Embed Size (px)
Citation preview

01.10WA192S
Combined Evidence ofCoverage and PolicyGeneral City of Seattle Employees,
Fire Chiefs, Library, SeattleHousing Authority
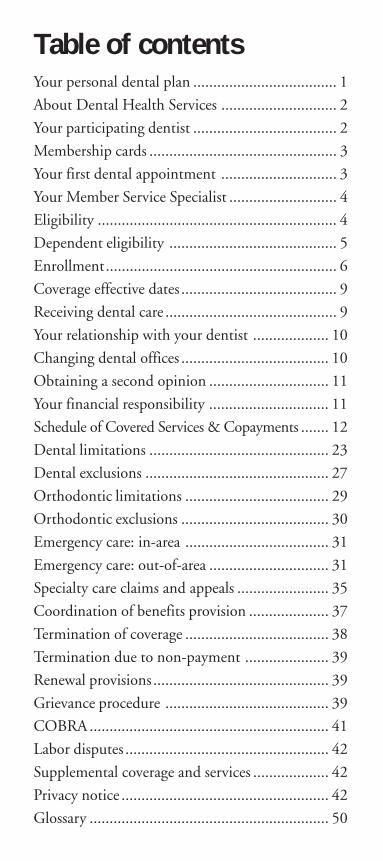
Table of contentsYour personal dental plan .................................... 1
About Dental Health Services ............................. 2
Your participating dentist .................................... 2
Membership cards ............................................... 3
Your first dental appointment ............................. 3
Your Member Service Specialist ........................... 4
Eligibility ............................................................ 4
Dependent eligibility .......................................... 5
Enrollment.......................................................... 6
Coverage effective dates ....................................... 9
Receiving dental care ........................................... 9
Your relationship with your dentist ................... 10
Changing dental offices ..................................... 10
Obtaining a second opinion .............................. 11
Your financial responsibility .............................. 11
Schedule of Covered Services & Copayments ....... 12
Dental limitations ............................................. 23
Dental exclusions .............................................. 27
Orthodontic limitations .................................... 29
Orthodontic exclusions ..................................... 30
Emergency care: in-area .................................... 31
Emergency care: out-of-area .............................. 31
Specialty care claims and appeals ....................... 35
Coordination of benefits provision .................... 37
Termination of coverage .................................... 38
Termination due to non-payment ..................... 39
Renewal provisions ............................................ 39
Grievance procedure ......................................... 39
COBRA ............................................................ 41
Labor disputes ................................................... 42
Supplemental coverage and services ................... 42
Privacy notice .................................................... 42
Glossary ............................................................ 50
Your personal dental planWelcome to Dental Health Services! We want tokeep you smiling by helping you protect yourteeth, saving you time and saving you money. Weare proud to offer you and your family excellentdental coverage that:
Encourages treatment by eliminating the burdens ofdeductibles and plan maximums.
Makes it easy to receive your dental care withoutclaim forms for most procedures.
Recognizes receiving regular diagnostic andpreventive care with low, or no copayments is the keyto better health and long term savings.
Facilitates care by making all covered servicesavailable as soon as membership becomes effective.
Simplifies access by not requiring pre-authorizationfor treatment from the general dentist you’veselected from our network.
Assures availability of care with high-quality, easy tofind dental offices throughout Washington Stateand our network is continually expanding; pleasecontact our office at 206.788.3444 or877.495.4455, or visit www.smartsmile.com/cityofseattle for the latest listing of our dentists.
Allows you to take an active role in your dental healthand treatment by fully disclosing coverages andexact copayments prior to treatment.
Recognizes the importance of appearance andaesthetics by offering a discount for cosmetic dentalprocedures.
1
In addition to your ongoing dental hygiene andcare, the following are available for plan members:
• ToothTipsSM oral health information sheets
• Member Service Specialists to assist you bytelephone, fax, or e-mail
• Web access to valuable plan and oral healthinformation at www.smartsmile.com/cityofseattle
About Dental Health ServicesDental Health Services has been a licensed limitedhealthcare service contractor since 1984. We arededicated to assuring your satisfaction and tokeeping your plan as simple and clear as possible.
Part of our service focus includes easy, toll-freeaccess to your knowledgeable Member ServiceSpecialist, an automated member assistance andeligibility system, and www.smartsmile.com/cityofseattle to help answer questions about yourplan and its benefits.
Your participating dentistService begins with the selection of local,independently owned, Quality Assured dentaloffices. Professional skill, commitment toprevention and wellness, convenience of locationand flexibility in appointment scheduling are someof the most important criteria involved inapproving a participating dentist. The ongoingcare of each dental office is monitored regularlythrough our rigorous Quality Assurance standards.You can rest assured that you are getting thequality care you deserve.
2
Membership cardsAt approximately the time your coverage becomeseffective, you will receive one membership card perfamily. Your participating dentist receives anupdated membership list each month, so it is notnecessary to have your membership card to makean appointment or receive care. If you would likean additional card, please contact your MemberService Specialist or request one online atwww.smartsmile.com/cityofseattle.
Your first dental appointmentYour initial appointment is an opportunity for youto meet your selected participating dentist. Yourdentist will complete an oral examination andformulate a treatment plan with you based on hisor her assessment of your oral health.
Your initial exam may require additional diagnosticservices such as periodontal charting and x-rays.You may also be charged copayments for additionalservices as necessary. There is also an office visitcopayment that is charged for each office visitregardless of the procedures performed.
After your initial visit, you may schedule anappointment for future care, such as cleanings, tocomplete your treatment plan. You may referenceyour treatment plan with your Schedule ofCovered Services and Copayments (starting onpage 12) to determine the copayments for yourscheduled procedures.
Please note that crowns and bridges may require anextra charge for metal upgrades or upgradedspecialized porcelain. Copayments are due in full atthe time services are performed.
3
EligibilityYou are in an eligible class if you: (a) work at least80 hours per month and are an active, regular full-time employee or a temporary employee* in abenefits-eligible assignment and work at least 80hours per month, or (b) are a temporary employeewho is not in a benefits-eligible assignment, buthave worked at least 1,040 cumulative non-overtime hours and at least 800 non-overtimehours in the previous 12 month period.
You must not be represented by a bargaining groupfor which a separate summary of coverage isavailable. Your employer will provide you with thisinformation. Employees, temporary and regular,losing eligibility due to a reduction of hours maycontinue coverage through the COBRA plan asdescribed in the COBRA section (page 40).
* Other than a Seattle Police Officers’ Guild, Local77 or Fire Chief employee
Your Member Service SpecialistPlease feel free to call, fax, e-mail through ourwebsite, or write us anytime with questions orcomments. We are ready to help you. YourMember Service Specialist can be reached throughany of the following ways:
Phone: 206.788.3444 or 877.495.4455Fax: 206.624.8755Web: www.smartsmile.com/cityofseattleMail: Dental Health Services
936 N 34th St., Ste. 208Seattle, WA 98103
4
Dependent eligibilityTo be eligible for coverage as a dependent, thedependent must be one of the following (proof ofdependency may periodically be required byDental Health Services):
• Lawful wife or husband (unless legallyseparated);
• Domestic partner who you have named in anAffidavit of Marriage/Domestic Partnership onfile with your employer; and
• Children who are under 26 years of age.
• A dependent child who is covered by thecontract as a dependent child on the day beforehis or her 26th birthday and continues to beboth:
(a) incapable of self-sustaining employment byreason of developmental disability orphysical challenge, and;
(b) chiefly dependent upon the Subscriber,spouse, domestic partner or non-coveredlegal parent for support and maintenancewill be eligible for coverage during theuninterrupted continuance of theincapacity and dependency, provided proofof incapacity and dependency is furnishedto Dental Health Services within 31 daysof the request for that information byDental Health Services or Group, but notmore frequently than annually after thetwo year period following the child'sattainment of 26 years of age.
5
Your children include:
• Your biological children
• Your adopted or legally placed for adoptionchildren
• Your stepchildren for whom your home is theirpermanent residence
• Your domestic partner’s children for whomyour home is their permanent residence
• Children for whom you are a legal guardianand for whom your home is their permanentresidence
EnrollmentAn employee of the Group who is eligible forcoverage on the effective date of the contract mustbecome a Subscriber at that time or wait until theGroup’s next open enrollment period.
If a person becomes an employee of the Groupafter the effective date of the Contract, DentalHealth Services must receive the enrollmentapplication for coverage within 31 days after theemployee first becomes eligible for coverage or theemployee must wait until the Group’s next openenrollment period.
Temporary employees must apply for coveragewhen first eligible in accordance with the termsestablished by the City or wait until the Group’snext open enrollment period. If an employee ofthe Group had other health coverage at the time ofinitial eligibility under this Contract and declinedenrollment under the Contract, in writing basedupon such coverage, the employee may apply for
6
coverage under the Contract prior to the Group’sopen enrollment period if Dental Health Servicesreceives the enrollment application within 31 daysof exhaustion of COBRA continuation coverage,or loss of the prior health coverage.
Dependents must be added at the time of initialenrollment or at the one year renewal date unlessone of the following apply:
1. Newborn children are covered from birth. Ifadding a newborn dependent increases yourpremium, Dental Health Services must receivea completed enrollment within 60 days tocontinue coverage for the newborn;
2. Adoptive children are covered from the date ofplacement for a period of 60 days. If theaddition of an adoptive or foster child as adependent increases your premium, DentalHealth Services must receive a completedenrollment form within 60 days to continuecoverage for the adoptive child;
3. New spouse or domestic partner may beenrolled within 31 days, and any additionalchildren due to marriage or signed domesticpartnership affidavit may be enrolled within 31days of the event; or
4. Loss of other coverage.
If any of these circumstances apply, please contactyour group administrator to enroll dependents.
7
All eligible employees, newly eligible employees,eligible temporary employees or eligibledependents who fail to enroll during the openenrollment period may enroll in the plan outside ofthe open enrollment period only if the followingapplies:
The deparment of social and health servicesdetermines that it is cost-effective to enrollany person (Subscriber or dependents)participating in a medical assistanceprogram under chapter 74.09 RCW in anemployer-sponsored dental plan, DentalHealth Services shall permit the enrollmentof the participant who is otherwise eligiblefor coverage in the dental plan withoutregard to any open enrollment restrictions.The request for special enrollment shall bemade by the department or participantwithin sixty days of the department’sdetermination that the enrollment wouldbe cost-effective.
It is recommended that Dental Health Services benotified in the event of a newborn or child receivedthrough adoption to notify the participatingdentist of coverage and eligibility and to ensurethey have access to member services. This allowsDental Health Services to provide preventivedental care and other services as necessary.
8
Coverage effective datesCoverage for a Subscriber and for any dependentincluded on the Subscriber’s initial enrollmentapplication will begin on the first day of the monthfollowing date of hire, or concurrent with the dateof hire if on paid status the first of the month,provided the application for coverage has beenmade and the premium has been paid.
Coverage for temporary employees will begin onthe first of the month following the date theapplication has been made and the premium paid.An employee who is absent without pay on thefirst of the month and returns by the 15th of themonth will not have a lapse in coverage. Coveragefor an employee who returns after the 15th of themonth will begin the first of the following month.
In the case of a Subscriber’s natural newborn child,coverage will be retroactive to the date of birth ifthe Subscriber applies for coverage as specified inthis Section. Coverage for the Subscriber’sadoptive child will be retroactive to the date ofplacement for adoption, or the date the Subscriberassumed a total or partial legal obligation forsupport of a child in anticipation of adoption.
Receiving dental careUpon enrolling in your plan, you should selectyour participating dentist. Directories are availableby calling your Member Service Specialist at206.788.3444 or 877.495.4455, or online throughwww.smartsmile.com/cityofseattle.
You may make an appointment with your dentistas soon as your eligibility has been confirmed.
9
Simply call the telephone number as it appearsbelow the dental office address in your Directory ofParticipating Dentists and request an appointment.Routine appointments will be scheduled within areasonable time; in non-emergency cases, areasonable time shall not be more than threeweeks. You are only eligible for services at yourparticipating dentist's office, except in anemergency situation.
Your relationship with your dentist
Dental Health Services values its members andparticipating dentists. Providing an environmentthat encourages healthy relationships betweenmembers and their dentists help to ensure thestability and quality of your dental plan.
Participating dentists are responsible for providingdental advice or treatment independently, andwithout interference, from Dental Health Servicesor any affiliated agents. If a satisfactoryrelationship cannot be established between amember and their participating dentist, DentalHealth Services, the member, or the dentistreserves the right to request the member’saffiliation with the dental office be terminated.
Any request to terminate a specific member/dentistrelationship should be submitted to Dental HealthServices and shall be effective the first day of themonth following receipt of the request. DentalHealth Services will always put forth its best effortto place the member with another dentist.
Changing dental officesIf you wish to change dentists you must notifyDental Health Services. This may be done by
10
phone, in writing, by fax, or online. Requests canbe made through 206.788.3444 or 877.495.4455,or by fax at 206.624.8755. Online changes can bedone through www.smartsmile.com/cityofseattle.
Requests received by the 20th of the currentmonth become effective the first day of thefollowing month. Changes made after the 20thbecome effective the first day of the second monthfollowing receipt.
Obtaining a second opinionIf you believe you need a second opinion for anyreason, Dental Health Services can arrange for youto be seen by another participating dentist. Youshould bring your x-rays to this consultation. If x-rays are unnecessary, you will pay only your officevisit and second opinion copayments.
After you receive your second opinion you mayreturn to your initial participating dental office fortreatment. If, however, you wish to select a newdentist you must contact Dental Health Servicesdirectly, either by phone or in writing, beforeproceeding with your treatment plan.
Your financial responsibilityYou are liable to your participating dentist forcopayments and incidental broken appointmentpenalties or interest charges. Please be aware thatyou are also liable for any other amounts owed foruncovered services. All dental treatmentcopayments are to be paid at the time of servicedirectly to your participating dental office.
As stated under the Emergency care: out-of-areasection of this booklet, for services rendered by a
11
non-contracted dentist, Dental Health Services willpay for the cost of emergency care beyond yourapplicable copayment. You are responsible for anyother costs.
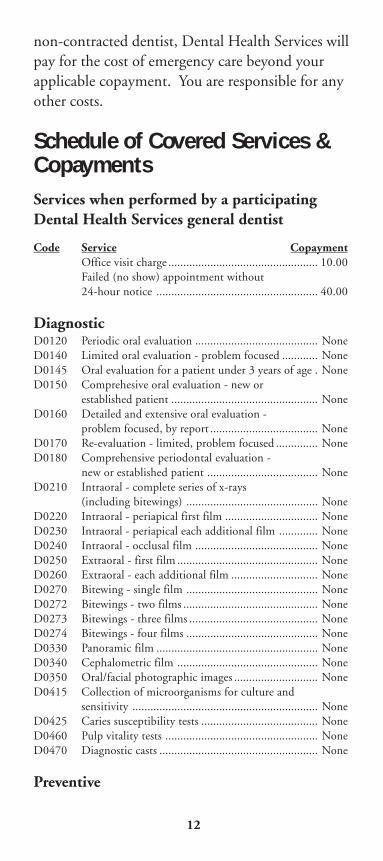
Schedule of Covered Services &CopaymentsServices when performed by a participatingDental Health Services general dentist
Code Service CopaymentOffice visit charge .................................................. 10.00Failed (no show) appointment without24-hour notice ...................................................... 40.00
DiagnosticD0120 Periodic oral evaluation ......................................... NoneD0140 Limited oral evaluation - problem focused ............ NoneD0145 Oral evaluation for a patient under 3 years of age . NoneD0150 Comprehesive oral evaluation - new or
established patient ................................................. NoneD0160 Detailed and extensive oral evaluation -
problem focused, by report .................................... NoneD0170 Re-evaluation - limited, problem focused .............. NoneD0180 Comprehensive periodontal evaluation -
new or established patient ..................................... NoneD0210 Intraoral - complete series of x-rays
(including bitewings) ............................................ NoneD0220 Intraoral - periapical first film ............................... NoneD0230 Intraoral - periapical each additional film ............. NoneD0240 Intraoral - occlusal film ......................................... NoneD0250 Extraoral - first film ............................................... NoneD0260 Extraoral - each additional film ............................. NoneD0270 Bitewing - single film ............................................ NoneD0272 Bitewings - two films ............................................. NoneD0273 Bitewings - three films ........................................... NoneD0274 Bitewings - four films ............................................ NoneD0330 Panoramic film ...................................................... NoneD0340 Cephalometric film ............................................... NoneD0350 Oral/facial photographic images ............................ NoneD0415 Collection of microorganisms for culture and
sensitivity .............................................................. NoneD0425 Caries susceptibility tests ....................................... NoneD0460 Pulp vitality tests ................................................... NoneD0470 Diagnostic casts ..................................................... None
Preventive
12
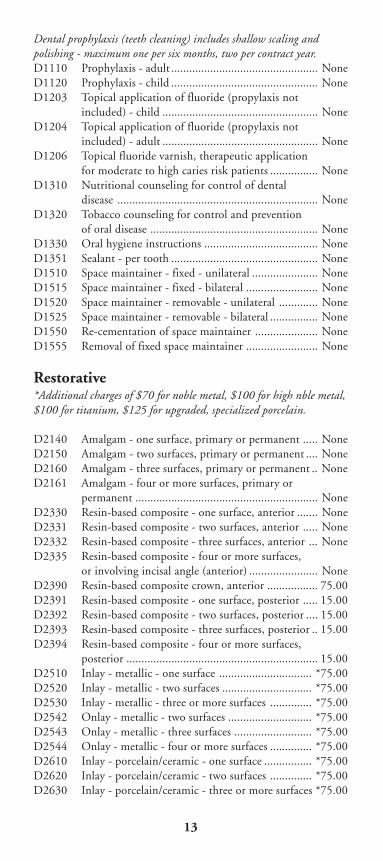
Dental prophylaxis (teeth cleaning) includes shallow scaling andpolishing - maximum one per six months, two per contract year.D1110 Prophylaxis - adult ................................................. NoneD1120 Prophylaxis - child ................................................. NoneD1203 Topical application of fluoride (propylaxis not
included) - child .................................................... NoneD1204 Topical application of fluoride (propylaxis not
included) - adult .................................................... NoneD1206 Topical fluoride varnish, therapeutic application
for moderate to high caries risk patients ................ NoneD1310 Nutritional counseling for control of dental
disease ................................................................... NoneD1320 Tobacco counseling for control and prevention
of oral disease ........................................................ NoneD1330 Oral hygiene instructions ...................................... NoneD1351 Sealant - per tooth ................................................. NoneD1510 Space maintainer - fixed - unilateral ...................... NoneD1515 Space maintainer - fixed - bilateral ........................ NoneD1520 Space maintainer - removable - unilateral ............. NoneD1525 Space maintainer - removable - bilateral ................ NoneD1550 Re-cementation of space maintainer ..................... NoneD1555 Removal of fixed space maintainer ........................ None
Restorative*Additional charges of $70 for noble metal, $100 for high nble metal,$100 for titanium, $125 for upgraded, specialized porcelain.
D2140 Amalgam - one surface, primary or permanent ..... NoneD2150 Amalgam - two surfaces, primary or permanent .... NoneD2160 Amalgam - three surfaces, primary or permanent .. NoneD2161 Amalgam - four or more surfaces, primary or
permanent ............................................................. NoneD2330 Resin-based composite - one surface, anterior ....... NoneD2331 Resin-based composite - two surfaces, anterior ..... NoneD2332 Resin-based composite - three surfaces, anterior ... NoneD2335 Resin-based composite - four or more surfaces,
or involving incisal angle (anterior) ....................... NoneD2390 Resin-based composite crown, anterior ................. 75.00D2391 Resin-based composite - one surface, posterior ..... 15.00D2392 Resin-based composite - two surfaces, posterior .... 15.00D2393 Resin-based composite - three surfaces, posterior .. 15.00D2394 Resin-based composite - four or more surfaces,
posterior ................................................................ 15.00D2510 Inlay - metallic - one surface ............................... *75.00D2520 Inlay - metallic - two surfaces .............................. *75.00D2530 Inlay - metallic - three or more surfaces .............. *75.00D2542 Onlay - metallic - two surfaces ............................ *75.00D2543 Onlay - metallic - three surfaces .......................... *75.00D2544 Onlay - metallic - four or more surfaces .............. *75.00D2610 Inlay - porcelain/ceramic - one surface ................ *75.00D2620 Inlay - porcelain/ceramic - two surfaces .............. *75.00D2630 Inlay - porcelain/ceramic - three or more surfaces *75.00
13
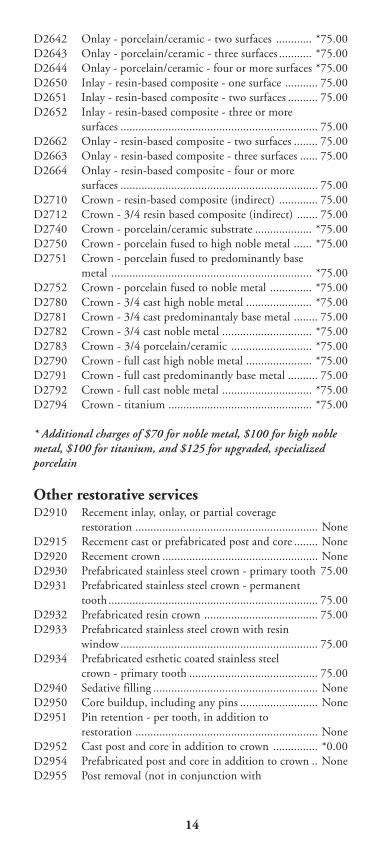
D2642 Onlay - porcelain/ceramic - two surfaces ............ *75.00D2643 Onlay - porcelain/ceramic - three surfaces ........... *75.00D2644 Onlay - porcelain/ceramic - four or more surfaces *75.00D2650 Inlay - resin-based composite - one surface ........... 75.00D2651 Inlay - resin-based composite - two surfaces .......... 75.00D2652 Inlay - resin-based composite - three or more
surfaces .................................................................. 75.00D2662 Onlay - resin-based composite - two surfaces ........ 75.00D2663 Onlay - resin-based composite - three surfaces ...... 75.00D2664 Onlay - resin-based composite - four or more
surfaces .................................................................. 75.00D2710 Crown - resin-based composite (indirect) ............. 75.00D2712 Crown - 3/4 resin based composite (indirect) ....... 75.00D2740 Crown - porcelain/ceramic substrate ................... *75.00D2750 Crown - porcelain fused to high noble metal ...... *75.00D2751 Crown - porcelain fused to predominantly base
metal ................................................................... *75.00D2752 Crown - porcelain fused to noble metal .............. *75.00D2780 Crown - 3/4 cast high noble metal ...................... *75.00D2781 Crown - 3/4 cast predominantaly base metal ........ 75.00D2782 Crown - 3/4 cast noble metal .............................. *75.00D2783 Crown - 3/4 porcelain/ceramic ........................... *75.00D2790 Crown - full cast high noble metal ...................... *75.00D2791 Crown - full cast predominantly base metal .......... 75.00D2792 Crown - full cast noble metal .............................. *75.00D2794 Crown - titanium ................................................ *75.00
* Additional charges of $70 for noble metal, $100 for high noblemetal, $100 for titanium, and $125 for upgraded, specializedporcelain
Other restorative servicesD2910 Recement inlay, onlay, or partial coverage
restoration ............................................................. NoneD2915 Recement cast or prefabricated post and core ........ NoneD2920 Recement crown .................................................... NoneD2930 Prefabricated stainless steel crown - primary tooth 75.00D2931 Prefabricated stainless steel crown - permanent
tooth ...................................................................... 75.00D2932 Prefabricated resin crown ...................................... 75.00D2933 Prefabricated stainless steel crown with resin
window.................................................................. 75.00D2934 Prefabricated esthetic coated stainless steel
crown - primary tooth ........................................... 75.00D2940 Sedative filling ....................................................... NoneD2950 Core buildup, including any pins .......................... NoneD2951 Pin retention - per tooth, in addition to
restoration ............................................................. NoneD2952 Cast post and core in addition to crown ............... *0.00D2954 Prefabricated post and core in addition to crown .. NoneD2955 Post removal (not in conjunction with
14
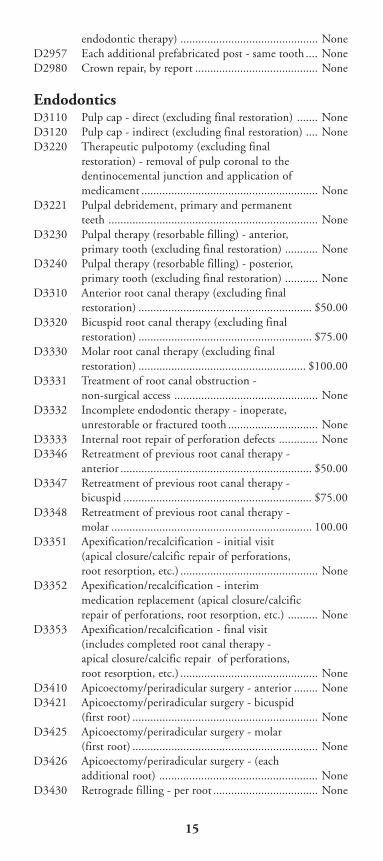
endodontic therapy) .............................................. NoneD2957 Each additional prefabricated post - same tooth .... NoneD2980 Crown repair, by report ......................................... None
EndodonticsD3110 Pulp cap - direct (excluding final restoration) ....... NoneD3120 Pulp cap - indirect (excluding final restoration) .... NoneD3220 Therapeutic pulpotomy (excluding final
restoration) - removal of pulp coronal to thedentinocemental junction and application ofmedicament ........................................................... None
D3221 Pulpal debridement, primary and permanentteeth ...................................................................... None
D3230 Pulpal therapy (resorbable filling) - anterior,primary tooth (excluding final restoration) ........... None
D3240 Pulpal therapy (resorbable filling) - posterior,primary tooth (excluding final restoration) ........... None
D3310 Anterior root canal therapy (excluding finalrestoration) .......................................................... $50.00
D3320 Bicuspid root canal therapy (excluding finalrestoration) .......................................................... $75.00
D3330 Molar root canal therapy (excluding finalrestoration) ........................................................ $100.00
D3331 Treatment of root canal obstruction -non-surgical access ................................................ None
D3332 Incomplete endodontic therapy - inoperate,unrestorable or fractured tooth .............................. None
D3333 Internal root repair of perforation defects ............. NoneD3346 Retreatment of previous root canal therapy -
anterior ................................................................ $50.00D3347 Retreatment of previous root canal therapy -
bicuspid ............................................................... $75.00D3348 Retreatment of previous root canal therapy -
molar ................................................................... 100.00D3351 Apexification/recalcification - initial visit
(apical closure/calcific repair of perforations,root resorption, etc.) .............................................. None
D3352 Apexification/recalcification - interimmedication replacement (apical closure/calcificrepair of perforations, root resorption, etc.) .......... None
D3353 Apexification/recalcification - final visit(includes completed root canal therapy -apical closure/calcific repair of perforations,root resorption, etc.) .............................................. None
D3410 Apicoectomy/periradicular surgery - anterior ........ NoneD3421 Apicoectomy/periradicular surgery - bicuspid
(first root) .............................................................. NoneD3425 Apicoectomy/periradicular surgery - molar
(first root) .............................................................. NoneD3426 Apicoectomy/periradicular surgery - (each
additional root) ..................................................... NoneD3430 Retrograde filling - per root ................................... None
15
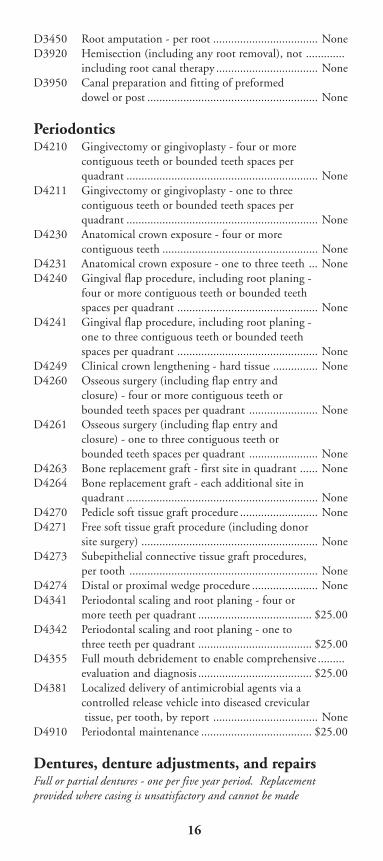
D3450 Root amputation - per root ................................... NoneD3920 Hemisection (including any root removal), not .............
including root canal therapy .................................. NoneD3950 Canal preparation and fitting of preformed
dowel or post ......................................................... None
PeriodonticsD4210 Gingivectomy or gingivoplasty - four or more
contiguous teeth or bounded teeth spaces perquadrant ................................................................ None
D4211 Gingivectomy or gingivoplasty - one to threecontiguous teeth or bounded teeth spaces perquadrant ................................................................ None
D4230 Anatomical crown exposure - four or morecontiguous teeth .................................................... None
D4231 Anatomical crown exposure - one to three teeth ... NoneD4240 Gingival flap procedure, including root planing -
four or more contiguous teeth or bounded teethspaces per quadrant ............................................... None
D4241 Gingival flap procedure, including root planing -one to three contiguous teeth or bounded teethspaces per quadrant ............................................... None
D4249 Clinical crown lengthening - hard tissue ............... NoneD4260 Osseous surgery (including flap entry and
closure) - four or more contiguous teeth orbounded teeth spaces per quadrant ....................... None
D4261 Osseous surgery (including flap entry andclosure) - one to three contiguous teeth orbounded teeth spaces per quadrant ....................... None
D4263 Bone replacement graft - first site in quadrant ...... NoneD4264 Bone replacement graft - each additional site in
quadrant ................................................................ NoneD4270 Pedicle soft tissue graft procedure .......................... NoneD4271 Free soft tissue graft procedure (including donor
site surgery) ........................................................... NoneD4273 Subepithelial connective tissue graft procedures,
per tooth ............................................................... NoneD4274 Distal or proximal wedge procedure ...................... NoneD4341 Periodontal scaling and root planing - four or
more teeth per quadrant ...................................... $25.00D4342 Periodontal scaling and root planing - one to
three teeth per quadrant ...................................... $25.00D4355 Full mouth debridement to enable comprehensive .........
evaluation and diagnosis ...................................... $25.00D4381 Localized delivery of antimicrobial agents via a
controlled release vehicle into diseased crevicular tissue, per tooth, by report ................................... None
D4910 Periodontal maintenance ..................................... $25.00
Dentures, denture adjustments, and repairsFull or partial dentures - one per five year period. Replacementprovided where casing is unsatisfactory and cannot be made
16
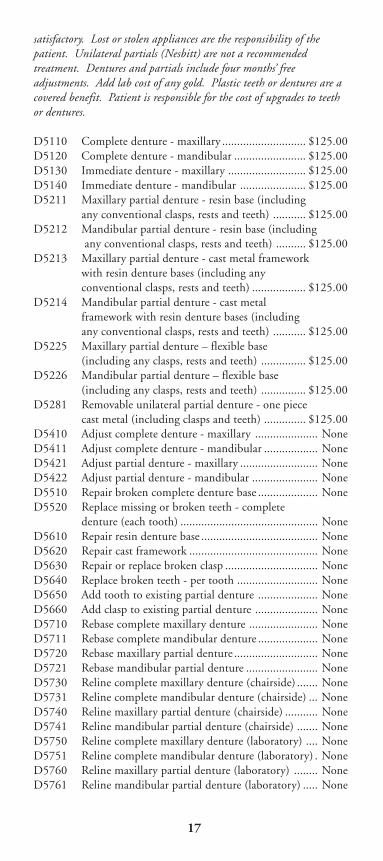
satisfactory. Lost or stolen appliances are the responsibility of thepatient. Unilateral partials (Nesbitt) are not a recommendedtreatment. Dentures and partials include four months’ freeadjustments. Add lab cost of any gold. Plastic teeth or dentures are acovered benefit. Patient is responsible for the cost of upgrades to teethor dentures.
D5110 Complete denture - maxillary ............................ $125.00D5120 Complete denture - mandibular ........................ $125.00D5130 Immediate denture - maxillary .......................... $125.00D5140 Immediate denture - mandibular ...................... $125.00D5211 Maxillary partial denture - resin base (including
any conventional clasps, rests and teeth) ........... $125.00D5212 Mandibular partial denture - resin base (including
any conventional clasps, rests and teeth) .......... $125.00D5213 Maxillary partial denture - cast metal framework
with resin denture bases (including anyconventional clasps, rests and teeth) .................. $125.00
D5214 Mandibular partial denture - cast metalframework with resin denture bases (includingany conventional clasps, rests and teeth) ........... $125.00
D5225 Maxillary partial denture – flexible base(including any clasps, rests and teeth) ............... $125.00
D5226 Mandibular partial denture – flexible base(including any clasps, rests and teeth) ............... $125.00
D5281 Removable unilateral partial denture - one piececast metal (including clasps and teeth) .............. $125.00
D5410 Adjust complete denture - maxillary ..................... NoneD5411 Adjust complete denture - mandibular .................. NoneD5421 Adjust partial denture - maxillary .......................... NoneD5422 Adjust partial denture - mandibular ...................... NoneD5510 Repair broken complete denture base .................... NoneD5520 Replace missing or broken teeth - complete
denture (each tooth) .............................................. NoneD5610 Repair resin denture base ....................................... NoneD5620 Repair cast framework ........................................... NoneD5630 Repair or replace broken clasp ............................... NoneD5640 Replace broken teeth - per tooth ........................... NoneD5650 Add tooth to existing partial denture .................... NoneD5660 Add clasp to existing partial denture ..................... NoneD5710 Rebase complete maxillary denture ....................... NoneD5711 Rebase complete mandibular denture .................... NoneD5720 Rebase maxillary partial denture ............................ NoneD5721 Rebase mandibular partial denture ........................ NoneD5730 Reline complete maxillary denture (chairside) ....... NoneD5731 Reline complete mandibular denture (chairside) ... NoneD5740 Reline maxillary partial denture (chairside) ........... NoneD5741 Reline mandibular partial denture (chairside) ....... NoneD5750 Reline complete maxillary denture (laboratory) .... NoneD5751 Reline complete mandibular denture (laboratory) . NoneD5760 Reline maxillary partial denture (laboratory) ........ NoneD5761 Reline mandibular partial denture (laboratory) ..... None
17
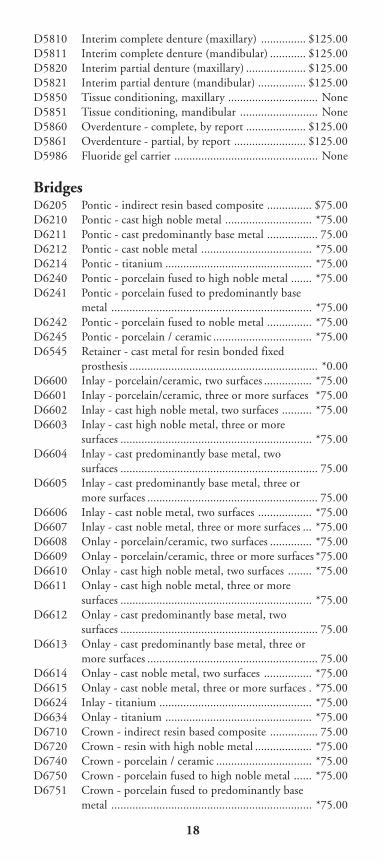
D5810 Interim complete denture (maxillary) ............... $125.00D5811 Interim complete denture (mandibular) ............ $125.00D5820 Interim partial denture (maxillary) .................... $125.00D5821 Interim partial denture (mandibular) ................ $125.00D5850 Tissue conditioning, maxillary .............................. NoneD5851 Tissue conditioning, mandibular .......................... NoneD5860 Overdenture - complete, by report .................... $125.00D5861 Overdenture - partial, by report ........................ $125.00D5986 Fluoride gel carrier ................................................ None
BridgesD6205 Pontic - indirect resin based composite ............... $75.00D6210 Pontic - cast high noble metal ............................. *75.00D6211 Pontic - cast predominantly base metal ................. 75.00D6212 Pontic - cast noble metal ..................................... *75.00D6214 Pontic - titanium ................................................. *75.00D6240 Pontic - porcelain fused to high noble metal ....... *75.00D6241 Pontic - porcelain fused to predominantly base
metal ................................................................... *75.00D6242 Pontic - porcelain fused to noble metal ............... *75.00D6245 Pontic - porcelain / ceramic ................................. *75.00D6545 Retainer - cast metal for resin bonded fixed
prosthesis ............................................................... *0.00D6600 Inlay - porcelain/ceramic, two surfaces ................ *75.00D6601 Inlay - porcelain/ceramic, three or more surfaces *75.00D6602 Inlay - cast high noble metal, two surfaces .......... *75.00D6603 Inlay - cast high noble metal, three or more
surfaces ................................................................ *75.00D6604 Inlay - cast predominantly base metal, two
surfaces .................................................................. 75.00D6605 Inlay - cast predominantly base metal, three or
more surfaces ......................................................... 75.00D6606 Inlay - cast noble metal, two surfaces .................. *75.00D6607 Inlay - cast noble metal, three or more surfaces ... *75.00D6608 Onlay - porcelain/ceramic, two surfaces .............. *75.00D6609 Onlay - porcelain/ceramic, three or more surfaces *75.00D6610 Onlay - cast high noble metal, two surfaces ........ *75.00D6611 Onlay - cast high noble metal, three or more
surfaces ................................................................ *75.00D6612 Onlay - cast predominantly base metal, two
surfaces .................................................................. 75.00D6613 Onlay - cast predominantly base metal, three or
more surfaces ......................................................... 75.00D6614 Onlay - cast noble metal, two surfaces ................ *75.00D6615 Onlay - cast noble metal, three or more surfaces . *75.00D6624 Inlay - titanium ................................................... *75.00D6634 Onlay - titanium ................................................. *75.00D6710 Crown - indirect resin based composite ................ 75.00D6720 Crown - resin with high noble metal ................... *75.00D6740 Crown - porcelain / ceramic ................................ *75.00D6750 Crown - porcelain fused to high noble metal ...... *75.00D6751 Crown - porcelain fused to predominantly base
metal ................................................................... *75.00
18
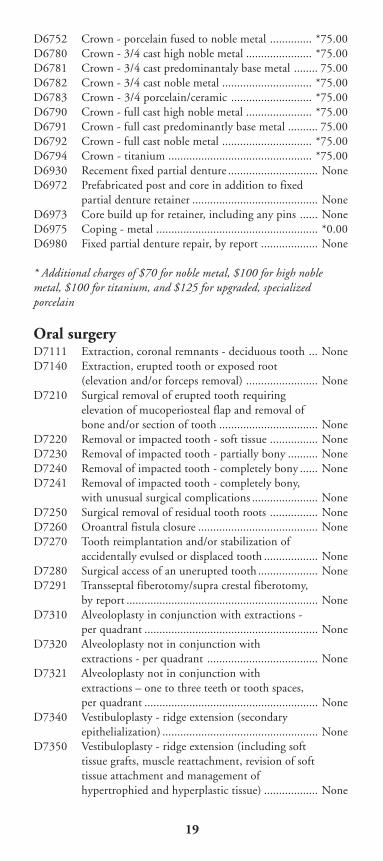
D6752 Crown - porcelain fused to noble metal .............. *75.00D6780 Crown - 3/4 cast high noble metal ...................... *75.00D6781 Crown - 3/4 cast predominantaly base metal ........ 75.00D6782 Crown - 3/4 cast noble metal .............................. *75.00D6783 Crown - 3/4 porcelain/ceramic ........................... *75.00D6790 Crown - full cast high noble metal ...................... *75.00D6791 Crown - full cast predominantly base metal .......... 75.00D6792 Crown - full cast noble metal .............................. *75.00D6794 Crown - titanium ................................................ *75.00D6930 Recement fixed partial denture .............................. NoneD6972 Prefabricated post and core in addition to fixed
partial denture retainer .......................................... NoneD6973 Core build up for retainer, including any pins ...... NoneD6975 Coping - metal ...................................................... *0.00D6980 Fixed partial denture repair, by report ................... None
* Additional charges of $70 for noble metal, $100 for high noblemetal, $100 for titanium, and $125 for upgraded, specializedporcelain
Oral surgeryD7111 Extraction, coronal remnants - deciduous tooth ... NoneD7140 Extraction, erupted tooth or exposed root
(elevation and/or forceps removal) ........................ NoneD7210 Surgical removal of erupted tooth requiring
elevation of mucoperiosteal flap and removal ofbone and/or section of tooth ................................. None
D7220 Removal or impacted tooth - soft tissue ................ NoneD7230 Removal of impacted tooth - partially bony .......... NoneD7240 Removal of impacted tooth - completely bony ...... NoneD7241 Removal of impacted tooth - completely bony,
with unusual surgical complications ...................... NoneD7250 Surgical removal of residual tooth roots ................ NoneD7260 Oroantral fistula closure ........................................ NoneD7270 Tooth reimplantation and/or stabilization of
accidentally evulsed or displaced tooth .................. NoneD7280 Surgical access of an unerupted tooth .................... NoneD7291 Transseptal fiberotomy/supra crestal fiberotomy,
by report ................................................................ NoneD7310 Alveoloplasty in conjunction with extractions -
per quadrant .......................................................... NoneD7320 Alveoloplasty not in conjunction with
extractions - per quadrant ..................................... NoneD7321 Alveoloplasty not in conjunction with
extractions – one to three teeth or tooth spaces,per quadrant .......................................................... None
D7340 Vestibuloplasty - ridge extension (secondaryepithelialization) .................................................... None
D7350 Vestibuloplasty - ridge extension (including softtissue grafts, muscle reattachment, revision of softtissue attachment and management ofhypertrophied and hyperplastic tissue) .................. None
19
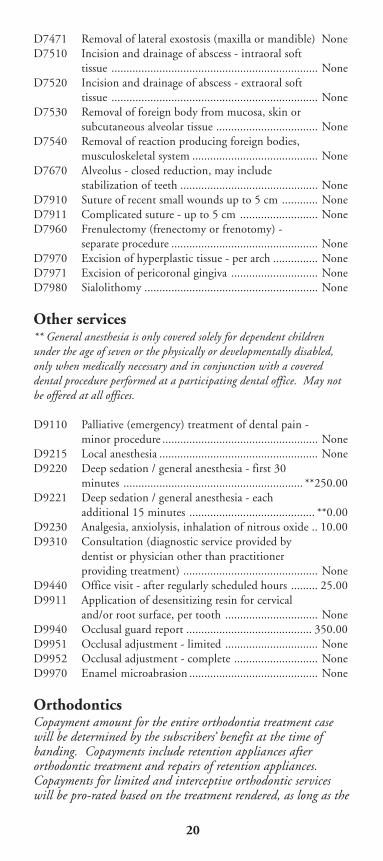
D7471 Removal of lateral exostosis (maxilla or mandible) NoneD7510 Incision and drainage of abscess - intraoral soft
tissue ..................................................................... NoneD7520 Incision and drainage of abscess - extraoral soft
tissue ..................................................................... NoneD7530 Removal of foreign body from mucosa, skin or
subcutaneous alveolar tissue .................................. NoneD7540 Removal of reaction producing foreign bodies,
musculoskeletal system .......................................... NoneD7670 Alveolus - closed reduction, may include
stabilization of teeth .............................................. NoneD7910 Suture of recent small wounds up to 5 cm ............ NoneD7911 Complicated suture - up to 5 cm .......................... NoneD7960 Frenulectomy (frenectomy or frenotomy) -
separate procedure ................................................. NoneD7970 Excision of hyperplastic tissue - per arch ............... NoneD7971 Excision of pericoronal gingiva ............................. NoneD7980 Sialolithomy .......................................................... None
Other services** General anesthesia is only covered solely for dependent childrenunder the age of seven or the physically or developmentally disabled,only when medically necessary and in conjunction with a covereddental procedure performed at a participating dental office. May notbe offered at all offices.
D9110 Palliative (emergency) treatment of dental pain -minor procedure .................................................... None
D9215 Local anesthesia ..................................................... NoneD9220 Deep sedation / general anesthesia - first 30
minutes ............................................................ **250.00D9221 Deep sedation / general anesthesia - each
additional 15 minutes .......................................... **0.00D9230 Analgesia, anxiolysis, inhalation of nitrous oxide .. 10.00D9310 Consultation (diagnostic service provided by
dentist or physician other than practitionerproviding treatment) ............................................. None
D9440 Office visit - after regularly scheduled hours ......... 25.00D9911 Application of desensitizing resin for cervical
and/or root surface, per tooth ............................... NoneD9940 Occlusal guard report .......................................... 350.00D9951 Occlusal adjustment - limited ............................... NoneD9952 Occlusal adjustment - complete ............................ NoneD9970 Enamel microabrasion ........................................... None
OrthodonticsCopayment amount for the entire orthodontia treatment casewill be determined by the subscribers’ benefit at the time ofbanding. Copayments include retention appliances afterorthodontic treatment and repairs of retention appliances.Copayments for limited and interceptive orthodontic serviceswill be pro-rated based on the treatment rendered, as long as the
20
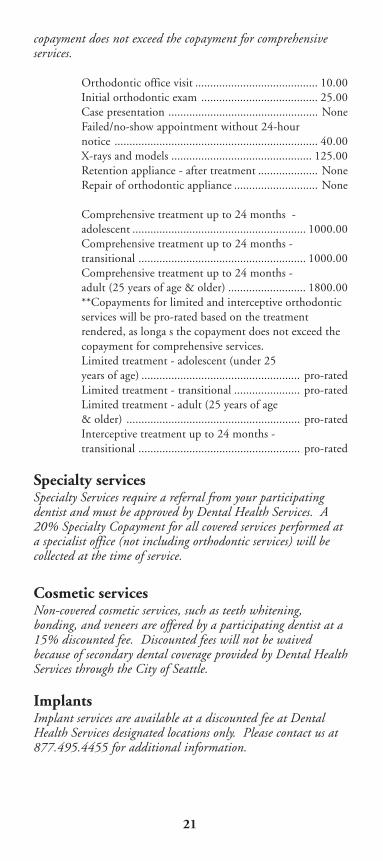
copayment does not exceed the copayment for comprehensiveservices.
Orthodontic office visit ......................................... 10.00Initial orthodontic exam ....................................... 25.00Case presentation .................................................. NoneFailed/no-show appointment without 24-hournotice .................................................................... 40.00X-rays and models ............................................... 125.00Retention appliance - after treatment .................... NoneRepair of orthodontic appliance ............................ None
Comprehensive treatment up to 24 months -adolescent .......................................................... 1000.00Comprehensive treatment up to 24 months -transitional ........................................................ 1000.00Comprehensive treatment up to 24 months -adult (25 years of age & older) .......................... 1800.00**Copayments for limited and interceptive orthodonticservices will be pro-rated based on the treatmentrendered, as longa s the copayment does not exceed thecopayment for comprehensive services.Limited treatment - adolescent (under 25years of age) ..................................................... pro-ratedLimited treatment - transitional ...................... pro-ratedLimited treatment - adult (25 years of age& older) .......................................................... pro-ratedInterceptive treatment up to 24 months -transitional ...................................................... pro-rated
Specialty servicesSpecialty Services require a referral from your participatingdentist and must be approved by Dental Health Services. A20% Specialty Copayment for all covered services performed ata specialist office (not including orthodontic services) will becollected at the time of service.
Cosmetic servicesNon-covered cosmetic services, such as teeth whitening,bonding, and veneers are offered by a participating dentist at a15% discounted fee. Discounted fees will not be waivedbecause of secondary dental coverage provided by Dental HealthServices through the City of Seattle.
ImplantsImplant services are available at a discounted fee at DentalHealth Services designated locations only. Please contact us at877.495.4455 for additional information.
21
Discounted fees will not be waived because of secondary dentalcoverage provided by Dental Health Services through the Cityof Seattle.
Pre-natal Periodontal BenefitIn order to improve the overall health of our enrollees, your planincludes a pre-natal health improvement program.
Numerous studies indicate that women who have periodontaldisease while pregnant are at much greater risk for having otherhealth issues. While you are pregnant, your benefit includes aprogram to reimburse your copayments for necessary periodonticservices when provided by a Dental Health Services’ GeneralDentist.
This includes additional cleanings, scalings and periodontalirrigation/antimicrobials treatment determined by your dentistto be necessary.
You must submit an itemized receipt from the dental office thatprovided the services and an attestation of your pregnancy toDental Health Services within 60 days of treatment.
Current Dental Terminology © 2007 American DentalAssociation. All rights reserved.
22
Dental limitationsA. Authorized treatment is rendered only by your
selected participating provider. Servicesprovided by a dentist other than the enrollee’sdesignated participating provider, except foremergency dental conditions, are not covered.(See item C. below)
B. Limitation on the frequency andappropriateness of services:
1. Prophylaxis (teeth cleaning, shallow scalingand polishing) – maximum one per sixmonths, 2 per contract year.
2. Periodontal scaling and periodontalmaintenance – limited to four quadrantsper six months.
3. Periodontal surgery: Periodontal surgicalprocedures are limited to 4 quadrants in 2years.
4. Full/partial dentures (upper and/or lower)– one per five year period. Replacement ofappliances that are causing pain, bleeding,swelling or are required due to additionaltooth loss which cannot be restored bymodification of the appliance are covered.New dentures are covered only if theexisting denture cannot be madesatisfactory by either a reline or repair.Lost or stolen appliances are theresponsibility of the patient.
5. Fixed bridges, crowns, gold restorations orjackets are available once per five years.Replacements are available after five years.
23
6. Denture relines – one per year, per arch
7. Full-mouth x-rays – once every three yearsor as determined necessary by your dentist.
8. Partial dentures are appropriate treatmentwhen dental spaces are bilateral and can besatisfactorily restored with removabledentures. Unilateral partials (Nesbitt) arenot a recommended treatment.
9. Acid etched bridge (Maryland) isappropriate only on the anterior area.
10. Fixed bridges are optional and restricted forpatients under the age of 16 whenperiodontal tissue is not supportive or inthe presence of bilateral spaces.
11. Treatment by a pedodontist for baby bottlemouth syndrome is limited to a lifetimebenefit of $500 per enrollee.
12. General anesthesia is only covered fordependent children aged 7 years and under.General anesthesia may not be offered at allparticipating provider offices.
C. Emergency dental condition – is the emergentand acute onset of a symptom or symptoms,including severe pain that would lead aprudent layperson acting reasonably to believethat dental condition exists that requiresimmediate, palliative care by a licensed dentistfor the relief of pain, swelling or bleeding.This does not include routine, extensive orpostponable treatment.
D. The additional cost to the enrollee for metalupgrades is $50 for noble metal, $80 forhigh noble metal and titanium, and $125 for
24
upgraded specialized porcelain.
E. Optional services (all cases in which theenrollee selects a plan of treatment that isconsidered unnecessary by the provider) arecharged to the enrollee at fee-for-service rates.
F. Cosmetic dentistry – services for appearanceonly are at a discount off full fees. Thisincludes the replacement of clinicallyacceptable amalgam fillings.
G. Implant services – implants are available at adiscounted fee at Dental Health Servicesdesignated locations only. Discounted servicesinclude evaluations and x-rays specific toimplants, surgical implant placement,abutments, and implant crowns. Not allservices related to implants are available at adiscount.
H. Unsatisfactory patient-doctor relationship:Dental Health Services providers reserve theright to limit or deny services to an enrolleewho fails to follow the prescribed course oftreatment, repeatedly fails to keepappointments, fails to pay applicablecopayments, is abusive to the participatingprovider or their staff, or obtains services byfraud or deception.
I. Submit claims within 60 days. Dental HealthServices shall not be liable to pay a claim foremergency care or for any Dental HealthServices authorized treatment provided by adentist other than a participating providerunless the enrollee submits the claim to DentalHealth Services within 60 days after treatment.
25
J. Denturist benefit is subject to existence andavailability of a licensed denturist within a 30mile radius. Enrollees may elect to travel to thenearest participating denturist for services.
K. Third molars (wisdom teeth) – complicatedextractions of third molars are at the discretionof the general dentist and are often referred tooral surgeons (specialist).
L. Specialty services requiring any referral to aspecialist must be pre-authorized by DentalHealth Services.
M. Not all participating dentists can perform alldental procedures, please verify what servicesyour selected provider can perform for you.
N. Services which are compensable under Worker’sCompensation or employer liability laws.
O. All treatment of temporomandibular joint(TMJ) disorders must be pre-authorized beforetreatment begins. Benefits will be denied iftreatment is not pre-authorized. Benefits arelimited to a maximum of $1,000 per year, notto exceed a lifetime maximum of $5,000. Nobenefits will be provided for the repair orreplacement of lost, stolen, or broken TMJappliances. All covered services must beprovided or ordered by a participating dentistand be:
1. Reasonable and appropriate for thetreatment of a disorder of thetemporomandibular joint;
2. Effective for the control or elimination ofone or more of the following, caused by adisorder of the temporomandibular joint:
26
pain, infection, disease, difficulty inspeaking, or difficulty in chewing andswallowing food;
3. Recognized as effective, according to theprofessional standards of good dentalpractice;
4. Not investigational;
5. Not primarily for cosmetic purposes.
Dental exclusionsA. Services not specifically covered in the
Schedule of Covered Services and Copayments.
B. Work in progress: Dental work in progress(non-emergency/temporary procedures startedbut not finished prior to the date of eligibility)is not covered. This includes crown prepsprepared and temporized but not cemented,root canals in mid-treatment, prosthetic casespost final impression stage (sent to the lab),etc. This does not include teeth slated for rootcanal treatment and/or canals filled during anemergency visit.
C. Services that in the opinion of the attendingdentist are not necessary for the patient’shealth. Extractions of non-pathologic,asymptomatic (healthy or non-symptomatic)teeth including extractions for orthodonticreasons.
D. Dispensing of drugs not normally supplied in adental office.
E. Any dental procedure or service rendered while
27
a patient is hospitalized or not in the dentaloffice.
F. Treatment for malignancies or neoplasms(tumors).
G. Procedures or charges for services prior to thedate the enrollee became eligible for benefitsunder this plan, or re-treatment of theseprocedures within one (1) year of completionor charges incurred following termination ofbenefits under this plan.
H. Any dental procedure that cannot beperformed in the dental office due to thegeneral health of the enrollee.
I. Procedures, appliances or restorations otherthan fillings that are necessary to alter, restoreor maintain occlusion, or are necessary for full-mouth rehabilitation, i.e. night guards,occlusal adjustments, etc.
J. Orthognathic treatment – surgical proceduresand other treatment to correct the malpositionof the maxilla and/or the mandible.
K. Full mouth rehabilitation is not covered.Procedures requiring extensive restorativetreatment involving more than 10 crowns in aone year period and/or an increase or decreaseof the horizontal or vertical dimension,gnathological recordings, full mouthequilibration, periodontal splinting, temporaryprocessed functional crowns/appliances andrealignment of teeth are not covered.
L. Services and supplies incurred vefore youreffective date under the plan except as may beprovided under the other continuation options
28
administered through your employer.
M. Any dental expense that is covered by a thirdparty, such as sautomobile insurance, otherliability insurance, etc.
N. Services and supplies for treatment of illness orinjury for which a third party is or may beresponsible.
O. Expenses for services and supplies incurred as aresult of any work related injury or illness,including any claims that are resolved relatedto a disputed claim settlement. The onlyexception is if an enrolled employee is exemptfrom state or federal workers’ compensationlaw.
Orthodontic limitations
A. Changes in treatment necessitated by accidentof any kind.
B. Services which are compensable underWorker’s Compensation or employer liabilitylaws.
C. Malocclusions too severe or mutilated whichare not amenable to ideal orthodontic therapy.
D. Orthodontic fees are based on treatment up to24 months.
Orthodontic exclusionsA. Replacement of lost or broken appliances.
29
B. Retreatment of orthodontic cases.
C. Treatment of a case in progress at inception ofeligibility, unless authorized by Dental HealthServices.
D. Surgical procedures (including extraction ofteeth) incidental to orthodontic treatment.
E. Treatment and/or surgical procedures relatedto cleft palate, micrognathia or microdontia.
F. Treatment related to temporomandibular jointdisturbances and/or hormonal imbalances.
G. Any dental procedures considered to be withinthe field of general dentistry, including but notlimited to:
1. Myofunctional therapy.
2. General anesthetics including intravenousand inhalation sedation.
3. Dental services of any nature performed ina hospital.
4. Services which are compensable underWorker’s Compensation or employerliability laws.
H. Payment by Dental Health Services fortreatment rendered or required after enrollee isno longer eligible for coverage. The cost oftreatment will be pro-rated and converted by aUCR (fee-for-service) amount.
Emergency care: in-areaPalliative care for emergency dental conditions in
30
which acute pain, bleeding, or dental infectionexists is a benefit according to your Schedule ofCovered Services and Copayments.
If you have a dental emergency and needimmediate care, first call your selected participatingdental office. Dental offices maintain 24-houremergency communication accessibility and areexpected to see you within 24 hours of initialcontact, or within such lesser time as may bemedically necessary. If your dentist is notavailable, call your Member Service Specialist at206.788.3444 or 877.495.4455.
If both your dental office and Dental HealthServices cannot be reached, you are covered foremergency care from another participating dentaloffice, or from any licensed dentist. You will bereimbursed for the cost of emergency palliativetreatment less any copayments that apply. Contactyour selected participating dentist for follow-upcare as soon as possible.
If you have a medical emergency, receive careimmediately by calling 911 or by going to thenearest hospital emergency room.
Emergency care: out-of-areaAll participating dental offices are expected tomaintain 24-hour emergency communicationaccessibility. Emergency (palliative) treatment canbe obtained from any participating dentist. In caseof an emergency dental condition, where noparticipating dentist within a reasonable distanceor time is available, no prior authorization isrequired to have emergency palliative treatmentperformed. Dental Health Services will beresponsible for dental service fees beyond all
31
applicable copayments in an emergency situation.Services for the treatment of emergency dentalconditions are solely limited to procedures to stopbleeding, and to reduce swelling and pain. Afteremergency treatment is performed the coveredperson must see their participating dentist to becovered by Dental Health Services.
If services for the treatment of an emergency dentalcondition are authorized by any service staffmember of Dental Health Services, Dental HealthServices may not deny the responsibility of feesbeyond all applicable copayments, unless approvalwas based on misrepresentation about the coveredperson's condition made by the dentist performingthe emergency treatment.
If an enrollee receives services for the treatment ofan emergency dental condition from a non-participating dentist, an additional $50.00 may becharged above the applicable copayments, unlessthe enrollee falls in one of the categories statedbelow. Dental Health Services will not charge anadditional $50.00 copayment for services for thetreatment of an emergency dental condition if:
1. Due to uncontrollable circumstances thecovered person is unable to go to aparticipating dentist in a timely fashionwithout serious detriment to their health.
2. A prudent layperson possessing averageknowledge of health and medicine would havereasonably believed that the covered personwould have been unable to arrive at aparticipating dental office in a timely fashionwithout serious impairment to the coveredperson's health.
After receiving treatment for an emergency dental
32
condition, Dental Health Services requires pre-authorization for out-of-network post-emergencytreatment. Dental Health Services shall provideaccess to an authorized representative 24 hours aday, seven days a week to facilitate reviews. Toobtain access to an authorized representative, call206.788.3444 or 877.495.4455 for instructions.
In order for services for the treatment of post-emergency dental condition(s) to be covered, thenon-participating dentist or facility must make adocumented good faith effort to contact DentalHealth Services within 30 minutes of stabilization.
Dental Health Services will respond within 30minutes. Failure to do so authorizes immediatelyrequired medically necessary services for thetreatment of post-emergency dental condition(s)unless Dental Health Services makes a good faitheffort to contact the non-participating dentistwithin 30 minutes. Dental Health Services shallimmediately arrange for an alternate plan oftreatment for the covered person if Dental HealthServices and the non-participating dentist cannotreach an agreement regarding necessary servicesbeyond those needed for the treatment of theemergency dental condition.
Dental Health Services may require that afterservices for the treatment of an emergency dentalcondition are performed, the covered person betransferred to a participating dental office for post-emergency dental condition treatment. Follow-upcare that is a direct result of the emergency must beobtained within Dental Health Services’ usualterms and conditions of coverage.
For an emergency handled by an out-of-networkdentist, enrollees are responsible for the entire bill.To be reimbursed for any amount over the
33
emergency copayment, plan members must submita Dental Health Services claim form, along withthe itemized dental bill. Dental Health Servicesonly reimburses for the amount over yourcopayment for dental work done to eliminate pain,swelling or bleeding. Dental Health Services claimforms may be requested directly from yourMember Service Specialist. Within 60 days of theoccurrence, send the claim form & itemized bill to:
Dental Health Services936 N 34th St., Suite 208Seattle, WA 98103
If you do not submit this information within 60days, Dental Health Services reserves the right torefuse payment.
All approved post-service emergency dental claimsare paid within 30 working days. If you submit acompleted claim appeal, a decision regarding yourappeal will be decided within 30 working days ofthe receipt of your appeal. You will be also notifiedof this decision within these 30 working days. Ifany additional information is needed by DentalHealth Services in order to reach a decisionregarding your claims appeal, you will be notifiedwithin 14 working days of your appeal’s receipt.
If you submit a claim involving urgent care, DentalHealth Services will notify you within 72 hoursafter receiving your claim. If information tocomplete the claim is insufficient, we will notifyyou of any additional information needed orprocedures that must be followed within 24 hours.Dental Health Services’ notification may be oral orwritten. Once we receive the needed informationto complete your claim, you will be notified within48 hours of your claim's approval or denial.
34
If you wish to appeal the result of your emergencycare claim, Dental Health Services will treat yourappeal as a grievance. Dental Health Services’Dental Director and Service Review Committeewill review your claim and make a determination.If your claim is denied and you appeal thedecision, a reviewer other than the dentistproviding the initial determination will review yourappeal. If the decision is based on medicaljudgment, the consulting dentist will be differentthan the one from the initial review process.Secondary appeals are referred to our Peer ReviewCommittee, which is comprised of independentdentists.
All urgent or emergency care appeals are decidedwithin 72 hours. If you appeal a claim decisionmade after you received the dental care uponwhich the claim is based, your appeal will bedecided within 30 days. You have 180 days toappeal any denied claim.
Specialty care claims and appealsAll treatment received from participatingspecialists must be pre-authorized.
Dental Health Services claim forms may berequested directly from your Member ServiceSpecialist. Within 60 days of the occurrence, sendthe claim form and itemized bill to:
Dental Health Services936 N 34th St., Suite 208Seattle, WA 98103
If you do not submit the invoice within 60 days,Dental Health Services reserves the right to refuse
35
payment.
If you submit a pre-service claim for authorization,within 15 days of receiving your claim you will benotified if your claim is approved or denied. This15 day period may be extended one time, for up toan additional 15 days, provided such an extensionis necessary due to circumstances beyond DentalHealth Services’ control. In the event an extensionis necessary, we will notify you of thesecircumstances requiring this extension within 5days of receiving your claim.
If you fail to submit your pre-service claim forauthorization according to the procedures outlinedin this brochure, within 5 days following DentalHealth Services’ discovery of any procedural error,you will be notified of the failure and the properprocedures to be followed in submitting yourclaim. Notification may be oral or written.
All approved dental claims are paid within 30working days. If you submit a completed claimappeal, a decision regarding your appeal will bedecided within 30 working days of the receipt ofyour appeal. You will be also notified of thisdecision within these 30 working days. If anyadditional information is needed by Dental HealthServices in order to reach a decision regarding yourclaims appeal, you will be notified within 14working days of the receipt of your appeal.
If you submit a claim involving urgent care, DentalHealth Services will notify you within 72 hoursafter receiving your claim. If information tocomplete the claim is insufficient, we will notifyyou of any additional information needed orprocedures that must be followed within 24 hours.Dental Health Services’ notification may be oral or
36
written. Once we receive the needed informationto complete your claim, you will be notified within48 hours of your claim's approval or denial.
If you wish to appeal the result of your claim,Dental Health Services will treat your appeal as agrievance. Dental Health Services’ Dental Directorand Service Review Committee will then reviewyour claim and make a determination. If yourclaim is denied and you appeal the decision, areviewer other than the dentist providing the initialdetermination will review your appeal. If thedecision is based on medical judgment, theconsulting dentist will be different than the onefrom the initial review process. Secondary appealsare referred to our Peer Review Committee, whichis comprised of independent dentists.
All urgent or emergency care appeals are decidedwithin 72 hours. If you appeal a claim decisionmade after you received the dental care uponwhich the claim is based, your appeal will bedecided within 30 days. You have 180 days toappeal any denied claim.
Coordination of benefits provision
This plan does not provide for coordination ofbenefits with other coverage. However, if yoursecondary dental coverage is provided by DentalHealth Services through the City of Seattle, allcopayments will be waived for all covered services.
Cosmetic services and implant services are at adiscounted fee and fees for these services will notbe waived.
Member is responsible to inform Dental HealthServices if they have dual coverage (both City ofSeattle employees and their spouse or domestic
37
partner have both elected Dental Health Servicesfor their primary dental plan). Member is to payall applicable copayments to the dental office at thetime of service (except for orthodontic treatmentcopayments, as these cases are pre-authorized).Member is to submit receipts for copayments(within 60 days of service) to Dental HealthServices and they will be reimbursed directly.
Termination of coverageCoverage of a subscriber and/or their dependentsmay be terminated for any of the followingreasons:1. Termination of the Group Dental Care
Services agreement by written notice 30 daysbefore annual anniversary date.
2. Failure of an enrollee to meet or maintaineligibility requirements.
3. Material misrepresentation (fraud) in obtainingcoverage.
4. Permitting the use of a Dental Health Servicesmembership card by another person, or usinganother person’s membership card oridentification to obtain care other than that towhich one is entitled.
5. Failure of the group to pay premium in atimely manner (30 days after payment is due.)
Termination due to non-paymentBenefits under your plan depend on the group'spremium payments staying current. If payment ismore than 30 days overdue, your eligibility may beterminated. Any previously initiated service(s)then “in progress” must be completed within 30days from the last appointment date occurring
38
prior to the termination date. The subscriber willremain liable for the scheduled copayment, if any.If your coverage is terminated, you will be requiredto pay your participating dentist’s usual fees forcontinuing the prescribed treatment.
Renewal provisionsThe group contract may be extended or renewedfrom year to year after its initial period. Renewalmay change the copayment and/or premium feespaid by the group and/or the subscriber. You mayobtain information about these changes, if any,from a Dental Health Services representativeduring the open enrollment period or by callingyour Member Service Specialist at 206.788.3444or 877.495.4455.
Grievance procedureComplaints by subscribers and enrollees shall behandled in the following manner:
A. Complaints may be made by phone or inwriting by a subscriber, enrollee, a participatingdentist, or an authorized representative.Complaints in writing may be made on formsprovided by Dental Health Services or simplyby providing a brief written explanation of thefacts and issue(s). Personnel at participatingdental offices are requested to be available toprovide assistance in the preparation andsubmission of any complaints.
B. Within 3 days of receiving a complaint, DentalHealth Services will acknowledge its receipt inwriting, including the name and telephonenumber of the contact person assigned tohandle the complaint.
39
C. Dental Health Services will collect and reviewall relevant information from the complainantand participating dentists involved, and thecomplainant is invited to present his or herissues in person. If the Dental Director feels aclinical examination is required, thecomplainant may be referred to anotherparticipating dentist or specialist for a secondopinion. When all information has beencollected and reviewed, a decision is made bythe appropriate Dental Health Servicesadministrator.
D. Every effort will be made by Dental HealthServices to provide a disposition of thecomplaint within 14 days of its receipt.However, Dental Health Services may notifythe complainant that an extension is necessaryto complete the review. This extension will notexceed 30 days from the receipt of thecomplaint without the written consent of thecomplainant.
E. When the complaint involves an adversedecision by Dental Health Services and a delayin its review would jeopardize thecomplainant’s life or materially jeopardize thecomplainant’s health, Dental Health Serviceswill expedite and process a complaint in nolater than 72 hours after receipt of thecomplaint. If the treating participating dentistdetermines that a delay in review wouldjeopardize the complainant’s life or materiallyjeopardize the person’s health, Dental HealthServices shall presume the need for expeditiousreview.
F. Once a decision is made, Dental Health
40
Services will promptly notify the complainantin writing of the disposition of his or hercomplaint. The notification will include theactual reason(s) for the determination, theinstructions for obtaining an appeal of thedecision, a written statement of the clinicalrationale for the decision, and instructions forobtaining the clinical review criteria used tomake the determination.
G. If the complainant is not satisfied with thedisposition of his or her complaint, thecomplainant may appeal the decision byrequesting non-binding mediation. If DentalHealth Services is not able to provide adisposition to a complaint within 30 days of itsreceipt by Dental Health Services or within thetime frame agreed to in writing by thecomplainant, the complainant may proceed asif the complaint had been rejected and requestnonbinding mediation.
COBRAIf you qualify for continuing coverage throughCOBRA (Consolidated Omnibus BudgetReconciliation Act), Dental Health Services willgladly provide benefits through your employer.Please contact your benefits administrator.
Labor disputesIn the event of suspension or termination ofemployee compensation due to a strike, lockout, orother labor dispute, a subscriber may continueuninterrupted coverage for the family unit bypaying to the Group the monthly premium chargethat the Group would otherwise have paid Dental
41
Health Services. Coverage may be continued onthis self-payment basis for up to six months.
Supplemental coverage andservicesIf you have additional coverage for TMJ disorderor orthodontia through your group agreement,your Schedule of Covered Services andCopayments will indicate your coverage for eitheror both of these additional benefits.
Privacy noticeDental Health Services is committed to protectingyour privacy and the confidentiality of your dental,medical, and personal health information that wemay obtain or to which we have access. We do notsell our client information. Your personalinformation will not be disclosed to non-affiliatedthird parties unless permitted or required by law, orauthorized in writing by you.
Throughout this Notice, unless otherwise stated,your medical and dental health information refersto only health information created or received byDental Health Services and identified in thisNotice as Protected Health Information (PHI).Please note that your dentist maintains your dentalrecords, including payments and charges. DentalHealth Services will have a record of this portion ofyour PHI only in special or exceptional cases.
Dental Health Services’ privacy policies describewho has access to your PHI, how it will be used,when your PHI may be disclosed, safeguards toprotect the privacy of your PHI and the trainingwe provide our employees regarding maintainingand protecting your privacy.
42
Under what circumstances must Dental HealthServices share my PHI?
Dental Health Services is required to disclose yourPHI to you, and to the U.S. Department of Healthand Human Services (HHS) when it is conductingan investigation of compliance with legalrequirements. Dental Health Services is alsorequired to disclose your PHI, subject to certainrequirements and limitations, if the disclosure iscompelled by (any of the following):
A. A court order.
B. A board, commission or administrative agency,pursuant to its lawful authority.
C. A party to a proceeding pursuant to asubpoena, subpoena duces tecum, or otherauthorized discovery in a proceeding before acourt or an administrative agency.
D. An arbitrator or panel of arbitrators in a lawfully-requested arbitration.
E. A search warrant.
F. A coroner in the course of an investigation.
G. By other law.
When may Dental Health Services disclose myPHI without my authorization?
Dental Health Services is permitted by law to useand disclose your PHI, without your authorization,for purposes of payment and health careadministration.
A. Payment purposes include activities to collect
43
premiums and to determine or maintaincoverage. These include using PHI in billingand collecting premiums, and related dataprocessing including how your dentist obtainspre-authorization for certain dental services.For example, Dental Health Servicesperiodically conducts quality assuranceinspections of your dentist’s office and duringsuch visits may review your dental records aspart of this audit.
B. Health Care Administration means basicactivities essential to Dental Health Services’function as a licensed limited healthcare servicecontractor, and includes reviewing thequalifications and competence of your dentist;evaluating the quality of his/her services;providing subscriber services and informationincluding answering enrollee inquiries butwithout disclosing PHI. Dental HealthServices may, for example, review your dentist’srecords to determine if the copayments beingcharged by the office comply with the contractunder which you receive dental coverage.
C. In addition, Dental Health Services ispermitted to use and disclose your PHI,without your authorization, in a variety ofother situations, each subject to limitationsimposed by law. These situations include, butare not limited to, the following uses anddisclosures:
1. Public health activities.
2. Concerning victims of abuse, neglect ordomestic violence.
3. Health oversight agency.
44
4. Judicial and administrative proceedingsincluding the defense by Dental HealthServices of a legal action or proceedingbrought by you.
5. Law enforcement purposes, subject tosubpoena of law.
6. Workers’ Compensation purposes.
7. Parents or guardians of a minor.
8. Persons or entities who perform services onbehalf of Dental Health Services and fromwhom Dental Health Services has receivedcontractual assurances to protect theprivacy of your PHI.
Is Dental Health Services ever required to get mypermission before sharing my PHI?
Uses and disclosures of PHI other than thoserequired or permitted by law will be made byDental Health Services only with your writtenauthorization. You may revoke any authorizationgiven to Dental Health Services at any time bywritten notice of revocation to Dental HealthServices, except to the extent that Dental HealthServices has relied on the authorization beforereceiving your written revocation. Uses anddisclosures beyond those required or permitted bylaw, or authorized by you, are prohibited.
Does my employer have the right to access myPHI?
If you are an enrollee under a plan sponsored byyour employer, Dental Health Services will notdisclose PHI to your employer except under thefollowing conditions:
45
A. You sign an authorization for release of yourmedical/dental information.
B. Health care services were provided with specificprior written request and expense of theemployer, and are relevant in a grievance,arbitration or lawsuit, or describe limitationsentitling you to leave from work or limit workperformance.
Any such disclosure is subject to Dental HealthServices' minimum necessary disclosure policy.
What is Dental Health Services' minimumnecessary disclosure policy?
Dental Health Services uses reasonable efforts tolimit the use and disclosure of your PHI to theminimum necessary to accomplish the purpose ofthe use or disclosure. This restriction includesrequests for PHI from another entity, and torequests made by Dental Health Services to otherentities. This restriction does not apply to requestsby:
A. Your dentist for treatment purposes.
B. You.
C. Disclosures covered by an authorization youprovided to another entity.
What are my rights regarding the privacy of myPHI?
Your rights respecting your PHI, and how you mayexercise these rights are summarized here.
A. You may request Dental Health Services to
46
restrict uses and disclosures of your PHI in theperformance of its payment or health careoperations. However, a written request isrequired. Your health is the top priority andDental Health Services is not required to agreeto your requested restriction. If Dental HealthServices agrees to your requested restriction,the restriction will not apply in situationsinvolving emergency treatment by a health careprovider.
B. Dental Health Services will comply with yourreasonable request that you wish to receivecommunications of your PHI by alternativemeans or at alternative locations. Suchrequests must be made to Dental HealthServices in writing.
C. You have a right, subject to certain limitations,to inspect and copy your PHI. Your requestmust be made in writing. Dental HealthServices will act on such request within 30 daysof receipt of request.
D. You have the right to amend your PHI. Therequest to amend must be made in writing, andmust contain the reason you wish to amendyour PHI. Dental Health Services has theright to deny such requests under certainconditions provided by law. Dental HealthServices will respond to your request within 60days of receipt of the request and, in certaincircumstances may extend this period for up toan additional 30 days.
E. You have the right to receive an accounting ofdisclosures of your PHI made by DentalHealth Services for up to 6 years preceding
47
such request subject to certain exceptionsprovided by law. These exceptions include, butare not limited to:
1. Disclosures made for payment orhealthcare operations purposes.
2. Disclosures occurring prior to February 26,2002.
Your request must be made in writing. DentalHealth Services will provide the accountingwithin 60 days of your request but may extendthe period for up to an additional 30 days.The first accounting requested during any 12-month period will be made without charge.There is a $25 charge for each additionalaccounting requested during such 12-monthperiod. You may withdraw or modify anyadditional requests within 30 days of the initialrequest in order to avoid or reduce the fee.
F. You have the right to receive a copy of thisNotice, and any amended Notice, uponwritten or telephone request made to DentalHealth Services.
G. All written requests for the purposes describedin this section, and all other writtencommunications to Dental Health Servicesdesired or required by this Notice, must bedelivered to:
Dental Health Services936 N 34th St., Ste. 208Seattle, WA 98103
by any of the following means:
1. Personal delivery.
48
2. E-mail delivery [email protected].
3. First class or certified U.S. Mail.
4. Overnight or courier delivery, chargesprepaid.
What duties does Dental Health Services agreeto perform?
A. Dental Health Services will maintain theprivacy of your PHI and provide you withnotice of its legal duties and privacy practiceswith respect to PHI.
B. Dental Health Services will abide by the termsof this Notice and any revised Notice, duringthe period that it is in effect.
C. Dental Health Services reserves the right tochange the terms of this Notice or any revisedNotice. Any new terms shall be effective for allPHI that it maintains including PHI created orreceived by Dental Health Services prior to theeffective date of the new terms.
Each time Dental Health Services makes a revisedNotice, it shall 1) post it on its website, and 2)distribute a written copy personally by first classU.S. mail to each of its subscribers who areenrolled with Dental Health Services during theperiod that such revised Notice remains effective.
What if I am dissatisfied with Dental HealthServices' compliance with HIPAA (HealthInsurance Portability and Accountability Act)privacy regulations?
49
You have the right to express your dissatisfaction orobjection to:
Dental Health ServicesAttn: Privacy Officer936 N 34th St., Ste. 208Seattle, WA 98103
Your written dissatisfaction must describe the actsor omissions you believe to be in violation of theprovisions of this Notice or applicable laws. Yourwritten objection to HHS or Dental HealthServices must be filed within 180 days of when youknew or should have known of the act or omission.You will not be penalized or retaliated against forcommunicating your dissatisfaction.
Who should I contact if I have any questionsregarding my privacy rights with Dental HealthServices?
You may obtain further information regarding yourPHI privacy rights by contacting your MemberService Specialist at 206.788.3444 or877.495.4455 during regular office hours or atwww.smartsmile.com/cityofseattle.
GlossaryBenefits mean services performed by a dentist thatare covered under this contract and any paymentsmade by Dental Health Services for an enrollee forservices or supplies covered under this contract.
Calendar year means January 1 throughDecember 31.
Child includes a natural child, an adopted child, achild for whom the subscriber assumes a legal
50
obligation for total or partial support inanticipation of adoption, a stepchild and a childfor whom the subscriber or the subscriber’s spouseis the legal guardian.
Copay and copayments means the dollar amountthat will be the patient’s responsibility to pay forcertain services received under the Contract.Copayments for each service covered under yourplan are listed in your Schedule of CoveredServices and Copayments.
Dependent means a person listed on thesubscriber’s enrollment application as a dependentof the subscriber, who is eligible for dependentcoverage under the terms of the contract, andwhose enrollment application for coverage hasbeen accepted by Dental Health Services, and forwhom the applicable premium for coverage hasbeen paid.
Dental emergency means the emergent and acuteonset of a symptom or symptoms, including severepain, that would lead a prudent layperson, actingreasonably, to believe that a dental condition existsthat requires immediate care by a licensed dentistto relieve pain, swelling or bleeding only. This doesnot include routine, extensive or postponabletreatment.
Enrollee or member means a person who isentitled to receive dental services under thisagreement. The term includes both subscribers andthose family members (and dependents) enrolledby subscribers for whom a premium has been paid.
Exclusion means treatment or coverage notincluded as a benefit.
51
Family unit means a unit composed of asubscriber and each person whose eligibility forbenefits is based upon such person's relationshipwith, or dependency upon such subscriber.
Group means the employer (including approvedaffiliates and subsidiaries) that has entered into anagreement with Dental Health Services for dentalcare coverage.
Group representative means the employer or aperson who has been designated by the group toact as its agent to remit the premium to DentalHealth Services and to give and receive any noticesunder this contract.
Licensed dentist means a licensed doctor of dentalsurgery (D.D.S) or a licensed doctor of medicaldentistry (D.M.D).
Limitation means a provision other than anexclusion which restricts coverage available underthe plan.
Optional treatment means any treatment otherthan covered services which, in the opinion of theattending dentist, is not necessary for the patient’sdental health. If an enrollee chooses an optionaltreatment, the enrollee is responsible to pay thecost on a fee-for-service basis.
52
Participating dentist means a licensed dentalprofessional who has entered into a writtenagreement with Dental Health Services to providedental care services to subscribers and theirdependents covered under the plan. The contractincludes provisions in which the participatingdentist agrees that the subscriber shall be heldliable only for their copayment (and related laband metal costs) and no additional amount.
Participating specialist means a participatinglicensed dentist who has completed additionaltraining in one or more areas of dental treatmentand who provides services to an enrollee uponreferral by a participating dentist.
Plan means dental benefits or coverages availableto the subscriber and any eligible dependents inexchange for the payment of membership dues(premium).
Premium means the total money to be paid toDental Health Services each month as specified inArticle 6 of this contract, as consideration for thebenefits offered by this contract.
Subscriber means a person whose employment, orother relationship to or membership in group is thebasis for eligibility for participation in the plan andwhose application for coverage has been acceptedby Dental Health Services, and for whomapplicable premium has been paid.
Temporomandibular joint syndrome means adisorder that has one or more of the followingcharacteristics: pain in the musculature associatedwith the temporomandibular joint, internalderangements of the temporomandibular joint,arthritic problems with the temporomandibularjoint, or an abnormal range of motion orlimitation of the temporomandibular joint.
53

936 N 34th St, Suite 208 • Seattle, WA 98103877.495.4455 • www.smartsmile.com/cityofseattle
© 2010 Dental Health Services AN EMPLOYEE-OWNED COMPANY












![LOS ANGELES PREPAID HEALTH PLAN COMBINED … · Access Dental Plan Los Angeles Prepaid Health Plan [4] INTRODUCTION Using this Booklet This booklet is the Combined Evidence of Coverage](https://img.pdfslide.us/doc/110x75/5bcb7f6809d3f24a0c8b97d2/los-angeles-prepaid-health-plan-combined-access-dental-plan-los-angeles-prepaid.jpg)





![[Certificate] [Evidence] of Coverage](https://img.pdfslide.us/doc/110x75/62e47c982c4738519865f2f4/certificate-evidence-of-coverage.jpg)










