Embed Size (px)
Citation preview
1. Introduction
2. Antihypertensive combination
therapy
3. Olmesartan medoxomil plus
hydrochlorothiazide
4. Conclusions
5. Expert opinion
Drug Evaluation
Combination therapy forhypertension: focus on high-doseolmesartan medoxomil (40 mg)plus hydrochlorothiazideLars Christian Rump† & Lorenz SellinHeinrich-Heine-University Dusseldorf, Department of Internal Medicine/Nephrology,
Dusseldorf, Germany
Importance of the field: Cardiovascular disease is a major cause of premature
death and disability worldwide, and effective blood pressure (BP) control is
crucial for the reduction of cardiovascular risk in patients with hypertension.
Despite this, many will fail to attain recommended BP goals. A reappraisal
of European guidelines led to revised recommendations for BP reduction to
values within the SBP/DBP range of 130 -- 139/80 -- 85 mmHg in all patients
with hypertension, including higher-risk groups such as those with diabetes.
Areas covered in this review: The majority of hypertensive patients will
require the enhanced blood-pressure-lowering effects of at least two anti-
hypertensive drugs with complementary mechanisms of action to achieve
these goals.
What the reader will gain: The angiotensin II receptor blocker (ARB)
olmesartan medoxomil and the thiazide diuretic hydrochlorothiazide (HCTZ)
provide greater antihypertensive efficacy when used in combination than as
monotherapy with either component, with a similar tolerability profile. In
addition, there is evidence that higher doses of olmesartan may prolong the
antihypertensive effect of this ARB, and a number of US ‘treat-to-target’
and European add-on clinical trials have been conducted to assess the efficacy
and safety of high-dose olmesartan plus HCTZ in a wide range of patients with
mild-to-severe hypertension.
Take home message: Combination therapy with olmesartan, including the
high 40-mg dose, plus HCTZ is an effective and safe treatment option for con-
trolling BP in patients with mild-to-severe hypertension, particularly those
who fail to achieve recommended BP goals with monotherapy.
Keywords: angiotensin II type 1 receptor blocker, combination therapy, hydrochlorothiazide,
hypertension, olmesartan medoxomil
Expert Opin. Pharmacother. (2010) 11(13):2231-2242
1. Introduction
Hypertension is a global health issue that affects as many as 1 billion people world-wide [1] and is the leading cause of death in both developed and developing coun-tries [2]. Elevated blood pressure (BP) has been shown to be strongly associatedwith cardiovascular morbidity and mortality [3,4], and patients with hypertensionhave a two- to three-fold increase in the risk of both cardiovascular and renal dis-ease [4]. Hypertensive patients with chronic kidney disease have particularly highrates of cardiovascular as well as renal morbidity and mortality, and patients withnephropathy are in fact more likely to die from cardiovascular disease than renalcauses [5,6]. Therefore, it is essential that BP is effectively lowered in patients withhypertension, to minimize the risk of future cardiovascular and renal events.
10.1517/14656566.2010.510834 © 2010 Informa UK, Ltd. ISSN 1465-6566 2231All rights reserved: reproduction in whole or in part not permitted
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
echn
isch
e U
nive
rsite
it E
indh
oven
on
06/0
6/14
For
pers
onal
use
onl
y.
According to the 2007 guidelines for the management ofarterial hypertension of the European Society of Hyperten-sion (ESH) and the European Society of Cardiology (ESC),BP should be lowered to < 140/90 mmHg in all patientswith hypertension and < 130/80 mmHg in patients with dia-betes mellitus and/or those at high cardiovascular risk [7].However, a recent reappraisal of these guidelines recom-mended that the < 130/80-mmHg goal for diabetic patientsshould no longer be used because of a lack of supporting clin-ical evidence, and that treatment should be initiated in thesepatients when BP is ‡ 140/90 mmHg [8].A meta-analysis of outcome data from > 1 million patients
with hypertension, which showed that usual BP is stronglyand directly related to vascular and overall mortality, withoutany evidence of a threshold down to ‡ 115/75 mmHg,has alluded to the possible consequences of untreated orundertreated hypertension [3]. Moreover, previous studieshave shown that initiating antihypertensive therapy with asingle agent resulted in < 50% of patients achieving a BPlevel of < 140/90 mmHg [9-13], and a study in high-riskpatients with hypertension reported that ~ 90% of patientsrequired two or more antihypertensive drugs to achieve BPof < 140/90 mmHg [14]. The need for combination therapywas further demonstrated in the ADVANCE study, whichshowed that > 50% of diabetic patients with hypertensionhad uncontrolled BP (‡ 140/90 mmHg) despite the useof BP-lowering therapies at baseline in more than three-quarters of the study population [15]. This suggests that themajority of patients with hypertension will require a combi-nation of at least two antihypertensive agents to achieveoptimal BP control [7,8]. Indeed, a recent large, randomized,
controlled trial (ACCOMPLISH) that assessed the effi-cacy of an angiotensin-converting enzyme (ACE) inhibitorin combination with a calcium channel blocker (CCB) ora thiazide diuretic demonstrated that > 70% of highcardiovascular risk patients with hypertension achieved BPof < 140/90 mmHg [16].
2. Antihypertensive combination therapy
The antihypertensive efficacy of combination therapy withany two drug classes over monotherapy was demonstrated ina recent meta-analysis of 42 studies [17]. This analysis indicatesthat the combination of antihypertensive agents from differ-ent drug classes can be considered if i) they have differentand complementary mechanisms of action, ii) there is evi-dence that the antihypertensive effect of the combinationis greater than that of either combination component andiii) the combination may have a favorable tolerance profile,the complementary mechanisms of action of the componentsminimizing their individual side effects.
Indeed, the value of combining two antihypertensiveagents as a fixed-dose combination to improve efficacy, safetyand treatment compliance has been demonstrated in recentmeta-analyses [18,19]. As a result, fixed-dose combinations oftwo drugs can be administered following initial monotherapywhen addition of a second drug is required to control BP, orbe the first treatment step in patients at high cardiovascularrisk who require early BP control [7,8].
Current treatment guidelines indicate that there are anumber of possible combinations of antihypertensive drugclasses; these classes include thiazide diuretics, ACE
Box 1. Drug summary.
Drug name Olmesartan medoxomil + thiazide diuretichydrochlorothiazide (HCTZ)
Phase LaunchedLaunched indication HypertensionPharmacology description Thiazide diuretic
Angiotensin II antagonistRoute of administration Alimentary, p.o.Chemical structure
N
N
O
OO
O
O
ON
NN
N
N
NSS
O
Cl
OONO
Pivotal trial(s) [42,45-50]
Pharmaprojects -- copyright to Citeline Drug Intelligence (an Informa business). Readers are referred to Pipeline (http://informa-pipeline.citeline.com) and
Citeline (http://informa.citeline.com).
Olmesartan medoxomil plus hydrochlorothiazide
2232 Expert Opin. Pharmacother. (2010) 11(13)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
echn
isch
e U
nive
rsite
it E
indh
oven
on
06/0
6/14
For
pers
onal
use
onl
y.

inhibitors, angiotensin II type 1 (AT1) receptor blockers(ARBs), CCBs, b-blockers and a-blockers [7]. It should benoted that the well-established b-blocker--diuretic combina-tion is associated with adverse metabolic effects and increasesthe risk of new-onset diabetes mellitus in predisposed patientssuch as those with metabolic syndrome or impaired glucosetolerance [20-22]. Based on this evidence, the European guide-lines state that this combination should be avoided in thesepatients [7,8]. In addition, the recently completed ONTARGETstudy did not show an improvement in the primary compositeoutcome of cardiovascular death, myocardial infarction, strokeor heart failure due to hospitalization following treatment withan ACE inhibitor--ARB combination (telmisartan plus rami-pril) in patients at high risk of vascular events [23]. An increasein the incidence of adverse events and a worsening of majorrenal outcomes was also seen with this combination [23,24].The ACCOMPLISH trial has shown that the combination ofa renin-angiotensin system (RAS) blocker with either a CCBor a thiazide diuretic produced a high rate of BP control,although the RAS blocker plus CCB combination was asso-ciated with greater benefit with respect to cardiovascularoutcomes in hypertensive patients [16].
As previously stated, it is important to use agents withcomplementary mechanisms of action in order to optimize acombination therapy regimen [7]. For example, the additionof a thiazide diuretic such as hydrochlorothiazide (HCTZ)to an ARB enhances its BP-lowering effect by making BPmore dependent on angiotensin II [25]. Moreover, the addi-tion of ARBs may minimize the risk of metabolic side effectsassociated with thiazide diuretics, including hypokalemia,elevated serum uric acid, lipid and blood glucose levels [26-28].
2.1 Angiotensin II receptor blocker plus
hydrochlorothiazide combination therapyAngiotensin II receptor blocker are well-established anti-hypertensive agents with a placebo-like tolerability profile inpatients with hypertension. However, ARBs, like ACE inhib-itors, are associated with a near-flat dose--response curve whenadministered as monotherapy. This was demonstrated in ameta-analysis of 43 randomized, controlled trials, whichshowed modest incremental reductions in BP during ARBmonotherapy dose escalation, compared with the initial doseof ARB [29]. By contrast, combining ARBs with low-doseHCTZ resulted in substantial improvements in BP-loweringefficacy [29]. ARBs have since been successfully combinedwith HCTZ to provide increased antihypertensive efficacywithout major tolerability concerns in patients with hyperten-sion, including those who were not adequately controlled bymonotherapy [30-36].
Studies have shown that ARBs have different binding proper-ties with the different subtypes of angiotensin II receptors. As aconsequence of this, olmesartan medoxomil (OM; Box 1), anARB with a rapid onset of action, has been shown to providea higher affinity for, and a slower dissociation from, the AT1
receptor than other ARBs, such as telmisartan [37]. This may
in part explain the effective and prolonged antihypertensiveeffect that is provided by OM, which makes it a good candidatefor antihypertensive therapy in combination with HCTZ.
3. Olmesartan medoxomil plushydrochlorothiazide
Several large clinical trials of up to 12 weeks in duration havedemonstrated the superior antihypertensive efficacy of OMplus HCTZ to OM monotherapy in patients with mild-to-moderate hypertension [34,38,39]. In addition, the combinationof OM 20 mg plus HCTZ has been shown to provide signif-icantly better 24-h BP reduction than OM monotherapy inpatients with mild-to-moderate hypertension [34].
Olmesartan medoxomil plus HCTZ has also been shownto be effective compared with other HCTZ-based com-bination therapies, including nitrendipine/HCTZ [40] andatenolol plus HCTZ [41]. However, there are limited pub-lished data directly comparing OM plus HCTZ with otherARB--HCTZ combination therapies. In patients with moder-ate to severe hypertension, OM plus HCTZ was at least aseffective as losartan plus HCTZ [42]. In addition, a review offactorial-design studies demonstrated that OM plus HCTZprovided the largest placebo-corrected BP reductions, com-pared with other ARB--HCTZ combinations, includingirbesartan, telmisartan and valsartan [43].
Recent evidence has shown that OM dose dependentlyblocks the AT1 receptor, with the 40-mg dose producing agreater increase in plasma renin activity than the 20-mgdose [44]. This suggests that the use of a 40-mg dose may pro-long the duration of the antihypertensive effect of OM, whichmay translate into further improvements in the antihyperten-sive efficacy of OM--HCTZ combination therapy. Severalnew studies in the USA and in Europe have now assessedthe efficacy of using treatment with OM that includes theuse of the 40-mg dose and HCTZ.
3.1 High-dose olmesartan medoxomil plus
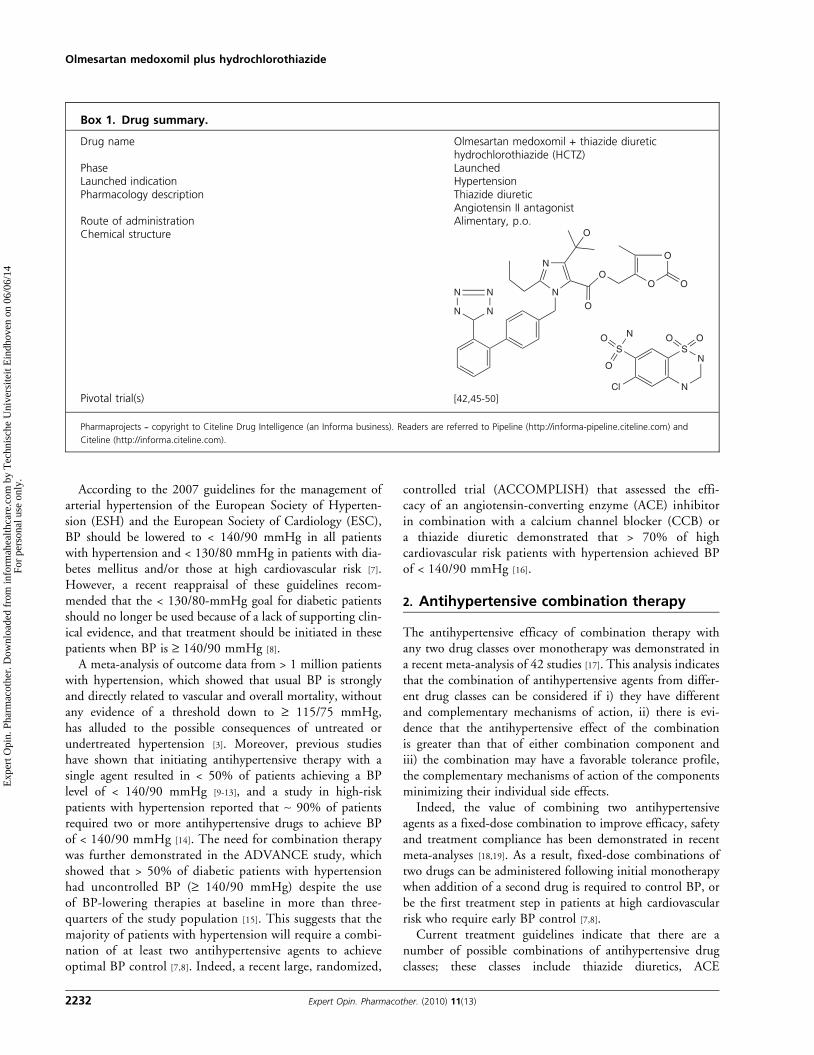
hydrochlorothiazide combination therapyThe benefits of combining a high dose ARB with HCTZ wasdemonstrated in a 16-week, open-label study that used anaggressive OM-based treatment algorithm in patients with stage2 systolic hypertension (pretreatment SBP ‡ 160 mmHg) [45].After an initial 3 weeks of treatment with OM 20 mg, patientswere uptitrated using a stepwise algorithm from OM 20 to40 mg, followed by the addition of HCTZ 12.5 mg andthen 25 mg until BP was normalized to < 120/80 mmHg.The primary end point for this study was the mean changefrom baseline in SBP after 12 weeks of treatment; second-ary end points included the proportions of patients whoachieved BP goal (< 140/90 mmHg) and BP normalization(< 120/80 mmHg) [45].
The uptitration of OM to 40 mg and the addition of increas-ing doses of HCTZ produced significant dose-dependent meanreductions in SBP that ranged from 18.4 mmHg with
Rump & Sellin
Expert Opin. Pharmacother. (2010) 11(13) 2233
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
echn
isch
e U
nive
rsite
it E
indh
oven
on
06/0
6/14
For
pers
onal
use
onl
y.

OM 40 mg to 34.5 mmHg with OM/HCTZ 40/25 mg(Figure 1) [45]. This enabled the majority of patients (70.4%)to achieve BP goal; ~ 15% of this stage 2 systolic hypertensionpopulation also achieved full BP normalization [42].An elective 4-week extension phase was also conducted
to assess the efficacy of uptitrating OM/HCTZ 40/25 --40/50 mg in patients whose BP remained > 120/80 mmHgat the end of the main 16-week study [46]. Patients whoentered and completed this extension phase had an additionalSBP reduction of 3.6 mmHg, which led to an improvementin both BP goal (from 70.4 to 77.5%) and BP normalization(from 15.4 to 27.8%) achievement rates [46].Based on these results, uptitrating OM to 40 mg and com-
bining high-dose OM with HCTZ not only improves BPlowering, but also enables the majority of patients to achieverecommended BP goals.Pivotal trials of high-dose OM have used two distinctly dif-
ferent types of study design. The US ‘treat-to-target’ studiesinvolved the same open-label, noncomparative study designto reflect real-world clinical practice and to provide insightsinto how the OM-based dose titration algorithm may beimplemented and the results that may be achieved. By con-trast, the European ‘add-on’ studies, in which nonresponderswere randomized to addition of a second drug or continuationof monotherapy, reflected the requirements mentioned in theEuropean regulatory guidelines for combination products inthe treatment of hypertension.
3.2 US ‘treat-to-target’ studiesFour studies conducted in the USA have confirmed the effec-tiveness of a dose titration treatment regimen comprisinghigh-dose OM/HCTZ [45-50].Three open-label studies, each of 12 weeks duration and
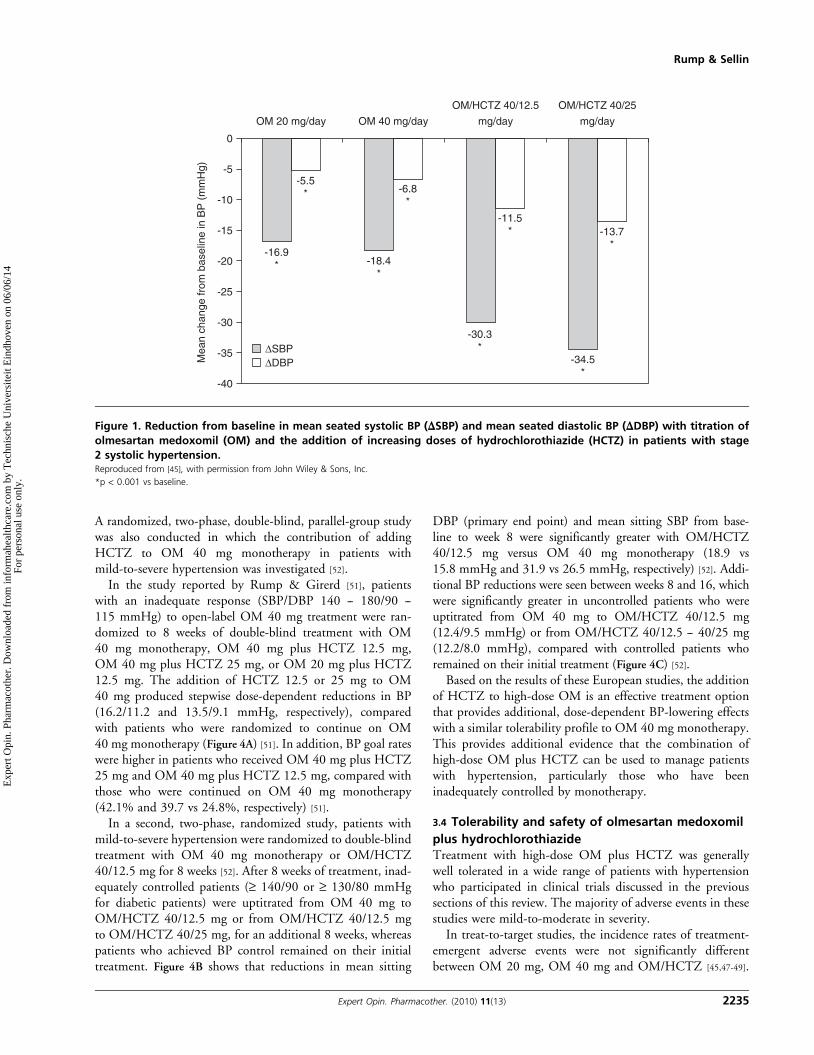
using the same OM-based dose-titration algorithm havebeen carried out in patients with stage 2 systolic hyperten-sion [45], in patients aged > 65 years [47] and in patients withdiabetes [48]. In the study of patients with stage 2 systolichypertension [45], the treatment algorithm began with once-daily OM 20 mg, followed by uptitration to the next doselevel (OM 40 mg, then with HCTZ 12.5 or 25 mg addedon) at 3-week intervals if seated SBP was ‡ 120/80 mmHg.Patients who achieved the BP goal of < 120/80 mmHg didnot undergo uptitration. Blood pressure reductions were dosedependent, largest in patients who received OM/HCTZ40/25 mg (34.5/13.7 mmHg), and 75.1% of patients achievedthe SBP goal of < 140 mmHg by the end of the 12-weekstudy [45]. The study of elderly patients with hypertensionused the same doses, combinations and uptitration timepoints, but patients were uptitrated if their seated SBP was‡ 120/70 mmHg [47]. At study end, a significant reduction inmean 24-h ambulatory BP was seen, along with progressiveimprovements in seated BP reductions that ranged from13.1/6.1 mmHg with OM 40 mg to 25.8/11.0 mmHg withOM/HCTZ 40/25 mg (Figure 2). Blood pressure goal ratesimproved from 19.3% with OM 20 mg to 33.0% with OM
40mg and 67.0% with OM/HCTZ 40/25 mg [47]. In addition,the majority of patients achieved 24-h ambulatory BP goals of< 140/90 (88.7%), < 130/85 (82.7%) and < 130/80 (73.3%)mmHg [47]. The BENIFICIARY trial used a similar titrationalgorithm to the elderly study to treat patients with hyper-tension and type 2 diabetes [48]. This approach resulted in asignificant reduction from baseline in mean 24-h ambulatoryBP (20.4/11.1 mmHg) and reductions in cuff seated BP,which ranged from 10.4/5.5 mmHg with OM 40 mg mono-therapy to 21.8/9.9 mmHg with OM/HCTZ 40/25 mg. Bystudy end, 61.6% of patients had achieved an ambulatoryBP goal of < 130/80 mmHg and 39.0% had achieved a goalof < 120/80 mmHg [48].
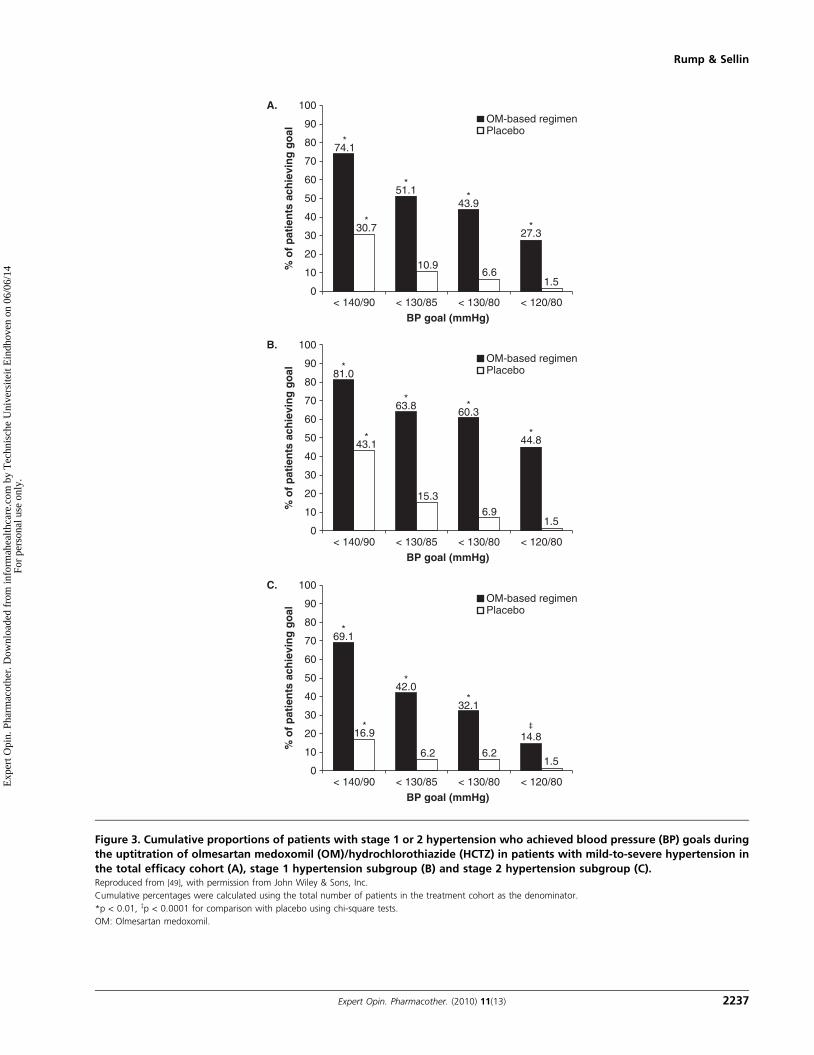
In addition to the three open-label studies, BENIFORCEwas a 12-week, double-blind, randomized, placebo-controlledtrial that also used a similar OM-based treatment algorithm inpatients with stage 1 or 2 hypertension [49]. The primary effi-cacy end point for this study was the change from baseline inmean SBP after 12 weeks of treatment; secondary end pointsincluded the change in mean DBP and the percentages ofpatients achieving a BP goal of < 140/90 mmHg and BPnormalization (< 120/80 mmHg). Significant BP reductionswere seen in the active treatment group, ranging from13.0/6.9 mmHg with OM 40 mg to 23.2/12.3 mmHg withOM/HCTZ 40/25 mg. Overall, 74.1% of patients achievedBP goal and 27.3% had their BP normalized, comparedwith 30.7 and 1.5% of placebo recipients, respectively(Figure 3) [49]. Furthermore, a large proportion of patients(44.8%) with stage 1 hypertension achieved BP normalizationwith OM-based therapy, compared with 1.4% in the placebogroup [49]. This indicates that a significant number of patientscan be treated with OM/HCTZ to ‘normotensive’ BP levels(i.e., levels not usually targeted in major clinical trials).A subgroup analysis of BENIFORCE was recently under-taken [50], which confirmed the ability of this OM-based treat-ment algorithm effectively to lower BP and improve BPgoal attainment in patients with stage 1 or 2 hypertension,regardless of race, gender or age.
It should be noted that a high proportion of patientsrequired uptitration to the highest dose combination(OM/HCTZ 40/25 mg) in these studies. This highlights theneed for uptitration using a treat-to-goal strategy based ontreatment guidelines when patients do not adequately respondto lower doses of antihypertensive therapy, and supports theuse of high-dose OM in combination with HCTZ to providesustained and improved BP control in a range of patients,including the elderly and those with diabetes.
3.3 European add-on studiesIn Europe, a large-scale, double-blind, randomized add-onstudy was conducted to assess the antihypertensive efficacyof high-dose OM (40 mg) plus HCTZ (12.5 or 25 mg) inpatients with moderate-to-severe hypertension who hadfailed to achieve a satisfactory level of BP control after8 weeks of treatment with OM 40 mg monotherapy [51].
Olmesartan medoxomil plus hydrochlorothiazide
2234 Expert Opin. Pharmacother. (2010) 11(13)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
echn
isch
e U
nive
rsite
it E
indh
oven
on
06/0
6/14
For
pers
onal
use
onl
y.
A randomized, two-phase, double-blind, parallel-group studywas also conducted in which the contribution of addingHCTZ to OM 40 mg monotherapy in patients withmild-to-severe hypertension was investigated [52].
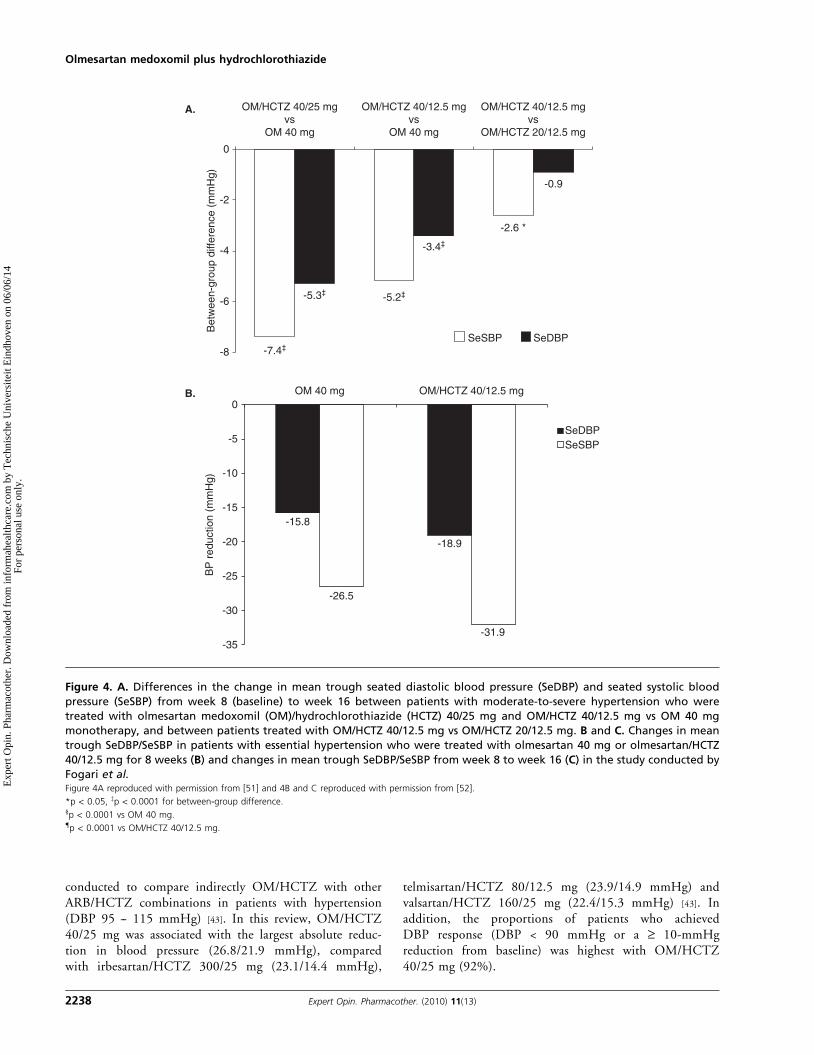
In the study reported by Rump & Girerd [51], patientswith an inadequate response (SBP/DBP 140 -- 180/90 --115 mmHg) to open-label OM 40 mg treatment were ran-domized to 8 weeks of double-blind treatment with OM40 mg monotherapy, OM 40 mg plus HCTZ 12.5 mg,OM 40 mg plus HCTZ 25 mg, or OM 20 mg plus HCTZ12.5 mg. The addition of HCTZ 12.5 or 25 mg to OM40 mg produced stepwise dose-dependent reductions in BP(16.2/11.2 and 13.5/9.1 mmHg, respectively), comparedwith patients who were randomized to continue on OM40 mg monotherapy (Figure 4A) [51]. In addition, BP goal rateswere higher in patients who received OM 40 mg plus HCTZ25 mg and OM 40 mg plus HCTZ 12.5 mg, compared withthose who were continued on OM 40 mg monotherapy(42.1% and 39.7 vs 24.8%, respectively) [51].
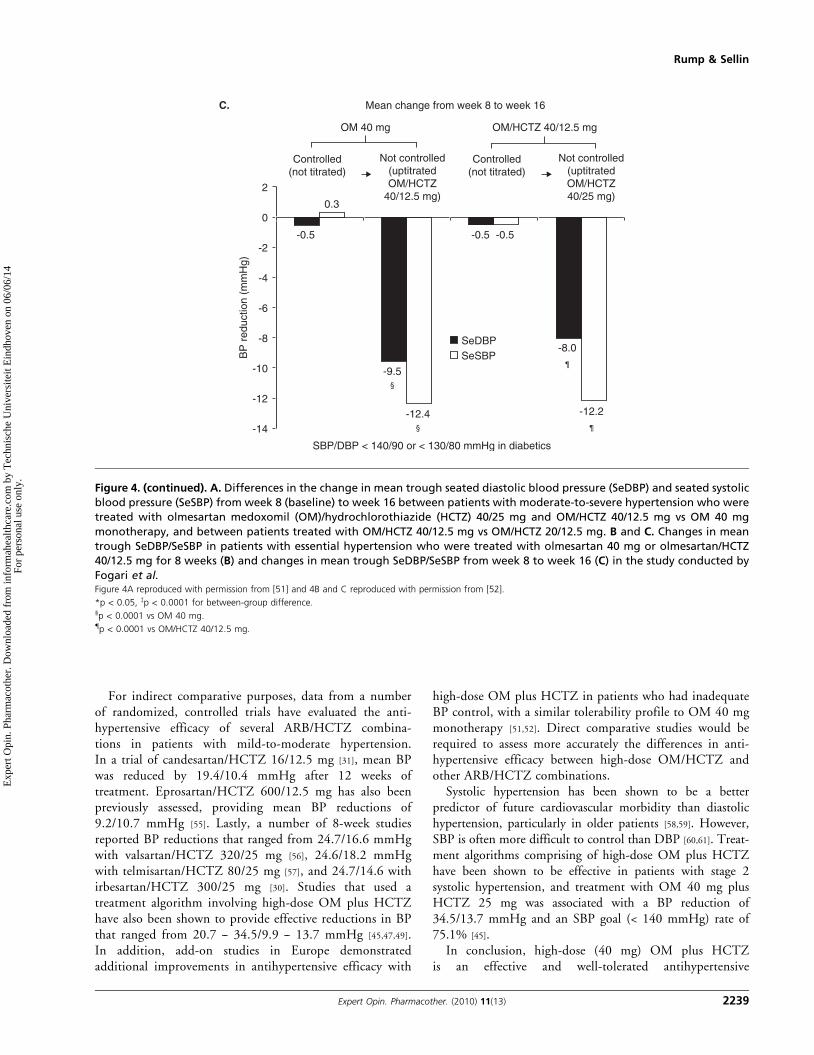
In a second, two-phase, randomized study, patients withmild-to-severe hypertension were randomized to double-blindtreatment with OM 40 mg monotherapy or OM/HCTZ40/12.5 mg for 8 weeks [52]. After 8 weeks of treatment, inad-equately controlled patients (‡ 140/90 or ‡ 130/80 mmHgfor diabetic patients) were uptitrated from OM 40 mg toOM/HCTZ 40/12.5 mg or from OM/HCTZ 40/12.5 mgto OM/HCTZ 40/25 mg, for an additional 8 weeks, whereaspatients who achieved BP control remained on their initialtreatment. Figure 4B shows that reductions in mean sitting
DBP (primary end point) and mean sitting SBP from base-line to week 8 were significantly greater with OM/HCTZ40/12.5 mg versus OM 40 mg monotherapy (18.9 vs15.8 mmHg and 31.9 vs 26.5 mmHg, respectively) [52]. Addi-tional BP reductions were seen between weeks 8 and 16, whichwere significantly greater in uncontrolled patients who wereuptitrated from OM 40 mg to OM/HCTZ 40/12.5 mg(12.4/9.5 mmHg) or from OM/HCTZ 40/12.5 -- 40/25 mg(12.2/8.0 mmHg), compared with controlled patients whoremained on their initial treatment (Figure 4C) [52].
Based on the results of these European studies, the additionof HCTZ to high-dose OM is an effective treatment optionthat provides additional, dose-dependent BP-lowering effectswith a similar tolerability profile to OM 40 mg monotherapy.This provides additional evidence that the combination ofhigh-dose OM plus HCTZ can be used to manage patientswith hypertension, particularly those who have beeninadequately controlled by monotherapy.
3.4 Tolerability and safety of olmesartan medoxomil
plus hydrochlorothiazideTreatment with high-dose OM plus HCTZ was generallywell tolerated in a wide range of patients with hypertensionwho participated in clinical trials discussed in the previoussections of this review. The majority of adverse events in thesestudies were mild-to-moderate in severity.
In treat-to-target studies, the incidence rates of treatment-emergent adverse events were not significantly differentbetween OM 20 mg, OM 40 mg and OM/HCTZ [45,47-49].
-40
ΔSBP
-16.9* -18.4
*
-30.3*
-34.5*
-5.5* -6.8
*
-11.5* -13.7
*
ΔDBP-35
-30
-25
Mea
n ch
ange
from
bas
elin
e in
BP
(m
mH
g)
-20
-15
-10
-5
0
OM 20 mg/day OM 40 mg/day mg/day
OM/HCTZ 40/12.5 OM/HCTZ 40/25
mg/day
Figure 1. Reduction from baseline in mean seated systolic BP (DSBP) and mean seated diastolic BP (DDBP) with titration of
olmesartan medoxomil (OM) and the addition of increasing doses of hydrochlorothiazide (HCTZ) in patients with stage
2 systolic hypertension.Reproduced from [45], with permission from John Wiley & Sons, Inc.
*p < 0.001 vs baseline.
Rump & Sellin
Expert Opin. Pharmacother. (2010) 11(13) 2235
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
echn
isch
e U
nive
rsite
it E
indh
oven
on
06/0
6/14
For
pers
onal
use
onl
y.
Moreover, the tolerability of OM-based therapy was notaffected by gender, age or race in a subgroup analysis of theBENIFORCE study [50]. Although uric acid concentrationswere reported to increase in OM/HCTZ recipients withincreasing doses of HCTZ, these were not considered tobe clinically significant, and no cases of gout were reportedin these patients [45,47]. Serum potassium concentrationswere also unaffected by the uptitration of OM/HCTZ40/25 -- 40/50 mg during the extension phase of the studyconducted by Izzo et al. [46], which indicates that the coad-ministration of OM and HCTZ may reduce the potassiumloss that is associated with HCTZ therapy.In the European add-on study conducted by Rump &
Girerd [51], treatment-emergent adverse events were similar infrequency among the OM 40-mg, OM/HCTZ 20/12.5-mg,OM/HCTZ 40/12.5-mg and OM/HCTZ 40/25-mg groups,with no significant changes in clinical laboratory tests.
4. Conclusions
Combination antihypertensive therapy with high-dose OM(40 mg) plus HCTZ has been shown to be an effectiveand well tolerated treatment option for the managementof patients with inadequately controlled mild-to-severehypertension. Treat-to-target studies conducted in the USAdemonstrate that OM/HCTZ provides dose-dependentimprovements in BP reduction and BP goal attainment ina wide range of patients, with a similar tolerability profileto OM monotherapy. The maximal obtainable efficacy
with these treatment strategies was achieved by OM/HCTZ40/25 mg. Furthermore, a number of European studies havealso demonstrated that the addition of HCTZ to high-doseOM significantly improves the antihypertensive efficacy inpatients who are inadequately controlled by OM monother-apy and brings more patients to goal levels of BP. Olmesartanmedoxomil 40 mg plus HCTZ also produces better 24-hambulatory BP reductions than OM 20 mg plus HCTZ,which indicates sustained BP control over the 24-hdosing period.
5. Expert opinion
Despite the availability of numerous treatment options forthe management of hypertension, an estimated 30 -- 50% ofpatients are inadequately controlled on their current antihy-pertensive regimens [53,54]. As a result, European treatmentguidelines indicate that the majority of patients with hyper-tension will require combination therapy with two or moreantihypertensive agents to achieve optimal blood pressurecontrol [7,8].
The high-dose OM (40 mg) plus HCTZ combinationwas introduced in Europe in December 2009 and clinicaltrials have demonstrated its effectiveness and safety asan additional treatment option to treat patients to goal.So far, there have been no published data that directlycompare high-dose OM plus HCTZ with other ARB--HCTZ combinations. However, an analysis of randomized,double-blind, placebo-controlled, factorial studies was
-25.7*-30
-25
-20
-15
Cha
nge
from
bas
elin
e to
wee
k 12
inam
bula
tory
BP
(m
mH
g)
-10
-5
0
24-h
Daytime(8 am-4 pm)
Nighttime(10 pm-6 am) Last hours of dosing interval
6 h 4 h 2 h
SBP
DBP
-26.5*
-24.4*
-24.1*
-24.4*
-24.2*
-12.3*
-13.0*
-11.5*
-11.6*
-11.8*
-11.4*
Figure 2. Blood pressure (BP)-lowering efficacy of the olmesartan medoxomil (OM)-based treatment algorithm in elderly
($ 65 years) patients with hypertension: change from baseline in mean 24-h, daytime, and night-time ambulatory BP (± SE)
and during the last 6, 4 and 2 h of the 24-h dosing interval at week 12, as assessed by ambulatory BP monitoring.Reproduced from [47], with permission from John Wiley & Sons, Inc.
*p < 0.0001 vs baseline.
DBP: Diastolic blood pressure; HCTZ: Hydrochlorothiazide; SBP: Systolic blood pressure; SE: Standard error.
Olmesartan medoxomil plus hydrochlorothiazide
2236 Expert Opin. Pharmacother. (2010) 11(13)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
echn
isch
e U
nive
rsite
it E
indh
oven
on
06/0
6/14
For
pers
onal
use
onl
y.
< 140/900
10
20
30
40
50
60
% o
f p
atie
nts
ach
ievi
ng
go
al
70
80
90
100A.
74.1*
30.7*
51.1*
43.9
10.96.6
1.5
*
OM-based regimenPlacebo
27.3*
< 130/85
BP goal (mmHg)< 130/80 < 120/80
B.
< 140/900
10
20
30
40
50
60
% o
f p
atie
nts
ach
ievi
ng
go
al
70
80
90
100
81.0*
43.1*
63.8*
60.3
15.3
6.91.5
*
OM-based regimenPlacebo
44.8*
< 130/85
BP goal (mmHg)< 130/80 < 120/80
C.
< 140/900
10
20
30
40
50
60
% o
f p
atie
nts
ach
ievi
ng
go
al
70
80
90
100
69.1*
16.9*
42.0*
32.1
6.2 6.21.5
*
OM-based regimenPlacebo
14.8‡
< 130/85
BP goal (mmHg)< 130/80 < 120/80
Figure 3. Cumulative proportions of patients with stage 1 or 2 hypertension who achieved blood pressure (BP) goals during
the uptitration of olmesartan medoxomil (OM)/hydrochlorothiazide (HCTZ) in patients with mild-to-severe hypertension in
the total efficacy cohort (A), stage 1 hypertension subgroup (B) and stage 2 hypertension subgroup (C).Reproduced from [49], with permission from John Wiley & Sons, Inc.
Cumulative percentages were calculated using the total number of patients in the treatment cohort as the denominator.
*p < 0.01, zp < 0.0001 for comparison with placebo using chi-square tests.
OM: Olmesartan medoxomil.
Rump & Sellin
Expert Opin. Pharmacother. (2010) 11(13) 2237
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
echn
isch
e U
nive
rsite
it E
indh
oven
on
06/0
6/14
For
pers
onal
use
onl
y.
conducted to compare indirectly OM/HCTZ with otherARB/HCTZ combinations in patients with hypertension(DBP 95 -- 115 mmHg) [43]. In this review, OM/HCTZ40/25 mg was associated with the largest absolute reduc-tion in blood pressure (26.8/21.9 mmHg), comparedwith irbesartan/HCTZ 300/25 mg (23.1/14.4 mmHg),
telmisartan/HCTZ 80/12.5 mg (23.9/14.9 mmHg) andvalsartan/HCTZ 160/25 mg (22.4/15.3 mmHg) [43]. Inaddition, the proportions of patients who achievedDBP response (DBP < 90 mmHg or a ‡ 10-mmHgreduction from baseline) was highest with OM/HCTZ40/25 mg (92%).
-5.3‡
-3.4‡
-0.9
-2.6 *
-7.4‡
-5.2‡
-8
-6
-4
-2
0
Bet
wee
n-gr
oup
diffe
renc
e (m
mH
g)
SeSBP SeDBP
OM/HCTZ 40/12.5 mgvs
OM/HCTZ 20/12.5 mg
OM/HCTZ 40/12.5 mgvs
OM 40 mg
OM/HCTZ 40/25 mgvs
OM 40 mg
B.
A.
-35
-30
-25
-20
-15.8
-26.5
-18.9
-31.9
SeDBPSeSBP
BP
red
uctio
n (m
mH
g)
-15
-10
-5
0OM 40 mg OM/HCTZ 40/12.5 mg
Figure 4. A. Differences in the change in mean trough seated diastolic blood pressure (SeDBP) and seated systolic blood
pressure (SeSBP) from week 8 (baseline) to week 16 between patients with moderate-to-severe hypertension who were
treated with olmesartan medoxomil (OM)/hydrochlorothiazide (HCTZ) 40/25 mg and OM/HCTZ 40/12.5 mg vs OM 40 mg
monotherapy, and between patients treated with OM/HCTZ 40/12.5 mg vs OM/HCTZ 20/12.5 mg. B and C. Changes in mean
trough SeDBP/SeSBP in patients with essential hypertension who were treated with olmesartan 40 mg or olmesartan/HCTZ
40/12.5 mg for 8 weeks (B) and changes in mean trough SeDBP/SeSBP from week 8 to week 16 (C) in the study conducted by
Fogari et al.Figure 4A reproduced with permission from [51] and 4B and C reproduced with permission from [52].
*p < 0.05, zp < 0.0001 for between-group difference.§p < 0.0001 vs OM 40 mg.{p < 0.0001 vs OM/HCTZ 40/12.5 mg.
Olmesartan medoxomil plus hydrochlorothiazide
2238 Expert Opin. Pharmacother. (2010) 11(13)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
echn
isch
e U
nive
rsite
it E
indh
oven
on
06/0
6/14
For
pers
onal
use
onl
y.
For indirect comparative purposes, data from a numberof randomized, controlled trials have evaluated the anti-hypertensive efficacy of several ARB/HCTZ combina-tions in patients with mild-to-moderate hypertension.In a trial of candesartan/HCTZ 16/12.5 mg [31], mean BPwas reduced by 19.4/10.4 mmHg after 12 weeks oftreatment. Eprosartan/HCTZ 600/12.5 mg has also beenpreviously assessed, providing mean BP reductions of9.2/10.7 mmHg [55]. Lastly, a number of 8-week studiesreported BP reductions that ranged from 24.7/16.6 mmHgwith valsartan/HCTZ 320/25 mg [56], 24.6/18.2 mmHgwith telmisartan/HCTZ 80/25 mg [57], and 24.7/14.6 withirbesartan/HCTZ 300/25 mg [30]. Studies that used atreatment algorithm involving high-dose OM plus HCTZhave also been shown to provide effective reductions in BPthat ranged from 20.7 -- 34.5/9.9 -- 13.7 mmHg [45,47,49].In addition, add-on studies in Europe demonstratedadditional improvements in antihypertensive efficacy with
high-dose OM plus HCTZ in patients who had inadequateBP control, with a similar tolerability profile to OM 40 mgmonotherapy [51,52]. Direct comparative studies would berequired to assess more accurately the differences in anti-hypertensive efficacy between high-dose OM/HCTZ andother ARB/HCTZ combinations.
Systolic hypertension has been shown to be a betterpredictor of future cardiovascular morbidity than diastolichypertension, particularly in older patients [58,59]. However,SBP is often more difficult to control than DBP [60,61]. Treat-ment algorithms comprising of high-dose OM plus HCTZhave been shown to be effective in patients with stage 2systolic hypertension, and treatment with OM 40 mg plusHCTZ 25 mg was associated with a BP reduction of34.5/13.7 mmHg and an SBP goal (< 140 mmHg) rate of75.1% [45].
In conclusion, high-dose (40 mg) OM plus HCTZis an effective and well-tolerated antihypertensive
C.
-14
-12
-10
BP
red
uctio
n (m
mH
g)
-8
-6
-4
-2
0
-0.5 -0.5 -0.5
-8.0
¶-9.5
§
-12.4§
SeDBPSeSBP
SBP/DBP < 140/90 or < 130/80 mmHg in diabetics
-12.2
¶
0.3
Mean change from week 8 to week 16
OM 40 mg
Controlled(not titrated)
Controlled(not titrated)
Not controlled(uptitratedOM/HCTZ
40/12.5 mg)
Not controlled(uptitratedOM/HCTZ40/25 mg)
OM/HCTZ 40/12.5 mg
2
Figure 4. (continued). A. Differences in the change in mean trough seated diastolic blood pressure (SeDBP) and seated systolic
blood pressure (SeSBP) from week 8 (baseline) to week 16 between patients with moderate-to-severe hypertension who were
treated with olmesartan medoxomil (OM)/hydrochlorothiazide (HCTZ) 40/25 mg and OM/HCTZ 40/12.5 mg vs OM 40 mg
monotherapy, and between patients treated with OM/HCTZ 40/12.5 mg vs OM/HCTZ 20/12.5 mg. B and C. Changes in mean
trough SeDBP/SeSBP in patients with essential hypertension who were treated with olmesartan 40 mg or olmesartan/HCTZ
40/12.5 mg for 8 weeks (B) and changes in mean trough SeDBP/SeSBP from week 8 to week 16 (C) in the study conducted by
Fogari et al.Figure 4A reproduced with permission from [51] and 4B and C reproduced with permission from [52].
*p < 0.05, zp < 0.0001 for between-group difference.§p < 0.0001 vs OM 40 mg.{p < 0.0001 vs OM/HCTZ 40/12.5 mg.
Rump & Sellin
Expert Opin. Pharmacother. (2010) 11(13) 2239
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
echn
isch
e U
nive
rsite
it E
indh
oven
on
06/0
6/14
For
pers
onal
use
onl
y.

combination therapy for the management of hypertension.This combination therapy has been shown to be more effi-cacious than OM 40 mg monotherapy and may be a use-ful treatment option in patients who are unable to achieverecommended BP goals with monotherapy. However,large, well-controlled, long-term studies are required todetermine if these improvements in antihypertensive effi-cacy will translate into beneficial effects on clinical out-comes and the overall risk profile of patientswith hypertension.
Acknowledgement
We thank S Lancaster of inScience Communications, aWolters Kluwer business, UK, for providing editorialassistance in the preparation of this review.
Declaration of interest
The editorial assistance was funded by Daiichi SankyoEurope GmbH.
BibliographyPapers of special note have been highlighted as
either of interest (�) or of considerable interest(��) to readers.
1. Kearney PM, Whelton M, Reynolds K,
et al. Global burden of hypertension:
analysis of worldwide data. Lancet
2005;365:217-23
2. Ezzati M, Lopez AD, Rodgers A,
et al. Selected major risk factors and
global and regional burden of disease.
Lancet 2002;360:1347-60
3. Lewington S, Clarke R, Qizilbash N,
et al. Age-specific relevance of usual
blood pressure to vascular mortality:
a meta-analysis of individual data for
one million adults in 61 prospective
studies. Lancet 2002;360:1903-13.. A large meta-analysis demonstrating
the strong and linear relationship
between blood pressure and
cardiovascular events. Results from
this analysis showed that the risk
of cardiovascular mortality increased
by more than two-fold for each
20-mmHg increase in systolic blood
pressure or 10-mmHg increase in
diastolic blood pressure in patients
aged 40 -- 69 years.
4. Padwal R, Straus SE, McAlister FA.
Evidence based management of
hypertension. Cardiovascular risk factors
and their effects on the decision to treat
hypertension: evidence based review.
BMJ 2001;322:977-80
5. Thorp ML, Eastman L, Smith DH,
Johnson ES. Managing the burden
of chronic kidney disease. Dis Manag
2006;9:115-21
6. Kopyt NP. Slowing progression
along the renal disease continuum.
J Am Osteopath Assoc 2005;105:207-15
7. Mancia G, De Backer G, Dominiczak A,
et al. 2007 Guidelines for the
Management of Arterial Hypertension:
the Task Force for the Management of
Arterial Hypertension of the European
Society of Hypertension (ESH) and
of the European Society of Cardiology
(ESC). J Hypertens 2007;25:1105-87
8. Mancia G, Laurent S, Agabiti-Rosei E,
et al. Reappraisal of European guidelines
on hypertension management:
a European Society of Hypertension
Task Force document. J Hypertens
2009;27:2121-58
9. ALLHAT Officers and Coordinators
for the ALLHAT Collaborative
Research Group. Major outcomes
in high-risk hypertensive patients
randomized to angiotensin-converting
enzyme inhibitor or calcium channel
blocker vs diuretic: the Antihypertensive
and Lipid-Lowering Treatment to
Prevent Heart Attack Trial (ALLHAT).
JAMA 2002;288:2981-97
10. Materson BJ, Reda DJ, Cushman WC,
et al. Single-drug therapy for
hypertension in men. A comparison
of six antihypertensive agents with
placebo. Department of Veterans
Affairs Cooperative Study Group
on Antihypertensive Agents.
N Engl J Med 1993;328:914-21
11. Philipp T, Anlauf M, Distler A, et al.
Randomised, double blind, multicentre
comparison of hydrochlorothiazide,
atenolol, nitrendipine, and enalapril
in antihypertensive treatment: results of
the HANE study. HANE Trial Research
Group. BMJ 1997;315:154-9
12. Dahlof B, Devereux RB, Kjeldsen SE,
et al. Cardiovascular morbidity and
mortality in the Losartan Intervention
for Endpoint reduction in hypertension
study (LIFE): a randomised trial against
atenolol. Lancet 2002;359:995-1003
13. Beckett NS, Peters R, Fletcher AE, et al.
Treatment of hypertension in patients
80 years of age or older. N Engl J Med
2008;358:1887-98
14. Dahlof B, Sever PS, Poulter NR,
et al. Prevention of cardiovascular events
with an antihypertensive regimen of
amlodipine adding perindopril as
required versus atenolol adding
bendroflumethiazide as required, in the
Anglo-Scandinavian Cardiac Outcomes
Trial-Blood Pressure Lowering Arm
(ASCOT-BPLA): a multicentre
randomised controlled trial. Lancet
2005;366:895-906
15. Patel A, MacMahon S, Chalmers J,
et al. Effects of a fixed combination
of perindopril and indapamide on
macrovascular and microvascular
outcomes in patients with type 2
diabetes mellitus (the ADVANCE
trial): a randomised controlled trial.
Lancet 2007;370:829-40
16. Jamerson K, Weber MA, Bakris GL,
et al. Benazepril plus amlodipine or
hydrochlorothiazide for hypertension
in high-risk patients. N Engl J Med
2008;359:2417-28
17. Wald DS, Law M, Morris JK, et al.
Combination therapy versus
monotherapy in reducing blood
pressure: meta-analysis on
11,000 participants from 42 trials.
Am J Med 2009;122:290-300. A recent, large meta-analysis that
assessed the antihypertensive efficacy
and safety of combination therapy
with drugs from different classes. One
of the key points in this analysis is
that it shows that combining agents
from two different drug classes
(thiazide diuretics, beta-blockers,
angiotensin-converting enzyme
inhibitors or calcium channel blockers)
is approximately five times more
effective at lowering blood pressure
than doubling the dose of a
single drug.
18. Bangalore S, Kamalakkannan G,
Parkar S, Messerli FH. Fixed-dose
Olmesartan medoxomil plus hydrochlorothiazide
2240 Expert Opin. Pharmacother. (2010) 11(13)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
echn
isch
e U
nive
rsite
it E
indh
oven
on
06/0
6/14
For
pers
onal
use
onl
y.
combinations improve medication
compliance: a meta-analysis.
Am J Med 2007;120:713-19
19. Gupta AK, Arshad S, Poulter NR.
Compliance, safety, and effectiveness
of fixed-dose combinations of
antihypertensive agents: a meta-analysis.
Hypertension 2010;55:399-407. A recent meta-analysis that
demonstrated that fixed-dose
antihypertensive combination therapy
led to significantly greater compliance
than combination therapy with the
same agents administered as free-drug
combinations, together with a trend
towards improved blood
pressure control.
20. Bangalore S, Parkar S, Grossman E,
Messerli FH. A meta-analysis of
94,492 patients with hypertension
treated with beta blockers to determine
the risk of new-onset diabetes mellitus.
Am J Cardiol 2007;100:1254-62
21. Elliott WJ, Meyer PM. Incident diabetes
in clinical trials of antihypertensive drugs:
a network meta-analysis. Lancet
2007;369:201-7
22. Mancia G, Grassi G, Zanchetti A.
New-onset diabetes and antihypertensive
drugs. J Hypertens 2006;24:3-10
23. Yusuf S, Teo KK, Pogue J, et al.
Telmisartan, ramipril, or both in
patients at high risk for vascular events.
N Engl J Med 2008;358:1547-59
24. Mann JF, Schmieder RE, McQueen M,
et al. Renal outcomes with telmisartan,
ramipril, or both, in people at high
vascular risk (the ONTARGET
study): a multicentre, randomised,
double-blind, controlled trial.
Lancet 2008;372:547-53
25. Kjeldsen SE, Os I, Hoieggen A,
et al. Fixed-dose combinations in the
management of hypertension: defining
the place of angiotensin receptor
antagonists and hydrochlorothiazide.
Am J Cardiovasc Drugs 2005;5:17-22
26. Hoieggen A, Alderman MH,
Kjeldsen SE, et al. The impact of
serum uric acid on cardiovascular
outcomes in the LIFE study.
Kidney Int 2004;65:1041-9
27. Lindholm LH, Ibsen H, Dahlof B, et al.
Cardiovascular morbidity and mortality
in patients with diabetes in the Losartan
Intervention for Endpoint reduction in
hypertension study (LIFE): a randomised
trial against atenolol. Lancet
2002;359:1004-10
28. Lindholm LH, Persson M, Alaupovic P,
et al. Metabolic outcome during 1 year
in newly detected hypertensives: results
of the Antihypertensive Treatment
and Lipid Profile in a North of Sweden
Efficacy Evaluation (ALPINE study).
J Hypertens 2003;21:1563-74
29. Conlin PR, Spence JD, Williams B,
et al. Angiotensin II antagonists for
hypertension: are there differences in
efficacy? Am J Hypertens
2000;13:418-26
30. Neutel JM, Franklin SS, Lapuerta P,
et al. A comparison of the efficacy
and safety of irbesartan/HCTZ
combination therapy with
irbesartan and HCTZ monotherapy
in the treatment of moderate
hypertension. J Hum Hypertens
2008;22:266-74
31. Ohman KP, Milon H, Valnes K.
Efficacy and tolerability of a
combination tablet of candesartan
cilexetil and hydrochlorothiazide
in insufficiently controlled primary
hypertension -- comparison with
a combination of losartan and
hydrochlorothiazide. Blood Press
2000;9:214-20
32. Plosker GL, White WB.
Telmisartan/hydrochlorothiazide:
a review of its use as fixed-dose
combinations in essential hypertension.
Drugs 2008;68:1877-99
33. Schmidt A, Adam SA, Kolloch R,
et al. Antihypertensive effects of
valsartan/hydrochlorothiazide combina-
tion in essential hypertension.
Blood Press 2001;10:230-7
34. Sellin L, Stegbauer J, Laeis P, Rump LC.
Adding hydrochlorothiazide to
olmesartan dose dependently improves
24-h blood pressure and response
rates in mild-to-moderate hypertension.
J Hypertens 2005;23:2083-92
35. Waeber B, Aschwanden R, Sadecky L,
Ferber P. Combination of
hydrochlorothiazide or benazepril
with valsartan in hypertensive patients
unresponsive to valsartan alone.
J Hypertens 2001;19:2097-104
36. Wagstaff AJ. Valsartan/
hydrochlorothiazide: a review of its
use in the management of hypertension.
Drugs 2006;66:1881-901
37. Le MT, Pugsley MK, Vauquelin G,
Van Liefde I. Molecular characterisation
of the interactions between olmesartan
and telmisartan and the human
angiotensin II AT1 receptor.
Br J Pharmacol 2007;151:952-62. An in vitro study which showed that
olmesartan (OM) was associated with
a more potent interaction with
the AT1 receptor than telmisartan
in CHO-K1 cells that express human
AT1 receptors.
38. Barrios V, Boccanelli A, Ewald S, et al.
Efficacy and tolerability of olmesartan
medoxomil in patients with mild to
moderate essential hypertension: the
OLMEBEST Study. Clin Drug Investig
2007;27:545-58
39. Chrysant SG, Weber MA,
Wang AC, Hinman DJ. Evaluation
of antihypertensive therapy with
the combination of olmesartan
medoxomil and hydrochlorothiazide.
Am J Hypertens 2004;17:252-9. A prospective clinical study with a
factorial design which demonstrates
that combining an angiotensin II
receptor blocker (ARB) with
hydrochlorothiazide (HCTZ) is
superior to increasing the dose of
either of the two individual agents.
40. Mallion JM, Heagerty A, Laeis P.
Systolic blood pressure reduction
with olmesartan medoxomil versus
nitrendipine in elderly patients
with isolated systolic hypertension.
J Hypertens 2007;25:2168-77
41. Ball KJ, Williams PA, Stumpe KO.
Relative efficacy of an angiotensin II
antagonist compared with other
antihypertensive agents. Olmesartan
medoxomil versus antihypertensives.
J Hypertens Suppl 2001;19:S49-56
42. Rump LC, Ambrosioni E, Burnier M,
et al. Initial combination therapy
with olmesartan/hydrochlorothiazide
in moderate-to-severe hypertension.
J Hum Hypertens 2006;20:299-301
43. Ram CV. Antihypertensive efficacy
of angiotensin receptor blockers in
combination with hydrochlorothiazide:
a review of the factorial-design studies.
J Clin Hypertens (Greenwich)
2004;6:569-77
Rump & Sellin
Expert Opin. Pharmacother. (2010) 11(13) 2241
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
echn
isch
e U
nive
rsite
it E
indh
oven
on
06/0
6/14
For
pers
onal
use
onl
y.
44. Jones MR, Sealey JE, Laragh JH.
Effects of angiotensin receptor
blockers on ambulatory plasma renin
activity in healthy, normal subjects
during unrestricted sodium intake.
Am J Hypertens 2007;20:907-16. An analysis of two small crossover
studies in volunteers, which showed
that OM 40 mg provided the greatest
change in 24-h plasma renin activity,
compared with high-dose valsartan
and high-dose irbesartan. The increase
in 24-h plasma renin activity is a
feedback effect of
AT1 receptor blockade.
45. Izzo Jr JL, Neutel JM, Silfani T, et al.
Efficacy and safety of treating stage
2 systolic hypertension with olmesartan
and olmesartan/HCTZ: results of an
open-label titration study. J Clin
Hypertens (Greenwich) 2007;9:36-44.. An open-label study evaluating the
antihypertensive efficacy and safety
of a titrate-to-goal treatment
algorithm comprising OM and
OM/HCTZ in patients with stage
2 systolic hypertension. The results
of titrate-to-goal studies like this
and the others reported in [44-46]
demonstrate the efficacy of
combination therapy and show that
the majority of patients can achieve
goal with a simple treatment algorithm
that avoids ‘physician inertia’. Studies
like these show that the therapeutic
tools available now are effective, and
that the reasons for the high rates of
uncontrolled hypertension seen in
many countries relate more to failure
to treat patients with sufficient vigor.
46. Izzo Jr JL, Neutel JM, Silfani T,
et al. Titration of HCTZ to 50 mg
daily in individuals with stage 2 systolic
hypertension pretreated with an
angiotensin receptor blocker. J Clin
Hypertens (Greenwich) 2007;9:45-8
47. Kereiakes DJ, Neutel J, Stoakes KA,
et al. The effects of an olmesartan
medoxomil-based treatment algorithm
on 24-hour blood pressure levels in
elderly patients aged 65 and older.
J Clin Hypertens (Greenwich)
2009;11:411-21
48. Neutel JM, Kereiakes DJ,
Waverczak WF, et al. Effects of an
olmesartan medoxomil based treatment
algorithm on 24-hour blood pressure
control in patients with hypertension
and type 2 diabetes. Curr Med Res Opin
2010;26:721-8
49. Oparil S, Chrysant SG, Kereiakes D,
et al. Results of an olmesartan
medoxomil-based treatment regimen in
hypertensive patients. J Clin Hypertens
(Greenwich) 2008;10:911-21
50. Oparil S, Pimenta E. Efficacy of an
olmesartan medoxomil-based treatment
algorithm in patients stratified by age,
race, or sex. J Clin Hypertens
(Greenwich) 2010;12:3-13.. A prespecified subgroup analysis of
the titrate-to-goal BENIFORCE trial,
which showed that an OM-based
titration regimen allowed effective
blood pressure goal achievement
in patients with stage 1 or 2
hypertension, irrespective of race,
gender or age. These results indicate
that ARB-based treat-to-goal regimens
can provide effective blood pressure
control in a range of patient types.
51. Rump LC, Girerd X.
Hydrochlorothiazide (HCTZ) provides
additional blood pressure (BP)-lowering
when used as an add-on therapy in
patients with moderate-to-severe
hypertension whose BP is not
adequately controlled by olmesartan
medoxomil (OM) 40 mg. J Hypertens
2009;27(Suppl 4):S282
52. Fogari R. Phase III study evaluating
the efficacy and safety of olmesartan
medoxomil/hydrochlorothiazide
40/12.5 mg combination therapy
versus olmesartan medoxomil
40 mg monotherapy in patients with
essential hypertension. J Hypertens
2009;27(Suppl 4):S275
53. EUROASPIRE II Study Group.
Lifestyle and risk factor management
and use of drug therapies in coronary
patients from 15 countries; principal
results from EUROASPIRE II Euro
Heart Survey Programme. Eur Heart J
2001;22:554-72
54. Primatesta P, Brookes M, Poulter NR.
Improved hypertension management and
control: results from the health survey for
England 1998. Hypertension
2001;38:827-32
55. Sachse A, Verboom CN, Jager B.
Efficacy of eprosartan in combination
with HCTZ in patients with essential
hypertension. J Hum Hypertens
2002;16:169-76
56. Pool JL, Glazer R, Weinberger M,
et al. Comparison of valsartan/
hydrochlorothiazide combination
therapy at doses up to 320/25 mg
versus monotherapy: a double-blind,
placebo-controlled study followed by
long-term combination therapy in
hypertensive adults. Clin Ther
2007;29:61-73
57. White WB, Murwin D, Chrysant SG,
et al. Effects of the angiotensin II
receptor blockers telmisartan versus
valsartan in combination with
hydrochlorothiazide: a large,
confirmatory trial. Blood Press Monit
2008;13:21-7
58. European Society of
Hypertension-European Society of
Cardiology Guidelines Committee.
2003 European Society of
Hypertension-European Society
of Cardiology guidelines for the
management of arterial hypertension.
J Hypertens 2003;21:1011-53
59. Izzo Jr JL, Levy D, Black HR.
Clinical Advisory Statement.
Importance of systolic blood
pressure in older Americans.
Hypertension 2000;35:1021-4
60. Mancia G, Bombelli M, Lanzarotti A,
et al. Systolic vs diastolic blood pressure
control in the hypertensive patients of
the PAMELA population. Pressioni
Arteriose Monitorate e Loro Associazioni.
Arch Intern Med 2002;162:582-6
61. Swales JD. Current clinical practice in
hypertension: the EISBERG (Evaluation
and Interventions for Systolic Blood
pressure Elevation-Regional and Global)
project. Am Heart J 1999;138:231-7
AffiliationLars Christian Rump† & Lorenz Sellin†Author for correspondence
Heinrich-Heine-University Dusseldorf,
Department of Internal Medicine/Nephrology,
Moorenstr. 5, 40225
Dusseldorf, Germany
E-mail: [email protected]
Olmesartan medoxomil plus hydrochlorothiazide
2242 Expert Opin. Pharmacother. (2010) 11(13)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
echn
isch
e U
nive
rsite
it E
indh
oven
on
06/0
6/14
For
pers
onal
use
onl
y.



















![[Product Monograph Template - Standard] · OLMETEC PLUS® (olmesartan medoxomil and hydrochlorothiazide) Page 1 of 36. PRODUCT MONOGRAPH . OLMETEC PLUS® Olmesartan Medoxomil and](https://img.pdfslide.us/doc/110x75/60922706910bc76da54dbac2/product-monograph-template-standard-olmetec-plus-olmesartan-medoxomil-and.jpg)








