Embed Size (px)
Citation preview
Combination of very low energy diets andpharmacotherapy in the treatment of obesity:meta-analysis of published data
Eleni Koutroumanidou1,2*Olga Pagonopoulou2
1Clinical and Public HealthNutrition MSc,University College London,London, UK2Department of Physiology,Medical School,Democritus University of Thrace,Alexandroupolis, Greece
*Correspondence to:Eleni Koutroumanidou, Departmentof Physiology, Medical School,Democritus University of Thrace,Dragana University Campus, 68100,Alexandroupolis, Greece.E-mail: [email protected]
Summary
Obesity has reached epidemic proportions globally, with more than 1 billionadults overweight – at least 300 million of them clinically obese – and is amajor contributor to the global burden of chronic disease (heart disease anddiabetes) and disability. The aim of the study was to perform a systematicreview and meta-analysis of published data on the combination of very lowenergy diets also known as very low calorie diets and pharmacotherapy forits effectiveness in the treatment of obesity. A MEDLINE (Pubmed) searchfrom 1970 to 2009 using multiple combinations of the relevant terms wascarried out; the matching articles were also searched for additional refer-ences. Meta-analysis tools were used to summarize results. Only randomizedcontrolled trials that compared pharmacotherapy with placebo after a verylow energy diet period were selected, and six articles were finally consideredto be appropriate for evaluation. The combination of very low energy diet andpharmacotherapy was found to be effective for people with obesity in clinicaltrials. The net effect of 6.1 kg placebo subtracted weight loss after 1 yearrepresents a clinically meaningful result that is comparable with the effectof drugs given at the start of a weight loss programme. The present meta-analysis contributes to the understanding that combination therapies areexpected to achieve greater weight loss than monotherapy; grasping thisunderstanding, researcher has introduced newer anti-obesity pharmacologi-cal approaches have embraced combination therapies. Copyright © 2013John Wiley & Sons, Ltd.
Keywords very low energy diets; pharmacotherapy; obesity
Introduction
The high prevalence of obesity and obesity-related diseases affirms theneed for effective treatments for weight loss. The present study dealswith the efficacy of pharmacotherapies for obesity in combination withvery low energy diets (VLEDs). Generally, there is evidence that byadding drugs to dietary advice long-term weight loss can be improved [1],better than introducing physical activity and/or dietary modification.
Firstly, we shall discuss all up-to-date information on anti-obesity drugsapproved for long-term therapy (orlistat), recently withdrawn therapies
REVIEW ARTICLE
Received: 23 November 2012Revised: 1 September 2013Accepted: 13 September 2013
Copyright © 2013 John Wiley & Sons, Ltd.
DIABETES/METABOLISM RESEARCH AND REVIEWSDiabetes Metab Res Rev 2014; 30: 165–174.Published online in Wiley Online Library (wileyonlinelibrary.com) DOI: 10.1002/dmrr.2475

(sibutramine and dexfenfluramine) and drugs evaluatedin phase III studies (taranabant, combination therapiesof topiramate plus phentermine) [2] as well as on VLEDs.
Sibutramine
Usually known as sibutramine hydrochloride monohydrate,it is an orally administered agent for the treatment ofobesity and works as an appetite suppressant that reducesfood intake by triggering the physiological response ofpost-ingestive satiety. It is a novel serotonin andnoradrenaline reuptake inhibitor that does not releaseserotonin [3].
Sibutramine was widely used after its approval by theUS Food and Drug Administration (US FDA) in 1997[4,5]. Glucose utilization studies demonstrate thatsibutramine-induced thermogenesis is mediated via selec-tive sympathetic activation of brown adipose tissue, withcentrally mediated effects [6]; these dual effects ofSibutramine on food intake and thermogenesis explainits anti-obesity effect [7].
The most frequently encountered side effects ofsibutramine are headache, dry mouth, insomnia and con-stipation [8]; most importantly, however, because of theconcern over blood pressure, sibutramine was notrecommended for use in patients with coronary heart dis-ease, cardiac arrhythmias, uncontrolled hypertension,congestive heart failure or a history of stroke [9].
The Sibutramine Cardiovascular OUTcomes (SCOUT)trial – a randomized, double-blind comparison ofsibutramine versus placebo, in addition to standard carefor weight management, in overweight/obese subjectswith an increased risk of cardiovascular disease –
suggested that 6-week treatment with sibutramineappears to be efficacious, tolerable and safe in thishigh-risk population for whom sibutramine is usuallycontraindicated [10].
Nevertheless, in January 2010, a preliminary report ofthe SCOUT study, which showed that sibutramine was as-sociated with an increased risk of serious, non-fatal car-diovascular events such as myocardial infarction orstroke as compared with placebo led to the recommenda-tion to suspend the use of sibutramine by the Committeefor Medicinal Products for Human Use of the EuropeanMedicine Agency [11,12]. Sibutramine was subsequentlywithdrawn from the European market [12] and onOctober 2010 by the US FDA [13].
Orlistat
Orlistat was approved in 1998 for more than 12 weeksuse, which is considered long-term [14]. It is the first
agent in the lipase inhibitor class of anti-obesitydrugs [15]. The drug is minimally absorbed and reducesdietary fat absorption by 30% by binding to pancreaticlipase [16].
Three randomized, double-blind, placebo-controlledtrials of orlistat lasting 2 years have been published;these showed that orlistat taken with an appropriatediet resulted in clinically significant weight loss and re-duced weight regain when compared with placebo[17–19].
The XENical in the Prevention of Diabetes in ObeseSubjects Study has indicated that the additionalweight loss induced by orlistat reduced the develop-ment of type 2 diabetes by 37% during the 4-yearstudy in obese patients [20]. Overall, when comparedwith treatment with placebo and diet, orlistat wasfound to significantly reduce waist circumference, totalcholesterol, low density lipoprotein-c and blood pres-sure and to improve blood glucose levels and insulinresistance [21,22].
The most commonly experienced side effects of orlistatare gastrointestinal and include diarrhoea, flatulence,bloating, abdominal pain and dyspepsia [5,23,24]. Inaddition, long-term use of orlistat can result in adeficiency of the fat-soluble vitamins; adequate vitaminsupplementation may therefore be needed for patientson orlistat [9].
Recently, severe liver injury has been reported; thisprompted the US FDA to undertake a review of the safetyof orlistat treatment and in May 2010 led to a label revi-sion and the addition of a warning of severe liver injury[2]. It should be remembered that there are very limiteddata on the long-term effects of orlistat on cardiovascularoutcomes [9].
Dexfenfluramine
Fenfluramine and dexfenfluramine (the d-isomer offenfluramine) are serotonergic drugs, which cause therelease of serotonin to suppress appetite and reduce foodintake [25]. Dexfenfluramine has potent anti-obesityproperties in man, which persist for at least 24 weeksaccording to Finer (1989) [26].
Finer (1987) [27] suggests that dexfenfluramine has arole in the treatment of refractory obesity after a clinicallysignificant weight loss and low incidence of unwantedeffects. In a second trial, 29 patients were treated for24 weeks with dexfenfluramine; average cumulativeweight loss after 12 weeks in these patients was signifi-cantly greater than in the patients who had been treatedinitially with placebo [27]. After 24 weeks of dexfenflura-mine treatment, there was a further significant increase incumulative weight loss [27].
166 E. Koutroumanidou and O. Pagonopoulou
Copyright © 2013 John Wiley & Sons, Ltd. Diabetes Metab Res Rev 2014; 30: 165–174.DOI: 10.1002/dmrr
Although randomized controlled trials with fenfluramines(fenfluramine and dexfenfluramine), either alone[28,29] or with phentermine [30] demonstrated sig-nificant weight loss, the drugs were withdrawn fromthe market due to increased reports of valvularheart disease and primary pulmonary hypertension[4,31–35]. Dexfenfluramine was withdrawn by theUS FDA in 1997; the prevalence rates of bothvalvular heart disease and primary pulmonaryhypertension were higher following longer exposureto the fenfluramines [4].
Taranabant (MK-0557)
Taranabant is a potent, highly selective, orally bioavail-able neuropeptide Y5 receptor (NPY5R) antagonist; ithas been shown that adjunctive pharmacotherapywith dexfenfluramine or sibutramine may lessen theweight regain that is typically observed after a VLEDtherapy [36].
Weight regain after a VLED likely involves a complexinteraction of physiologic, genetic and environmentalfactors; among the important anabolic pathways thatmight be expected to favour weight regain is the cen-tral neuropeptide Y (NPY) pathway, which promotesfood intake and decreases energy expenditure. Experi-mental evidence suggests that NPY mediates its ana-bolic effects through activation of the NPY Y1 and Y5receptors (NPY1R and NPY5R), and this concept isthe basis for the idea that the antagonism of theNPY5R might prove an effective method for the treat-ment of obesity.
The overall safety and efficacy profile of taranabantfrom phase III trials did not support its further develop-ment in the treatment of obesity and clinical trials wereceased [37–39].
Topiramate
Topiramate is an anti-epileptic drug that blocks voltage-dependent sodium channels, glutamate receptors andcarbonic anhydrase and augments the activity of gammaaminobutyrate. It has been observed to significantlyreduce body weight in patients treated for seizure,forming the basis for preclinical studies to study andcharacterize its effects in the regulation of energy balance[40]. Diarrhoea and leakage were observed in early clini-cal studies [9].
The drug acts probably by inhibiting fat deposi-tion, while reducing the activity of lipoprotein lipase(LPL) in various white adipose tissue stores. It hasalso been observed to increase LPL activity in brown
adipose tissue, which could reflect its ability to en-hance regulatory thermogenesis [40]. Furthermore,topiramate stimulates LPL activity in skeletal mus-cles, which emphasizes its potential to promote sub-strate oxidation. Concerns regarding central andperipheral nervous system adverse effects led tophase III trials of topiramate being halted andreformulated; as the sustained release formulationdid not have better tolerability and because of thehigh frequency of side effects [15], trials werediscontinued in December 2004 [2].
The combination of controlled release low dosetopiramate with low dose phentermine (Qnexa) has beenshown to be effective for weight loss treatment [41].The tolerance and safety of this drug combination wasevaluated in several Phase III trials [2]. In July 2010,an FDA advisory committee agreed that the phenter-mine/topiramate combination was effective in reducingweight loss; however, it refused to endorse a recom-mendation for the treatment of obesity due to safetyconcerns, which included increased heart rate, possiblebirth defects and psychiatric problems such as depres-sion, suicidal thoughts, impaired memory and concen-tration [42]. US FDA rejected Qnexa® on October2010 [43] owing to concerns over possible birth defectsbut, on re-file, this polytherapy was FDA-approved inJuly 2012 [44].
Combination agents such as Qnexa® are designedto simultaneously target more than one biologicalmechanism and that might ultimately be more effec-tive in producing sustained weight loss and improve-ments in comorbidities; advantages of polytherapy,that is, phentermine and fenfluramine combination,include the use of lower drug doses, possiblesynergistic but at least additive weight loss, less seri-ous side effects and reduced potential for counter-regulation [45–47].
Very low energy diets (VLEDs)
In current VLEDs, usual food intake is completelyreplaced by specific foods or liquid formulas containing<800 kcal/d or less; additional intake of at least1 g/kg of ideal body weight per day of protein ofhigh biologic value appears to be important inhelping to preserve lean body mass when followinga VLED. The amount of protein provided should beat least:
• 55 g for women of small or medium height and moder-ate obesity,
• 70 g for men and for tall or massively obese women,• 100 g for massively obese men.
VLEDs Pharmacotherapy in Obesity 167
Copyright © 2013 John Wiley & Sons, Ltd. Diabetes Metab Res Rev 2014; 30: 165–174.DOI: 10.1002/dmrr
Also, for all subjects, 1.5 l water/day and supplementa-tion of minerals, vitamins and trace elements according toRecommended Daily Allowance is necessary.
Evidence from a number of reviews [1,48] clearly dem-onstrates that VLEDs can result in significant weight loss.Such interventions produce better short-term results thanprogrammes without the diet [49], with concomitant im-provement in obesity-related conditions. It has to be men-tioned though that long-term maintenance of weight losswith VLEDs is not very satisfactory [50], along with theconcerns about weight regain following these diets.
Respecting any safety concerns on VLEDs, the AmericanDietetic Association states that the use of appropriatelevels of high biologic value protein, vitamin and mineralsupplementation – as already mentioned – together withcareful monitoring has shown that the VLED can be safe[51]. Of course, potential candidates for such programmesand health professionals should realize that VLEDs are notfor everyone and can be harmful for persons who do notmeet the following selection criteria:
• At least 30% overweight, with a minimum body massindex of 32,
• Free from contraindicated medical conditions: preg-nancy or lactation, active cancer, hepatic disease, renalfailure, active cardiac dysfunction or severe psycholog-ical disturbances,
• Committed to establishing new eating and lifestyle be-haviours that will assist the maintenance of weightloss,
• Committed to taking the time to complete both thetreatment and the maintenance components of aprogramme as well as detrimental health effectsdue to the rapid weight loss these diets induce[51].
Materials and methods
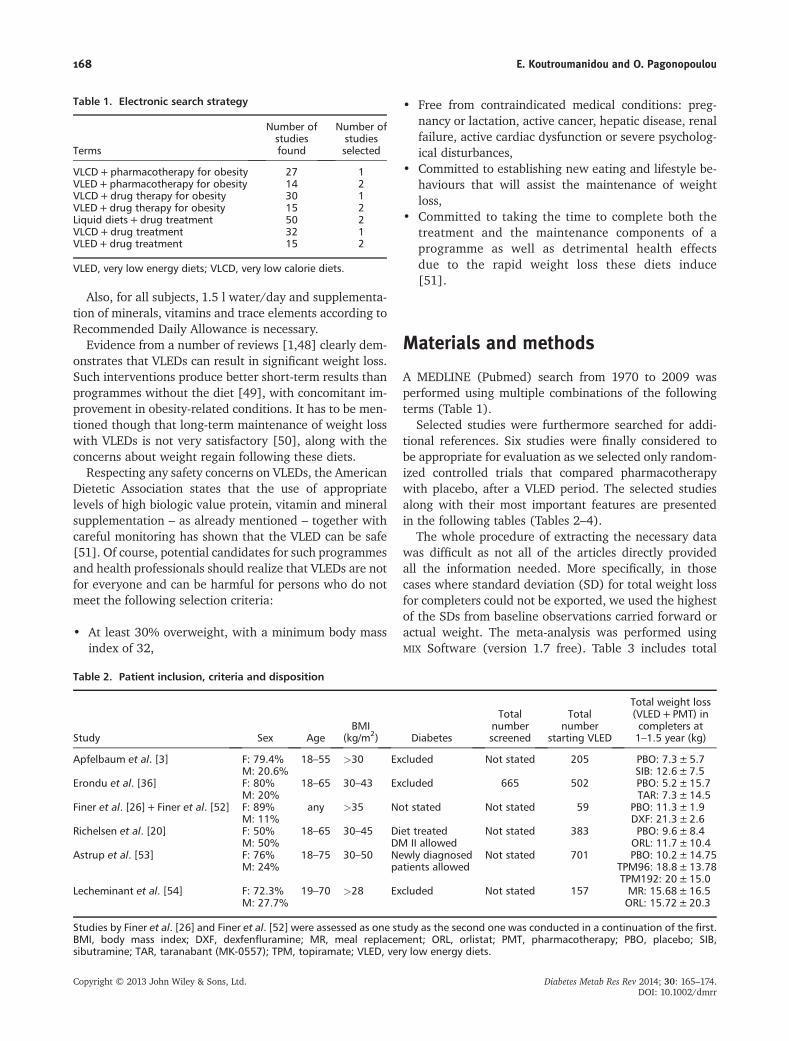
A MEDLINE (Pubmed) search from 1970 to 2009 wasperformed using multiple combinations of the followingterms (Table 1).
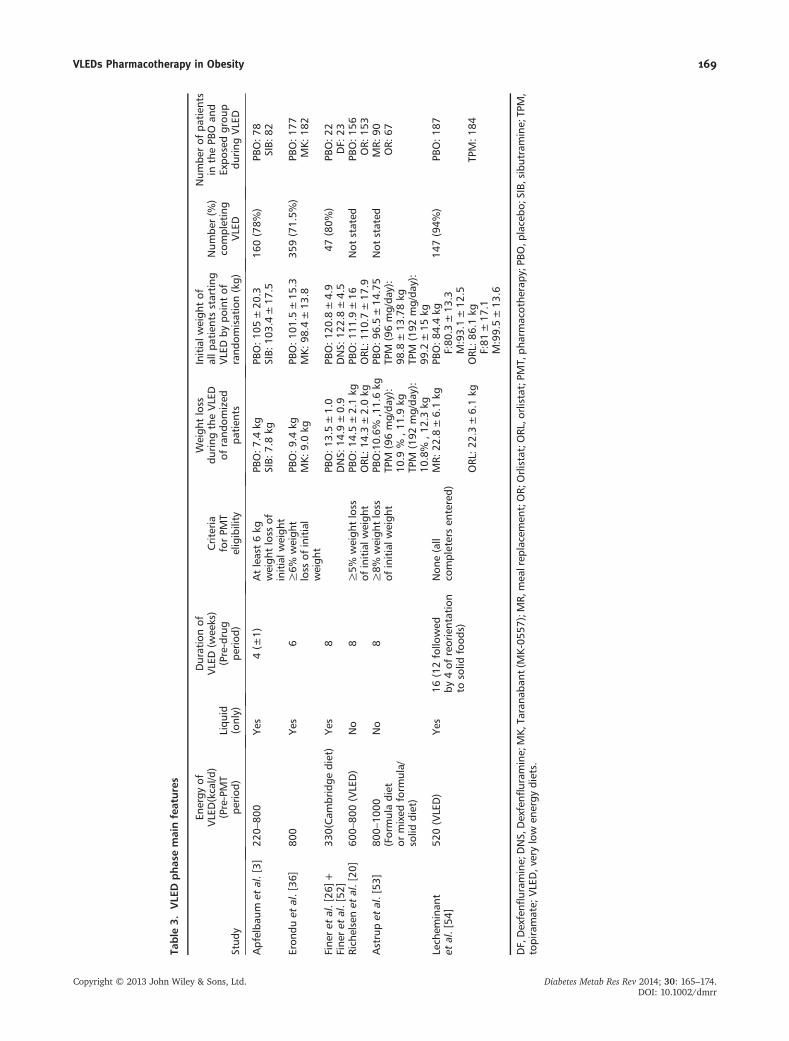
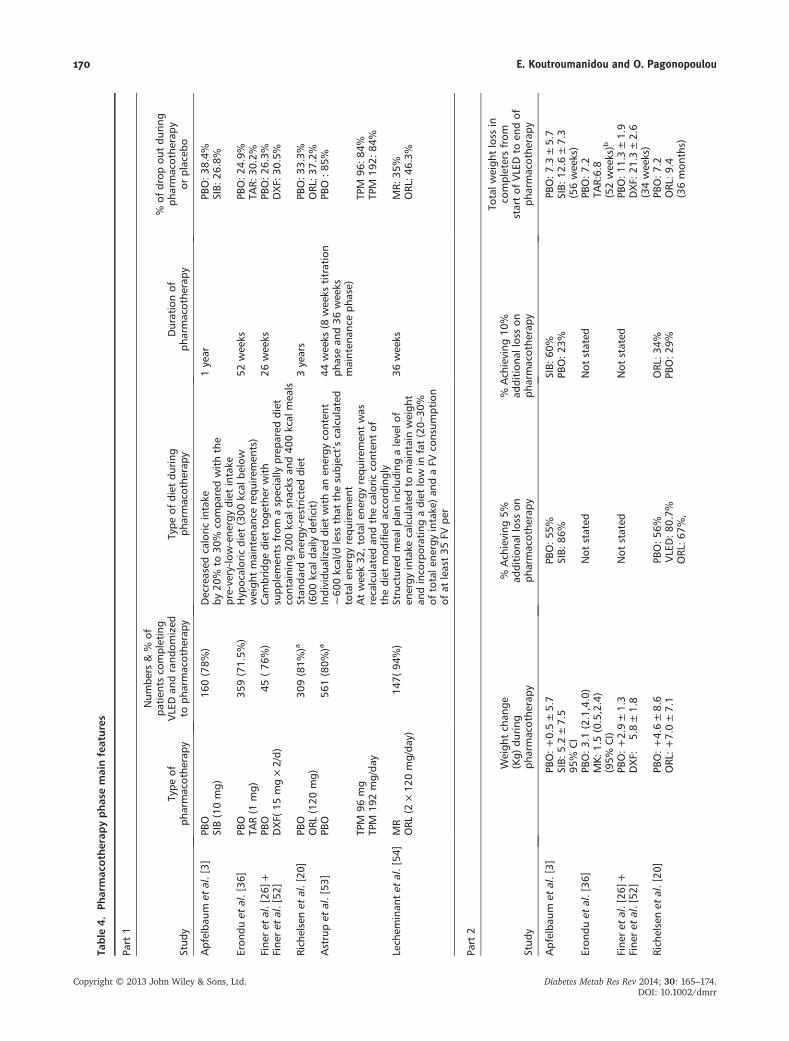
Selected studies were furthermore searched for addi-tional references. Six studies were finally considered tobe appropriate for evaluation as we selected only random-ized controlled trials that compared pharmacotherapywith placebo, after a VLED period. The selected studiesalong with their most important features are presentedin the following tables (Tables 2–4).
The whole procedure of extracting the necessary datawas difficult as not all of the articles directly providedall the information needed. More specifically, in thosecases where standard deviation (SD) for total weight lossfor completers could not be exported, we used the highestof the SDs from baseline observations carried forward oractual weight. The meta-analysis was performed usingMIX Software (version 1.7 free). Table 3 includes total
Table 1. Electronic search strategy
Terms
Number ofstudiesfound
Number ofstudiesselected
VLCD+pharmacotherapy for obesity 27 1VLED+pharmacotherapy for obesity 14 2VLCD+drug therapy for obesity 30 1VLED+drug therapy for obesity 15 2Liquid diets+drug treatment 50 2VLCD+drug treatment 32 1VLED+drug treatment 15 2
VLED, very low energy diets; VLCD, very low calorie diets.
Table 2. Patient inclusion, criteria and disposition
Study Sex AgeBMI
(kg/m2) Diabetes
Totalnumberscreened
Totalnumber
starting VLED
Total weight loss(VLED+PMT) incompleters at1–1.5 year (kg)
Apfelbaum et al. [3] F: 79.4% 18–55 >30 Excluded Not stated 205 PBO: 7.3±5.7M: 20.6% SIB: 12.6±7.5
Erondu et al. [36] F: 80% 18–65 30–43 Excluded 665 502 PBO: 5.2±15.7M: 20% TAR: 7.3±14.5
Finer et al. [26]+ Finer et al. [52] F: 89% any >35 Not stated Not stated 59 PBO: 11.3±1.9M: 11% DXF: 21.3±2.6
Richelsen et al. [20] F: 50% 18–65 30–45 Diet treatedDM II allowed
Not stated 383 PBO: 9.6±8.4M: 50% ORL: 11.7±10.4
Astrup et al. [53] F: 76% 18–75 30–50 Newly diagnosedpatients allowed
Not stated 701 PBO: 10.2±14.75M: 24% TPM96: 18.8±13.78
TPM192: 20±15.0Lecheminant et al. [54] F: 72.3% 19–70 >28 Excluded Not stated 157 MR: 15.68±16.5
M: 27.7% ORL: 15.72±20.3
Studies by Finer et al. [26] and Finer et al. [52] were assessed as one study as the second one was conducted in a continuation of the first.BMI, body mass index; DXF, dexfenfluramine; MR, meal replacement; ORL, orlistat; PMT, pharmacotherapy; PBO, placebo; SIB,sibutramine; TAR, taranabant (MK-0557); TPM, topiramate; VLED, very low energy diets.
168 E. Koutroumanidou and O. Pagonopoulou
Copyright © 2013 John Wiley & Sons, Ltd. Diabetes Metab Res Rev 2014; 30: 165–174.DOI: 10.1002/dmrr
Table
3.VLE
Dphas
emainfeatures
Stud
y
Energy
ofVLED(kcal/d
)(Pre-PMT
perio
d)Liqu
id(only)
Durationof
VLED(w
eeks)
(Pre-drug
period
)
Criteria
forPM
Teligibility
Weigh
tloss
during
theVLED
ofrand
omized
patien
ts
Initialw
eigh
tof
allp
atientsstarting
VLEDby
pointof
rand
omisation(kg)
Num
ber(%
)co
mpleting
VLED
Num
berof
patien
tsin
thePB
Oan
dExpo
sedgrou
pdu
ring
VLED
Apfelba
umet
al.[3]
220–
800
Yes
4(±
1)Atleast6kg
weigh
tloss
ofinitialw
eigh
t
PBO:7
.4kg
PBO:1
05±20
.316
0(78%
)PB
O:7
8SIB:
7.8kg
SIB:
103.4±17
.5SIB:
82
Eron
duet
al.[36
]80
0Ye
s6
≥6%
weigh
tloss
ofinitial
weigh
t
PBO:9
.4kg
PBO:1
01.5
±15
.335
9(71.5%
)PB
O:1
77MK:
9.0kg
MK:
98.4
±13
.8MK:
182
Fine
ret
al.[26
]+Fine
ret
al.[52
]33
0(Cam
bridge
diet)
Yes
8PB
O:1
3.5±1.0
PBO:1
20.8
±4.9
47(80%
)PB
O:2
2DNS:
14.9
±0.9
DNS:
122.8±4.5
DF:
23Rich
elsenet
al.[20
]60
0–80
0(VLED)
No
8≥5%
weigh
tloss
ofinitialw
eigh
tPB
O:1
4.5±2.1kg
PBO:1
11.9
±16
Not
stated
PBO:1
56ORL
:14.3±2.0kg
ORL
:110
.7±17
.9OR:
153
Astrupet
al.[53
]80
0–10
00(Formuladiet
ormixed
form
ula/
solid
diet)
No
8≥8%
weigh
tloss
ofinitialw
eigh
tPB
O:10.6%
,11.6kg
PBO:9
6.5±14
.75
Not
stated
MR:
90TP
M(96mg/da
y):
10.9
%,1
1.9kg
TPM
(96mg/da
y):
98.8
±13
.78kg
OR:
67
TPM
(192
mg/da
y):
10.8%
,12.3kg
TPM
(192
mg/da
y):
99.2
±15
kgLech
eminan
tet
al.[54
]52
0(VLED)
Yes
16(12follo
wed
by4of
reorientation
tosolid
food
s)
Non
e(all
completersen
tered)
MR:
22.8
±6.1kg
PBO:8
4.4kg
147(94%
)PB
O:1
87F:80
.3±13
.3M:93.1±12
.5ORL
:22.3±6.1kg
ORL
:86.1kg
TPM:1
84F:81
±17
.1M:99.5±13
.6
DF,Dexfenfl
uram
ine;
DNS,
Dexfenfl
uram
ine;
MK,
Tarana
bant
(MK-05
57);MR,
mea
lrep
lacemen
t;OR;
Orlistat;O
RL,o
rlistat;PM
T,ph
armacothe
rapy
;PBO
,placebo
;SIB,sibutramine;
TPM,
topiramate;
VLED,v
erylow
energy
diets.
VLEDs Pharmacotherapy in Obesity 169
Copyright © 2013 John Wiley & Sons, Ltd. Diabetes Metab Res Rev 2014; 30: 165–174.DOI: 10.1002/dmrr
Table
4.Ph
armac
oth
erap
yphas
emainfeatures
Part
1
Stud
yType
ofph
armacothe
rapy
Num
bers
&%
ofpa
tien
tsco
mpleting
VLEDan
drand
omized
toph
armacothe
rapy
Type
ofdiet
during
pharmacothe
rapy
Durationof
pharmacothe
rapy
%of
drop
outdu
ring
pharmacothe
rapy
orplaceb
o
Apfelba
umet
al.[3]
PBO
160(78%
)Decreased
caloric
intake
by20
%to
30%
compa
redwiththe
pre-very-lo
w-ene
rgydiet
intake
1year
PBO:3
8.4%
SIB(10mg)
SIB:
26.8%
Eron
duet
al.[36
]PB
O35
9(71.5%
)Hyp
ocaloric
diet
(300
kcal
below
weigh
tmainten
ance
requ
irem
ents)
52wee
ksPB
O:2
4.9%
TAR(1
mg)
TAR:
30.2%
Fine
ret
al.[26
]+Fine
ret
al.[52
]PB
O45
(76
%)
Cam
bridge
diet
toge
ther
with
supp
lemen
tsfrom
asp
ecially
prep
ared
diet
containing
200kcal
snacks
and40
0kcal
mea
ls
26wee
ksPB
O:2
6.3%
DXF(
15mg×2/d)
DXF:
30.5%
Rich
elsenet
al.[20
]PB
O30
9(81%
)aStan
dard
energy
-restricteddiet
(600
kcal
daily
deficit)
3years
PBO:3
3.3%
ORL
(120
mg)
ORL
:37.2%
Astrupet
al.[53
]PB
O56
1(80%
)aIndividu
alized
diet
withan
energy
conten
t~60
0kcal/d
less
that
thesubject’scalculated
totale
nergyrequ
irem
ent
44wee
ks(8
wee
kstitration
phasean
d36
wee
ksmainten
ance
phase)
PBO
:85%
TPM
96mg
Atwee
k32
,total
energy
requ
irem
entwas
recalculated
andthecaloric
conten
tof
thediet
mod
ified
acco
rdingly
TPM
96:8
4%TP
M19
2mg/da
yTP
M19
2:84
%
Lech
eminan
tet
al.[54
]MR
147(
94%)
Structured
mea
lplaninclud
ingalevelo
fen
ergy
intake
calculated
tomaintainweigh
tan
dinco
rporatingadiet
low
infat(20–
30%
oftotale
nergyintake
)an
daFV
consum
ption
ofat
least35
FVpe
r
36wee
ksMR:
35%
ORL
(2×12
0mg/da
y)ORL
:46.3%
Part
2
Stud
y
Weigh
tch
ange
(Kg)
during
pharmacothe
rapy
%Ach
ieving
5%ad
dition
alloss
onph
armacothe
rapy
%Ach
ieving
10%
addition
alloss
onph
armacothe
rapy
Totalw
eigh
tloss
inco
mpletersfrom
startof
VLEDto
endof
pharmacothe
rapy
Apfelba
umet
al.[3]
PBO:+
0.5±5.7
PBO:5
5%SIB:
60%
PBO:7
.3±5.7
SIB:
5.2±7.5
SIB:
86%
PBO:2
3%SIB:
12.6
±7.3
95%
CI
(56wee
ks)
Eron
duet
al.[36
]PB
O:3
.1(2.1,4.0)
Not
stated
Not
stated
PBO:7
.2MK:
1.5(0.5,2.4)
TAR:6.8
(95%
CI)
(52wee
ks)b
Fine
ret
al.[26
]+PB
O:+
2.9±1.3
Not
stated
Not
stated
PBO:1
1.3±1.9
Fine
ret
al.[52
]DXF:
�5.8
±1.8
DXF:
21.3
±2.6
(34wee
ks)
Rich
elsenet
al.[20
]PB
O:+
4.6±8.6
PBO:5
6%ORL
:34%
PBO:7
.2ORL
:+7.0±7.1
VLED:8
0.7%
PBO:2
9%ORL
:9.4
ORL
:67%
,(36mon
ths)
170 E. Koutroumanidou and O. Pagonopoulou
Copyright © 2013 John Wiley & Sons, Ltd. Diabetes Metab Res Rev 2014; 30: 165–174.DOI: 10.1002/dmrr

weight loss and SD for completers from the start of VLEDto the end of pharmacotherapy phase; these data wereused to perform the meta-analysis.
It is important to mention that exposed group ([e]) wasthe group of patients that received pharmacotherapy withthe active drug, whereas the control group ([c]) was thegroup of patients that did not receive actual drug treat-ment but placebo. Also, in all studies, there is the placeboand the drug group, apart from LeCheminant (2005) [54]where there is the meal replacement group instead of theplacebo group. Random effects was the chosen model forthe meta-analysis performance (Tables 5 and 6).
Results
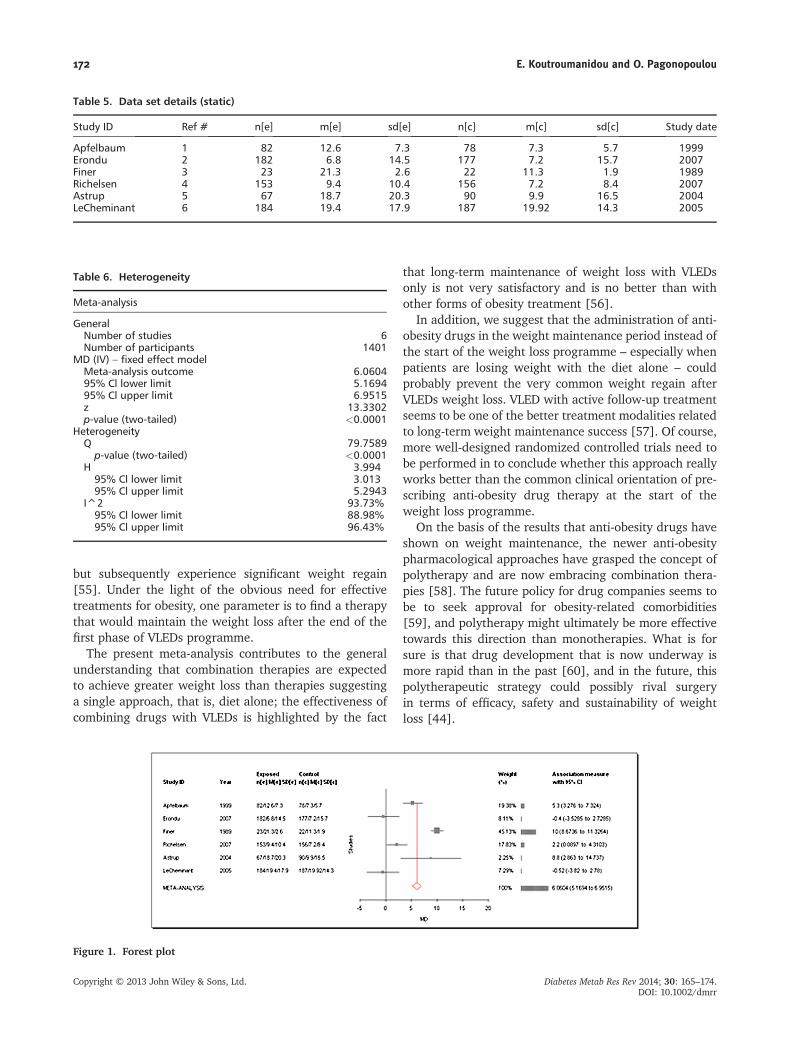
Q value from Table 2 indicates that there is heterogeneityamong the six studies but the extent of this heterogeneityis reflected on the I2 value, which is 93.73%. Besides,p-value (two-tailed) is 0.0001, which shows statisticallysignificant difference among the studies (Figure 1).
As we can see from the forest plot, four studies are locatedon the right of the zero-effect line indicating positive effect ofthe combination treatment VLED followed by pharmacother-apy. The two studies that cross the zero (black) line demon-strate negative results of the combination of VLED andpharmacotherapy. Although the examined studies were onlysix, it is obvious that the combination of VLED and pharma-cotherapy is effective for peoplewith obesity in clinical trials.
The two studies that failed to indicate a positive effectof the combination treatment on the weight loss outcomeand their basic characteristics are Erondu et al [36] andLeCheminant et al. [54] Erondu et al [36] is characterizedby 6-week VLED in the form of a liquid diet providing en-ergy of 800 kcal/day, followed by an either placebo ortaranabant pharmacotherapy phase of 52 weeks, whereasLeCheminant et al [54] includes 16 weeks on VLED(12 weeks of liquid diet providing 520 kcal/day and fourweeks on solid food) followed by an either meal replace-ment or orlistat phase of 36 weeks.
Although this ‘meta-analysis’ is not comparing multipletrials of the same drug, it does represent a synthesis of theevidence on efficacy of the paradigm of a VLED with phar-macotherapy, and the net effect of 6.1 kg placebosubtracted weight loss after 1 year represents a clinicallymeaningful result that is comparable with the effect ofdrugs given at the start of a weight loss programme.
Discussion
It is well known that individuals who lose weight usingVLEDs regimen achieve impressive short-term weight lossTa
ble
r247
5-tb
l-000
4.(continued
)
Part
1
Stud
yType
ofph
armacothe
rapy
Num
bers
&%
ofpa
tien
tsco
mpleting
VLEDan
drand
omized
toph
armacothe
rapy
Type
ofdiet
during
pharmacothe
rapy
Durationof
pharmacothe
rapy
%of
drop
outdu
ring
pharmacothe
rapy
orplaceb
o
Astrupet
al.[53
]PB
O:+
1.7
PBO:7
0%PB
O:3
5%PB
O:9
.9TP
M96
:�5.0
TPM96
:96%
TPM
96:7
8%TP
M96
:17.0
TPM
192:
�6.4
TPM19
2:97
%TP
M19
2:74
%TP
M19
2:18
.7(44wee
ks)c
Lech
eminan
tet
al.[54
]MR:
F:+2.3±5.8
Not
stated
Not
stated
MR:
F:18
.9%
(20.4±14
.3kg
)M:+
4.4±5.3
M:1
8.0%
(19.44
±14
.3kg
)ORL
:F:+
1.4±4.3
ORL
:F:1
8.7%
(20.2±17
.9)
M:+
5.7±5.1
M:1
7.3%
(18.86
±17
.9)
DXF,
dexfen
fluram
ine;
MR,
mea
lrep
lacemen
t;ORL
,orlistat;PB
O,p
lacebo
;SIB,sibutramine;
TAR,
tarana
bant
(MK-05
57);TP
M,top
iram
ate;
VLED,v
erylow
energy
diets.
a Inc
lude
sdrop
outby
VLEDan
dpa
tien
tsno
tachievingtarget
weigh
tloss.
bPe
rprotoc
olpo
pulation
.c M
odified
intentionto
trea
t,last
observationcarriedforw
ard.
VLEDs Pharmacotherapy in Obesity 171
Copyright © 2013 John Wiley & Sons, Ltd. Diabetes Metab Res Rev 2014; 30: 165–174.DOI: 10.1002/dmrr
but subsequently experience significant weight regain[55]. Under the light of the obvious need for effectivetreatments for obesity, one parameter is to find a therapythat would maintain the weight loss after the end of thefirst phase of VLEDs programme.
The present meta-analysis contributes to the generalunderstanding that combination therapies are expectedto achieve greater weight loss than therapies suggestinga single approach, that is, diet alone; the effectiveness ofcombining drugs with VLEDs is highlighted by the fact
that long-term maintenance of weight loss with VLEDsonly is not very satisfactory and is no better than withother forms of obesity treatment [56].
In addition, we suggest that the administration of anti-obesity drugs in the weight maintenance period instead ofthe start of the weight loss programme – especially whenpatients are losing weight with the diet alone – couldprobably prevent the very common weight regain afterVLEDs weight loss. VLED with active follow-up treatmentseems to be one of the better treatment modalities relatedto long-term weight maintenance success [57]. Of course,more well-designed randomized controlled trials need tobe performed in to conclude whether this approach reallyworks better than the common clinical orientation of pre-scribing anti-obesity drug therapy at the start of theweight loss programme.
On the basis of the results that anti-obesity drugs haveshown on weight maintenance, the newer anti-obesitypharmacological approaches have grasped the concept ofpolytherapy and are now embracing combination thera-pies [58]. The future policy for drug companies seems tobe to seek approval for obesity-related comorbidities[59], and polytherapy might ultimately be more effectivetowards this direction than monotherapies. What is forsure is that drug development that is now underway ismore rapid than in the past [60], and in the future, thispolytherapeutic strategy could possibly rival surgeryin terms of efficacy, safety and sustainability of weightloss [44].
Figure 1. Forest plot
Table 6. Heterogeneity
Meta-analysis
GeneralNumber of studies 6Number of participants 1401
MD (IV) – fixed effect modelMeta-analysis outcome 6.060495% Cl lower limit 5.169495% Cl upper limit 6.9515z 13.3302p-value (two-tailed) <0.0001
HeterogeneityQ 79.7589p-value (two-tailed) <0.0001
H 3.99495% Cl lower limit 3.01395% Cl upper limit 5.2943
I^2 93.73%95% Cl lower limit 88.98%95% Cl upper limit 96.43%
Table 5. Data set details (static)
Study ID Ref # n[e] m[e] sd[e] n[c] m[c] sd[c] Study date
Apfelbaum 1 82 12.6 7.3 78 7.3 5.7 1999Erondu 2 182 6.8 14.5 177 7.2 15.7 2007Finer 3 23 21.3 2.6 22 11.3 1.9 1989Richelsen 4 153 9.4 10.4 156 7.2 8.4 2007Astrup 5 67 18.7 20.3 90 9.9 16.5 2004LeCheminant 6 184 19.4 17.9 187 19.92 14.3 2005
172 E. Koutroumanidou and O. Pagonopoulou
Copyright © 2013 John Wiley & Sons, Ltd. Diabetes Metab Res Rev 2014; 30: 165–174.DOI: 10.1002/dmrr

Acknowledgements
This article is part of a 2009 project of the Clinical and PublicHealth Nutrition programme at University College London(UCL). Dr Nicolas Finer, Hon. Professor (Medicine) and Consul-tant in Endocrinology and Bariatric Medicine at UCL designedand supervised the project data of which was analysedtogether by the same and Koutroumanidou Eleni (MSc). Thepresent article was withdrawn from the project and written
by Eleni Koutroumanidou (MSc) under the guidelines of DrOlga Pagonopoulou.
Conflict of interest
None declared.
References
1. Avenell A, Broom J, Brown TJ, et al.Systematic review of the long-termeffects and economic consequences oftreatments for obesity and implic-ations for health improvement.Health Technol Assess 2004; 8(21):iii–iv, 1–182.
2. Ioannides-Demos LL, Piccenna L, McNeilJJ. Pharmacotherapies for obesity: past,current and future therapies. J Obes2011; 179674.
3. Apfelbaum M, Vague P, Ziegler O, et al.Long-term maintenance of weight lossafter a very-low-calorie diet: a random-ized blinded trial of the efficacy andtolerability of sibutramine. Am J Med1999; 106: 179–184.
4. Ioannides-Demos LL, Proietto J, TonkinAM, McNeil JJ. Safety of drug therapiesused for weight loss and treatment ofobesity. Drug Saf 2006; 29(4): 277–302.
5. Li M-F, Bernard MYC. Pharmacotherapyfor obesity. Br J Clin Pharmacol 2009;68(6): 804–810.
6. Heal DJ, Aspley S, Prow MR, et al.Sibutramine: a novel anti-obesity drug. Areview of the pharmacological evidenceto differentiate it from d-amphetamineand d-fenfluramine. Int J Obes 1999;22(suppl 1): S18–S28.
7. Stock MJ. Sibutramine: a review of thepharmacology of a new anti-obesityagent. Int J Obes 1997; 21(suppl 1):S25–S29.
8. Nisoli E, Carruba MO. A benefit-risk as-sessment of sibutramine in the manage-ment of obesity. Drug Saf 2003;26(14): 1027–1048.
9. Li M-F, Bernard MYC. Rise and fall ofanti-obesity drugs. World J Diabetes2011; 2(2): 19–23.
10. Torp-Pedersen C, Caterson I, CoutinhoW, et al. Cardiovascular responses toweight management and sibutramine inhigh-risk subjects: an analysis from theSCOUT trial. Eur Heart J 2007; 28:2915–2923.
11. Early communication about an ongoingsafety review of sibutramine, marketedas meridia. Available from: http://www.fda.gov/Drugs/DrugSafety/Postmarket-DrugSafetyInformationforPatientsandP-roviders/DrugSafetyInformationforHeath-care Professionals /ucm198206. htm[Accessed August 2013]
12. European Medicines Agency recom-mends suspension of marketingauthorisations for sibutramine. Pressrelease of the European MedicinesAgency, 2010; Available from: http://www.emea.europa.eu/ema/ index. jsp?curl=pages/news_and_events/news/2010/01/news_detail_000985.jsp [AccessedAugust, 2013]
13. FDA drug safety communication: FDA rec-ommends against the continued use ofmeridia (sibutramine). U.S. Food andDrugAdministration, 2010; Available from:http://www.fda.gov/Drugs/DrugSafety/Drug Safety Podcasts /ucm229245. htm[Accessed August, 2013]
14. Glandt M, Raz I. Present and future:pharmacologic treatment of obesity. JObes 2011; 636181. [Epub 2011 Feb 8]
15. Lucas KH, Kaplan-Machlis B. Orlistat-anovel weight loss therapy. AnnPharmacother 2001; 35(3): 314–328.
16. Raj P, Sumit RM. Drug treatments forobesity: orlistat, sibutramine, andrimonabant. Lancet 2007; 369: 71–77.
17. Jonathan H, Charles L, Mark NB, HarryC, Karen RS. Orlistat in the long-termtreatment of obesity in primary care set-tings. Arch Fam Med 2000; 9: 160–167.
18. Sjöström L, Rissanen A, Andersen T,et al. Randomised placebo-controlledtrial of orlistat for weight loss and pre-vention of weight regain in obese pa-tients. Lancet 1998; 352: 167–173.
19. Davidson MH, Hauptman J, DiGirolamoM, et al. Weight control and risk factorreduction in obese subjects treated for2 years with orlistat: a randomizedcontrolled trial. JAMA 1999; 281(3):235–242.
20. Richelsen B, Tonstad S, Rossner S, et al.Effect of orlistat on weight regain andcardiovascular risk factors following avery-low-energy diet in abdominallyobese patients - a 3-year randomized,placebo-controlled study. Diabetes Care2007; 30: 27–32.
21. Jarl S, Torgerson JS, Hauptman J,Boldrin MN, Sjöström L. XENical in thePrevention of Diabetes in Obese Subjects(XENDOS) Study. Diabetes Care 2004;27: 155–161.
22. Schneider R, Golzman B, Turkot S,Kogan J, Oren S. Effect of weight losson blood pressure, arterial compliance,
and insulin resistance in normotensiveobese subjects. Am J Med Sci 2005;330(4): 157–160.
23. Siebenhofer A, Horvath K, Jeitler K,et al. Long-term effects of weight-reducing drugs in hypertensive patients(Review). Cochrane Database Syst Rev2009; (3): CD007654.
24. Padwal R, Li SK, Lau DCW. Long-termpharmacotherapy for overweight andobesity: a systematic review andmeta-analysis of randomized controlledtrials. Int J Obes Relat Metab Disord2003; 27(12): 1437–1446.
25. Connolly HM, Jl C, McGoon MD, et al.Valvular heart disease associated withfenfluramine–Phentermine. N Eng JMed 1997; 337(9): 581–588.
26. Finer N, Finer S,NaoumovaRP. Prolongeduse of a very low calorie diet (Cambridgediet) in massively obese patients attend-ing an obesity clinic: safety, efficacy andadditional benefit from dexfenfluramine.Int J Obes 1989; 13(suppl. 2): 91–93.
27. Finer N, Craddock D, Lavielle R, Keen H.Prolonged weight loss with dexfenflura-mine treatment in obese patients.Diabete Metab 1987; 13(6): 598–602.
28. Guy-Grand B, Apfelbaum M, Crepaldi G,et al. International trial of long-termdexfenfluramine in obesity. Lancet1989; 2(8672): 1142–1145.
29. Mathus-Vliegen EM, van de Voorde K,Kok AM, Res AM. Dexfenfluramine inthe treatment of severe obesity: aplacebo-controlled investigation of theeffects onweight loss, cardiovascular riskfactors, food intake and eating behaviour.J Intern Med 1992; 232(2): 119–127.
30. Weintraub M. Long-term weight control:the national heart, lung, and blood insti-tute funded multimodal interventionstudy. Clin Pharmacol Ther 1992; 51(5):581–585.
31. Abenhaim L, Moride Y, Brenot F, et al.Appetite-suppressant drugs and the riskof primary pulmonary hypertension. NEng J Med 1996; 335(9): 609–616.
32. Griffen L, Anchors M. The “phen-pro”diet drug combination is not associatedwith valvular heart disease. Arch InternMed 1998; 158(11): 1278–1279.
33. Centers for Disease Control and Preven-tion (CDC). Cardiac valvulopathy associ-ated with exposure to fenfluramine or
VLEDs Pharmacotherapy in Obesity 173
Copyright © 2013 John Wiley & Sons, Ltd. Diabetes Metab Res Rev 2014; 30: 165–174.DOI: 10.1002/dmrr

dexfenfluramine: U.S. Department ofHealth and Human Services interimpublic health recommendations. MMWRMorb Mortal Wkly Rep 1997; 46(45):1061–1066.
34. Curfman GD. Diet pills redux. N Engl JMed 1997; 337: 629–630.
35. DelcroixM, Kurz X,Walckiers D, DemedtsM, Naeije R. High incidence of primarypulmonary hypertension associated withappetite suppressants in Belgium. EurRespir J 1998; 12: 271–276.
36. Erondu N, Wadden T, Gantz I, et al.Effect of NPY5R antagonist MK-0557on weight regain after very-low-caloriediet-induced weight loss. Obesity (SilverSpring) 2007; 15(4): 895–905.
37. Aronne LJ, Tonstad S, Moreno M, et al. Aclinical trial assessing the safety and effi-cacy of taranabant, a CB1R inverse ago-nist, in obese and overweight patients:a high-dose study. Int J Obes (Lond)2010; 34(5): 919–935.
38. Kipnes MS, Hollander P, Fujioka K,et al. A one-year study to assess thesafety and efficacy of the CB1R inverseagonist taranabant in overweight andobese patients with type 2 Diabetes. Di-abetes Obes Metab 2009; 12: 517–531.
39. Koch L. Obesity: taranabant no longerdeveloped as an antiobesity agent. NatRev Endocrinol 2010; 6(6): 300.
40. Richard D, Ferland J, Lalonde J, SamsonP, Deshaies Y. Influence of topiramate inthe regulation of energy balance. Nutri-tion 2000; 16: 961–966.
41. Kaplan LM. Pharmacologic therapies forobesity. Gastroenterol Clin North Am2010; 39(1): 69–79.
42. Pollack A. Diet drug wins panel’s ap-proval. The New York Times, 2010.
Available from: http://www.nytimes.com/2012/05/11/health/ diet- drug-wins-approval-of-fda-advisers.html?_r=0[Accessed August, 2013]
43. Pollack A. FDA rejects Qnexa, a thirdweight-loss drug. The New York Times,2010. Available from: http://www.nytimes.com/2010/10/29/health/ policy/ 29drug. html?pagewanted=all [AccessedAugust, 2013]
44. Rodgers RJ, Tschöp MH, Wilding JPH.Anti-obesity drugs: past, present andfuture. Dis Model Mech 2012; 5(5):621–626. doi:10.1242/dmm.009621.
45. Greenway FL, Whitehouse MJ,Guttadauria M, et al. Rational design ofa combination medication for thetreatment of obesity. Obesity 2009; 17:30–39.
46. Padwal R. Contrave, a bupropion andnaltrexone combination therapy for thepotential treatment of obesity. Curr OpinInvest Drugs 2009; 10: 1117–1125.
47. Roth JD, Trevaskis JL, Turek VF, ParkesDG. ‘Weighing in’ on synergy: preclinicalresearch on neurohumoral anti-obesitycombinations. Brain Res 2010; 1350:86–94.
48. Wadden TA. Treatment of obesity bymoderate and severe caloric restriction.Results of clinical research trials.Ann Intern Med 1993; 119(7 Pt 2):688–693.
49. Mustajoki P, Pekkarinen T. Very lowenergy diets in the treatment of obesity.The International Association forthe study of Obesity. Obes Rev 2001;2(1): 61–72.
50. National Task Force on the Preventionand Treatment of Obesity. Very low calo-rie diets. JAMA 1993; 270(8): 967–974.
51. Position of the American Dietetic Asso-ciation: very-low-calorie weight lossdiets. J Am Diet Assoc 1990; 90(5):722–726.
52. Finer N. Body weight evolution duringdexfenfluramine treatment after initialweight control. Int J Obes Relat MetabDisord 1992; 16(Suppl 3): S25–S29.
53. Astrup A, Caterson I, Zelissen P, et al.Topiramate: long-term maintenance ofweight loss induced by a low-calorie dietin obese subjects.Obes Res 2004; 12(10):1658–1669.
54. LeCheminant JD, Jacobsen DJ, Hall MA,Donnelly JE. A comparison of meal re-placements and medication in weightmaintenance after weight loss. J Am CollNutr 2005; 24(5): 347–353.
55. Marinilli PA, Gorin AA, Raynor HA, TateDF, Fava JL, Wing RR. Successful weightloss maintenance in relation to methodof weight loss. Obesity 2008; 16:2456–2461.
56. National Task Force on the Preventionand Treatment of Obesity, National In-stitutes of Health. Very low-calorie diets.JAMA 1993; 270(8): 967–974.
57. Saris WH. Very-low-calorie diets andsustained weight loss. Obes Res 2001;9(Suppl 4): 295S–301S.
58. Kushner RF. Pharmacologic manage-ment of obesity. Pediatr Blood Cancer2012; 58: 140–143.
59. Aronne LJ, Powell AG, Apovian CM.Emerging pharmacotherapy for obesity.Expert Opin Emerg Drugs 2011; 16(3):587–596. DOI: 10.1517/14728214.2011.609168 [Epub 2011 Aug 12]
60. Bray GA. Medications for weight reduc-tion. Med Clin North Am 2011; 95(5):989–1008.
174 E. Koutroumanidou and O. Pagonopoulou
Copyright © 2013 John Wiley & Sons, Ltd. Diabetes Metab Res Rev 2014; 30: 165–174.DOI: 10.1002/dmrr





























