Embed Size (px)
Citation preview

Cancer Program StandardsCommission on Cancer
2004


Cancer Program StandardsCommission on Cancer
2004

© 2003 American College of SurgeonsChicago, ILAll rights reserved
The American College of Surgeons does not warrant ormake any guarantees or assurances related to outcomes oftreatment provided by institutions that have cancerprograms approved by the Commission on Cancer.
The examples used herein are to be used as guidelines andare not wholly inclusive of all options.

DEDICATIONThis publication is dedicated to individual cancer program teammembers. Your participation in the Commission on Cancer ApprovalsProgram exemplifies a steadfast commitment to providing the bestcare possible for your cancer patients and members of your community.Your leadership and expertise contribute to the entire scope, organization,and performance of the cancer program. Your vision is a catalyst forcontinued growth and improvement to ensure the delivery of qualitycancer care.
iii

iv

v
DEDICATION ............................................................................................................ iii
FOREWORD ..............................................................................................................1
ACKNOWLEDGMENTS ..............................................................................................3
INTRODUCTION .................................................................................................. 5–14The Approvals Program .................................................................................................................... 5Eligibility .......................................................................................................................................... 5Cancer Program Category ................................................................................................................. 5The Survey Process ............................................................................................................................ 5The Survey Application Record (SAR) .............................................................................................. 6Documentation of Program Activity ................................................................................................. 6Payment of Survey Fee ...................................................................................................................... 8Guidelines for On-site Review ........................................................................................................... 8Cancer Program Standards Rating System ......................................................................................... 8Approval Awards ............................................................................................................................... 9Award Notification Process ............................................................................................................... 9The CoC Outstanding Achievement Award .................................................................................... 10The Postsurvey Evaluation .............................................................................................................. 10Guidelines for Merged or Network Programs .................................................................................. 10CoC Resources and Tools for Cancer Programs .............................................................................. 10
CHAPTER ONE—INSTITUTIONAL AND PROGRAMMATIC RESOURCES .............. 15–16Facility Accreditation ...................................................................................................................... 15
Standard 1.1 ............................................................................................................................. 15
CHAPTER TWO—CANCER COMMITTEE LEADERSHIP ........................................ 17–25Level of Responsibility and Accountability ...................................................................................... 17
Standard 2.1 ............................................................................................................................. 17Membership .................................................................................................................................... 17
Standard 2.2 ............................................................................................................................. 17Program Activity Coordinators ........................................................................................................ 19
Standard 2.3 ............................................................................................................................. 19Meeting Schedule ............................................................................................................................ 19
Standard 2.4 ............................................................................................................................. 19Duties and Responsibilities ............................................................................................................. 20
Standard 2.5–Standard 2.11 ..................................................................................................... 20
CHAPTER THREE—CANCER DATA MANAGEMENTAND CANCER REGISTRY OPERATIONS.............................................................. 27–33
Staff Qualifications .......................................................................................................................... 27Standard 3.1 ............................................................................................................................. 27
Data Collection ............................................................................................................................... 28Standard 3.2–Standard 3.5 ....................................................................................................... 28
Data Reporting ............................................................................................................................... 29Standard 3.6–Standard 3.7 ....................................................................................................... 29
Special Studies ................................................................................................................................. 30Standard 3.8 ............................................................................................................................. 30
TABLE OF CONTENTS

vi
CHAPTER FOUR—CLINICAL MANAGEMENT...................................................... 35–39Clinical Services .............................................................................................................................. 35Treatment Services .......................................................................................................................... 35
Standard 4.1–Standard 4.2 ....................................................................................................... 35Other Clinical Services .................................................................................................................... 36
Standard 4.3–Standard 4.7 ....................................................................................................... 36
CHAPTER FIVE—RESEARCH .............................................................................. 41–42Clinical Trial Information ............................................................................................................... 41
Standard 5.1 ............................................................................................................................. 41Clinical Trial Accrual ...................................................................................................................... 41
Standard 5.2 ............................................................................................................................. 41
CHAPTER SIX—COMMUNITY OUTREACH.......................................................... 43–44Supportive Services .......................................................................................................................... 43
Standard 6.1 ............................................................................................................................. 43Prevention and Early Detection Programs ....................................................................................... 43
Standard 6.2 ............................................................................................................................. 43Monitoring Community Outreach .................................................................................................. 44
Standard 6.3 ............................................................................................................................. 44
CHAPTER SEVEN—PROFESSIONAL EDUCATION AND STAFF SUPPORT...................45Facility-based Education ................................................................................................................. 45
Standard 7.1 ............................................................................................................................. 45Cancer Registry Staff Education ...................................................................................................... 45
Standard 7.2 ............................................................................................................................. 45
CHAPTER EIGHT—QUALITY IMPROVEMENT ..................................................... 47–49Studies of Quality and Outcomes .................................................................................................... 47
Standard 8.1 ............................................................................................................................. 47Patient Care Improvement .............................................................................................................. 48
Standard 8.2 ............................................................................................................................. 48
COC RESOURCES AND TOOLS FOR CANCER PROGRAMS .......................................51

1
The Commission on Cancer is aconsortium of professional organizationsdedicated to reducing the morbidity andmortality of cancer through education,standard setting, and the monitoring ofquality care.
FOREWORD
COMMISSION ON CANCERAPPROVALS PROGRAMThe Approvals Program encourages hospitals, treatmentcenters, and other facilities to improve their quality ofpatient care through various cancer-related programs.These programs are concerned with prevention, earlydiagnosis, pretreatment evaluation, staging, optimaltreatment, rehabilitation, surveillance for recurrent disease,support services, and end-of-life care. The availability of afull range of medical services along with a multidisciplinaryteam approach to patient care at approved cancer programshave resulted in approximately 80 percent of all newlydiagnosed cancer patients being treated in Commission onCancer approved cancer programs.
Obtaining care at a CoC-approved cancer program ensuresthat one will receive:
• Quality care close to home.
• Comprehensive care offering a range of state-of-the-artservices and equipment.
• A multispecialty, team approach to coordinate the bestcancer treatment options available.
• Access to cancer-related information, education, andsupport.
• A cancer registry that collects data on cancer type, stage,and treatment results, and offers lifelong patient follow-up.
• Ongoing monitoring and improvement of care.
• Information about clinical trials and new treatmentoptions.
Approval by the Commission on Cancer is granted only tothose facilities that have voluntarily committed to providethe best in cancer diagnosis and treatment and are able tocomply with established CoC standards. Each cancerprogram must undergo a rigorous evaluation and review ofits performance and compliance with the CoC standards.In order to maintain approval, facilities with approvedcancer programs must undergo an on-site review everythree years.
The structure outlined in CoC Cancer Program Standards2004 ensures that each cancer program seeking approvalprovides all patients with a full range of diagnostic,treatment, and supportive services either on-site at thefacility or by referral.
There are currently more than 1,400 CoC-approvedcancer programs in the United States and Puerto Rico,representing close to 25 percent of all hospitals. Theseprograms are supported by a network of more than 1,500volunteer physician representatives appointed to maintaincancer program approval, or establish a new program, andto work with the local American Cancer Society on cancer-control activities for the community.
Established by the American College of Surgeons (ACoS)in 1922, the multidisciplinary Commission on Cancer(CoC) sets standards for quality multidisciplinary cancercare delivered primarily in hospital settings; surveysfacilities to assess compliance with those standards; collectsstandardized and quality data from approved facilities tomeasure treatment patterns and outcomes; and uses thedata to evaluate hospital provider performance and developeffective educational interventions to improve cancer careoutcomes at the national and local levels.
Commission membership consists of more than 100individuals representing the multidisciplinary professionalsof the cancer care team. Members include representativesfrom the ACoS and 38 national, professional memberorganizations. Each representative serves on one standingcommittee or disease site team that works to reach theCommission’s goals by:
• Establishing standards for cancer programs andevaluating and accrediting programs according to thosestandards.
• Coordinating the annual collection, analysis, anddissemination of data from CoC-approved cancerprograms for all cancer sites and conducting nationalsite-specific studies. Each of these efforts supports theassessment of patterns of care and outcomes of patientmanagement, which lead to improvements in the qualityof cancer care.
• Coordinating the activities of a nationwide network ofmore than 1,500 physician-volunteers who provide stateand local support for Commission and American CancerSociety cancer control initiatives.
• Providing oversight and coordination for educationalprograms of the Commission that are geared towardphysicians, cancer registrars, cancer program leadership,and others.
• Providing clinical oversight and expertise forCommission standard-setting activities.

2
BENEFITS OF BEING A COC-APPROVED CANCER PROGRAMBENEFITS OF BEING A COC-APPROVED CANCER PROGRAM
The Commission on Cancer’s Approvals Program offersmany notable benefits that will enhance a cancer programand its quality of patient care.
CoC-approved cancer programs:
• Are recognized by other national health careorganizations, including the JCAHO, as havingestablished performance measures for high-quality cancercare.
• Serve as a model for organizing and managing a cancerprogram to ensure multidisciplinary, integrated, andcomprehensive oncology services.
• Meet the demands for oncology data from clinicians andother health care professionals, third-party payers andmanaged care organizations, and the public because ofthe requirement for a cancer registry.
• Participate in a network of quality cancer programs thatprovide care to 80 percent of newly diagnosed cancerpatients.
• Receive free marketing and national public exposure bypartnering with the CoC and American Cancer Society(ACS) in the Facility Information Profile System(FIPS)—an information sharing effort of resources,services, and cancer experience for the ACS NationalCall Center and Web site.
• Receive an Approved Cancer Program PerformanceReport that allows a facility to compare its mandatorystandard ratings with other approved programs in thestate, nationally, and in the same cancer programcategory to identify quality improvement initiatives.
• Participate in the National Cancer Data Base(NCDB)—a nationwide oncology outcomes database forCoC-approved cancer programs.
• Receive immediate feedback on the quality of datasubmissions to the NCDB based on nationalstandardized data edit reports.
• Have access to benchmark reports containing nationalaggregate data and individual facility data to assesspatterns of care and outcomes relative to national norms.
• Participate in CoC special studies for the ad hoccollection of specific data to address important cancerproblems.
Being a CoC-approved cancer program demonstrates afacility’s ongoing commitment to providing high-quality,multidisciplinary cancer care. The Commission wishes toacknowledge the hard work and dedication these programsput forth in meeting the CoC standards, improving thereliability of cancer data, and enabling the best possibleoutcomes for today’s cancer patients.
MEMBER ORGANIZATIONS OFTHE COMMISSION ON CANCER
American Academy of Hospice and Palliative Medicine(AAHPM)American Academy of Pediatrics (AAP)American Association for Cancer Education (AACE)American Cancer Society (ACS)American College of Obstetricians and Gynecologists(ACOG)American College of Oncology Administrators (ACOA)American College of Physicians-American Society ofInternal Medicine (ACP-ASIM)American College of Radiology (ACR)American College of Surgeons (ACoS)American Dietetic Association (ADA)American Head and Neck Society (AHNS)American Hospital Association (AHA)American Joint Committee on Cancer (AJCC)American Medical Association (AMA)American Pediatric Surgical Association (APSA)American Society for Psychosocial and Behavioral Oncol-ogy/AIDS (ASPBOA)American Society of Clinical Oncology (ASCO)American Society of Colon and Rectal Surgeons (ASCRS)American Society for Therapeutic Radiology and Oncol-ogy (ASTRO)American Urological Association (AUA)Association of American Cancer Institutes (AACI)Association of Cancer Executives (ACE)Association of Community Cancer Centers (ACCC)Association of Oncology Social Work (AOSW)Canadian Society of Surgical Oncology (CSSO)Centers for Disease Control and Prevention (CDC)College of American Pathologists (CAP)Department of Defense (DoD)Department of Veterans Affairs (VA)International Union Against Cancer (UICC)National Cancer Institute: Surveillance, Epidemiology,and End Results (SEER) ProgramNational Cancer Registrars Association (NCRA)National Surgical Adjuvant Breast and Bowel Project(NSABP)North American Association of Central Cancer Registries(NAACCR)Oncology Nursing Society (ONS)Society of Gynecologic Oncologists (SGO)Society of Surgical Oncology (SSO)Society of Thoracic Surgeons (STS)

3
ACKNOWLEDGMENTS
CANCER PROGRAM STANDARDS WORKGROUP MEMBERS
Albert M. Brady, MD, FACPAlfred M. Cohen, MD, FACS
Rosemary L. Dibble, CTRBeth Ann Erickson, MD
Peter J. Fabri, MD, FACSJon M. Greif, DO, FACS
Daniel E. Kenady, Sr., MD, FACSDavid K. King, MD
Patricia L. Owen, RN, MSNicholas J. Petrelli, MD, FACS
William P. Reed, Jr., MD, FACSPat Shifflett, RN, MS
Robert P. Sticca, MD, FACSMary E. Stith, CCS, CTR
COC STAFF CONTRIBUTORS
Connie M. BuraM. Asa Carter, CTR
Vicki M. Chiappetta, RHIANancy C. Etzold, CTR
E. Greer Gay, RN, PhD, MPHLina S. Patel, MHA
Jerri Linn Phillips, MA, CTRKelly J. Hecht
Cassie Simon, CTRAndrew K. Stewart, MA
Mary Jo Strebel, RHIT, CTRDavid P. Winchester, MD, FACS
SPECIAL ACKNOWLEDGMENTS
Cancer Program SurveyorsCancer Program Constituents

4
5
The basic services that must be provided by everyCommission-approved cancer program are:
• DiagnosticClinical laboratoryDiagnostic imaging
• TreatmentMedical oncologyRadiation oncologySurgical procedures
• Other clinicalAJCC stagingClinical researchPatient guidelinesOncology nursingPain management
• Rehabilitation
• SupportCounselingDischarge planningHospice careNutritional supportPastoral carePatient and family support
• Prevention and early detection
CANCER PROGRAM CATEGORYEach facility is assigned to a Cancer Program Category byCancer Programs staff. The type of facility or organization,services provided, and cases accessioned are consideredwhen making category assignments.
A community-based facility that accessions between 300and 649 analytic cases annually may choose either theCommunity Hospital or Community HospitalComprehensive Cancer Program category. The facilitymeets the requirements for the category selected.
The table of Cancer Program Category Definitions andRequirements on pages 11–14 defines each of the ninecancer program categories and describes the requirementsfor each as they relate to specific standards.
THE SURVEY PROCESSCommission-approved cancer programs are surveyed on atriennial schedule. To be considered for initial survey, thefacility or cancer committee:
• Ensures that the clinical services, cancer committee,cancer conferences, and quality management programare in place at the facility for one year.
THE APPROVALS PROGRAMStandards for the evaluation of cancer clinics and registrieswere first published in 1930 by the American College ofSurgeons Committee on the Treatment of MalignantDisease. The first surveys of cancer clinics were conductedin 1931. Since that time, the standards for cancerprograms have been revised and expanded to reflect boththe comprehensive scope of cancer programs and thecontinuous changes in the health care environment.
The Committee on Approvals administers the activities ofthe Commission on Cancer (CoC) Approvals Program,which was designed to ensure that the structures andprocesses necessary for quality cancer care are in place. TheCoC standards for cancer programs promote and supportthe four historic cornerstones of the Approvals Program:multidisciplinary cancer committee, cancer conferences,evaluation of quality outcomes and improvements, and acancer registry.
Recognizing that cancer is a complex group of diseases, theCoC Cancer Program Standards promote consultationamong surgeons, medical and radiation oncologists,diagnostic radiologists, pathologists, and other cancerspecialists. This multidisciplinary cooperation results inimproved patient care.
ELIGIBILITYHospitals, freestanding treatment facilities, and health carenetworks are eligible to participate in the CoC ApprovalsProgram. Each facility ensures that patients have access tothe full scope of services required to diagnose, treat,rehabilitate, and support patients with cancer and theirfamilies. Prevention and early detection services are madeavailable to the community. Services are provided on-site,by referral, or are coordinated with other facilities or localagencies.
Five elements are key to the success of a Commission-approved cancer program:
• The clinical services provide state-of-the-artpretreatment evaluation, staging, treatment, and clinicalfollow-up for cancer patients seen at the facility forprimary, secondary, tertiary, or quaternary care.
• The cancer committee leads the program throughsetting goals, monitoring activity, and evaluating patientoutcomes and improving care.
• The cancer conferences provide a forum for patientconsultation and contribute to physician education.
• The quality improvement program is the mechanism forevaluating and improving patient outcomes.
• The cancer registry and database is the basis formonitoring the quality of care.
INTRODUCTION

6
• Establishes a reference date and ensures that the cancerregistry database includes two complete years of data andone year of follow-up activity.
• Meets the requirements for all standards outlined inCancer Program Standards 2004.
• Participates in a consultative evaluation of the cancerprogram performed by a Commission-trainedindependent cancer program consultant or other cancerregistry professional.
• Submits a request for survey to Cancer Programs staff.
• Signs the American College of Surgeons Commission onCancer Business Associate Agreement in compliancewith the Health Insurance Portability andAccountability Act (HIPAA).
• Submits data for all analytic cases for the last completedyear to the NCDB.
At the beginning of the survey year, an initial notificationis provided to facilities due for survey that year. Inpreparation for survey, the cancer committee at eachCommission-approved facility:
• Assesses program compliance with the requirements forall standards outlined in Cancer Program Standards 2004.
Due to extenuating circumstances, a survey extension maybe required. Valid reasons for extensions include, but arenot limited to:
• Database conversion
• Extended registry staff shortage
• Hospital mergers
Each request is made in writing to Cancer Programs staffby the Cancer Committee Chair within 60 days of theinitial notification. Requests for extension are givenindividual consideration. A maximum extension of oneyear may be granted. Facilities are notified of extensiondecisions, and the new target date for survey is provided.
Cancer Programs staff match a cancer program surveyor toeach program due for survey. The facility is notified of thesurveyor assignment and target date for survey. Thesurveyor’s name, credential(s), mailing address, phonenumber, and e-mail address are provided to the facility.Surveyor curriculum vitae are kept on file and are madeavailable on request by the facility.
The facility may decline the assigned surveyor within 30days of notification of assignment if a conflict of interestexists. A conflict of interest is defined as:
• Affiliation with the facility being surveyed.
• Affiliation with another facility in direct competitionwith the facility being surveyed.
The new surveyor assignment will be provided to the facilitywithin 30 days of notification of the conflict of interest.
Selection of a survey date is coordinated among the facility,surveyor, and Cancer Programs staff and must be scheduled
within the year the survey is due. Confirmation of the surveydate and time is provided to the facility administrator aminimum of 30 days prior to the on-site visit.
THE SURVEY APPLICATION RECORD(SAR)To facilitate a thorough and accurate evaluation of thecancer program, the facility completes or updates the Web-based Survey Application Record (SAR) 30 days before thescheduled on-site visit. The cancer registrar is providedwith password-protected access to the facility’s SAR andnotified when the SAR is available for completion.Completion of the SAR should be a team effort ofmembers of the cancer committee, with one individualchosen to coordinate the activity and complete the SAR.Each year, the facility is notified of the areas requiringannual updates. If not updated on the annual schedule, allinformation must be provided prior to survey.
In addition to capturing information about cancerprogram activity, the individual(s) responsible forcompleting portions of the SAR will perform a selfassessment and rate compliance with each standard usingthe Cancer Program Standards Rating system.
A portion of the information collected in the SARdescribing the facility’s resources and services isautomatically shared with the American Cancer Society(ACS) as part of the Facility Information Profile System(FIPS) for posting on the ACS Web site (www.cancer.org).The data sharing activity of the FIPS program is designedto benefit all CoC-approved cancer programs. This facility-specific information is made available to cancer patients,caregivers, and the general public, which enables them tomake more informed decisions about their options forcancer care.
The facility can use the SAR or access FIPS directly toupdate the resource and service information for sharingwith the ACS. By accessing FIPS directly, the facility isalso provided the option to release annual caseload data assubmitted to the CoC’s National Cancer Data Base(NCDB). This provides the public with site and stage datafor cancer patients seen at the facility.
Password-protected access to FIPS is provided to thecancer registrar, cancer committee chair, and CancerLiaison Physician through an e-mail notification system.The SAR and FIPS are accessed through CoC Datalinkslocated on the Cancer Programs page of the AmericanCollege of Surgeons Web site at www.facs.org.
The Cancer Program Surveyor reviews the facility’s Web-based SAR prior to the on-site visit.
DOCUMENTATION OF PROGRAMACTIVITYFacilities document cancer program activity and provide thedocumentation outlined in each standard to the surveyor aminimum of 2 weeks (14 days) prior to the on-site visit.

7
Cancer committee minutes are a primary resource fordocumenting program organization and operation, andmonitoring programmatic activity. Other methods orsources of documentation are acceptable and are providedto the surveyor in advance of the on-site visit as specified.
The following documentation is provided to the surveyorin advance of the on-site visit:
• A copy of the certificate of accreditation or letter fromthe accrediting body.
• Bylaws, policies and procedures, or other facility-approved methods used to document the level ofresponsibility and accountability designated to thecancer committee.
• Copies of all cancer committee minutes from the time ofthe previous survey through the present date.
• Documentation of subcommittee and workgroupstructure and activity.
• Documentation of the annual goals, time frame forevaluation and completion, assigned coordinator, andresponsibilities of other committee members throughcancer committee minutes or other sources.
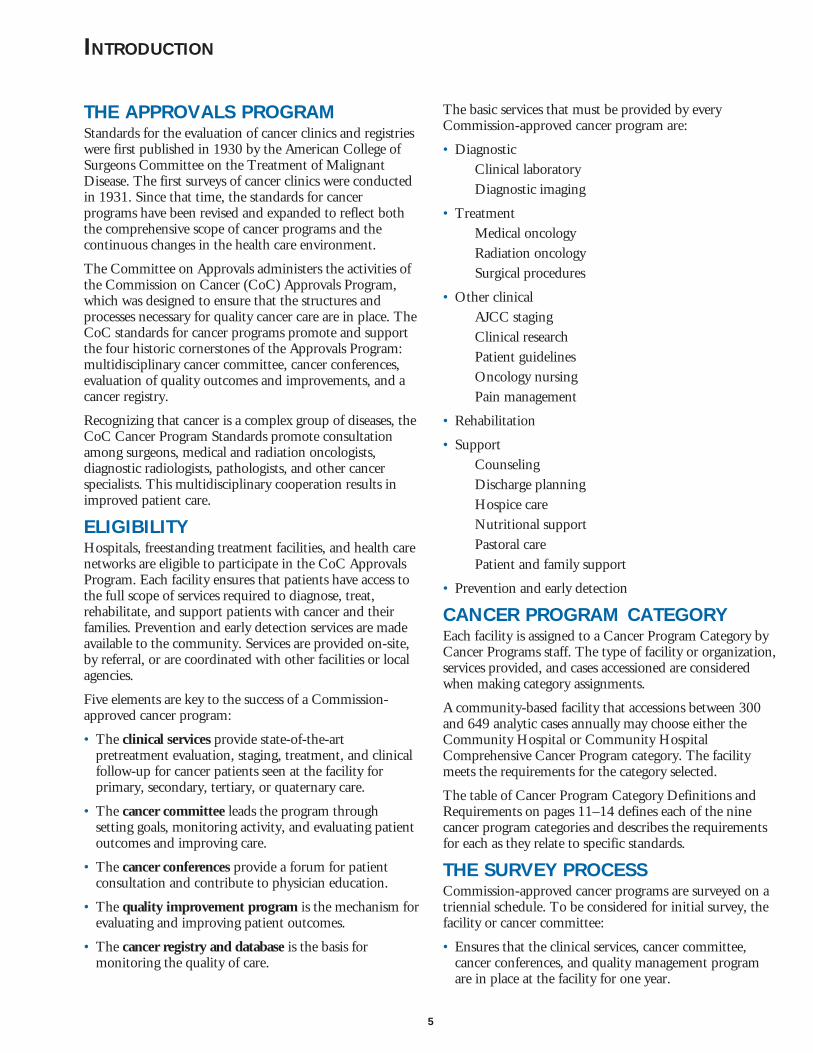
• Documentation of the annual frequency and format ofcancer conferences, the multidisciplinary attendancerequirement for the cancer conferences of the cancerprogram, the annual case presentation at cancerconferences, and the monitoring of cancer conferenceactivities and corrective action taken through cancercommittee minutes or other sources.
• Cancer committee minutes or other sources that showthe results of the outcomes analysis and method ofdissemination.
• A copy of the published annual report, if appropriate.
• Documentation of referred radiation oncology servicesand resources.
• Documentation that identifies the medical oncology unitor functional equivalent.
• A copy of the written policy and procedure for physicianstaging.
The surveyor will confirm cancer program activity duringthe on-site visit by reviewing the:
• Documentation of annual quality control activitiesthrough the cancer committee minutes or other sources.
• Verification of current credentialing from the NationalCancer Registrars Association (NCRA) for all CTRs onstaff at the facility, or documentation of recruitmentefforts and/or plans for current staff certificationincluding, but not limited to, education and trainingactivities and the target date for examination for facilitiesnot staffed by a CTR.
• Documentation of case abstracting by a CTR or datasupervision responsibilities of the CTR.
• Documentation that the cancer registry policy andprocedure manual or the registry software manualspecifies the use of the CoC data standards.
• Documentation of the cancer committee’s policies forobtaining follow-up information and a current follow-upreport.
• A copy of an organizational chart or a staff list notingcredentials of the nursing clinical expert(s), documenta-tion of orientation and annual competency evaluationfor each oncology nurse, and documentation of nursingmanagement of the medical oncology unit or functionalequivalent as appropriate to the category.
• A copy of the pathology report format for the majorcancer experience(s) at the facility showing the inclusionof the scientifically proven data elements.
• Documentation of the monitoring of and compliancewith the patient management and treatment guidelinescurrently required by the CoC as well as others adoptedand used by the facility.
• A copy of documentation of rehabilitation servicesavailable on-site or by referral, the process for access torehabilitation services, documentation of the annualevaluation of the rehabilitation services, and patientbrochures or other materials that outline rehabilitationservices.
• Documentation of policies and procedures for providinginformation about cancer-related clinical trials to patients.
• Documentation of the supportive services offered topatients and their families on-site or by referral.Documentation includes, but is not limited to,published brochures or flyers, meeting schedules, andInternet or Intranet postings.
• Documentation of two annual prevention or earlydetection programs through cancer committee minutesor other sources.
• Documentation of the methods to monitor and evaluatethe community outreach activities.
• Documentation of an annual educational activity, otherthan cancer conferences, including a published notice oragenda.
• Documentation of continuing education activity foreach member of the cancer registry staff.
• Summaries of each year’s studies of quality andoutcomes, including the study topic, analyses,recommendations, and follow-up.
• Summaries of each year’s patient care improvements.
The surveyor will review a minimum of 25 medical recordsto evaluate AJCC staging by the managing physician, thepathology reports that contain the scientifically validateddata items, and the quality of the abstracted data.

8
The surveyor may also review the following documentation:
• Written policy or plan outlining the system of referral
• Policy and procedure manual for:NursingSocial servicesRehabilitationHospiceDischarge planning teamInstitutional Review Board (if applicable)
• Policy and procedure for peer review (if applicable)
PAYMENT OF SURVEY FEEAn invoice for the survey fee will be mailed to the cancerregistrar within 30 days of the date of the scheduledsurvey. Payment of the invoice is due within 30 days ofreceipt. Survey results will not be released until the surveyfee is paid.
Programs are discouraged from canceling or postponingthe scheduled survey. If this becomes necessary, the facilitymust contact Cancer Programs staff and submit a writtennotification. The facility will be assessed a cancellation feein addition to nonrefundable fees incurred by the surveyor.
GUIDELINES FOR ON-SITE REVIEWThe cancer registrar confirms the agenda for the on-sitevisit with the surveyor at least 14 days prior to the visit.
The surveyor meets with key members of the program todiscuss the facility and the program and to verify data onthe SAR. The surveyor’s role is to assist in accuratelydefining the standards and verifying that the facility’scancer program is in compliance with the standards. Thesurveyor also discusses the goals and responsibilities of thecancer committee in relationship to the cancer program.
At a minimum, the surveyor must meet with:
• Member of Administration
• Cancer Committee Chair
• Cancer Liaison Physician
• Cancer Registrar
The surveyor may also request meetings with othermembers of the cancer committee or other members of thecancer care team:
Clinical research Hospice services
Nursing Social services
Quality improvement Diagnostic radiology
Radiation oncology Pastoral care
Discharge planning team Public education
Following a review of documentation and discussion withthe members of the cancer care team, a wrap-up session willbe held with all available members of the cancer care team.The Cancer Program Surveyor will delineate the program’s
strengths and weaknesses and offer suggestions to correctany noted deficiencies. The Cancer Program Surveyor willrespond to questions regarding the standards, SAR, andrating system with program leadership.
CANCER PROGRAM STANDARDSRATING SYSTEMThe following rating system is used to assign a compliancerating to each standard:
1+—Commendation1—Compliance5—Noncompliance8—Not Applicable
Based on the rating criteria specified for each standard, acompliance rating is assigned by the facility, surveyor, andCancer Programs staff.
A deficiency is defined as any standard with a rating of 5.A deficiency in one or more standards will affect theapproval award.
The Commendation rating (1+) is valid for nine (25percent) of the standards, as follows:
Standard 2.11 Each year the cancer committee analyzespatient outcomes and disseminates theresults of the analysis.
Standard 3.3 For each year between survey, 90 percentof cases are abstracted within six monthsof the date of first contact.
Standard 3.7 Cases submitted to the NCDB for themost recent accession year requested meetthe established quality criteria included inthe annual Call for Data.
Standard 4.3 AJCC staging is assigned by the managingphysician and recorded on a staging formin the medical record on 90 percent ofeligible annual analytic cases.
Standard 4.6 The guidelines for patient managementand treatment currently required by theCoC are followed.
Standard 5.2 As appropriate to category, the requiredpercentage of cases is accrued to cancer-related clinical trials on an annual basis.
Standard 6.2 Each year, two prevention or earlydetection programs are provided on-siteor coordinated with other facilities orlocal agencies.
Standard 7.2 Other than cancer conferences, allmembers of the cancer registry staffparticipate in a local, state, regional, ornational cancer-related educationalactivity each year.
Standard 8.2 Annually, the cancer committee imple-ments two improvements that directlyaffect cancer patient care. The improve-ments are documented.

9
Full Three-Year Approval is given to programs, either newor established, that comply with all standards. Theseprograms are surveyed at a three-year interval from thedate of the survey.
Three-Year Approval with Contingency is given when 1 to7 standards are rated deficient. The contingency status isresolved by the submission of documentation of compliancewithin 12 months. Documentation required to resolve thedeficiency for each standard is available on the CancerPrograms page of the American College of Surgeons Website. Full Approval is granted following submission ofdocumentation. These programs are surveyed at a three-yearinterval from the date of the survey.
Nonapproval is given when 8 or more standards are rateddeficient. Programs are encouraged to improve theirperformance and may reapply.
Approval Deferred is given when a new program is rateddeficient in 1 standard. The deferred status is resolved bythe submission of documentation of compliance within 12months. Documentation required to resolve the deficiencyfor each standard is available on the Cancer Programs pageof the American College of Surgeons Web site. FullApproval is granted following submission of documenta-tion without resurvey. These programs are surveyed at athree-year interval from the date of the submission ofdocumentation. Programs that do not resolve this status atthe end of the 12-month period must reapply for survey.
AWARD NOTIFICATION PROCESSAward notification takes place 8–12 weeks followingsurvey. The Approved Cancer Program PerformanceReport provides a comprehensive summary of the survey
APPROVAL AWARDS
outcome and approval award. It provides the facility’scompliance rating for each standard, an overall rating foreach section when compared with other approved facilities,a narrative description of deficiencies that requirecorrection, and any commendations awarded. Facilitieswill be given the option to submit a commentary on theperformance report that may include comments and/orcorrections. Comments will be reviewed by CancerPrograms staff and all appropriate corrections will beincorporated into the report before it is finalized.
By enabling each facility to compare its ratings for thestandards with Approved Programs, the reports willfacilitate the identification of areas for programimprovement. The report, along with a certificate ofapproval, press release, and marketing materials, is sent tothe cancer registrar with copies provided to theadministrator, cancer committee chair, Cancer LiaisonPhysician, and surveyor. A sample report appears on theCancer Programs page of the American College ofSurgeons Web site.
The facility can appeal the deficiency finding for anystandard or the approval award within 60 days of receiptof the Approved Cancer Program Performance Report.The appeal process is outlined in the cover letter thataccompanies the Approved Cancer Program PerformanceReport and also appears on the Cancer Programs page ofthe American College of Surgeons Web site.
A listing of all CoC-approved cancer programs appears onthe Cancer Programs page of the American College ofSurgeons Web site.
APPROVAL AWARD MATRIX
FULL APPROVALFULL APPROVALFULL APPROVALFULL APPROVALFULL APPROVAL(THREE YEARS)(THREE YEARS)(THREE YEARS)(THREE YEARS)(THREE YEARS)
36 Standards
APPROVAL DEFERREDAPPROVAL DEFERREDAPPROVAL DEFERREDAPPROVAL DEFERREDAPPROVAL DEFERRED(VALID ONLY FOR(VALID ONLY FOR(VALID ONLY FOR(VALID ONLY FOR(VALID ONLY FORNEW PROGRAMS)NEW PROGRAMS)NEW PROGRAMS)NEW PROGRAMS)NEW PROGRAMS)
NONAPPROVALNONAPPROVALNONAPPROVALNONAPPROVALNONAPPROVALTHREE-YEARTHREE-YEARTHREE-YEARTHREE-YEARTHREE-YEAR
APPROVAL WITHAPPROVAL WITHAPPROVAL WITHAPPROVAL WITHAPPROVAL WITHCONTINGENCYCONTINGENCYCONTINGENCYCONTINGENCYCONTINGENCY
Eight or moredeficiencies (22% ormore of Standards).Requires recom-mendation by theProgram ReviewSubcommittee andconfirmation by theCommittee onApprovals
No deficiencies One to sevendeficiency(ies)(up to 19% ofStandards)
One deficiency(2% of Standards)
Approval awards are based on consensus ratings by theCancer Program Surveyor, Cancer Programs staff, andwhen required, the Program Review Subcommittee for the36 standards.

10
THE COMMISSION ON CANCEROUTSTANDING ACHIEVEMENTAWARDThe CoC Outstanding Achievement Award will be grantedto any cancer program that:
• Receives a commendation rating in all nine definedareas, and
• Receives a compliance rating for all other (27) standards.
The purpose of this award is to:
• Recognize those cancer programs who strive forexcellence in providing quality care to the cancer patient.
• Motivate other programs to work toward improvingtheir care.
• Foster communication between award recipients andother programs to:
Share best practicesServe as a resourceAct as a “champion” for CoC cancer programapproval
Awards are granted to each program upon completion ofthe survey and evaluation of compliance with theestablished criteria. Cancer programs receiving this awardwill:
• Receive a letter of recognition from the CoC chairaddressed to the CEO/Administrator.
• Receive a specially designed press release, marketinginformation, and a special certificate.
• Receive CoC publicity via the CoC Flash and the CoCWeb site.
• Be acknowledged at a public forum including the CoCAnnual Meeting.
THE POSTSURVEY EVALUATIONThe postsurvey evaluation is a required part of the cancerprogram evaluation and is accessed through the SAR. Thisevaluation captures feedback from the facility, whichenables the CoC to evaluate and improve staff andsurveyor performance and develop educational trainingprograms for surveyors.
All responses are confidential and will not influence thecancer program evaluation or approval award. Responseson the evaluation form should represent a consensusopinion of the cancer program team about the quality ofthe Cancer Programs staff support during the surveyprocess and the performance of the surveyor. Thepostsurvey evaluation is completed within three weeksfollowing the survey date.
GUIDELINES FOR MERGED ORNETWORK PROGRAMSIf the facility has, is, or plans to merge or form a network,the facility must access and review either the Guidelines forMerged Programs or Guidelines for Network Programslocated on the Cancer Programs page of the AmericanCollege of Surgeons Web site (www.facs.org) TheGuidelines outline the requirements for cancer programcomposition as a merged or network program.
Once the respective guidelines have been reviewed, thefacility completes and submits a notification formdocumenting general information about the merger ornetwork. This information will allow Cancer Programsstaff to assign a new Facility Identification Number (FIN),cancer program category, approval award designation, andsurvey target date.
COC RESOURCES AND TOOLS FORCANCER PROGRAMSSurvey-related resources and tools are available on theCancer Programs page of the American College ofSurgeons Web site (www.facs.org). These resources andtools are listed in the Appendix.

11
CA
NC
ER
PR
OG
RA
M C
AT
EG
OR
Y D
EFI
NIT
ION
AN
D R
EQ
UIR
EM
EN
TS
(NC
P)
Net
wor
kC
ance
rP
rogr
am
(NC
IP)
NC
I-D
esig
nate
dC
ompr
ehen
sive
Can
cer
Pro
gram
(TH
CP
)T
each
ing
Hos
pita
lC
ance
rP
rogr
am
(CO
MP
)C
omm
unit
yH
ospi
tal
Com
preh
ensi
veC
ance
rP
rogr
am
(CH
CP
)C
omm
unit
yH
ospi
tal
Can
cer
Pro
gram
(HA
CP
)H
ospi
tal
Ass
ocia
teC
ance
rP
rogr
am
(AFC
P)
Aff
iliat
eH
ospi
tal
Can
cer
Pro
gram
(IC
P)
Inte
grat
edC
ance
rP
rogr
am
(FC
CP
) Fre
e-St
andi
ngC
ance
r C
ente
rP
rogr
am
Ove
rall
defi
niti
onT
he o
rgan
izat
ion
owns
mul
tipl
efa
cilit
ies
prov
idin
gin
tegr
ated
can
cer
care
and
off
ers
com
preh
ensi
vese
rvic
es. G
ener
ally
netw
orks
are
char
acte
rize
d by
ane
twor
k-w
ide
canc
er c
omm
itte
eor
func
tion
aleq
uiva
lent
,st
anda
rdiz
edre
gist
ry o
pera
tion
sw
ith
a un
iform
data
rep
osit
ory,
and
coor
dina
ted
serv
ice
loca
tion
san
d pr
acti
tion
ers.
The
net
wor
kpa
rtic
ipat
es in
clin
ical
res
earc
h.
The
faci
lity
secu
res
a N
atio
nal
Can
cer
Inst
itut
epe
er-r
evie
wed
Can
cer
Cen
ter
Supp
ort G
rant
and
is d
esig
nate
da
Com
preh
ensi
veC
ance
r C
ente
rPr
ogra
m b
y th
eN
CI.
A fu
ll ra
nge
of d
iagn
osti
c an
dtr
eatm
ent s
ervi
ces
and
staf
fph
ysic
ians
wit
hm
ajor
spe
cial
tybo
ards
, inc
ludi
ngth
ose
in o
ncol
ogy,
whe
re o
ffer
ed, a
reav
aila
ble.
Thi
sfa
cilit
ypa
rtic
ipat
es in
both
bas
ic a
ndcl
inic
al r
esea
rch.
The
faci
lity
isas
soci
ated
wit
h a
med
ical
sch
ool
and
part
icip
ates
in tr
aini
ngre
side
nts
in a
tle
ast f
our
area
s,tw
o of
whi
ch a
rem
edic
ine
and
surg
ery.
The
faci
lity
offe
rs th
efu
ll ra
nge
ofdi
agno
stic
and
trea
tmen
tse
rvic
es, o
n-si
te o
rby
ref
erra
l. T
hem
edic
al s
taff
are
boar
d-ce
rtifi
ed in
the
maj
or m
edic
alsp
ecia
lties
,in
clud
ing
onco
logy
, whe
reap
plic
able
. The
faci
lity
is r
equi
red
to p
arti
cipa
te in
clin
ical
res
earc
h.
The
faci
lity
prov
ides
a fu
llra
nge
ofdi
agno
stic
and
trea
tmen
t ser
vice
sth
at a
re a
vaila
ble
on-s
ite
or b
yre
ferr
al. T
hem
edic
al s
taff
are
boar
d ce
rtifi
ed in
the
maj
or m
edic
alsp
ecia
litie
sin
clud
ing
thos
e in
onco
logy
, whe
reap
plic
able
.Pa
rtic
ipat
ion
incl
inic
al r
esea
rch
isre
quir
ed.
The
faci
lity
prov
ides
a fu
llra
nge
ofdi
agno
stic
and
trea
tmen
tse
rvic
es, b
utre
ferr
al fo
r a
port
ion
oftr
eatm
ent i
sco
mm
on. T
hem
edic
al s
taff
are
boar
d ce
rtifi
ed in
the
maj
or m
edic
alsp
ecia
lties
.Fa
cilit
ies
may
part
icip
ate
incl
inic
al r
esea
rch.
The
faci
lity
has
limit
ed r
ange
of
diag
nost
ic a
ndtr
eatm
ent s
ervi
ces
on-s
ite.
Oth
erse
rvic
es a
reav
aila
ble
byre
ferr
al. C
linic
alre
sear
ch is
not
requ
ired
.
Thi
s fa
cilit
y ha
slim
ited
acc
ess
tose
rvic
es o
n-si
tean
d fo
rms
apa
rtne
rshi
p w
ith
asp
onso
ring
hosp
ital
faci
lity
topr
ovid
e ac
cess
toth
e fu
ll ra
nge
ofdi
agno
stic
and
trea
tmen
t se
rvic
es.
Clin
ical
res
earc
his
not
req
uire
d.
The
faci
lity
offe
rson
e tr
eatm
ent
mod
alit
y an
dfo
rms
apa
rtne
rshi
p w
ith
a ho
spit
al fa
cilit
yto
pro
vide
acc
ess
to th
e fu
ll ra
nge
of d
iagn
osti
c an
dtr
eatm
ent
serv
ices
.Pa
rtic
ipat
ion
byth
e in
tegr
ated
faci
lity
in c
linic
alre
sear
ch d
epen
dson
the
requ
irem
ents
for
the
hosp
ital
part
ner.
The
faci
lity
offe
rsa
min
imum
of
two
trea
tmen
tm
odal
itie
s and
the
full
rang
e of
diag
nost
ic a
ndtr
eatm
ent s
ervi
ces
are
avai
labl
e by
refe
rral
. Ref
erra
lto
a C
oC-
appr
oved
prog
ram
ispr
efer
red.
Part
icip
atio
n in
clin
ical
res
earc
h is
opti
onal
.
Res
iden
cies
Opt
iona
lA
s re
quir
ed b
yN
CI
Surg
ery
and
med
icin
e an
d an
ytw
o of
the
follo
win
g:di
agno
stic
radi
olog
y, fa
mily
prac
tice
,gy
neco
logy
,pa
thol
ogy,
radi
atio
non
colo
gy,
urol
ogy,
or
anon
colo
gic
fello
wsh
ip
Opt
iona
lO
ptio
nal
Opt
iona
lN
one
Opt
iona
lO
ptio
nal
Tab
le c
ontin
ues o
n fo
llow
ing
page

12
CA
NC
ER
PR
OG
RA
M C
AT
EG
OR
Y D
EFI
NIT
ION
AN
D R
EQ
UIR
EM
EN
TS
(NC
P)
Net
wor
kC
ance
rP
rogr
am
(NC
IP)
NC
I-D
esig
nate
dC
ompr
ehen
sive
Can
cer
Pro
gram
(TH
CP
)T
each
ing
Hos
pita
lC
ance
rP
rogr
am
(CO
MP
)C
omm
unit
yH
ospi
tal
Com
preh
ensi
veC
ance
rP
rogr
am
(CH
CP
)C
omm
unit
yH
ospi
tal
Can
cer
Pro
gram
(HA
CP
)H
ospi
tal
Ass
ocia
teC
ance
rP
rogr
am
(AFC
P)
Aff
iliat
eH
ospi
tal
Can
cer
Pro
gram
(IC
P)
Inte
grat
edC
ance
rP
rogr
am
(FC
CP
) Fre
e-St
andi
ngC
ance
r C
ente
rP
rogr
am
Cas
eloa
dre
quir
emen
tsba
sed
onan
alyt
ic c
asel
oad
Non
eN
one
Non
e65
0 or
mor
e10
0–64
9 (
A c
omm
unit
y-ba
sed
faci
lity
that
acce
ssio
nsbe
twee
n 30
0 an
d64
9 an
alyt
ic c
ases
annu
ally
may
choo
se e
ithe
r th
eC
omm
unit
yH
ospi
tal o
r th
eC
omm
unit
yH
ospi
tal
Com
preh
ensi
veC
ance
r Pr
ogra
mca
tego
ry. T
hefa
cilit
y m
eets
the
requ
irem
ents
for
the
cate
gory
sele
cted
.)
50–9
91–
49N
one
Non
e
JCA
HO
AA
AH
CA
CR
JCA
HO
AA
AH
CA
CR
JCA
HO
AO
ASt
ate
leve
l of
accr
edit
atio
n fo
rho
spit
als
JCA
HO
AO
ASt
ate
leve
l of
accr
edit
atio
n fo
rho
spit
als
JCA
HO
AO
ASt
ate
leve
l of
accr
edit
atio
n fo
rho
spit
als
JCA
HO
AO
ASt
ate
leve
l of
accr
edit
atio
n fo
rho
spit
als
JCA
HO
AO
ASt
ate
leve
l of
accr
edit
atio
n fo
rho
spit
als
JCA
HO
AO
ASt
ate
leve
l of
accr
edit
atio
n fo
rho
spit
als
Stan
dard
1.1
:A
ccre
diti
ngbo
dy
Cha
pter
1
JCA
HO
AO
ASt
ate
leve
l of
accr
edit
atio
n fo
rho
spit
als
Cha
pter
2
Stan
dard
2.2
:C
ance
rC
omm
itte
em
embe
rshi
p(a
ddit
iona
lm
embe
rs)
Net
wor
kad
min
istr
ator
Am
bula
tory
onco
logy
nur
seC
linic
al r
esea
rch
data
man
ager
or
nurs
ePa
in c
ontr
ol/
palli
ativ
e ca
reph
ysic
ian
Phar
mac
ist
Die
tary
/nut
riti
onsp
ecia
list
Hos
pice
nur
se o
rad
min
istr
ator
Clin
ical
res
earc
hda
ta m
anag
er o
rnu
rse
Pain
con
trol
/pa
lliat
ive
care
phys
icia
n
Clin
ical
res
earc
hda
ta m
anag
er o
rnu
rse
Pain
con
trol
/pa
lliat
ive
care
phys
icia
n or
spec
ialis
t
Pain
con
trol
/pa
lliat
ive
care
phys
icia
n or
spec
ialis
t
No
addi
tion
alm
embe
rsR
epre
sent
ativ
efr
om h
ospi
tal
part
ner
No
addi
tion
alm
embe
rsFo
r ce
nter
spr
ovid
ing
radi
atio
non
colo
gy:
dosi
met
rist
or
radi
atio
n ph
ysic
ist
No
addi
tion
alm
embe
rs

13
CA
NC
ER
PR
OG
RA
M C
AT
EG
OR
Y D
EFI
NIT
ION
AN
D R
EQ
UIR
EM
EN
TS
(NC
P)
Net
wor
kC
ance
rP
rogr
am
(NC
IP)
NC
I-D
esig
nate
dC
ompr
ehen
sive
Can
cer
Pro
gram
(TH
CP
)T
each
ing
Hos
pita
lC
ance
rP
rogr
am
(CO
MP
)C
omm
unit
yH
ospi
tal
Com
preh
ensi
veC
ance
rP
rogr
am
(CH
CP
)C
omm
unit
yH
ospi
tal
Can
cer
Pro
gram
(HA
CP
)H
ospi
tal
Ass
ocia
teC
ance
rP
rogr
am
(AFC
P)
Aff
iliat
eH
ospi
tal
Can
cer
Pro
gram
(IC
P)
Inte
grat
edC
ance
rP
rogr
am
(FC
CP
) Fre
e-St
andi
ngC
ance
r C
ente
rP
rogr
am
Stan
dard
2.4
:C
ance
rC
omm
itte
em
eeti
ngsc
hedu
le a
ndst
ruct
ure
Eve
ry o
ther
mon
thR
ecom
men
dsu
bcom
mit
tee
orw
orkg
roup
s
Qua
rter
lyR
ecom
men
dsu
bcom
mit
tee
orw
orkg
roup
s
Qua
rter
lyR
ecom
men
dsu
bcom
mit
tee
orw
orkg
roup
s
Qua
rter
lyO
ptio
nal
subc
omm
itte
e or
wor
kgro
ups
Qua
rter
lyO
ptio
nal
subc
omm
itte
e or
wor
kgro
ups
Qua
rter
lyO
ptio
nal
subc
omm
itte
e or
wor
kgro
ups
Qua
rter
lyO
ptio
nal
subc
omm
itte
e or
wor
kgro
ups
Qua
rter
lyO
ptio
nal
subc
omm
itte
e or
wor
kgro
ups
Stan
dard
2.6
:C
ance
rC
onfe
renc
efr
eque
ncy
and
form
at
Wee
kly
Net
wor
k-w
ide,
site
-foc
used
Wee
kly
Dep
artm
enta
l,si
te-f
ocus
ed, o
rgr
and
roun
ds
Wee
kly
Dep
artm
enta
l,si
te-f
ocus
ed, o
rfa
cilit
y-w
ide
Wee
kly
Dep
artm
enta
l,si
te-f
ocus
ed, o
rfa
cilit
y-w
ide
Mon
thly
Faci
lity-
wid
eM
onth
ly w
ith
hosp
ital
par
tner
Faci
lity-
wid
e
Mon
thly
wit
hho
spit
al p
artn
erFa
cilit
y-w
ide
Mon
thly
Faci
lity-
wid
e
Exe
mpt
Exe
mpt
Exe
mpt
Func
tion
aleq
uiva
lent
Func
tion
aleq
uiva
lent
Des
igna
ted
inpa
tien
t med
ical
onco
logy
uni
t
Des
igna
ted
inpa
tien
t med
ical
onco
logy
uni
t or
func
tion
aleq
uiva
lent
Des
igna
ted
inpa
tien
t med
ical
onco
logy
uni
t
Des
igna
ted
inpa
tien
t med
ical
onco
logy
uni
t
Req
uire
dR
equi
red
Req
uire
dR
equi
red
Req
uire
dR
equi
red
Req
uire
dR
equi
red
Req
uire
dSt
anda
rd 4
.4:
Spec
ializ
edkn
owle
dge
and
skill
s in
onco
logy
nurs
ing
Cha
pter
2 (
cont
inue
d)
Mon
thly
Faci
lity-
wid
e
Qua
rter
lyO
ptio
nal
subc
omm
itte
e or
wor
kgro
ups
Cha
pter
4
Cha
pter
5
Stan
dard
4.5
:E
xem
ptE
xem
ptE
xem
ptO
ncol
ogy
Nur
seM
anag
erO
ncol
ogy
Nur
seM
anag
erO
ncol
ogy
Nur
seM
anag
erO
ncol
ogy
Nur
seM
anag
er(d
esig
nate
d un
it)
or R
egis
tere
dN
urse
(fu
ncti
onal
equi
vale
nt)
Reg
iste
red
Nur
seR
egis
tere
d N
urse
Stan
dard
5.2
:P
erce
ntag
eac
crua
l to
clin
ical
tri
als
6% o
f the
num
ber
of a
nnua
lan
alyt
ic c
ases
for
the
netw
ork
10%
of t
henu
mbe
r of
ann
ual
anal
ytic
cas
es
4% o
f the
num
ber
of a
nnua
lan
alyt
ic c
ases
2% o
f the
num
ber
of a
nnua
lan
alyt
ic c
ases
Exe
mpt
Exe
mpt
Exe
mpt
Exe
mpt
Exe
mpt
Stan
dard
4.2
:In
pati
ent
med
ical
onco
logy
uni
tor
func
tion
aleq
uiva
lent
Tab
le c
ontin
ues o
n fo
llow
ing
page

14
CA
NC
ER
PR
OG
RA
M C
AT
EG
OR
Y D
EFI
NIT
ION
AN
D R
EQ
UIR
EM
EN
TS
(NC
P)
Net
wor
kC
ance
rP
rogr
am
(NC
IP)
NC
I-D
esig
nate
dC
ompr
ehen
sive
Can
cer
Pro
gram
(TH
CP
)T
each
ing
Hos
pita
lC
ance
rP
rogr
am
(CO
MP
)C
omm
unit
yH
ospi
tal
Com
preh
ensi
veC
ance
rP
rogr
am
(CH
CP
)C
omm
unit
yH
ospi
tal
Can
cer
Pro
gram
(HA
CP
)H
ospi
tal
Ass
ocia
teC
ance
rP
rogr
am
(AFC
P)
Aff
iliat
eH
ospi
tal
Can
cer
Pro
gram
(IC
P)
Inte
grat
edC
ance
rP
rogr
am
(FC
CP
) Fre
e-St
andi
ngC
ance
r C
ente
rP
rogr
am
2 qu
alit
yim
prov
emen
ts
1 st
udy
on a
nyto
pic
inco
oper
atio
nw
ith
hosp
ital
part
ner
Stan
dard
8.2
:Q
ualit
yim
prov
emen
ts
Cha
pter
8
Stan
dard
8.1
:St
udie
s of
qual
ity
2 qu
alit
yim
prov
emen
ts2
qual
ity
impr
ovem
ents
2 qu
alit
yim
prov
emen
ts2
qual
ity
impr
ovem
ents
2 qu
alit
yim
prov
emen
ts2
qual
ity
impr
ovem
ents
1 st
udy
base
d on
regi
stry
dat
a2
addi
tion
alst
udie
s
1 st
udy
base
don
reg
istr
y da
ta2
addi
tion
alst
udie
s
1 st
udy
base
d on
regi
stry
dat
a1
addi
tion
alst
udy
1 st
udy
base
d on
regi
stry
dat
a1
addi
tion
al s
tudy
1 st
udy
base
d on
regi
stry
dat
a1
addi
tion
al s
tudy
1 st
udy
base
d on
regi
stry
dat
a1
addi
tion
al s
tudy
1 st
udy
base
d on
regi
stry
dat
a1
addi
tion
al s
tudy
1 st
udy
base
d on
regi
stry
dat
a1
addi
tion
al s
tudy
2 qu
alit
yim
prov
emen
ts2
qual
ity
impr
ovem
ents

Chapter
15
1
Institutional and Programmatic ResourcesPurpose: The standard confirms the accreditation standing for the facility or
facilities.
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
FACILITY ACCREDITATIONStandard 1.1 The facility is accredited by a recognized authority appropriate to the
facility type.
DEFINITION AND REQUIREMENTSAccreditation ensures that care is provided in a safeenvironment. The boundary of the cancer programapproval is established by the facility(ies) and/or locationsincluded in the accreditation.
The accrediting organizations recognized by the Commis-sion on Cancer (CoC) are:• Joint Commission on Accreditation of Healthcare
Organizations (JCAHO)
• American Osteopathic Association (AOA)• Accreditation Association of Ambulatory Healthcare
Agencies (AAAHC)• American College of Radiology (ACR)• Health facility licensure agency (usually located within
the State Department of Health)
No survey will be performed if the facility is not accreditedby a recognized authority.
SPECIFICATIONS BY CATEGORY
ACCEPTED ACCREDITING BODIES BY CATEGORY
CATEGORYCATEGORYCATEGORYCATEGORYCATEGORY REQUIRED ACCREDITATIONREQUIRED ACCREDITATIONREQUIRED ACCREDITATIONREQUIRED ACCREDITATIONREQUIRED ACCREDITATION(one of the following)(one of the following)(one of the following)(one of the following)(one of the following)
Network Cancer Program (NCP) JCAHOAOAHealth facility licensure agency
NCI-designated Comprehensive Cancer Program (NCIP) JCAHOAOAHealth facility licensure agency
Teaching Hospital Cancer Program (THCP) JCAHOAOAHealth facility licensure agency
Community Hospital Comprehensive Cancer Program (COMP) JCAHOAOAHealth facility licensure agency
Community Hospital Cancer Program (CHCP) JCAHOAOAHealth facility licensure agency
Hospital Associate Cancer Program (HACP) JCAHOAOAHealth facility licensure agency
Affiliate Hospital Cancer Program (AFCP) JCAHOAOAHealth facility licensure agency
Integrated Cancer Program (ICP) JCAHOAAAHCACR
Freestanding Cancer Center Program (FCCP) JCAHOAAAHCACR

16
RATING(1) Compliance: The facility is accredited by a recognized
accrediting organization.
(5) Noncompliance: The facility is not accredited, or isaccredited by an organization not recognized by theCoC. No survey will take place.
DOCUMENTATIONThe facility completes the Survey Application Record (SAR).A minimum of 2 weeks (14 days) prior to the on-site visit, thefacility provides the surveyor with a copy of the certificate ofaccreditation or letter from the accrediting body.

Chapter
17
2
Cancer Committee LeadershipPurpose: The standards establish the cancer committee’s leadership responsibility and
accountability for cancer program activities at the facility.
LEVEL OF RESPONSIBILITY AND ACCOUNTABILITYStandard 2.1 The organizational structure of the facility or medical staff gives the
cancer committee responsibility and accountability for the cancerprogram activities.
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
DEFINITION AND REQUIREMENTSLeadership is the key element in an effective cancerprogram and program success depends on an effectivecancer committee (or a functional equivalent). The cancercommittee is responsible for goal setting, planning,initiating, implementing, evaluating, and improving allcancer-related activities in the facility.
The facility or medical staff formally establishes theresponsibility, accountability, and multidisciplinarymembership required for the cancer committee to fulfill itsrole. The facility documents the cancer committee’sresponsibility and accountability using a method appropri-ate to the facility’s organizational structure. Examplesinclude, but are not limited to:• The facility bylaws designate the cancer committee to be
a standing committee with authority defined.• The medical staff bylaws designate the cancer committee
to be a standing committee with authority defined.• Policies and procedures for the facility define authority
of the cancer committee.
• Policies and procedures for the medical staff define theauthority of the cancer committee.
Other methods that are consistent with the facilityorganization and operation are acceptable.
SPECIFICATIONS BY CATEGORYAll cancer programs must fulfill this standard.
DOCUMENTATIONA minimum of 2 weeks (14 days) prior to the on-site visit,the facility provides the surveyor with a copy of the bylaws,policies and procedures, or other facility-approvedmethods used to document the level of responsibility andaccountability designated to the cancer committee.
RATING(1) Compliance: The cancer committee’s responsibility
and accountability are documented in bylaws, policiesand procedures, or other facility approved methods.
(5) Noncompliance: The cancer committee’s responsibil-ity and accountability are not documented.
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
Required physician members:• Diagnostic radiologist• Pathologist• General surgeon• Medical oncologist• Radiation oncologist (If all radiation oncology services
are provided by referral, and the facility’s medical staffdoes not include a radiation oncologist, then a cancercommittee member from radiation oncology isrecommended, but not required.)
MEMBERSHIPStandard 2.2 The cancer committee membership is multidisciplinary, representing
physicians from the diagnostic and treatment specialties andnonphysicians from administrative and supportive services.
DEFINITION AND REQUIREMENTSCancer patient care requires a multidisciplinary approachand encompasses numerous physician and nonphysicianprofessionals.
The committee responsible for program leadership ismultidisciplinary and represents the full scope of care.Required members include at least one physicianrepresenting each of the diagnostic and treatment services.Required nonphysician representatives from each of theadministrative, clinical, and supportive services available atthe facility are also to be members of the committee. Thecommittee fulfills the attendance and quorumrequirements set by the facility.

18
Required nonphysician members:• Cancer program administrator• Oncology nurse• Social worker or case manager• Certified Tumor Registrar (CTR)• Performance improvement or quality management
professional
Additional physician or nonphysician cancer committeemembers are required for specific categories. These in-clude, but are not limited to:• Hospice/home care nurse or administrator• Pain control/palliative care physician or specialist• Clinical research data manager or nurse
The Cancer Liaison Physician must be a member of thecancer committee. The Cancer Liaison Physician may also
fulfill the role of one of the required physician specialties.The cancer committee chair is a physician who may alsofulfill the role of one of the required physician specialties.
Each facility should assess the scope of services offered anddetermine the need for additional cancer committeemembers based on the major cancer sites seen by thefacility. Additional members may include, but are notlimited to:• Specialty physicians representing the major cancer
experience(s) at the facility• Dietary/nutrition specialist• Pharmacist• Pastoral care representative• Psychiatric or mental health professional• American Cancer Society Cancer Control representative• A public member of the community served
SPECIFICATIONS BY CATEGORY
DOCUMENTATIONThe facility completes the Survey Application Record(SAR). The surveyor will evaluate cancer committeemembership by reviewing cancer committee minutes.
RATING(1) Compliance: All required cancer committee members
are appointed.
(5) Noncompliance: One or more of the required cancercommittee members are not appointed.
ADDITIONAL REQUIRED CANCER COMMITTEE MEMBERSADDITIONAL REQUIRED CANCER COMMITTEE MEMBERSADDITIONAL REQUIRED CANCER COMMITTEE MEMBERSADDITIONAL REQUIRED CANCER COMMITTEE MEMBERSADDITIONAL REQUIRED CANCER COMMITTEE MEMBERS
Network administrator
Oncology nurse from the ambulatory care setting
Clinical research data manager or nurse
Pain control/palliative care physician
Pharmacist
Dietary/nutrition specialist
Hospice nurse or administrator
Clinical research data manager or nurse
Pain control/palliative care physician
Clinical research data manager or nurse
Pain control/palliative care physician or specialist
Pain control/palliative care physician or specialist
None
None
Representative from hospital partner
None
For Freestanding Cancer Centers providing radiationoncology: dosimetrist or radiation physicist
CATEGORYCATEGORYCATEGORYCATEGORYCATEGORY
Network Cancer Program (NCP)
NCI-designated Comprehensive Cancer Program (NCIP)
Teaching Hospital Cancer Program (THCP)
Community Hospital Comprehensive Cancer Program(COMP)
Community Hospital Cancer Program (CHCP)
Hospital Associate Cancer Program (HACP)
Affiliate Hospital Cancer Program (AFCP)
Integrated Cancer Program (ICP)
Freestanding Cancer Center Program (FCCP)
ADDITIONAL REQUIRED CANCER COMMITTEE MEMBERS BY CATEGORY

19
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
PROGRAM ACTIVITY COORDINATORSStandard 2.3 One coordinator is designated for each of the four areas of cancer
committee activity: cancer conference, quality control of cancerregistry data, quality improvement, and community outreach.
DEFINITION AND REQUIREMENTSTo promote team involvement and shared responsibilities,one member of the cancer committee is designated tocoordinate one of the four major areas of program activity.The Cancer Liaison Physician is assigned to coordinate thecommunity outreach activities. The other coordinators arechosen on the basis of their specialty, knowledge, andskills. Both physician and nonphysician members of thecommittee may be selected as coordinators.
Coordinator roles and responsibilities are defined by thecancer committee. These include, but are not limited to:• Contributing to the development of the annual goals
and objectives of the cancer committee.• Monitoring the activity of the assigned area of
responsibility.• Reporting regularly to the cancer committee.• Recommending corrective action if activity falls below
the annual goal or requirements.
Cancer committee minutes identify the designatedcoordinators, their assigned area of activity, and the defined
duties and responsibilities. The minutes also document thereported results of activities and recommendations forcorrective action.
In some facilities, the coordinator(s) works cooperativelywith established departments or staff leadership tocoordinate, monitor, and recommend improvements to theassigned areas or programs. In this instance, thecoordinator(s) acts as the cancer committee liaison to theestablished departments or staff leadership.
SPECIFICATIONS BY CATEGORYAll cancer programs must fulfill this standard.
DOCUMENTATIONThe facility completes the SAR.
RATING(1) Compliance: A coordinator is designated for each of
the four specified areas of activity.
(5) Noncompliance: A designated coordinator is notappointed for one or more of the four specified areasof activity.
MEETING SCHEDULEStandard 2.4 The cancer committee meeting schedule and structure fulfill the
requirements for the category.
DEFINITION AND REQUIREMENTSRegular meetings assure that administrative responsibilitiesrelated to cancer program leadership are carried out.
In Network Cancer Programs, the cancer committee meetsevery other month to complete the administrativeresponsibilities related to cancer program leadership. In allother categories, the cancer committee meets at leastquarterly. More frequent meetings may be required tomeet the overall program needs.
In larger programs, the cancer committee establishessubcommittees or workgroups to manage specific activities.Subcommittees may include, but are not limited to:• Cancer conference activity• Quality control of registry data
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
• Quality management activity• Community outreach• Review of policies and procedures
The subcommittees and workgroups may call onphysicians and nonphysicians outside of the cancercommittee to accomplish their assignment. The assignedcoordinator chairs the appropriate subcommittee orworkgroup. Other subcommittee or workgroup chairs arechosen from the members of the cancer committee.
Meetings of subcommittees and workgroups do notconstitute meetings of the full cancer committee.

20
DOCUMENTATIONThe facility completes the SAR. A minimum of 2 weeks(14 days) prior to the on-site visit, the facility provides thesurveyor with copies of all cancer committee minutes fromthe time of the previous survey through the present date,and documentation of subcommittee and workgroupstructure and activity through minutes or other sources.
RATING(1) Compliance: The cancer committee fulfills meeting
requirements specified for the category.
(5) Noncompliance: The cancer committee does not fulfillmeeting requirements specified for the category.
SPECIFICATIONS BY CATEGORY
CATEGORYCATEGORYCATEGORYCATEGORYCATEGORY
CANCER COMMITTEE MEETING SCHEDULE AND STRUCTURE RECOMMENDATIONS BY CATEGORY
SUBCOMMITTEES/WORKGROUPSSUBCOMMITTEES/WORKGROUPSSUBCOMMITTEES/WORKGROUPSSUBCOMMITTEES/WORKGROUPSSUBCOMMITTEES/WORKGROUPSREQUIRED SCHEDULEREQUIRED SCHEDULEREQUIRED SCHEDULEREQUIRED SCHEDULEREQUIRED SCHEDULE
Recommended
Recommended
Recommended
Optional
Optional
Optional
Optional
Optional
Optional
Every other month
Quarterly
Quarterly
Quarterly
Quarterly
Quarterly
Quarterly
Quarterly
Quarterly
Network Cancer Program (NCP)
NCI-designated ComprehensiveCancer Program (NCIP)
Teaching Hospital Cancer Program(THCP)
Community Hospital ComprehensiveCancer Program (COMP)
Community Hospital Cancer Program(CHCP)
Hospital Associate Cancer Program(HACP)
Affiliate Hospital Cancer Program(AFCP)
Integrated Cancer Program (ICP)
Freestanding Cancer Center Program(FCCP)
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
DUTIES AND RESPONSIBILITIESStandards 2.5 through 2.11 are the minimum activities required for program leadership andoperation. The cancer committee duties and responsibilities must specify the activities describedin each of these standards. Additional duties and responsibilities are defined by each cancerprogram based on the size of the facility and scope of services provided.
Standard 2.5 The cancer committee develops and evaluates the annual goalsand objectives for the clinical, community outreach, qualityimprovement, and programmatic endeavors related to cancer care.
DEFINITION AND REQUIREMENTSAnnual goals provide direction for cancer programactivities and serve as the basis for cancer programevaluation. The cancer committee establishes goalsappropriate to the facility. The scope of this activity andmethod of documentation will vary, depending on the sizeof the facility; however, goals must be documented incancer committee minutes.
Examples of goals include, but are not limited to:• Clinical Goal: Improve turn-around time for chemotherapy
administration in the outpatient infusion center.• Community Outreach: Improve follow-up of positive
findings from the prostate screening program.
• Quality Improvement: Implement the use of a stagingform in the medical record.
• Programmatic: Earn the CoC Outstanding AchievementAward.
The cancer committee chair is responsible for guiding thecommittee through the development and evaluation of theannual goals. The cancer committee establishes a timeframe for achieving each goal. Frequent monitoring andevaluation are necessary.
SPECIFICATIONS BY CATEGORYAll cancer programs must fulfill this standard.

21
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
SPECIFICATIONS BY CATEGORY
DOCUMENTATIONThe facility completes the SAR. The facility provides thesurveyor with copies of cancer committee minutes or othersources that document the annual goals, time frame forevaluation and completion, assigned coordinator, andresponsibilities of other committee members.
RATING(1) Compliance: Annual cancer program goals are docu-
mented and evaluated.
(5) Noncompliance: Annual cancer program goals are notdeveloped and/or documented.
Standard 2.6 The cancer committee establishes the cancer conference frequencyand format on an annual basis.
DEFINITION AND REQUIREMENTSSetting the cancer conference frequency and format allowsfor prospective review of cancer cases that encouragesmultidisciplinary involvement. Cancer conferences areintegral to improving the care of cancer patients bycontributing to the patient management process andoutcomes and providing education to physicians and otherstaff in attendance.
The annual cancer conference frequency and format aredocumented in cancer committee minutes. The cancercommittee considers the minimum percentage of cases tobe presented at cancer conferences (Standard 2.8) whendetermining the cancer conference frequency.
Frequency and format should be based on the following:• Category• Number of annual analytic accessions
• Types of cases seen by the facility• Need for consultative services• Need for educational activities
Conferences that include case presentation should beavailable to the entire medical staff and are the preferredformat for community-based facilities. Network CancerPrograms use current technology to offer network-wideconferences to multiple locations. Departmental and site-focused conferences or grand rounds are appropriate forlarger community-based facilities, teaching hospitals, NCI-designated Comprehensive Cancer Programs, andNetwork Cancer Programs. Departmental or site-focusedconferences or lectures may be included in the cancerconference program by any facility at the discretion of thecancer committee.
CATEGORYCATEGORYCATEGORYCATEGORYCATEGORY RECOMMENDED MINIMUM FREQUENCYRECOMMENDED MINIMUM FREQUENCYRECOMMENDED MINIMUM FREQUENCYRECOMMENDED MINIMUM FREQUENCYRECOMMENDED MINIMUM FREQUENCY RECOMMENDED FORMATRECOMMENDED FORMATRECOMMENDED FORMATRECOMMENDED FORMATRECOMMENDED FORMAT
Network-wideSite-focused
DepartmentalSite-focusedGrand rounds
DepartmentalSite-focusedFacility-wide
DepartmentalSite-focusedFacility-wide
Facility-wide
Facility-wide
Facility-wide
Facility-wide
Facility-wide
Weekly
Weekly
Weekly
Weekly
Monthly
Monthly
Monthly with hospital partner
Monthly with hospital partner
Monthly
Network Cancer Program(NCP)
NCI-designated ComprehensiveCancer Program (NCIP)
Teaching Hospital CancerProgram (THCP)
Community HospitalComprehensive CancerProgram (COMP)
Community Hospital CancerProgram (CHCP)
Hospital Associate CancerProgram (HACP)
Affiliate Hospital CancerProgram (AFCP)
Integrated Cancer Program (ICP)
Freestanding Cancer CenterProgram (FCCP)
CANCER CONFERENCE FREQUENCY AND RECOMMENDED FORMAT BY CATEGORY
22
RATING(1) Compliance: The annual conference frequency and
format are established and documented.
(5) Noncompliance: The annual conference frequencyand format are not established and/or documented.
DOCUMENTATIONThe facility completes the SAR. A minimum of 2 weeks(14 days) prior to the on-site visit, the facility provides thesurveyor with copies of cancer committee minutes or otherdocumentation showing the annual frequency and formatof cancer conferences of the cancer program.
A cancer conference grid, calendar, or tracking tool thatshows the annual conference schedule and format isrecommended.
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
Standard 2.7 The cancer committee establishes the multidisciplinary atten-dance requirements for cancer conferences on an annual basis.
DEFINITION AND REQUIREMENTSSetting the multidisciplinary attendance requirement forcancer conferences encourages multidisciplinaryinvolvement in prospective discussion of cancer cases.Cancer conferences are integral to improving the care ofcancer patients by contributing to the patient managementprocess and outcomes and providing education tophysicians and other staff in attendance.
Consultative services are optimal when physicianrepresentatives from diagnostic radiology, pathology,surgery, medical oncology, and radiation oncologyparticipate in facility-wide or network-wide cancerconferences.
The multidisciplinary cancer conference attendancerequirement is established by the cancer committee anddocumented in cancer committee minutes.
The minimum multidisciplinary attendance should bebased on:• Types of cases seen by the facility• Format of conferences (facility-wide or network-wide,
departmental, site-focused, grand rounds)
Multidisciplinary physician attendance at departmental orsite-focused conferences or grand rounds will depend onthe diagnostic and treatment needs of the sites presented.On an annual basis, the cancer committee defines themultidisciplinary attendance for each departmental or site-focused conference held at the facility. The cancercommittee may modify the multidisciplinary attendancerequirement for these conferences.
Network-wide cancer conferences involve physicians fromall sites within the network who provide diagnostic andtreatment services. All members of the medical staff of theCancer Program Network are actively involved in network-wide cancer conferences.
SPECIFICATIONSAll cancer programs must fulfill this standard.
DOCUMENTATIONThe facility completes the SAR. A minimum of 2 weeks(14 days) prior to the on-site visit, the facility provides thesurveyor with copies of cancer committee minutes or otherdocumentation showing the multidisciplinary attendancerequirement for the cancer conferences of the cancerprogram.
A cancer conference grid, calendar, or tracking tool thatshows the multidisciplinary attendance is recommended.
RATING(1) Compliance: The multidisciplinary conference
attendance requirement is established and documentedby the cancer committee on an annual basis.
(5) Noncompliance: The cancer committee does notestablish and document the multidisciplinary confer-ence attendance on an annual basis.
RECOMMENDED MULTIDISCIPLINARY ATTENDANCE
Conference Type Diagnostic Radiology Pathology Surgery Medical Oncology Radiation Oncology
Leukemia x x
Brain/CNS x x x x
EXAMPLES OF MODIFICATIONS FOR MULTIDISCIPLINARY ATTENDANCE AT SITE-FOCUSED CONFERENCES

23
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
Standard 2.8 The cancer committee ensures that the required number of cases arediscussed at the cancer conference on an annual basis and that at least75 percent of the cases discussed are presented prospectively.
DEFINITION AND REQUIREMENTSCancer conferences are an essential forum to providemultidisciplinary consultative services for patients as wellas offer education to physicians and allied healthprofessionals. The number of cases presented each year atcancer conferences is a percentage of the number of annualanalytic cases added to the cancer registry database.
Programs accessioning 3,000 or more cases annuallypresent 300 cases each year at cancer conferences. All otherprograms present at least 10 percent of the number ofannual analytic cases seen at the facility each year. InNetwork Cancer Programs, the cases selected ensure equalrepresentation of each network site.
To provide a consultative service for patients andphysicians, 75 percent of the cases presented must bediscussed prospectively, that is, addressing patientmanagement issues. Cases selected for discussion includethe five major sites seen at the institution, as well as caseswith unusual sites and/or histologies and challengingmanagement issues. The number of cases presented at eachconference is monitored to ensure adequate time forthorough discussion.
Prospective cases include, but are not limited to:• Newly diagnosed and treatment not yet initiated.• Newly diagnosed and treatment initiated, but discussion
of additional treatment is needed.
• Previously diagnosed, initial treatment completed, butdiscussion of adjuvant treatment or treatment forrecurrence or progression is needed.
• Previously diagnosed, and discussion of supportive orpalliative care is needed.
SPECIFICATIONS BY CATEGORYAll programs must fulfill this standard.
DOCUMENTATIONThe facility completes the SAR. A minimum of 2 weeks(14 days) prior to the on-site visit, the facility provides thesurveyor with copies of cancer committee minutes or otherdocumentation showing the annual case presentation atcancer conferences.
A cancer conference grid, calendar, or tracking tool thatshows the annual conference schedule and format isrecommended.
RATING(1) Compliance: Presentation of 10 percent of the annual
analytic caseload or 300 cases annually and 75 percentof the cases presented are discussed prospectively.
(5) Noncompliance: Presentation of less than 10 percentof the annual analytic caseload or 300 cases annuallyor less than 75 percent of the cases presented arediscussed prospectively.
Standard 2.9 The cancer committee monitors and evaluates the cancer conferencefrequency, multidisciplinary attendance, total case presentation, andprospective case presentation on an annual basis.
DEFINITION AND REQUIREMENTSMonitoring of cancer conference activity assures thatconferences provide consultative services for patients aswell as offer education to physicians and allied healthprofessionals. Monitoring cancer conference activity alsoensures that the educational and consultative goals of thecancer program are fulfilled. The cancer committeemonitors cancer conference activity through the work ofthe cancer conference coordinator.
Routine evaluation of cancer conference activity in each offour areas is essential to ensure compliance with therequirements set by the cancer committee:• Conference frequency• Multidisciplinary attendance• Total case presentation• Prospective case presentation
The methods used to monitor cancer conference activityare set by the cancer committee and documented in cancercommittee minutes.
The assigned coordinator monitors each area of cancerconference activity, reports regularly to the cancercommittee, and recommends corrective action if any areafalls below the annual goal or requirements. The resultsand recommendations are documented in cancercommittee minutes.
SPECIFICATIONS BY CATEGORYAll cancer programs must fulfill this standard.
DOCUMENTATIONA minimum of 2 weeks (14 days) prior to the on-site visit,the facility provides the surveyor with copies of cancercommittee minutes or other documentation showing themonitoring of cancer conference frequency, multidis-ciplinary attendance, total case presentation, prospectivecase presentation, and corrective action taken for any areathat falls below the annual goal.
A cancer conference grid, calendar, or tracking tool thatshows the annual conference schedule and format isrecommended.

24
RATING(1) Compliance: The four areas of the cancer conference
activity are monitored and evaluated by the cancercommittee on an annual basis.
(5) Noncompliance: The four areas of the cancer confer-ence activity are not monitored and evaluated by thecancer committee on an annual basis.
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
Standard 2.10 The cancer committee establishes and implements a plan toevaluate the quality of cancer registry data and activity on anannual basis. The plan includes procedures to monitorcasefinding, accuracy of data collection, abstracting timeliness,follow-up, and data reporting.
DEFINITION AND REQUIREMENTSHigh quality cancer registry data are essential to accuratelyassess treatment outcomes and patient survival. The cancercommittee ensures the quality of cancer registry data byestablishing and implementing a quality control plan tomonitor multiple areas of cancer registry activity and theaccuracy and completeness of abstracted data.
The quality control plan:
1. Sets the review criteria2. Sets the quality control time table3. Specifies the quality control methods and individuals
involved
Required activitiesRandom sampling of annual analytic caseloadPhysician review (residents and other physicians
may be included)
4. Identifies the activities to be evaluated
Required activitiesCasefindingAbstracting timelinessAccuracy of abstracted data
Class of CasePrimary siteHistologyFirst course of treatment
Follow-up informationCompletion and accuracy of AJCC staging by the
managing physicianNCDB data submission, correction of data errors,
and resubmission of corrected data
5. Defines the scope of the evaluation
Required scopeMinimum: 10 percent of annual analytic caseloadMaximum: 300 cases annually
6. Establishes the minimal quality benchmarks
Required accuracyCancer registry data submitted to the NCDB meet
the established quality criteria included in theannual Call For Data
Recommended accuracy90 percent of AJCC staging assigned by the
managing physician is accurate
7. Maintains documentation of the quality controlactivity
Required documentationReview criteriaCases reviewedIdentified errors and resolutionsReports to the cancer committee
The assigned coordinator works cooperatively with registrystaff or other departments to implement the qualitycontrol plan. The assigned coordinator monitors each areaof cancer registry activity, reports regularly to the cancercommittee, and recommends corrective action if any areafalls below the annual goal. The results andrecommendations are documented in the cancercommittee minutes or other sources.
SPECIFICATIONS BY CATEGORYAll cancer programs must fulfill this standard.
DOCUMENTATIONAt the on-site visit, the facility provides the surveyor withdocumentation of annual quality control activities throughthe cancer committee minutes or other sources. Thesurveyor discusses the cancer registry quality controlactivities and results with the quality control coordinatorand other members of the cancer committee during theon-site visit.
RATING(1) Compliance: The cancer committee establishes and
implements a plan to evaluate the required areas ofcancer registry activity on an annual basis.
(5) Noncompliance: The cancer committee does notestablish and implement a plan to evaluate the requiredareas of cancer registry activity on an annual basis.

25
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
Dissemination of results is documented in cancercommittee minutes.
An annual report may be published at the discretion of thecancer committee. If an annual report is published, thecancer committee is responsible for determining the reportcontent and publication schedule. The cancer committee’sanalysis of patient outcomes must be included.
SPECIFICATIONS BY CATEGORYAll cancer programs must fulfill this standard.
DOCUMENTATIONThe facility completes the SAR. A minimum of 2 weeks(14 days) prior to the on-site visit, the facility provides thesurveyor with copies of cancer committee minutes or othersources that show the results of the outcomes analysis andmethod of dissemination.
If an annual report is published, a copy is provided to thesurveyor a minimum of 2 weeks (14 days) prior to the on-site visit.
RATING(1+) Commendation: Documentation and dissemination
of an analysis of more than one site of cancer annually,or an annual report of cancer program activity ispublished.
(1) Compliance: The cancer committee documents anddisseminates results of a patient outcome analysis withthe medical staff and administration annually.
(5) Noncompliance: The cancer committee does notdocument and disseminate results of a patient out-come analysis with the medical staff and administra-tion annually.
Standard 2.11 Each year, the cancer committee analyzes patient outcomes anddisseminates the results of the analysis.
DEFINITION AND REQUIREMENTSClinically meaningful analyses of patient diagnosis,treatment, and outcomes are necessary to ensure thatquality care is administered to cancer patients.
A survival analysis of one cancer site is the preferredmethod; however, other outcome measures may be selectedat the discretion of the cancer committee.
This analysis includes the facility’s experience andcomparison to NCDB data through benchmark reports.Additional sources of comparative data may also be used.
The analysis includes the program’s experience with:• Diagnostic evaluation• Treatment modalities• Prognostic factors• Survival data by AJCC stage of disease• Comparison with NCDB benchmarks and other
comparative data
The results of the cancer committee’s analysis are sharedwith the medical staff and administration annually.Acceptable methods for disseminating results include, butare not limited to:• Written reports• Presentation at cancer committee meetings or cancer
conferences• Presentations at lectures or workshops• Electronic postings on internal or external Web sites

26

Chapter
27
3
Cancer Data Management and CancerRegistry OperationsPurpose: The standards ensure accurate and timely collection of cancer patient
data, which allow for the evaluation of patient outcomes andidentification of opportunities for improvement. Lifetime follow-up ofpatients included in the database encourages clinical follow-up andsurveillance of additional primaries.
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
STAFF QUALIFICATIONSStandard 3.1 Case abstracting is performed or supervised by a Certified Tumor
Registrar (CTR).
DEFINITION AND REQUIREMENTSTo positively impact cancer patient care, the facility mustensure that case abstracting is performed or supervised by aCTR. Successful operation of the cancer registry requirescredentialed staff who are trained and knowledgeable in allaspects of oncology data collection and case abstracting.
The recognized credential for a cancer registry professionalis CTR, which is granted through the National CancerRegistrars Association (NCRA). Details on eligibility,testing, and recredentialing are available from the NCRA.
Methods to ensure case abstracting by a CTR include, butare not limited to:• Facility-employed CTR• Contracted data collection, using a registry service
agency or company or independent contractor• Enabling current staff to earn the CTR credential
In all instances, case abstracting must be performed orsupervised by a CTR. The case abstracting or datasupervision responsibilities of the CTR are documented.
All cancer programs approved by the Commission onCancer (CoC) must comply with this standard by January1, 2006. Programs surveyed prior to January 1, 2006, thatare working toward compliance with this standard, mustshow documentation of recruitment efforts and/or plansfor current staff certification. This includes, but is notlimited to:
• Education and training activities• The target date for examination
The same applies to positions vacant at the time of survey.New programs must comply with this standard at the timeof the initial survey.
SPECIFICATIONS BY CATEGORYAll cancer programs must fulfill this standard.
DOCUMENTATIONThe facility completes the Survey Application Record(SAR). During the on-site visit, the facility provides thesurveyor with verification of current credentialing fromNCRA for all CTRs on staff at the facility. During the on-site visit, the facility also provides the surveyor withdocumentation showing that the case abstracting or datasupervision is performed by the CTR.
Facilities not staffed by a CTR show documentation ofrecruitment efforts and/or plans for current staffcertification.
RATING(1) Compliance: Case abstracting is performed or super-
vised by a CTR, or documentation of recruitmentefforts and/or a plan for current staff certification is inplace.
(5) Noncompliance: Case abstracting is not performed orsupervised by a CTR, and no recruitment efforts and/or plans for current staff certification are in place.

28
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
DEFINITION AND REQUIREMENTSCoC data standards ensure consistent and accurate hospitalcancer registry data that support the meaningful evaluationof patient diagnosis and treatment. All CoC-approvedcancer programs use the data standards defined by theCoC appropriate for the year of diagnosis for that case.
Cancer registries may be required to comply withadditional mandates pertaining to case and data reportingestablished by the federal or state government, or by thefacility’s cancer committee.
SPECIFICATIONS BY CATEGORYAll cancer programs must fulfill this standard.
DOCUMENTATIONDuring the on-site visit, the facility providesdocumentation that the cancer registry policy andprocedure manual or the registry software manual requiresthe use of the CoC data standards. The surveyor confirmsthe use of CoC data standards and coding instructionsduring the on-site visit.
RATING(1) Compliance: Appropriate CoC data standards and coding
instructions are used to describe all reportable cases.
(5) Noncompliance: The cancer registry does not useappropriate CoC data standards and coding instruc-tions to describe all reportable cases.
DATA COLLECTIONStandard 3.2 CoC data standards and coding instructions are used to describe all
reportable cases.
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
DOCUMENTATIONThe facility completes the SAR. The surveyor will verifythe abstracting currency during the on-site visit through areview of a random sample of cancer registry abstracts.
RATING(1+) Commendation: More than 90 percent of cases are
abstracted within six months of the date of firstcontact for each year between survey.
(1) Compliance: For each year between survey, 90 percentof cases are abstracted within six months of the date offirst contact.
(5) Noncompliance: For each year between survey, fewerthan 90 percent of cases are abstracted within sixmonths of the date of first contact.
DEFINITION AND REQUIREMENTSOngoing timely abstracting is essential for accurate datacollection, evaluation, and reporting of outcomes.
Abstracting timeliness is calculated from the “Date of FirstContact” (see definition in current version of CoC datastandards) to the date the case is abstracted. Abstractingtimeliness is maintained throughout the survey cycle.
Abstracting timeliness can be estimated by using thefollowing formula:• Total cases for last completed accession year = 1,200• Monthly case average: 1,200÷12 = 100• If the date is January 1, then approximately 600 cases
(100 × 6 = 600) from the previous year should beabstracted.
SPECIFICATIONS BY CATEGORYAll cancer programs must fulfill this standard.
Standard 3.3 For each year between survey, 90 percent of cases are abstractedwithin six months of the date of first contact.
TARGETED ABSTRACTING TIME LINE FOR THE MONTH OF SURVEYMONTH OF SURVEYMONTH OF SURVEYMONTH OF SURVEYMONTH OF SURVEYMONTH OF SURVEY TARGETED ABSTRACTING TIME LINETARGETED ABSTRACTING TIME LINETARGETED ABSTRACTING TIME LINETARGETED ABSTRACTING TIME LINETARGETED ABSTRACTING TIME LINE
January July 1 of previous yearFebruary August 1 of previous yearMarch September 1 of previous yearApril October 1 of previous yearMay November 1 of previous yearJune December 1 of previous yearJuly January 1 of current yearAugust February 1 of current yearSeptember March 1 of current yearOctober April 1 of current yearNovember May 1 of current yearDecember June 1 of current year

29
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
Standard 3.4 An 80 percent follow-up rate is maintained for all analytic patientsfrom the cancer registry reference date.
Standard 3.5 A 90 percent follow-up rate is maintained for all analytic patientsdiagnosed within the last five years, or from the cancer registry refer-ence date, whichever is shorter.
DEFINITION AND REQUIREMENTSLong-term follow-up is essential to evaluate outcomes ofcancer care. Accurate follow-up data enable the facility tocompare outcomes with regional, state, or nationalstatistics. Follow-up information is obtained at leastannually for all living analytic patients included in thecancer registry database.
All reportable cases are followed, except:• Residents of foreign countries• Cases that are reportable-by-agreement• Patients whose age exceeds 100 years and who are
without contact for more than 12 months
Methods to obtain follow-up information include, but arenot limited to:• Letters or phone calls to the physician(s)• Letters or phone calls to the patient or the patients’ next
of kin• Admission or readmission to the facility• Pathology reports• Clinic and outpatient visits• Internet sources• Death certificate matches• Review of newspaper obituary columns
SPECIFICATIONS BY CATEGORYAll cancer programs must fulfill these standards.
DOCUMENTATIONThe facility completes the SAR. During the on-site visit,the facility provides the surveyor with a copy of the cancercommittee’s policies for obtaining follow-up informationfrom the cancer registry policy and procedure manual. Thefacility also provides a current follow-up report to thesurveyor on the day of the on-site visit.
RATINGStandard 3.4(1) Compliance: An 80 percent follow-up rate is main-
tained for all analytic patients from the cancer registryreference date.
(5) Noncompliance: A follow-up rate of less than 80percent is maintained for all analytic patients from thecancer registry reference date.
Standard 3.5(1) Compliance: A 90 percent follow-up rate is main-
tained for all analytic patients diagnosed within thelast five years, or from the cancer registry referencedate, whichever is shorter.
(5) Noncompliance: A follow-up rate of less than 90percent is maintained for all analytic patients diag-nosed within the last five years, or from the cancerregistry reference date, whichever is shorter.
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
DEFINITION AND REQUIREMENTSData submitted to the NCDB are used to provide feedbackto assess the quality of patient care. This feedback enablescancer programs to compare treatment and outcomes withregional, state, and national patterns.
The NCDB is a nationwide oncology outcomes databaseused as a clinical surveillance mechanism to monitorchanges and variations in patterns of cancer care andpatient outcomes. NCDB data are useful benchmarks forpatient care and continuous quality improvement forcancer programs.
DATA REPORTINGStandard 3.6 Complete data for all analytic cases are submitted to the National
Cancer Data Base (NCDB) in accordance with the annual Call forData.
Data submission to the NCDB must be performedutilizing the CoC’s secure Web-based data submissionapplication.
New programs submit data to the NCDB after the requestfor initial survey is accepted by the CoC and prior toscheduling the initial survey.
SPECIFICATIONS BY CATEGORYAll cancer programs must fulfill this standard.
DOCUMENTATIONData submission history is confirmed by the CoC.

30
RATING(1) Compliance: Complete data for all analytic cases are
submitted to the NCDB for each call year betweensurvey in accordance with the annual Call for Data.
(5) Noncompliance: Incomplete data for all analytic casesare submitted or no data are submitted for one or moreyears between survey in accordance with the annual Callfor Data.
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
Standard 3.7 Cases submitted to the NCDB for the most recent accessionyear requested meet the established quality criteria included inthe annual Call for Data.
DEFINITION AND REQUIREMENTSAccurate data are necessary for meaningful comparison oftreatment and patient outcomes. These data are the basisfor the feedback provided to cancer programs.
As part of its annual Call for Data, the NCDB willdocument the conditions that will cause the casessubmitted to the NCDB to be rejected. Rejected cases donot meet specified data quality criteria.
Standardized, nationally accepted data edits are applied toall analytic cases submitted. The reporting registry isnotified of the problematic cases through an edit report.
Beginning with the 2003 NCDB Call for Data for casesaccessioned during the year 2002, cancer programs mustdo the following:• Resolve errors resulting in rejected records• Correct outstanding data quality errors
Problematic cases are corrected and resubmitted inaccordance with the annual Call for Data. The cancercommittee monitors the resolution and resubmission ofproblematic cases (Standard 2.10).
The cases for the most current accession year satisfy theestablished quality criteria by September 1 of the yearfollowing the Call for Data. New programs correct andresubmit cases prior to scheduling the initial survey.
SPECIFICATIONS BY CATEGORYAll cancer programs must fulfill this standard.
DOCUMENTATIONResubmission history is confirmed by the CoC.
RATING(1+) Commendation: Cases for the most recent accession
year requested meet the quality criteria for the annualCall for Data on initial submission.
(1) Compliance: Cases for the most recent accession yearrequested meet the established quality criteria bySeptember 1 of the year following the Call for Data.
(5) Noncompliance: Cases for the most recent accessionyear requested do not meet the established qualitycriteria by September 1 of the year following the Callfor Data.
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
SPECIAL STUDIESStandard 3.8 The facility participates in special studies as requested by
the CoC.
DEFINITION AND REQUIREMENTSHypothesis-based special studies are designed to evaluatepatient care, set benchmarks, and provide feedback toimprove patient care in cancer programs.
Based on study criteria, the CoC will determine if CoC-designed special studies will fulfill the requirements forStandard 8.1. This information will be documented inCoC communications and provided to programs selectedto participate.
The CoC will design and conduct at least two specialstudies annually. Based on study criteria, select approvedprograms will participate in each study. Facilities keep arecord of all communication(s), and information/dataprovided to the CoC for these special studies.
SPECIFICATIONS BY CATEGORYUpon request, all cancer programs must fulfill thisstandard.
DOCUMENTATIONThe facility completes the SAR. Participation in CoCspecial studies is confirmed by the CoC.
RATING(1) Compliance: Complete data are submitted for each
special study in which the facility is requested toparticipate.
(5) Noncompliance: Incomplete or no data are submittedfor each special study in which the facility is requestedto participate.
(8) Not applicable: The facility was not requested toparticipate in special studies.

31
CANCER REGISTRY OPERATIONSThe Commission on Cancer has established theseoperational requirements for hospital-based cancerregistries.
CANCER REGISTRYThe cancer registry is a component of the cancer programdesigned to accession, abstract, and conduct follow-up forreportable primaries diagnosed and/or initially treated atthe facility since the registry reference date. The cancerregistry database is a vital tool for programmatic andadministrative planning and research and for monitoringpatient outcomes.
Data are collected according to the current CoC datastandards and coding instructions. These data includepatient identification, cancer identification, stage of diseaseat diagnosis, first course of treatment, outcomes, andadministrative information. Facility-defined data itemsand/or benign or borderline histologies are also included,as requested by the cancer committee.
Network Cancer Programs establish a uniform datarepository with the means to enter data from each of thenetwork service locations. A system is in place to providefor unduplicated data.
CoC-approved cancer programs routinely communicatewith the cancer registry software provider to assure changesin data and cancer program requirements are appropriatelyreflected in the cancer registry software.
PROCEDURE MANUALA procedure manual is necessary to document policies andprocedures for the daily operations of the cancer registryand may also include policies and procedures for thecancer program. The cancer committee reviews andupdates the procedure manual annually. Changes topolicies and procedures are approved by the cancercommittee and documented in the cancer committeeminutes.
The cancer registry procedure manual includes, but is notlimited to:• Abstracting• Case accessions• Case eligibility• Casefinding• Coding references• Confidentiality and release of information• Dates of implementation or changes in policies or
registry operations• Follow-up• Job descriptions• Maintaining and using the suspense system• Quality control of registry data
• Reference date• Reporting requirements and mechanisms• Retention of documents• Staging systems
Areas of program activity include, but are notlimited to:• Cancer committee meetings• Cancer conference activities• Cancer program objectives• Policy for AJCC staging• Studies of quality and quality improvement system
REFERENCE DATEThe reference date is the date after which all eligible casesmust be included in the registry. A reference date isestablished by the cancer committee prior to the initialsurvey. The reference date is January 1 of the specifiedyear.
Once approved, programs cannot change the referencedate unless circumstances cause a need to petition the CoCfor a change. Each request is given individual considerationbased on changes in the patient population or hospitalcensus, flaws or lapses in data collection, changes in dataacquisition methods, or a high lost-to-follow-up rate dueto the longevity of the registry.
One disadvantage of changing the reference date is thatcases accessioned prior to the new reference date aredeleted or become non-analytic (Class of Case 4) and arenot included in outcomes analysis.
The reference date is documented in the cancer registrypolicy and procedure manual.
CASE ELIGIBILITYThe CoC requires registries in approved cancer programsto accession, abstract, and conduct follow-up forreportable primaries diagnosed and/or initially treated atthe facility. The tumors must meet the criteria for analyticcases (Class 0, 1, or 2). Both pathologically and clinicallydiagnosed cases are included.
Please refer to the current CoC data standards and codinginstructions for specific requirements describing:• Ambiguous terminology• Cases reportable–by–agreement• Case eligibility• Class of Case• Tumors accessioned, abstracted, and followed
The case eligibility criteria are documented in the cancerregistry policy and procedure manual.

32
CASEFINDINGCasefinding is a systematic method of identifying alleligible cases that are included in the cancer registrydatabase. All points of service in the health care deliverysystem must be included in the casefinding process.Casefinding will identify both new cases and those alreadyincluded in the cancer registry database. Information aboutcases that are already included in the registry can be usedfor follow-up.
Multiple sources are used to identify eligible cases. Primarysources include, but are not limited to:• Disease index• Medical oncology log• Operative reports• Pathology reports• Radiation oncology log
Secondary sources include, but are not limited to:• Cytology reports• Diagnostic/medical imaging• Discharge log• Other outpatient logs
The casefinding procedures are documented in the cancerregistry policy and procedure manual.
SUSPENSE SYSTEMA suspense system provides temporary storage for potentialcases and those cases that have not been completelyabstracted. A case is entered into the suspense systemduring the casefinding process and remains there until caseabstracting is completed.
A suspense system typically includes:• Patient name• Patient identifier• Date of diagnosis or date of first contact• Primary site
Most cancer registry software includes an automatedsuspense system. If the cancer registry software does notinclude a suspense system, a spreadsheet can be used totrack cases held in suspense.
Cases are listed by the date of diagnosis or date of firstcontact and cases are abstracted in date order to ensurethat abstracting timeliness is maintained.
The policies and procedures for the suspense system aredocumented in the cancer registry policy and proceduremanual.
ACCESSION REGISTERThe accession register is an annual, sequential listing of alleligible cases included in the registry database. The acces-sion register includes, but is not limited to:• Accession and sequence number• Date of initial diagnosis• Patient name• Primary site
The accession register is used to:• Assess registry workload• Audit other registry files• Monitor casefinding• Plan cancer conferences• Select cases for quality control review
If a registry serves multiple facilities, the accession registerincludes facility identifiers.
The policies and procedures for the accession register aredocumented in the cancer registry policy and proceduremanual.
PATIENT INDEXThe patient index is an alphabetical list of each patiententered into the registry since the reference date. Thetypical index includes, but is not limited to:• Date of birth• Date of diagnosis• Date of last contact or death• Histology• Laterality• Medical record number• Patient name• Primary site(s)• Sequence number• Sex
For patients with multiple reportable primaries, the patientindex also includes, but is not limited to, the following foreach primary:• Date of diagnosis• Histology• Laterality• Primary site• Sequence number
If a registry serves multiple facilities, the patient indexincludes facility identifiers.
The policies and procedures for the master patient indexare documented in the cancer registry policy and proceduremanual.
ABSTRACTThe abstract is a summary of pertinent information aboutthe patient, cancer diagnosis and treatment, and patientfollow-up. Accurate and complete registry data allow foroptimal cancer program and administrative planning toallocate hospital resources. The cancer registry database isalso a valuable resource for research investigations, studiesof quality, and outcome evaluation.
An abstract must be completed for all reportable primariesdiagnosed and/or initially treated at the facility since theregistry reference date. If a patient has multiple cancers, anabstract must be prepared for each reportable primarydiagnosed or treated at the reporting institution after thereference date.

33
The components of an abstract are outlined in the currentCoC data standards and include:• Patient identification• Cancer identification• Stage of disease at diagnosis• First course of treatment• Outcomes• Case administration descriptors
Refer to Standard 3.3 for specific requirements regardingabstracting timeliness.
The policies and procedures for abstracting aredocumented in the cancer registry policy and proceduremanual.
RETENTION OF DOCUMENTSAbstracted data for cases diagnosed and/or treated at thefacility after the cancer registry reference date are retainedin perpetuity. If the reference date is changed, abstracteddata for cases diagnosed and/or treated at the facility priorto the new reference date are deleted or archived.
All other documentation of cancer program and cancerregistry activity meet the facility standard for retention ofdocuments or five years, whichever is longer.
This includes, but is not limited to:• Cancer conference documentation or grids• Minutes of cancer committee meetings• Outcome analysis and reports• Results of quality control of cancer registry data• Results of studies of quality
The policy for retention of documents is documented inthe cancer registry policy and procedure manual.
QUALITY CONTROL OF CANCER REGISTRYDATAThe cancer committee is responsible for supervising thecancer registry and quality control of cancer registry data.The quality control plan and cancer committeeinvolvement in quality control activities are outlined inStandard 2.10.
The cancer registry staff is responsible for visual review ofabstracts and the accession register and periodicreabstracting of cases. The cancer registry staff is alsoresponsible for reviewing edit reports from centralregistries, state registries, and the National Cancer DataBase, and for correcting and resubmitting cases to theseagencies.
The policies and procedures for quality control of cancerregistry data are documented in the cancer registry policyand procedure manual.
LIFETIME FOLLOW-UPLifetime follow-up collects information about the cancerand patient status throughout the life of the patient.Follow-up data include:• Cancer status• Date of first recurrence• Date of last contact or death• Following registry• Follow-up source• Type of first recurrence• Vital status
Refer to Standards 3.4 and 3.5 for specific requirementsregarding follow-up rates.
The policies and procedures for follow-up are documentedin the cancer registry policy and procedure manual.
CONFIDENTIALITY, RELEASE OF INFORMA-TION, AND REQUEST LOGThe cancer registry activities and database meet the patientconfidentiality standards defined by the facility as well asstate and federal regulations. These policies and proceduresaddress the following:• Data release criteria• Informed consent and authorization• Patient rights
Data requests are documented in a data request log thatincludes, but is not limited to:• Copy of data provided• Data requested• Date request was fulfilled• Intended use of data• Request date• Requestor’s name or organization
The policies and procedures for confidentiality, release ofinformation, and the request log are documented in thecancer registry policy and procedure manual.

34
Chapter
35
4
Clinical ManagementPurpose: The standards identify the minimum scope of clinical services needed
to provide high-quality cancer care to patients. The managing physicianis essential to coordinating a multidisciplinary team approach to patientcare including the accurate and complete staging of each patient.
CLINICAL SERVICESCancer patients require specialized diagnostic andtherapeutic services. Care often continues for weeks ormonths following diagnosis. Depending on the facility,some services may be provided by referral, including theadministration of chemotherapy and radiation therapy.
The minimum scope of clinical services is available topatients diagnosed and treated at the cancer program.Referral services and sources are documented for internaluse and the information is available to patients.
Diagnostic Services Clinical laboratoryDiagnostic imaging
Treatment Services Surgical proceduresRadiation treatmentSystemic therapy
Other Clinical Services AJCC stagingOncology nursingPatient guidelinesRehabilitation
TREATMENT SERVICESStandard 4.1 Radiation treatment services are available on-site or by referral.
DEFINITION AND REQUIREMENTSRadiation therapy is a primary component ofmultimodality treatment. Radiation therapy services areavailable on-site or by referral to one or more locations.
Information on referral services and locations are providedto patients seen at the facility.
SPECIFICATIONS BY CATEGORYAll cancer programs must fulfill this standard.
DOCUMENTATIONThe facility completes the Survey Application Record(SAR). A minimum of 2 weeks (14 days) prior to theon-site visit, the facility provides the surveyor with
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
Standard 4.2 Based on the category, an inpatient medical oncology unitor a functional equivalent exists to provide specialized careto patients.
DEFINITION AND REQUIREMENTSMedical oncology (systemic therapy) is a primarycomponent of multimodality treatment. Patients needinghospitalization for chemotherapy or as a result of treatmentare assured of receiving comprehensive and specializedcancer-related care in a safe environment.
Based on the category, the facility may designateone or more inpatient areas as a medical oncologyunit. Smaller facilities may set aside certain beds oran area of an inpatient unit as a functionalequivalent of a medical oncology unit. In thisinstance, specialized care is provided to the patientregardless of the location.
documentation of referred radiation oncologyservices and locations. The surveyor confirmsradiation therapy services available at the facility,and through referral, with members of the cancerprogram team during the on-site visit. The surveyorexamines the methods for distributing informationto patients.
RATING(1) Compliance: Radiation therapy services are
available on-site or by referral.
(5) Noncompliance: Radiation therapy services arenot available on-site or by referral.

36
Policies and procedures address the special needs of thepatients cared for on the medical oncology unit or func-tional equivalent. These include, but are not limited to:• Adequate nursing coverage
• Criteria for patient admission• Management of immunocompromised patients• Nursing staff orientation and training• Safe handling and disposal of chemotherapy agents
SPECIFICATIONS BY CATEGORY
DOCUMENTATIONThe facility completes the SAR. A minimum of 2 weeks(14 days) prior to the on-site visit, the facility provides thesurveyor with documentation that identifies the medicaloncology unit or functional equivalent. The surveyor visitsthe medical oncology unit or functional equivalent duringthe on-site visit.
RATING(1) Compliance: Depending on the category, an inpatient
medical oncology unit or a functional equivalent is inplace at the facility.
(5) Noncompliance: Depending on the category, aninpatient medical oncology unit or a functionalequivalent is not in place at the facility.
(8) Not applicable: Facility is exempt from this standard.
CATEGORYCATEGORYCATEGORYCATEGORYCATEGORY MEDICAL ONCOLOGY SERVICESMEDICAL ONCOLOGY SERVICESMEDICAL ONCOLOGY SERVICESMEDICAL ONCOLOGY SERVICESMEDICAL ONCOLOGY SERVICES
Network Cancer Program (NCP) One or more designated inpatient medical oncologyunit(s)
NCI-designated Comprehensive Cancer Program (NCIP) Designated inpatient medical oncology unit
Teaching Hospital Cancer Program (THCP) Designated inpatient medical oncology unit
Community Hospital Comprehensive Cancer Program Designated inpatient medical oncology unit or a(COMP) functional equivalent
Community Hospital Cancer Program (CHCP) Functional equivalent
Hospital Associate Cancer Program (HACP) Functional equivalent
Affiliate Hospital Cancer Program (AFCP) Exempt
Integrated Cancer Program (ICP) Functional equivalent
Freestanding Cancer Center Program (FCCP) Exempt
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
OTHER CLINICAL SERVICESStandard 4.3 AJCC staging is assigned by the managing physician and
recorded on a staging form in the medical record on 90 per-cent of eligible annual analytic cases.
DEFINITION AND REQUIREMENTSProper staging of cancer allows the physician to determineappropriate treatment. Staging enables the reliableevaluation of treatment results and outcomes reported fromvarious institutions on a local, regional, and national basis.
The cancer committee develops and documents a stagingpolicy and procedure. The policy and procedure guidelinesinclude, but are not limited to:• Acceptable methods for completion and signature• Definition of the managing physician• Placement of the staging forms in the medical record• Quality control of completeness and accuracy• Requirements for completion (if applicable)• Resolution of staging differences
The managing physician assigns the AJCC stage to 90percent of the annual analytic cases for which a stagingscheme exists.
Either clinical or pathologic staging is assigned to eachprimary. Both should be assigned if appropriate. Use thecriteria for clinical and pathologic staging outlined in thecurrent edition of the AJCC Cancer Staging Manual todetermine the appropriate stage.
Beginning January 1, 2005, a staging form is used todocument staging in the medical record. Use of the AJCCstaging forms is highly recommended.
The term “managing physician,” for the purposes ofrecording stage in the medical record, must be defined bythe cancer committee. More than one specialty may beinvolved in staging, depending on the need formultimodality treatment.
The patient’s managing physician evaluates all availablestaging information (x-rays, scans, lab tests, and operativeand pathology reports), records the staging elements (stagingclassification, T, N, M, and stage group) on the staging formin the medical record, and signs or initials the form.Electronic signatures are acceptable.
INPATIENT MEDICAL ONCOLOGY SERVICE REQUIREMENT BY CATEGORY

37
CLARIFICATION OF STAGING ROLESIn the medical record:The managing physician records the staging elements T,N, and M, and the stage group on the staging form in themedical record. The managing physician signs the stagingform. Forms that do not include the elements T, N, andM; the stage group; and the signature of the managingphysician do not meet the requirement for this standard.
The pathologist can contribute to the staging process byrecording the elements T, N, or M in the pathology reportof the specimen being examined and on the staging formin the medical record. The pathologist, however, cannotassign the stage group or sign the form.
Staging elements or stage group assigned by medicalstudents or residents, cancer registrars, or othernonphysician professionals and recorded on the stagingform in the medical record do not meet the requirementfor this standard.
In the cancer registry database:If the managing physician records the staging elements T,N, and M on the staging form, but has not recorded astage group, then the cancer registrar can assign a stagegroup based on the staging elements and record thisinformation in the cancer registry database. Completestaging information in the cancer registry database doesnot meet the requirement for this standard.
Accurate staging is essential for accurate evaluation of
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
Standard 4.4 Nursing care is provided by nurses with specialized knowledge andskills in oncology. Competency is evaluated annually.
Standard 4.5 An Oncology Nurse Manager or a Registered Nurse (RN) providesdirection to the inpatient medical oncology unit or the functionalequivalent as appropriate to the category.
DEFINITION AND REQUIREMENTSThe complex needs of cancer patients and their familiesrequire specialized oncology nursing knowledge and skillsto achieve optimal patient care outcomes.
The oncology nurse is an integral member of themultidisciplinary team. Oncology nursing services aremanaged by a registered nurse who has appropriateexperience and educational background to provide effectiveleadership and direction to the nurses providing care tocancer patients and their families.
A clinical expert in oncology nursing can be:• A master’s prepared oncology clinical nurse specialist• A nurse practitioner• An Oncology Certified Nurse (OCN)
As appropriate to the category, an oncology nurse managerprovides day-to-day direction to staff of the medicaloncology unit. An oncology nurse manager is an RN with
three years’ clinical experience and at least one year inoncology nursing. An OCN is preferred. An RN providesday-to-day direction to staff of a functional equivalent.
Orientation and annual competency of oncologyknowledge and skills are documented for nurses providingcare to oncology patients. Adequate staffing by oncologynurses is provided to meet the needs of cancer patients andfamilies. Staffing needs are evaluated by the nursingadministration at least annually.
Oncology Nursing Society standards and guidelines for allaspects of patient care, professional practice, research,education, and administrative topics should be used whendeveloping the facility standards and guidelines. Oncologynursing policies and procedures are documented andapproved by the nursing administration in consultation withthe cancer committee. Standards are reviewed and revised bythe nursing administration in consultation with the cancercommittee as needed on an annual basis.
patient outcomes. The cancer committee should monitorand improve the accuracy of AJCC staging assigned by themanaging physician and recorded on a staging form in themedical record so that 90 percent of the cases are stagedcorrectly. Staging accuracy is not rated at this time.
SPECIFICATIONS BY CATEGORYAll cancer programs must fulfill this standard.
DOCUMENTATIONThe facility completes the SAR. A minimum of 2 weeks (14days) prior to the on-site visit, the facility provides the surveyorwith a copy of the written policy and procedure for physicianstaging. During the on-site visit, the facility provides medicalrecords and abstracts for a random sample of analytic cases fromthe last complete year of abstracting for review by the surveyorduring the on-site visit. A minimum of 25 medical records willbe reviewed.
RATING(1+) Commendation: The managing physician assigns AJCC staging
and records it on the staging form in the medical record formore than 95 percent of eligible annual analytic cases.
(1) Compliance: The managing physician assigns AJCC stagingand records it on the staging form in the medical record for90 percent of eligible annual analytic cases.
(5) Noncompliance: The managing physician assigns AJCCstaging and records it on the staging form in the medicalrecord for less than 90 percent of eligible annual analytic cases.

38
CATEGORY STANDARD 4.4 STANDARD 4.5
Network Cancer Program (NCP) Required Oncology Nurse Manager
NCI-designated Comprehensive Cancer Program (NCIP) Required Oncology Nurse Manager
Teaching Hospital Cancer Program (THCP) Required Oncology Nurse Manager
Community Hospital Comprehensive Cancer Program (COMP) Required Oncology Nurse Manager(designated unit)orRegistered Nurse(functional equivalent)
Community Hospital Cancer Program (CHCP) Required Registered Nurse
Hospital Associate Cancer Program (HACP) Required Registered Nurse
Affiliate Hospital Cancer Program (AFCP) Required Exempt
Integrated Cancer Program (ICP) Required Exempt
Freestanding Cancer Center Program (FCCP) Required Exempt
Standard 4.6 The guidelines for patient management and treatment cur-rently required by the CoC are followed.
SPECIFICATIONS BY CATEGORY
DOCUMENTATIONThe facility completes the SAR. During the on-site visit,the facility provides the surveyor with:• An organizational chart or staff list noting credentials of
the clinical expert(s).• Documentation of orientation and annual competency
evaluation for each oncology nurse.• Documentation of nursing management of the medical
oncology unit or functional equivalent as appropriate tothe category.
RATINGStandard 4.4(1) Compliance: Nurses with specialized oncology knowl-
edge and skills in oncology are available at the facility.Documentation is available to verify annual competency.
(5) Noncompliance: Nurses with specialized oncologyknowledge and skills in oncology are not available atthe facility and/or documentation is not available toverify annual competency.
Standard 4.5(1) Compliance: Based on the category, an oncology nurse
manager provides day-to-day direction for the inpa-tient medical oncology unit, or an RN provides day-to-day direction to the functional equivalent.
(5) Noncompliance: Based on the category, an oncologynurse manager does not provide day-to-day directionfor the inpatient medical oncology unit, or an RNdoes not provide day-to-day direction to the func-tional equivalent.
(8) Not Applicable: The facility is exempt from thisstandard.
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
DEFINITION AND REQUIREMENTSPatient management and treatment guidelines promote anorganized approach to providing quality care.
The CoC requires that 90 percent of pathology reports thatinclude a cancer diagnosis will contain the scientificallyvalidated data elements outlined on the surgical casesummary checklist of the College of American Pathologists(CAP) publication, Reporting on Cancer Specimens.
In addition to CoC required guidelines, the cancercommittee should review and consider adoption of other
Policies and procedures include, but are not limited to:
• Administration and safe handling of cytotoxic agents• Blood product administration• Care of immunocompromised patients
• Management of vascular access devices• Oncologic emergencies• Radiation safety• Symptom management
guidelines appropriate to the patients diagnosed andtreated by the facility.
National organizations have developed cancer-focusedguidelines. These organizations include, but are notlimited to:• American Cancer Society• American College of Surgeons• American Head and Neck Society• American Society of Clinical Oncology• American Urological Association
ONCOLOGY NURSING SERVICE REQUIREMENTS BY CATEGORY

39
• Association of Community Cancer Centers• College of American Pathologists• The National Cancer Institute• The National Comprehensive Cancer Network• Oncology Nursing Society• Society of Surgical Oncology
Other guidelines adopted by the cancer committee for useby the facility are documented in cancer committee minutes.
The cancer committee monitors and reports compliancewith the patient management and treatment guidelinescurrently required by the CoC as well as others adopted foruse by the facility. At a minimum, the pathology reportsfor a random sample of 10 percent of the annual analyticcases or a maximum of 300 cases are reviewed each year todocument compliance with this standard.
SPECIFICATIONS BY CATEGORYAll cancer programs must fulfill this standard.
DOCUMENTATIONThe facility completes the SAR. During the on-site visit,the facility provides the surveyor with:
• The pathology report format for the major cancerexperience(s) at the facility showing the inclusion of thescientifically proven data elements.
Standard 4.7 Rehabilitation services are provided on-site or by referral. This isevaluated on an annual basis.
• Documentation of the monitoring of and compliancewith the patient management and treatment guidelinescurrently required by the CoC as well as others adoptedfor use by the facility.
The surveyor will evaluate compliance with this standardby reviewing the medical records and abstracts for arandom sample of analytic cases for the last complete yearof abstracting. A minimum of 25 medical records will bereviewed.
RATING(1+) Commendation: Ninety (90) percent of cancer
pathology reports include the scientifically validateddata elements as outlined in the CAP protocols, andguidelines from national organizations (other thanCAP) are followed.
(1) Compliance: Ninety (90) percent of cancer pathologyreports include the scientifically validated data ele-ments as outlined in the CAP protocols.
(5) Noncompliance: Ninety (90) percent of cancerpathology reports do not include the scientificallyvalidated data elements as outlined in the CAPprotocols and/or not all of the scientifically validateddata elements as outlined in the CAP protocols areincluded on cancer pathology reports.
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
DEFINITION AND REQUIREMENTSRehabilitation services help patients cope with activities ofdaily living affected by the cancer experience and enablesthem to resume normal activities. The cancer committeedocuments policies and procedures to access rehabilitationservices.
Rehabilitation services include, but are not limited to:• Career counseling• Physical therapy• Speech therapy• Stomal therapy
The cancer committee evaluates the needs of their patientson an annual basis and offers services that can be used by amajority of patients as well as those targeting specialpopulations. Results of the annual evaluation aredocumented in cancer committee minutes.
SPECIFICATIONS BY CATEGORYAll cancer programs must fulfill this standard.
DOCUMENTATIONThe facility completes SAR. During the on-site visit, thefacility provides the surveyor with:
• Documentation of rehabilitation services available on-site or by referral.
• The process for access to rehabilitation services.• Documentation of the annual evaluation of the
rehabilitation services.• Patient brochures or other materials that outline
rehabilitation services.
RATING(1) Compliance: Rehabilitation services are provided on-
site or by referral, and documentation of the annualevaluation of these services is available.
(5) Noncompliance: Rehabilitation services are notprovided on-site or by referral, and/or documentationof the annual evaluation of these services is notavailable.

40

Chapter
41
5
ResearchPurpose: The standards promote advancement in cancer treatment through the
provision of clinical trial information and patient accrual to cancer-related clinical trials.
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
CLINICAL TRIAL INFORMATIONStandard 5.1 Information about the availability of cancer-related clinical trials is
provided to patients through a formal mechanism.
DEFINITION AND REQUIREMENTSBy providing information about the availability of cancer-related clinical trials, the facility offers patients theopportunity to participate in the advancement of evidence-based medicine.
A formal mechanism is established to provide informationabout cancer-related clinical trials to patients seen at the facility.
Methods to provide information include, but are notlimited to:• Access to the Internet or Internet search services through
the patient library• Articles in facility newsletters• Pamphlets or brochures in patient waiting rooms or
patient information packets
The cancer committee documents the mechanism andmonitors the effectiveness of the formal mechanismannually, making revisions as needed. The review isdocumented in cancer committee minutes.
SPECIFICATIONS BY CATEGORYAll cancer programs must fulfill this standard.
DOCUMENTATIONThe facility completes the Survey Application Record(SAR). During the on-site visit, the facility provides thesurveyor with documentation of policies and procedures forproviding information about cancer-related clinical trials topatients or samples of written/printed information providedto patients to the surveyor during the on-site visit.
RATING(1) Compliance: A formal mechanism is used to provide
information to patients about cancer-related clinical trials.
(5) Noncompliance: A formal mechanism is not used toprovide information to patients about cancer-relatedclinical trials.
CLINICAL TRIAL ACCRUALStandard 5.2 As appropriate to the category, the required percentage of cases
is accrued to cancer-related clinical trials on an annual basis.
DEFINITION AND REQUIREMENTSClinical research advances science and ensures that patientcare approaches the highest possible level of quality.
Facilities that accrue patients to cancer-related clinicalresearch enter at least the minimum percentage based onthe category and number of annual analytic accessions.Patients eligible to meet this standard are those:• Seen at the facility for diagnosis and/or treatment and
placed on a trial through the facility.• Seen at the facility for diagnosis and/or treatment and
placed on a trial through the office of a staff physician.• Seen at the facility for diagnosis and/or treatment and
placed on a trial through another facility.
• Seen at the facility for any reason and placed on aprevention or cancer control trial.
Basic scientific research is generally conducted incancer centers supported by grants from theNational Cancer Institute (NCI) or in academichealth centers. Research in community hospitalstypically involves cancer control protocols ortreatment trials.
Treatment-related clinical trial groups include, butare not limited to:• NCI-sponsored programs such as the
Community Clinical Oncology Program(CCOP) or Cooperative Group OutreachProgram (CGOP)

42
• Cooperative Trial Groups such as the American Collegeof Surgeons Oncology Group (ACOSOG)
• University-related research• Pharmaceutical company research (Phase IV)• Locally developed, peer-reviewed studies
Cancer control research studies include, but are not limited to:• Primary prevention (ie, Study of Tamoxifen and
Raloxifene [STAR])• Early detection• Quality of life• Economics of care
Facilities participating in clinical research show that anindependent peer review mechanism consistent with national
standards is in place and used. Research projects involvingparticipation by human subjects must be approved by aninternal or external Institutional Review Board (IRB).Patients participating in clinical trials must give theirinformed consent.
A data manager is available to assist with enrolling patients,monitoring patient accrual, and identifying and providinginformation/education about new trials in NetworkCancer Programs, NCI-designated Comprehensive CancerPrograms, and Teaching Hospital Cancer Programs. Adata manager may also be available at facilities in othercategories accruing a large number of patients to cancer-related clinical trials.
Patient accrual is monitored and the results aredocumented in cancer committee minutes.
SPECIFICATIONS BY CATEGORY
MINIMUM REQUIRED PERCENTAGE COMMENDATION PERCENTAGECATEGORY ACCRUAL TO CLINICAL TRIALS ACCRUAL TO CLINICAL TRIALS
Network Cancer Program (NCP) 6% of the number of annual 8% of the number of annualanalytic cases analytic cases
NCI-designated Comprehensive 10% of the number of annual 15% of the number of annualCancer Program (NCIP) analytic cases analytic cases
Teaching Hospital Cancer Program (THCP) 4% of the number of annual 6% of the number of annualanalytic cases analytic cases
Community Hospital Comprehensive 2% of the number of annual 4% of the number of annualCancer Program (COMP) analytic cases analytic cases
Community Hospital Cancer Exempt 2% of the number of annualProgram (CHCP) analytic cases
Hospital Associate Cancer Program (HACP) Exempt 2% of the number of annualanalytic cases
Affiliate Hospital Cancer Program (AFCP) Exempt 2% of the number of annualanalytic cases
Integrated Cancer Program (ICP) Exempt 2% of the number of annualanalytic cases
Freestanding Cancer Center Program (FCCP) Exempt 2% of the number of annualanalytic cases
DOCUMENTATIONThe facility completes the SAR. The surveyor discusses theclinical trials program with the cancer program teamduring the on-site visit.
RATING(1+) Commendation: The commendation percentage of
cases for the category is accrued to cancer-relatedclinical trials each year.
(1) Compliance: The required percentage of cases forthe category is accrued to cancer-related clinical trialseach year.
(5) Noncompliance: Less than the required percentage ofcases for the category is accrued to cancer-relatedclinical trials each year.
(8) Not Applicable: The facility is exempt from thisstandard.
MINIMUM REQUIRED AND COMMENDATION CLINICAL TRIAL ACCRUAL PERCENTAGE FOR EACH CATEGORY

Chapter
43
6
Community OutreachPurpose: The standards ensure that supportive services and prevention and
early detection opportunities are provided to cancer patients andtheir families.
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
SUPPORTIVE SERVICESStandard 6.1 Supportive services are provided on-site or coordinated with local
agencies and facilities.
DEFINITION AND REQUIREMENTSTotal patient care extends beyond that provided byphysicians and nurses. Supportive services help patientsand their families cope with changes resulting from acancer diagnosis.
Supportive services address the needs of the majority ofpatients as well as provide for special populations or needs.The supportive services offered on-site will vary dependingon the scope of the facility, local staff expertise, and patientmix. Supportive services not provided on-site are providedthrough referral to other facilities and/or local agenciessuch as the American Cancer Society.
Supportive services include, but are not limited to:• Genetic testing and counseling• Grief counseling• Home care and/or hospice• Nutritional counseling• Pastoral services• Reference library• Support groups
Patient assessment, discharge planning, and referral shouldbegin on the day of admission and is documented in thepatient chart and/or in team minutes.
Procedures are followed to ensure that patient needs are antici-pated and managed. The process includes the mechanism to:• Evaluate patient needs
• Facilitate direct access or referral• Monitor quality• Evaluate the effectiveness of the access and referral
process
SPECIFICATIONS BY CATEGORYAll programs must fulfill this standard.
DOCUMENTATIONThe facility completes the Survey Application Record(SAR). During the on-site visit, the facility provides thesurveyor with documentation of the supportive servicesoffered to patients and their families available on-site or byreferral. Documentation includes, but is not limited to:• Published brochures or flyers• Meeting schedules• Electronic media such as Internet or Intranet postings
The surveyor will discuss the community outreachprogram with the designated coordinator (Cancer LiaisonPhysician) and cancer committee members during the on-site visit.
RATING(1) Compliance: Supportive services are available on-site
or coordinated with other facilities or local agencies.
(5) Noncompliance: Supportive services are either notavailable on-site or not coordinated with other facili-ties or local agencies.
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
PREVENTION AND EARLY DETECTION PROGRAMSStandard 6.2 Each year, two prevention or early detection programs are provided
on-site or coordinated with other facilities or local agencies.
DEFINITION AND REQUIREMENTSPrevention programs use strategies to modify attitudes andbehaviors to reduce the risk of developing a malignancy.Early detection discovers cancer at an early stage when theapplication of prompt treatment can increase survival anddecrease morbidity.
Prevention and early detection programs are offered atscheduled intervals as defined by the cancer committeeand the designated Community Outreach Coordinator.Prevention and early detection programs are provided on-site or coordinated with other facilities and/or localagencies such as the American Cancer Society.

44
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
SPECIFICATIONS BY CATEGORYAll cancer programs must fulfill this standard.
DOCUMENTATIONThe facility completes the SAR. During the on-site visit,the facility provides the surveyor with copies of cancercommittee minutes or other sources that document themethods to monitor and evaluate the community outreachactivities. The surveyor will discuss the communityoutreach program with the designated coordinator (CancerLiaison Physician) and cancer committee members duringthe on-site visit.
RATING(1) Compliance: Community outreach activities are
monitored each year. The findings are documented.
(5) Noncompliance: Community outreach activities arenot monitored each year and/or the findings are notdocumented.
Prevention programs include, but are not limited to:• Chemoprevention programs (ie, Study of Tamoxifen
and Raloxifene [STAR])• Skin cancer prevention (ie, Slip, Slap, Slop)• Smoking cessation• Smoking prevention in adolescents
Early detection programs include, but are not limited to:• Breast care education• Colonoscopy, flexible sigmoidoscopy, or Hemoccult
stool testing• PAP testing• Prostate exams with or without PSA testing• Screening mammography and clinical exams• Skin surveys• Surveillance of high risk groups
SPECIFICATIONS BY CATEGORYAll programs must fulfill this standard.
DOCUMENTATIONThe facility completes the SAR. During the on-site visit,the facility provides the surveyor with documentation oftwo annual prevention or early detection programsthrough cancer committee minutes or other sources. Thesurveyor will discuss the community outreach programwith the designated coordinator (Cancer LiaisonPhysician) and cancer committee members during the on-site visit.
RATING(1+) Commendation: Three or more prevention or early
detection programs are offered each year, either on-siteor coordinated with other facilities or local agencies.
(1) Compliance: Two prevention or early detectionprograms are offered each year either on-site orcoordinated with other facilities or local agencies.
(5) Noncompliance: Two prevention or early detectionprograms are not offered each year either on-site orcoordinated with other facilities or local agencies.
MONITORING COMMUNITY OUTREACHStandard 6.3 The cancer committee monitors the community outreach
activities on an annual basis. The findings are documented.
DEFINITION AND REQUIREMENTSSupportive services, prevention, and early detectionprograms are monitored to ensure that appropriate servicesare provided to patients and the community.
Both the scope of services and the methods to access servicesand programs are evaluated annually. The methods used tomonitor outreach activity are set by the cancer committeeand are documented in cancer committee minutes.
The assigned coordinator (Cancer Liaison Physician)monitors outreach activity, reports regularly to the cancercommittee, and recommends corrective action if activityfalls below the annual goal or requirements. The resultsand recommendations are documented in cancercommittee minutes.
In some facilities, the community outreach coordinatorworks cooperatively with established departments or staffleadership to coordinate, monitor, and recommendimprovements to community outreach programs. In thisinstance, the Cancer Liaison Physician acts as the cancercommittee liaison to the established departments or staffleadership.

Chapter
45
7
Professional Education and Staff SupportPurpose: The standards promote increased knowledge through annual
educational programs and registry staff participation in local,regional, or national educational activities.
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
FACILITY-BASED EDUCATIONStandard 7.1 Other than cancer conferences, the cancer committee offers one
cancer-related educational activity each year.
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
DOCUMENTATIONThe facility completes the Survey ApplicationRecord (SAR). During the on-site visit, the facilityprovides the surveyor with documentation ofcontinuing education activity for each member ofthe cancer registry staff.
RATING(1+) Commendation: The cancer registry staff who
are CTRs attend a national cancer-relatededucational activity annually.
(1) Compliance: Other than cancer conference, allmembers of the cancer registry staff participatein a local, state, regional, or national cancer-related educational activity annually.
(5) Noncompliance: Other than cancer conference,all members of the cancer registry staff do notparticipate in a local, state, regional, or nationalcancer-related educational activity annually.
SPECIFICATIONS BY CATEGORYAll programs must fulfill this standard.
DOCUMENTATIONThe facility completes the Survey Application Record(SAR). During the on-site visit, the facility provides thesurveyor with documentation of an annual educationalactivity other than cancer conferences, including apublished notice or agenda.
RATING(1) Compliance: Other than cancer conferences, the
cancer committee offers a cancer-related educationalactivity each year.
(5) Noncompliance: Other than cancer conferences, thecancer committee does not offer a cancer-relatededucational activity each year.
DEFINITION AND REQUIREMENTSEducational activities ensure that members of the cancercare team possess current knowledge of cancer prevention,early detection, diagnosis, treatment, and follow-up care.
The cancer committee offers a cancer-related educationalactivity to all members of the medical staff and alliedhealth professionals each year. As appropriate, AJCCstaging is part of the cancer-related educational activity.The cancer committee may coordinate this activity withthe facility’s continuing education department, medicalstaff office, or other department as appropriate.
This includes, but is not limited to:• An educational symposium• A lecture on a cancer-related topic• A video conference
CANCER REGISTRY STAFF EDUCATIONStandard 7.2 Other than cancer conferences, all members of the cancer
registry staff participate in a local, state, regional, or nationalcancer-related educational activity each year.
DEFINITION AND REQUIREMENTSOngoing cancer-related education enhances knowledge and skills.
To facilitate accurate data collection and gain or maintaintheir credentials, all members of the cancer registry staffparticipate in ongoing cancer-related education at thelocal, state, regional, or national level. This includes, but isnot limited to:• Advances in cancer diagnosis and treatment• Changes in cancer program standards• Changes in data collection requirements
Educational activities include, but are not limited to:• A cancer-related lecture• A local, state, regional, or national meeting or workshop• A video conference• A Web-based training module
SPECIFICATIONS BY CATEGORYAll programs must fulfill this standard.

46

Chapter
47
8
Quality ImprovementPurpose: The standards ensure that cancer services, care, and patient outcomes
are evaluated and improved so that patients receive care that iscomparable to national standards.
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
STUDIES OF QUALITY AND OUTCOMESStandard 8.1 Each year, based on category, the cancer committee completes and
documents the required studies that measure quality and outcomes.
DEFINITION AND REQUIREMENTSThe annual evaluation of services and care provides abaseline to measure quality and an opportunity to corrector enhance patient outcomes.
The cancer committee focuses on quality-related issuesrelevant to the facility and local patient population andany area of cancer program activity. Studies of qualityshould include patient outcomes, if appropriate. Survivalanalysis is the preferred method; however, other outcomemeasures may be selected at the discretion of the cancercommittee.
For each quality study, the cancer committee is responsible for:• Establishing the study topic.• Defining quality measures to evaluate the topic.• Evaluating the data related to the quality measures.• Designing and initiating actions based on the evaluation
of the data.• Monitoring the effectiveness of action plans and all
cancer-related quality improvement activities at thefacility.
Examples of study topics include, but are not limited to:• What is the processing turnaround for ERA/PRA results
on breast cancer specimens, and does this meet the needsof the physician?
• Why are cases not staged using the AJCC system?• Is the evaluation and management of pain adequate in
our patient population?• Is the same level of care provided to English and non–
English-speaking patients?
Considering the following questions may help to design,conduct, and evaluate a study.
What is the problem? How is quality measured? How areproblems defined? What is the scope of the problem?Who/what are affected by the problem? What is the sourceof the problem?
What should be done to address the problem?What initiatives/interventions are needed?
How effective was the intervention, and howcould further improvements be made in thefuture? Were goals accomplished? What waslearned?
A summary of each study’s findings, analysis,recommendations, and the process to implementchanges in program activity is documented incancer committee minutes. The documentationincludes:• The study topic• Criteria for evaluation• A summary of the findings• The actions recommended• Follow-up steps to monitor the actions
implemented
The methods used to monitor studies of quality areset by the cancer committee and documented incancer committee minutes.
The assigned coordinator monitors activity relatedto studies of quality, reports regularly to the cancercommittee, and recommends corrective action ifany area falls below the annual goal or require-ments. The results and recommendations aredocumented in cancer committee minutes.
Note that duplicated study topics and criteria, andongoing monitoring without analysis of thefindings, does not fulfill this standard. Based onstudy criteria, the CoC will determine if CoC-designed special studies will fulfill this standard.This information will be documented in CoCcommunications to programs selected toparticipate.
Examples of studies of quality and outcomes appearat the end of this chapter.

CATEGORYCATEGORYCATEGORYCATEGORYCATEGORY NUMBER AND TYPE OF STUDIESNUMBER AND TYPE OF STUDIESNUMBER AND TYPE OF STUDIESNUMBER AND TYPE OF STUDIESNUMBER AND TYPE OF STUDIES
Network Cancer Program (NCP) 1 study based on registry data2 additional studies
NCI-designated Comprehensive Cancer Program (NCIP) 1 study based on registry data2 additional studies
Teaching Hospital Cancer Program (THCP) 1 study based on registry data1 additional study
Community Hospital Comprehensive Cancer Program 1 study based on registry data(COMP) 1 additional study
Community Hospital Cancer Program (CHCP) 1 study based on registry data1 additional study
Hospital Associate Cancer Program (HACP) 1 study based on registry data1 additional study
Affiliate Hospital Cancer Program (AFCP) 1 study of any topic in cooperation withhospital partner
Integrated Cancer Program (ICP) 1 study based on registry data1 additional study
Freestanding Cancer Center Program (FCCP) 1 study based on registry data1 additional study
SPECIFICATIONS BY CATEGORY
DOCUMENTATIONThe facility completes the Survey Application Record(SAR). During the on-site visit, the facility provides thesurveyor with summaries of each year’s studies, analyses,recommendations, and follow-up.
RATING(1) Compliance: Each year, the cancer committee com-
pletes and documents the required studies that mea-sure quality and outcomes as appropriate to category.
(5) Noncompliance: Each year, the cancer committee doesnot complete and/or document the required studies thatmeasure quality and outcomes as appropriate to category.
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
PATIENT CARE IMPROVEMENTStandard 8.2 Annually, the cancer committee implements two improvements
that directly affect cancer patient care. The improvementsare documented.
DEFINITION AND REQUIREMENTSQuality or performance improvements are the actions taken,processes implemented, or services created to improvepatient care. Implementation of improvements demonstratesa program’s continuous commitment to providing high-quality cancer care. The results of a study of quality providea baseline to measure and improve quality.
Sources for improvements include, but are not limited to:• Actions based on analysis of a study• Actions to address undesirable performance• Changes to improve acceptable performance• Additional programs or services addressing patient needs
or staff concerns
The methods used to monitor the quality improvementprogram are set by the cancer committee and documentedin cancer committee minutes.
The assigned coordinator monitors activity related to the qualityimprovement program, reports regularly to the cancer
committee, and recommends corrective action if any area fallsbelow the annual goal or requirements. The results andrecommendations are documented in cancer committee minutes.
SPECIFICATIONS BY CATEGORYAll programs must fulfill this standard.
DOCUMENTATIONThe facility completes the SAR. During the on-site visit,the facility provides the surveyor with summaries of eachyear’s patient care improvements.
RATING(1+) Commendation: More than two improvements that
directly affect patient care are implemented anddocumented each year.
(1) Compliance: Two improvements that directly affectpatient care are implemented and documented each year.
(5) Noncompliance: Two improvements that directlyaffect patient care are not implemented and/or docu-mented each year.
48
THE NUMBER AND TYPE OF STUDIES TO BE COMPLETED EACH YEAR FOR EACH CATEGORY

EXAMPLES OF COMPLETED STUDIES AND IMPROVEMENTSSAMPLE STUDY 1: STUDY USING FACILITY DATA
Study topic: Are treatment alternatives for prostate cancer patients available at this facility?Presented to cancer committee 3/02.
Criteria: Investigate the number of patients with local prostate cancer who would beeligible for seed implants as an alternative to surgery.
Findings: 115/127 (90 percent) patients diagnosed in 2001 were eligible for seed implants.Reviewed the number of cases from 1995–2000 treated with surgery that wereeligible for alternative therapy. Found 455/645 (70 percent) eligible for thesurgical alternative. Results presented to the cancer committee 12/02.
Recommendations: The cancer committee recommended that a seed implant program for prostatecancer and multidisciplinary prostate clinic program be established.
Improvement: Beginning in January 2003, urology worked with radiation oncology to develop aseed implant program for prostate cancer patients. Budget requests were approvedand renovations begun. A multidisciplinary prostate clinic was opened in August2003. Marketing undertook promotional efforts (informational pamphlets andnewspaper articles) announcing the new clinic.
SAMPLE STUDY 2: STUDY USING THE NATIONAL CANCER DATA BASE (NCDB) BENCHMARK REPORTS
Study topic: Are patients with ductal carcinoma in situ (DCIS) receiving breast conservationservices? Presented to cancer committee 1/03.
Criteria: Breast-conserving surgery along with postoperative radiation is the treatment ofchoice for DCIS.
Methodology: Analyzed the cancer registry data to compare percentages of patients who receivedbreast conservation surgery to those who had more radical surgical treatment byresidence within hospital market.
Findings: 15/25 (60 percent) of the DCIS patients were treated with breast conservingsurgery (BCS) in 2001. When broken down by residence within hospital market,that percentage is higher (13/18 or 72.2 percent). Seven patients were referredfrom outside the facility’s market area. Two of these patients were located inmarkets with radiation facilities available; five were from rural locations, morethan 50 miles from any facility to which they could be referred for radiationtherapy postoperatively.
Recommendations: The cancer committee reviewed the findings in light of the benchmarkestablished within the 1999 NCDB. That percentage was reported to be 69percent, up slightly from 68.8 percent in 1998. Last year, the Cancer Committeerecommended expansion of radiation services for breast cancer patients seen atthe facility.
Improvement: The clinic added evening hours during the week and is now open on Saturday.Since this change, treatment of breast cancer patients has increased by 30 percentin the last year.
49

50

Chapter
51
CoC Resources and Tools
The following are resources
and tools for cancer programs
available on the Cancer
Programs pages of the
American College of Surgeons
Web site (www.facs.org).
SURVEY-RELATED RESOURCES• Appeals Process
• CoC-Trained Independent Cancer Consultant List
• Deficiency Resolution Documentation
• Guidelines for Merged Programs
• Guidelines for Network Cancer Programs
• Information for CoC Special Studies
• NCDB Case Submission, Transmission FileSpecifications/Format
• NCDB Hospital Edit Report Documentation
• Sample Approved Cancer Program Performance Report
CANCER PROGRAM TRACKING TOOLS• AJCC Staging Quality Control Tool
• Cancer Conference Grid
• Cancer Registry Abstracting Quality Control Tool
• Pathology Report Quality Control Tool
OTHER CANCER PROGRAM RESOURCES• ACS Publications and Services Catalog
• Benefits of Being an Approved Cancer Program
• Benefits of Being an Approved Cancer ProgramNetwork
• Cancer Liaison Physician Membership Criteria andMembership Application
• CoC Cancer Program Data Standards
• Facility Information Profile System (FIPS)
• Find an Approved Cancer Program Near You
• How are Cancer Programs Approved?
• How to Start an Approved Cancer Program
• Inquiry and Response (I&R) System
• NCDB Benchmark Reports
• Quality Improvement Best Practices in CoC-ApprovedCancer Programs
• What is an Approved Cancer Program?
for Cancer Programs

52

American College of Surgeons633 N. Saint Clair St.
Chicago, IL 60611-3211