Embed Size (px)
Citation preview

cg
Combined Treatmentof Depression
Fredric N. Busch, MDa,b,*, Larry S. Sandberg, MD
a,b
KEYWORDS
• Combined treatment • Medication • Psychotherapy• Depression • Research
Multiple medications and some forms of psychotherapy have demonstrated efficacyin the treatment of depression.1 However, despite these interventions, many patientscontinue to respond only partially to available treatments2 and nonadherence tomedication is common,3,4 adding to the tendency of depression to recur.5 Manylinicians believe that a combination of medication and psychotherapy provides thereatest potential for long-term relief of depression,6 and a number of studies have
focused on the relative value of combined compared to single treatments.Given our current state of knowledge, for which patients should a combination of
medication and psychotherapy be recommended and employed? The AmericanPsychiatric Association Practice guideline for the treatment of patients with majordepressive disorder1 identifies a broad range of conditions for which combinedtreatment should be considered (Box 1): “Combining a depression-focused psycho-therapy and pharmacotherapy may be a useful initial treatment choice for patientswith moderate to severe major depressive disorder. Other indications for combinedtreatment include chronic forms of depression, psychosocial issues, intrapsychicconflict, interpersonal problems, or a co-occurring Axis II disorder. In addition,patients who have had a history of only partial response to adequate trials of singletreatment modalities may benefit from combined treatment. Poor adherence withpharmacotherapy may also warrant combined treatment with medications andpsychotherapy focused on treatment adherence.”1(p28)
There are several reasons to believe that medication and psychotherapy should beutilized together for treatment of depression.7 These approaches probably affectdifferent areas of the brain, potentially creating a synergistic neurophysiologic effect.8
Given that different patients demonstrate different responses to various treatments,combining two treatments increases the likelihood patients will respond to at least
The authors have nothing to disclose.a Weill Cornell Medical College, 1300 York Avenue, New York, NY 10065, USAb Columbia University Center for Psychoanalytic Training and Research, 180 Fort, WashingtonAvenue, New York, NY 10032, USA* Corresponding author. 10 East 78th Street, #5A, New York, NY 10075.E-mail address: [email protected]
Psychiatr Clin N Am 35 (2012) 165–179doi:10.1016/j.psc.2011.10.002 psych.theclinics.com
0193-953X/12/$ – see front matter © 2012 Elsevier Inc. All rights reserved.
tm
166 Busch & Sandberg
one of them. In addition, the persistent and recurrent nature of depressive syn-dromes5,9 and the adverse impact of residual symptoms10,11 indicate the importanceof reducing vulnerability to depression, and psychotherapy and medication may beadditive in their impact on this vulnerability. Each modality can potentially enhance theother: medication allowing for more effective use of psychotherapy (eg, throughincreasing concentration and motivation) and psychotherapy aiding with adherenceto medication.3,12 Combining psychotherapy with medication may allow for reduceddoses and a diminished side effect burden of medications, and medication canreduce the need for persistent or more intensive psychotherapy through reduction ofsymptoms.
However, there are also arguments against combination treatments. Not allpatients require medication and psychotherapy to achieve remission of symptoms orprevent recurrence. Therefore combination treatments may expose patients to moretreatment and side effects than is necessary. Questions of cost effectiveness arise inthe greater expense of psychotherapy plus medication, although potential benefitsover the long term need to be considered.13 Problems in delivery of combinedreatments (“split treatment” vs a psychiatrist providing both psychotherapy andedication) may reduce overall effectiveness of one or the other approaches.14
Thus, many questions remain regarding the need for and relative efficacy ofcombined treatment. What types of patients may require a combination approach andwhich may need only a single treatment? What may be the value of sequencingtreatments? Do some forms of depression benefit more from combined treatmentthan others? What factors may moderate response to combined treatment? Whattypes of psychotherapy are most effective for depression in a combination treatment?How does delivery of combined treatment by a single practitioner compare to a “splittreatment” involving a psychotherapist and psychopharmacologist? What do re-search studies show about combined treatment and how might they aid in clinicaldecision making? What are limitations and problems with these research studies?
Given these varied viewpoints and remaining questions, clinical decisions are oftenbased on the skill set and belief system of the particular clinician who is treating thepatient. In many cases a single treatment is initiated that is changed to a combinationtreatment if there is a limited response. Through such strategies patients frequentlyshow adequate response to treatment, although many will not achieve remission orwill experience a recurrence of depression. In this article we review the literature oncombined treatment to develop a rationale for addressing these questions based on
Box 1Recommendations for combined treatment: practice guidelines
● Patients with moderate to severe major depressive disorder
● Chronic forms of depression
● Psychosocial issues, intrapsychic conflict, interpersonal problems
● A co-occurring Axis II disorder
● Partial response to adequate trials of single treatment modalities
● Poor adherence with pharmacotherapy
theory, clinical experience, and research studies.

tmmbsde
ttdTpogf
167Combined Treatment of Depression
THE BIOPSYCHOSOCIAL MODEL IN CONSIDERING COMBINED TREATMENTS
A biopsychosocial model is of particular utility in conceptualizing the value ofcombining medication and psychotherapy, identifying how biological and psycholog-ical interventions can work together in depression treatment.15 Kendler16 attemptedo further delineate these processes, suggesting a model of bidirectional causality:ental phenomena have an impact on brain function and brain function impacts theind. Thus medication affects mental phenomena, and psychotherapy becomes aiological treatment affecting brain function. In accord with this model, increasinglytudies have identified neurophysiological changes that accompany improvement inepression and anxiety disorders through psychotherapy.8 This model helps toxplain how medication and psychotherapy can operate synergistically.
At the same time, this model can be employed to argue for providing a singlereatment. If medication and psychotherapy both affect mind and brain, then why arewo treatments necessary? Kendler16 employs the term “patchy reductionism” inescribing how unitary causal models are not sufficient for most mental disorders.he relative value of psychotherapy and medication varies on the basis of thearticular form of depressive disorder; the life history, psychology, and environmentf the patient; the presence of other disorders; and the particular susceptibility of aiven patient to different approaches. Clinical and research efforts are necessary tourther identify how to best approach individual patients.
RESEARCH ON COMBINED TREATMENTS
Research studies have attempted to answer the following questions (Box 2): Iscombined treatment more effective? Does combined treatment provide advantages inthe short term, long term, or both? Is there a benefit to sequencing treatments? Dodifferent types of depression respond differentially to combined treatments? Whatfactors moderate treatment outcomes? What types of psychotherapy may be mosteffective in a combined treatment? This article reviews the status of the research oncombined treatments to best provide answers for these questions. The summaries inthe text that follows are not meant to be an exhaustive review of the researchliterature, but are intended to be representative, with a focus on recent studies thatare of higher quality. In addition, questions have been raised about the value ofevidence-based medicine, including randomized controlled trials (RCTs) and meta-analyses.17 These issues are not a focus of this article, but call attention to the needfor being circumspect in interpreting the research literature.
Box 2Areas of research
● Comparing combined to single treatments
● Follow-up studies
● Sequencing of treatments
● Types of depression
● Moderators of outcome
● Split versus single treatments

btccabesf
168 Busch & Sandberg
Combining Psychotherapy and Medication
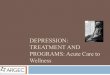
Most reviews and meta-analyses12,18–24 have determined that combined treatment issomewhat more efficacious than a single treatment, although negative studies haveraised questions about whether different treatments or patient subgroups affect theseresults.20–24 Three recent comprehensive meta-analyses20–22 demonstrated small
ut significant advantages of combined treatments and attempted to identify factorshat may be relevant to efficacy and treatment choice (Table 1). Cuijpers andolleagues20 reviewed 18 randomized studies in which a psychological treatment wasompared to the same psychological treatment combined with medication. This meta-nalysis demonstrated a mean effect size of 0.35 in favor of combined treatment, a smallut significant advantage. In studies in which cognitive–behavioral therapy (CBT) wasxamined, the difference between CBT and the combined treatment was significantlymaller, suggesting that CBT may be a more efficacious treatment. In addition, atollow-up of 3 to 6 and 12 months, no significant differences were found.
Cuijpers and colleagues21 identified 25 randomized trials in which medication wascompared to a combination of medication and psychotherapy. A mean effect size infavor of the combined treatment of 0.31 was found, indicating a small but significantadvantage for combined treatment compared to medication alone. In patients withdysthymia, the value of adding psychotherapy was significantly less. The dropout ratewas significantly lower in combined treatment, indicating that combined treatmentmay allow for improved adherence. Most recently, Cuijpers and coworkers22 com-pared RCTs in which medication and psychotherapy were compared to psychother-apy and placebo to evaluate better the advantage of active medication treatment. Inexamining 16 studies the authors found an effect size of 0.25 in favor of activemedication, again demonstrating a small but significant advantage in the combinedactive treatment. No subgroup differences were found in this study.
The authors point out that the small to moderate effect sizes found in these
Table 1Recent comprehensive meta-analyses
Type of Study Effect Size Other Findings
Cuijperset al20
Psychological treatment wascompared to the samepsychological treatmentcombined with medication.
0.35 in favor ofcombinedtreatment
The difference between CBTand the combinedtreatment wassignificantly smaller.
At follow-up of 3–6 and 12months, no significantdifferences were found.
Cuijperset al21
Medication was compared to acombination of medicationand psychotherapy.
0.31 in favor ofcombinedtreatment
In patients with dysthymia,the value of addingpsychotherapy wassignificantly less.
The dropout rate wassignificantly lower incombined treatment.
Cuijperset al22
Medication and psychotherapywere compared topsychotherapy and placebo.
0.25 in favor of thecombined activetreatment
The result indicates that theimpact of medication incombined treatment isnot just a placebo effect.
meta-analyses, despite their statistical significance, raise a question about the actual

frrtfcl
169Combined Treatment of Depression
degree of clinical advantage of combined treatment. Possible explanations of therelatively small advantage found in these studies20–22 are the relative effectiveness ofcombined treatments for certain subgroups, the significant treatment impact of singletreatments for many patients, or problems with the quality of studies done thus far.Overall, the data to date show that the average patient will have a better outcome withcombined treatment than with unimodal approaches. However, given the relatively smalleffect sizes, and the potential costs of treatment (in money, time, and side effects), patientpreference, clinical features of depression, and various complicating factors should beconsidered in the clinician’s decision to recommend combined treatment.
Assessing Follow-Up
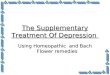
In addition to assessing whether the combination of psychotherapy and medication issuperior to single treatments, a critical factor is the impact of these treatments overthe long term. Given the persistent and recurrent nature of depression,5,9 it isimportant to evaluate whether a combined treatment can reduce vulnerability to thesedisorders. The capacity to affect persistent symptoms is also relevant to the costeffectiveness of combined treatments. Although Cuijpers and colleagues20 found thatdifferences between combined treatment and psychotherapy in the short term werelost in follow-up, several recent studies that examined longer term follow-up suggestthat these gains may be maintained (Table 2).
Schramm and coworkers25 studied patients hospitalized with major depressivedisorder (MDD) in an RCT, comparing 5 weeks of interpersonal psychotherapy (IPT)modified for depressed inpatients plus medication to intensive clinical managementplus medication. Patients receiving IPT plus medication showed higher response andremission rates after treatment and higher response rates and Global Assessment ofFuntioning (GAF) at 3- and 12-month follow-up. Zobel and coworkers26 looked atollow-up over 5 years for the patients in the study by Schramm and colleagues.25 Theate of reduction of symptoms and the percentage of patients who sustainedemission over the 5-year period was higher for those receiving IPT (28%) comparedo the clinical management group (11%). Combination treatment was more effectiveor patients with a history of trauma, a finding concordant with that of Nemeroff andolleagues,27 which is discussed further in the text that follows. Maina and col-
eagues28 studied patients with MDD who met criteria for remission after a 6-monthtreatment with either medication or medication plus brief dynamic therapy (BDT). Afterthe initial treatment there was a 6-month continuation phase with medications alone,followed by an assessment at 48 months. Patients who received combined treatmentin the initial phase had significantly lower rates of relapse at 48-month follow-up.Other follow-up studies, involving sequential treatment, are discussed later.29,30 Theemerging data on the value of combined treatment over the long term suggests thatit should be more strongly considered, despite the costs of these treatments.Clinicians should remain alert to further follow-up studies in the literature in guidingtheir decisions.
Sequencing of Treatments
Sequencing of treatments can be employed as an augmenting strategy in the acutephase or as a shift in approaches to treat different phases of the illness. The conceptinherent in the latter is that the mechanisms involved in depression onset differ fromthose contributing to its recurrence, and thus each phase benefits from differentinterventions.31 In his review of studies on combined treatment, Petersen found that“. . .sequential use of psychotherapy after induction of remission with acute antide-
pressant drug therapy may confer a better long-term prognosis in terms of preventing
Table 2Recent long-term follow-up studies
Treatments Compared Length of Follow-Up Results
Schramm et al25 IPT modified for depressed inpatientsplus medication to intensive clinicalmanagement plus medication
3 and 12 months IPT plus medication showed higher response ratesand GAF.
Zobel et al26 further follow-upfrom Shramm et al25
IPT modified for depressed inpatientsplus medication to intensive clinicalmanagement plus medication
5 years Rate of reduction of symptoms and percentage ofpatients who sustained remission over the 5-year period was higher for those receiving IPT(28%) compared to the clinical managementgroup (11%).
Maina et al28 BDT plus medication compared tomedication alone
48 months Combined treatment had significantly lower ratesof relapse at 48-month follow-up.
Bockting et al29 Brief CBT added to usual care to usualcare alone
5.5 years CBT plus usual care provided a significantprotective effect against relapse/recurrence.
170B
usch
&San
db
erg

acuccd
ipft
ct
dwAat
t
171Combined Treatment of Depression
relapse or recurrence and, for some patients, may be a viable alternative tomaintenance medication therapy.”7(p19)
Several studies suggest that a switch to or addition of psychotherapy either doesnot adversely affect or decreases the risk of depression recurrence (Table 3). Segaland colleagues32 studied patients whose symptoms remitted with antidepressantsnd then randomized them to eight weekly group sessions of mindfulness basedognitive therapy (MBCT), continuing on medication, or switching to placebo. Amongnstable remitters, patients treated with either medication or MBCT showed signifi-antly reduced risk of relapse compared to placebo, suggesting comparable out-omes for the sequencing of treatments. Among stable remitters, there was noifference between the groups. Bockting and colleagues29 found that brief CBT, when
added to usual care and initiated after episode remission in patients with recurrentdepression, provided a significant protective effect during a 5.5-year period com-pared with usual care alone. Kennard and coworkers33 examined adolescents withMDD who responded to medication treatment and randomized them to eithercontinued medication or medication plus CBT focused on relapse prevention. Theyfound an eightfold reduction in relapse in patients receiving the combined treatment.Fava and colleagues30,34 studied patients with recurrent depression who had remittedn response to antidepressant medications. Medications were discontinued andatients were randomized to receive either CBT or clinical management. At 6-year
ollow-up patients receiving CBT had a significantly lower relapse rate (40%) thanhose receiving clinical management (90%).
Frank and coworkers35 applied an alternate approach in studying two successivecohorts of women with recurrent major depression. One group was treated with IPTplus medication and the other group was treated first with IPT with the addition ofmedication if they did not remit. The second group showed a significantly higherremission rate (79%) than those who received combined treatment from the outset(66%). Although the reason for the higher remission rate was unclear and this was nota randomized trial, the study suggests that many patients can benefit from psycho-therapy alone, requiring medication only if they are nonresponsive. Overall, studiessuggest that sequencing treatment can allow the clinician to identify patients that mayneed only a single treatment, and that psychotherapy after medication can help toreduce the risk of relapse.
Types of Depression
Subcategories of depression that have been considered to potentially responddifferentially to a combination treatment include dysthymia and chronic depression.Interpretation of studies of dysthymia are complicated by the inclusion of manypatients who have “double depression” (MDD plus dysthymia), as opposed to “pure”dysthymia.36 As noted in the preceding text, Cuijpers and colleagues21 found that theombination of psychotherapy and medication adds little to medication alone in thereatment of dysthymia. Imel and coworkers36 found medication to have greater
efficacy in a meta-analysis of studies comparing psychotherapy and medication in thetreatment of dysthymia. Markowitz and colleagues37 studied 94 subjects with “pure”
ysthymia (no episodes of MDD in 6 months before presentation) randomized to 16eeks of IPT, brief supportive psychotherapy (BSP), sertraline, or sertraline plus IPT.lthough subjects were responsive to all of the treatments, responses were highernd at a similar rate with sertraline (58%) and combined treatment (57%) comparedo IPT (35%) and BSP (31%).
Patients with chronic depression have been found to be less responsive to
reatment.24 In a landmark study, Keller and colleagues38 found a significantly higher
Table 3Studies on sequencing of treatments
Subjects Studied Treatments Sequenced/Compared Results
Segal et al32 Patients whose symptoms remittedwith antidepressants
Eight weekly group sessions of MBCT,continuing on medication, orswitching to placebo
Among unstable remitters, patients treatedwith either medication or MBCT showedsignificantly reduced risk of relapsecompared to placebo.
Among stable remitters, there was nodifference between the groups.
Bockting et al29 Remitted patients with recurrentdepression
Brief CBT added to usual care to usualcare alone
CBT plus usual care provided a significantprotective effect againstrelapse/recurrence.
Kennard et al33 Adolescents with MDD whoresponded to medicationtreatment
Continued medication or medicationplus CBT focused on relapseprevention
There was an eightfold reduction in relapsein patients receiving the combinedtreatment.
Fava et al30,34 Patients with recurrent depressionwho had remitted withantidepressant medications
Medications discontinued andpatients randomized to either CBTor clinical management
At 6-year follow-up, patients receiving CBThad a significantly lower relapse rate(40%) than those receiving clinicalmanagement (90%).
Frank et al35 Women with recurrent majordepression
One group IPT plus medication; onegroup treated first with IPT withmedication added if they did notremit
IPT with medication added if they did notremit showed a significantly higherremission rate (79%) than those whoreceived combined treatment from theoutset (66%).
172B
usch
&San
db
erg

scdfmepiavc
ahatoI
173Combined Treatment of Depression
rate of response in chronically depressed patients receiving a combination of CBASP(cognitive–behavioral analysis system of psychotherapy) and nefazodone comparedto either treatment alone. Subjects were considered to have chronic depression if “(1)criteria for MDE were met continuously for at least 2 years, with no antecedent dysthymia;(2) the MDE was superimposed on antecedent dysthymia; or (3) the MDE was recurrent,with incomplete interepisode recovery, and lasted at least 2 years.”39(p460) A subsequentreanalysis of the data39 found that patients receiving the combination treatment showedmore rapid remission. Hollon and coworkers,18 in their review of the literature,uggested that combination treatment may be particularly valuable for patients withhronic depression. In a negative study, Kocsis and colleagues24 studied chronicallyepressed patients who did not achieve remission (60% reduction in Hamilton Scale
or Depression [HAM-D] score, a 24-item HAM-D total score �8, and no longereeting DSM-IV criteria for MDD for 2 consecutive visits) and randomized them to
ither medication alone, medication plus CBASP, or medication plus brief supportivesychotherapy. In their study, 37.5% of patients remitted or showed partial response
n phase II, but no differences were found in response to the various treatments. Theuthors acknowledge that the number of sessions of CBASP received was lower (12.5s 16) than in those of Keller and coworkers.38 Overall, these studies indicate thatombined treatment should be strongly considered in cases of chronic depression.
Moderators of Outcome
Two major potential moderators explored in the literature on combined treatment arepersonality disorders and trauma, addressing the question of whether psychotherapy,in addition to medication, may be necessary to adequately address these factors.Many studies indicate that depression accompanied by personality disorders is lessresponsive to treatment. For example, Grilo and colleagues40 studied patients withMDD, assessing for the presence of personality disorders. They found that patientswith personality disorders at baseline took a longer time to achieve remission andrelapsed much more rapidly after remission compared to patients without personalitydisorders after achieving remission. Kool and colleagues41 studied patients withmajor depression randomized to receive combined medication and short-termpsychodynamic psychotherapy or medication alone. In secondary analyses theyfound that combined treatment was more effective in treating patients who also hadpersonality disorders but not more effective in patients who did not have personalitydisorders. Maddux and colleagues42 examined chronically depressed patientstreated with CBASP, nefazodone, or their combination. In this study the presence ofpersonality disorders did not have an impact on outcome. However, the studyexcluded borderline, schizotypal, and antisocial personality disorders.
In the examination by Nemeroff and colleagues27 of the data of Keller andcolleagues,38 681 patients with chronic forms of major depression were treated withn antidepressant (nefazodone), CBASP, or the combination. Among those with aistory of early childhood trauma (loss of parents at an early age, physical or sexualbuse, or neglect), psychotherapy alone was superior to antidepressant mono-herapy. Moreover, the combination of psychotherapy and pharmacotherapy wasnly marginally superior to psychotherapy alone among the childhood abuse cohort.
n the study by Zobel and coworkers26 described in the preceding text, combinationtreatment was found to be more effective for patients with a history of trauma. Theresults of these studies suggest that psychotherapy may be an essential element inthe treatment of depressed patients with a history of childhood trauma and a
comorbid personality disorder.
a
ttsc
daoca
174 Busch & Sandberg
Types of Psychotherapy
Significantly more evidence has been garnered for CBT and IPT compared topsychodynamic psychotherapy with regard to combined treatment of depression.1
Hollon and colleagues,18 in their review, surmised that “interpersonal psychotherapy(IPT) appears to have a delayed effect on the quality of interpersonal relationships notfound for medications, and cognitive-behavioral therapy (CBT) appears to have anenduring effect that reduces risk for subsequent symptom return even after treatmentis over.”18(p456) As noted in the preceding text, several studies have found that CBTdded to medication can reduce the risk of relapse.29,33 Although research on psychody-
namic psychotherapy is more limited, several studies28,41,43 and recent meta-analy-ses19,44 indicate that this treatment can also be effective in achieving remission andreducing relapse. It is unclear at this time what type of psychotherapy in combination withmedication may best address co-occurring personality disorders.45,46
Single Provider Versus Split Treatment
No studies were located comparing the relative efficacy of a single clinician providingcombined treatment and a split treatment. Two studies47,48 suggest that it is relativelymore cost effective to have a psychiatrist providing both treatments. Dewan47 foundhat combined treatment by a psychiatrist cost about the same or less than splitreatment with either a social worker or psychologist/psychotherapist based on feechedules of a variety of managed care organizations and Medicare. Goldman andolleagues,48 reviewing retrospective data of claims from a managed care organiza-
tion over an 18-month period, found that patients seeing a psychiatrist in combinedtreatment had lower costs and fewer total visits than patients in a split treatment.These findings are counterintuitive, raising questions about the presumption thatsplit treatment is less expensive.
As noted in the preceding text, the issues of combined treatment delivery is of greatsignificance but relatively ignored in the literature. There are a variety of clinicaldiscussions on managing these situations14 but minimal research comparing thesetreatments. A psychiatrist providing psychotherapy and medication has the advantage ofavoiding conflicts between two treating clinicians. In addition, the greater frequency ofvisits to the psychiatrist allows more frequent opportunities to monitor for persistent orrecurrent depressive symptoms. There are potential problems with this approach,however, including that a psychiatrist providing psychotherapy can lose sight of the moresystematic assessment of symptoms and medication that are done automatically inpharmacologic visits.14 In addition, psychiatrists often do not have competency in thedepression-focused psychotherapies that have been found to be effective for treatmentof depression. This could certainly be addressed through additional training.
Several papers have been written that describe the potential areas of conflict insplit treatments between the two providers and in patients’ experience and percep-tion of these providers.49,50 Competitive and professional tensions, as well as
ifferent theoretical and clinical models, can generate problems in treatment man-gement. Patients may idealize and devalue one or the other of the clinicians, or actut in ways that may be difficult to address. A triadic therapeutic alliance andommunication about problems have been recommended as ways of identifying andddressing potential problems.
DISCUSSION
Research studies overall substantiate an advantage of combined treatment over a
single treatment for depression and the vulnerability to persistence or recurrence (a
175Combined Treatment of Depression
summary of recommendations is provided in Box 3). Further studies are required,however, to better determine the types of patients and treatments for which combinedtreatments are most appropriate or necessary. From the clinical and researchstandpoint, the broad range of conditions suggested for combined treatment in thePractice Guideline1 seems appropriate. Studies thus far suggest an advantage forcombined treatment in patients with chronic depression (other than “pure” dysthy-mia), co-occurring personality disorders, and a history of trauma. Although thePractice Guideline suggests an advantage for combined treatment for dysthymia,1
research thus far suggests limited value for psychotherapeutic or combined treatmentof this disorder. The development of therapies targeted for chronic disorders and themore careful distinction between dysthymia and double depression may affect thisrecommendation.
From the clinician’s standpoint, combination treatment represents a powerfulintervention that can be synergistic across the biopsychosocial spectrum. Medicationprovides rapid relief of symptoms, but includes the problems of persistent side effectsand potential for recurrence when medication is discontinued. Psychotherapy may beslower in its impact on symptoms and more labor intensive, but can aid in reductionof persistent symptoms and relapse recurrence. Psychotherapy provides an oppor-tunity to address co-occurring personality disorders, trauma sequelae, and intrapsy-chic conflicts that can add to persistent depression vulnerability, psychosocialdisruption, and suffering. Studies of cost effectiveness are limited,13 but given thehigh cost of depression, any form of treatment that diminishes vulnerability over thelong term should be given serious consideration. Combined treatment may aid inadherence to both medication and psychotherapy.3,12,21
With regard to types of psychotherapy, thus far CBT and IPT have much broaderevidence bases for treatment of depression and depression vulnerability, including aspart of combined treatment. Given the limited studies, much more research needs tobe done before an accurate picture can be obtained comparing psychodynamic
Box 3Recommendations on combined treatments based on clinical experience and researchstudies
● Despite an edge in efficacy, the clinician should consider costs of treatment, patient preference,clinical features of depression, and complicating factors (eg, poor treatment adherence, psycho-social problems, co-occurring personality disorders) in recommending combined treatments.
● Sequencing treatment can allow the clinician to identify patients who may need only a singletreatment, and psychotherapy following medication can help to reduce the risk of relapse.
● Psychotherapy may be a necessary component of treatment in depressed patients withcomborbid personality disorders or a history of trauma.
● Chronic depression appears to respond best to combined treatment, whereas “pure” dysthymiathus far has been found to respond better to medication.
● Although CBT and IPT have more definitively demonstrated efficacy in the treatment ofdepression, studies suggest that psychodynamic psychotherapy may be of significant valuealone or in combined treatments.
● Studies have yet to clarify the relative cost effectiveness or efficacy of single practitioner versus splittreatment, although each benefits from clinicians being alert to potential clinical problems of eachapproach.
psychotherapy to these psychotherapies. Focused psychodynamic psychotherapies

iit
176 Busch & Sandberg
for depression are increasingly being developed and more systematic assessment oftestable psychodynamic treatments is underway. Difficult as they are, direct compar-isons of CBT, IPT, and psychodynamic therapy over the short and long term will beessential to fully clarify the relative value of these treatments. There is reason tobelieve that psychodynamic psychotherapy, with its broad range of focus onsymptom meanings, intrapsychic conflicts, personality dysfunction, and interpersonalrelationships and their internal representations may have a broader impact ondepression vulnerability than other treatments. A recent meta-analysis51 suggeststhat long-term psychodynamic psychotherapy may be valuable for complex mentaldisorders (personality disorders, chronic illness of at least 1 year’s duration, andmultiple comorbid disorders).
Further studies are essential to compare the relative efficacy of a single providerversus split treatment. From the clinical standpoint, clinicians should adopt strategiesthat minimize potential problems with either approach: a single clinician providingboth treatments developing a means of regular medication assessment, and com-munication between providers to address problem areas in a split treatment.
Additional studies are clearly required to delineate further the value of combinedversus single treatments in depression. There are no “cookbook” means of approach-ing depressed patients, although the information discussed can aid clinicians inchoosing treatment options. In addition, the evidence base and recommendationscontinue to shift; for example, an increase in targeted psychotherapy studies led tothese treatments being more highly recommended in the most recent PracticeGuideline.1 It is important for clinicians to be knowledgeable about the variousnterventions available for depression, to be willing to employ more than a singlentervention, and to stay informed of ongoing developments regarding thesereatments.
REFERENCES
1. American Psychiatric Association. Practice guideline for the treatment of patients withmajor depressive disorder. 3rd edition. Am J Psychiatry 2010;167(10 Suppl):1–118.
2. Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes indepressed outpatients requiring one or several treatment steps: a STAR*D report. AmJ Psychiatry 2006;163(11):1905–17.
3. Bockting CL, ten Doesschate MC, Spijker J, et al. Continuation and maintenanceuse of antidepressants in recurrent depression. Psychother Psychosom 2008;77(1):17–26.
4. Simon GE, Von Korff M, Rutter CM, et al. Treatment process and outcomes formanaged care patients receiving new antidepressant prescriptions from psychiatristsand primary care physicians. Arch Gen Psychiatry 2001;58:395–401.
5. Judd LL, Akiskal HS, Zeller PJ, et al. Psychosocial disability during the long-termcourse of unipolar major depressive disorder. Arch Gen Psychiatry 2000;57:375–80.
6. Kornbluh R, Papakostas GI, Petersen T, et al. A survey of prescribing preferences inthe treatment of refractory depression: recent trends. Psychopharmacol Bull 2001;35:150–6.
7. Petersen TJ. Enhancing the efficacy of antidepressants with psychotherapy. J Psy-chopharm 2006;20:19–28.
8. Goldapple K, Segal Z, Garson C, et al. Modulation of cortical-limbic pathways in majordepression: treatment-specific effects of cognitive behavior therapy. Arch Gen Psy-chiatry 2004;61:34–41.
9. Eaton WW, Shao H, Nestadt G, et al. Population-based study of first onset and
chronicity in major depressive disorder. Arch Gen Psychiatry 2008;65:513–20.
177Combined Treatment of Depression
10. Judd LL, Akiskal HS, Paulus MP. The role and clinical significance of subsyndromaldepressive symptoms(SSD) in unipolar major depressive disorder. J Affect Disord1997;45(1–2):5–18.
11. Paykel ES, Ramana R, Cooper Z, et al. Residual symptoms after partial remission: animportant outcome in depression. Psychol Med 1995;25(6):1171–80.
12. Pampallona S, Bollini P, Tibaldi G, et al. Combined pharmacotherapy and psycholog-ical treatment for depression: a systematic review. Arch Gen Psychiatry 2004;61:714–9.
13. Lynch FL, Dickerson JF, Clarke G, et al. Incremental cost-effectiveness of combinedtherapy vs medication only for youth with selective serotonin reuptake inhibitor-resistant depression: treatment of SSRI-resistant depression in adolescents trialfindings. Arch Gen Psychiatry 2011;68:253–62.
14. Busch FN, Sandberg LS. Psychotherapy and medication: the challenge of integration.Hillsdale (NJ): The Analytic Press; 2007.
15. Engle GL. The need for a new model: a challenge for biomedicine. Science 1977;196:129–36.
16. Kendler KS. Toward a philosophical structure for psychiatry. Am J Psychiatry 2005;162:433–40.
17. Gupta M. Does evidence-based medicine apply to psychiatry? Theor Med Bioeth2007;28:103–20.
18. Hollon SD, Jarrett RB, Nierenberg AA, et al. Psychotherapy and medication in thetreatment of adult and geriatric depression: which monotherapy or combined treat-ment? J Clin Psychiatry 2005;66:455–68.
19. de Maat S, Dekker J, Schoevers R, et al: Short psychodynamic supportive psycho-therapy, antidepressants, and their combination in the treatment of major depression:a mega-analysis based on three randomized clinical trials. Depress Anxiety 2008;25:565–74.
20. Cuijpers P, van Straten A, Warmerdam L, et al. Psychotherapy versus the combina-tion of psychotherapy and pharmacotherapy in the treatment of depression: ameta-analysis. Depress Anxiety 2009;26(3):279–88.
21. Cuijpers P, Dekker J, Hollon SD, et al. Adding psychotherapy to pharmacotherapy inthe treatment of depressive disorders in adults: a meta-analysis. J Clin Psychiatry2009;70(9):1219–29.
22. Cuijpers P, van Straten A, Hollon SD, et al. The contribution of active medication tocombined treatments of psychotherapy and pharmacotherapy for adult depression: ameta-analysis. Acta Psychiatr Scand 2010;121:415–23.
23. Vitello B. Combined cognitive-behavioural therapy and pharmacotherapy for adoles-cent depression: does it improve outcomes compared with monotherapy? CNSDrugs 2009;23(4):271–80.
24. Kocsis JH, Gelenberg AJ, Rothbaum BO, et al. Cognitive behavioral analysis systemof psychotherapy and brief supportive psychotherapy for augmentation of antidepres-sant nonresponse in chronic depression The REVAMP trial. Arch Gen Psychiatry2009;66:1178–88.
25. Schramm E, van Calker D, Dykierek P, et al. An intensive treatment program ofinterpersonal psychotherapy plus pharmacotherapy for depressed inpatients: acuteand long-term results. Am J Psychiatry 2007;164:768–77.
26. Zobel I, Kech S, van Calker D, et al. Long-term effect of combined interpersonalpsychotherapy and pharmacotherapy in a randomized trial of depressed patients.
Acta Psychiatr Scand 2011;123:276–82.
178 Busch & Sandberg
27. Nemeroff CB, Heim CM, Thase ME, et al. Differential responses to psychotherapyversus pharmacotherapy in patients with chronic forms of major depression andchildhood trauma. Proc Natl Acad Sci USA 2003;100:14293–6.
28. Maina G, Rosso G, Bogetto F. Brief dynamic therapy combined with pharmacother-apy in the treatment of major depressive disorder: long-term results. J Affect Disord2009;114:200–7.
29. Bockting CL, Spinhoven P, Wouters LF, et al. DELTA Study Group. Long-term effectsof preventive cognitive therapy in recurrent depression: a 5.5–year follow-up study. JClin Psychiatry 2009;70(12):1621–8.
30. Fava GA, Ruini C, Rafanelli C, et al. Six-year outcome of cognitive behavior therapy forprevention of recurrent depression. Am J Psychiatry 2004;161:1872–6.
31. Post RM. Transduction of psychosocial stress into the neurobiology of recurrentaffective disorder. Am J Psychiatry 1992;149:999–1010.
32. Segal ZV, Bieling P, Young T, et al. Antidepressant monotherapy vs sequentialpharmacotherapy and mindfulness-based cognitive therapy, or placebo, for relapseprophylaxis in recurrent depression. Arch Gen Psychiatry 2010;67:1256–64.
33. Kennard BD, Emslie GJ, Mayes TL. Cognitive-behavioral therapy to prevent relapse inpediatric responders to pharmacotherapy for major depressive disorder J Am AcadChild Adolesc Psychiatry 2008;47(12):1395–404.
34. Fava GA, Rafanelli C, Grandi S, et al. Prevention of recurrent depression with cognitivebehavioral therapy: preliminary findings. Arch Gen Psychiatry 1998;55:816–20.
35. Frank E, Grochocinski VJ, Spanier CA, et al. Interpersonal psychotherapy andantidepressant medication: evaluation of a sequential treatment strategy in womenwith recurrent major depression. J Clin Psychiatry 2000;61(1):51–7.
36. Imel ZE, Malterer MB, Mckay KM, et al. A metaanalysis of psychotherapy andmedication in unipolar depression and dysthymia. J Affect Disord 2008;110:197–206.
37. Markowitz JC, Kocsis JH, Bleiberg KL, et al. Research report a comparative trial ofpsychotherapy and pharmacotherapy for “pure” dysthymic patients. J Affect Disord2005;89: 167–75.
38. Keller MB, Mccullough JP, Klein DN, et al. A comparison of nefazodone, the cognitivebehavioral-analysis system of psychotherapy, and their combination for the treatmentof chronic depression. N Engl J Med 2000;342:1462–70.
39. Manber R, Kraemer HC, Arnow BA, et al. Faster remission of chronic depression withcombined psychotherapy and medication than with each therapy alone. J ConsultClin Psychol 2008;76:459–67.
40. Grilo CM, Stout RL, Markowitz JC, et al. Personality disorders predict relapse afterremission from an episode of major depressive disorder: a 6-year prospective study.J Clin Psychiatry 2010;71:1629–35.
41. Kool S, Dekker J, Duijsens IJ, et al. Changes in personality pathology afterpharmacotherapy and combined therapy for depressed patients. J Pers Disord2003;17:60 –72.
42. Maddux RE, Riso LP, Klein DN, et al. Select comorbid personality disorders and thetreatment of chronic depression with nefazodone, targeted psychotherapy, or theircombination. J Affect Disord 2009;117:174–9.
43. Maina G, Rosso G, Crepi C, et al. Combined brief dynamic therapy and pharmaco-therapy in the treatment of major depressive disorder: a pilot study. PsychotherPsychosom 2007;76:298–305.
44. Driessen E, Cuijpers P, de Maat SC, et al. The efficacy of short-term psychodynamic
psychotherapy for depression: a meta-analysis. Clin Psychol Rev 2010;30(1):25–36.
179Combined Treatment of Depression
45. Joyce PR, McKenzie JM, Carter JD, et al. Temperament, character and personalitydisorders as predictors of response to interpersonal psychotherapy and cognitive-behavior therapy for depression. Br J Psychiatry 2007;190:503–8.
46. Dixon-Gordon K, Turner B, Chapman A. Psychotherapy for personality disorders. IntRev Psychiatry 2011;23(3):282–302.
47. Dewan M. Are psychiatrists cost-effective? An analysis of integrated versus splittreatment. Am J Psychiatry 1999;156(2):324–6.
48. Goldman W, McCulloch J, Cuffel B, et al. Outpatient utilization patterns of integratedand split psychotherapy and pharmacotherapy for depression. Psychiatr Serv 1998;49:477–82.
49. Busch FN, Gould E. Transference/countertransference in the pharmacotherapy/psychotherapy triangle. Hosp Community Psychiatry 1993;44:772–4.
50. Gould E, Busch FN. Special issues in the psychopharmacology/psychotherapytriangle. Psychoanal Inq 1998;18:730–45.
51. Leichsenring F, Rabung S. Effectiveness of long-term psychodynamic psychother-apy: a meta-analysis. JAMA 2008;300(13):1551–65.