Embed Size (px)
Citation preview
Combating Antimicrobial Resistance with Extended Infusion Beta-lactamsStephen Andrews, PharmDPGY-1 Pharmacy Practice Resident
Disclosure• The presenter has no conflicts of interest to
disclose with material in this presentation.
4/3/2017 2

Objectives• Review pharmacokinetic and pharmacodynamic
(PK/PD) properties of beta-lactam antibiotics
• Evaluate the literature for using extended infusion beta-lactam antibiotics
• Determine candidates for extended infusion beta-lactam therapy
• Identify obstacles in administering extended infusion beta-lactam therapy
4/3/2017 3

No Longer a Threat: Reality of Resistance
• “Pan-Resistant New Delhi Metallo-Beta-Lactamase-Producing Klebsiella pneumoniae” -Washoe County, Nevada– Resistant to 26 antibiotics
• 10-50% of patients treated for nosocomial pneumonia develop antimicrobial resistance
• No new classes of antibiotics since the 1980s
4/3/2017 4Asin-Prieto E, et al. J Infect Chemother 2015;21:319-329Bao H, et al. Eur J Clin Microbiol Infect Dis. 2017;36(3):459-466MMWR Morb Mortal Wkly Rep 2017:66:33

Isolate Susceptibility – Antibiogram 2015Piperacillin-tazobactam
Cefepime Ertapenem Meropenem
P. aeruginosa(n=1,065)
66% 77% -- 66%
E. coli(n=3,481)
96% 91% 100% 100%
K. pneumoniae(n=881)
95% 99% 100% --
A. baumanii(n=119)
42% 69% -- 79%
4/3/2017 5The University of Kansas Health System, Clinical Lab

Outline• Common PK/PD parameters
• Monte Carlo simulations
• Literature evaluation
• Practical considerations
4/3/2017 6

Time-Dependent (Time > MIC)
• Longer duration of exposure above the MIC results in greater bactericidal activity– Beta-lactam antibiotics
4/3/2017 7MIC: Minimum Inhibitory ConcentrationCraig WA. Clin Infect Dis. 1998 Jan;26(1):1-10

Concentration-Dependent (Peak / MIC)
• Higher concentrations result in greater bactericidal activity– Aminoglycosides
4/3/2017 8MIC: Minimal inhibitory concentrationCraig WA. Clin Infect Dis. 1998 Jan;26(1):1-10
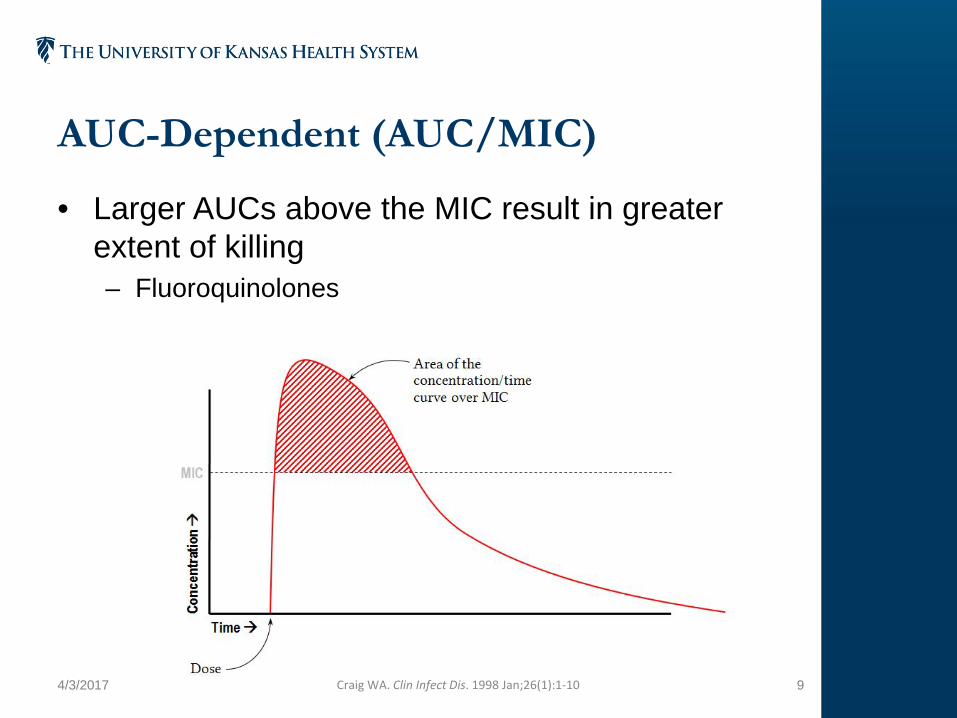
AUC-Dependent (AUC/MIC)
• Larger AUCs above the MIC result in greater extent of killing– Fluoroquinolones
4/3/2017 9Craig WA. Clin Infect Dis. 1998 Jan;26(1):1-10

Beta-lactams: Time-Dependent• Approved dosing regimens occurred before robust
PK / PD studies
• Bactericidal response is predicted by the amount of time above the MIC
• Regrowth occurs rapidly when concentrations are below MIC between administrations– Chance for resistance increases
4/3/2017 10Osthoff M, et al. Swiss Med Wkly. 2016;146:w14368Craig WA. Clin Infect Dis. 1998 Jan;26(1):1-10
Options for Increasing Time above MIC
• Option 1: Increase the dose– Increases risk of concentration-dependent toxicities
• Option 2: Extend the infusion time
4/3/2017 11Craig WA. Clin Infect Dis. 1998 Jan;26(1):1-10
Duration Above MIC is Drug-Specific
• Optimal time above MIC by drug class– Carbapenems: 30-60%– Cephalosporins: 60-70%– Penicillins: 50-60%
• PK / PD parameters initially studied in neutropenic animal models
• Validated in healthy adults
4/3/2017 12Craig WA. Clin Infect Dis. 1998 Jan;26(1):1-10Drusano G. Clin Infect Dis. 2003;36:S42-50Drusano G. Nat Rev Microbiol. 2004;2:289-300
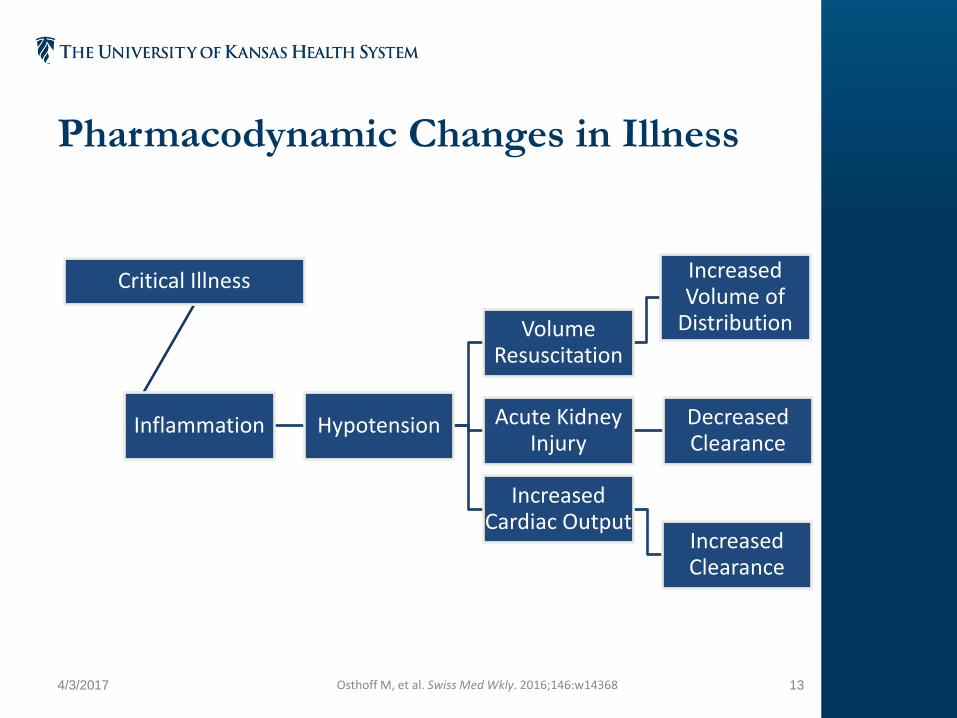
Pharmacodynamic Changes in Illness
4/3/2017 13Osthoff M, et al. Swiss Med Wkly. 2016;146:w14368
Critical Illness
Inflammation Hypotension
Volume Resuscitation
Increased Volume of
Distribution
Acute Kidney Injury
Decreased Clearance
Increased Cardiac Output
Increased Clearance
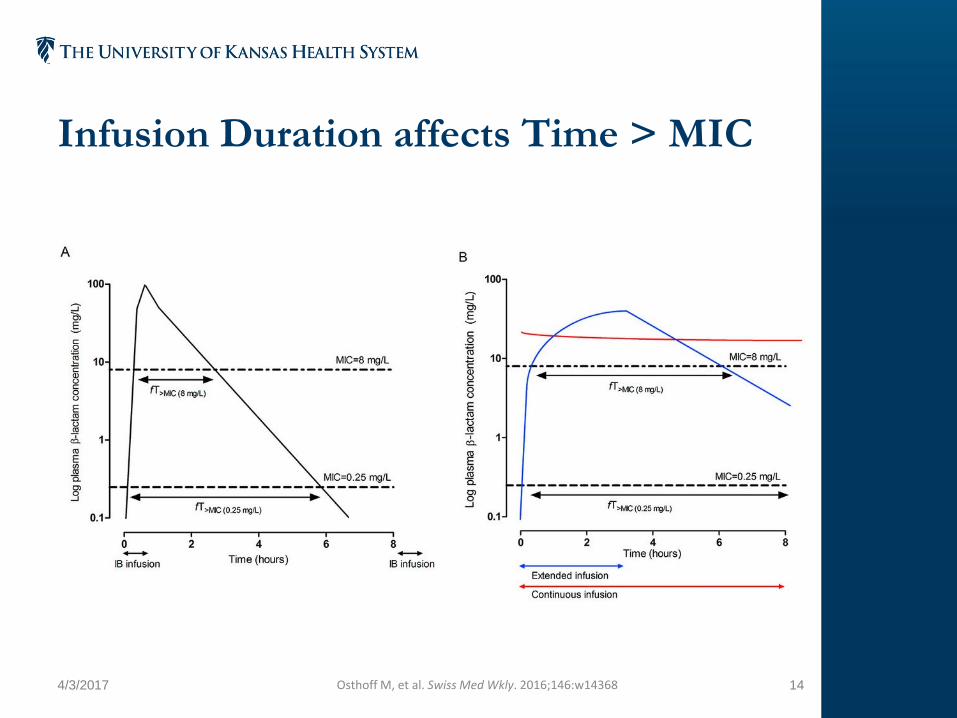
Infusion Duration affects Time > MIC
4/3/2017 14Osthoff M, et al. Swiss Med Wkly. 2016;146:w14368

Therapeutic Drug Monitoring• Not routine practice for beta-lactams
• Monte Carlo simulations used to determine optimal dosing strategies
• Statistical model to predict achievement of a PK / PD target– Probability of target attainment– Cumulative fraction of response
4/3/2017 15Asin-Prieto E, et al. J Infect Chemother 2015;21:319-29Mouton JW, et al. J Antimicrob Chemother 2005;55:601-7

Review Question 1• Which of the following describes the PK / PD
parameter for beta-lactam antibiotics?
A. Concentration / MIC
B. Time / MIC
C. AUC / MIC
4/3/2017 16

What is the clinical evidence supporting extended infusion beta-lactam antibiotics?
4/3/2017 17

Extended Infusion vs. Traditional Dosing Piperacillin-tazobactam with P. aeruginosa
Objective
• Evaluate efficacy of extended infusion piperacillin-tazobactam vs. traditional dosing for P. aeruginosa infections
Outcomes
• 14-day Mortality• Length of Hospital Stay
Dosing
• Extended Infusion: 3.375g q8h over 4 hours• Traditional: 3.375g q6h over 30 minutes
4/3/2017 18EI: Extended InfusionLodise TP, et al. CID 2007;44:357-63

Extended Infusion vs. Traditional Dosing Piperacillin-tazobactam with P. aeruginosa
Inclusion Criteria
• Adults with confirmed P. aeruginosa infections• Absolute neutrophil count >1000• Piperacillin-tazobactam given within 72 hours of
infection and continued at least 48 hours• ICU and floor patients
Exclusion Criteria
• > 1 day of traditional dosing before extended infusion• Reported resistance• Dialysis, cystic fibrosis, solid organ or bone marrow
transplant patients • Beta-lactam therapy within 5 days of initiation of
piperacillin-tazobactam
4/3/2017 19Lodise TP, et al. CID 2007;44:357-63

Study Design• Single-center, retrospective cohort study
• No loading dose reported– Loading dose: same dose given as an intermittent
infusion prior to beginning extended infusion
4/3/2017 20Lodise TP, et al. CID 2007;44:357-63

Justification of Dosing Strategy• High probability of achieving piperacillin
concentrations above MIC for 50% of dosing interval (50% ƒT>MIC)
4/3/2017 21Lodise TP, et al. CID 2007;44:357-63

Patient Characteristics
Source of Infection Extended(n = 102)
Intermittent(n = 92) P - value
Pulmonary (%) 55 (53.9) 48 (52.2) 0.8
Intra-abdominal (%) 4 (3.9) 1 (1.1) 0.2
Urinary (%) 21 (20.6) 12 (13) 0.2
Skin & soft tissue (%) 11 (10.8) 23 (25) 0.009
Bloodstream (%) 3 (2.9) 0 (0) 0.1
Other (%) 8 (7.8) 8 (8.7) 0.8
4/3/2017 22Lodise TP, et al. CID 2007;44:357-63
• 126 patients (64.9%) in the ICU when therapy started
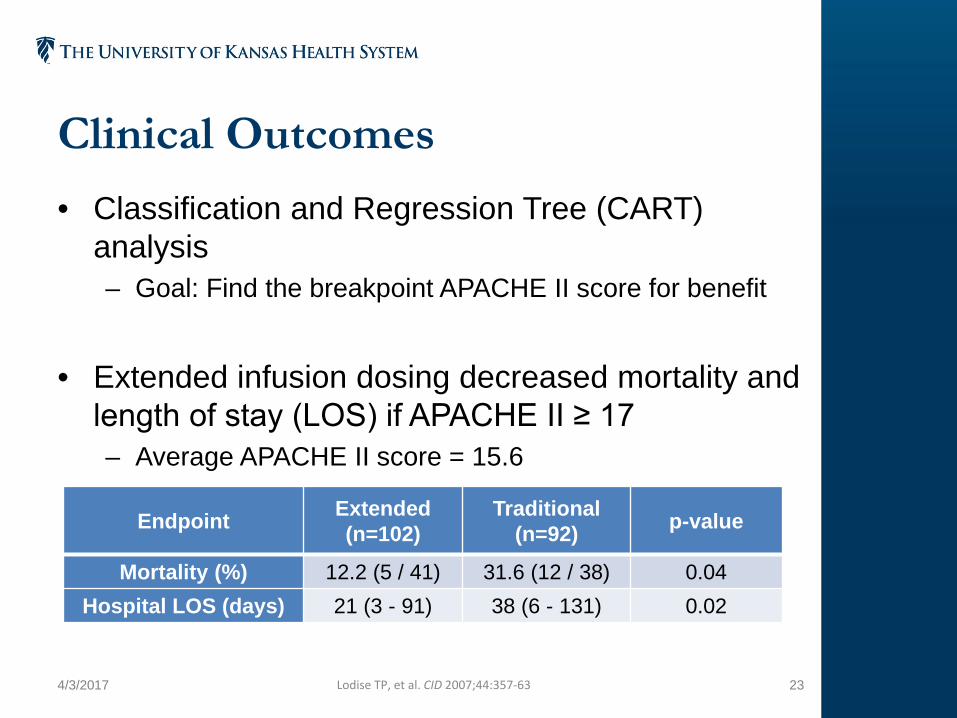
Clinical Outcomes• Classification and Regression Tree (CART)
analysis– Goal: Find the breakpoint APACHE II score for benefit
• Extended infusion dosing decreased mortality and length of stay (LOS) if APACHE II ≥ 17– Average APACHE II score = 15.6
4/3/2017 23
Endpoint Extended(n=102)
Traditional(n=92) p-value
Mortality (%) 12.2 (5 / 41) 31.6 (12 / 38) 0.04Hospital LOS (days) 21 (3 - 91) 38 (6 - 131) 0.02
Lodise TP, et al. CID 2007;44:357-63

Limitations• Retrospective study design
• Potentially suboptimal dose for P. aeruginosa in traditional infusion group
• Only P. aeruginosa confirmed infections
• No MIC data available
• Variable indications for treatment
• No subgroup analysis based on infection source
4/3/2017 24Lodise TP, et al. CID 2007;44:357-63

Unanswered Questions• Does the benefit of extended infusion apply to all
gram-negative pathogens or only Pseudomonas ?
• Should the MIC dictate whether extended infusions are necessary?
• Do extended infusion beta lactam dosing strategies improve mortality outcomes beyond 14 days?
4/3/2017 25

Extended Infusion vs. Traditional Dosing with Gram-negative Infections
Objective
• Evaluate efficacy of extended infusion piperacillin-tazobactam vs. traditional dosing for gram-negative infections
Outcomes
• 30-day Mortality• Length of Hospital Stay• Results stratified by MIC: <8, 8 to 16, >16 mg/L
Dosing
• Extended Infusion: 3.375g q8h over 4 hours• Traditional: 3.375g to 4.5g q6-8h over 30 minutes
4/3/2017 26Patel GW, et al. Diagnostic Microbiology and Infectious Disease 64 (2009) 236-240

Extended Infusion vs. Traditional Dosing with Gram-negative Infections
Inclusion Criteria
• Age 18 or older, ANC ≥1000• Confirmed infection with gram-negative pathogen• Piperacillin-tazobactam given within 72 hours of
infection continued at least 48 hours
Exclusion Criteria
• >1 day of traditional piperacillin-tazobactam before EI• Reported resistance• Dialysis, cystic fibrosis, solid organ or bone marrow
transplant patients• Concurrent beta-lactam therapy within 5 days of
initiation of piperacillin-tazobactam
4/3/2017 27Patel GW, et al. Diagnostic Microbiology and Infectious Disease 64 (2009) 236-240

Study Design• Retrospective, multisite cohort study
• Power not set
4/3/2017 28Patel GW, et al. Diagnostic Microbiology and Infectious Disease 64 (2009) 236-240

Patient Characteristics
4/3/2017 29
Source of Infection Extended(n=70)
Intermittent(n=59)
Pulmonary (%) 17 (20.4) 20 (33.9)Intra-abdominal (%) 9 (12.9) 10 (16.9)Urinary (%) 27 (38.6) 18 (30.5)Skin & soft tissue infection (%) 10 (14.3) 10 (16.9)Bloodstream (%) 4 (5.7) 1 (1.7)Other (%) 3 (4.3) 0(0)
Organisms Present(>10% frequency)
Extended(n=70)
Intermittent(n=59)
Escherichia coli 27 (28.6) 23 (39)Psuedomonas aeruginosa 14 (20) 14 (23.7)Klebsiella pneumoniae 14 (20) 12 (20.3)Proteus spp. 3 (4.3) 13 (22)
Patel GW, et al. Diagnostic Microbiology and Infectious Disease 64 (2009) 236-240
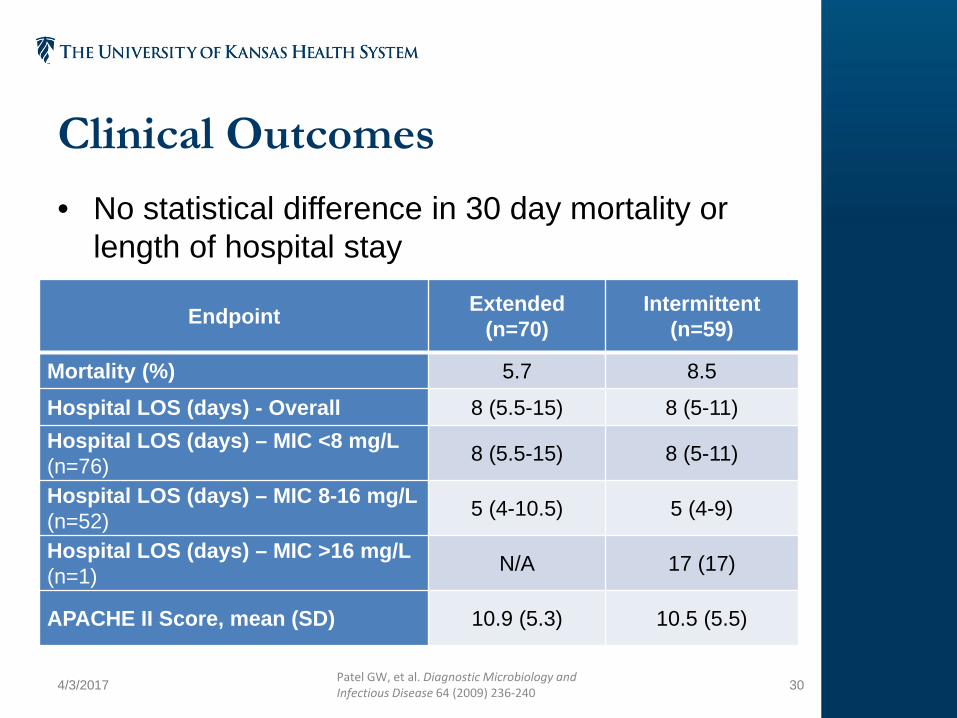
Clinical Outcomes• No statistical difference in 30 day mortality or
length of hospital stay
4/3/2017 30
Endpoint Extended(n=70)
Intermittent(n=59)
Mortality (%) 5.7 8.5
Hospital LOS (days) - Overall 8 (5.5-15) 8 (5-11)Hospital LOS (days) – MIC <8 mg/L(n=76) 8 (5.5-15) 8 (5-11)
Hospital LOS (days) – MIC 8-16 mg/L(n=52) 5 (4-10.5) 5 (4-9)
Hospital LOS (days) – MIC >16 mg/L(n=1) N/A 17 (17)
APACHE II Score, mean (SD) 10.9 (5.3) 10.5 (5.5)
Patel GW, et al. Diagnostic Microbiology and Infectious Disease 64 (2009) 236-240

Why did the study fail to find benefit in using extended infusions?• Smaller study size (n=129)
• 43% of patients in traditional dosing group had a CrCl <40 mL/min
• 59% of patients in traditional dosing had MIC <8 mg/L
• 35% of patients had a urinary infection
4/3/2017 31Patel GW, et al. Diagnostic Microbiology and Infectious Disease 64 (2009) 236-240
Summary• More likely to benefit:
– Pseudomonal strains– Pulmonary source of infection– APACHE II ≥ 17
• Less likely to benefit:– Gram-negative infections with lower MICs– Patients with urinary tract infections
• Does this phenomenon hold up when compared to all beta-lactams with similar spectrums?
4/3/2017 32
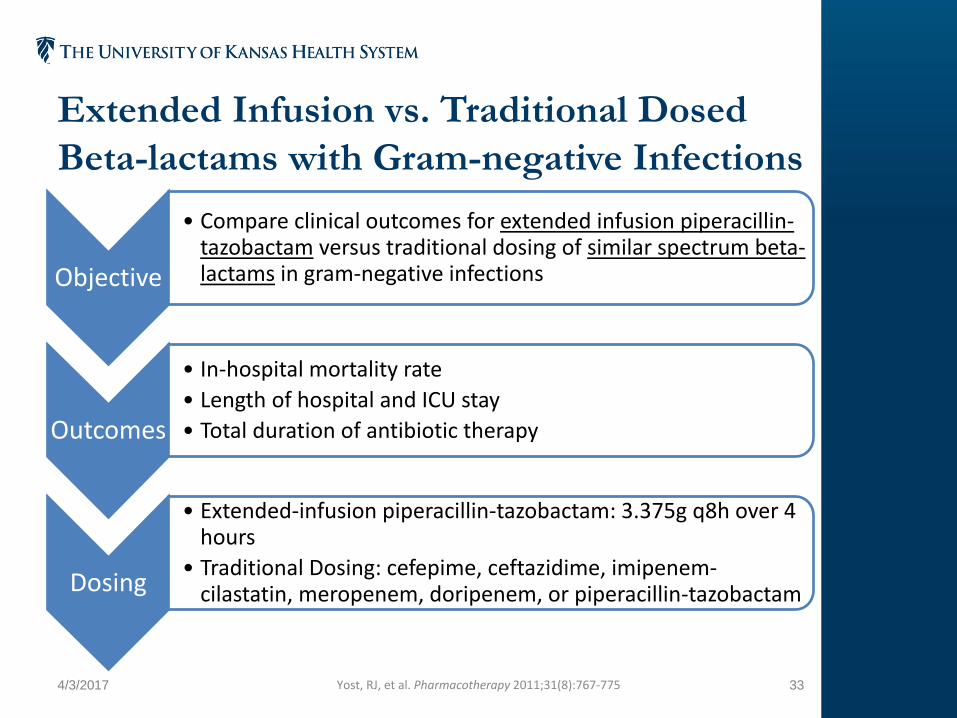
Extended Infusion vs. Traditional Dosed Beta-lactams with Gram-negative Infections
Objective
• Compare clinical outcomes for extended infusion piperacillin-tazobactam versus traditional dosing of similar spectrum beta-lactams in gram-negative infections
Outcomes
• In-hospital mortality rate• Length of hospital and ICU stay• Total duration of antibiotic therapy
Dosing
• Extended-infusion piperacillin-tazobactam: 3.375g q8h over 4 hours
• Traditional Dosing: cefepime, ceftazidime, imipenem-cilastatin, meropenem, doripenem, or piperacillin-tazobactam
4/3/2017 33Yost, RJ, et al. Pharmacotherapy 2011;31(8):767-775

Extended Infusion vs. Traditional Dosed Beta-lactams with Gram-negative Infections
Inclusion Criteria
• Adults with confirmed gram-negative infections• Mixed infections were allowed
• Patients hospitalized for >72 hours• Antibiotics given for >48 hours
Exclusion Criteria
• >1 day of traditional piperacillin-tazobactam before extended infusion
• Intermediate or resistant to initial therapy• Concomitant beta-lactam therapy• Gram-positive or fungal coverage was inappropriate
4/3/2017 34Yost, RJ, et al. Pharmacotherapy 2011;31(8):767-775
Study Design
• Multicenter, retrospective study
• Included a multivariate analysis
4/3/2017 35

Clinical Outcomes
• Extended infusion piperacillin-tazobactamreduced in-hospital mortality
• No difference in antibiotic duration, hospital or ICU length of stay
4/3/2017 36
Endpoint Extended(n=186)
Intermittent(n=173) p-value
Mortality (%) 9.7% 17.9% 0.02
Yost, RJ, et al. Pharmacotherapy 2011;31(8):767-775
Multivariate Endpoint Odds Ratio 95% CI p-value
Mortality 0.22 0.07-0.76 0.053
Survival (days) 2.77 0.85-4.7 <0.01
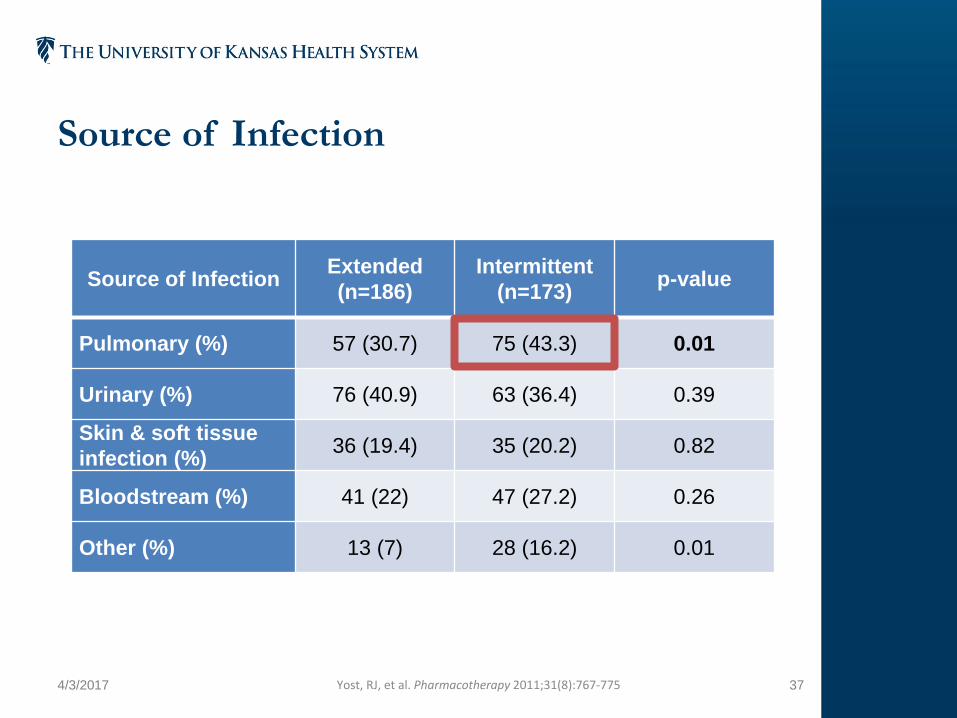
Source of Infection
4/3/2017 37
Source of Infection Extended(n=186)
Intermittent(n=173) p-value
Pulmonary (%) 57 (30.7) 75 (43.3) 0.01
Urinary (%) 76 (40.9) 63 (36.4) 0.39
Skin & soft tissue infection (%) 36 (19.4) 35 (20.2) 0.82
Bloodstream (%) 41 (22) 47 (27.2) 0.26
Other (%) 13 (7) 28 (16.2) 0.01
Yost, RJ, et al. Pharmacotherapy 2011;31(8):767-775
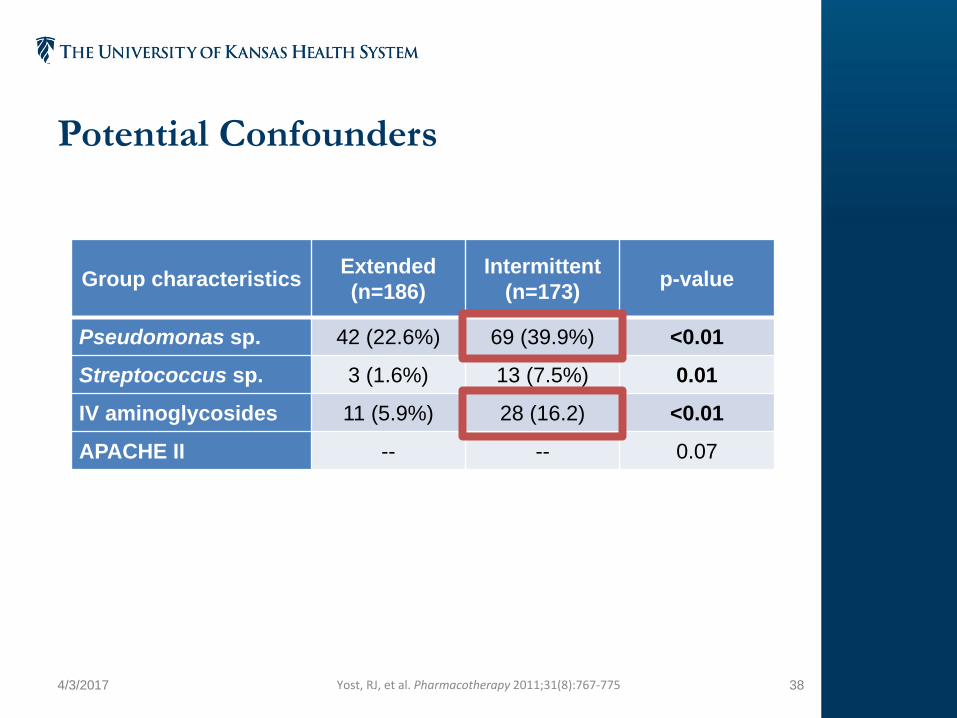
Potential Confounders
4/3/2017 38
Group characteristics Extended(n=186)
Intermittent(n=173) p-value
Pseudomonas sp. 42 (22.6%) 69 (39.9%) <0.01
Streptococcus sp. 3 (1.6%) 13 (7.5%) 0.01
IV aminoglycosides 11 (5.9%) 28 (16.2) <0.01
APACHE II -- -- 0.07
Yost, RJ, et al. Pharmacotherapy 2011;31(8):767-775
Does this show extended infusion beta-lactam dosing is superior?Supportive
• Extended infusion outperformed combination therapy with aminoglycosides (5.9% vs. 16.2%)
Confounding
• More P. aeruginosa in traditional dosing group
– Potential higher MIC
• More respiratory tract infections with traditional dosing group
– Potentially more difficult to treat
– No group specific mortality information published
4/3/2017 39Yost, RJ, et al. Pharmacotherapy 2011;31(8):767-775

Review Question 2• Which of the following groups are more likely to
benefit from extended infusion beta-lactam therapies?
A. Patients who are more critically ill
B. Patients who have P. aeruginosa infections
C. Patients who have urinary tract infections
D. Both A and B
4/3/2017 40

Empiric Coverage for SuspectedGram-negative Infections
Objective
• Determine if extended infusion beta-lactams improve outcomes in critically ill patients with suspected or confirmed gram-negative infections• Expect lower rate of mortality based on patient population
Primary Outcome
• Resolution of fever to < 38.3°C and > 36°C for 24 consecutive hours, and/or
• WBC decrease to < 12,000/μL or 50% decrease within 7 days
Secondary Outcomes
• Time to defervescence• All-cause hospital-, 14-, and 30-day mortality• ICU and hospital length of stay
4/3/2017 41Arnold HM, et al. Ann Pharmacother 2013;47:170-80

Standardized Dosing Schemes
4/3/2017 42Arnold HM, et al. Ann Pharmacother 2013;47:170-80
• All extended infusions occurred over 3 hours
Drug CrCl (ml/min) IV Dose
Cefepime ≥6030-60
2g every 8 hours2g every 12 hours
Meropenem ≥5030-50
1g every 8 hours1g every 12 hours
Piperacillin-tazobactam ≥4030-40
4.5g every 6 hours3.375g every 6 hours

Empiric Coverage for Suspected Gram-negative Infections
Inclusion Criteria
• ICU status receiving empiric gram-negative coverage• Suspected health-care associated infection• Fever (>38.3°C) and/or WBC >12,000/μL• Cultures drawn within 24 hours of the antibiotic start
time
Exclusion Criteria
• <48 consecutive hours of antibiotics while in ICU• CrCl <30 ml/min or renal replacement therapy• Antibiotic dose outside protocol• Urinary tract infection• Only gram-positive, fungal, or viral pathogen identified
4/3/2017 43Arnold HM, et al. Ann Pharmacother 2013;47:170-80

Study Design• Single center, pre/post implementation trial
• 162 patients needed to detect 50% relative risk reduction in treatment failure
4/3/2017 44Arnold HM, et al. Ann Pharmacother 2013;47:170-80
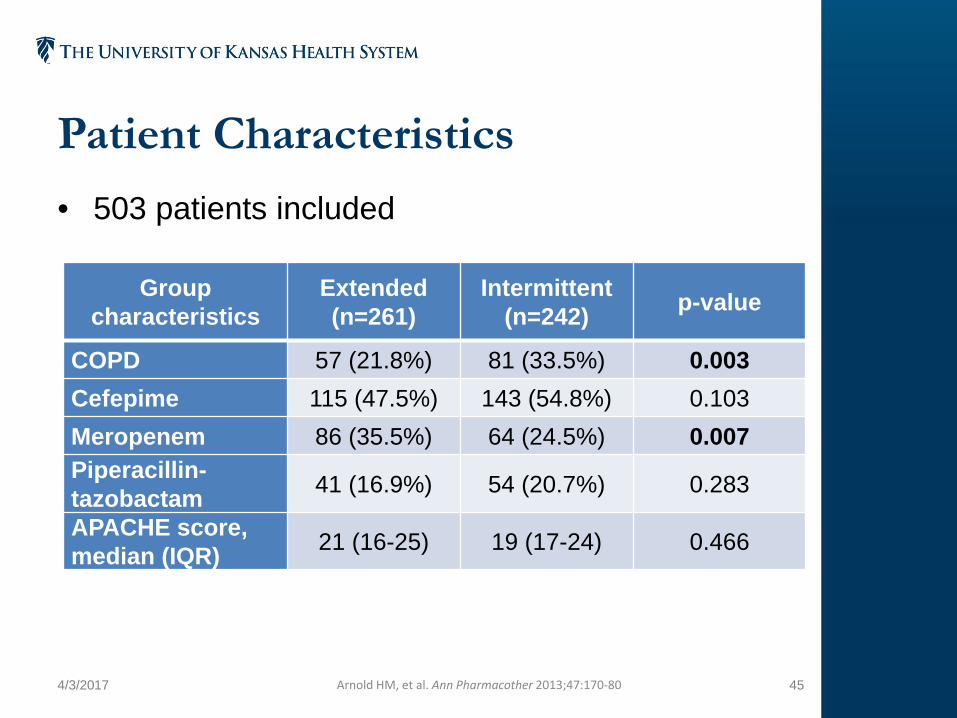
Patient Characteristics• 503 patients included
4/3/2017 45Arnold HM, et al. Ann Pharmacother 2013;47:170-80
Group characteristics
Extended(n=261)
Intermittent(n=242) p-value
COPD 57 (21.8%) 81 (33.5%) 0.003Cefepime 115 (47.5%) 143 (54.8%) 0.103Meropenem 86 (35.5%) 64 (24.5%) 0.007Piperacillin-tazobactam 41 (16.9%) 54 (20.7%) 0.283
APACHE score,median (IQR) 21 (16-25) 19 (17-24) 0.466

Clinical Outcomes• No statistically significant difference in primary
outcome or secondary outcomes
4/3/2017 46Arnold HM, et al. Ann Pharmacother 2013;47:170-80
Endpoint Extended (n=261)
Intermittent(n=242) p-value
Resolution of fever and WBC 51% 56.6% 0.204
30 day Mortality (%) 25.7% 23.6% 0.542
ICU LOS (days) 10.8 (5-17) 9.3 (5.6-19.2) 0.138

Limitations• Only 41% of patients had confirmed infections
• Limited number of patients with high MIC organisms identified:– n=25 of 206 patients with identified organisms– Enterobacteriaceae, P. aeruginosa, Acinetobacter
• No loading dose given– Low serum concentrations initially could impact
outcomes– Time to first antibiotic doses are determinants of
mortality
4/3/2017 47Arnold HM, et al. Ann Pharmacother 2013;47:170-80Gaieski DF, et al. Crit Care Med 2010;38(4):1045-53

Does prospective data show similar results?
4/3/2017 48

Continuous vs. Intermittent Infusions BLING II & BLISSStudy BLING II (2015) BLISS (2016)
Objective Evaluate efficacy of continuous infusion beta-lactams in critically ill patients with severe sepsis
Primary Outcome
Number of alive ICU-freedays at Day 28
Clinical cure at 14 days after antibiotic cessation
Secondary Outcome(s)
- 90-day mortality- Clinical cure at 14 days
after antibiotic cessation- Alive organ failure-free
days at Day 14- Duration of bacteremia
post randomization
- 14- and 30-day survival- PK/PD target attainment- ICU and ventilator-free
days at 28 days post randomization
4/3/2017 49Abdul-Aziz, MH, et al. Intensive Care Med 2016;42:1535-1545Dulhunty JM, et al. Am J Respir Crit Care Med 2015;192(11):1298-1305

Continuous vs. Intermittent Infusions BLING II & BLISSStudy BLING II (2015) BLISS (2016)
Study Design - Randomized controlled trial
- Open label
- Randomized controlled trial
- Double-blinded
Medications Similar spectrum of activity
- Piperacillin/tazobactam- Ticarcillin/clavulanate- Meropenem
- Piperacillin/tazobactam- Cefepime- Meropenem
Dosing Loading dose givenAllowed concomitant, non-beta-lactam antibiotics
4/3/2017 50Abdul-Aziz, MH, et al. Intensive Care Med 2016;42:1535-1545Dulhunty JM, et al. Am J Respir Crit Care Med 2015;192(11):1298-1305

Continuous vs. Intermittent Infusions BLING II & BLISSStudy BLING II (2015) BLISS (2016)
Inclusion Criteria
≥18 years oldSevere sepsis criteria
Exclusion Criteria
- >24 hours beta-lactam before randomization
- Pregnancy- Allergy to study drug
- Continuous renal replacement therapy
- Impaired hepatic function- Inadequate central venous
access
4/3/2017 51Abdul-Aziz, MH, et al. Intensive Care Med 2016;42:1535-1545Dulhunty JM, et al. Am J Respir Crit Care Med 2015;192(11):1298-1305

Patient CharacteristicsBLING II
4/3/2017 52Dulhunty JM, et al. Am J Respir Crit Care Med 2015;192(11):1298-1305
Group characteristics Continuous(n=212)
Intermittent(n=220)
Identified gram-negatives 29 (72.5%) 31 (72.1%)
Pulmonary Infection 115 (54.2%) 120 (54.5%)
APACHE II 21 (17-26) 21 (16-25)

Patient CharacteristicsBLISS• Same total daily dose of antibiotics regardless of infusion
strategy
4/3/2017 53Abdul-Aziz, MH, et al. Intensive Care Med 2016;42:1535-1545
Group characteristics Continuous(n=70)
Intermittent(n=70)
P. aeruginosa 37% 31%
A. baumannii 25% 23%
Pulmonary Infection 46 (66%) 36 (51%)
Concomitant antibiotic 33 (47%) 33 (47%)
APACHE II 21 (17-26) 21 (15-26)

Clinical OutcomesBLING II & BLISSStudy BLING II (2015) BLISS (2016)
Results - No statistically significant difference between groups in any outcome
- Clinical cure at 14 days higher after cessation of antibiotic
- 56% vs. 34%, p=0.011
Limitations - 26% of patients had renal replacement therapy
- Median length of treatment: 3 days
- Median length of treatment: 7 days
4/3/2017 54Abdul-Aziz, MH, et al. Intensive Care Med 2016;42:1535-1545Dulhunty JM, et al. Am J Respir Crit Care Med 2015;192(11):1298-1305
Extended Infusion Carbapenems?• Limited data available – mainly case reports
• Risk documented with extended infusion doripenem– Doripenem 1g q8h over 4 hours for 7 days vs.
imipenem-cilastatin 1g q8h over 30 minutes for 10 days– Study stopped early due to inferior efficacy and
increased mortality– Limitation: first dose was the extended infusion
4/3/2017 55Kollef et al. Critical Care 2012, 16:R218Osthoff M, et al. Swiss Med Wkly. 2016;146:w14368
Indications• Confirmed P. aeruginosa infections
• Critically ill patients
• Pulmonary infections
• Severe sepsis
• Institution-specific resistance patterns
4/3/2017 56Osthoff M, et al. Swiss Med Wkly. 2016;146:w14368

Dosing Strategy• Loading dose before using extended infusion or
continuous infusion
• Quicker attainment of MIC with loading doses
• Start extended infusion dosing schedule at next interval
4/3/2017 57

Other Hospitals that Use Extended or Continuous Infusions• Out of 17 responses:
– All hospitals used extended or continuous infusion beta-lactam therapy
– All hospitals used piperacillin-tazobactam as an extended infusion
– Five hospitals used meropenem extended infusion
– Three hospitals used cefepime extended infusion
4/3/2017 58
Other Hospitals that Use Extended or Continuous Infusions• University of Missouri Health Care• Oklahoma Heart Hospital• University of California – Davis Medical Center• UC – San Diego Health• Detroit Medical Center• University of Chicago• Beth Israel Deaconess Medical Center• Gulf Coast Regional Medical Center• UW Health• UCLA• Johns Hopkins• University of Utah
4/3/2017 59

Obstacles for Extended Infusion Beta-lactam Implementation
4/3/2017 60

IV Medication Compatibility• Doses can run for 12 hours each day• Requires multiple peripheral lines or a central line
4/3/2017 61
Piperacillin-tazobactam
Cefepime Meropenem
- Levofloxacin, vancomycin
- Diltiazem, dobutamine, hydralazine, labetalol, nicardipine
- Famotidine, prochlorperazine, promethazine, pantoprazole, insulin
- Midazolam
- Diltiazem, dobutamine, nicardipine
- Diphenhydramine, propofol
- Famotidine, pantoprazole, prochlorperazine, promethazine
- Midazolam, dopamine, morphine
- Magnesium sulfate
- Amiodarone,nicardipine
- Diazepam, propofol- Pantoprazole
*Not an inclusive list of incompatibilitiesTrissel’s 2 Database
Cost Benefits of Extended Infusion Beta-lactams• Reduced cost of piperacillin-tazobactam
– Decrease of one dose per day– Potential decrease in length of hospital stay
• Possible decreased length of ICU stay and hospital stay with other beta-lactams– No decrease in total daily drug dosage
4/3/2017 62Brunetti L, et al. Ann Pharmacother 2015; 49:754Schmees PM, et al. Am J Health Syst Pharm 2016; 73:S100

Review Question 4• Which of the following is an area where
pharmacists can make an impact on proper use of extended infusion beta-lactams?A. Administration technique of extended infusion beta-
lactams
B. IV incompatibility surveillance
C. Diagnosis of an infectious disease process
D. All the above
4/3/2017 63
Steps Toward Implementation
4/3/2017 64
Nursing• Education on benefit and purpose of extended
infusion therapy
• Maintain cleanliness of line sites to prevent infections
• PT / OT issues with IV administration of medications
4/3/2017 65

Pharmacy• Configuration of smart pumps and CPOE entries
• Selection of appropriate patient
• Considerations: – IV incompatibilities– Line access
4/3/2017 66
Summary• Time-dependent properties allows extended-infusions
• Piperacillin-tazobactam has the most evidence for use
• Extended infusion beta-lactams should be used in:– Critically ill patients– Pulmonary infections
• Patient outcomes are improved when used appropriately
• Multidisciplinary implementation is required for successful extended-infusion beta lactams
4/3/2017 67
Acknowledgement• Kane Hosmer, PharmD, BCOP
4/3/2017 68

Combating Antimicrobial Resistance with Extended Infusion Beta-lactamsStephen Andrews, PharmDPGY-1 Pharmacy Practice [email protected]