Embed Size (px)
Citation preview
Research in Developmental Disabilities 33 (2012) 224–228
Contents lists available at SciVerse ScienceDirect
Research in Developmental Disabilities
College students’ conceptualizations of deficits involved in mildintellectual disability
Mandi W. Musso *, Alyse A. Barker, Daniel A. Proto, Wm. Drew Gouvier
Louisiana State University, Department of Psychology, Baton Rouge, LA, USA
A R T I C L E I N F O
Article history:
Received 6 September 2011
Received in revised form 7 September 2011
Accepted 8 September 2011
Available online 11 October 2011
Keywords:
Mild intellectual disability
Mental retardation
Misconceptions
Adaptive behavior
Deficits
A B S T R A C T
Precedential rulings in recent capital murder trials may, in some cases, leave it up to a jury
to determine whether or not an individual meets criteria for an intellectual disability (ID)
and should be spared from the death penalty. Despite the potential for misconceptions
about ID to bias decisions, few empirical studies have examined the public’s
conceptualizations of individuals with ID. This study sought to examine 890 college
students’ conceptualizations of the deficits involved in mild ID. Students were asked to
respond to two online surveys about the cognitive and adaptive behavior deficits that
people with mild ID may experience. While most students were correct about basic facts,
such as ID is not contagious and not curable, there was no clear consensus regarding beliefs
about individuals with ID getting married, having children, or engaging in other
mainstream activities of adult living. Students’ responses are examined in light of results
of studies that identify and examine bona fide deficits and areas of successful
mainstreaming among persons with ID. Implications of misconceptions are discussed.
� 2011 Elsevier Ltd. All rights reserved.
1. Introduction
In 2002, a ruling on the case of Atkins v. Virginia deemed the death penalty to be a cruel and unusual punishment, and thusin violation of the Eighth Amendment, for individuals diagnosed with intellectual disability (ID; Atkins v. Virginia, 2002).Most states that enforce the death penalty have elected to resolve the issue of a defendant’s Atkins claim via a pre-trial benchhearing in which a judge rules whether or not the defendant has ID (Ellis, 2003). However, the Constitutionality of this issuehas been questioned (Ring v. Arizona, 2002). It has been argued that having a judge determine whether or not the defendanthas ID violates that individual’s Sixth Amendment rights and that the issue should be brought before a jury (Bauerman, 2005;Ellis, 2003). The determination of ID may ultimately be decided by 12 lay people who are often provided with contradictoryexpert testimony. Individuals’ preconceived notions about what mental retardation ‘‘looks like’’ could possibly bias opinions.
Few studies to date have examined individuals’ understandings of deficits involved in ID. Caruso and Hodapp (1988)surveyed college undergraduates to assess their perceptions of intellectual disability and mental illness and found thatcollege undergraduates tended to associate intellectual disability with physical stigmata and cognitive deficiencies, and thestudents unanimously reported that intellectual disability was caused by brain damage or genetics rather thanenvironmental stimuli.
* Corresponding author at: Louisiana State University, Department of Psychology, 236 Audubon Hall, Baton Rouge, LA 70803-5501, USA.
Tel.: +1 337 654 0636; fax: +1 225 358 1092.
E-mail addresses: [email protected] (M.W. Musso), [email protected] (A.A. Barker), [email protected] (D.A. Proto), [email protected]
(W.D. Gouvier).
0891-4222/$ – see front matter � 2011 Elsevier Ltd. All rights reserved.
doi:10.1016/j.ridd.2011.09.009
M.W. Musso et al. / Research in Developmental Disabilities 33 (2012) 224–228 225
More recently, McCaughey and Strohmer (2005) asked college students to list 10 attributes of persons with varyingdisabilities, including ID. Two core prototypes were: needs help/dependent on others and slow learner/comprehensionproblems. Secondary prototypes listed included: speech impairment, impaired motor skills/wheelchair use, childlike, looksphysically different, special education, condition at birth, and happy/loving. Tertiary prototypes identified were cannotfunction normally in society/work and brain dysfunction.
Taken together, these two studies indicate that many individuals in the public may not have a clear understanding of mildID (MID). Moreover, these studies suggest that many college students conceptualize MID as more severe and easilyidentifiable than is often the case, suggesting that people may have difficulty making informed decisions about ID diagnosesin the presence of such misconceptions. While numerous studies have examined college students’ perceptions and attitudestowards persons with intellectual disabilities (Akrami, Ekehammar, Claesson, & Sonnander, 2006; Corrigan et al., 2000;Meyer, Gouvier, Duke, & Advokat, 2001; Panek & Junger, 2008), to date, no studies have broadly surveyed public perceptionsof the possible adaptive behavior deficits found in MID. Thus, the current study sought to address this gap in the literature byinvestigating college students’ understanding of intellectual and adaptive behavior deficits involved in MID.
2. Material and methods
2.1. Participants
Participants were 890 college students enrolled at a large, southern university. Mean age of the sample was 19.9 years(SD = 2.51). Of the sample, 72% (n = 641) were female. The majority of participants were Caucasian (81.5%). Of the remainingparticipants, 6.7% were African American, 1% were Asian, 2.1% were Hispanic, and 2.8% were of another ethnicity. Studentsreceived credit in undergraduate psychology courses for participation in this survey. Overall, 534 students indicated thatthey did know someone diagnosed with an intellectual disability (first-degree relative, n = 9; second-degree relative, n = 140;non-family member, n = 360, no response to this question, n = 18).
2.2. Materials and procedure
All information collected in the present study was anonymous and presented to students in an online survey format. Theprocedure was approved by the university’s institutional review board. After granting informed consent, the students wereasked to complete a brief demographic questionnaire. Finally, students were presented with two surveys. The surveys werepresented in random order as were the questions within each survey. Students were informed that their responses wouldremain anonymous and were asked to answer honestly as their responses would influence future research in this area.
2.3. Surveys
Survey one presented 22 brief statements about individuals with MID (Table 1). These items were chosen because theyrepresent a broad range of possible misconceptions relevant to adults with mild ID. Students were asked to respond on afour-point Likert scale (almost never, sometimes, often, almost always) indicating how often they believed the statementapplied to individuals with MID. It should be noted that, for the purposes of this survey, the term ‘‘mentally retarded’’ waschosen over ‘‘intellectual disability’’ in order to ensure college students’ understanding of the construct being assessed, asintellectual disability is a newer term and some college students may not be aware of the change in terminology. Survey twobegan with the statement, ‘‘individuals with mild mental retardation have problems with:’’ and then listed 41 itemsencompassing aspects of all adaptive behavior domains as well as several cognitive domains (i.e. memory and attention;Table 2). Individuals responded using a four-point Likert scale (almost never, somewhat, often, and almost always) toindicate the degree to which they thought individuals with MID experienced the deficits listed.
3. Results and discussion
Data for surveys one and two can be found in Tables 1 and 2, respectively. Most students correctly responded that MIDcannot be cured and is not contagious. However, there appeared to be more ambiguity in responses related to rates thatindividuals with MID marry and rear children. 23.7% and 35.7% of the college students reported that individuals with mildmental retardation ‘‘almost never’’ marry and rear children, respectively. Hall and colleagues found that most individualswith mild intellectual impairment married (73%) and had children (62%; Hall et al., 2005). Also, Maughan, Collishaw, andPickles (1999) estimated that 95% of women and 80% of men with MID marry or cohabit with significant others. Anotherstudy reported that individuals with MID did not differ from their siblings with average intellectual functioning in rates ofmarriage, family formation, or ability to maintain employment, though the siblings with lower IQ scores typically had lesseducation and lower-paying jobs (Seltzer et al., 2005).
Over a quarter (29.3%) of college students surveyed in this study indicated they believed individuals with mild ID ‘‘almostnever’’ hold jobs in the competitive workforce. A meta-analysis of the literature found that individuals with MID are 3–4times more likely to be unemployed compared to intellectually average individuals and individuals with other disabilities(Verdonschot, de Witte, Reichrath, Buntinx, & Curfs, 2009). However, a study conducted in the United Kingdom found that
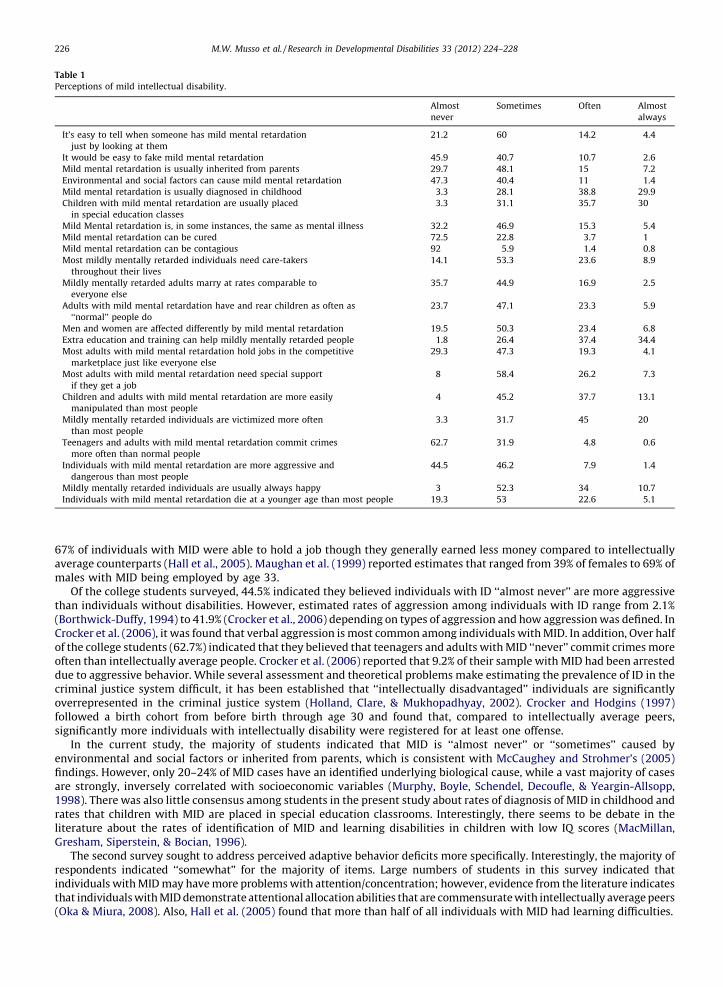
Table 1
Perceptions of mild intellectual disability.
Almost
never
Sometimes Often Almost
always
It’s easy to tell when someone has mild mental retardation
just by looking at them
21.2 60 14.2 4.4
It would be easy to fake mild mental retardation 45.9 40.7 10.7 2.6
Mild mental retardation is usually inherited from parents 29.7 48.1 15 7.2
Environmental and social factors can cause mild mental retardation 47.3 40.4 11 1.4
Mild mental retardation is usually diagnosed in childhood 3.3 28.1 38.8 29.9
Children with mild mental retardation are usually placed
in special education classes
3.3 31.1 35.7 30
Mild Mental retardation is, in some instances, the same as mental illness 32.2 46.9 15.3 5.4
Mild mental retardation can be cured 72.5 22.8 3.7 1
Mild mental retardation can be contagious 92 5.9 1.4 0.8
Most mildly mentally retarded individuals need care-takers
throughout their lives
14.1 53.3 23.6 8.9
Mildly mentally retarded adults marry at rates comparable to
everyone else
35.7 44.9 16.9 2.5
Adults with mild mental retardation have and rear children as often as
‘‘normal’’ people do
23.7 47.1 23.3 5.9
Men and women are affected differently by mild mental retardation 19.5 50.3 23.4 6.8
Extra education and training can help mildly mentally retarded people 1.8 26.4 37.4 34.4
Most adults with mild mental retardation hold jobs in the competitive
marketplace just like everyone else
29.3 47.3 19.3 4.1
Most adults with mild mental retardation need special support
if they get a job
8 58.4 26.2 7.3
Children and adults with mild mental retardation are more easily
manipulated than most people
4 45.2 37.7 13.1
Mildly mentally retarded individuals are victimized more often
than most people
3.3 31.7 45 20
Teenagers and adults with mild mental retardation commit crimes
more often than normal people
62.7 31.9 4.8 0.6
Individuals with mild mental retardation are more aggressive and
dangerous than most people
44.5 46.2 7.9 1.4
Mildly mentally retarded individuals are usually always happy 3 52.3 34 10.7
Individuals with mild mental retardation die at a younger age than most people 19.3 53 22.6 5.1
M.W. Musso et al. / Research in Developmental Disabilities 33 (2012) 224–228226
67% of individuals with MID were able to hold a job though they generally earned less money compared to intellectuallyaverage counterparts (Hall et al., 2005). Maughan et al. (1999) reported estimates that ranged from 39% of females to 69% ofmales with MID being employed by age 33.
Of the college students surveyed, 44.5% indicated they believed individuals with ID ‘‘almost never’’ are more aggressivethan individuals without disabilities. However, estimated rates of aggression among individuals with ID range from 2.1%(Borthwick-Duffy, 1994) to 41.9% (Crocker et al., 2006) depending on types of aggression and how aggression was defined. InCrocker et al. (2006), it was found that verbal aggression is most common among individuals with MID. In addition, Over halfof the college students (62.7%) indicated that they believed that teenagers and adults with MID ‘‘never’’ commit crimes moreoften than intellectually average people. Crocker et al. (2006) reported that 9.2% of their sample with MID had been arresteddue to aggressive behavior. While several assessment and theoretical problems make estimating the prevalence of ID in thecriminal justice system difficult, it has been established that ‘‘intellectually disadvantaged’’ individuals are significantlyoverrepresented in the criminal justice system (Holland, Clare, & Mukhopadhyay, 2002). Crocker and Hodgins (1997)followed a birth cohort from before birth through age 30 and found that, compared to intellectually average peers,significantly more individuals with intellectually disability were registered for at least one offense.
In the current study, the majority of students indicated that MID is ‘‘almost never’’ or ‘‘sometimes’’ caused byenvironmental and social factors or inherited from parents, which is consistent with McCaughey and Strohmer’s (2005)findings. However, only 20–24% of MID cases have an identified underlying biological cause, while a vast majority of casesare strongly, inversely correlated with socioeconomic variables (Murphy, Boyle, Schendel, Decoufle, & Yeargin-Allsopp,1998). There was also little consensus among students in the present study about rates of diagnosis of MID in childhood andrates that children with MID are placed in special education classrooms. Interestingly, there seems to be debate in theliterature about the rates of identification of MID and learning disabilities in children with low IQ scores (MacMillan,Gresham, Siperstein, & Bocian, 1996).
The second survey sought to address perceived adaptive behavior deficits more specifically. Interestingly, the majority ofrespondents indicated ‘‘somewhat’’ for the majority of items. Large numbers of students in this survey indicated thatindividuals with MID may have more problems with attention/concentration; however, evidence from the literature indicatesthat individuals with MID demonstrate attentional allocation abilities that are commensurate with intellectually average peers(Oka & Miura, 2008). Also, Hall et al. (2005) found that more than half of all individuals with MID had learning difficulties.
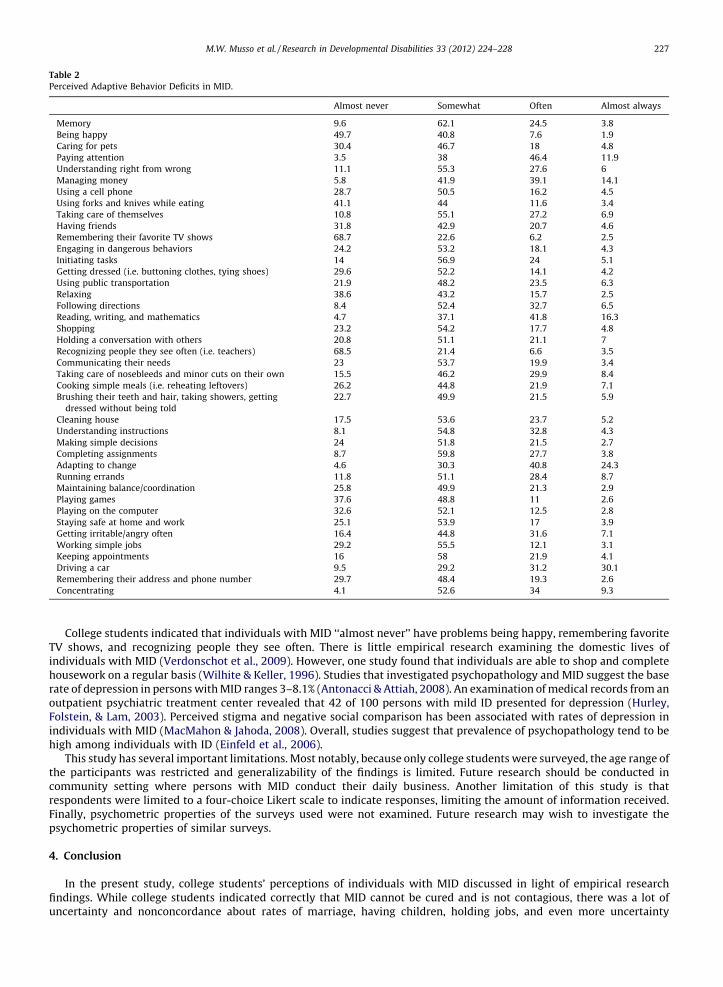
Table 2
Perceived Adaptive Behavior Deficits in MID.
Almost never Somewhat Often Almost always
Memory 9.6 62.1 24.5 3.8
Being happy 49.7 40.8 7.6 1.9
Caring for pets 30.4 46.7 18 4.8
Paying attention 3.5 38 46.4 11.9
Understanding right from wrong 11.1 55.3 27.6 6
Managing money 5.8 41.9 39.1 14.1
Using a cell phone 28.7 50.5 16.2 4.5
Using forks and knives while eating 41.1 44 11.6 3.4
Taking care of themselves 10.8 55.1 27.2 6.9
Having friends 31.8 42.9 20.7 4.6
Remembering their favorite TV shows 68.7 22.6 6.2 2.5
Engaging in dangerous behaviors 24.2 53.2 18.1 4.3
Initiating tasks 14 56.9 24 5.1
Getting dressed (i.e. buttoning clothes, tying shoes) 29.6 52.2 14.1 4.2
Using public transportation 21.9 48.2 23.5 6.3
Relaxing 38.6 43.2 15.7 2.5
Following directions 8.4 52.4 32.7 6.5
Reading, writing, and mathematics 4.7 37.1 41.8 16.3
Shopping 23.2 54.2 17.7 4.8
Holding a conversation with others 20.8 51.1 21.1 7
Recognizing people they see often (i.e. teachers) 68.5 21.4 6.6 3.5
Communicating their needs 23 53.7 19.9 3.4
Taking care of nosebleeds and minor cuts on their own 15.5 46.2 29.9 8.4
Cooking simple meals (i.e. reheating leftovers) 26.2 44.8 21.9 7.1
Brushing their teeth and hair, taking showers, getting
dressed without being told
22.7 49.9 21.5 5.9
Cleaning house 17.5 53.6 23.7 5.2
Understanding instructions 8.1 54.8 32.8 4.3
Making simple decisions 24 51.8 21.5 2.7
Completing assignments 8.7 59.8 27.7 3.8
Adapting to change 4.6 30.3 40.8 24.3
Running errands 11.8 51.1 28.4 8.7
Maintaining balance/coordination 25.8 49.9 21.3 2.9
Playing games 37.6 48.8 11 2.6
Playing on the computer 32.6 52.1 12.5 2.8
Staying safe at home and work 25.1 53.9 17 3.9
Getting irritable/angry often 16.4 44.8 31.6 7.1
Working simple jobs 29.2 55.5 12.1 3.1
Keeping appointments 16 58 21.9 4.1
Driving a car 9.5 29.2 31.2 30.1
Remembering their address and phone number 29.7 48.4 19.3 2.6
Concentrating 4.1 52.6 34 9.3
M.W. Musso et al. / Research in Developmental Disabilities 33 (2012) 224–228 227
College students indicated that individuals with MID ‘‘almost never’’ have problems being happy, remembering favoriteTV shows, and recognizing people they see often. There is little empirical research examining the domestic lives ofindividuals with MID (Verdonschot et al., 2009). However, one study found that individuals are able to shop and completehousework on a regular basis (Wilhite & Keller, 1996). Studies that investigated psychopathology and MID suggest the baserate of depression in persons with MID ranges 3–8.1% (Antonacci & Attiah, 2008). An examination of medical records from anoutpatient psychiatric treatment center revealed that 42 of 100 persons with mild ID presented for depression (Hurley,Folstein, & Lam, 2003). Perceived stigma and negative social comparison has been associated with rates of depression inindividuals with MID (MacMahon & Jahoda, 2008). Overall, studies suggest that prevalence of psychopathology tend to behigh among individuals with ID (Einfeld et al., 2006).
This study has several important limitations. Most notably, because only college students were surveyed, the age range ofthe participants was restricted and generalizability of the findings is limited. Future research should be conducted incommunity setting where persons with MID conduct their daily business. Another limitation of this study is thatrespondents were limited to a four-choice Likert scale to indicate responses, limiting the amount of information received.Finally, psychometric properties of the surveys used were not examined. Future research may wish to investigate thepsychometric properties of similar surveys.
4. Conclusion
In the present study, college students’ perceptions of individuals with MID discussed in light of empirical researchfindings. While college students indicated correctly that MID cannot be cured and is not contagious, there was a lot ofuncertainty and nonconcordance about rates of marriage, having children, holding jobs, and even more uncertainty

M.W. Musso et al. / Research in Developmental Disabilities 33 (2012) 224–228228
regarding these individuals’ specific adaptive behavior deficits. Overall, this study highlights the need for better education ofthe general public about misconceptions of intellectual disability. In addition to perpetuating stigma of intellectualdisability, such misconceptions could have serious implications if they influence juror’s decisions about diagnoses of mildintellectual disability.
References
Antonacci, D. J., & Attiah, N. (2008). Diagnosis and treatment of mood disorders in adults with developmental disabilities. Psychiatric Quarterly, 79(3), 171–192.Akrami, N., Ekehammar, B., Claesson, M., & Sonnander, K. (2006). Classical and modern prejudice: Attitudes toward people with intellectual disabilities. Research
in Developmental Disabilities, 27, 605–617.Atkins v. Virginia (2002), 260 Va. 375, 534S. E. 2d 312.Bauerman, S. B. (2005). Balancing the burden: The constitutional justification for requiring the government to prove the absence of intellectual disability before
imposing the death penalty. American University Law Review, 54, 401–438.Borthwick-Duffy, S. A. (1994). Prevalence of destructive behaviors: A study of aggression, self-injury, and property destruction. In T. Thompson & D. B. Gray (Eds.),
Destructive Behavior in Developmental Disabilities: Diagnosis and Treatment (pp. 3–23). Thousand Oaks, CA: Sage.Caruso, D. R., & Hodapp, R. M. (1988). Perceptions of intellectual disability and mental illness. American Journal on Intellectual Disability, 93(2), 118–124.Corrigan, P. W., River, L. P., Lundin, R. K., Wasowski, K. U., Campion, J., Mathisen, J., et al. (2000). Stigmatizing attributions about mental illness. Journal of
Community Psychology, 28(1), 91–102.Crocker, A. G., & Hodgins, S. (1997). The criminality of noninstitutionalized mentally retarded persons: Evidence from a birth cohort followed to age 30. Criminal
Justice and Behavior, 24(4), 432–454 doi:10.1177/0093854897024004003.Crocker, A. G., Mercier, C., Lachapelle, Y., Brunet, A., Morin, D., & Roy, M.-E. (2006). Prevalence and types of aggressive behavior among adults with intellectual
disabilities. Journal of Intellectual Disability Research, 50(9), 652–661.Einfeld, S. L., Piccinin, A. M., Mackinnon, A., Hofer, S. M., Taffe, J., Gray, K. M., et al. (2006). Psychopathology in young people with intellectual disability. Journal of
the American Medical Association, 296(16), 1981–1989.Ellis, J. W. (2003). Mental retardation and the death penalty: A guide to state legislative issues. Retrieved from: http://www.deathpenaltyinfo.org/documents/
MREllisLeg.pdf.Hall, I., Strydom, A., Richards, M., Hardy, R., Bernal, J., & Wadsworth, M. (2005). Social outcomes in adulthood of children with intellectual impairments: Evidence
from a birth cohort. Journal of Intellectual Disability Research, 49(3), 171–182.Holland, T., Clare, I. C. E., & Mukhopadhyay, T. (2002). Prevalence of ‘criminal offending’ by men and women with intellectual disability and the characteristics of
‘offenders’: Implications for research and service development. Journal of Intellectual Disability Research, 46(1), 6–20.Hurley, A. D., Folstein, M., & Lam, N. (2003). Patients with and without intellectual disability seeking outpatient psychiatric services: Diagnoses and prescribing
pattern. Journal of Intellectual Disability Research, 47(1), 39–50 doi:10.1046/j.1365-2788.2003.00463.x.MacMillan, D. L., Gresham, F. M., Siperstein, G. N., & Bocian, K. M. (1996). The labyrinth of IDEA: School decisions on referred students with subaverage general
intelligence. American Journal on Mental Retardation, 101(2), 161–174.MacMahon, P., & Jahoda, A. (2008). Social comparison and depression: People with mild and moderate intellectual disabilities. American Journal on Mental
Retardation, 113(4), 307–318.Maughan, B., Collishaw, S., & Pickles, A. (1999). Mild mental retardation: Psychosocial functioning in adulthood. Psychological Medicine, 29, 351–366.McCaughey, T. J., & Strohmer, D. C. (2005). Prototypes as an indirect measure of attitudes toward disability groups. Rehabilitation Counseling Bulletin, 48(2), 89–99.Meyer, L., Gouvier, W. D., Duke, M., & Advokat, C. (2001). Influence of social context on reported attitudes of nondisabled students toward students with
disabilities. Rehabilitation Counseling Bulletin, 45(1), 50–52.Murphy, C. C., Boyle, C., Schendel, D., Decoufle, P., & Yeargin-Allsopp, M. (1998). Epidemiology of mental retardation in children. Mental Retardation and
Developmental Disabilities, 4, 6–13.Oka, K., & Miura, T. (2008). Allocation of attention and effect of practice on persons with and without mental retardation. Research in Developmental Disabilities,
29(2), 1665–2175.Panek, P. E., & Junger, M. K. (2008). Effects of age, gender, ad causality on perceptions of persons with intellectual disability. Research in Developmental Disabilities,
29, 125–132.Ring v. Arizona (2002), 122 S. Ct. 2428.Seltzer, M. M., Floyd, F., Greenberg, J., Lounds, J., Lindstromm, M., & Hong, J. (2005). Life course impacts of mild intellectual deficits. American Journal of Mental
Retardation, 110(6), 451–468.Verdonschot, M. M. L., de Witte, L. P., Reichrath, E., Buntinx, W. H. E., & Curfs, L. M. G. (2009). Community participation of people with an intellectual disability: A
review of empirical findings. Journal of Intellectual Disability Research, 53(4), 303–318.Wilhite, B. C., & Keller, M. J. (1996). Integration, productivity, and independence among adults with developmental disabilities: Implications for therapeutic
recreation. Therapeutic Recreation Journal, 30, 64–78.





























