Embed Size (px)
Citation preview

o
Colostomy
Procedure Part II - Colostomy
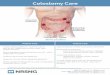
The proximal end of the healthy colon is brought out to the skin of the abdominal wall, where it is sutured in place. An adhesive drainage bag (stoma appliance) is placed around the opening. The abdominal incision is then closed.
Home > Medical Reference > Surgeries and Procedures
Colostomy
Procedure Part I - Colostomy

A colostomy creates an opening on the abdomen (stoma) for the drainage of stool (feces) from the large intestine (colon). Colostomies are usually performed after resection of the diseased colon. Colostomies may be temporary or they may be permanent. The procedure is performed while you are deep asleep and pain-free (under general anesthesia). An incision is made in the abdomen and the diseased colon is removed
Home > Medical Reference > Surgeries and Procedures
Colostomy
Indications- Colostomy

A colostomy is performed when the lower large intestine, rectum, or anus is unable to function normally, or needs rest from normal functions. Intestinal obstruction with associated inflammation, as in diverticulitis, is a common indication for colostomy

More than 90% of colostomy cases are successful. There is considerable pain after surgery as the anus tightens and relaxes, but medications are available to relieve this. To avoid straining, stool softeners are used. Avoid any straining during bowel movement or urination. Soaking in a warm bath also brings additional comfort. Depending on the disease process being treated, colostomies can be "taken down," and the colon is reconnected in a second operation within weeks to months after the first operation
Gallstones
Definition
Gallstones are formed within the gallbladder, an organ that stores bile excreted from the liver. Bile is a solution of water, salts, lecithin, cholesterol, and other substances. If the concentration of these components changes, they may precipitate from solution and form gallstones.
Alternative Names
Cholelithiasis

Causes, incidence, and risk factors
Gallstones often have no symptoms and are usually discovered incidentally by a routine x-ray, surgery, or autopsy.
Page: 1 2 Next >
DefinitionGallstones are formed within the gallbladder, an organ that stores bile excreted from the liver. Bile is a solution of water, salts, lecithin, cholesterol, and other substances. If the concentration of these components changes, they may precipitate from solution and form gallstones.
Gallstones may be as small as a grain of sand, or they may become as large as an inch in diameter, depending on how much time has elapsed from their initial formation.
Alternative Names
Signs and testsThere are numerous tests to detect the presence of gallstones or gallbladder inflammation:
Abdominal ultrasound Abdominal CT scan Abdominal x-ray Oral cholecystogram Gall bladder radionuclide scan ERCP (endoscopic retrograde cholangiopancreatography
TreatmentModern advances in surgery have revolutionized the treatment of gallstones. In general, surgery is used only if you have symptoms.
In the past, open cholecystectomy (gallbladder removal) was the usual procedure for uncomplicated cases. This operation required a medium to large incision just below the right lower rib in order to access the gallbladder. After this operation, a patient typically spent 3-5 days in the hospital recovering.
However, a minimally-invasive technique called laparoscopic cholecystectomy was introduced in the 1980s which uses small incisions and camera guidance to remove the gallbladder.

Currently, laparoscopic cholecystectomy is the gold standard for treating gallstones that cause symptoms and is one of the most common operations performed in hospitals today.
ERCP (Endoscopic Retrograde Cholangiopancreatography)
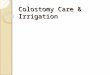
Endoscopic retrograde cholangiopancreatography (en-doh-SKAH-pik REH-troh-grayd koh-LAN-jee-oh-PANG-kree-uh-TAH-gruh-fee) (ERCP) enables the physician to diagnose problems in the liver, gallbladder, bile ducts, and pancreas. The liver is a large organ that, among other things, makes a liquid called bile that helps with digestion. The gallbladder is a small, pear-shaped organ that stores bile until it is needed for digestion. The bile ducts are tubes that carry bile from the liver to the gallbladder and small intestine. These ducts are sometimes called the biliary tree. The pancreas is a large gland that produces chemicals that help with digestion and hormones such as insulin.
ERCP is used primarily to diagnose and treat conditions of the bile ducts, including gallstones, inflammatory strictures (scars), leaks (from trauma and surgery), and cancer. ERCP combines the use of x rays and an endoscope, which is a long, flexible, lighted tube. Through the endoscope, the physician can see the inside of the stomach and duodenum, and inject dyes into the ducts in the biliary tree and pancreas so they can be seen on x rays.
For the procedure, you will lie on your left side on an examining table in an x-ray room. You will be given medication to help numb the back of your throat and a sedative to help you relax during the exam. You will swallow the endoscope, and the physician will then guide the scope through your esophagus, stomach, and duodenum until it reaches the spot where the ducts of the biliary tree and pancreas open into the duodenum. At this time, you will be turned to lie flat on your stomach, and the physician will pass a small plastic tube through the scope. Through the tube, the physician will inject a dye into the ducts to make them show up clearly on x rays. X rays are taken as soon as the dye is injected.
If the exam shows a gallstone or narrowing of the ducts, the physician can insert instruments into the scope to remove or relieve the obstruction. Also, tissue samples (biopsy) can be taken for further testing.
Possible complications of ERCP include pancreatitis (inflammation of the pancreas), infection, bleeding, and perforation of the duodenum. Except for pancreatitis, such problems are uncommon. You may have tenderness or a lump where the sedative was injected, but that should go away in a few days.
The digestive system

ERCP takes 30 minutes to 2 hours. You may have some discomfort when the physician blows air into the duodenum and injects the dye into the ducts. However, the pain medicine and sedative should keep you from feeling too much discomfort. After the procedure, you will need to stay at the hospital for 1 to 2 hours until the sedative wears off. The physician will make sure you do not have signs of complications before you leave. If any kind of treatment is done during ERCP, such as removing a gallstone, you may need to stay in the hospital overnight.
Preparation
Your stomach and duodenum must be empty for the procedure to be accurate and safe. You will not be able to eat or drink anything after midnight the night before the procedure, or for 6 to 8 hours beforehand, depending on the time of your procedure. Also, the physician will need to know whether you have any allergies, especially to iodine, which is in the dye. You must also arrange for someone to take you home—you will not be allowed to drive because of the sedatives. The physician may give you other special instructions
ERCP (Endoscopic Retrograde Cholangiopancreatography)
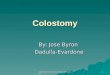
Endoscopic retrograde cholangiopancreatography (en-doh-SKAH-pik REH-troh-grayd koh-LAN-jee-oh-PANG-kree-uh-TAH-gruh-fee) (ERCP) enables the physician to diagnose problems in the liver, gallbladder, bile ducts, and pancreas. The liver is a large organ that, among other things, makes a liquid called bile that helps with digestion. The gallbladder is a small, pear-shaped organ that stores bile until it is needed for digestion. The bile ducts are tubes that carry bile from the liver to the gallbladder and small intestine. These ducts are sometimes called the biliary tree. The pancreas is a large gland that produces chemicals that help with digestion and hormones such as insulin.
ERCP is used primarily to diagnose and treat conditions of the bile ducts, including gallstones, inflammatory strictures (scars), leaks (from trauma and surgery), and cancer. ERCP combines the use of x rays and an endoscope, which is a long, flexible, lighted tube. Through the endoscope, the physician can see the inside of the stomach and duodenum, and inject dyes into the ducts in the biliary tree and pancreas so they can be seen on x rays.
For the procedure, you will lie on your left side on an examining table in an x-ray room. You will be given medication to help numb the back of your throat and a sedative to help you relax during the exam. You will swallow the endoscope, and the physician will then
The digestive system

guide the scope through your esophagus, stomach, and duodenum until it reaches the spot where the ducts of the biliary tree and pancreas open into the duodenum. At this time, you will be turned to lie flat on your stomach, and the physician will pass a small plastic tube through the scope. Through the tube, the physician will inject a dye into the ducts to make them show up clearly on x rays. X rays are taken as soon as the dye is injected.
If the exam shows a gallstone or narrowing of the ducts, the physician can insert instruments into the scope to remove or relieve the obstruction. Also, tissue samples (biopsy) can be taken for further testing.
Possible complications of ERCP include pancreatitis (inflammation of the pancreas), infection, bleeding, and perforation of the duodenum. Except for pancreatitis, such problems are uncommon. You may have tenderness or a lump where the sedative was injected, but that should go away in a few days.
ERCP takes 30 minutes to 2 hours. You may have some discomfort when the physician blows air into the duodenum and injects the dye into the ducts. However, the pain medicine and sedative should keep you from feeling too much discomfort. After the procedure, you will need to stay at the hospital for 1 to 2 hours until the sedative wears off. The physician will make sure you do not have signs of complications before you leave. If any kind of treatment is done during ERCP, such as removing a gallstone, you may need to stay in the hospital overnight.
Preparation
Your stomach and duodenum must be empty for the procedure to be accurate and safe. You will not be able to eat or drink anything after midnight the night before the procedure, or for 6 to 8 hours beforehand, depending on the time of your procedure. Also, the physician will need to know whether you have any allergies, especially to iodine, which is in the dye. You must also arrange for someone to take you home—you will not be allowed to drive because of the sedatives. The physician may give you other special instructions

LAPAROSCOPIC CHOLECYSTECTOMY
Dr. Steven Bolton is presenting a case of laparoscopic cholecystectomy.
This is a case of a 42 year old male with a previous history of abdominal pain for 6 months. He was admitted to the hospital with nausea but vomiting or fever. An ultrasound study showed gallstones with some thickening of the gallbladder wall. The diagnosis of cholecystitis was made and the patient was scheduled to undergo a laparoscopic cholecystectomy. This picture shows the omentum partially covering the gallbladder in its normal position.

Hook electrocautery is used to dissect the gallbladder off the liver bed
This picture shows the body of the gallbladder, that becomes distended during removal. Caution must be used to avoid rupture while pulling
This picture shows the body of the gallbladder, that becomes distended during removal. Caution must be used to avoid rupture while pulling
Laparoscopic Cholecystectomy
The gallbladder is a pear-shaped organ that sits beneath the liver in the right-upper abdomen. It's function is to store bile. It is attached to the bile ducts that come from the

liver. These ducts carry bile from the liver to the gallbladder and intestine where the bile helps digest food. The gallbladder is not necessary to maintain good health.
Gallstones. They are a very common medical problem. When they cause pain or other problems, treatment is usually needed. The removal of the gallbladder is one of the most common types of surgery done in this country. In the past, open abdominal surgery was the standard treatment. This procedure required a 3 to 7 day stay in the hospital and a 3 to 7 inch incision and scar on the abdomen.
LaparoscopyMost females have heard of laparoscopy, also known as "bellybutton" or "Band-Aid" surgery. Gynecologists have long used this technique to tie the Fallopian tubes and to inspect the female reproductive organs. Now the use of laparoscopy has been expanded to include removing a diseased gallbladder. With new video technology, the laparoscope has become a miniature television camera. Powerful magnification is now possible, showing the intestinal organs in great detail.
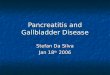
Laparoscopic CholecystectomyA cholecystectomy is the surgical removal of the gallbladder. Using advanced laparoscopic technology, it is now possible to remove the gallbladder through a tiny incision at the navel. The technique is performed as follows. The patient receives general anesthesia. Then a small incision is made at the navel (point A) and a thin tube carrying the video camera is inserted. The surgeon inflates the abdomen with carbon dioxide, a harmless gas, for easier viewing and to provide room for the surgery to be performed. Next, two needle-like instruments are inserted (points B). These instruments serve as tiny hands within the abdomen. They can pick up the gallbladder, move intestines around, and generally assist the surgeon. Finally, several different instruments are inserted (point C) to clip the gallbladder artery and bile duct, and to safely dissect and remove the gallbladder and stones. When the gallbladder is freed, it is then teased out of the tiny navel incision. The entire procedure normally takes 30 to 60 minutes. The three puncture wounds require no stitches and may leave very slight blemishes. The navel incision is barely visible.
What Are the Benefits?The main benefit of this procedure is the ease of recovery for the patient. There is no incision pain as occurs with standard abdominal surgery. The patient is up and about the same day. In fact, up to 90% of patients go home the same day. The remainder are usually discharged the next day. And within several days, normal activities can be resumed. So the recovery time is much quicker. Also, there is no scar on the abdomen.
What Are the Complications?While the procedure seems very easy for the patient, it is still abdominal surgery. And, even though infrequent, it still carries the same risks as general surgery. Current medical reports indicate that the low complication rate is about the same for this procedure as for standard gallbladder surgery. These complications may include:

In about 5 to 10% of cases, the gallbladder cannot be safely removed by laparoscopy. Standard open abdominal surgery is then immediately performed.
Nausea and vomiting may occur after the surgery. Injury to the bile ducts, blood vessels, or intestine can occur, requiring corrective
surgery. Quite uncommonly, a diagnostic error or oversight may occur.
Indications
Gallbladder surgery is done to treat gallbladder disease, which consists predominantly of the formation of gallstones in the gallbladder (cholelithiasis) which can cause:
In each case, removal of the gallbladder (cholecystectomy) is indicated.