the ‘eyes and ears’ functions) to bebrought together and reconciled in an openand transparent way (that equates to the‘conscience’). The CPLNHS reorganisationis not therefore a simple ‘shuffling of thedeckchairs’ on board the NHS ship, it isconcerned with an expansion in thecommissioning function, and with creatingprocesses of governance that enable PCTsto act as truly legitimate and sovereign ‘NHSLocal’ organisations.
The commissioning governance ‘web’Figure 4 (p.14) sets out a possiblerepresentation of the network or ‘web’ ofrelationships that will exist within the healthsystem following the implementation ofCPLNHS. It attempts to demonstrate thechains of accountability for commissioningand service delivery, not for every form oforganisational interaction. It does notinclude, for example, the requirement forprovider organisations to account directly totheir patients, e.g. in dealing with complaints,
or to independent regulators, e.g. Monitorand the Healthcare Commission, for theirstandards of safety, clinical and corporategovernance.
Figure 4 demonstrates that future PCT andpractice based commissioners will be at theheart of a complex web of different types ofinteraction with other constituents of thehealth system, namely in different elementsof governance. Some of these relationshipswill be statutory or contractual in nature, forexample in the case of a legally bindingcontract between a PCT and anindependent sector provider for the deliveryof specific health services. In other cases,such as the relationship of NHS trusts topractice based commissioners,accountability is implicit, but not direct,(because the contractual relationship will bebetween the PCT and trust). A furthercategory of relationship does not involve ahierarchy of accountability at all, but ratherconstitutes a partnership betweencommissioning and planning bodies (such aswithin local strategic partnerships),designed to deliver a common health orsocial objective. The level of complexity ofthe relationships between these parties alsovaries, from the relatively straight-forwardrequirement for PCTs to account to theirstrategic health authority for theircommissioning performance, to whatcurrently appear to be highly complex andintertwined relationships between PCTs andpractice based commissioners, involvingboth contractual and indirectaccountabilities, as well as ‘partnership’working.
External regulation of thecommissioning function
One important aspect of governance withinthe new system will be external regulationof the commissioning function. In a systemin which the PCT is the ‘sovereign’commissioner, and where more providerswill be moving ‘beyond the reaches of state-directed performance management’ (Dixon,2005, p.9), commissioners will increasinglyfind themselves the focus of scrutiny andregulation, possibly from a new orreconstituted body established to undertakethis task. However, pertinent issuesregarding regulation of the new system arediscussed in detail elsewhere (see Dixon,2005) and, while PCTs clearly have a role ininfluencing national policy, they will notimmediately be responsible for this elementof the reforms. The focus here is thereforeon the governance mechanisms required atthe level of PCT and practice-based
commissioning, and not on the widerregulation of commissioning.
The PCT as ‘sovereign’ in the localhealth system
It was suggested above that a critical test ofthe new system will be the extent to whichcommissioning organisations, having beenpositioned as the accountable bodies withintheir local health care communities, are infact recognised as its ‘sovereign’ decision-makers and leaders. It is clear that this willnot happen immediately. The operatingguidelines for the NHS in 2006/07acknowledge the organisational disruption tocome, and place responsibility foroverseeing reconfiguration and assuringbusiness continuity with strategic healthauthorities and regional ‘transition leaders’.NHS trusts will continue to be directlyaccountable to strategic health authoritiesfor performance against targets and forfinancial stability, while PCTs will be requiredto lodge any commissioning reserves withthe strategic health authority for regionalbrokerage (Department of Health, 2006b).
In the medium term, however, the rationalefor the introduction of a market-basedsystem is that the market regulations andincentives will erode the need for directstate-driven performance management,facilitating a shift from a centrally driven, toa ‘self-improving’ system where the ‘NHSlocal’ PCT can be properly sovereign. Theextent to which PCTs and practice basedcommissioners will be left to manage thismarket at a local level will depend, largely,on the response of the Government to earlyfeedback. It is certainly possible that earlyhigh profile market failures, such as a GPpractice or a new private provider losingtheir NHS contract as a result of failing todeliver services to the requiredspecification, could trigger a retreat bypoliticians, whether due to real failure of thesystem, or to loss of nerve before ‘reformedcommissioning’ has been given time to takeroot.
Critical issues for the governance ofPCT commissioning
Assuming that the current programme ofsystems reform is maintained, perceptionsof commissioners’ ability to manage risk andcomplexity will play a large part in theGovernment’s assessment of the level oftrust and autonomy to grant them from 2008,when the reforms will have been fullyimplemented. It is suggested that there arefive critical issues to be considered
Commissioning in the reformed NHS: policy into practice 13

Figure 4: The commissioning governance ‘web’
carefully by commissioning bodies if thelegitimacy and credibility of their decision-making and governance regimes is to bewidely accepted:
i. Partnership relationships between PCTsand other commissioning/planningauthorities (including the local authorityand other PCTs)
ii. Market-based contractual relationshipsbetween PCTs and service providers
iii. Relationship between PCTs and practicebased commissioners
iv.The involvement of, and relationship to,patients and the public, includingconsideration of fundamentally differentforms of PCT governance
v. Professional advice and clinical leadership
Governing partnershipsWhatever the outcome of the currentconsultation on PCT (re)configuration, oneconclusion that seems inevitable is that newPCTs will be expected to work in closepartnership with other bodies to ensureoptimal integration and efficiency in theachievement of policy outcomes. Thisprinciple appears fundamental to the drive toachieve co-terminosity between PCTs andlocal authorities, and is emphasised in thewhite paper on community health servicesas a means of achieving well-being for localpopulations (Department of Health, 2006a).
Most of the respondents in this researchsupported the move towards PCT/localauthority co-terminosity as a positive orlogical development, specifically as a route
for focusing public health activity, and forsupporting joint commissioning and/orservice delivery. The anticipated need towork in partnership with neighbouring PCTsto achieve economies of scale and tostrengthen market power was alsofrequently referred to by those currentlyengaged in PCT development. Even wherePCTs expect (or hope) not to be merged inthe current round of reforms, they are stillanticipating greater sharing of resourceswith other organisations – confirming thefindings of the initial phase of this researchwhere interdependence was identified asthe defining element of PCT configuration(Peck and Freeman, 2005).
It might be assumed that extending orstrengthening partnerships following (or aspart of) reconfiguration would be relativelyuncontroversial. In terms of the principle,this may well be the case. However, inorder for such partnerships to deliver theiranticipated benefits their processes must berobust, and their structures sensitive to localrequirements. Three examples of ways inwhich PCTs have established arrangementsfor the governance of commissioningpartnerships, and some of the challengesthey face in managing these, are set out onthe following pages
These case studies, and other evidence onthe governance of partnerships (e.g. AuditCommission 2005), demonstrate that if PCTsare expecting to increase the extent towhich they are working with otherorganisations to deliver their commissioningfunctions, careful consideration must begiven to how these relationships aremanaged. They may even need to questionwhether a ‘partnership’ is in fact the mostappropriate model for stakeholderinteraction. It is possible, for example, thateven when working with another statutorybody, the most effective relationship toensure a particular outcome would be acontract (or service level agreement),through which one organisation is explicitlycommissioned to provide a service for(rather than with) others. An increase in theuse of the contract as a mechanism forinfluencing stakeholder behaviour is, ofcourse, becoming increasingly common asthe provider market is extended into theindependent sector.
Governing marketsAs we have seen, one of the of the keycomponents of the current system reformsis to increase the number and range ofhealth service suppliers, creating for thefirst time an extensive external health
Contracting/payment/ data processing agency
Patients
PCT/’NHS Local’/ Commissioning body
Local Authorities
Other PCTs Clinical
Networks Practice Based Commissioners (Primary Care
Medical Service Providers)
Strategic Health
Authority
Department of Health/Ministers
Public/ Taxpayer
Other Primary Care and
Community Health Service
Providers
PCT run Community
Health Services Providers
NHS and Mental Health
Trusts
Foundation Trusts
Contractual or performance management accountability
Non-contractual accountability
Partnership relationship
Independent Regulator
Independent Sector providers Voluntary
organisations
Public accountability
14 Commissioning in the reformed NHS: policy into practice

Case study: Hertfordshire Joint Commissioning Team (JCT)The Hertfordshire JCT was formed in 2002, and is responsible for commissioning drugand alcohol, adult learning disability, and mental health services on behalf ofHertfordshire County Council (HCC) and the 8 Hertfordshire primary care trusts(HPCTs). It is hosted by and operationally managed through the performance andcommissioning division of HCC’s adult care services department. The functions of theJCT go beyond transactional contracting tasks, and include strategic responsibilitiessuch as planning, service development, monitoring and performance management. Thehealth and social care economy’s commissioning expertise on these services istherefore concentrated within a single agency. Budgets are formally pooled under aSection 31 Agreement, and each partner then delegates commissioning responsibility toa joint commissioning partnership board, to which the JCT is accountable. The board ismade up of four members of the county council, and four PCT directors (eitherexecutive or non-executive). The rationale for the JCT is based on the view that thismodel is more effective than the council and each PCT discharging their functionsseparately. Some stakeholders see potential for extending the arrangements to includeintegrated commissioning of community services for older people. However, evenwithin this well-established arrangement, some of the common challenges ofpartnership working have been observed. These include:
the risk that the JCT might ‘lose touch’ with local needs, and with the needs ofindividual service users and carers, due to its size and centralised structure;
the range of partners and stakeholders involved means that reaching consensus isnot always straightforward, and the structure is ‘high-maintenance’;
value for money of the team, and accountability to PCTs for financial balance hasbeen questioned;
the complexity of the task and the knowledge, skills and resources required by theJCT may be underestimated by partner organisations, which then have unrealisticexpectations of the capacity and capability of the team;
the different decision-making procedures and organisational styles of the NHS andlocal authority can create tensions and imbalances in power relationships within thepartnership;
the role and responsibilities of individuals appointed to the partnership board (e.g.non-executive directors), and the knowledge and expertise required of them, maynot be clear; and
lack of involvement of some key partners (including service users and carers).
The Hertfordshire experience demonstrates that while strategic partnerships can bringmany advantages, there are also a range of risks involved. Partners need to dedicatetime to ensure these are addressed, and that appropriate risk-managementarrangements are in place.
Contact: Mark Jordan – Head of Joint Commissioning, Hertfordshire Joint CommissioningTeam - [email protected]
Case study: NorthumberlandCare TrustThe North of Tyne CommissioningConsortium (covering NorthumberlandCare Trust, North Tyneside PCT andNewcastle PCT) is responsible forcontracting with the major health careproviders in the region on behalf of thethree local commissioning bodies. Allactivities associated with contracting,invoicing, and monitoring are carried outby the consortium, which is staffed andhosted by Newcastle PCT. However,commissioning responsibility is nottransferred to the consortium. Thecare trust and PCTs continue toundertake needs assessment,decision-making and servicedevelopment work, but feed theoutcomes in to the consortium forimplementation at a contractual/operational level. Contracting withsmaller providers (including primarycare providers) is currently undertakenby the care trust and PCTs, whichmeans there is some duplication offunctions at commissioner andconsortium level in relation to invoicing/monitoring/reporting etc. Thesearrangements are being reviewed inthe context of PCT reconfiguration andit is anticipated that this joint working islikely to be extended in some way,whether through PCT mergers, orsharing of additional functions.
While demonstrating the possibilities ofeffective shared commissioningfunctions, this site also highlightspotential limits to the benefits ofaggregation. With responsibilities forcommissioning adult health and socialcare services, partnership workingwith the local authority is crucial forNorthumberland Care Trust, which hasworked hard with the local council toestablish strong, effective relationships.The care trust now faces tensions,therefore, between potentialefficiencies to be gained throughworking in partnership with other PCTs,and those advantages achieved thoughconcentrating on integration at a locallevel.
Contact: Sue Cornick, Head of Planningand Performance, Northumberland CareTrust [email protected]
service market, and as such makingcontestability ‘real’. It will fall to PCTs ascommissioners to shape and manage thismarket in the local situation, by designingand administering incentives that willmotivate providers to participate and interactin ways that deliver defined national andlocal objectives. There is an implicitassumption within such a policy that directcontrol and performance management willbecome less desirable and necessary, asthe system becomes self-regulating.
Learning from other sectors
Similar trends towards increasingcontestability and managing delivery throughcontracts are currently being observed inother sectors in the UK, including highereducation and criminal justice. Highereducation institutions operate with asignificant degree of autonomy from centralgovernment (certainly in comparison withthe NHS) and as such, it is down toindividual institutions to develop a model ofgovernance that makes sense in relation tooverall objectives and stakeholders. Apossible scenario being explored in some
Commissioning in the reformed NHS: policy into practice 15

Case study: Torbay Care Trust - Commissioning Partnerships for OlderPeople‘s ServicesTorbay Council Social Services and Torbay PCT have recently formed a new care trust,responsible for delivering health and social care services to adults. They have usedthis organisational restructuring as an opportunity to reconsider their entire approach tocommissioning services for older people, and have developed a commissioning strategythat aims to bring together commissioners, service users and service providers inpartnerships with mutual benefit. One of the principal intended results of the strategy isto empower service users, both in relation to securing services to meet their ownindividual needs, but also in making a real contribution as decision-makers in the overallplanning of local service provision. Options for allocating individual budgets are beingexplored to support the former objective, while proposed ‘commissioning partnerships’,involving community based organisations for older people and other representatives oflocal communities, are intended to place strategic decision-making in the hands of thosewho will use the services. The commissioning partnerships will be designed to involveall key stakeholders and, to reflect the specific needs of local areas, will be located ineach of the trust’s five ‘zones’ which are based on GP practice areas. Partnershipmeetings (alongside other communication mechanisms such as inter-/intranet sites) willprovide opportunities for users, carers, providers and the trust to work together inidentifying needs, agreeing preferred service delivery models, and setting serviceobjectives, minimum standards, and outcome measures. The partnerships will initiallywork with an ‘indicative’ financial allocation but, over time, may well take on the directmanagement of the older people’s commissioning budget for their locality. Followinginitial consultation, plans for establishing the partnerships are now being developed by agroup including a local clinician, service user, carer, councillor, service provider, andvoluntary sector representative. This group is clarifying the concept and purpose of thepartnerships and considering appropriate terms of reference, governance andmembership, as well as the likely training and development needs of their constituents.It is hoped that the first partnerships will be established from May 2006. Anticipatedchallenges are: ensuring that the partnerships have real influence over decision-makingand resource allocation (and are not just perceived as ‘talking shops’); and aligning ormaking mutually supportive links between the commissioning partnerships and practicebased commissioning groups
Contact: John Bryant – Head of Market Development, Torbay Care [email protected] or 07773 343743
higher education establishments is one inwhich the ‘core university’ is no longerseen as the provider of education, but hasas its primary role the commissioning ofcourses and programmes from individual/organisational providers working undercontract rather than tenure. The aim ofsuch an approach is to offer real choice tostudents by commissioning programmesthey want (not what academics want toteach) and by working in partnership withresearch funders to deliver research thatfunders require, while the key task of seniormanagers is to act as champions ofstakeholders (potential students, localcommunities, employers etc.) (McCaffrey,2004, p.53). Of particular relevance to theNHS of the ‘commissioning university’ modelis the fundamental rethinking of both thefunction and purpose of the core of theorganisation (University local, as per NHSlocal) and the renegotiation of the
relationship between providers and thecommissioning core. As with the NHS,universities rely on highly independentprofessionals to deliver their main business,and need to find approaches to governancethat satisfy the needs of both clients(students, research funders, employers)and professionals (academics as individualsand groups).
In another area of public life, that of themanagement of offenders, a commissioningapproach has similarly been implemented asa way of seeking to specify services in amore sophisticated manner, moreappropriately matching services to thedemands as expressed by the courtssystem and with a reduced reliance onproviders’ shaping of the market. Details ofhow the market for offender services isbeing governed are set out in the casestudy to the right.
Neither of these examples from othersectors is yet sufficiently well embedded tooffer an analysis of what their experiencesuggests for the most appropriate modes ofoperation for PCTs. Consequently, AsShapiro has pointed out, in discussing howthe new commissioning mechanisms willwork within a public service framework, “…we are moving into the realm of hypothesis”as, not only is this something new within theUK health care system but, to date, no othercountry seems “… to have genuinelycombined the rigour and equity of centralplanning with the freedom and innovation ofa real market economy” (2005, p.385).
Case study – National OffenderManagement ServiceIn 2003, a review of correctionalservices was commissioned in acontext of increasing use of prison andprobation services; increasing severityof sentencing practice (having a limitedimpact on rates of crime); improving butfragile public confidence in sentencing;and significant additional investment inprison and probation (Carter, 2003).The objective was to ensure that theadditional investment was being usedto best effect to reduce crime andmaintain public confidence. The reportrecommended that effectiveness andvalue for money could be improvedthrough introducing commissioning andcontestability, with greater use ofprivate and voluntary sector providers.The result was the establishment of aNational Offender Management Service,responsible for punishing offendersand reducing re-offending throughcommissioning a range of custodial andcommunity-based interventions. Tenregional offender managers now directwork in their regions to develop andintroduce the concept of offendermanagement. By 2006-2007 they will:hold the budgets for the probationareas and prisons in their regions;commission services from prisons andlocal probation boards and hold bothprisons and probation areas to accountfor their performance; and improveperformance by developingcontestability - allowing alternativeservice providers to compete for workso that regions obtain the best value formoney in managing offenders.
Contact:www.noms.homeoffice.gov.uk
16 Commissioning in the reformed NHS: policy into practice

Transaction costs
Where there is evidence on themanagement of markets in health care (albeitin a different context), it suggests thatrelationships based on contracts mayrequire a more ‘labour-intensive’ approach togovernance than that in ‘hierarchical’ or‘trust-based’ arrangements. This is becausemanaging the ‘imperfections’ in therelationship between purchasers andproviders and their associated risks,requires a proactive approach to marketstimulation and a high level of monitoring bythe commissioner. There are also hightransaction costs associated withcontracting, billing, payment etc.Consequently, despite the intended aim ofdriving down costs through competition,total system costs can actually be greater ina ‘market’.
Another issue that will have to be takenseriously by commissioners is the fact that,in an external market, relationships betweenstakeholders are governed by legal andtechnical frameworks (including, forexample, competition and contract law) thatwill have to be adhered to. Decision-makingprocesses and operating procedures willneed to take account of these, or be subjectto legal challenge. This context raises thebar in terms of the required capacity andskills of commissioners, who must developmarket management strategies that deal withthe prevailing system imperfections, andfollow due process, without creatingdisproportionate levels of bureaucracy andperformance management. These arediscussed further in section 4.
Governing practice basedcommissioningPractice based commissioning as a specificactivity has a clear defined accountabilitystructure, with the PCT being the formal andresponsible body that delegates budgetaryand service design activities to practices orgroups of practices. Contracts for servicesdesigned within practice basedcommissioning are signed by the PCT, andthe PCT is thus the formal contractor for allservices bought through practice basedcommissioning. The degree of attention thathas been attached to the accountabilityframework for practice basedcommissioning is in contrast to theexperience of GP fundholding in the 1990swhen an accountability framework wasonly put in place a few years after theinception of the scheme. There arehowever three areas where practice basedcommissioning poses a governancechallenge to PCTs:
i) there is a conflict of interest inherent inpractices’ role as both commissioner andprovider of services (where they mightwish to commission services from theirown practice);
ii) there is a lack of sanctions enabling PCTsto deal with poorly performing practice-based commissioners. Although practicebased commissioners could be strippedof their rights to commission if theyconsistently failed to deliver objectives,there is no direct mechanism for dealingwith inappropriate use of resourcesresulting from poor clinical practice (orfrom practices declining to take on acommissioning budget, and taking noresponsibility for the impact of their‘commissioning’ decisions in the firstplace);
iii) practice based commissioning calls intoquestion some of the ways in whichprimary care professionals havetraditionally been involved in providingclinical advice and planning expertise toPCTs.
In relation to the first issue of potentialconflicts of interest, the dual role ofpractices as providers and commissionerswill require PCTs to design and implementnew models of governance in order toassure probity and transparency in thedesign of services and placing of contracts.In doing this, PCTs will be able to draw onthe experience of previous approaches tohandling the placing of contracts withpractices for the development of premises,enhancing existing services, and agreeingand reviewing general/personal medicalservices contracts. As noted in section 2 itcould prove instructive to treat practicebased commissioning as a form of extendedprimary care provision in this regard. In sodoing, PCTs could adapt existinggovernance models developed in thecontext of contracting with providers.
As Lewis and Dixon (2005, p.19) havepreviously identified, this approach wouldalso help resolve the problems raised inpoint ii) above. If commissioningresponsibilities formed part of the corecontractual obligations of primary careproviders, and were “ …regulated throughgreater powers for PCTs in the giving andtaking away of contracts”, PCTs would havereal levers in the case of poor performanceor failure.
Finally, practice based commissioning callsinto question the model of the professionalexecutive committee (PEC) as the mainclinical advisory and planning forum for the
PCT. While certainly not exclusively thecase, many PECs have been chaired by andcomprised a majority of GPs. The potentialconflict inherent in this model is two-fold.Firstly, the GPs providing advice to the PCTabout planning and commissioning strategyare at the same time providers of servicesto the PCT under contract (and possibly viapractice based commissioning agreements)and may have a vested interest in thedevelopment or otherwise of certain localservices. Secondly, in an increasinglydiverse market of health care providers,there is a need to question what is specialabout NHS GPs or community staff asmembers of PEC. It can be argued that stafffrom other provider bodies, such as privateor third sector organisations, shouldlikewise be eligible to provide clinical input tothe PEC (or other forum for such advice.)
The area of clinical advice to PCTs clearlyrequires careful thought and planning bynew PCTs. Research evidence consistentlyunderlines the importance of effectiveclinical engagement in any primary care-ledcommissioning approach, and also points tothe tension that is frequently experiencedbetween clinical engagement on the onehand and managerial and publicaccountability on the other (Smith et al,2004). Thus the current dilemma facingPCTs as they seek to govern practice basedcommissioning in a way that does notcompromise clinical engagement (or evenbetter in a way that enhances suchinvolvement) is not of itself original, but inthe new context of NHS systems reforms,original solutions will be required (see belowfor further discussion).
Governing internal commissioner-provider relationshipsIt is important to note that just as the statusand relationships between thecommissioning and providing roles ofpractice-based commissioners must bemade more transparent, PCTs themselvesare going to have to similarly adopt a clearseparation (and ‘quasi-contractual’relationships) between in-house providerfunctions and their role as localcommissioner of community health services.In this respect, practice basedcommissioners and PCT providers need tobe treated on the same basis. A range ofmodels are emerging within PCTs inresponse to the steer in CPLNHS aboutseparating commissioning and providerfunctions within a PCT – two case studyexamples are set out overleaf.
Commissioning in the reformed NHS: policy into practice 17

Case study – Brighton and Hove PCTBrighton and Hove City Teaching PCT does not directly provide any services. For thosewith experience of working in the ‘traditional’ PCT model, the benefits of the Brightonarrangement come from the ability to really focus effort, skills and resources on thecommissioning task. In PCTs that provide services, the weight in staffing terms clearlysits within the service delivery directorates. Inevitably, therefore, while in terms of thetotal financial responsibilities of the PCT directly provided services represent a relativelysmall proportion of the risk, board members, senior managers and support staff can findthat they are dedicating a relatively large amount of time and energy to providerbusiness. This situation can frustrate a PCT’s attempts to align resources withpriorities. Brighton and Hove City Teaching PCT do not face this conflict, as all of thework carried out by its 155-160 strong staff is in relation to the role of the PCT as acommissioner. Their response to CPLNHS is therefore focussed on reviewing their‘fitness for purpose’ as a strong, lean commissioning body. Changes they are currentlyputting in place include merging public health functions with the council, aligning PCT andlocal authority commissioning much more closely, and establishing ‘virtual’ teams,consisting of commissioning, public health and finance staff, to support networks ofpractice-based commissioners at a locality level.
Contact: John James - Interim Chief Executive- [email protected]
Case study – Hounslow PCTOther PCTs, although not ‘pure’ commissioning bodies, had also taken steps towardsformally separating commissioning and provider functions some time before thepublication of CPLNHS. Hounslow PCT, for example, established an ‘arms-length’provider unit (using the SPMS contract as a model) in 2004, with responsibility forproviding a range of primary care services to the PCT (including the management of the7 PCT-run practices), and some community health services (including night nursing).While SPMS staff were still employed by the PCT, the body was developing its ownbusiness and service development strategy, which included plans for full independencefrom the PCT, and expansion of income generating activity (e.g. providing managementand clinical services to other PCTs). A ‘shadow’ service level agreement was beingdeveloped to set out the services and standards the PCT required the SPMS to deliver,with the expectation that this would be performance managed by the commissioningdirectorate along with all other contracts and SLAs. The SPMS encountered difficultiesin attempting to develop as an autonomous provider, while remaining formally subject tothe constraints and regulations of the PCT, but the publication of CPLNHS providedsupport for the direction of travel towards separation of commissioning and provision.The original business plan, which was originally due to be reviewed in 2006/07, is nowbeing re-evaluated in the context of the wider discussion of the future for primary careprovision.
Contact: Kirstie McLachlan, SPMS Project Director,[email protected]
There is UK and international evidence, forexample, that patients are more likely toaccept decisions to deny access to specifictreatments if the priority setting process isseen to be fair (Daniels and Sabin, 1998;Ham and Coulter, 2001). Thus, while callsfrom groups or individuals for centralintervention in PCT decision-making willnever be entirely eliminated, they might bereduced if there are effective systems foreducating the public about the need forpriority setting, and by involving them moreboldly in these processes.
Research evidence paints a gloomy picturein relation to the track record ofcommissioning organisations in assuring anydegree of strong accountability to localpopulations (Smith et al, 2004). Differentforms of NHS commissioning have sought toinvolve users and patients in their activitiesand decision making, yet these attempts arefrequently compromised by the centrallymanaged nature of the NHS andcommissioners’ sense of their accountabilityto the Department of Health in practice takingprecedence over their accountability to localpopulations (Dixon et al, 2001; Milewa et al,2003). A review of the experience of NHSprimary care-led commissioning concludedthat there was an inevitable trade-off to bemade between the managerial accountabilityof a statutory body and the degree offreedom to innovate and respond to localpublic and professional needs (Smith et al,2004). This experience underlines the needfor new PCTs to re-think carefully theirapproach to governance and to theinvolvement of the public in their decisionmaking processes, if they are not to repeatthe mistakes of the past, which in turnwould preclude the new PCTs frombecoming a real ‘NHS Local’.
The development of a sense of local‘community ownership’ of the commissioningbody is also important to the level of politicalsupport afforded to it and its decisions –indeed, this is about creating the ‘NHSLocal’. Studies of social health insurancesystems in Europe confirm the importance ofsuch local ownership, demonstrating thathigh levels of support for insurance funds,and the ‘social capital’ vested in them, areassociated with their subsidiarity, andconnection with a particular history ortradition (e.g. employment or labourorganisations) (Chinitz et al, 2004). Whileoverall levels of support for the NHS arealso high in the UK, arguably, they have adifferent genesis, and are focussed on theidea of universal and consistent entitlement,
18 Commissioning in the reformed NHS: policy into practice
Involving patients and the public infundamentally different waysAs well as the direct relationships betweencommissioning bodies and their serviceproviders, the accountability of PCTs topatients, and the involvement of the public indecision-making, will be fundamentalelements of good governance withincommissioning. The importance of this isunderlined in the recent NHS white paper oncommunity health services that notes(Department of Health, 2006a, p157):
‘At the same time as giving peoplegreater choice and control over theservices they use, we also need toensure that everyone in society hasa voice that is heard. When peopleget involved and use their voice theycan shape improvements in provisionand contribute to greater fairness inservice use.’.
Effective public involvement will be key togaining legitimacy and support for the PCTas the local NHS.

rather than on identification with a localbody and decision makers. On this basis,the suggestion that the PCT should become‘NHS Local’ seems both appropriate andessential, if the PCT is to be able to makeeffective and legitimate local funding andservice planning decisions.
Debate on the appropriate involvement ofthe public in public-service governance hastended to distinguish between two levels ofengagement: that of choice (betweenpersonal options) and voice (in influencingcollective decisions) (e.g. House ofCommons, 2005). In the context of healthcare, the former is being addressed veryexplicitly through the Patient Choice policy,which gives individuals requiring a particularservice an opportunity for direct involvementin decision-making over their care options.As the roll-out of this system beyond pilotsites has been very recent, there is as yetlittle evidence against which to test eitherthe assumptions that patient choice willapply competitive pressure on providers andimprove patient satisfaction, or the concerns(discussed on p. 7), that that it couldincrease inequities in access experiencedby disadvantaged and vulnerable patients. Itis clear, however, that there will always becompromises to be made when balancingresponsibilities to both improve the health ofa population, and secure optimal servicesfor individual patients. In addition toindividual choice, then, involvement of thepublic and (perhaps in particular) groups orcommunities that are at risk and highlydependent on local services, must also takethe form of a collective voice at a morestrategic decision-making level.
Securing appropriate ‘voice’ within NHScommissioning post-CPLNHS requires theconsideration of a new approach to PCTgovernance, that is, of how PCTs canproperly act as and claim to be the ‘NHSLocal’. In statutory terms, the representationof the public in healthcare decision making iscurrently through the non-executivedirectors on the boards of PCTs, andthrough patient forums. The extent to whichthese are seen by the public as effectivemechanisms for exerting influence isextremely questionable, however, and toachieve a real and sustainable form ofpublic engagement, alternative models needto be explored.
There are already many examples ofstrategies and initiatives to involve the publicmore actively in PCT planning, from patientsurveys, citizen’s panels/juries, consultation
events and workshops, and service userrepresentation on commissioning or strategygroups. Again, however, we are proposingthat a more fundamental rethink of PCTgovernance is now required, beyond simplyseeking strategies for seeking people’sviews or responses to consultationexercises.
One possible model to consider here is thegovernance framework for NHS foundationtrusts. With the concept of public ‘members’electing governors of the organisation who,in turn, appoint the management board anddirectors, this arrangement could have thepotential to secure a closer relationshipbetween a local community and an NHSbody than any existing alternativemechanism.
It is acknowledged that the success of thisapproach in promoting meaningful publicengagement has yet to be seen, and thatthere is a degree of scepticism amongobservers that ‘members’ and ‘governors’will have any real influence or power.
However, the possibility of a similar systemapplied to commissioning organisations doeswarrant further consideration. While publicallegiance to and interest in NHSorganisations continues to centre aroundhospitals, public membership of acommissioning body is, arguably, far moremeaningful than membership of a foundationtrust (FT). It might be expected that theactive ‘constituency’ of an FT would bemade up largely of individuals connected insome way through their own, or a familymembers’ use of the services (andtherefore restricted to relatively smallnumbers, but not necessarily with ageographical focus). In contrast, almost allindividuals have some stake in “Our TownNHS” as the steward of all local health careresources.
PCTs with local governors elected by a‘membership’ of local people may be in abetter position to articulate this role, as wellas being able to make claims for greaterlegitimacy for their decision-making than iscurrently the case within corporate boardstructures (comprising executive directorsand non-executive members appointed bythe NHS Appointments Commission).
While the model may not translate directly,the FT membership system provides someuseful ideas for commissioners to consider.Likewise, there is learning to be gained fromthe experience of governing local strategic
partnerships, bodies that seek tocommission services on a joint basis forspecific communities and interest groups,and that include elected members of localauthorities, senior public officials, andcommunity interest groups within theirgoverning bodies. In some areas,community empowerment networks havebeen established as a means of co-ordinating community involvement in LSPs –this experience offers potential for thefuture role of PCT patients’ forums.
Finally, there may useful be examples fromother health care systems. Chinitz, et al(2004) make the interesting point, forexample, that competitive reforms inEuropean social health insurance systemsdo not appear to have diminished collectiveforms of member engagement ingovernance. Indeed, rather than leading toa greater exercise of ‘choice’ (or ‘exit’),competition between insurers appears tohave only encouraged the deployment ofvarious mechanisms for citizen involvement,and joint decision making betweenstakeholders.
Securing professional advice andclinical leadershipPCTs need effective methods of securingclinical advice into their overall developmentof strategy and a local health market. Localprimary care professionals, acting asProfessional Executive Committee (PEC)members, have generally been consideredby PCTs to be their most appropriate sourceof such advice (along with the input ofpublic health specialists). Under currentarrangements, members of PECs aretypically expected to undertake this clinicaladvisory role as representatives on PCTstrategy and planning groups. Practicebased commissioning is designed toincrease this type of input from primary careprofessionals, by re-engaging those whohave distanced themselves from PCTs inrecent years. However, there are somequestion marks emerging over the relianceon existing local primary care practitionersto fulfil this function.
As discussed above, the introduction ofpractice based commissioning createspotential conflicts of interest for practice-based staff (who may be involved incommissioning decisions about pathways ofcare in which they intend to participate asproviders), thereby impacting on their abilityto act as truly independent advisers.
Commissioning in the reformed NHS: policy into practice 19

This issue is not new to PCTs. There havealways been potential conflicts of interestwithin PEC arrangements, for examplewhere independent contractor membershave been involved in making decisionsabout how best to implement and monitor thenew medical, dental and communitypharmacy contracts to which they werethemselves subject. The point made here iscertainly not intended to suggest thatprimary care professionals can somehowno longer be trusted to act with probity andprofessionalism in such circumstances, orthat it is inappropriate for (potential) serviceproviders to ever be involved in servicedesign and planning.
However, in an increasingly open healthcare market, it will be important for PCTs tobe able to demonstrate the transparency oftheir decision-making processes, and themanner in which they select and regulateproviders. In some circumstances, this mayrequire a more arms-length relationshipbeing established between PCTs andexisting local practices.
The related point has also been made that, inan NHS with a greater plurality of providers,a wider range of clinicians (including thoseworking outside the traditional ‘NHS-family’ inthe private or ‘third’ sector) should have arole to play in working with PCTs to shape alocal market of care. While some otherindependent contractors (including dentists,pharmacists and optometrists) have taken avery active role in their local PCTs, this hasnot always been the case, with GPs andPCT-employed community staff forming theclinical majority on many PECs. Again, ifPCTs are to be seen to be offering a ‘levelplaying field’ for providers, they may need toconsider the place of other existing andpotential providers within their decision-making structures.
There is also a third, more practicalargument here, that primary careprofessionals have never in fact been wellplaced to advise on the commissioning ofspecialist services of which they have littleknowledge or experience, such as tertiarycancer care. Collectively, these issuesthrow into question current professionalexecutive committee arrangements forsecuring clinical advice and leadership.
However, as they attempt to capture andprocess the ‘facts and figures’ within a localhealth economy (that is, ensure their ‘eyesand ears’ function), PCTs will of coursecontinue to require expertise in interpreting
these data in the context of clinicians’understanding of patient needs, clinicaleffectiveness and professional behaviour.To some extent, this advice can be drawnfrom service providers, in the context ofmature commissioning relationships in whichpurchaser and provider work together toidentify good practice, and design innovativesolutions to shared problems. Advice onevidence-based practice will also continueto be produced and disseminated at anational level, and will be supplemented byanalysis from the public health networks.Commissioners will still require more specificand detailed clinical guidance on the natureof the local health market, however,including optimal ways of applying sanctionsand rewards, alongside the ability toappraise service options from aprofessional perspective.
Commissioning bodies may therefore needto consider alternative options for securingclinical expertise. This might include one ormore of the following:
establishing a restructured professionalexecutive committee - this may be basedon the idea of the ‘clinical executive’proposed by the NHS Alliance (NHSAlliance, 2006) developed further toconsider the eligibility for, role of andselection to this executive;contracting with clinicians outside thelocal health economy to provide advice onspecific service areas;developing secondment opportunities formanagers and clinicians from providerservices who wish to gain commissioningexpertise,the formal appointment of ‘clinicaladvisers’ in the way that many PCTscontract with dental, optometric andcommunity pharmacy advisors. UnlikePEC members, these individuals areusually professionals who work outsidethe PCT area, and who are contracted notto ‘represent’ their profession within thePCT decision-making process, but toprovide independent advice, and toundertake specific functions in relation tothe approval and monitoring ofindependent contractors. A similar systemcould be developed for other areas ofservice planning and monitoring wherebyexpertise is obtained from individualsindependent of the local market, but who,unlike an entirely independent consultant,are committed to an ongoing relationshipwith the commissioner.
The potential contribution of clinicalmanagers and practitioners currentlyworking within the provider directorates ofPCTs should also be considered here. Thefocus of these staff groups recently hasbeen on the implications of their potentialtransfer out of PCTs as providers in thefuture. However, there may be alternativeopportunities for some individuals to remainwithin commissioning PCTs, working in newroles as clinical/professional advisors.Again, however, such positions would bedifferent from that of current PEC nurse andtherapist members, as it would not be as a‘representative’ of a profession, but as anindividual contracted specifically to bringprofessional expertise to the commissioningprocess.
4. Developing commissioningcapacity
Clarity of purpose, alongside transparentand inclusive governance mechanisms, willbe critical in establishing the ‘sovereignty’ ofcommissioning bodies as the stewards oftheir local health systems. Ultimately,however, the credibility and effectivenessof commissioning organizations will hang noton the theoretical appropriateness of theirstructures, but on their actual ability todischarge their functions with expertise,judgment and confidence.
The successive reorganization ofcommissioning bodies since they were firstintroduced in the early 1990s has disruptedthe development of commissioning as aprofession or corporate function within theNHS. While a significant degree of expertisehas been developed over the past 15 years,individuals have been moved frequently andspread thinly around the system with littlecoherent succession planning. There havebeen few formal training and developmentprogrammes designed exclusively forcommissioning managers and clinicians; andlimited attention has been paid to developingthe infrastructure required to supportcommissioning work.
Given this context, PCT commissioningteams have risen admirably to thechallenges of their role and, as seen in theinitial phase of this research, have employeda variety of mechanisms to make best useof the scarce and dispersed resourcesavailable to them. However, with thespotlight now turned on their profession,questions about the underlying knowledge
20 Commissioning in the reformed NHS: policy into practice

and skills of commissioning teams havebeen brought into focus. Even where teamsare seen to be well developed, the reformprogramme presents commissioners with adirect challenge to ‘raise their game.’ AsLight points out (1998, p. 67), in the US,where healthcare purchasing has a muchlonger history, the importance of establishinghighly expert commissioning teams hasalready been recognized:
The best American commissioninggroups have concluded that healthcare is far more complicated topurchase than anything else …Their salary and bonus packagesare designed to attract the best andthe brightest. They require excellentdata systems analysts andprogrammers, clinicalepidemiologists, clinical managers,organizational experts, financialspecialists and legal advisers.
The importance of specialist knowledge andskills is also being highlighted in localgovernment in England, wherecommissioning and contracting aresomewhat more established than within theNHS. In a recent evaluation of localgovernment procurement, the mostcommonly cited obstacle to the local deliveryof national procurement strategy objectiveswas lack of staff ability (Hughes 2005). Ifsimilar conclusions are to be avoided infuture evaluations of NHS commissioning,enhancing both the breadth and the depth ofexpertise available to commissioning bodiesmust be seen as an early priority at anational and local level.
This fact has been acknowledged by theDepartment of Health, which hasannounced the launch of ‘flagship’organisational development programmes forPCTs and GP practices to support thegrowth of the skills and behaviours that willbe required as they take on their newcommissioning roles (Department of Health2005a, p.33). For any such programme tobe effective, it must be designed withreference to a well articulated idea of whatthose skills and behaviours will be. Thisfinal section sets out some of thecommissioning tasks that may change oremerge as a result of the current reforms,and the type of knowledge, skills andexpertise that commissioning organisationswill consequently require. Based on ouranalysis of commissioning functions andgovernance arrangements, the followingareas of organizational and individual
development emerge as priorities:
LeadershipData capture, processing and analysisProcurement and contractingMarketing and public relationsPublic engagement
The following sections discuss why theseskills are needed, and the extent to whichthey must be developed within thecommissioning organisations themselves, orcould be made available from externalsources.
LeadershipThe term ‘leadership’ is much used but oftenill-defined, both within and beyond the NHS.One useful conceptualization, however, is tomake the distinction between goodmanagement, as coordinating the effectiveapplication of proven solutions to knownproblems, and leadership, as building thecapacity for groups and individuals to “learntheir way out of problems that could nothave been predicted” (Day 2001, p.582).While all of the functions described abovewill obviously require excellent management,effective leadership, in this contextsupporting the emergence of new skills andprocesses while steering the systemthrough a period of profound and rapidchange and intense political scrutiny, will becritical if an actual ‘step-change’ inoutcomes is to be delivered.
This capacity to deal with change andcomplexity in a political environment will berequired not only from chief executives andboards, but must be a feature of theorganisation as a whole, including its fullrange of commissioners – directors,managers, analysts, planners, and practicebased commissioners. If the PCT is to beacknowledged as the embodiment of thelocal NHS, this leadership must be seen tobe provided by the clinicians and managerswhose accountability resides inside the NHShierarchy.
How to develop this form of leadershipwithin the commissioning function isperhaps the greatest development challengefacing new PCTs. The task to beundertaken by PCTs is at once larger andmore complex that in the past and, for manyindividuals working within them, requires acategorically different approach to thatdemanded by their current roles andresponsibilities. For example, a recentregional review of the future role ofDirectors of Nursing identified that, as the
focus of PCT work moves from provision tocommissioning, the role of nurse leadershipin these organisations will need to shift fromthat of managing and developing aworkforce, to one of influencing strategicchange through others (Renshaw, 2005). Aneed was identified for both structuredtraining and development in specific aspectsof commissioning, as well as individuallytailored skills development to support nurseleaders in making this shift.
In designing national programmes to supportthe strengthening of commissioning, it will beimportant for personal and leadershipdevelopment to be addressed alongsideimportant technical, analytical and planningskills.
Data capture, processing and analysisImproving the ability of commissioning bodiesto collate, analyse and interpret data will becritical to their success. Effective planning,decision-making, risk assessment andmonitoring are all dependent on theavailability of timely, accurate informationthat is understood by the organisation.Many of these data sources, skills and toolsare already available within PCTs, but thereis often a lack of capacity to make full use ofthe data in a manner that is timely andappropriate for commissioning decisions.
Since the introduction of Payment byResults, much has been learned about thecollection and validation of ‘hard’ referraland activity data from the secondary caresector, while the Quality and OutcomesFramework assessment process hasfocussed attention on the measurement ofboth clinical and organisational indicators inprimary care. Public health specialists andepidemiologists have expertise in projectingthe future disease burden and health profileof a population, while individuals involved inservice redesign and trained in the‘collaborative’ methodologies have anunderstanding of capacity and demandanalysis at the level of services orspecialities. Participants in ‘Evercare’ pilotsand similar schemes have also begun todevelop ways of using data to identify andmanage the care of individuals likely to befrequent users of services, usingtechniques and expertise drawn largelyfrom the United States.
It is becoming accepted within NHScommissioning that this type of detailed dataanalysis and modelling is an essentialprerequisite to effective service planningand resource allocation, as witnessed by
Commissioning in the reformed NHS: policy into practice 21

the recent release by the King’s Fund ofDepartment of Health-supported ‘Patients atRisk of Re-hospitalisation’ case finding tool(King’s Fund, 2006).
However, commentators continue tohighlight the fact that NHS commissioningorganisations are data-rich and information-poor, having relatively little capacity fortimely analysis and hence use of what areextensive data collection systems.
Some support to assess and improveinformation requirements is being developednationally. For example, the AuditCommission will be leading a Payment ByResults assurance programme in 2006,strengthening local arrangements formonitoring data and payments, and carryingout a series of random and targeted externalaudits of clinical coding and reporting. TheDepartment of Health has also developed atoolkit that allows the use of the nationalresource allocation formula to calculateindicative weighted capitation budgets atpractice level to support the implementationof practice based commissioning. A practicebased commissioning information template isalso being developed, to assist PCTs inproviding information to practices in aconsistent format (Department of Health,2006b).
However, responsibility for ensuring moresophisticated data capture, processing andanalysis will ultimately be at a local level.The risks to PCTs of miscalculating futurepressures on service utilisation takeplanning requirements beyond the broadassessment of future epidemiologicalprofiles, towards the actuarial modellingtechniques used by insurance companies toforecast demand and analyse risk. Thechallenge for new PCTs and practice basedcommissioners is how to choose theappropriate tools and expertise for serviceanalysis and planning in the local context,and to determine how best to source thatexpertise. Options include contracting witha private company for some or all of thisanalytical work (as in the North EasternDerbyshire PCT case study), trainingexisting staff in new techniques, developinga pooled central resource for such activitywith other PCTs (as in the Birmingham andthe Black country case study), or acombination of all three.
Procurement and ContractingAs noted in section 2, commissioning is aprocess involving a series of specificactivities, including needs assessment,service specification, procurement,purchasing, contracting, and monitoring.The relative importance and exact nature ofeach activity depends on the context inwhich they take place. For example, inEngland, where up to now commissioninghas occurred primarily within an internalNHS market with relatively limited choice ofproviders, there has been a greater role forpurchasing (buying or funding services inresponse to demand or usage), than forprocurement (stimulation and identificationof suppliers through advertising andcompetitive tendering). The policy contexthas also meant that contracting has involvedthe specification, negotiation and monitoringof service agreements rather than legallybinding contracts, and has taken placewithin short-term (annual) cycles. In somecases, particularly in relation to primary careproviders, the responsibility for securingservices has until recently hardly been seenas a commissioning function at all, given thelimited scope for performance managementand market-exit within the nationally agreedcontracts.
Consequently, current commissioningreforms, in particular the increasinginvolvement of the independent sector, aretaking NHS commissioners into new territory.Specific areas of procurement andcontracting where PCTs will require moreexpertise in future to deal with this include:marketing and market research; competitivetendering and contract law; supply-chainmanagement; and strategic commissioning.
i) Market Management: marketing, marketresearch and market developmentIn order to reap the anticipated benefits andminimise the potential risks of a morecompetitive market between providers,commissioners will need to learn how tomanage this market in line with theirorganisation’s interests. This will involvedeveloping a detailed understanding of theenvironment, and encouraging a range ofpotential suppliers to take an interest in thepublic service market place. Given thesometimes poor reputation of the statutorysector as a commissioner among ‘thirdsector’ providers, and the relatively limitedmarket capacity in some areas of provision,the latter objective cannot be taken forgranted, and may require sophisticatedmarket management skills. This will includemarketing the PCT itself as a commissioner.
Some techniques identified in local authorityprocurement include: publishing anddistributing a forward procurement plan;providing information about tenderopportunities on websites; holding seminarsto introduce potential providers to contractopportunities; and producing guidance andrunning training on ‘how to bid for Councilcontracts’ (Hughes 2005). The concept ofcommissioners ‘selling’ themselves asreliable, constructive, attractive tradingpartners in this way may be new to thoseworking in a PCT context, and will requireexpertise in advertising, communicationsand public relations management.
Commissioners will also need to undertake‘market research’, to ensure that theyunderstand the environment they areoperating in, and the degree of competitiveadvantage they hold (or otherwise). Thiswill inform both negotiating positions, andthe design of contracts. In particular,commissioners will need to think about howthey ‘package’ work, potentially movingaway from traditional service specifications,to ‘out-put based’ requirements, that do notassume a particular organisational orprofessional model of delivery.
Finally, in constrained markets,commissioners may need to engage incapacity building and market developmentactivities, proactively supporting providersto develop their services in line with thelocal commissioning strategies.
ii) Competitive tendering and contract lawIn a more open or external market, PCTs willincreasingly be subject to challenge if theirpurchasing processes are not transparentand in line with formal procedures.Commissioners must therefore be fullyconversant with, or have access toexpertise regarding, both their internalfinancial instructions, EU regulations onadvertising and awarding contracts, and thelegal framework of competition law.
Legally binding contracts entered into withindependent sector organisations create adifferent type of commissioning relationshipfrom that experienced with other NHSproviders. As well as emphasising theimportance of properly defined servicespecifications, this will have implications forrisk-management strategies, and couldimpact on the insurance and liability statusof the PCT. Similar issues have beenidentified by foundation trusts (FTs) which,although as providers rather thancommissioners, have also recently ventured
22 Commissioning in the reformed NHS: policy into practice

Case Study: Market Development in Torbay Care TrustTorbay Care Trust has established the position of Head of Market Development.The remit of this individual (who brings commercial sector experience of businessdevelopment) is to work with local providers in developing their capacity to delivermodern, high quality services that meet the needs of the population. The post-holderacts as a communications link between commissioners and providers, identifyingcommon challenges and objectives, and ensuring suppliers are involved in decisionsthat may influence future demand, so they can adapt accordingly. The aim is to removethe perception of adversarial contracting relationships and facilitate a move towardsmore mature, constructive partnerships. Over the next year, the care trust will beworking with local residential and domiciliary care services to develop and test outcomebased reimbursement mechanisms, that will encourage providers to focus on quality,and to develop innovate approaches to rehabilitation and intermediate care.
Contact: John Bryant – Head of Market Development (07773 343 743)
outside the boundaries of the internal NHSmarket and into a new legislative arena.The response of several FTs has been toestablish a company secretary role,equivalent to that seen within the privateand mutual sector (Foundation TrustNetwork, 2005). In some cases this hasbeen achieved through extending theresponsibilities of existing ‘corporate affairs’managers, but others have explicitly broughtin qualified individuals with experience in thebusiness sector. PCTs may want toconsider whether it is most cost effective todevelop equivalent roles for theirorganisations (given the wider remit of acompany secretary to support all aspects ofcorporate governance), to buy in legalexpertise, possibly as part of a broader‘procurement’ service, or even to employ asolicitor to work in behalf of a number ofPCTs. Either way, they will increasinglyrequire access to such expertise.
iii) Supply chain managementSupply chain management is a commonelement of procurement withinmanufacturing and production sectors, inwhich many large global companies such asFord and IBM no longer operate asintegrated production systems, but insteadeffectively provide the ‘control centre’ for anetwork of suppliers contributing todevelopment of their products (Departmentof Trade and Industry, 1998). As discussedearlier, it is not yet clear how practice basedcommissioners will be positioned on thecommissioner/provider spectrum, nor towhat extent they will be allowed tosubcontract services themselves.However, whether through contracting withpractice based commissioners, dealing withlarge companies operating on a franchisebasis, or purchasing from NHS trustsworking in partnership with the independent
sector to deliver additional diagnosticcapacity, PCTs are likely to find themselvesincreasingly distanced from the ‘productionprocess’, and taking on this ‘control centre’role in an increasingly diverse and externalmarket. Although more usually associatedwith physical supplies and logistics, supplychain management will become a criticalresponsibility for NHS commissioners. Anunderstanding of the theory and practice asapplied in other sectors will provideimportant insights for PCT commissioners.
iv) Strategic PartneringWhile the negotiation of service agreementswithin the NHS has been an annual eventdriven by the need for NHS bodies tobalance their books each year, ‘intelligent’commissioning in other sectors inincreasingly based on the development oflong-term, risk-sharing relationships withsuppliers and other partners. Mechanismsused by local authorities to support relationalcontracting, and to reduce the transaction-costs of a market-based system include theestablishment of:
approved lists and accreditation wherebypotential suppliers apply to become amember of the approved list. If they meetthe requirements of the list they are ableto bid for, or be offered work for as longas their approval remains valid;procurement compacts, for example withthe voluntary sector, where a frameworkfor the local role of the voluntary andcommunity sector in delivering publicservices is agreed, and procurementactivities take place within the context ofthat agreement; andframework agreements and ‘open’contracts, where the contractsnegotiated by one council are madeavailable to other organisations.
Arrangements such as these areincreasingly familiar in other sectors andwould seem to have relevance for thedevelopment of more effective andsophisticated commissioning in the NHS.PCTs will in future want to engage withsome providers in sustained and matureways, particularly those delivering complex,ongoing disease management programmes,and core local services such as accidentand emergency. The increasingindependence of providers from the NHS’sannual financial cycle, and consequentability to extend financial planning and risk-management strategies over a greaterperiod of time, will make it easier for them toenter into longer-term agreements. To takefull advantage of these opportunities,however, commissioners will need todevelop their own skills in long-term planningand management of contracts.
Once again, the type of expertise describedabove is certainly not entirely absent fromthe NHS. Many commissioning managers,particularly those involved in jointcommissioning with local authorities orspecialised commissioning for low-volume/high-need groups of patients, haveextensive experience of purchasing carefrom and contracting with the independentsector. Similarly, individuals employed inpurchasing and supplies departments will beskilled in the more technical aspects ofprocurement, and those involved in PFIprogrammes will be engaged in long-termstrategic relationships with independentsector partners. As in the case ofinformation specialists, however, suchexpertise may currently be fragmentedacross organisations and departments, andit will inevitably take some time for PCTs todevelop a coherent, effective procurementfunction, whether on a stand-alone orcollaborative (with other PCTs) basis.
External Communications: publicrelations and public engagementAs discussed above, establishing thelegitimacy of commissioning bodies as thelocal NHS may require the development ofnew forms of relationship and dialogue withthe local population.
Marketing and Public RelationsOne particular area where the nature of thiscommunication needs to be carefullyconsidered is in the provision of informationto patients in the context of Patient Choice.There are two critical issues here:
Commissioning in the reformed NHS: policy into practice 23

i) As ‘stewards’ of local public health, andwith a responsibility for reducing healthinequalities, PCTs must ensure that theoperation of Patient Choice does not work todisadvantage particular groups orindividuals. Farrington-Douglas and Allen(2005) argue that in order to avoid this,commissioners must provide (or commissionand regulate) effective information, supportand advocacy for individuals whenexercising choice, and engage withcommunities and service users tounderstand why particular choices aremade by patients.
ii) Under Patient Choice, PCTs and practicebased commissioners will not be able torigidly specify service options, yet will beresponsible for establishing strategiccommissioning relationships with providers.The information presented to patientsregarding their options, and the impact thishas on the choices they make, may becritically important to the ability ofcommissioners to manage and channeldemand in line with commissioningstrategies. Provider organisations,particularly foundation trusts, are alreadydeveloping marketing strategies.Commissioners will need not only to monitorsuch advertising by providers to ensure it isappropriate, but also to develop their owncommunication campaigns, potentially tocounteract the effects of advertising onpatient demand and acute activity levels.
For both reasons, PCTs will requireexpertise in consumer research, marketing,tailoring information to the needs of differentgroups and individuals, and public relations.The Department of Health is currentlyconsulting, and planning to produceguidance, on the regulation of marketingactivity carried out by service providers, toensue information they produce is fair andaccurate, and that their advertisingstrategies are in line with statutoryguidelines (Department of Health, 2006b).There is no reference to the marketingactivities of PCTs, but this may well beconsidered at a later stage, andcommissioners will need to be aware of anyrelevant protocols.
Public EngagementFinally, a related, but distinct set of skills willbe required in commissioners if they are tobe successful in establishing the PCT orcommissioning body as ‘the NHS Local’.Effectively co-ordinating meaningfulconsultation, engaging members of thepublic in the complexity of decision-making,
and encouraging active participation(potentially as ‘members’ of the PCT) insetting priorities and reviewing services willrequire individuals with charisma, politicalastuteness, and the ability to developnetworks across communities.
Summary – developingcommissioning capacityMany of the knowledge and skill setsidentified above as critical for newcommissioners are already available withinPCTs and other NHS organisations.However, harnessing these skills andapplying them to the commissioning tasksidentified above will require the redesign ofmany roles, and the development of staff.For example, primary care developmentteams, procurement and suppliesprofessionals, corporate affairs managers,modernisation facilitators, public healthspecialists, and clinical managers will allhave some of the expertise discussed here,but may never have seen their roles as partof a commissioning function.
An early priority for PCTs will therefore be tocarry out a detailed and sophisticated skillsaudit, mapping the knowledge and expertisethat exists among staff, establishing wheremajor skills gaps lie, and helping individualsto see how they might fit into newstructures and roles.
It has only been possible here to develop anoutline of the knowledge and skills set likelyto be required by PCT and practice basedcommissioners. There is clearly furtherwork required in some instances todetermine a detailed knowledge base andcompetency profile, but the framework setout above provides a basis for this task.
Where skills are not available and cannot bedeveloped in the timescales required, therewill be increasing examples of sharedarrangements across multiple agencies, andof contracting out of the NHS. There isevidence that interest from the independentsector in entering the market for providingcommissioning expertise, and theDepartment of Health is considering howthis can best be channelled (2005b). Whatis clear is that new PCTs will face asignificant challenge in relation to both thedesign of the local commissioningarchitecture (mapping functions toorganisations and roles) and then insecuring the necessary skills and expertiseto make the new system work in aneffective manner.
5. Conclusion: what needs to bedone to put policy intopractice?
It is clear that the overall commissioning taskfacing PCTs in 2006 has expanded beyondanything known to date. There is a greaterrange of functions to be performed and theexpectations on commissioners are higherthan ever before. In a more complex healthsystem, the PCT is being looked to as the‘sovereign’ local commissioner, and as suchneeds to become ‘NHS Local’, a strong,legitimate and recognised body that peopleconsider to be responsible for ‘their’ NHS.
The expanded commissioning taskcomprises three sets of functions that canbe considered within the metaphoricalframework of the ‘conscience’, ‘eyes andears’, and ‘brain’. This reflects the corefunctions of governance, data gathering andanalysis, and purchasing/procurement. ThePCT as sovereign local commissioner hasthe responsibility for deciding where tolocate the many different activities that fallinto the conscience, eyes and ears, andbrain categories. Some of these activitieswill be aggregated upwards to supra-PCTbodies, others will be contained within thePCT, and others will be sub-contracted topractice based commissioners or otherorganisations.
The PCT will however remain as the overallguardian of all commissioning activities in itslocal area, and hence will need to developstronger and more sophisticatedgovernance of the ‘web’ of accountabilityrelationships in the middle of which it findsitself. In developing governancearrangements, PCTs will need to givespecific consideration to how they willgovern partnerships (NHS, local authorityand other), markets (including therelationship with providers), theirrelationship with patients and the public, andthe securing of clinical advice andleadership. NHS commissioning has a poorrecord in relation to the involvement ofpatients and the public in decision making.New PCTs need to explore differentapproaches to developing strong localidentity and legitimacy if they are to avoidthe mistakes of the past, and becomecommissioning bodies that are respected ata local level and able to withstand centralpressures to alter decisions made locally.
Thus the current PCT stakeholder model of acorporate board taking advice from apatients’ forum is unlikely to be fit for
24 Commissioning in the reformed NHS: policy into practice

purpose in the reformed NHS if the PCT is tobe a strong and legitimate ‘NHS Local’.Other models of PCT governance need to beexplored as a matter of urgency and there isrelevant experience within the wider publicsector (e.g. local strategic partnerships andcommunity empowerment networks) andwithin health in foundation trusts. Likewise,practice based commissioning calls intoquestion current mechanisms for involvingGPs and other primary care professionals inPCT decision making and planning, and thereis a need for careful review of the role ofprofessional executive committees, and forconsideration to be given to additional andalternative models of gaining clinical adviceand input.
Practice based commissioning also calls fora more sophisticated approach to themonitoring and management of conflicts ofinterest at a practice level, and it might behelpful to consider practice basedcommissioning as a form of extendedservice provision in this regard.
In order to deliver the extended range ofcommissioning functions in a manner that isproperly governed and viewed as legitimateto local populations, there is a need for PCTsto undertake a detailed skills audit as animmediate priority. This should seek toidentify existing skills within PCT andpractice teams, gaps in the skill base, andplans for ensuring a proper skill base withinthe new commissioning arrangements. Thisis likely to involve a process of personal andorganisational development, accompaniedby sub-contracting areas of work tospecialist agencies, other PCTs, practicesand other providers.
NHS commissioning has been a largelyneglected and under-developed function todate, with few resources being targeted atthe development of clinical and managerialcapacity in this area, and little attention givento growing the next generation ofcommissioning specialists. The currentprocess of commissioning reform offers anunrivalled opportunity for detailed analysisof the commissioning task, how it can bemade real in practice, and to develop far-reaching plans to enhance the skills of thepeople charged with what is probably themost responsible of management activitieswith a health system. However, thechallenges of this task are not to beunderestimated, particularly in the context ofincreasing pressure on management andinfrastructure budgets. This researchseeks to add to the process of
understanding and developing thecommissioning function, and to offer insightsinto how those leading PCTs and practicebased commissioning might take the next
steps in addressing these challenges, anddelivering effective commissioning in thereformed NHS.
Summary of report conclusions
In 2006, PCTs face an expansion in the overall commissioning function.
The PCT will need to become ‘NHS Local’, a strong, legitimate and recognised bodythat people consider to be responsible for ‘their’ NHS.
The expanded commissioning task comprises three sets of functions that wedescribe as being the conscience, eyes and ears, and brain - this reflects corefunctions of governance, data gathering and analysis, and procurement.
The PCT is responsible for deciding where to locate these functions - some will beaggregated upwards to supra-PCT bodies, others will be contained within the PCT,and others will be sub-contracted to practice based commissioners or otherorganisations.
The PCT will be the overall guardian of local commissioning activities and hence willneed to develop stronger and more sophisticated governance of the ‘web’ ofaccountability relationships in the local health system.
PCTs will need to give specific consideration to how they will govern partnerships,markets, their relationship with patients and the public, and the securing of clinicaladvice and leadership.
The current PCT stakeholder model of a corporate board taking advice from apatients’ forum is unlikely to be fit for purpose in the reformed NHS.
Other models of PCT governance need to be explored as a matter of urgency andthere is relevant experience within the wider public sector and within NHS foundationtrusts.
Practice based commissioning calls into question current mechanisms for involvingclinicians in PCT decision making, and there is a need for careful review of the role ofprofessional executive committees, and for consideration to be given to additional andalternative models of gaining clinical advice and input.
Practice based commissioning calls for a more sophisticated approach to themonitoring and management of conflicts of interest at a practice level, and it might behelpful to consider practice based commissioning as a form of extended serviceprovision in this regard.
In order to deliver the extended range of commissioning functions in a manner that isproperly governed, there is a need for PCTs to undertake a detailed skills audit as animmediate priority.
This audit should seek to identify existing skills within PCT and practice teams, gaps inthe skill base, and plans for ensuring a proper skill base within the newcommissioning arrangements.
NHS commissioning has been a largely neglected and under-developed function todate, with little attention having been given to growing the next generation ofcommissioning specialists.
The current process of commissioning reform offers an unrivalled opportunity fordetailed analysis of the commissioning task and to develop far-reaching plans toenhance the skills of the people charged with what is probably the most responsibleof management activities with a health system.
Commissioning in the reformed NHS: policy into practice 25

References
Audit Commission (2005) GoverningPartnerships: Bridging the accountabilitygap, London, Audit Commission
Bramley-Harker E and Lewis D (2005)Commissioning in the NHS: challengesand opportunities, London, NERAEconomic Consulting
Carter, P (2003) Managing Offenders,Reducing Crime: A new approach, HomeOffice Strategy Unit
Chinitz, D, Wismar, M and le Pen, C (2004)“Governance and (self-) regulation insocial health insurance systems” in RBSaltman, R Busse and J Figueras [eds.]Social health insurance systems inwestern Europe, Maidenhead, OpenUniversity Press
Contandriopoulos D, Denis J-L, Langley Aand Valette A (2004) “Governancestructures and political processes in apublic system: lessons from Quebec”,Public Administration, vol.82, no.3,pp627-655
Daniels N and Sabin J (1998) “The ethics ofaccountability in managed care reform,”Health Affairs, vol 17, no.5, pp50-64
Day, D. (2001) “Leadership development: Areview in context” in LeadershipQuarterly, vol 11 no.4, pp.581-613
Department of Health (2000) The NHS Plan:a plan for investment, a plan for reform,London, Department of Health
Department of Health (2001) Shifting theBalance of Power, London, Department ofHealth
Department of Health (2005a)Commissioning a Patient Led NHS,London, Department of Health
Department of Health (2005b) Health reformin England: update and next steps,London, Department of Health
Department of Health (2006a) Our health,our care, our say: a new direction forcommunity services, London, Departmentof Health
Department of Health (2006b) The NHS inEngland: the operating framework for2006/7, Department of Health, London,Department of Health
Department of Trade and Industry (1998)How supply chain management works,Department of Trades and Industry.Available at: http://www.dti.gov.uk/energy/eid/publications.shtml
Dixon J (2005) Regulating Health Care: Theway forward, London, King’s Fund
Dixon J, Goodwin N and Mays N (2001)“Holding total purchasing pilots toaccount”, in N Mays, S Wyke, G Malbonand N Goodwin N [eds], The Purchasingof Health Care by Primary CareOrganisations. An Evaluation and Guideto Future Policy, Buckingham, OpenUniversity Press, pp 208-229
Dranove D, Kessler D, McClellan M andSatterthwaite M, (2003), “Is moreinformation better? The effects of reportcards on health care providers”, Journalof Political Economy, vol. 111 no. 3, pp555-588.
Farrington-Douglas, J. and Allen, J. (2005)Equitable Choices for Health, London,Institute for Public Policy Research
Foundation Trust Network (2005) Newvoices new accountabilities: A guide towider governance in foundation trusts,NHS Confederation
Ham C and Coulter A (2001) “Explicit andimplicit rationing: taking responsibility andavoiding blame for health care choices”,Journal of Health Services Research andPolicy, vol. 6 no.3, pp163-169
House of Commons (2005) Choice, Voiceand Public Services, London, House ofCommons
House of Commons (2006) Changes toPrimary Care Trusts, London, House ofCommons
Hughes M (2005) Evaluation of the localGovernment Procurement Agenda:Baseline Survey Report, London, ODPM
James, C, Dixon, M and Sobanja, M (2002),Re-focusing Commissioning for PrimaryCare Trusts: An NHS Alliance discussionpaper, Retford, NHS Alliance
King’s Fund (2006) Care for people withlong-term conditions receives boost withlatest tool to cut hospital admissions,press release, London, King’s Fund
Lewis, R and Dixon, J (2005) The Future ofPrimary Care: Meeting the Challenges ofthe New NHS Market, London, King’sFund
Light, D W (1998), Effective Commissioning:lessons from purchasing in Americanmanaged care, Office of HealthEconomics, London.
Lloyd, I. (2006) “Warning on choice ‘spin’”,Health Service Journal, 2nd March 2006
Lyons Inquiry into Local Government (2005)Lyons Inquiry into Local Government:Consultation and Interim Report,Norwich, HMSO
McCaffery P (2004) The Higher EducationManager’s Handbook, Abingdon: Oxon,RoutledgeFalmer
Milewa T, Harrison S and Dowswell G(2003) ‘Public Involvement and DemocraticAccountability in Primary CareOrganisations’, in B Dowling B and CGlendinning [eds], The New Primary Care:Modern, Dependable, Successful?, OpenUniversity Press, Maidenhead, pp 179-195
NHS Alliance (2006) The Future of ClinicalLeadership in Primary Care and PCTs,Retford, NHS Alliance
Ovretveit J (1995) Purchasing for health: amulti-disciplinary introduction to thetheory and practice of purchasing,Buckingham, Open University Press
Peck E and Freeman,T (2005) ReconfiguringPCTs: influences and options,Birmingham, Health Services ManagementCentre
Renshaw, C. (2005) Mapping Our Futures:The Role of Director of Nursing – A WestMidlands Wide Perspective –unpublished report, Birmingham and theBlack Country Strategic Health Authority
Robinson R, Jakubowski E and Figueras J(2005) “Organization of purchasing inEurope”, in J Figueras, R Robinson and EJakubowski [eds], Purchasing to improvehealth systems performance,Maidenhead, Open University Press,pp11-43
Shapiro J (2005) “Markets in heath care:taking the tiger by the tail?” in AustralianHealth Review, vol. 29, no.4, pp 383-385
Smith J and Goodwin N (2002) Developingeffective commissioning by primary caretrusts: lessons from the researchevidence, Birmingham, Health ServicesManagement Centre
Smith J, Mays N, Dixon J, Goodwin N, LewisR, McClelland S, Mcleod H and Wyke S(2004) A review of the effectiveness ofprimary-care led commissioning and itsplace in the UK NHS, London, HealthFoundation
Smith J and Mays N (2005) ‘Primary caretrusts: do they have a future?’ in BritishMedical Journal, vol. 331, pp 1156-1157
Starfield B (1998) Primary care: balancinghealth needs, services and technology,Oxford, Oxford University Press
Wilson T, Roland M and Ham C (2006) “Thecontribution of general practice and thegeneral practitioner to NHS patients”,Journal of the Royal Society of Medicine,vol. 99, pp24-28
Woodin, J. (forthcoming) “Health carecommissioning and contracting” in WalsheK and Smith J [eds], HealthcareManagement, Open University Press
26 Commissioning in the reformed NHS: policy into practice

Name Job Title Organisation
Bill Barker Chairman Wakefield West PCT
Will Blandamer Associate Director of Partnership
Association of Greater Manchester PCTs
Mike Chew Deputy Chief Executive Milton Keynes PCT
Andrew Coulson
Institute of Local Government Studies, University of Birmingha
Lucy Docherty Chair Fareham & Gosport PCT
Buzz Dodd Head of Commissioning Southampton City PCT
Alastair Gibbons Head of Adult Social Care Milton Keynes Council
Jeannette McMillan Clinical Services Director Mercury Health Limited
Martin McShane Chief Executive North Eastern Derbyshire PCT
Claire Molloy Director of Commissioning and Modernisation
Sandwell PCTs
Pauline Quan-Arrow Chairman Southampton City PCT
Nick Relph Chief Executive Thames Valley StHA
Jonathan Shapiro Chair Birmingham and Solihull Mental Health Trust
Robert Sloane
Leadership development lead
NHS Alliance
Michael Sobanja
Chief Executive NHS Alliance
Rita Symons Programme Lead for Choice
Birmingham and the Black Country Strategic Health Authority
Commissioning in the reformed NHS: policy into practice 27
Appendix A –attendees at research workshop
Appendix B –interviewees for research
Cynthia Bower – Managing Director, Birmingham and Black Country SHA
John Bryant – Head of Market Development, Torbay Care Trust
Sue Cornick - Head of Planning and Performance, Northumberland Care Trust
John James – Interim Chief Executive, Brighton and Hove City Teaching PCT
Paula Kerr - Non Executive Director, Bedfordshire and Hertfordshire Strategic HealthAuthority
Martin McShane - Chief Executive, North Eastern Derbyshire PCT
Claire Molloy – Director of Commissioning and Modernisation, Sandwell PCTs
Adrian Osbourne – Corporate Projects Manager, Hampshire and Isle of Wight SHA
Denise Radley - Assistant Director for Performance & Commissioning, HertfordshireCounty Council

Health Services Management Centre40 Edgbaston Park Road,Edgbaston, BirminghamB15 2RT, United Kingdom
www.hsmc.bham.ac.uk