Embed Size (px)
Citation preview

Colonic Atresia
Melissa Wong, M.D. SUNY Downstate Medical Center 24 July 2014
www.downstatesurgery.org

Case Presentation
2d old F, born 41+2 GA ● Pregnancy:
o recurrent UTIs o normal amniocentesis o prenatal US: cystic structure adjacent to GB (not
seen on subsequent study) o C-section for NRFHT
● Birth weight 3070 g ● Apgar 91’ / 95’ ● Breastfed ● “Passed meconium but no BM”
www.downstatesurgery.org

Case Presentation
● DoL 2: bilious “spit up”, abdomen distended o NPO
o transfer to NICU
o hydrated, electrolytes corrected
o Ped Surg consult
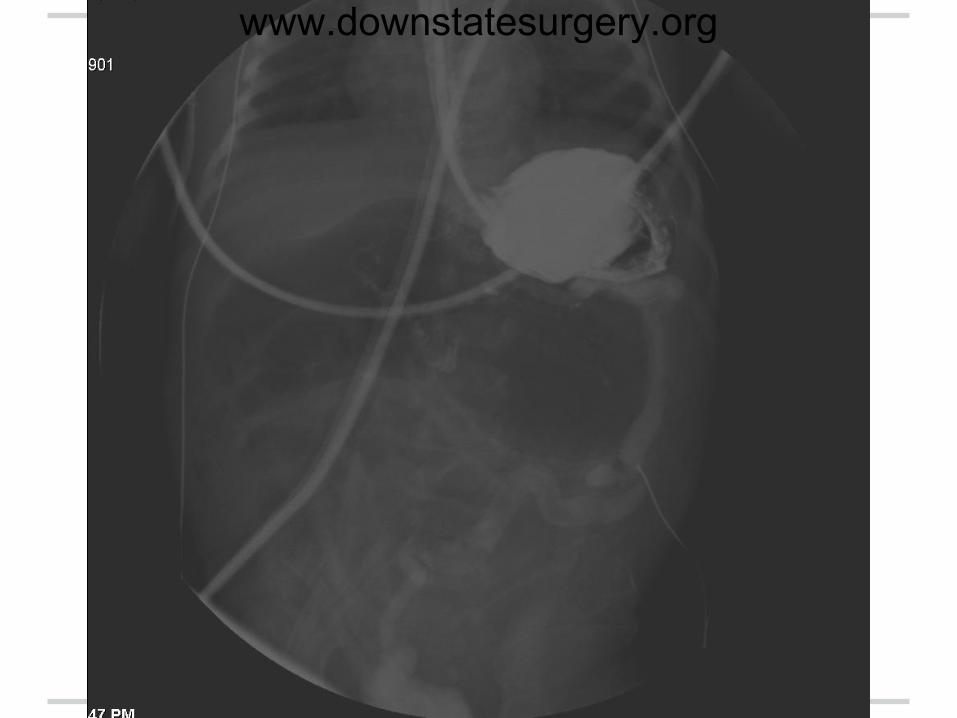
o UGIS and BE on DoL 3
www.downstatesurgery.org
Case Presentation
Physical Exam ● Vitals stable on room air ● OG sump tube ● Triangular faces, low set ears ● Abdomen soft, distended ● Normal external genitalia ● Patent anus
www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org
www.downstatesurgery.org

www.downstatesurgery.org

Operation DoL #4
Findings ● 2 colonic atresias:
o membranous atresia at hepatic flexure o blind sac atresia at R transverse colon
● proximal dilated terminal ileum & R colon; microcolon distally o jejunum collapsed
● other findings: o staggered diverticuli of distal colon o normal appendix
www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org

Operation DoL #4
Procedure ● Atresias resected ● distal colon irrigated w/ saline → patent ● stapled tapering coloplasty of dilated R colon ● hand-sewn end-to-end anastomosis x2
www.downstatesurgery.org
Pathology
● Thinned colonic wall c/w atresia ● Dilated adjacent colon ● Ganglion cells present throughout, incl
atretic & dilated parts
www.downstatesurgery.org

Post-Op Course POD 1: TPN started POD 2: Passed BM POD 4 / 7 / 11: abd distended, free air on XR → BE (+) for anastomotic leak
● 4 & 7: Ex Lap, washout, repair of anastomotic leaks (from both), omentopexy, Broviac placement
● 11: Ex Lap, resection of anastomoses x2, primary colo-colonic anastomosis
POD #13: BE shows no leak
www.downstatesurgery.org

Colonic Atresia
Melissa Wong, M.D. SUNY Downstate Medical Center 24 July 2014
www.downstatesurgery.org
History
● 1673: 1st case reported by Binninger
● 1922: 1st survivor reported by Dr. Gaub o sigmoid atresia → colostomy
● 1947: 1st case of 1º anastomosis reported
by Dr. Potts o transverse colon atresia
www.downstatesurgery.org

Epidemiology
● Intestinal atresias: 1 in 1500 - 40,000 o <10% colonic
● M = F ● full term ● 47% have other anomalies
o Gastroschisis o intestinal atresias o malrotation o Hirschsprung’s
www.downstatesurgery.org

www.downstatesurgery.org

Etiology
● Vascular o Louw & Barnard 1955: dog fetus study o mechanical:
volvulus, intussusception, gastroschisis o fetal Varicella or Borrellia infection:
injury to enteric plexus → poor vessel development → ischemia
o genetic: familial clustering
www.downstatesurgery.org

Presentation & Imaging
● bilious vomiting ● distension ● failure to pass meconium ● US
o prenatal US
● XR o dilated loops o air-fluid levels o intraperitoneal calcifications
www.downstatesurgery.org
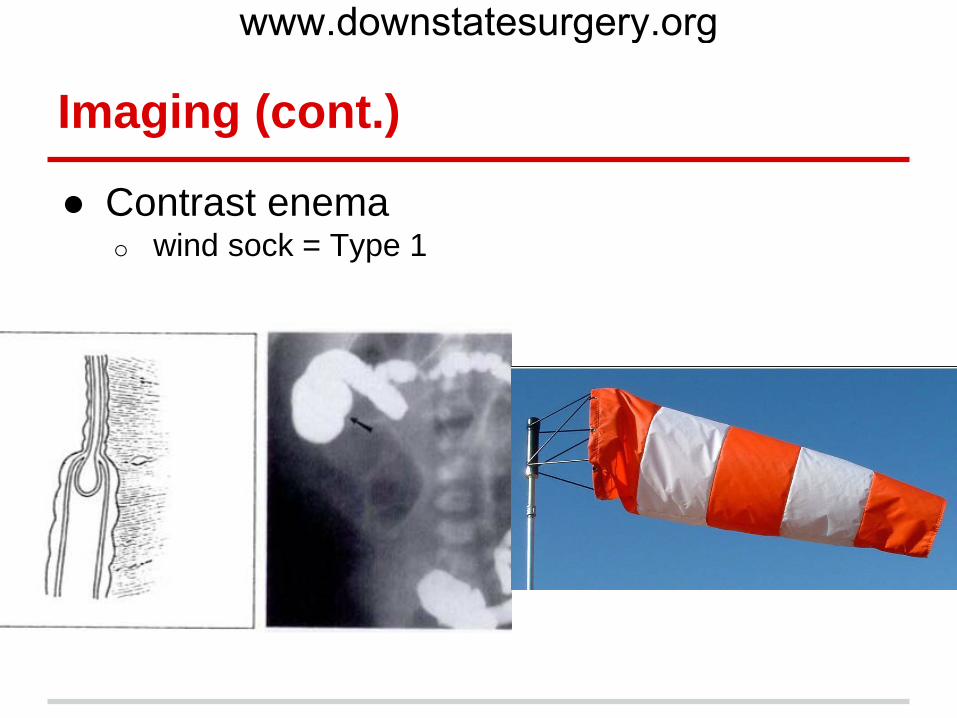
Imaging (cont.)
● Contrast enema o wind sock = Type 1
www.downstatesurgery.org

Imaging (cont.)
● Contrast enema o hook sign = Type 3a
www.downstatesurgery.org

Operative Approaches
● Historically: by location o proximal to splenic flexure → 1º anastomosis o distal → ostomy
● Calibre discrepancy
www.downstatesurgery.org

www.downstatesurgery.org

Operative Approaches
● Historically: by location o proximal to splenic flexure → 1º anastomosis o distal → ostomy
● Calibre discrepancy o ostomy o tapering o end ileostomy + cecal blow hole + mucus fistula
(Corbett, Turnock) ● Current approach: primary anastomosis
www.downstatesurgery.org

Operative Approaches
● Operate early o surgery at >72 hrs → higher mortality
o closed loop obstruction
● Check patency
● Rule out other anomalies
● Resect both atretic ends
● Decompress proximal bowel
www.downstatesurgery.org

Outcomes
● low operative mortality
● major risk factors for poor outcome: o associated anomalies
o late diagnosis/tx
o TPN-related complications (e.g. cholestatic liver
damage, line sepsis)
www.downstatesurgery.org

Summary
● Rarest type of intestinal atresia ● Probable vascular etiology ● 4 types ● Workup: AXR, BE ● OR: resect atretic ends, primary
anastomosis
www.downstatesurgery.org

References Benawra R, Puppala BL, Mangurten HH, Booth C, Bassuk A. Familial occurrence of congenital colonic atresia. J Pediatr 1981;99:435-6. Chester ST, Robinson WT. Congenital Atresia of the Transverse Colon. Ann Surg 1957 Nov;146(5):824-9. Corbett HJ, Turnock RR. An alternative management option for colonic atresia preventing loss of the ileocecal valve. J Pediatr Surg 2010;45:1380-2. Cox SG, Numanoglu A, Millar AJW, Rode H. Colonic atresia: spectrum of presentation and pitfalls in management. A review of 14 cases. Pediatr Surg Int 2005;21:813-8. Dalla Vecchia LK, Grosfeld JL, West KW, Rescorla FJ, Scherer LR, Engum SA. Intestinal Atresia and Stenosis. Arch Surg 1998 May;133:490-7. Dassinger M, Jackson R, Smith S. Management of colonic atresia with primary resection and anastomosis. Pediatr Surg Int 2009;25:579-582. England RJ, Scammell S, Murthi GV. Proximal colonic atresia: is right hemicolectomy inevitable? Pediatr Surg Int 2011;27:1059-1062. Etensel B, Temir G, Karkiner A, Melek M, Edirne Y, Karaca I, Mir E. Atresia of the Colon. J Pediatr Surg 2005;40:1258-1268. Haxhija EQ, Schalamon J, Hollwarth ME. Management of isolated and associated colonic atresia. Pediatr Surg Int 2011;27:411-6. Karnak I, Ciftci AO, Senocak ME, Tanyel FC, Buyukpamukcu N. Colonic atresia: surgical management and outcome. Pediatr Surg Int 2001;17:631-5. Louw JH, Barnard CN. Congenital Intestinal Atresia: Observations on its origin. Lancet 1955;2:1065-7. Selke AC, Jona JZ. The Hook Sign in Type 3 Congenital Colonic Atresia. Am J Roentgenol 1978 Aug;131:350-1. Watts AC, Sabharwal AJ, MacKinlay GA, Munro FD. Congenital colonic atresia: should primary anastomosis always be the goal? Pediatr Surg Int 2003;19:14-7. Winters WD, Weinberger E, Hatch E. Atresia of the Colon in Neonates: Radiographic Findings. Am J Roentgenol 1992 Dec;159:1273-6.
www.downstatesurgery.org