Embed Size (px)
Citation preview

Collagen Disorders
Michael H. Wilhelm, CRNA, APRN

Collagen Vascular Diseases
The four most common disorders of this group are rheumatoid arthritis, systemic lupus erythematosus, scleroderma, and polymyositis.
The etiology of the collagen vascular diseases is unknown, however the immune system has been implicated.
All of these diseases effect the joints, each has systemic effects as well.
Rheumatoid Arthritis
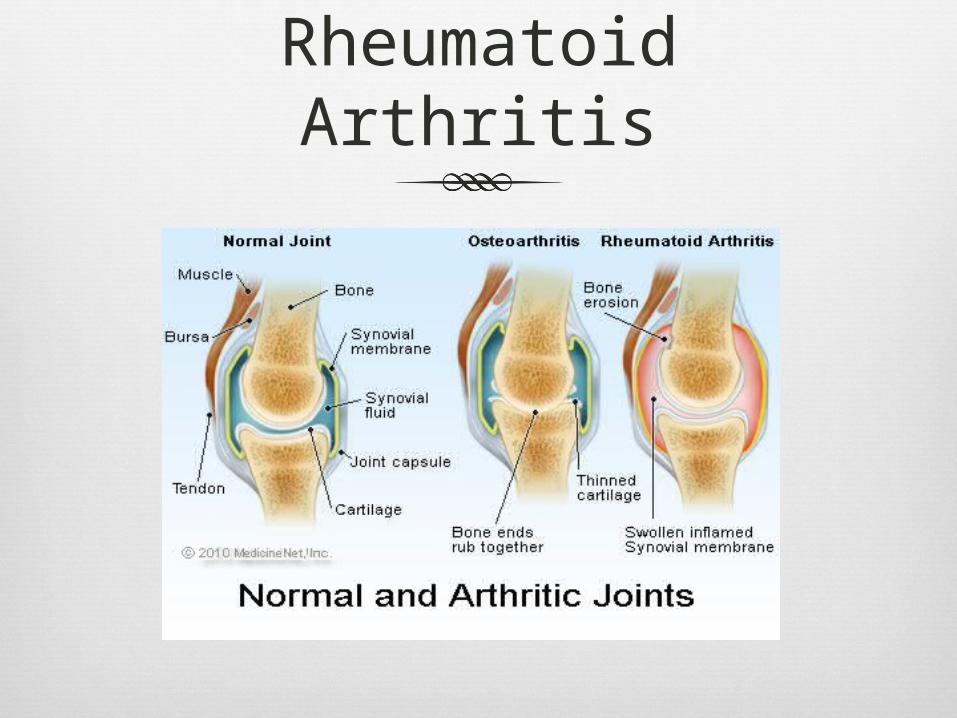
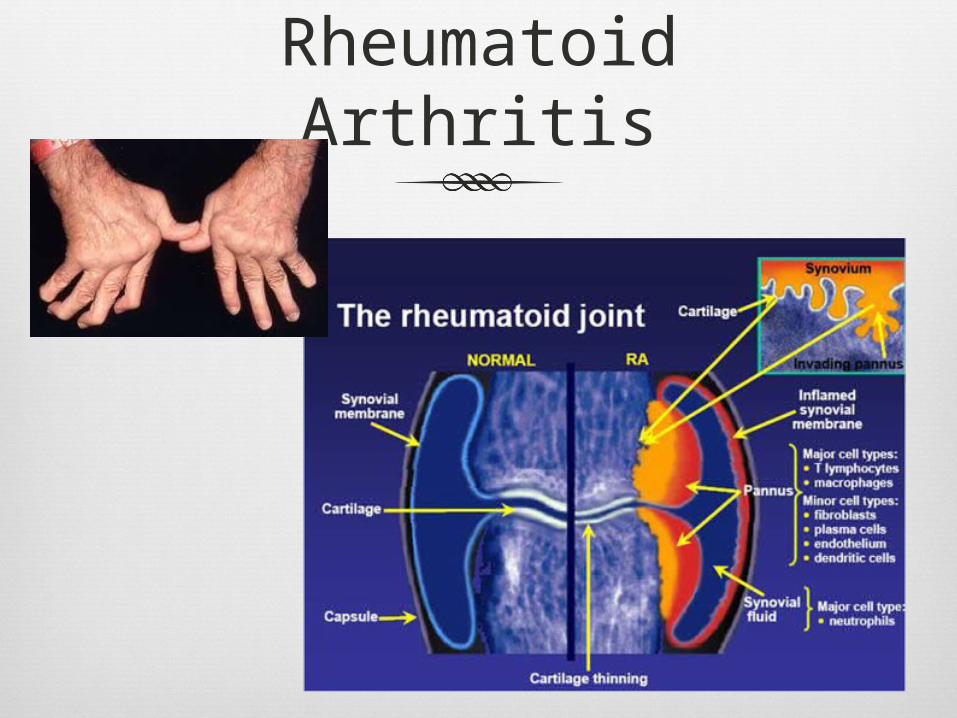
Pathophysiology Rheumatoid arthritis begins with cellular
hyperplasia of the synovium, followed by invasion of the synovium by lymphocytes, plasma cells, and fibroblasts. Ultimately, the cartilage and articular surfaces are destroyed.
The cause of Rheuatoid Arthritis is unknown, but rheumatoid factor (an antiimmunoglobulin antibody) is present in 90% of patients
The hands and wrist are the first to be effected, especially the metacarpophalangeal and proximal interphalangeal joints.

Rheumatoid Arthritis
Compression of lower extremity peripheral nerves can produce paresis and sensory loss over the leg.
Spinal cord compression does not correlate with patient’s symptoms, and asymptomatic patients may have a high degree of cord compression.
Rheumatoid arthritis affects the joints of the larynx, cervical spine, and temporomandibular joint.

Rheumatoid Arthritis
Peripheral Joints Hands, feet, wrist (most common)
Nonarticular muscular structures Tendons, ligaments and fascia
Systemic Involvement Blood Vessels, heart, lungs, etc.

Rheumatoid Arthritis
Manifestations involving other systems: Skin : Raynaud’s, Digital necrosis Eyes : Scleritis, corneal ulceration Lung : Pleural effusion, pulmonary
effusion Heart : Pericarditis, cardiac tamponade,
coronary arteritis, aortic insufficiency Kidney : Interstitial fibrosis,
glomerulonephritis, amyloid deposition PNS : Compression syndromes,
mononeuritis

Rheumatoid Arthritis
Manifestations continued: Liver : Hepatitis Blood: Anemia, leukopenia
Rheumatoid Arthritis
About 6 million American have Rheumatoid Arthritis
75% of them are women
Can occur at any age Women: between ages 35-50 Men: somewhat later
Rheumatoid Arthritis
Joint Involvement Morning Stiffness – joints of the hand, feet, wrist and knees Nearly every joint is effected
Thoracic, lumbar, sacral spine almost always spared Cervical spine involvement is frequent
Atlantoaxial subluxation (partial or complete dislocation of the 1st and 2nd cervical vertebrae)
Cricoarytenoid arthritus Edema of the arytenoids, upper airway obstruction
Tempromandibular Joint Limitations in mandibular motion
Joints of the Larynx Limitations of the vocal cord movement, edema

Rheumatoid Arthritis
Systemic Involvement Vascular
Vasculitis – peripheries Aortitus – dilation of the aortic root resulting in aortic regurgitation
Cardiovascular Pericarditus, endocarditis, LV Failure (CHF), valve fibrosis, arteritis
involving coronary arteries, myocardial infarction Pulmonary
Pleural effusions, fibrosis Costochondral involvement
Decreases lung volumes Decreases vital capacity Leads to V/Q Mismatch decreasing arterial oxygenation

Rheumatoid Arthritis
Neuromuscular Loss of strength in muscle adjacent to joints Neuropathy resulting from nerve compression
Hematologic Anemia
Liver/Kidney Rarely problems occur
Rheumatoid Arthritis
Rheumatoid Arthritis

Rheumatoid Arthritis
Treatment: Analgesics, NSAIDS,Methotrexate, COX-2
inhibitors, and corticosteroids. Many of these dugs cause anemia,
thrombocytopenia, and hepatitis. Steroids are reserved for those patients
who fail to respond to first line drugs such as Methotrexate due to the long term effects of taking steroids.
Surgical procedures such as synovectomy, tenolysis, and joint replacement.

Rheumatoid Arthritis
Management of anesthesia: Baseline ABGs, PFTs, clotting times,
CBC, ECHO/Stress Test Assess cervical spine ROM and airway Assess steroid use Possible awake FOI, glidescope Proper positioning Careful airway
management/ventilation
Rheumatoid Arthritis
Management of anesthesia: Intubation: cricoarytenois arthritis may
be recognized by erythema and edema of vocal cords which may decrease glottic opening. A smaller ETT may be needed. Exaggerated edema and stridor may occur postextubation.
Corticosteroids may be needed perioperatively.
Careful positioning.

Systemic Lupus Erythematosus
An autoimmune disease in which patients produce autoantibodies to DNA and also to RNA polymerase, cardiolipin, and ribosomal phosphoproteins.
Clinical manifestations may be due to the production of and autoantibody highly specific for a single protein within an organ.
Common manifestations are polyarthritis and dermatitis.

Systemic Lupus Erythematosus
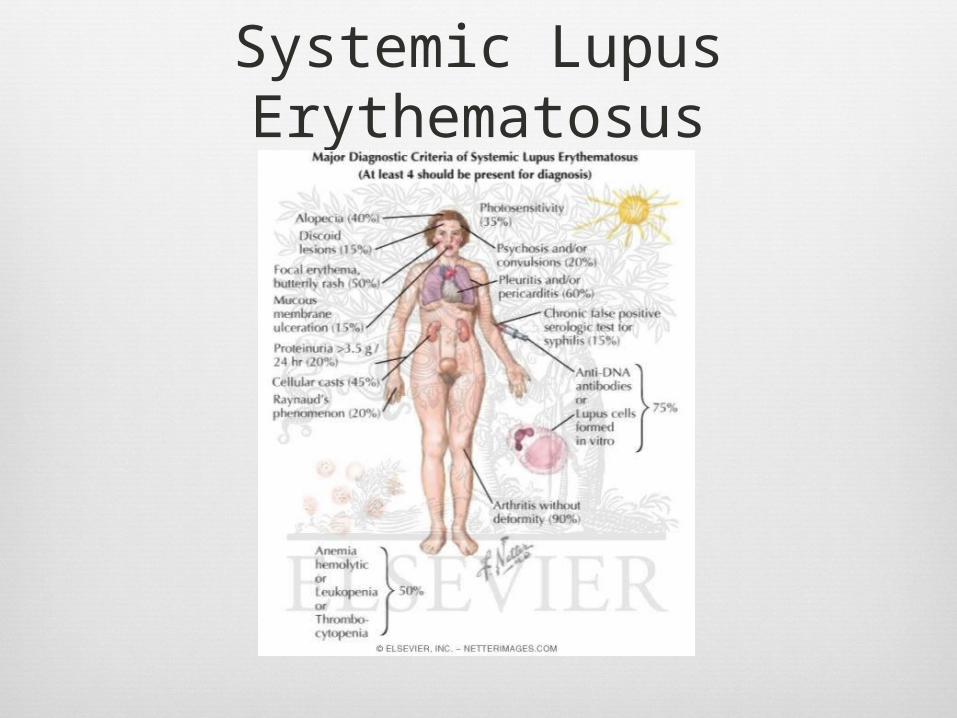
A diagnosis of SLE is likely when patients have three of four manifestations Antinuclear
antibodies Characteristic rash Thrombocytopenia Serositis Nephritis
Common Presenting Features Fever Malaise Joint Pain Myalgias Fatigue

Systemic Lupus Erythematosus
About 1.5 Million Americans have SLE
Affects women 9 times more likely than men
Can occur at any age
Higher incident in African-American women

Systemic Lupus Erythematosus
Systemic Involvement Cardiovascular
Pericarditis, pericardial effusions, friction rub, tachycardia, CHF, LV dysfunction, valve abnormalities (aortic, mitral)
Pulmonary Pleural effusions, pneumonia, dry cough, dyspnea, pulmonary
HTN PFTs show restrictive lung disease Recurrent atelectasis can result in “shrinking lung syndrome” Involvement of the larynx and the trachea is rare, but may
include true vocal fold thickening or paralysis, cricoarytenois arthritis, and subglottic stenosis

Systemic Lupus Erythematosus
CNS Cognitive dysfunction occurs in approximately 1/3 of the
patients Mood Disturbances Deterioration of intellectual capacity
Atypical migraine headaches followed by visual disturbances
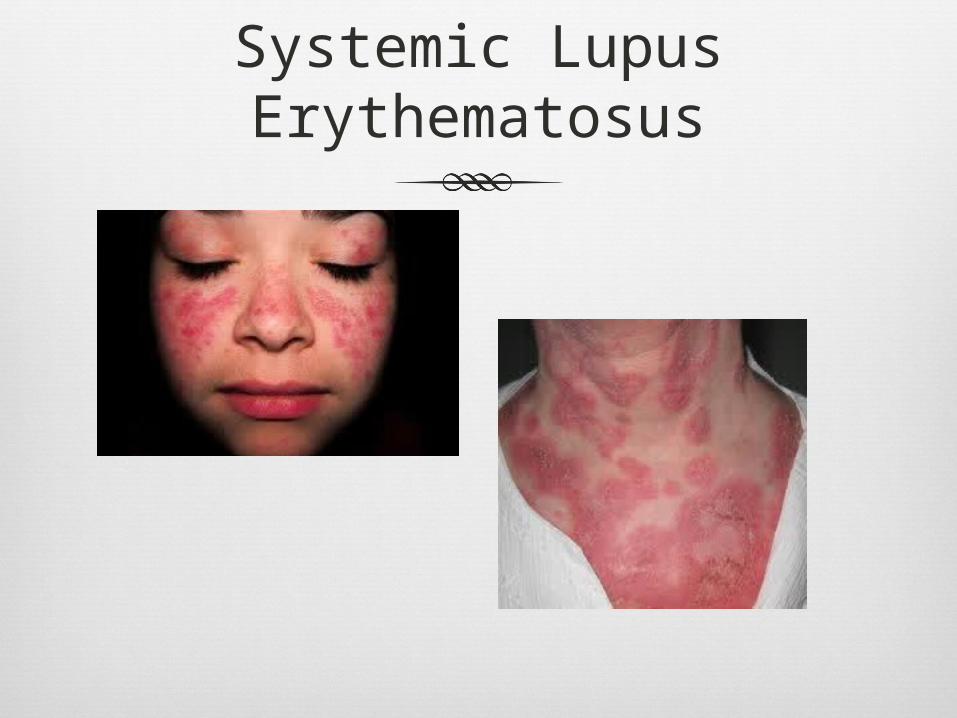
Cutaneous Mala or “butterfly” rash is presenting sign in 50% of patients Rash on trunk (red scaly patches), alopecia Photosensitivity

Systemic Lupus Erythematosus
Neuromuscular Loss of strength in muscle adjacent to joints Neuropathy resulting from nerve compression
Hematologic Anemia, Thrombocytopenia, leukopenia, Prolonged PT
and PTT Liver
Autoimmune Hepatitis in severe cases Kidney
Glomerulonephritis, proteinuria, hypoalbuminemia, renal failure
Systemic Lupus Erythematosus
Systemic Lupus Erythematosus

Systemic Lupus Erythematosus I
MMUNOLOGY
OMG
Systemic Lupus Erythematosus
Management of Anesthesia: Careful pre-operative assessment including CXR,
echo, renal function, liver function, and PFT’s. Airway Assessment Proper Positions/Peripheral Neuropathy Careful muscle relaxation titration Arthritic involvement is rare in the cervical spine. If postextubation laryngeal edema or stridor
occur IV administration of corticosteroids is effective.
Patients receiving corticosteroids may require intraoperative steroids.
Scleroderma
A chronic autoimmune disease of the connective tissue
Characterized by the formation of scar tissue (fibrosis) in the skin and organs of the body and presence of autoantibodies
The cause of Scleroderma is unknown, but the disease process has the characteristics of both a collagen disease and an autoimmune process
Progressive fibrosis, resulting form increases collagen deposits in the interstitium and intima of small arteries and connective tissue of involved organs is the pathologic hall mark of the disease
Scleroderma
Affects approximately 300,000 people in the US
Affects women 4 times more likely than men
Juvenile scleroderma affects approximately 7000 children in the US
Choctaw Native Americans have the highest reported prevalence
Men and African-American women have the worse prognosis

Scleroderma
Limited form of Scleroderma tends to be confined to the skin, fingers and face
Often referred to as “CREST” Syndrome C – Calcinosis – Calcium deposits in the skin R – Raynaud’s Phenomenon – Spasms of tiny blood vessels in
response to cold or stress E – Esophagus Dysfunction – Acid reflux and decreased
motility of the esophagus S – Sclerodactyly – Thickening and tightening of the skin on
the fingers and hands T – Telangiectasis – Dilation of capillaries causing red marks
on surface of the skin

Scleroderma
Systemic Involvement Skin/Musculoskeletal
Inflammation and taut skin leading to decreased ROM of the fingers, toes and jaw
Skeletal muscle myopathy leading to muscle weakness
Cardiovascular Sclerosis of coronary arteries, fibrous tissue replaces
cardiac muscle, systemic and pulmonary HTN Dysrhythmias, cardiac conduction abnormalities,
CHF, pericarditis, pericardial effusion

Scleroderma
Pulmonary Interstitial fibrosis, pulmonary HTN, decreases
inspiratory capacity, increases residual volume, chest wall restriction
GI GI fibrosis, hypomotility of the esophagus and
small intestine, decreased lower esophageal sphincter tone, reflux esophagitis
Renal Renal artery obstruction, decreased renal blood
flow, systemic HTN, renal failure

Scleroderma
Scleroderma
Management of anesthesia: Baseline ABGs, PFTs, CXR, EKG, Room Air
Sat Full stomach precautions Managing BP/Fluid Mangement Avoid hypothermia Careful airway management/ventilation Avoid hypoxemia and respiratory acidosis Possible awake FOI, glidescope
Scleroderma
Regional Anesthesia Advantages
Post operative analgesia Peripheral vasodilation Decreased risk of post operative ventilation
support Disadvantages
Regional Anesthesia may be technically difficult due to the taut skin and joint changes

Scleroderma
Management of Anesthesia: Ventilation with increased FiO2 is required Invasive cardiac monitoring due to
exaggerated responses to inhaled anesthetics.
Difficult venous access. Muscle involvement may increase
sensitivity to muscle relaxants (use short acting).
Regional anesthetics may be prolonged. Avoid stellate ganglion block.
Marfan’s Syndrome
Autosomal dominant, multisystem, fibrous connective tissue disorder
Affects blood vessel walls, tendons, ligaments, cartilage, heart walls/valves, aorta, and other structures
Characterized by disproportionately long limbs, long thin fingers, a typically tall stature and a predisposition to cardiovascular abnormalities

Marfan’s Syndrome
Approximately 200,000 people in the US
Each parent with the condition has a 50% chance of passing onto offspring
Men and women are equally likely to have disease
Caused by a mutation of a gene on Chromosome 15
Marfan’s Syndrome
Systemic Involvement Musculoskeletal
Grows to about average height Arachnodactyly (long slender limbs, fingers and toes) Scoliosis, thoracic lordosis Pectus excavatum or pectus cairnatum High palates and jaws
Cardiovascular Dilated aorta, risk of ruptured aortic aneurysm Prolapse of the mitral or aortic valves Palpitations, tachydysrhythmia Raynaud’s Phenomenon

Marfan’s Syndrome
Pulmonary Spontaneous Pneumothorax Sleep Apnea Obstructive Lung Disease
CNS Dural ectasia (weaking of the connective tissue of the
dural sac) Lower back pain, leg pain, abdominal pain, neuropathy,
headache
Eye Retinal detachment, glaucoma, lens discoloration,
myopia, corneal flatness

Marfan’s Syndrome
Marfan’s Syndrome
Anesthesia Management Careful airway management Minimize pain/stress Positioning Cardiac Workup Careful Ventilation Careful blood pressure monitoring Intraoperative Medications
Beta Blockers ACE Inhibitors ARBs Antibiotics

Epidermolysis Bullosa
A rare skin disease which can be inherited or acquired. The acquired forms are autoimmune.
The end result is loss or absence of normal intercellular bridges and separation of skin layers. The separation of skin layers results in intradermal fluid accumulation and bullae formation.
Minor skin trauma produces skin blisters.

Epidermolysis Bullosa
Involves fingers and toes mostly.
Esophageal involvement is common, resulting in dysphasia and esophageal strictures
Anemia and hypoalbuminemia lead to increased infection.
Glomerulonephritis secondary to strep infection.
Patients rarely survive over 30 years.

Epidermolysis Bullosa
Therapy is rather unsuccessful and steroids tend not to work.
Management of Anesthesia: Avoid trauma to the skin and mucous
membranes Trauma from tape, BP cuffs, tourniquets, and
EKG pads can cause bullae. Pad BP cuffs Lubrication of face mask Avoid upper airways.
Epidermolysis Bullosa
Management of anesthesia:
Lubricate laryngoscope to reduce friction.
Scarring of the oral cavity can produce immobility of the tongue, therefore consider awake fiberoptic.
Avoid esophageal stethoscopes.
Ketamine is a good choice due to most surgeries are superficial and to the extremities.
Regional has been successful.

Pemphigus
An autoimmune disease where auto antibodies are highly specific and result in the excessive production of proteolytic enzymes that disrupt cell adhesion, leading to separation of epithelial layers.
Pemphigus vulgaris is most common and most clinically important to anesthesiologists because of the occurrence of oral lesions.
Lesions of the pharynx, larynx, esophagus, conjunctiva, urethra, cervix, and anus also develop.
Pemphigus
Treatment with corticosteroids and immunosupressants is highly effective.
Management of Anesthesia: Corticosteroid supplementation. Upper airway techniques are similar to
epidermolysis bullosa. Ketamine and regional are also successful for
these patients. Look for side effects of treatment drugs with
anesthesia. Such as cyclophosphamide may prolong SCH and mivacurium by inhibiting cholinesterase activity.
Questions
?