Embed Size (px)
Citation preview
Colorectal CancerAn oncologists perspective
SpR Teaching Dec 2012Erica Beaumont

Summary
• Neoadjuvant Radiotherapy for rectal cancer• Neoadjuvant Chemotherapy for colon cancer• Adjuvant chemotherapy• Liver metastases• Palliative treatments
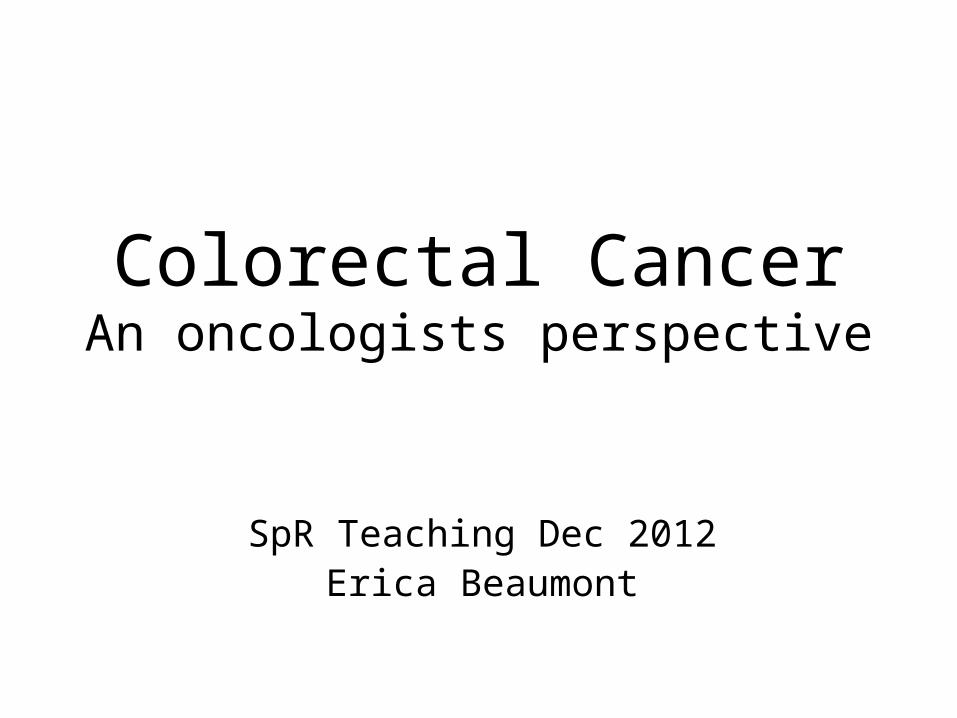
The MDT
Neoadjuvant Radiotherapy
• Operable rectal cancer (SCPRT)
• Inoperable / threatened CRM (CRT)
• Modern Context– MRI staging– TME
• Gina Brown et al. Radiol 1999;211:215-222
• MERCURY study gp. Diagnostic accuracy of preop MRI in prediciting curative
resection of rectal cancer: prospective observational study. BMJ 2006; 333: 779
MERCURY Study
• 428 pts
• MRI mesorectal fascia involvement by tumour significantly predicted for local recurrence
• DFS and OS showed that avoidance of preop RT safe in patients with MRI defined good prognosis disease (3% local recurrence)
• Allows stratification of patients and better targeting of preoperative radiotherapy for reduced patient toxicity and morbidity
• Phase II/III trials to identification of key imaging predictors of patients at risk of developing metastatic disease on initial staging
MERCURY staging study in rectal cancer Bmj, 2006; Salerno,Daniels et al. Dis Colon Rectum, 2009).
TME Surgery
• Total mesorectal excision reduces local recurrence rates
• 30-40% without TME, 3.7% with TME
• TME varies between surgeons (experience, training technique )
• How can oncologists assess quality of surgery? Surgeons objectively assess Sx?
Heald Lancet 1986; 1(8496):1479-82Heald Lancet 1993; 341(8843):457-60
Quality of Surgery
• Quirke
– Raised awareness of importance the circumferential resection margin and quality of TME specimen
– Developed graded assessment of TME
– Used in Dutch study & CR07
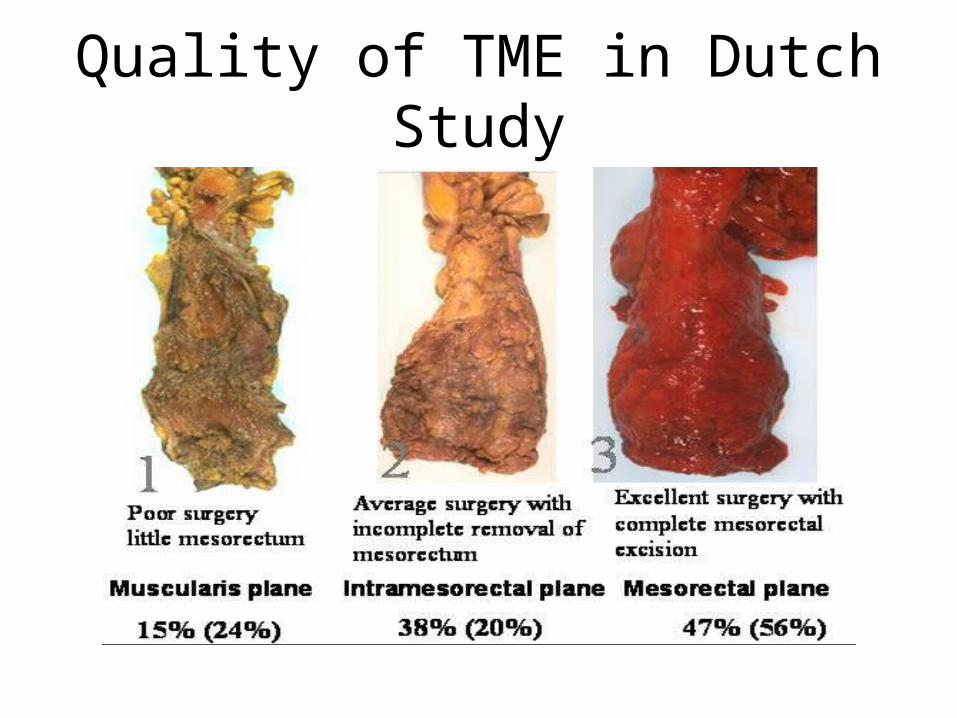
Quality of TME in Dutch Study
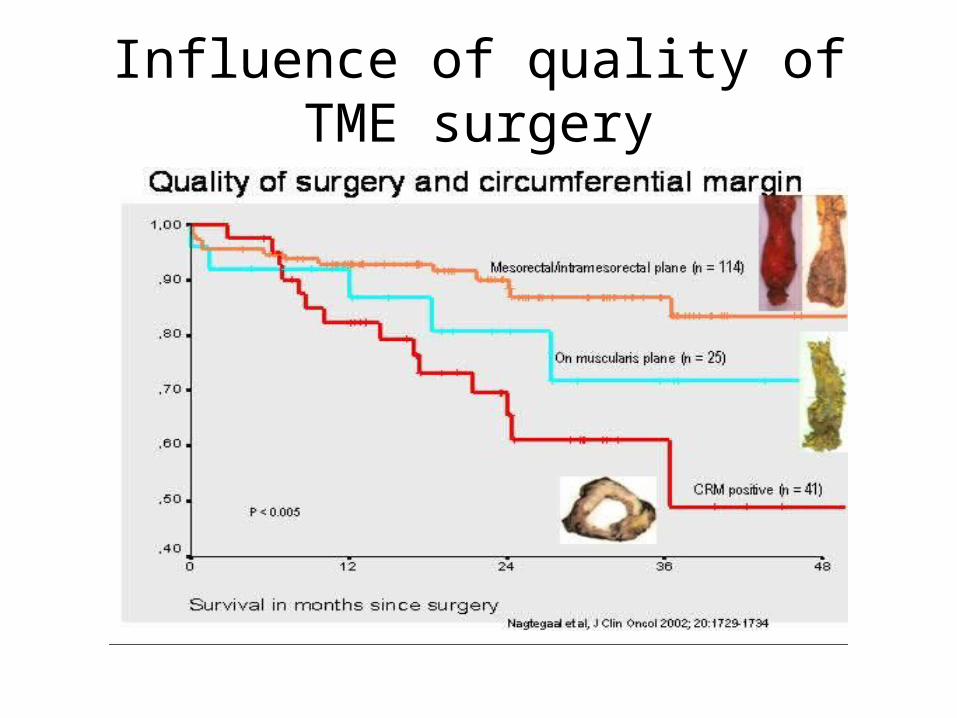
Influence of quality of TME surgery
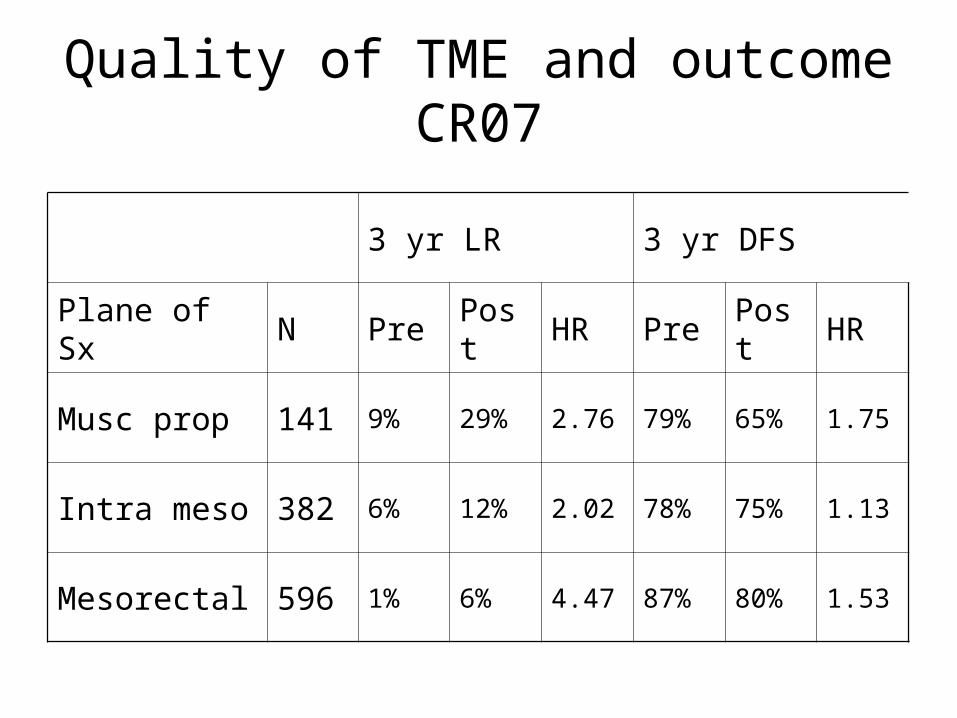
Quality of TME and outcome CR07
3 yr LR 3 yr DFS
Plane of Sx N Pre Post HR Pre Post HR
Musc prop 141 9% 29% 2.76 79% 65% 1.75
Intra meso 382 6% 12% 2.02 78% 75% 1.13
Mesorectal 596 1% 6% 4.47 87% 80% 1.53
Potential benefits of neoadjuvant RT
• Improving survival• Reducing risk of local recurrence• Improving the chance of sphincter
saving surgery• Increasing the chance of complete
resection in advanced disease
Post Op RT
• Decrease rel risk LR by 30-40%
• Absolute decrease 25.8% vs 16.7% (p<0.00002)
• Rectal cancer † decreases by 8.6%
*Lancet Meta-analysis 2001. CRC collaborative gp. >2000 pts 8 post op RCTs
Pre op RT
• >6000 pts 14 RCTs
• Decrease relative risk LR of 50-60%
• Absolute decrease 22.2% vs 12.5% (p< 0.00001)
• Rectal cancer † decrease by 22%
Lancet meta-analysis 2001
Short Course Preoperative RTSCPRT
SCPRT – Swedish studies
• >1100 pts with resectable rectal Ca Sx vs RT 25/5 + Sx (1986-1990)
– Not TME– 25/5#/1W– 5 yr LR 27% vs 12% – 5 yr OS 48% vs 58% – Only pre op study showing survival benefit – Benefits maintained - most recent update JCO 2005
Swedish Rectal Cancer Trial. N Engl J Med 1997; 336: 980-7
SCPRT – Dutch study
• Sx vs preop RT 25/5 + Sx in operable Rectal cancer
• 1748 pts underwent complete resection• 2yr LR 8.2% vs 2.4% *
• Longer FU relative benefit maintained• Also assessed importance of CRM and quality of
surgery* *
* Kapiteijn et al. Preop RT combined with TME for resectable rectal cancer. NEJM 2001; 345: 638
* * Nagtegaal et al. Dutch CCG co-operative. Macroscopic evaluation of rectal cancer specimen. 2002; 20: 1729
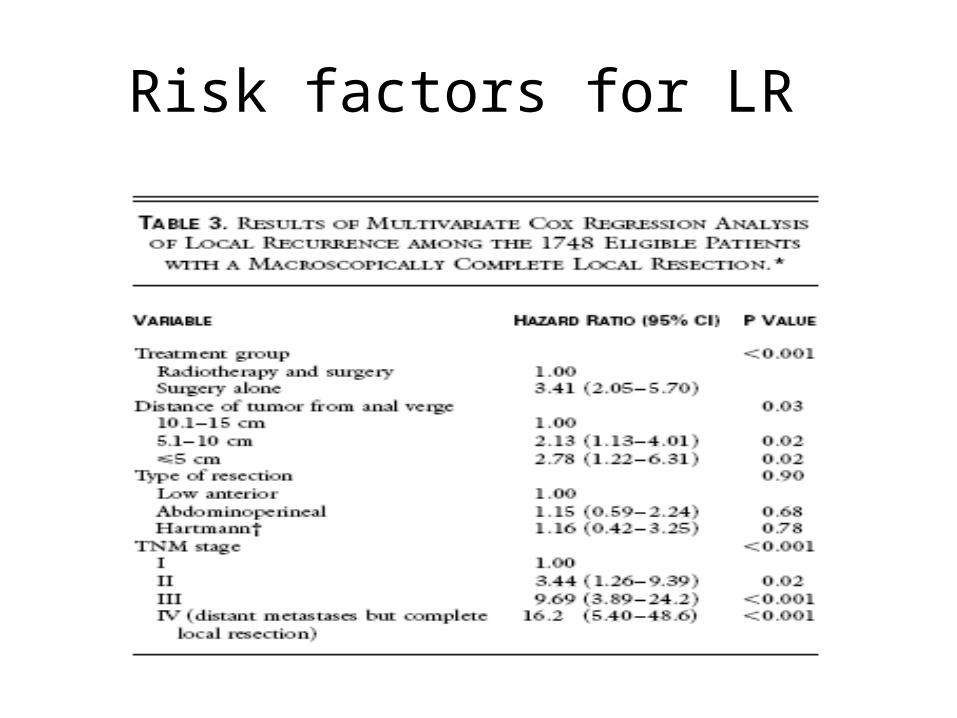
Risk factors for LR
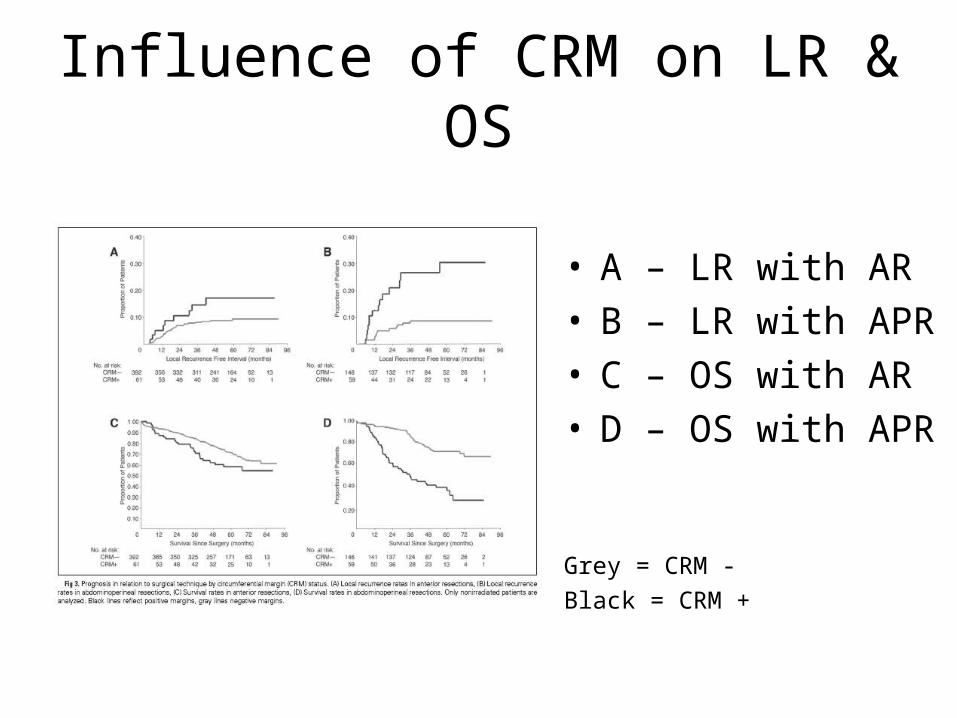
Influence of CRM on LR & OS
• A – LR with AR• B – LR with APR• C – OS with AR• D – OS with APR
Grey = CRM -
Black = CRM +

Low rectal cancers have worse outcomes
APR v AR in Dutch study
• OS– 38.5% v 57.6% (p=0.008)
• CRM+– 30.4% v 10.7% (p=0.002)
• Perforation rate– 13.7% v 2.5% (p<0.001)
SCPRT – CR07
• SCPRT vs selective post op CRT with TME Sx• 1350 pts
– 674 25/5 SCPRT– 676 Sx alone of whom 11% CRM +
• 3 yr LR 4.7% v 11.1% (HR 2.47, 95% CI 1.61-3.79)
• 3 yr DFS 79.5% v 74.9% (HR 1.31, 95% CI 1.02-1.67)
• Benefit consistent for all levels & stages
JCO 2006 ASCO Proceedings Part I. Vol 24; No. 18S: 3511
Side effects of SCPRT
• Minimal acute toxicity
• Poor wound healing (esp perineal)
• Bowel dysfunction – faecal incontinence
• Less of a problem for patients post APR
Who should have SCPRT?
• To reduce local recurrence in:
– Low rectal cancers (APR)– Bulky T3– Node positive disease
Long Course Chemoradiotherapy
Polish study• 312 pts with rectal cancer palpable by
DRE
• Primary end point – sphincter preservation
• Secondary endpoints –LR, toxicity
• Operation specified by surgeon pre RT
• Randomised to 25/5 vs 45/25 + 5FU wk 1&5
• Reassessed to decide on final operation post RT
Bujko et al. Radioth Oncol 2004; 72: 15
Polish study
• No difference in sphincter-preservation rates
• More acute Gd 3 & 4 toxicity with CRT– 18% v 3% (p=0.001)
• More pCR, less N+ & CRM+ with CRT– 16.1% v 0.7%, 31.6% v 47.6%, 4.4%v 12.9%
Polish study
• No difference late toxicity– 28.3% v 27%
• No difference in 4 yr LR– 15.6% v 10.6% (p=0.21)
Why give CRT?
• Downstage inoperable tumours (but is there a role for SCPRT?)
• Downstage tumours where there is a threatened CRM (by primary or node)
Practicalities of RT
• Tattoos
• Empty rectum, full bladder
• CT scan
• SCPRT: 5 daily treatments the week before surgery
• CRT: 25-28 daily treatments with bd capecitabine chemotherapy
Toxicities of RT
• Acute: sore skin, tiredness, nausea, diarrhoea, PR bleeding, urinary
• Late: bowel dysfunction, urinary, small bowel stricture, infertility, menopause, poor wound healing, vaginal stricture, impotence, pelvic bone fragility, risk of second malignancy
Planning RT
• CT scan
• Fields vs volumes
• Aristotle trial
• Include – mesorectum– Extension of tumour beyond mesorectum
(+margin)– Sup: sacral promontory– Inf: obturator foramen, or 2-3cm below tumour
Adjuvant Radiotherapy
• Post-op if positive margin (R1 resection)
• Only if no pre-op RT given
• Not as effective as pre-op RT
• Better than nothing
Neoadjuvant chemotherapy for colon cancer
FOXTROT trial
• Ongoing
• Initial data: 150 patients
• Locally advanced (T3/4) colon tumours on CT
• 3 cycles (6 weeks) FOLFOX chemo and Surgery vs Surgery alone
FOXTROT
• No diff post-op morbidity (p=0.8)
• Decreased T and N stage with neoadjuvant chemo (p=0.04)
• Decreased margin involvement (p=0.002)
Lancet Oncol 2012; 13:1152-60
Adjuvant Chemotherapy
Rectal Cancer
• All data extrapolated from colon cancer
• SCPRT – does not downstage cancer
• CRT – downstages cancer
• Treat on initial clinical staging
• Chronicle trial failed to recruit
• Good prognostic group: ypT0 ypN0 M0– Distant metastases 8.9%, 5yr DFS 85%
Colon cancer
• Initial studies done with 5FU
• Intergroup 035 (5FU vs no chemo)– 5yr OS benefit for Dukes C 13%– 5yr OS benefit for Dukes B 3-5%
• X-ACT (capecitabine vs 5FU)– 4% benefit for cap
• MOSAIC (5FU /oxaliplatin vs 5FU)– 3yr DFS benefit of 5%
Current Practice
• Node positive tumours– 5FU / Oxaliplatin– If less fit / elderly, Cap alone
• High risk node negative tumours– EMVI, T4, R1, Emergency presentation, <12
nodes– Cap / 5FU alone– 5FU / Oxalipatin if lots of risk factors
What does this mean for patients?
• 6 months treatment (SCOT trial ongoing)
• Tiredness, nausea, diarrhoea, stomatitis
• Palmar plantar syndrome
• Neuropathy, orolaryngeal spasm
• Haematological toxicity
• Cardiac toxicity
• Thromboembolic disease
• DPD deficiency
Follow Up
• Often CNS led
• Risk stratified
• Regular CT scans– Timing controversial– To assess for resectable liver mets
Treatment of liver metastases
Liver only disease
• Assessment– CT, MRI Liver, PET
• Resectable– Refer for surgery, ?chemo upfront– EPOC B
• Unresectable– K-Ras status– Chemotherapy for 3 months and reassess– SIRT (FOXFIRE trial)
Chemotherapy
• FOLFOX
• Every 2 weeks for 6 cycles, PICC line
• If k-ras wild-type and unresectable for Cetuximab
• mAb EGFR
• Celim study: ph 2 (Lancet Oncol 2010)– RR: 68% with FOLFOX and Cetuximab– Resectability increased from 32% to 60%
Why liver resection?
• Historically 50% colorectal cancer patients develop liver mets
• 30% present with liver mets
• Resection can give 5yr OS rates of 21-43%
After liver resection
• 3 months adjuvant chemotherapy
• 6 monthly CT scans
• Further liver resections may be possible
Presentation with liver mets
• 2 problems: liver and primary
• Which will kill patient first?
• Risk of obstruction – surgery vs stent?
• Will delaying chemo harm patient?
• Risk of micrometastatic disease elsewhere
• Synchronous resections?
• Controversial area
Lung metastases
• Extrapolate from liver data
• Resection of <5 lung mets
• No adjuvant chemo
• PULMIC study

Palliative Treatments
Primary in situ
• Does resecting the primary give an advantage?
• Assess for obstruction
• Stents
• May prevent use of bevacizumab (anti-angiogenesis Ab)
Chemotherapy
• In fit patients (PS 0-1), multiple lines of chemotherapy can give 18-24 months survival
• Chemo drugs: 5FU / Capecitabine, Oxaliplatin, Irinotecan
• Biological therapies: Cetuximab, Bevacizumab, Panitumumab
• New agents: Aflibercept, Regorafenib
Liver therapies
• RFA
• Chemoembolisation
• SIRT
Radiotherapy
• Rectal cancer– 25Gy/5# can downstage– 8Gy/1# can stop bleeding– Hard to give if has had RT pre-op
• Bone mets
• Back pain from para-aortic disease
• Lung met with haemoptysis