Embed Size (px)
Citation preview

Colorectal DiscussionBeyond Progression: Is this progress?
Alan P. Venook, MD
University of California, SF

Disclosures
• Roche / Genentech, Regeneron and Sanofi have provided me with background information
• I have served on Data Safety Monitoring Boards related to studies with Bevacizumab and Brivanib
• I helped design the original CRC Bevacizumab trial and prescribe Bevacizumab
• I had no involvement in the Aflibercept or Brivanib trials nor have I ever prescribed the drugs
• Thanks to Drs. Arnold, Allegra and Siu being timely• Thanks to Lee Ellis and Napo Ferrara for trying to educate
me about VEGF biology
PRESENTED BY:

Colorectal abstracts
• Review data (briefly)• Mechanism of action (minimal)• Clinical impact• Research implications• Next steps
PRESENTED BY:

Theme: Beyond Progression
• TML – BEV* beyond progression– Initiated by AIO; completed by Roche / Genentech
• VELOUR - 2nd line Aflibercept in pts PD on Bev– Regeneron / Sanofi
• CO.20 – Cetuximab +/- Brivanib– NCIC + AGITG
* BEV = Bevacizumab
PRESENTED BY:

Themes: Beyond Progression
• TML – Bev beyond progression OS IMPROVED– Initiated by AIO; completed by Roche / Genentech
• VELOUR - 2nd line Aflibercept in pts PD on Bev– Regeneron / Sanofi SAME BENEFIT +/- PRIOR BEV
• CO.20 – Cetuximab +/- Brivanib CLOSE BUT NOT QUITE– NCIC + AGITG
PRESENTED BY:

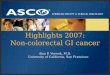
SWOG 0600/iBET: A Phase III of Irinotecan and Cetuximab With or Without Bevacizumab in Patients With mCRC That Progressed During First-Line Therapy
Gold, Grothey et al..
• Primary endpoint: OS
• Secondary endpoints: PFS, objective tumor response, tolerability, and safety
• June 2007
Second line
PD
RANDOMIZE
CT + dual biologic arm removed
mCRCKRAS
wild-typepreviously
treated with Bevacizumab
and oxaliplatin- based CT(n=1260)
Bevacizumab 5 mg/kg +(FOLFIRI or Irinotecan +
Capecitabine)
Cetuximab +(FOLFIRI or Irinotecan +
Capecitabine)
6

7
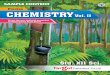
BRiTE Registry: Bevacizumab Regimens: Investigation Treatment Effects Grothey et al, ASCO, 2007
• A longer median OS in the BBP subgroup was observed compared with the No BBP subgroup (Table 4).
• A longer survival beyond 1st PD was observed in the BBP subgroup versus the No BBP subgroup.
Median OS: 19.9 v. 31.8 mos
OS Beyond PD: 9.5 v. 19.2 mos

SWOG 0600/iBET: A Phase III of Irinotecan and Cetuximab With or Without Bevacizumab in Patients With mCRC That Progressed During First-Line Therapy
Gold, Grothey et al..
• Primary endpoint: OS
• Secondary endpoints: PFS, objective tumor response, tolerability, and safety
• June 2007 – October 2010
Second line
PD
RANDOMIZE
CT + dual biologic arm removed
mCRCKRAS
wild-typepreviously
treated with Bevacizumab
and oxaliplatin- based CT(n=1260)
Bevacizumab 5 mg/kg +(FOLFIRI or Irinotecan +
Capecitabine)
Cetuximab +(FOLFIRI or Irinotecan +
Capecitabine)
8
N = 68

Bev + standard first-line CT (either
oxaliplatin oririnotecan-based)
(n=820)
Randomize 1:1
Standard second-line CT (oxaliplatin or irinotecan-
based) until PD
Bev (2.5 mg/kg/wk) + standard second-line CT (oxaliplatin or irinotecan-
based) until PD
PD
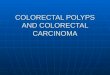
TML – Treatment Multiple Lines
Cross-over:
Oxaliplatin → Irinotecan
Irinotecan → Oxaliplatin
Study conducted in 220 centres in Europe and Saudi Arabia
Primary endpoint Overall survival from randomization
Statistics: Designed to detect 30% (HR 0.77) improvement in median OS (90% power,
2-sided 5%)

TML features and findings
• Very select patient population – Tolerant of long-term Bev, not curable– PFS 1st line > 3 months
• Responses infrequent (4-5%)• Median 4 months additional Bev• Chemotherapy backbone did not matter• BEV beyond PD improves OS 1.4 months (HR = 0.81)
PRESENTED BY:

TML: missing in abstract presentation
• Impact of subsequent treatment• KRAS status
– Only 40% received anti-EGFR
• BRAF status• Primaries in place ?• OS from diagnosis, not randomization
The word: BIOMARKER
PRESENTED BY:

What else does TML teach us?
• Affirms the limited utility of Registry studies regarding interventions and outcomes:– BRITE: 9.5 v. 19.2 OS beyond PD– TML: 9.8 v. 11.2
BRiTE findings not replicated; the publication* could be cited as an example of the pitfalls of Registry data
* Grothey et al, JCO, 2008
PRESENTED BY:

Aflibercept
• Fusion protein of key domains from human VEGF receptors 1 and 2 with human IgG Fc¹
• Blocks all human VEGF-A isoforms, VEGF-B, and placental growth factor (PlGF)²
• High affinity – binds VEGF-A and PlGF more tightly than native receptors
1. Holash J et al. Proc Natl Acad Sci USA. 2002;99:11393-11398.2. Tew WP et al. Clin Cancer Res. 2010;16:358-366.

VELOUR – VEGF-trap with irinotecan in coLOrectal cancer after failURe of oxaliplatin
Metastatic Colorectal Cancer
RANDOMIZE
Aflibercept 4 mg/kg IV, day 1 + FOLFIRI q2 weeks
Placebo IV, day 1+ FOLFIRIq2 weeks
1:1 Disease Progression Death
600
600Stratification factors:• ECOG PS (0 vs 1 vs 2)• Prior bevacizumab (Y/N)
OS: 12.06 v 13.5 HR = 0.817 p =0.0032

ASCO 2012
15
Consistency of OS and PFS With and Without Prior Bevacizumab
Prior Bevacizumab No Prior Bevacizumab
Placebo/ FOLFIRI(n=187)
Aflibercept/FOLFIRI(n=186)
ΔPlacebo/ FOLFIRI(n=427)
Aflibercept/FOLFIRI(n=426)
Δ
OS (months) (95.34% CI)
11.7(9.8-13.8)
12.5(10.8-15.5)
0.812.4
(11.2-13.5)13.9
(12.7-15.6)1.5
PFS (months) (99.99% CI)
3.9(2.9-5.4)
6.7(4.8-8.7)
2.85.4
(4.2-6.7)6.9
(5.8-8.2)1.5
• Interaction between “treatment arm” and “prior bevacizumab” factor was not significant at the 2-sided 10% level (P=0.57 for OS; P=0.2 for PFS)
Response rate 8.4 11.7 12.4 23.3

NCIC CTG CO.20: Schema
RANDOMI Z E
Brivanib
+ Cetuximab
n = 376
Placebo
+ Cetuximab
n = 374
1° endpoint: Overall Survival
Total sample size: 750
Trial: 2008 - 2011
Median follow-up: updated analysis: 34 months (694 deaths)
1:1
Stratify by Center and ECOG 0/1 versus 2

What do we learn from NCI CTG CO.20?
PRESENTED BY:
• PFS improvement does not mean OS as well• The study was powered such that 0.7 mos would
not be statistically significant• TML & VELOUR were powered differently
– 1.4 mos OS benefit
Ask yourselves: is 1.4 mos clinically significant ?

Colorectal abstracts
• Review data (briefly)• Mechanism of action (minimal)• Clinical Impact• Research Implications• Next steps
PRESENTED BY:

Anti-VEGF mechanism of action: evolving
Ellis, Hicklin. Nat Rev Ca 2008
Proposed MOA 1995 2000 2005 2010 2012 2015?
Anti-angiogenic (EC proliferation)
+++ +++ +++ ++ ?
Anti-angiogenic(Bone Marrow Derived Progenitor Cells)
+ +++ ?
“Normalization” improve delivery chemo
+++ ?
Direct effect on tumor + + + ?
Vascular “constriction” ++ +++ +++ ?
Offset effects of stress ++ ++ ++ ?
Disrupt the cancer stem cell niche
+ + ?
Immune function + ++ ++ ?
Courtesy Lee Ellis, MD
Difficult to explain mechanism of VEGF inhibition beyond progression when we are not sure of the
mechanism(s) of action in the first place

Colorectal abstracts
• Review data (briefly)• Mechanism of action (minimal) • Clinical Impact• Research Implications• Next steps
PRESENTED BY:

Clinical Impact -- Regulatory
• Drugs likely to be approved by FDA– Aflibercept in 2nd line metastatic CRC w/ FOLFIRI– Regorafenib in “refractory” metastatic colorectal cancer
• Label addition for old drug– Bevacizumab beyond progression
• Drug with uncertain future– Brivanib awaits other maturing trials
(will not discuss further since may never be available)
PRESENTED BY:

Clinical Impact – Precision Medicine ? Current Practice Pattern in US
While we say CONTINUUM OF CARE, in practice:
• FOLFOX / BEV 1st line until neurotoxicity +/- PD,• Then KRAS status:
– (FOLF) Irinotecan +/- EGFR Ab– FOLFOX + EGFR
• Not established– Regorafenib– Aflibercept– Clinical Trial
PRESENTED BY:

Clinical Impact: Whither FOLFOX / BEV?
Hurwitz, et al. NEJM, 2004
= 4.7 mos

Clinical Impact: Whither FOLFOX / BEV? History Lesson
Hurwitz data: BEV a difference-maker with IFL
IN RETROSPECT:• BEV approved “with FU regimen”; FOLFOX > IFL• FOLFOX / BEV: 2nd-line in BEV naïve patients • Subsequent studies: no increase RR, marginal OS• Although not limited by neurotoxicity, FOLFIRI less popular
as backbone
BY DEFAULT:
FOLFOX / BEV 1st-line metastatic CRC
PRESENTED BY:

Clinical Impact – Paradigm shift? Current Practice Pattern in US
While we say CONTINUUM OF CARE, in practice:
• FOLFOX / BEV 1st line until neurotoxicity +/- PD,• Then KRAS status:
– (FOLF) Irinotecan +/- EGFR Ab– FOLFOX + EGFR
• Not established– Regorafenib– Aflibercept– Clinical Trial
PRESENTED BY:
BEV beyond PD

Clinical Impact – Paradigm shift Anti-VEGF therapy: Interpreting TML
If TML correctly predicts that continuing 1st-line BEV beyond PD improves outcomes in 2nd-line: • Why would that not apply for 3rd line ?• For subsequent line(s) ?• For EGFR Ab’s in KRAS wt patients?• Should we be stopping BEV before elective surgery?• What toxicities justify stopping BEV?• Treatment Holidays?• Are Aflibercept and Regorafenib extensions of this effect?
PRESENTED BY:

Clinical Impact: Anti-VEGF therapy What do we tell our patients?
WHY: • Once initiated, discontinuing anti-VEGF therapy may lead
to a small survival disadvantage• Anti-VEGF therapy works in subsequent lines as well
FOREVER:• In fact, it may be a mistake to discontinue anti-VEGF
therapy at any time and that effects all the decisions we will make over the course of your disease
WHEN ?
• So while anti-VEGF therapy is a standard 1st line treatment, it may make more sense to use it in 2nd and subsequent lines rather than up-front
PRESENTED BY:

Colorectal abstracts
• Review data (briefly)• Mechanism of action(minimal) • Clinical Impact• Research Implications• Next steps
PRESENTED BY:

Implications: from Clinical Care to Research
• Is FOLFOX / BEV the optimal 1st line choice?• Can we distinguish BEV v. Aflibercept ?• Is Regorafenib different ?• Have we reached the ceiling with VEGF as a target?• What about EGFR antibodies? When?• Should we revisit dual antibodies?
WHO BENEFITS and WHO DOES NOT?
PRESENTED BY:

Put some “precision” into Precision Medicine
• Treating many patients to help few• Missed opportunity and added toxicities• Paucity of biomarkers for colorectal cancer:
– KRAS: who does NOT benefit from EGFR inhibition– MSI: who may not need chemotherapy– BRAF: who does very poorly overall
• Need to inform choice of treatment by biomarkers if at all possible
PRESENTED BY:

Colorectal abstracts
• Review data (briefly)• Mechanism of action (minimal) • Clinical Impact• Research Implications• Next steps
PRESENTED BY:

CALGB/SWOG # 80405
Untreatedadvancedor mCRCN =1142
Bevacizumab+
FOLFOX or FOLFIRIq 2 wks
Cetuximab+
FOLFOX or FOLFIRIq 2 wks
Screenfor
eligibility
Sendtumortissue
block toSWOGPCO
RandomizePatients
w/Wild type
K-ras tumor
Shameless advertising: clinical and correlative
results expected 2013 +/-
Re-open: 6/09Closed to accrual: 2/12
Patients enrolled: N = 2334 (total) 1177 (final endpt)

Search for anti-VEGF biomarkers
• Bevacizumab– Plasma; blood mRNA & DNA; tumor IHC, mRNA, DNA– pVEGF-A putative biomarker (JCO, 2012)
• Aflibercept– Plasma for pK and pD; VEGF
• Regorafenib– Anticipate extensive biomarker analysis– Yes/no nature of outcome may yield biomarker
• Brivanib– Plasma 83-analyte (data analysis)
PRESENTED BY:

PRESENTED BY:
COST of CARE
The Elephant in the Room

Meropol and Schulman, JCO, 2007
Cost of Cancer Care: Issues and Implications

Impact on Cost of Care: back of the envelope
• Bevacizumab – $2864 per 400 mg vial*– Average weekly dose = 175 mg
• Regorafenib – Sorafenib $8377 / month
• Aflibercept
PRESENTED BY:
$$ per UCSF pharmacy
$$$ unknown

Colorectal cancer in 2012: my reality check
• These are modest advances• A minority of patients appear to benefit• And the costs are unsustainable
THE CHALLENGE
• Actually deliver on promise of personalized medicine• To do so, we need better tools to predict outcomes• And it must be affordable
PRESENTED BY:

CRC 2012: making it affordable Multiple Choice (may select more than one)
1. Implement an agency like NICE
PRESENTED BY:

NICE: National Institute for Health and Clinical Excellence
• Critical analysis of cost:benefit• Determines what will be covered by National
Health Insurance in UK• Approval does not mean coverage• Non-approval does not mean non-coverage
http://guidance.nice.org.uk/CG131
PRESENTED BY:

CRC 2012: how to live within our means Multiple Choice (may select more than one)
1. Implement an agency like NICE
2. Let the market take care of things (as with generic drugs)
3. Await a bold cost-slashing move by Pharma (e.g. Cipla)
4. Give the FDA (or other panel) authority over drug pricing
5. Moratorium on studies powered to find clinically insignificant impact (to be defined)
6. Make the discovery of predictive biomarkers as high a priority as finding new drugs or indications
PRESENTED BY:

















![Current Status of Folic Acid Supplementation on Colorectal ...DNA methylation [69]; and the promotion of progression of existing precancerous lesions or cancer [1, 2, 15, 16]. Folate](https://img.pdfslide.us/doc/110x75/5f21ed2f4fdfe027bb1d28ce/current-status-of-folic-acid-supplementation-on-colorectal-dna-methylation-69.jpg)