Embed Size (px)
Citation preview

In 1981 Francis Crick commentedthat Òthe origin of life appears to bealmost a miracle, so many are the
conditions which would have to be sat-isÞed to get it going.Ó Now, several Þnd-ings have rendered lifeÕs conceptionsomewhat less implausible. The resultsall bolster what is already the dominanttheory of genesis: the RNA world.
The theory helped to solve what wasonce a classic chicken-or-egg problem.Which came Þrst, proteins or DNA? Pro-teins are made according to instructionsin DNA, but DNA cannot replicate itselfor make proteins without the help ofcatalytic proteins called enzymes. In1983 researchers found the solution tothis conundrum in RNA, a single-strand
molecule that helps DNA make protein.Experiments revealed that certain
types of naturally occurring RNA, nowcalled ribozymes, could act as their ownenzymes, snipping themselves in twoand splicing themselves back togetheragain. Biologists realized that ribozymesmight have been the precursors of mod-ern DNA-based organisms. Thus wasthe RNA-world concept born.
The Þrst ribozymes discovered wererelatively limited in their capability. Butin recent years, Jack W. Szostak, a mo-
SCIENTIFIC AMERICAN January 1996 27
The World According to RNAExperiments lend support to the leading theory of lifeÕs origin
Amillion people worldwide, about 145,000 of them in the U.S., will be diagnosed with colorectal cancer this
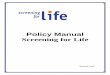
year. Up to half a million, about 55,000 in the U.S., will dieof the disease. Mortality from colorectal cancer rises pro-gressively with age: in western Europe and English-speak-ing countries, it typically increases from fewer than oneper 100,000 among those in the age 25 to 34 group to170 or more in the age 75 to 84 group.
The highest rates are in Hungary and the former Czech-oslovakia, which recorded, respectively, 46 and 47 deathsper 100,000. In the U.S., white males average 26 deathsper 100,000, whereas black men, who generally receiveinferior medical care, average 32 per 100,000. The lowestmortality from colorectal cancer is in developing coun-tries, such as India, which is estimated to have a rate lessthan one twentieth that of Western countries.
The large differences between developed and develop-ing countries reflect differences in environment, geneticinheritance, way of life and, most important, diet. Coun-tries such as the U.S. and Great Britain, where people typi-cally eat meals rich in fat, meat, dairy products and pro-tein, tend to have high rates of colorectal cancer; coun-tries such as India and China, where diets are traditionally
high in fiber, cereals and vegetables, tend to have lowrates. People who migrate from a low-rate to a high-ratecountry—such as Greek migrants to Australia—tend to de-velop high rates of the disease as they acquire the habitsof the host country, especially diet. The role of individualelements of diet in colorectal cancer is not clear, but di-etary fat is perhaps the chief suspected culprit. There isalso evidence supporting a beneficial effect from the con-sumption of vegetables.
In most industrial countries, mortality rates from col-orectal cancer have declined in recent years because ofgreater use of early-detection methods and also, possibly,because of increasing awareness of the hazards of rich di-ets. A significant exception to the overall trend is in Japan,where rates have more than doubled since the 1950s astraditional diets were replaced by richer foods.
Exposure in the workplace to carcinogens such as as-bestos may explain, at least in part, the high rates in Hun-gary and the former Czechoslovakia, where environmen-tal safeguards have been lax, and in the northeastern U.S.Men have more exposure to workplace carcinogens thanwomen do, which may help explain why rates for womenare generally below those for men. —Rodger Doyle
Age-adjusted rates are shown for 36 industrial countries tabulated by the U.S. Centers for Disease Control and Prevention. Also shown are data for 13 developing countries (stars), as estimated from incidence data supplied by the World Health Organization. Data for most countries are for 1989, 1990 or 1991. Data for the individual successor states to the U.S.S.R.,Yugoslavia and Czechoslovakia are not available separately.
U.S. BLACKS
COSTA RICA
U.S.WHITES
30 OR MORE PER 100,000
20 TO 29.9 PER 100,000
LESS THAN 20 PER 100,000
NOT STATISTICALLY SIGNIFICANT OR NO DATA
GAMBIA
ISRAELKUWAIT
SINGAPORE
HONG KONG
BR
YA
N C
HR
IST
IEColorectal Cancer Mortality among Men
Copyright 1995 Scientific American, Inc.