Embed Size (px)
Citation preview
Combined Anatomic and Perfusion Imaging of the Heart
Bilal Ali & Edward Hsiao & Marcelo F. Di Carli
Published online: 7 January 2010# Springer Science+Business Media, LLC 2010
Abstract Recent technological advances provided clinicianswith multiple options for diagnosing and prognosticatingpatients with coronary artery disease (CAD). Myocardialperfusion imaging with single photon emission computedtomography and positron emission tomography is a powerfultool for assessing physiologically significant coronary athero-sclerosis, but is unable to detect subclinical atherosclerosis.Coronary computed tomographic angiography permits rapidnoninvasive assessment of the coronaries and demonstrates animpressive negative predictive value in the clinical literature.Nevertheless, the positive predictive value of computedtomographic angiography for clinically significant CAD issuboptimal. The combination of both of these techniquesprovides an opportunity to the clinician to assess for subclinicalatherosclerosis (with important implications for therapy in low-intermediate risk patients) and functionally significant lesionsin patients with extensive CAD. However, the application ofthis technology has to be implemented on a case-by-case basisto avoid unnecessary radiation exposure and cost.
Keywords Cardiac PET. Cardiac CTA . Perfusion imaging .
Subclinical atherosclerosis
Clinical Trial AcronymsACCURACY Assessment by Coronary Computed
Tomographic Angiography of IndividualsUndergoing Invasive CoronaryAngiography
CORE 64 Coronary Artery Evaluation Using64-Row Multidetector ComputedTomography Angiography
NHANES National Health and Nutrition SurveysSCCT Society of Cardiovascular Computed
Tomography
Introduction
Coronary artery disease (CAD) is the leading cause ofmortality in the developed world. Data from the NHANESsuggest that 13.7 million persons in the United States haveCAD [1]. Because this data relies on self-reported myocar-dial infarctions and angina from health interviews, itprobably underestimates the actual prevalence of CAD.Nevertheless, this represents an extensive disease burdenwith profound economic and public health implications.
The pathogenesis of CAD has been studied extensively,and has been found to involve a progression from fattystreaks in the intima of the coronary arteries to fibrous andthen fatty plaques, which may then calcify [2, 3]. The riskfactors for CAD are well recognized at this time and therate of plaque progression appears to depend on the numberof risk factors, as well as the underlying severity of theseconditions. Noninvasive imaging can provide powerful andaccurate assessments of the burden of this disease as well asthe biologic activity and functional significance of anatomicdisease.
In recent years, rapid developments occurred in nonin-vasive anatomic and physiologic imaging techniques. Dueto the unique strength and limitations of each modality— aswell as the overlap of information acquired—it remainschallenging to clearly define the clinical roles of thesetechniques in diagnosing, prognosticating, and guidingclinical management of CAD. Among various noninvasivecardiac imaging modalities, nuclear myocardial perfusionimaging (MPI) is the most widely used in clinical practicefor diagnosing and risk stratifying these patients.
B. Ali : E. Hsiao :M. F. Di Carli (*)Division of Nuclear Medicine and Molecular Imaging,Department of Radiology, Brigham and Women’s Hospital,ASB L1-037C, 75 Francis Street,Boston, MA 02115, USAe-mail: [email protected]
Curr Cardiol Rep (2010) 12:90–97DOI 10.1007/s11886-009-0081-1

In this context, the integration of nuclear medicine cameraswith multidetector CT scanners (eg, positron emissiontomography [PET]-CT and single photon emission computedtomography [SPECT]-CT) provides an opportunity to dem-onstrate cardiac and vascular anatomic abnormalities, andtheir physiologic consequences in a single setting. This articlereviews potential clinical applications of combined anatomicand perfusion imaging in cardiovascular disease.
Functional Imaging of the Heart
MPI, alongwith stress echocardiography, has been the preferredmethod of functional evaluation of patients for CAD over thepast few decades. Stress MPI has been used for diagnosingobstructive CAD, assessing the magnitude of myocardium atrisk, determining myocardial viability, and following uppatients with stable CAD. Advantages of stress MPI includewidespread availability and familiarity with the technology, aswell as an extensive body of literature supporting its use.
The published literature with SPECT indicates that theaverage sensitivity for detecting greater than 50% stenosisis 87%, with the average specificity of 73% [4]. Limitationsof SPECT include suboptimal tracer kinetics that limitsensitivity and susceptibility to attenuation artifacts, mostcommonly due to body habitus. In addition, although it is ahighly sensitive approach to diagnosing CAD, SPECTmyocardial perfusion is limited in its delineation of theextent of underlying CAD because only the coronaryterritories supplied by the relatively more severe stenosisare identified [5, 6], and left ventricular function is notmeasured at peak stress [7••].
MPI by cardiac PET is gaining widespread acceptance as analternative to cardiac SPECT. Specific advantages of cardiacPET compared with SPECT include more robust attenuationcorrection algorithms and thus less diagnostic uncertainty fromartifacts. This leads to an improvement in sensitivity andspecificity for detection of greater than 50% stenosis [7••–10•].
In addition, cardiac PET offers specific advantages inpatients with multivessel disease. The technique allows thedetermination of left ventricular ejection fraction (LVEF) atpeak stress, which has been demonstrated to be predictiveof the extent and severity of CAD [7••, 9, 11•]. Previousstudies suggested that in healthy subjects, LVEF increasesduring vasodilator stress PET imaging. In the presence ofCAD, however, changes in LVEF are inversely related tothe degree of observed perfusion abnormalities. In patientswith multivessel disease or left main CAD, LVEF duringstress has been reported to decrease even in the absence ofapparent perfusion abnormalities. The negative predictivevalue of an increase in LVEF (from baseline to peak stress)of greater than 5% to exclude the presence of three-vesselCAD or left main CAD is 97% [7••].
Another advantage of cardiac PET is the ability tomeasure coronary flow reserve by measurements ofmyocardial blood flow (in mL/min/g) of myocardium[12]. Conceptually, this should permit the detection ofmultivessel disease in the setting of “balanced” ischemia,which may potentially improve the identification of high-risk patients.
Several studies in the clinical literature demonstrate thatmyocardial blood flow and coronary flow reserve by PETare inversely related to stenosis severity in experimentaland clinical settings [5, 13]. However, there are noprospective clinical data at this time to confirm its use inthe diagnostic and/or prognostic work-up in patients withCAD. Another advantage of cardiac PET relates to theradiation dose, which with PET is generally lower thanSPECT. This is due to the short half-lives of the perfusionagents (Rb-82, N-13 ammonia, and O-15 water) [14]. Thisis particularly relevant to dual-modality imaging withcomputed tomographic angiography (CTA).
Despite the extensive clinical experience with MPI withSPECT and PET, the technique has some important limi-tations. The most important relates to the fact that the presenceor absence of CAD is not ascertained; rather, this techniquepermits the detection of lesions that are of physiologicsignificance [15, 16••]. This is potentially important espe-cially in patient subgroups with intermediate-high clinicalrisk in whom there may be extensive subclinical CAD, andaggressive medical therapy with cholesterol-limiting agentsmay be indicated.
Anatomic Imaging of the Heart: Cardiac CT
Recent advances in hardware and software, as well as thedevelopment of specific imaging protocols, enabled accu-rate visualization of the coronary arteries by cardiac CT.Three large clinical trials of 64-detector row cardiac CTA(ACCURACY, CORE 64, and the European study con-ducted by Meijboom et al. [18]) demonstrated averagesensitivity and specificity for detecting greater than 50%CAD to be 83% and 91% based on per-vessel analysis,respectively [17–19]. One of the main advantages ofcardiac CTA is the excellent negative predictive value,with an average of 96% (89% to 99%).
Although the negative predictive value of CAD makes itan excellent tool for ruling out CAD, accurate estimation ofcoronary artery stenosis in patients with CAD is problem-atic for several reasons. The first is the presence of calcifiedplaque, which may lead to partial volume and/or bloomingartifacts. These artifacts can result in under- and overesti-mation of plaque severity by visual analysis. In fact,according to the guidelines of the SCCT, proceeding withCTA in the presence of extensive calcification is “contro-
Curr Cardiol Rep (2010) 12:90–97 91
versial” [20]. Some centers do not proceed with CTA in thepresence of a calcium score greater than 600 [19].
The same issues lead to problems with imaging in thepresence of coronary artery stents. Studies evaluatingcoronary stents in vessels other than left main arteries
suggest an acceptable negative predictive value of 98%,but the positive predictive value is only about 50%. Themain determinant of stent visualization is vessel and stentdiameter, with stents less than 3 mm being particularlydifficult to evaluate.
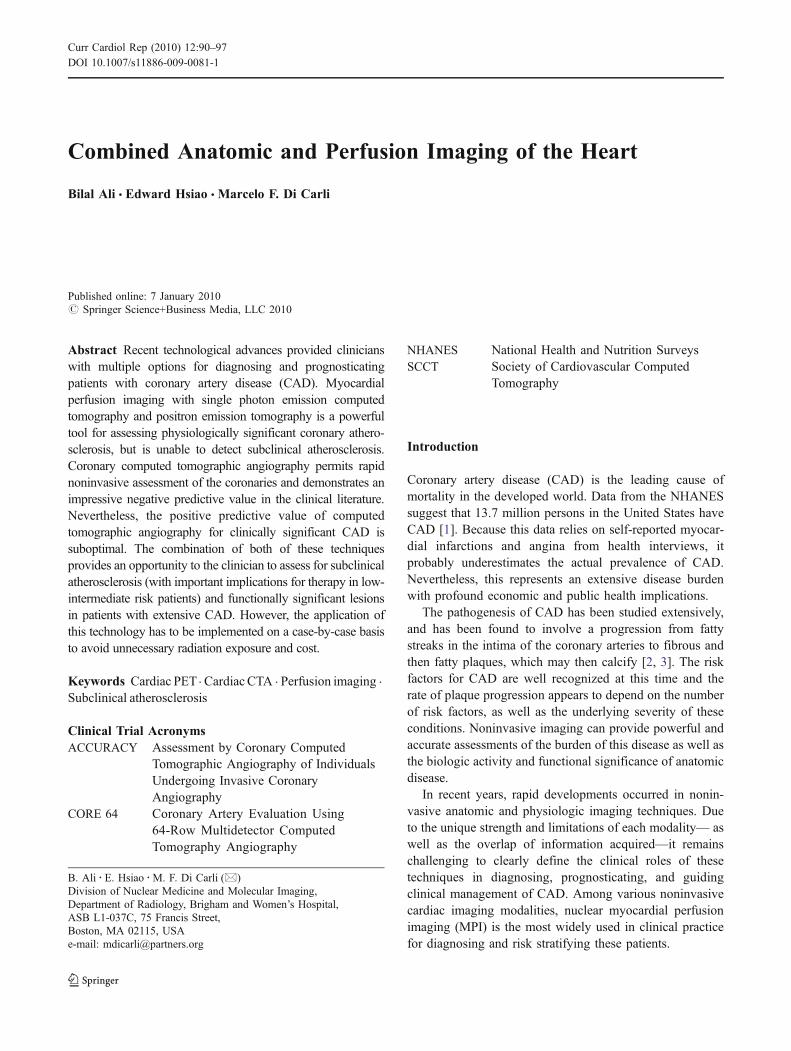
Fig. 1 Rest (Rst) and stress (Str) Rb-82 positron emission tomography(PET)/CT in a 65-year-old man with chest discomfort and several riskfactors for coronary artery disease. a The PET images demonstrate asmall-sized defect of moderate intensity involving the mid and basalinferior wall segments. However, there is intense adjacent splanchnictracer uptake that may affect interpretation. b A cardiac CTangiography obtained immediately afterward revealed severe athero-
sclerosis of the right coronary artery (RCA) with complete occlusionafter the proximal segment. c A hybrid display in which the severestenosis in the RCA is seen to correspond with an area of basal andmid inferior wall ischemia (normal myocardium is red, ischemic areasare blue). AC—attenuation corrected images; ANT—anterior; HLA—horizontal long-axis images; INF—inferior; LAT—lateral; SA—shortaxis; SEP—septal; VLA—vertical long-axis images
92 Curr Cardiol Rep (2010) 12:90–97

Another limitation of coronary CTA is its limitedprecision of stenosis severity. Quantification of coronaryartery stenosis by CTA correlates fairly well with invasivecoronary angiography, but a large standard deviation hasbeen observed. The current literature suggests that CTAcorrelates with quantitative coronary angiography (QCA) to± 25% at best [20]. This is probably due to the artifactsmentioned previously, as well as the fact that percentdiameter stenosis is not a precise descriptor of coronaryresistance. In addition, vasomotor tone and collateral bloodflow are not assessed with this technique.
Emerging Applications of Cardiac PET/CT
Attenuation Correction
Attenuation correction is one of the main applications of CTin the setting of cardiac PET. The increased energy of thepositrons emitted during PET leads to a greater degree ofattenuation and, therefore, a greater need for accurateattenuation correction. The acquisition parameters for CT-based transmission vary with the configuration of theCT scanner and protocol. The general scan settings for CTtransmission imaging generally have 1) slow gantry rotationsspeed (1 sec/revolution), combined with a relatively highpitch (0.5-0.6); 2) nongated scan; 3) low tube current (10–20 mA); and 4) a CT acquisition obtained during tidalexpiration breathhold or shallow breathing [8].
Attenuation correction for SPECT has been demonstratedto increase diagnostic accuracy in several studies, but needsto be performed meticulously. One of the major challengeswith this technique is the potential for misregistrationartifacts due to patient, cardiac, and or respiratory motion.Misregistration artifacts may lead to erroneous reporting ofperfusion defects; therefore, proper quality control andreview of registration is critical during image interpretation.
Calcium Scoring and MPI
Measurement of coronary artery calcium (CAC) has beenadvocated as a tool for risk stratification in asymptomaticindividuals, particularly those with an intermediate-highrisk of CAD. The relationship between CAC measurementsby CT and myocardial perfusion was the subject of severalrecent studies [21–23]. In general, a higher CAC scoreappears to be more likely to be associated with the presenceof ischemia on MPI. The ability of CAC scoring to detectatherosclerosis could potentially be helpful for detectingCAD in the setting of balanced ischemia. A recent studyreported that a CAC score greater than 709 increased thesensitivity of SPECT MPI for detecting obstructive CADdespite normal perfusion [24].
However, there are several caveats to the use of CACwith perfusion imaging for determining the severity ofCAD. CAC provides no information about stenosis sever-ity. In addition, absent calcium or low CAC scores aregenerally unreliable for excluding underlying obstructiveCAD in symptomatic individuals, especially in youngerpatients and women. This is probably because CAC scoringmisses noncalcified plaque, which is often the culprit inacute coronary syndromes. A recent publication by Rosenet al. [25] demonstrated that in a subset of 175 patients whohad CAC scoring and then coronary angiography for chestpain, 4% had significant coronary obstructive diseasedespite having a CAC score of 0 at baseline. They alsofound that assessing coronary calcium on a per-vessel levelwas less predictive of stenoses than the per-patient analysis.
Regarding prognosis, CAC scoring potentially provides anopportunity for early aggressive pharmacotherapy if subclin-ical atherosclerosis is identified in the absence of anyperfusion abnormalities. In a study of 695 patients undergoingstress PET imaging and CAC scoring in the same clinicalsetting, risk-adjusted analysis demonstrated that for anydegree of perfusion abnormality there was a stepwise increasein adverse events with increasing CAC scores [22•]. Thisfinding was observed in patients with and without evidence ofischemia on PET MPI. The annualized event rate in patientswith normal PET MPI and no CAC was substantially lowerthan among those with ischemia and a CAC greater than1,000, demonstrating that the presence of subclinical athero-sclerosis itself is associated with a worse overall prognosis.
Combined Coronary CTA/Perfusion Imaging
Technical advances in CT scanner technology now permit theperformance of combined PET/CTA in the same clinicalsetting. Protocols for combined cardiac PET/CTA generallyinvolve the performance of PET before CTA. This approachavoids the potential interference of intravenous β blockersused for heart rate control with the maximal hyperemic orheart rate responses during vasodilator and/or dobutaminestress perfusion. Several reviews in the cardiac literaturediscuss CTA protocols in detail. Factors to consider whilechoosing protocols include the mode of acquisition(retrospective vs prospective), contrast dosage, and radi-ation dose [8, 26–29]. Tube current and voltage should beadjusted on an individual basis to minimize unnecessaryradiation exposure.
The integration of myocardial perfusion offers severaltheoretical advantages. Cardiac CTA provides anatomicinformation that enables the detection of multivesseldisease, as well as subclinical atherosclerosis, both ofwhich could potentially be missed by MPI alone. Con-versely, myocardial perfusion provides functional informa-
Curr Cardiol Rep (2010) 12:90–97 93
94 Curr Cardiol Rep (2010) 12:90–97

tion that is particularly important for indeterminate lesionsthat may be identified on CTA as well as distal segment orcalcified lesions that are difficult to visualize with currentCTA technology (Figs. 1 and 2).
The dual-modality approach to diagnosing CAD hasbeen studied for PET and SPECT. Di Carli et al. [16••]examined the value of CTA to identify the presence ofischemia, as determined by stress perfusion imaging, usingintegrated rubidium PET/CT imaging. CTA was found tohave an excellent negative predictive value (> 95%); thepositive predictive value for identifying myocardial ische-mia was limited (14% to 53% depending on the degree ofCTA-detected stenosis severity). Of interest, nearly half ofsignificant angiographic stenoses (47%) occurred withoutevidence of myocardial ischemia, whereas 50% of normalPET studies were associated with some degree of athero-sclerosis identified on CTA.
Rispler et al. [30••] reported a significant improvementin specificity (63% to 95%) and positive predictive value(31% to 77%) for detecting obstructive CAD as defined byQCA in 56 patients with known or suspected CADundergoing hybrid SPECT/CTA. Although these resultshighlight some advantages of the dual-modality approach,the clinical use of this approach requires an understandingof how to use these results in clinical practice. Physiologicevidence of ischemia—determined by exercise stresstesting, myocardial perfusion, or fractional flow reserveon coronary angiography—remains superior to anatomicinformation for identifying patients more likely to benefitfrom revascularization [31]. This is reinforced by the datafrom Di Carli et al. [16••], in which the positive predictivevalue of CTA for identifying coronary stenoses producingischemia was around 50% at best.
Challenges in the Application of Dual-Modality Imaging
The appropriate use of cardiac imaging has recentlyreceived a great deal of attention in the cardiologycommunity because of concerns about costs and radiationexposure. Although conceptually attractive, there is a greatdeal of debate and controversy about the possible role of
hybrid imaging. As described previously, there is evidenceto suggest that assessing CAC scores at the time of MPIprovides incremental value for risk assessment in symp-tomatic patients without prior CAD.
In general, myocardial perfusion and CTA should beperformed in a fashion that maximizes their particularlydiagnostic advantages. For instance, in patients at low-intermediate risk for CAD with equivocal perfusion images,CTA can be performed sequentially in the same scannerwith minimal delay and provides a noninvasive method forruling out significant CAD. Conversely, in patients withhigh-risk perfusion scans and/or patients with a history ofcoronary stents/calcified vessels, the likelihood of subse-quent cardiac catheterization is high and therefore CTAwould lead to unnecessary contrast and radiation exposure.In all cases, effective communication with the patient andthe referring physician is critical to assure that theappropriate test is performed for an individual patient.
Another important issue is the radiation dose fromcombined myocardial perfusion/CTA protocols. Conven-tional spiral CTA protocols with retrospective gatingwere associated with a wide range of radiation expo-sures, ranging from 4 to 21.4 mSv [14]. In combinationwith SPECT MPI, radiation doses as high as 41.5 mSvwere reported and led to heightened concern aboutexcessive radiation dosage with this approach. However,rapid advances in scanning technology addressed theseconcerns. With newer low-dose CTA acquisition proto-cols using prospective electrocardiogram gating, theradiation dose can be reduced up to 70% with no reduc-tion in diagnostic accuracy [32]. These latest combinedPET/CTA protocols can now be performed with radiationdoses ≤ 10 mSv [33].
Conclusions and Future Directions
Myocardial perfusion and CTA are extremely powerfultools for functional and anatomic assessment of CAD.Recent technological advances in both these techniquespermit rapid acquisition of data and minimization ofpatient radiation dose. The combination of both modal-ities provides valuable information, although this needsto be assessed on an individual patient basis. Future areasfor research include the development of standard proto-cols for imaging and interpretation, studies of cost-effectiveness, and the translation of this approach toclinical outcomes.
Disclosure Dr. Marcelo Di Carli has received research grants fromGE, Siemens, Bracco, and Astellas. No other potential conflicts ofinterest relevant to this article were reported.
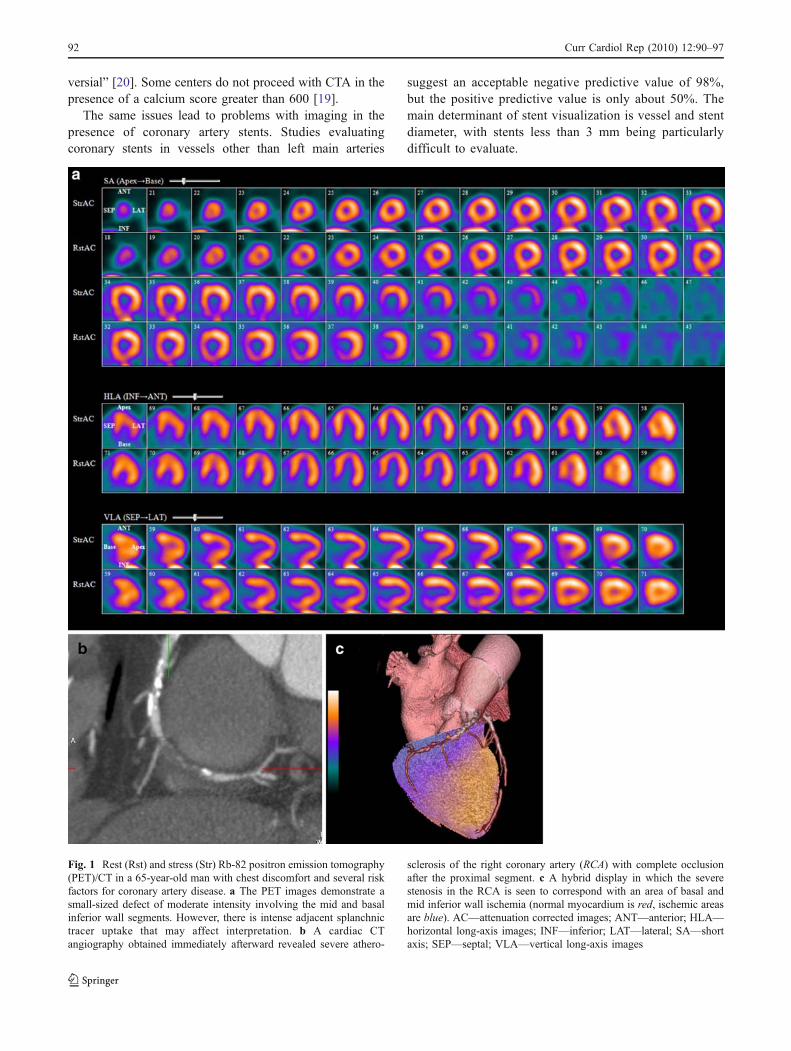
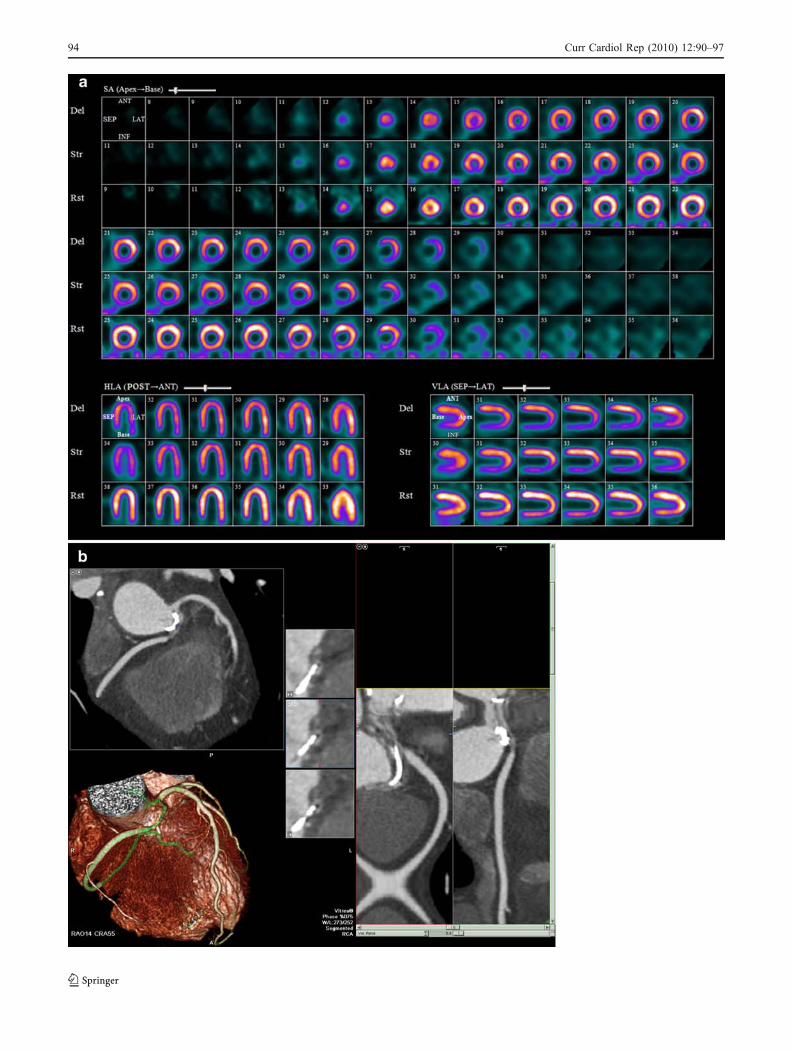
Fig. 2 Rest (upright) (Rst), stress (upright) (Str), and delayed (Del)stress (supine) Tc99m-sestamibi myocardial perfusion imagesobtained with a D-SPECT (Spectrum Dynamics, Caesarea, Israel)system in a 60-year-old patient complaining of chest discomfortseveral months after aortic valve replacement. Her angiogram beforesurgery was reported as normal. a The perfusion images demonstratea medium-sized defect of severe intensity involving the inferior wall.b Cardiac CT angiography reveals an anomalous right coronaryartery (RCA) from the left coronary cusp with severe associatedproximal stenosis. ANT—anterior; HLA—horizontal long-axisimages; INF—inferior; LAT—lateral; POST—posterior; SA—shortaxis; SEP—septal; VLA—vertical long-axis images
R
Curr Cardiol Rep (2010) 12:90–97 95

References
Papers of particular interest, published recently, have beenhighlighted as:• Of importance•• Of major importance
1. Lloyd-Jones D, Adams R, Carnethon M, et al.: Heart Disease andStroke Statistics—2009 Update: a report from the American HeartAssociation Statistics Committee and Stroke Statistics Subcommit-tee. Circulation 2009, 119:e21–e181.
2. Stary HC, Chandler AB, Dinsmore RE, et al.: A definition ofadvanced types of atherosclerotic lesions and a histologicalclassification of atherosclerosis. A report from the Committee onVascular Lesions of the Council on Arteriosclerosis, AmericanHeart Association. Circulation 1995, 92:1355–1374.
3. Kockx MM, De Meyer GR, Muhring J, et al.: Apoptosis andrelated proteins in different stages of human atheroscleroticplaques. Circulation 1998, 97:2307–2315.
4. Klocke FJ, Baird MG, Lorell BH, et al.: ACC/AHA/ASNCguidelines for the clinical use of cardiac radionuclide imaging—executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines(ACC/AHA/ASNCCommittee to Revise the 1995 Guidelines for theClinical Use of Cardiac Radionuclide Imaging). J Am Coll Cardiol2003, 42:1318–1333.
5. Uren NG, Crake T, Lefroy DC, et al.: Reduced coronaryvasodilator function in infarcted and normal myocardium aftermyocardial infarction. N Engl J Med 1994, 331:222–227.
6. Yoshinaga K, Katoh C, Noriyasu K, et al.: Reduction ofcoronary flow reserve in areas with and without ischemia onstress perfusion imaging in patients with coronary artery disease:a study using oxygen 15-labeled water PET. J Nucl Cardiol2003, 10:275–283.
7. •• Dorbala S, Vangala D, Sampson U, et al.: Value of vasodilatorleft ventricular ejection fraction reserve in evaluating themagnitude of myocardium at risk and the extent of angiographiccoronary artery disease: a 82Rb PET/CT study. J Nucl Med2007, 48:349–358. This paper discusses a study of 510 patientswith suspected CAD who underwent gated rest and vasodilatorstress Rb-82 PET/CT. LVEF reserve was the only predictor ofleft main/three-vessel disease, with an LVEF reserve of greaterthan +5% demonstrating a negative predictive value of 975 forexcluding left main/three-vessel CAD.
8. Di Carli MF, Dorbala S, Hachamovitch R: Integrated cardiac PET-CT for the diagnosis and management of CAD. J Nucl Cardiol2006, 13:139–144.
9. Lertsburapa K, Ahlberg AW, Bateman TM, et al.: Independentand incremental prognostic value of left ventricular ejectionfraction determined by stress gated rubidium 82 PET imaging inpatients with known or suspected coronary artery disease. J NuclCardiol 2008, 15:745–753.
10. • Sampson UK, Dorbala S, Limaye A, et al.: Diagnostic accuracyof rubidium-82 myocardial perfusion imaging with hybridpositron emission tomography/computed tomography in thedetection of coronary artery disease. J Am Coll Cardiol 2007,49:1052–1058. This paper discuses a study of 64 consecutivepatients with suspected CAD undergoing rest-stress Rb-82 cardiacPET/CT and coronary angiography within 7 days. The sensitivityfor detecting CAD in patients with single and multivessel diseasewas 92% and 95%, respectively.
11. • Dorbala S, Hachamovitch R, Curillova Z, et al.: Incrementalprognostic value of gated Rb-82 positron emission tomographymyocardial perfusion imaging over clinical variables and rest
LVEF. JACC Cardiovasc Imaging 2009, 2:846–854. This paperdiscusses a study examining the incremental value of gated Rb-82PET MPI over clinical variables for predicting survival and futurecardiac events. Rb-82 PET MPI provided significant incrementalprognostic value to historical/clinical variables and rest LVEF topredict survival free of cardiac events and all-cause death.
12. Anagnostopoulos C, Almonacid A, El Fakhri G, et al.: Quantita-tive relationship between coronary vasodilator reserve assessed by82Rb PET imaging and coronary artery stenosis severity. Eur JNucl Med Mol Imaging 2008, 35:1593–1601.
13. Di Carli M, Czernin J, Hoh CK, et al.: Relation among stenosisseverity, myocardial blood flow, and flow reserve in patients withcoronary artery disease. Circulation 1995, 91:1944–1951.
14. Einstein AJ, Moser KW, Thompson RC, et al.: Radiation dose topatients from cardiac diagnostic imaging. Circulation 2007,116:1290–1305.
15. Schuijf JD, Wijns W, Jukema JW, et al.: Relationship betweennoninvasive coronary angiography with multi-slice computedtomography and myocardial perfusion imaging. J Am Coll Cardiol2006, 48:2508–2514.
16. •• Di Carli MF, Dorbala S, Curillova Z, et al.: Relationshipbetween CT coronary angiography and stress perfusion imaging inpatients with suspected ischemic heart disease assessed byintegrated PET-CT imaging. J Nucl Cardiol 2007, 14:799–809.The authors studied 110 consecutive patients with suspected CADundergoing stress Rb-82 PET MPI and CTA in the same setting.CTA was found to have an excellent negative predictive value fordiagnosis of CAD (> 95%), but had poor predictive value foridentifying myocardial ischemia. A normal PET was a poordiscriminator of patients with subclinical atherosclerosis, suggest-ing complementary roles for these two modalities.
17. Budoff M, Dowe D, Jollis J, et al.: Diagnostic performance of 64–multidetector row coronary computed tomographic angiography forevaluation of coronary artery stenosis in individuals without knowncoronary artery disease: results from the prospective multicenterACCURACY (Assessment by Coronary Computed TomographicAngiography of Individuals Undergoing Invasive Coronary Angiog-raphy) trial. J Am Coll Cardiol 2008, 52:1724–1732.
18. Meijboom WB, Meijs MFL, Schuijf JD, et al.: Diagnosticaccuracy of 64-slice computed tomography coronary angiography:a prospective, multicenter, multivendor study. J Am Coll Cardiol2008, 52:2135–2144.
19. Miller JM, Rochitte CE, Dewey M, et al.: Diagnostic performanceof coronary angiography by 64-row CT. N Engl J Med 2008,359:2324–2336.
20. Raff GL, Abidov A, Achenbach S, et al.: SCCT guidelines for theinterpretation and reporting of coronary computed tomographicangiography. J Cardiovasc Comput Tomogr 2009, 3:122–136.
21. Haramati LB, Levsky JM, Jain VR, et al.: CT angiography forevaluation of coronary artery disease in inner-city outpatients: aninitial prospective comparison with stress myocardial perfusionimaging. Int J Cardiovasc Imaging 2009, 25:303–313.
22. • Schenker MP, Dorbala S, Hong ECT, et al.: Interrelation ofcoronary calcification, myocardial ischemia, and outcomes inpatients with intermediate likelihood of coronary artery disease: acombined positron emission tomography/computed tomographystudy. Circulation 2008, 117:1693–1700. This paper discusses astudy of 695 intermediate-risk patients undergoing combined Rb-82 PET MPI and CAC scoring. There was an increase in eventrates (death and myocardial infarction) with increasing CACscores in patients with and without ischemia on PET MPI.
23. Scholte AJ, Schuijf JD, Kharagjitsingh AV, et al.: Differentmanifestations of coronary artery disease by stress SPECTmyocardial perfusion imaging, coronary calcium scoring, andmultislice CT coronary angiography in asymptomatic patientswith type 2 diabetes mellitus. J Nucl Cardiol 2008, 15:503–509.
96 Curr Cardiol Rep (2010) 12:90–97

24. Schepis T, Gaemperli O, Koepfli P, et al.: Added value ofcoronary artery calcium score as an adjunct to gated SPECT forthe evaluation of coronary artery disease in an intermediate-riskpopulation. J Nucl Med 2007, 48:1424–1430.
25. Rosen BD, Fernandes V, McClelland RL, et al.: Relationship betweenbaseline coronary calcium score and demonstration of coronaryartery stenoses during follow-up MESA (Multi-Ethnic Study ofAtherosclerosis). JACC Cardiovasc Imaging 2009, 2:1175–1183.
26. Di Carli MF: Hybrid imaging: integration of nuclear imaging andcardiac CT. Cardiol Clin 2009, 27:257–263.
27. Kaufmann PA: Cardiac hybrid imaging: state-of-the-art. Ann NuclMed 2009, 23:325–331.
28. Kaufmann PA, Di Carli MF: Hybrid SPECT/CT and PET/CTimaging: the next step in noninvasive cardiac imaging. SeminNucl Med 2009, 39:341–347.
29. Knuuti J: Integrated positron emission tomography/computed tomog-raphy (PET/CT) in coronary disease. Heart 2009, 95:1457–1463.
30. •• Rispler S, Keidar Z, Ghersin E, et al.: Integrated single-photonemission computed tomography and computed tomography
coronary angiography for the assessment of hemodynamicallysignificant coronary artery lesions. J Am Coll Cardiol 2007,49:1059–1067. This paper discusses a study of 56 patients withangina who underwent single-session SPECT MPI and coronaryCTA with a hybrid system and coronary angiography within4 weeks. Hybrid SPECT/coronary CTA imaging resulted inimproved specificity and positive predictive value to detecthemodynamically significant lesions in patients with chest pain.
31. Shaw LJ, Berman DS, Maron DJ, et al.: Optimal medical therapywith or without percutaneous coronary intervention to reduceischemic burden: results from the Clinical Outcomes UtilizingRevascularization and Aggressive Drug Evaluation (COURAGE)trial nuclear substudy. Circulation 2008, 117:1283–1291.
32. Javadi M, Mahesh M, McBride G, et al.: Lowering radiation dosefor integrated assessment of coronary morphology and physiolo-gy: first experience with step-and-shoot CT angiography in arubidium 82 PET-CT protocol. J Nucl Cardiol 2008, 15:783–790.
33. Knuuti J: Cardiac hybrid imaging with low radiation dose. J NuclCardiol 2008, 15:743–744.
Curr Cardiol Rep (2010) 12:90–97 97





























