Embed Size (px)
Citation preview
Hematology 2002 511
Color Figures
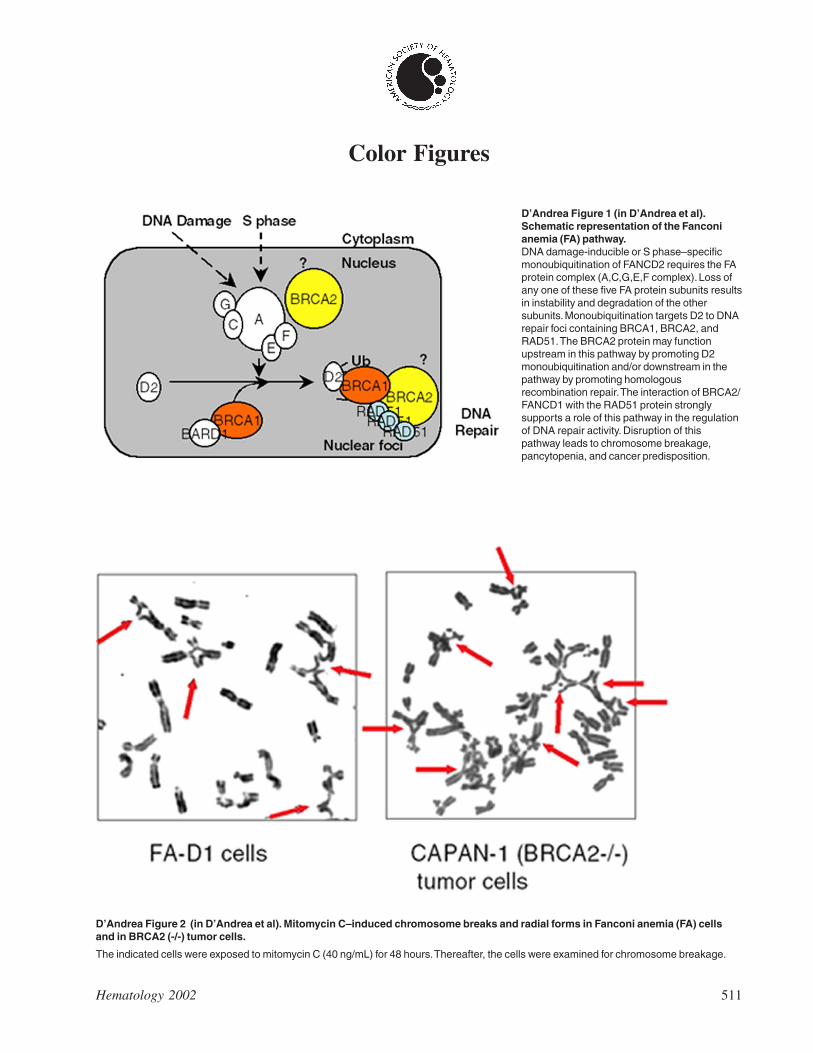
D’Andrea Figure 1 (in D’Andrea et al).Schematic representation of the Fanconianemia (FA) pathway.DNA damage-inducible or S phase–specificmonoubiquitination of FANCD2 requires the FAprotein complex (A,C,G,E,F complex). Loss ofany one of these five FA protein subunits resultsin instability and degradation of the othersubunits. Monoubiquitination targets D2 to DNArepair foci containing BRCA1, BRCA2, andRAD51. The BRCA2 protein may functionupstream in this pathway by promoting D2monoubiquitination and/or downstream in thepathway by promoting homologousrecombination repair. The interaction of BRCA2/FANCD1 with the RAD51 protein stronglysupports a role of this pathway in the regulationof DNA repair activity. Disruption of thispathway leads to chromosome breakage,pancytopenia, and cancer predisposition.
D’Andrea Figure 2 (in D’Andrea et al). Mitomycin C–induced chromosome breaks and radial forms in Fanconi anemia (FA) cellsand in BRCA2 (-/-) tumor cells.
The indicated cells were exposed to mitomycin C (40 ng/mL) for 48 hours. Thereafter, the cells were examined for chromosome breakage.
512 American Society of Hematology
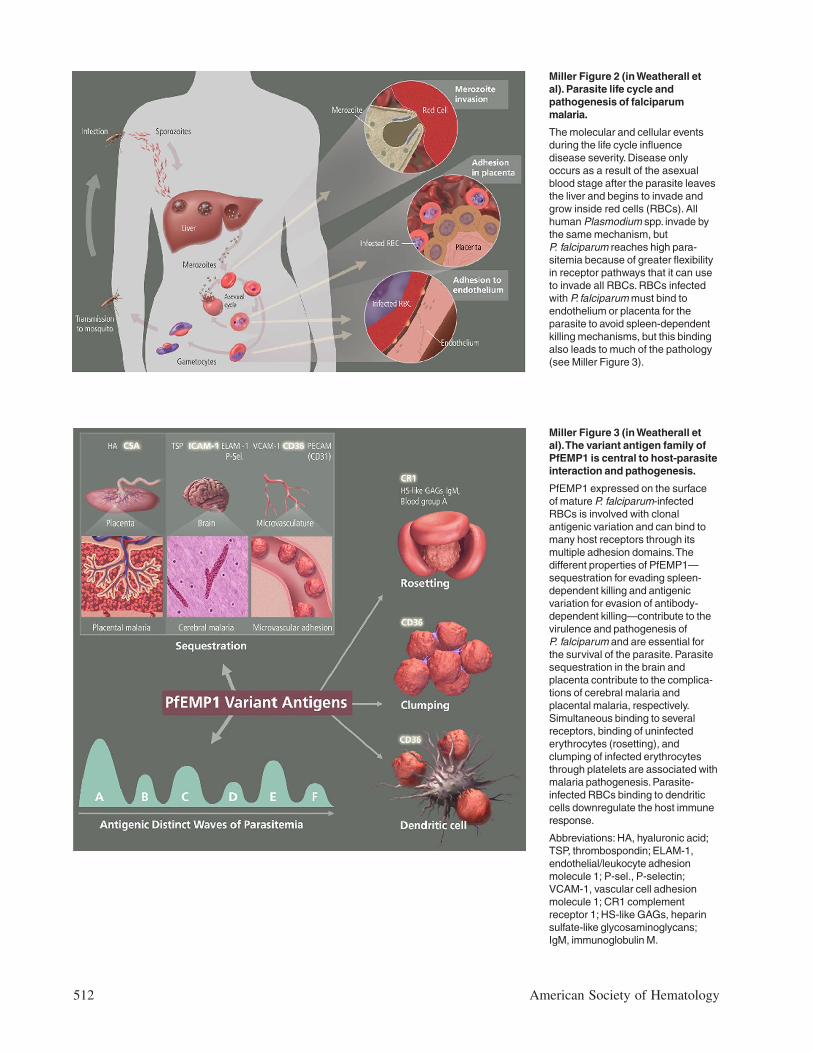
Miller Figure 3 (in Weatherall etal). The variant antigen family ofPfEMP1 is central to host-parasiteinteraction and pathogenesis.
PfEMP1 expressed on the surfaceof mature P. falciparum-infectedRBCs is involved with clonalantigenic variation and can bind tomany host receptors through itsmultiple adhesion domains. Thedifferent properties of PfEMP1—sequestration for evading spleen-dependent killing and antigenicvariation for evasion of antibody-dependent killing—contribute to thevirulence and pathogenesis ofP. falciparum and are essential forthe survival of the parasite. Parasitesequestration in the brain andplacenta contribute to the complica-tions of cerebral malaria andplacental malaria, respectively.Simultaneous binding to severalreceptors, binding of uninfectederythrocytes (rosetting), andclumping of infected erythrocytesthrough platelets are associated withmalaria pathogenesis. Parasite-infected RBCs binding to dendriticcells downregulate the host immuneresponse.
Abbreviations: HA, hyaluronic acid;TSP, thrombospondin; ELAM-1,endothelial/leukocyte adhesionmolecule 1; P-sel., P-selectin;VCAM-1, vascular cell adhesionmolecule 1; CR1 complementreceptor 1; HS-like GAGs, heparinsulfate-like glycosaminoglycans;IgM, immunoglobulin M.
Miller Figure 2 (in Weatherall etal). Parasite life cycle andpathogenesis of falciparummalaria.
The molecular and cellular eventsduring the life cycle influencedisease severity. Disease onlyoccurs as a result of the asexualblood stage after the parasite leavesthe liver and begins to invade andgrow inside red cells (RBCs). Allhuman Plasmodium spp. invade bythe same mechanism, butP. falciparum reaches high para-sitemia because of greater flexibilityin receptor pathways that it can useto invade all RBCs. RBCs infectedwith P. falciparum must bind toendothelium or placenta for theparasite to avoid spleen-dependentkilling mechanisms, but this bindingalso leads to much of the pathology(see Miller Figure 3).
Hematology 2002 513
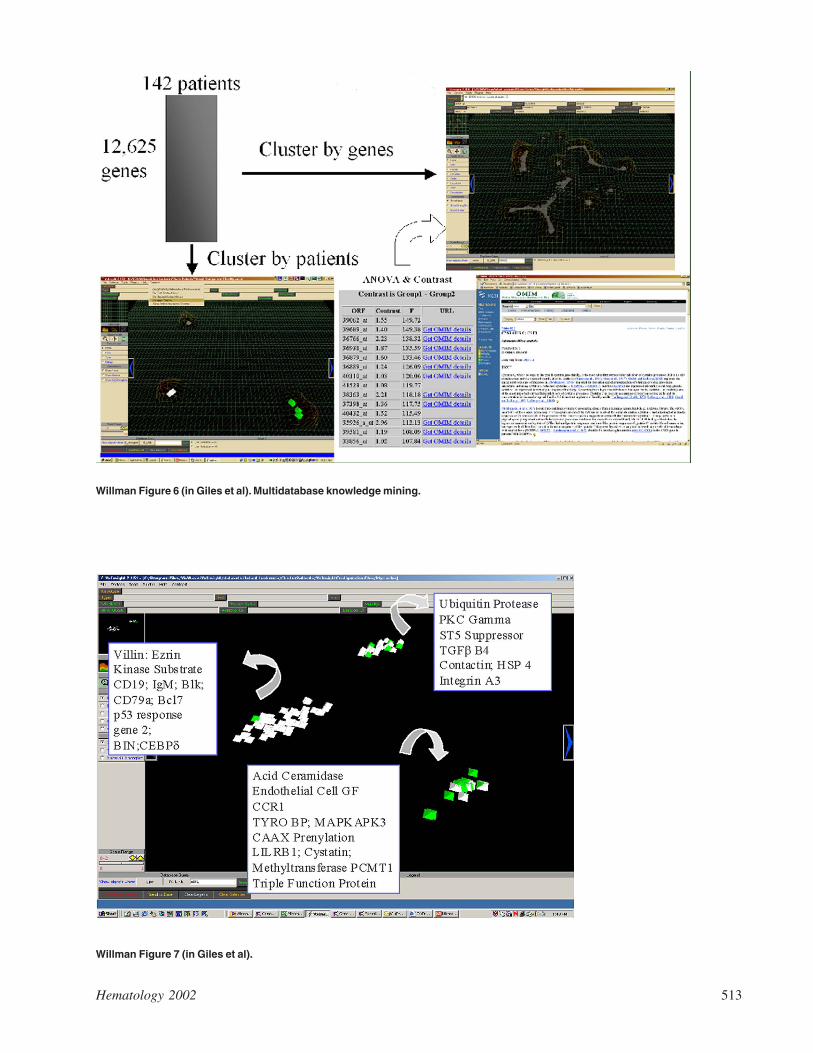
Willman Figure 6 (in Giles et al). Multidatabase knowledge mining.
Willman Figure 7 (in Giles et al).
514 American Society of Hematology
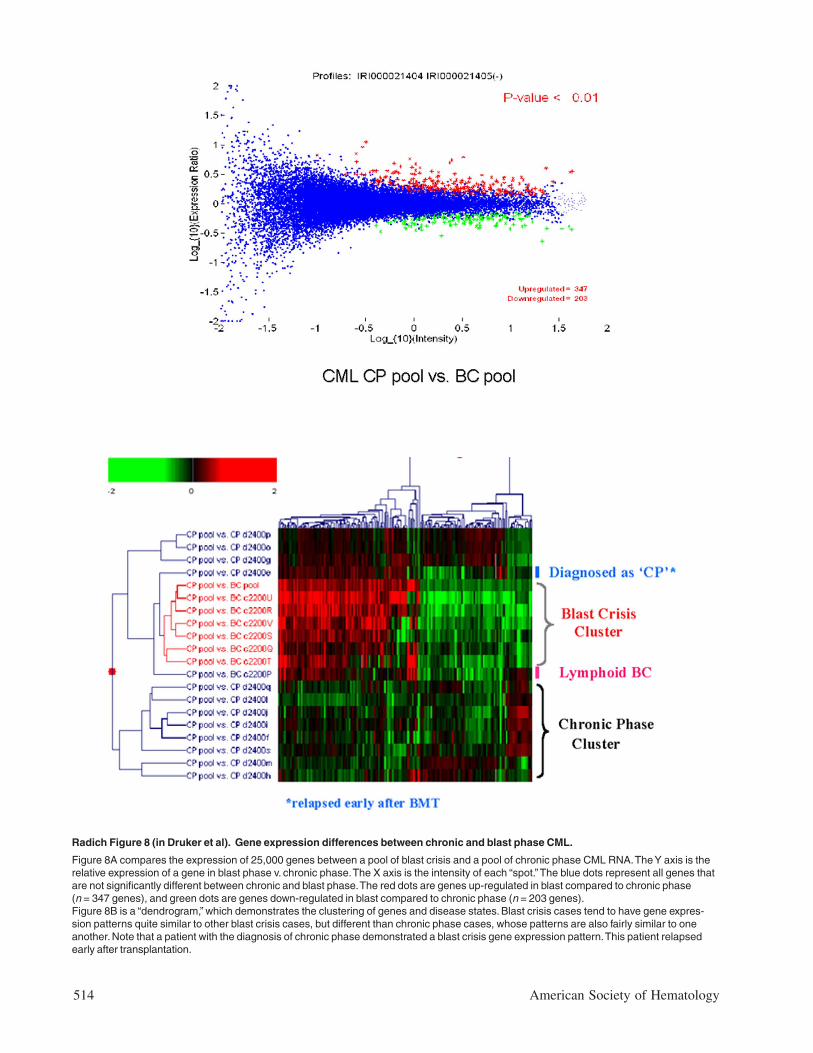
Radich Figure 8 (in Druker et al). Gene expression differences between chronic and blast phase CML.
Figure 8A compares the expression of 25,000 genes between a pool of blast crisis and a pool of chronic phase CML RNA. The Y axis is therelative expression of a gene in blast phase v. chronic phase. The X axis is the intensity of each “spot.” The blue dots represent all genes thatare not significantly different between chronic and blast phase. The red dots are genes up-regulated in blast compared to chronic phase(n = 347 genes), and green dots are genes down-regulated in blast compared to chronic phase (n = 203 genes).Figure 8B is a “dendrogram,” which demonstrates the clustering of genes and disease states. Blast crisis cases tend to have gene expres-sion patterns quite similar to other blast crisis cases, but different than chronic phase cases, whose patterns are also fairly similar to oneanother. Note that a patient with the diagnosis of chronic phase demonstrated a blast crisis gene expression pattern. This patient relapsedearly after transplantation.
Hematology 2002 515
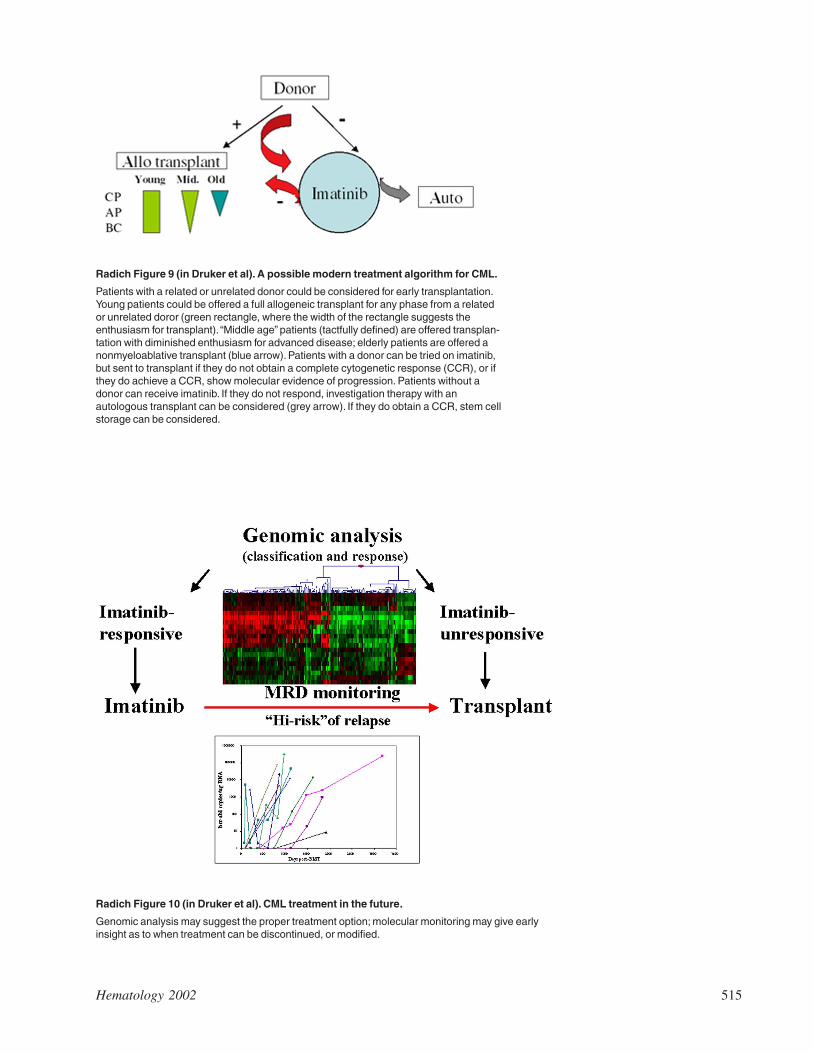
Radich Figure 9 (in Druker et al). A possible modern treatment algorithm for CML.
Patients with a related or unrelated donor could be considered for early transplantation.Young patients could be offered a full allogeneic transplant for any phase from a relatedor unrelated doror (green rectangle, where the width of the rectangle suggests theenthusiasm for transplant). “Middle age” patients (tactfully defined) are offered transplan-tation with diminished enthusiasm for advanced disease; elderly patients are offered anonmyeloablative transplant (blue arrow). Patients with a donor can be tried on imatinib,but sent to transplant if they do not obtain a complete cytogenetic response (CCR), or ifthey do achieve a CCR, show molecular evidence of progression. Patients without adonor can receive imatinib. If they do not respond, investigation therapy with anautologous transplant can be considered (grey arrow). If they do obtain a CCR, stem cellstorage can be considered.
Radich Figure 10 (in Druker et al). CML treatment in the future.
Genomic analysis may suggest the proper treatment option; molecular monitoring may give earlyinsight as to when treatment can be discontinued, or modified.
516 American Society of Hematology
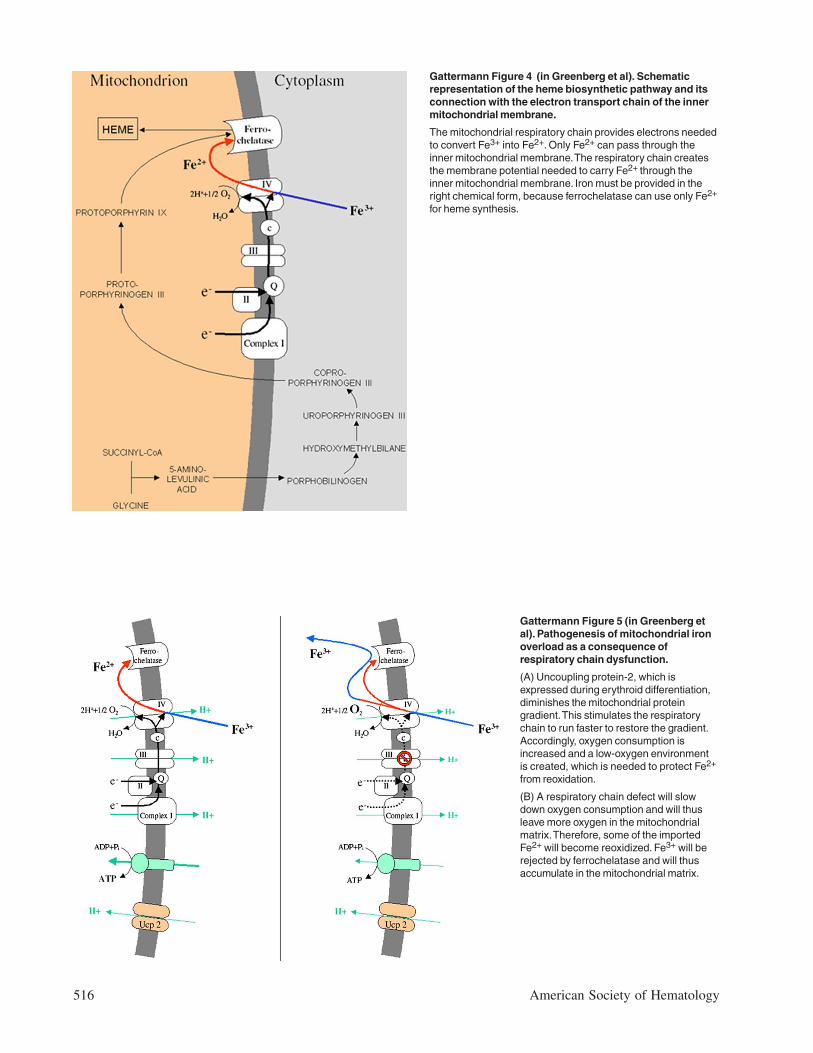
Gattermann Figure 4 (in Greenberg et al). Schematicrepresentation of the heme biosynthetic pathway and itsconnection with the electron transport chain of the innermitochondrial membrane.
The mitochondrial respiratory chain provides electrons neededto convert Fe3+ into Fe2+. Only Fe2+ can pass through theinner mitochondrial membrane. The respiratory chain createsthe membrane potential needed to carry Fe2+ through theinner mitochondrial membrane. Iron must be provided in theright chemical form, because ferrochelatase can use only Fe2+
for heme synthesis.
Gattermann Figure 5 (in Greenberg etal). Pathogenesis of mitochondrial ironoverload as a consequence ofrespiratory chain dysfunction.
(A) Uncoupling protein-2, which isexpressed during erythroid differentiation,diminishes the mitochondrial proteingradient. This stimulates the respiratorychain to run faster to restore the gradient.Accordingly, oxygen consumption isincreased and a low-oxygen environmentis created, which is needed to protect Fe2+
from reoxidation.
(B) A respiratory chain defect will slowdown oxygen consumption and will thusleave more oxygen in the mitochondrialmatrix. Therefore, some of the importedFe2+ will become reoxidized. Fe3+ will berejected by ferrochelatase and will thusaccumulate in the mitochondrial matrix.
Hematology 2002 517
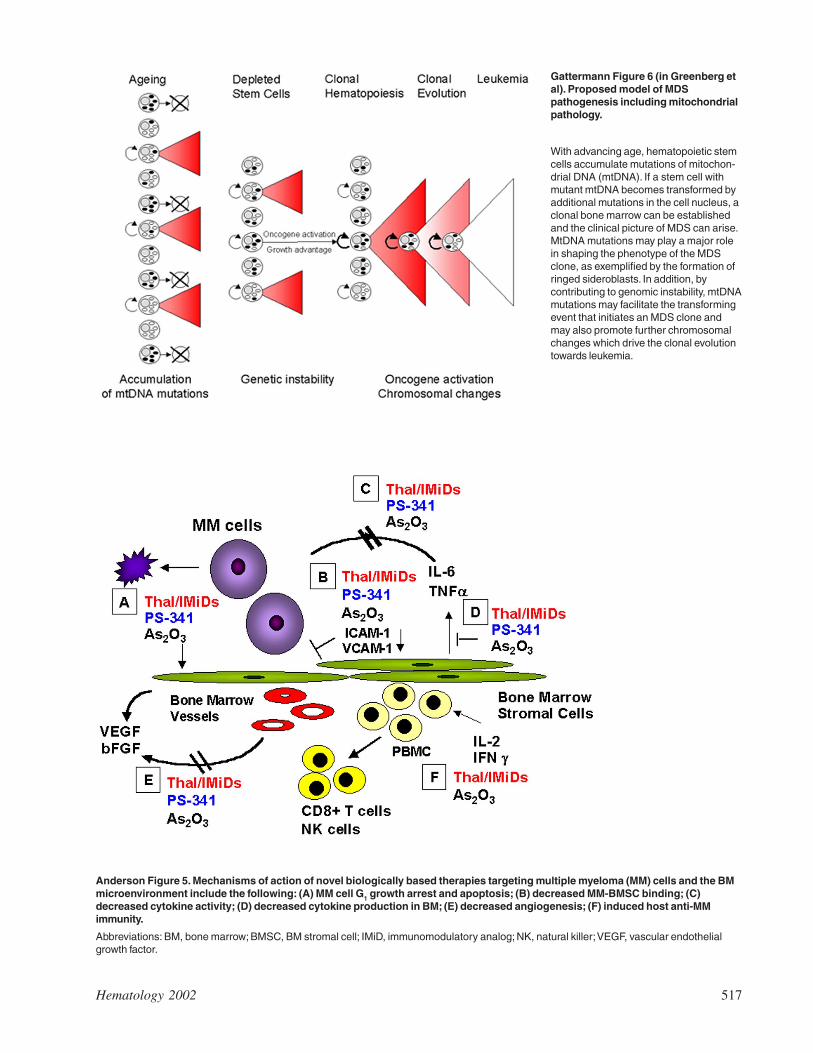
Gattermann Figure 6 (in Greenberg etal). Proposed model of MDSpathogenesis including mitochondrialpathology.
With advancing age, hematopoietic stemcells accumulate mutations of mitochon-drial DNA (mtDNA). If a stem cell withmutant mtDNA becomes transformed byadditional mutations in the cell nucleus, aclonal bone marrow can be establishedand the clinical picture of MDS can arise.MtDNA mutations may play a major rolein shaping the phenotype of the MDSclone, as exemplified by the formation ofringed sideroblasts. In addition, bycontributing to genomic instability, mtDNAmutations may facilitate the transformingevent that initiates an MDS clone andmay also promote further chromosomalchanges which drive the clonal evolutiontowards leukemia.
Anderson Figure 5. Mechanisms of action of novel biologically based therapies targeting multiple myeloma (MM) cells and the BMmicroenvironment include the following: (A) MM cell G1 growth arrest and apoptosis; (B) decreased MM-BMSC binding; (C)decreased cytokine activity; (D) decreased cytokine production in BM; (E) decreased angiogenesis; (F) induced host anti-MMimmunity.
Abbreviations: BM, bone marrow; BMSC, BM stromal cell; IMiD, immunomodulatory analog; NK, natural killer; VEGF, vascular endothelialgrowth factor.
518 American Society of Hematology
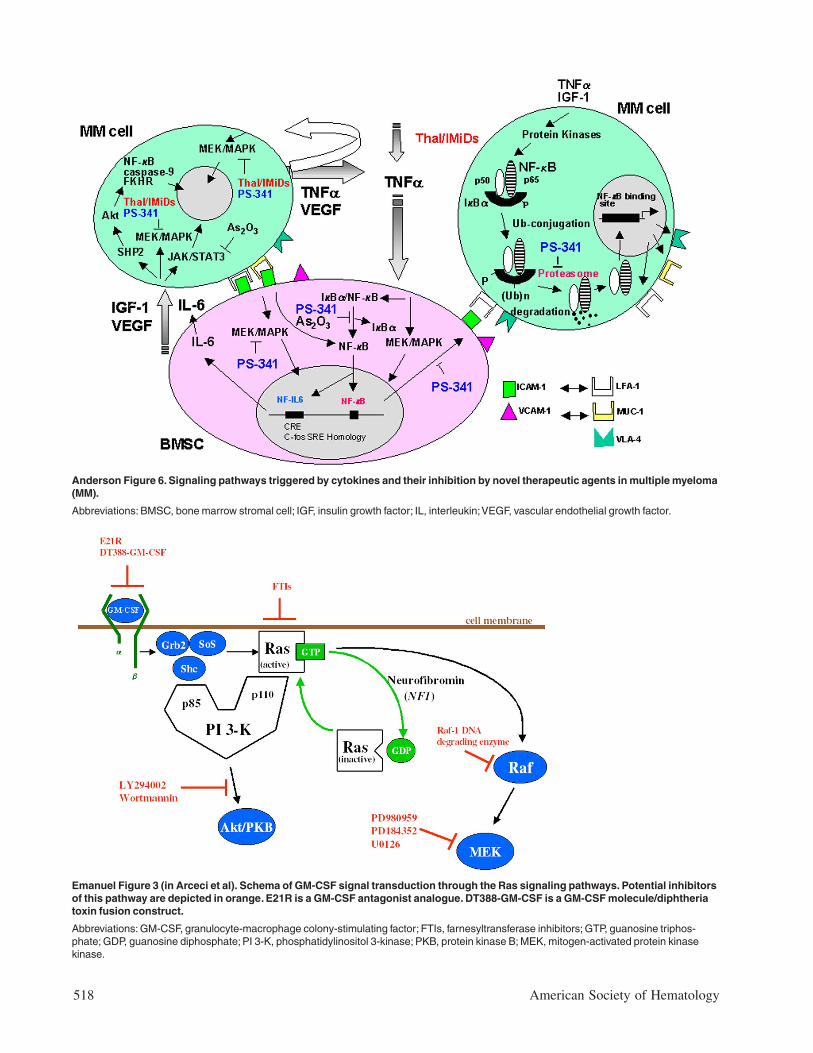
Emanuel Figure 3 (in Arceci et al). Schema of GM-CSF signal transduction through the Ras signaling pathways. Potential inhibitorsof this pathway are depicted in orange. E21R is a GM-CSF antagonist analogue. DT388-GM-CSF is a GM-CSF molecule/diphtheriatoxin fusion construct.
Abbreviations: GM-CSF, granulocyte-macrophage colony-stimulating factor; FTIs, farnesyltransferase inhibitors; GTP, guanosine triphos-phate; GDP, guanosine diphosphate; PI 3-K, phosphatidylinositol 3-kinase; PKB, protein kinase B; MEK, mitogen-activated protein kinasekinase.
Anderson Figure 6. Signaling pathways triggered by cytokines and their inhibition by novel therapeutic agents in multiple myeloma(MM).
Abbreviations: BMSC, bone marrow stromal cell; IGF, insulin growth factor; IL, interleukin; VEGF, vascular endothelial growth factor.
Hematology 2002 519
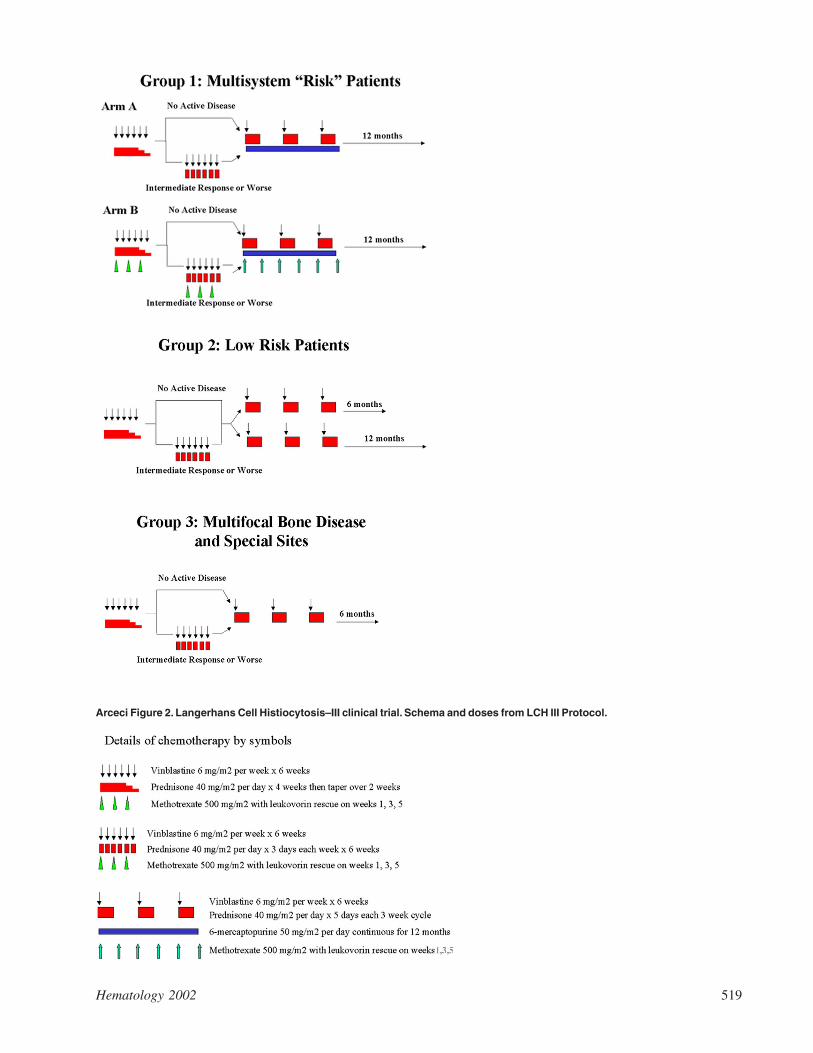
Arceci Figure 2. Langerhans Cell Histiocytosis–III clinical trial. Schema and doses from LCH III Protocol.
520 American Society of Hematology
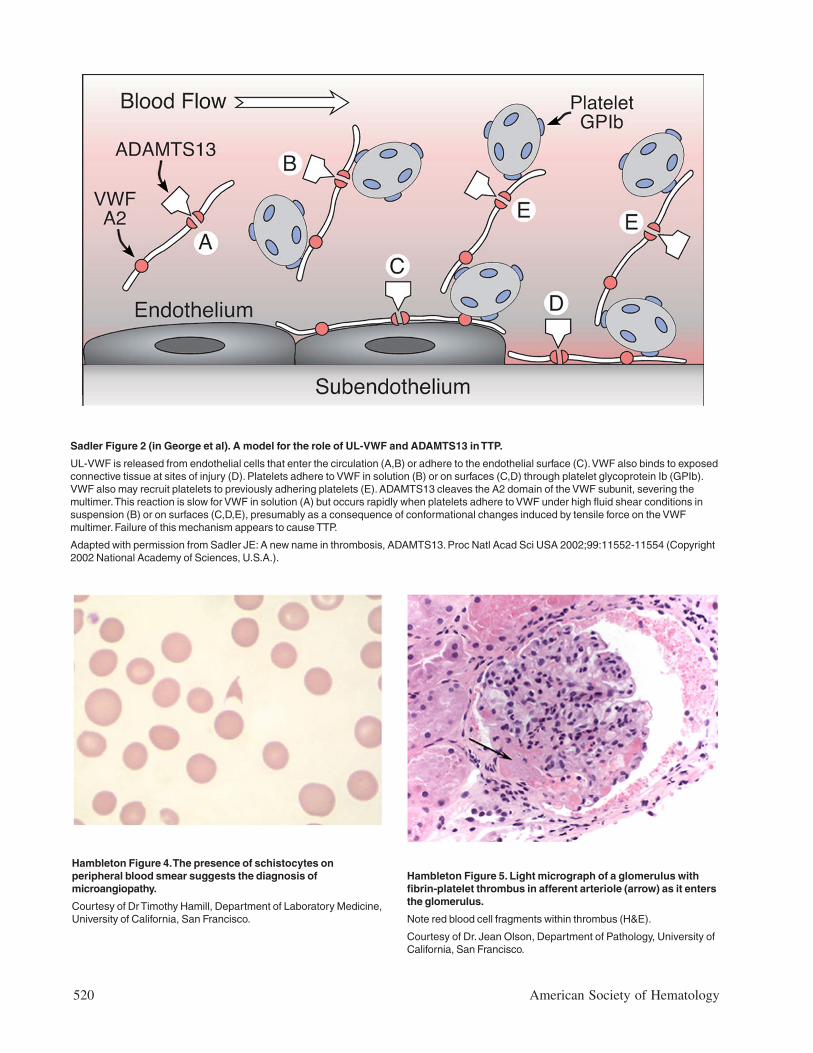
Hambleton Figure 5. Light micrograph of a glomerulus withfibrin-platelet thrombus in afferent arteriole (arrow) as it entersthe glomerulus.
Note red blood cell fragments within thrombus (H&E).
Courtesy of Dr. Jean Olson, Department of Pathology, University ofCalifornia, San Francisco.
Hambleton Figure 4. The presence of schistocytes onperipheral blood smear suggests the diagnosis ofmicroangiopathy.
Courtesy of Dr Timothy Hamill, Department of Laboratory Medicine,University of California, San Francisco.
Sadler Figure 2 (in George et al). A model for the role of UL-VWF and ADAMTS13 in TTP.
UL-VWF is released from endothelial cells that enter the circulation (A,B) or adhere to the endothelial surface (C). VWF also binds to exposedconnective tissue at sites of injury (D). Platelets adhere to VWF in solution (B) or on surfaces (C,D) through platelet glycoprotein Ib (GPIb).VWF also may recruit platelets to previously adhering platelets (E). ADAMTS13 cleaves the A2 domain of the VWF subunit, severing themultimer. This reaction is slow for VWF in solution (A) but occurs rapidly when platelets adhere to VWF under high fluid shear conditions insuspension (B) or on surfaces (C,D,E), presumably as a consequence of conformational changes induced by tensile force on the VWFmultimer. Failure of this mechanism appears to cause TTP.
Adapted with permission from Sadler JE: A new name in thrombosis, ADAMTS13. Proc Natl Acad Sci USA 2002;99:11552-11554 (Copyright2002 National Academy of Sciences, U.S.A.).
Hematology 2002 521
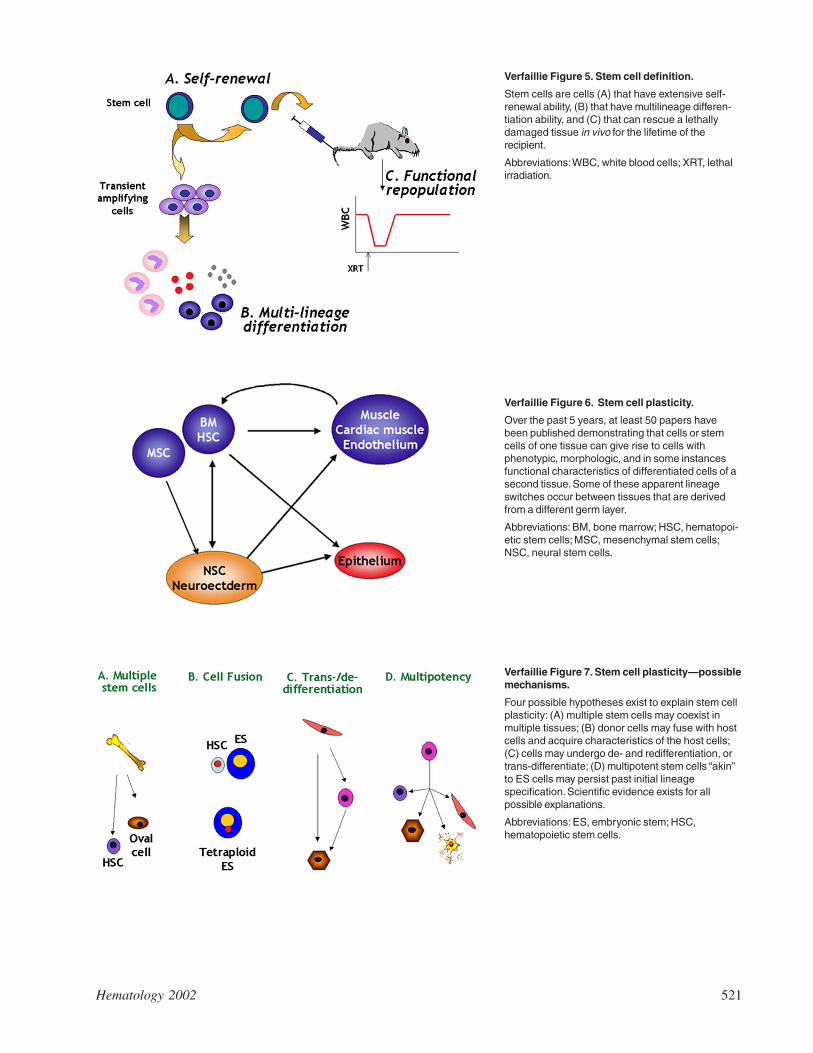
Verfaillie Figure 5. Stem cell definition.
Stem cells are cells (A) that have extensive self-renewal ability, (B) that have multilineage differen-tiation ability, and (C) that can rescue a lethallydamaged tissue in vivo for the lifetime of therecipient.
Abbreviations: WBC, white blood cells; XRT, lethalirradiation.
Verfaillie Figure 6. Stem cell plasticity.
Over the past 5 years, at least 50 papers havebeen published demonstrating that cells or stemcells of one tissue can give rise to cells withphenotypic, morphologic, and in some instancesfunctional characteristics of differentiated cells of asecond tissue. Some of these apparent lineageswitches occur between tissues that are derivedfrom a different germ layer.
Abbreviations: BM, bone marrow; HSC, hematopoi-etic stem cells; MSC, mesenchymal stem cells;NSC, neural stem cells.
Verfaillie Figure 7. Stem cell plasticity—possiblemechanisms.
Four possible hypotheses exist to explain stem cellplasticity: (A) multiple stem cells may coexist inmultiple tissues; (B) donor cells may fuse with hostcells and acquire characteristics of the host cells;(C) cells may undergo de- and redifferentiation, ortrans-differentiate; (D) multipotent stem cells “akin”to ES cells may persist past initial lineagespecification. Scientific evidence exists for allpossible explanations.
Abbreviations: ES, embryonic stem; HSC,hematopoietic stem cells.
522 American Society of Hematology
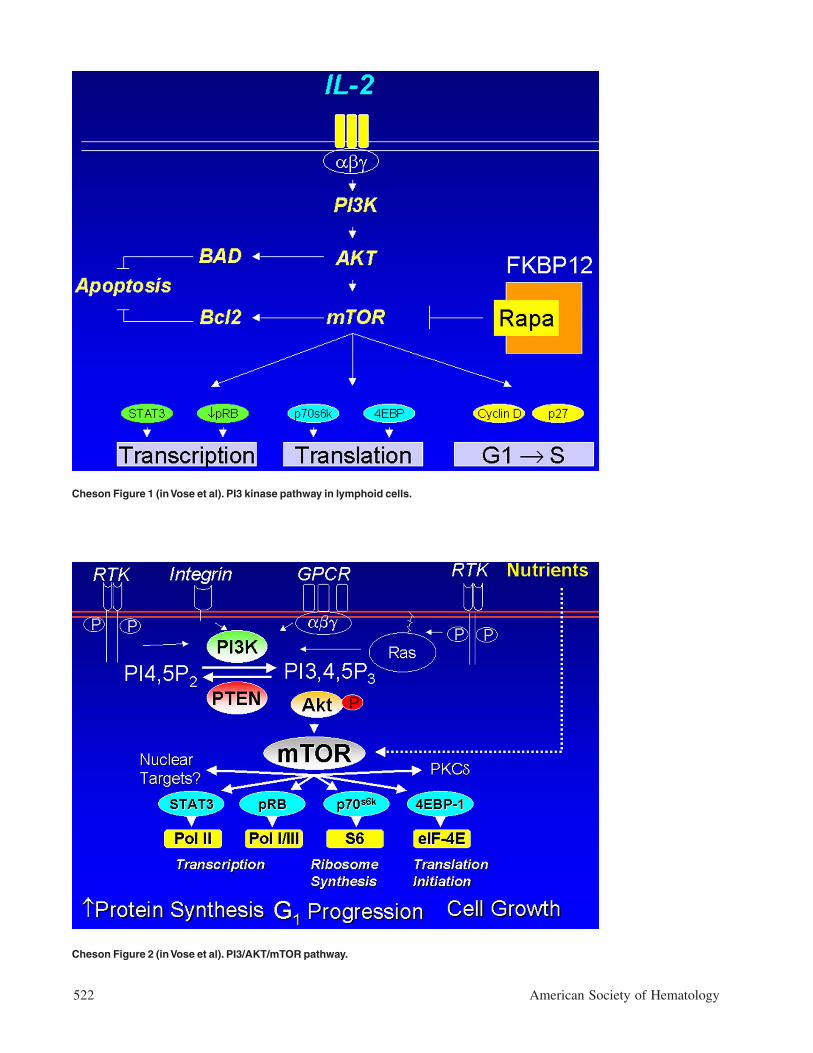
Cheson Figure 1 (in Vose et al). PI3 kinase pathway in lymphoid cells.
Cheson Figure 2 (in Vose et al). PI3/AKT/mTOR pathway.
Hematology 2002 523
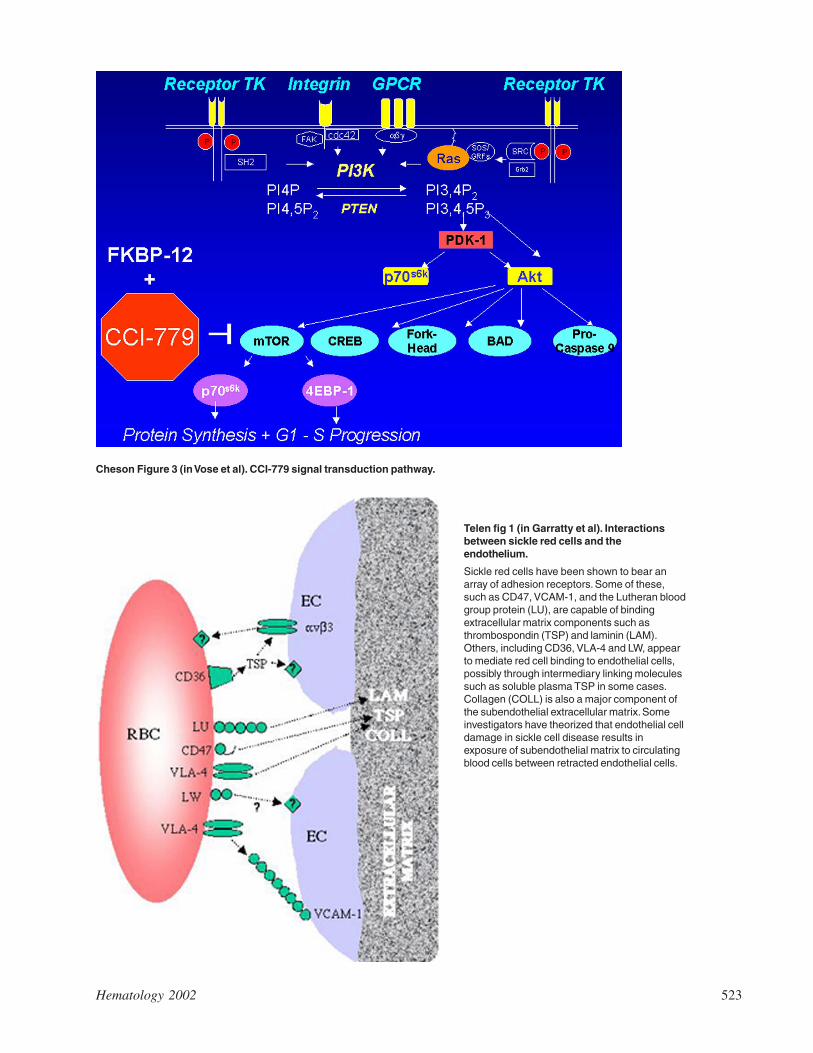
Cheson Figure 3 (in Vose et al). CCI-779 signal transduction pathway.
Telen fig 1 (in Garratty et al). Interactionsbetween sickle red cells and theendothelium.
Sickle red cells have been shown to bear anarray of adhesion receptors. Some of these,such as CD47, VCAM-1, and the Lutheran bloodgroup protein (LU), are capable of bindingextracellular matrix components such asthrombospondin (TSP) and laminin (LAM).Others, including CD36, VLA-4 and LW, appearto mediate red cell binding to endothelial cells,possibly through intermediary linking moleculessuch as soluble plasma TSP in some cases.Collagen (COLL) is also a major component ofthe subendothelial extracellular matrix. Someinvestigators have theorized that endothelial celldamage in sickle cell disease results inexposure of subendothelial matrix to circulatingblood cells between retracted endothelial cells.

524 American Society of Hematology


















![Final Manuscript with Color Figures[1]](https://img.pdfslide.us/doc/110x75/55ac72981a28ab7f278b45b7/final-manuscript-with-color-figures1.jpg)









