Embed Size (px)
Citation preview

Commentary:
Priming of alloreactive T cells – where does ithappen?
Dela Golshayan and Robert Lechler
Department of Immunology, Imperial College, Hammersmith Hospital, London, UK
Host lymphocytes can recognize alloantigens directly on transplanted donor tissue or
indirectly after these antigens are processed and presented on host APC. Here, we outline the
features of alloresponses that distinguish them from responses to conventional antigens,
then we discuss various study systems that have examined where the priming of alloreactive
CD4+ and CD8+ T cells occurs. Finally, we discuss the implications of recent data which
suggest that direct responses originate in the graft itself whereas indirect responses are
initiated in the draining lymph nodes.
See accompanying article: http://dx.doi.org/10.1002/eji.200425309
Key words: Transplantation / Allorecognition / Direct and indirect pathways
1 Introduction
Whether adaptive immune responses to transplant
antigens are initiated within the organized structures of
secondary lymphoid organs or in the graft itself has long
been amatter of debate among transplant immunologists
[1, 2]. Several recent studies have attempted to
determine where alloreactive T cells are primed in
response to the placing of an allograft in vivo. The latest
of these studies is published in this issue of the European
Journal of Immunology [3] and adds an additional
dimension to this controversial question by the indepen-
dent analysis of direct and indirect alloresponses (Fig. 1).
2 Features that distinguish alloresponsesfrom responses to conventional antigens
Before considering any of the reported experiments in
detail, it is worth emphasizing that, in general, allor-
esponses are not qualitatively different from conventional
responses to protein antigens. Consequently it is
reasonable to assume that professional APC, namely
DC, are pre-eminent in the initiation of the immune
response against transplantation antigens. Naive T cells
respond to foreign antigens if these antigens are
presented in the context of appropriate co-stimulatory
signals and within secondary lymphoid organs because
these cells are inefficient at crossing vascular endothe-
lium to enter peripheral tissues [4]. This implies that, as
classically described for responses to microbial antigens
[5], the first meeting point between host naive Tcells and
transplant antigens, leading to the initiation of the
alloresponse, would be in the secondary lymphoid
organs rather than in the transplanted tissue itself.
There are however unique features of the immune
response in the transplant setting. First, the grafted
tissue contains its own APC that can trigger direct-
pathway alloresponses. In the early stages after trans-
plantation, tissue-resident antigen-loaded donor imma-
ture DC will migrate out of the graft via the blood and/or
lymph towards secondary lymphoid organs (graft-drain-
ing lymph nodes and spleen) where they will mature and
encounter recipient resting T cells. The trafficking and
maturation of donor DC is triggered by pro-inflammatory
signals produced as a result of tissue injury in the early
post-transplant period and is the cornerstone for the
initiation of effective adaptive immune responses [6]. A
second distinguishing feature of alloimmune responses is
that they involve two pathways, direct and indirect, as
illustrated in Fig. 1. We proposed over two decades ago
that, once donor bone-marrow-derived APC are de-
pleted, the immune response against an allograft is
maintained by indirect-pathway allospecific T cells [7].
The indirect pathway involves allogeneic MHCmolecules
that are shed from the graft being taken up, processed
and presented as peptides by recipient APC to the Tcells
circulating between secondary lymphoid organs.
[DOI 10.1002/eji.200425506]
Received 27/7/04Revised 31/8/04Accepted 1/9/04
Abbreviation: EC: Endothelial cell
Eur. J. Immunol. 2004. 34: 3301–3304 Priming of alloreactive T cells 3301
f 2004 WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim www.eji.de
When analyzing the location of Tcell priming and the type
of APC involved, there is a second issue to consider,
namely that the memory subset of circulating T cells
contributes to primary alloresponses. In adult humans,
where memory Tcells account for a bigger proportion of
the alloreactive T cell repertoire as compared with
experimental rodent models, approximately 50% of the
T cells responding in the ‘primary’ mixed-leukocyte
reaction are pre-existing memory cells. This reflects the
fact that direct alloresponses result from a cross-reaction
by Tcells with specificity for complexes of self-MHC with
peptide [8–10]. As memory T cells have different homing
patterns and have less-stringent activation requirements,
their involvement may help to explain the rapidity and
vigor of in vivo alloresponses.
However, this raises a further issue, namely the role of
graft parenchymal cells in priming and maintaining direct
pathway alloresponses. Activated vascular endothelial
cells (EC) express MHC class I and II as well as
expressing adhesion molecules. But these non-profes-
sional APC may be limited in their ability to effectively
activate Tcells, because of their limited expression of co-
stimulatory molecules and the brevity of the encounter
between T cells and EC. Indeed, alloantigen recognition
on graft parenchymal cells was shown in some in vitro
studies to induce allospecific T cell hyporesponsiveness
rather than activation [11, 12]. These findings were also
supported in vivo by the fall observed in the frequency of
T cells with direct anti-donor specificity in renal and
cardiac transplant patients [13]. Other studies have
challenged these conclusions by showing that EC could
induce the proliferation of allogeneic T cells and their
differentiation into effector Tcells, albeit during a five-day
in vitro co-culture [14, 15]. EC may also play a role in the
local recruitment and maturation of circulating host
monocytes into efficient APC [16]. It is true that, in the
setting of primarily vascularized allografts, EC of donor
origin offer a unique interface for donor–recipient cross-
talk during the lifetime of the organ and it is attractive to
hypothesize that they are implicated in acute and/or
chronic graft rejection, if not as initiators at least as
targets.
3 Systems used to study where alloreactiveT cells are primed
Turning to the various studies that have addressed the
anatomy of alloreactive T cell priming, there are several
important points that need to be borne in mind in the
interpretation of the reported results.
The first is that some studies have used skin allografts in
which the vascular endothelium is host, not donor,
derived [1, 17]. Other reports have used cardiac or renal
allografts, in which the vascular endothelium is of donor
origin [2, 18–21]. This has obvious implications for
alloantigen encounter by circulating Tcells. As previously
discussed, it remains a point of debate as to whether the
luminal surface of the vascular endothelium is a possible
site of T cell priming but, in theory at least, T cells
circulating in the bloodstream have the opportunity to
encounter alloantigens on the graft EC. If not activating
the T cells directly, by displaying graft alloantigens, EC
could promote the recruitment and selective transmigra-
tion of antigen-specific T cells at the site of inflammation
[22].
Second, the experimental systems used to address this
issue have varied enormously in terms of the frequency of
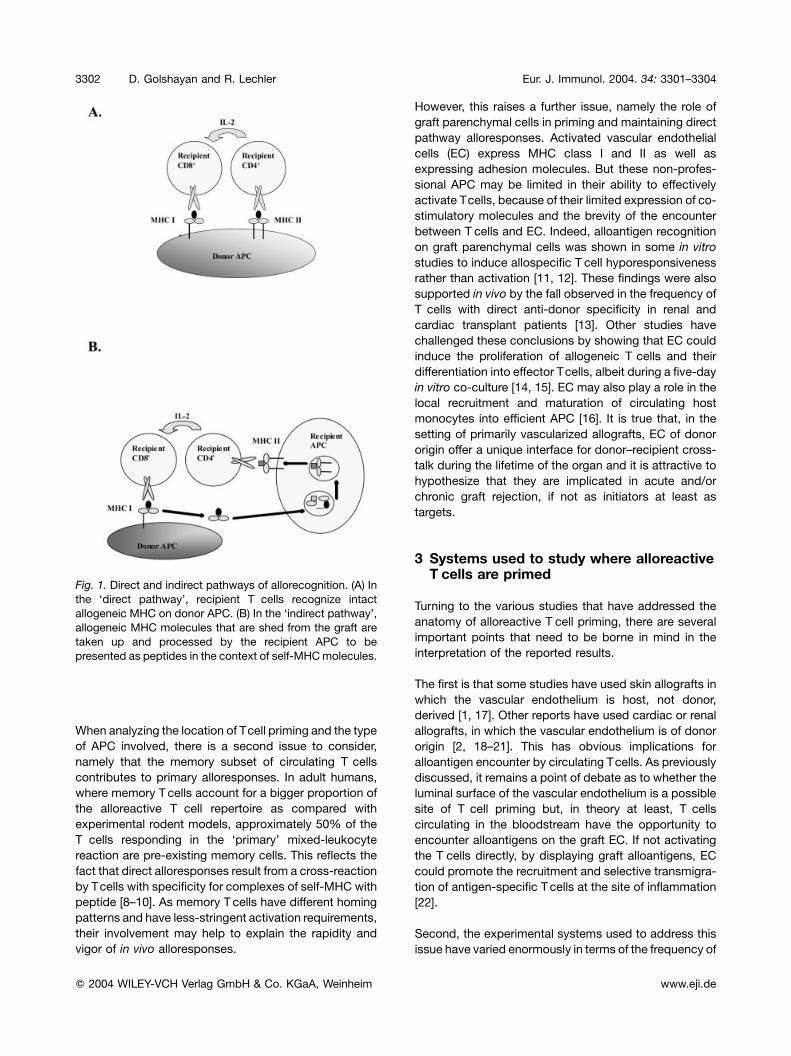
Fig. 1. Direct and indirect pathways of allorecognition. (A) In
the ‘direct pathway’, recipient T cells recognize intact
allogeneic MHC on donor APC. (B) In the ‘indirect pathway’,
allogeneic MHC molecules that are shed from the graft are
taken up and processed by the recipient APC to be
presented as peptides in the context of self-MHCmolecules.
3302 D. Golshayan and R. Lechler Eur. J. Immunol. 2004. 34: 3301–3304
f 2004 WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim www.eji.de

alloreactive T cells that have been employed. In their
study, Lakkis et al. showed that splenectomized aly/aly
recipients could not reject cardiac allografts, thus
demonstrating the role of secondary lymphoid organs
in initiating an alloresponse by naive T cells [20]. They
reached their conclusions using an adoptive transfer
model of polyclonal populations of T cells isolated from
naive or sensitized wild-type mice with a ‘physiological’
frequency of alloreactive T cells. In contrast, the study
published in this issue of the European Journal of
Immunology [3] used transgenic mice with a monoclonal
alloreactive TCR. The latter system has the potential to
yield somewhat misleading results, because of the highly
artefactual alloreactive T cell frequency. Although it may
be a rare event for naive T cells to traverse the vascular
endothelium, in a monoclonal T cell repertoire, any T cell
that accesses the graft is allospecific. This issue is also
relevant to the interpretation of the observations reported
by Kreisel et al. who investigated the possibility of
peripheral sensitization within a vascular allograft [21].
Using TCR-transgenic mice (BM3), they concluded that
mouse vascular endothelium could activate directly
allospecific CD8+ T cells in vitro and in vivo, leading to
the rejection of cardiac allografts.
This raises another important variable in the experiments
that have analyzed the question of the first encounter of
host T cells with transplant antigens using T cells from
TCR-transgenic mice, namely the activation require-
ments of the T cells. In some cases, such T cells have
rather aberrant properties; for example, the TCR genes
used to generate the BM3 (H-2k) transgenic mice with
specificity for H-2Kb were derived from a Tcell clone that
was CD8-independent in its activation [23]. This pre-
sumably reflects a particularly high TCR avidity. In the
experiments by Baratin et al. [3] the activation require-
ments of the TCR-transgenic T cells in response to their
two defined ligands were not studied in detail. Were the
responses to hemoglobin (Hb) + H-2Ek and to H2-Ep
equally dependant on mature DC, or was the direct
response to H-2Ep less stringent in its requirement for co-
stimulation?
The use of separated populations of CD4+ or CD8+ Tcells
for the study of the host immune alloresponses is also an
important variable. CD4+ T cells can initiate allograft
rejection through direct recognition of allogeneic MHC
class II antigens as well as indirect recognition of
allogeneic MHC peptides processed by self-APC. Both
pathways have been shown to help direct-pathway CD8+
T cells that eventually injure allogeneic MHC class I-
presenting target cells. Although less studied, CD8+ T
cells primed through the indirect pathway can also
mediate allograft rejection [24]. Furthermore, various
experimental models have demonstrated that CD4+ or
CD8+ T cells, alone, are sufficient to initiate rejection of
MHC I or II-mismatched allografts. Clearly, donor MHC I
antigenswill persist for the life of the graft. However, MHC
II antigens may be less abundant once donor passenger
leucocytes have migrated out of the graft, and died or
been eliminated. Hence, the direct-pathway CD4+ T cell
response is likely to be limited to the early post-transplant
period.
Finally, the relative contribution of the two major path-
ways of MHC alloantigen recognition, the direct and the
indirect pathways, needs to be addressed. This is the
attractive aspect of the study of Baratin et al. [3]. They
made intelligent use of amouse transgenic for a TCRwith
direct allospecificity for H-2Ep, and indirect specificity for
the mouse Hb b chain presented by H-2Ek. Thus by using
H-2p donors they could analyze the direct response,
whereas use of C57BL/6 mice transgenic for the
Hb(64–76) epitope allowed the study of the indirect
response following transplantation into an H-2k recipient.
The results suggest a clear distinction between the site of
priming of direct compared with indirect alloresponses.
The initiation of direct responses was largely visualized
within the skin graft, whereas indirect responses
appeared to originate in the draining lymph nodes, and
only later did activated Tcells appear within the graft. It is
not entirely clear why this distinction should be so abrupt.
If the direct response against donor alloantigens was
initiated by donor APC, such as Langerhans cells, there is
no obvious reason why infiltrating Tcells that had indirect
allospecificity would not have been activated within the
graft at the surface of infiltrating recipient DC.
4 Conclusion
In conclusion, it seems likely that the dominant pathway
for the initiation of both direct and indirect T cell
alloresponses involves DC of donor and recipient origin,
respectively. However, the data described in the paper by
Baratin et al. [3] highlight the fact that under some
circumstances priming can occur within the graft itself.
Future experiments should pursue these issues using
mice engineered to have much lower frequencies of
alloreactive T cells, using the adoptive transfer model
pioneered by Jenkins and colleagues, for example [25].
Similarly, the relevance of pre-existing memory T cells
and their contribution to the direct and indirect allor-
esponses should more carefully be examined.
References
1 Barker, C. F. and Billingham, R. E., The role of afferentlymphatics in the rejection of skin homografts. J. Exp. Med. 1968.128: 197–221.
Eur. J. Immunol. 2004. 34: 3301–3304 Priming of alloreactive T cells 3303
f 2004 WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim www.eji.de

2 Vetto, R. M. and Lawson, R. K., The role of vascular endotheliumin the afferent pathway as suggested by the alymphatic renalhomotransplant. Transplantation 1967. 5: 1537–1539.
3 Baratin, M., Bonin, K. and Daniel, C., Peripheral priming ofalloreactive Tcells by the direct pathway of allorecognition. Eur. J.Immunol. 2004. 34: this issue.
4 Reinhardt, R. L., Khoruts, A., Merica, R., Zell, T. and Jenkins,M. K., Visualizing the generation of memory CD4 T cells in thewhole body. Nature 2001. 410: 101–105.
5 Karrer, U., Althage, A., Odermatt, B., Roberts, C. W.,Korsmeyer, S. J., Miyawaki, S., Hengartner, H. and Zinkerna-gel, R. M., On the key role of secondary lymphoid organs inantiviral immune responses studied in alymphoplastic (aly/aly)spleenless (Hox1–/–) mutant mice. J. Exp. Med. 1997. 185:2157–2170.
6 Gallucci, S., Lolkema, M. and Matzinger, P., Natural adjuvants:endogenous activators of dendritic cells. Nat. Med. 1999. 11:1249–1255.
7 Lechler, R. I. and Batchelor, J. R., Restoration of immunogeni-city to passenger cell-depleted kidney allografts by the addition ofdonor strain dendritic cells. J. Exp. Med. 1982. 155: 31–41.
8 Lombardi, G., Sidhu, S., Daly, M., Batchelor, J. R., Makgoba,W. and Lechler, R. I., Are primary alloresponses truly primary?Int. Immunol. 1990. 2: 9–13.
9 Mason, D., A very high level of cross-reactivity is an essentialfeature of the T-cell receptor. Immunol. Today 1998. 19: 395–404.
10 Pantenburg, B., Heinzel, F., Das, L., Heeger, P. S. andValujskikh, A., T cells primed by Leishmania major infectioncross-react with alloantigens and alter the course of allograftrejection. J. Immunol 2002. 169: 3686–3693.
11 Marelli-Berg, F. M., Hargreaves, R. E., Carmichael, P., Dorling,A., Lombardi, G. and Lechler, R. I., Major histocompatibilitycomplex class II-expressing endothelial cells induce allospecificnonresponsiveness in naive T cells. J. Exp. Med 1996. 183:1603–1612.
12 Marelli-Berg, F. M., Scott, D., Bartok, I., Peek, E., Dyson, J.and Lechler, R. I., Activated murine endothelial cells havereduced immunogenicity for CD8+ T cells: a mechanism ofimmunoregulation? J. Immunol. 2000. 165: 4182–4189.
13 Baker, R. J., Hernandez-Fuentes, M. P., Brookes, P. A.,Chaudhry, A. N., Cook, H. T. and Lechler, R. I., Loss of directand maintenance of indirect alloresponses in renal allograftrecipients: implications for the pathogenesis of chronic allograftnephropathy. J. Immunol. 2001. 167: 7199–7206.
14 Briscoe, D. M., Alexander, S. I. and Lichtman, A. H.,Interactions between T lymphocytes and endothelial cells inallograft rejection. Curr. Opin. Immunol. 1998. 10: 525–531.
15 Biedermann, B. C. and Pober J. S., Human endothelial cellsinduce and regulate cytolytic T cell differentiation. J. Immunol1998. 161: 4679–4687.
16 Denton, M. D., Geehan, C. S., Alexander, S. I., Sayegh, M. H.and Briscoe, D. M., Endothelial cells modify the costimulatorycapacity of transmigrating leukocytes and promote CD28-mediated CD4(+) T cell alloactivation. J. Exp. Med. 1999. 190:555–566.
17 Larsen, C. P., Steinman, R. M., Witmer-Pack, M., Hankins, D.F., Morris, P. J. and Austyn, J. M., Migration and maturation ofLangerhans cells in skin transplants and explants. J. Exp. Med1990. 172: 1483–1493.
18 Zhou, P., Hwang, K. W., Palucki, D., Kim, O., Newell, K. A., Fu,Y. X. and Alegre, M. L., Secondary lymphoid organs areimportant but not absolutely required for allograft responses.Am. J. Transplant. 2003. 3: 259–266.
19 Larsen, C. P., Morris, P. J. and Austyn, J. M., Migration ofdendritic leukocytes from cardiac allografts into host spleens. Anovel pathway for initiation of rejection. J. Exp. Med. 1990. 171:307–314.
20 Lakkis, F. G., Arakelov, A., Konieczny, B. T. and Inoue, Y.,Immunologic ‘ignorance’ of vascularized organ transplants in theabsence of secondary lymphoid tissue. Nat. Med. 2000. 6:686–688.
21 Kreisel, D., Krupnick, A. S., Gelman, A. E., Engels, F. H.,Popma, S. H., Krasinskas, A. M., Balsara, K. R., Szeto, W. Y.,Turka, L. A. and Rosengard, B., Non-hematopoietic allograftcells directly activate CD8+ Tcells and trigger acute rejection: Analternative mechanism of allorecognition. Nat. Med. 2002. 8:233–239.
22 Marelli-Berg, F. M., James, M. J., Dangerfield, J., Dyson, J.,Millrain, M., Scott, D., Simpson, E., Nourshargh, S. andLechler, R. I., Cognate recognition of the endothelium inducesHY-specific CD8+ T-lymphocyte transendothelial migration (dia-pedesis) in vivo. Blood 2004. 103: 3111–3116.
23 Sponaas, A. M., Tomlinson, P. D., Schulz, R., Antoniou, J., Ize-Iyamu, P., Schmitt-Verhulst, A. M. and Mellor, A. L., Toleranceinduction by elimination of subsets of self-reactive thymocytes.Int. Immunol. 1994. 10: 1593–1604.
24 Valujskikh, A., Lantz, O., Celli, S., Matzinger, P. and Heeger, P.S.,Cross-primedCD8+ Tcells mediate graft rejection via a distincteffector pathway. Nat. Immunol. 2002. 3: 803–804.
25 Pape, K. A., Kearney, E. R., Khoruts, A., Mondino, A., Merica,R., Chen, Z. M., Ingulli, E., White, J., Johnson, J. G. andJenkins, M. K., Use of adoptive transfer of T cell-antigen-receptor-transgenic Tcell for the study of Tcell activation in vivo.Immunol. Rev. 1997. 156: 67–78.
Correspondence: Robert Lechler, Department of Immunol-
ogy, Imperial College, Hammersmith Hospital, Du Cane
Road, London W12 ONN, UK
Fax: +44-208-3832788
e-mail: [email protected]
3304 D. Golshayan and R. Lechler Eur. J. Immunol. 2004. 34: 3301–3304
f 2004 WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim www.eji.de





























