Embed Size (px)
Citation preview

Collaborative practice within the in tensive care unit:
a deconstruction Julie S. Taylor
julie s. Taylor MSc, RGN, Pathway leader (Critical care), North Yorkshire College of Health Studies, York District Hospital, Wigginton Road, York YO2 INN, UK
(Requests for offprints to JST) Manuscript accepted 20 February 1996
The concept of collaborative practice has attracted much attention in the last few years - - how well do doctors and nurses work together as a team in providing the best possible care for their patients? Consequently there are numerous articles on the subject, most of which seem to suggest that collaborative practice is essential, particularly within the intensive care unit ( ICU). It has been linked to both job satisfaction and to patient outcomes (mortality or readmission to the ICU). Indeed, it seems to have evolved as a benchmark for good ICU practice. This paper focuses on some of the most influential writings on this phenomenon, the first stage of a postgraduate study on collaborative practice in intensive care. A decon- structive reading of such literature raises some interesting questions. There are inadequacies in the existing claims, which perhaps suggest that a re-examination of both the feasibility and desirability of collaborative practice is needed.
I N T R O D U C T I O N
This paper developed from a longstanding interest in doctor-nurse relationships. Intensive care units (ICUs) provide a unique environ- ment in which to examine these, as doctors and nurses work more closely together in ICUs than they do in some other areas. The literature surrounding collaborative practice is both myriad and persuasive, and indeed, claims that collaborative practice improves patient out- comes in ICUs must be taken seriously. Research undertaken for a postgraduate study
(Taylor 1995) was designed to reconstruct this phenomenon, using Denzin's (1989) method- ology of interpretive interactionism. Integral in this is a &constructive reading and critical. analysis of how the phenomenon has been pre- sented, studied and analysed in the literature, leading to a presentation of any biases and pre- conceptions that may be found there. This paper is an account of that analytical reading (or &construction), which provided the comer- stone of the subsequent enquiry.
D E F I N I N G C O L L A B O R A T I V E P R A C T I C E
The concept of collaborative practice between doctors and nurses is widely written about, although it is difficult to find an agreed state- ment of meaning. Despite the lack of clarity about the term, or any empirical basis for it, collaborative practice is promoted as a way to improve patient outcomes (Dunbar & Bryan- Brown 1988). Broadly, it could mean that it is a process of individuals or institutions working together to achieve a common goal (Hiderly 1991, Jones 1994), or to plan and implement care (Lewis 1985). Others have attempted to define collaborative practice more precisely:
Collaboration is the most positive way to resolve con f l i c t . . , requiring the finding of solutions where both parties' concerns are openly shared and recognised in a way con- sistent with identified, broad, comprehen- sive common goals (Wonsetter 1987, p.30).
Collaboration implies sharing of informa- tion and also implies that each participant in the health care system respects the other's skill and expertise. Collaboration also requires that nurses and physicians recon- sider their definition o f clinical decision- making to recognise the contributions of others to patient care (Roberts 1987, p.81).
Col laborat ion. . .
is a cooperative venture based on shared power and authority. It is non-hierarchical in nature, and it assumes power based on a knowledge or expertise rather than power based on role or function (Kraus 1980, p.12).
Collaboration is joint-communicating and decision-making with the expressed goal of satisfying the patient's wellness and illness needs whilst respecting the unique qualities and abilities of each professional (Coluccio & Maguire 1983, p.59).
And so the literature goes on, with the con- cept o f collaborative practice a little woolly,
Intensive and Critical Care Nursing (1996) 12,64-70 © 1996PearsonProfessJonalLtd

Collaborative practice within the intensive care unit: a deconstruction 65
extremely difficult to measure and possibly unrealistic. I concur with King et al (1993), that collaborative practice is more an attitude than anything else. Despite that, it has been a widely debated concept for the last decade or so in the American literature. It has not just been debated, but apparently practised as well. 'Despite its elu- siveness, its essence continues to be sought after as a means of improving working relationships and patient outcomes' (Henneman et al 1995, p.103). In 1982, following some of their Demonstration Projects, the American Association of Critical Care Nurses (AACN) claimed that collaboration in care decisions was a crucial variable in improving patient outcomes. However, their model provided no theoretical framework, nor did it suggest guidelines for implementation of the model (King et al 1993). The National Committee for Joint Practice (NCJP) identified the following elements as essential for collaborative practice environments:
• primary nursing • integrated patient records • clinical decision-making by nurses to be
encouraged • a joint practice committee • joint patient care reviews (NCJP 1981).
At a critical care conference sponsored by the National Institute of Health (1983), the value of collaborative practice was recognised. Since then, copious articles have appeared in the nurs- ing literature, all describing (and praising) A A C N Demonstration Projects on collaborative practice. Some writers have emerged more influentially than others and it is their work which is the focus of attention here first.
COLLABORATIVE PRACTICE SCALES
When deconstructing the literature, it became clear that many writers had based their defini- tion of collaboration on a model conceptualised by Thomas (1976) and Kilmann & Thomas (1977). Weiss & Davis (1985)broadened this model, rewriting it to cover interpersonal rela- tionships generally, as a two-dimensional model. This is apparently fairly fundamental work in defining collaboration, as at least half of
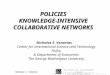
1"+ Desire to satisfy own concern
$-
[ ] Competition [~ Collaboration
[] Sharing
[] Avoidance [] Accommodation
- ~-- Desire tosatisfy ~> + other's concern
Fig. I Conflict solving model. Reproduced with the kind permission of Rand McNally (Thomas 1976, p. 900).
the literature makes reference to the Weiss & Davis model. It could thus be argued that this is possibly the most influential work on collabora- tion. As such, it is worth further examination.
The original Thomas model (1976) examined conflict-solving behaviours, concluding that coll- aboration combines a high level of cooperative- ness (concern for another's interests) with a high level of assertiveness (concern for own interests). This is shown more clearly in Figure 1.
Weiss & Davis used this model to develop two Collaborative Practice Scales (CPS), one for nurses, one for doctors. Collaborative practice was defined 'as interactions between nurse and physician that enable the skills and knowledge of both professionals to synergistically influence the patient care being provided' (p.299). They adapted the model so that it could be used for interpersonal problem-solving behaviour (Fig. 2).
In both models, collaboration is regarded as a high level of concern for self (assertiveness), combined with a high level o f concern for others (cooperativeness). Interestingly, both Thomas and Weiss & Davis use the term 'assertiveness' in a context that implies self- interest, in a manner that for many may be con- fused with aggression (Holland & Ward 1990). From this, Weiss & Davis developed their col- laborative practice scales, which were Likert- type statements to measure features of coll- aboration within the doctor-nurse relationship. For example 'I tell MDs when, in my judge- ment, their orders seem inappropriate' or 'I consider nurses' opinions when developing a treatment plan' (Weiss & Davis 1985, p.300).
Weiss had previously developed the items for inclusion on the scales by using structured dialogues with nurses, physicians and con- sumers (Weiss 1983). In Weiss & Davis's study (1985) higher scores imply greater use of col- laborative practice by doctor or nurse. Random selection of 200 doctors and 200 nurses to receive the CPS yielded a poor response (nurses 47.5%; doctors 21.5%), so another 200 doctors were approached. A similar response from the second batch gave the researchers a total physi- cian sample of 94. Statistical analyses using Eigenvalues and alpha coefficients are endlessly paraded, with the conclusion that the CPS are valid and reliable. Overall, the authors' con- clusions are vague in this difficult paper, but they do discuss the limitations in some depth.
This paper is particularly interesting when considering the research literature on collabo- rative practice. It is cited in numerous other studies on the phenomenon and is hailed as a rewriting of Thomas's 1976 model into a two- dimensional model; b u t in this analysis of the literature it was difficult to discern any appre- ciable differences between Thomas's original concept (Fig. 1) and the ' improved' Weiss &

66 Intensive and Critical Care Nursing
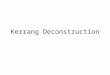
Assertion
Assertiveness $
Unassertion
[] Competition [] Collaboration
[] Sharing
[] Avoidance [] Accommodation
Uncooperation Cooperation ~- Cooperativeness -~
Fig. 2 Collaboration model, Reproduced with the kind permission of Nursing Research (Weiss & Davis 1985, p. 299).
Davis version (Fig. 2). Weiss & Davis applied this to nurses and doctors (CPS), although they made full acknowledgement to "Thomas's work. However, more recent studies have claimed this to be new and influential work (for example Johnson 1992, Jones 1994a,b). From the Weiss & Davis model, collaboration appears to imply inclusion of only doctor/nurse con- cerns. Assertiveness and cooperation levels define the relationship, from which everything else can then be explained (communication, autonomy, role definition, competence and other such factors). Somewhere the patient seems to have been lost, thus this two-dimen- sional model does not satisfactorily embrace all the views proffered in the literature.
Another fundamental problem pertains to the well-documented limitations of this sort of ques- tionnaire, one that asks people to rate their behaviour. When respondents are asked ques- tions on the CPS, how valid are the responses in real terms? It is possible that perceived rather than actual actions were often described. The initial low response rate that sent the researchers trawling for more subjects is also slightly ques- tionable. This is an extremely tortuous paper to read and most writers on the subject of collabo- rative practice have probably read abridged interpretations of it that do not quite reflect its original substance. For example, Jones (1994b) describes how Weiss & Davis measured assertiveness for nurses and cooperativeness for doctors, rather than both domains for each prac- titioner. The many articles charting the 'success' of Collaborative Practice Demonstration Units refer to the work by Weiss & Davis without actually referencing it (for example Mitchell et al 1989, Hamilton 1991, Birenbanm 1994). In this way, the CPS have become an integral feature of many other similar studies and appear to be regarded as almost the definitive word on the subject. It appears that ira behaviour appears on the CPS, it must be collaborative practice.
D E C I S I O N A B O U T T R A N S F E R S C A L E S
One of the most prolific writers on collaborative practice must be Judith Baggs, sometimes alone,
sometimes with others; thus her work must be considered when dealing with this phenom- enon. Again American, Baggs has published extensively, although after the first few readings it becomes clear that most of her articles are cit- ing the same study in a slightly different format (a not uncommon practice). The apparent qual- it,/and reputation of her work, then, is possibly unjustifiably enhanced by the quanti W of her publications. The impetus for her studies came from the work by Knaus et al (1986), which concluded that the relationship between doctors and nurses in ICUs was a significant element in lower patient mortality rates. From an extensive literature review, Baggs & Schmitt (1988) criti- cised the prevalent use of the term collaborative practice, which was being used without any agreed definition. Examining the literature on teamwork and communication, they concluded that collaborative practice had four other critical attributes besides cooperation and assertiveness. These were:
1. shared responsibility for planning 2. shared decision-making 3. open communications 4. coordination.
From this they were able to define collabo- rative practice as:
Nurses and physicians cooperatively work- ing together, sharing responsibility for prob- lem-solving and decision-making, to for- mulate and carry out plans for patient care (Baggs & Schmitt 1988, p.145).
Baggs & Schmitt argued that the NCJP pro- vided little theoretical justification for their choice of es,entlal factors for collaborative practice, but that anecdotal evidence from both doctors and nurses working in Demonstration Project Units suggested that patient care had improved.
Baggs & Schmitt's paper provides a critical review of the major work on this concept. In a series of relational statements taken from the literature, they underpin the reasons why the subject is so important. Summarised, they state that effective collaboration can lead to improved patient mortality rates, fewer patient readmissions to ICU, decreased costs, better efficiency, less nursing stress, improved quality of care, increased patient satisfaction, and greater nursing job satisfaction. It is immedi- ately apparent that whilst patients and nurses gain from collaborative practice according to this summary, doctors are not mentioned. It seems feasible that Baggs & Schmitt have either assumed that the medical staff will focus upon better patient outcomes as reason enough to support collaboration, or that they have marginalised the medical staff. Based upon the

Collaborative practice within the intensive care unit: a deconstruction 67
conclusions in this review, however, Baggs &
Schmitt emphasised that there was a need for an instrument to measure collaborative practice - - which Baggs then went on to develop.
Following the arguments cited above, Baggs et al (1992) conducted a research study that gen- erated data supporting the association of coll- aboration and ICU patient outcomes. They chose one aspect of specific ICU decision-mak- ing, that of transfer of a patient from ICU. It is well-documented that transferring a patient, either within a hospital or to another setting (per- haps for specialist treatment or to be nearer rela- fives) can be linked to patient outcomes of either death or readmission to ICU (Franklin &Jackson 1983, 1Kubins & Moscowitz 1988). Baggs et al (1992) distributed a questionnaire to 56 nurses and 31 physicians working on one Medical ICU. They had developed a new Likert-type instru- ment of global questions, known as a Decision about Transfer Scale (DATS), which investigated satisfaction as well as outcome. Both nurses and physicians were given the CPS (Weiss & Davis 1985), and nurses were given the Index of Work Satisfaction (IWS). Both instruments had estab- lished validity and reliability (Weiss & Davis 1985, Stamps & Piedmonte 1986). It is not clear why medical staff were not given the IWS. Although the IWS concerns nursing job satisfac- tion, Baggs et al do not specify how they then measured physician job satisfaction.
The questionnaires were distributed during 286 consecutive patient decisions regarding transfer of patients to a ward within the same hospital, consequently before outcomes were known. Patients were observed for 30 days after transfer, or until hospital discharge or death, whichever occurred first. The nurse and physician responsible for each patient were asked to complete the DATS. As there were more patient transfers than there were individ- uals in the sample, it is reasonable to assume that the sample group must have completed more than one DATS each, although this is not made particularly explicit.
Nurses and doctors scored quite similarly on satisfaction, but very differently on collabora- tion. Baggs et al (1992) concluded that satisfac- tion and collaboration were strongly linked for nurses, but only weakly to moderately for doc- tors. However , they could not elicit whether collaboration had the same meaning for the
two groups, nor how much influence on patient outcomes collaboration had. Despite printing their definition of collaboration on the form, there were widely differing ideas o f how much collaboration occurred. Nurses felt it meant a better outcome, but medical staff did not. Baggs et al generated the theory that the more complex a situation was, the more important collaboration became.
Severity of illness has long been an indicator of patient outcome, and most ICUs have both
accepted and adopted a tool known as APACHE II (Acute Physiology and Chronic Health Evaluation). APACHE II allocates points for age, chronic disease, and the degree of physi- ological derangement as indicated by specified tests. These points as a total score are a useful predictor of patient outcome and are widely used (Knaus et al 1986). Although there are crit- icisms of this tool (Boyd & Grounds 1993, Oh et al 1993), it does provide some objective data regarding outcomes. Baggs et al (1992) con- trolled for this by collecting APACHE II scores for all eligible patients during their first and last 24 hours on the ICU, but found that this had no statistically significant relationship to collabora- tion as measured in the study.
Overall, the study appears to have been rig- orously conducted, although there were no definitive conclusions. Collaboration could not really be identified as a factor in patient out- comes, as it was not a crucial variable. The writers were cautious in stating their results, emphasising the need for replication studies in other areas. It is clear from Baggs' work with others, however, that collaboration is linked to nursing job satisfaction and could possibly be a factor in ICU patient outcomes (Baggs & Schmitt 1988, Baggs et al 1992). Her most recent work, the development of an instrument to measure collaboration and satisfaction about care decisions (CSACD), has further confirmed this (Baggs 1994). Indeed, many articles in the literature have utilised the CSACD in under- lining the importance of collaboration.
T H E D O C T O R - N U R S E G A M E
The impetus for the study, which included this analysis of literature, was further influenced by the proposals of Stein et al (1990): the 'doc- tor-nurse game'. This is a series of reflections comparing the current scenario with the find- ings of a study they had conducted in 1967. Twenty years ago, both doctors and nurses agreed that their relationship was hierarchical. Nurses made recommendations to doctors without appearing to do so and the resultant actions were seen to have been initiated by the doctor. Likewise, a doctor could ask for advice from a nurse, but in such a way that it did not look as if they were asking. The cardinal rule was to avoid open disagreement, and if the game succeeded both parties were rewarded. Patient care was efficient and the physicians used nurses as consultants, which raised nurses' self-esteem. Through the alliance, doctors gained respect. There were penalties for failure

68 Intensive and Critical Care Nursing
too, as doctors who did not recognise nurses were seen as 'clods'. Likewise, nurses who were too outspoken had 'hell to pay!' Their respec- tive training enforced the rules of the game. Nurses learnt that making a suggestion to a doctor was paramount to an insult, because it was questioning the doctor's knowledge. At the same time, nurses were told they had to make suggestions, thus 'the way out of the bind was to use the doctor-nurse game and commu- nicate the recommendation without appearing to do so' (p.546). Stein et al describe many changes since then: an increase in female doc- tors and male nurses; fewer nurses; the erosion of the handmaiden image; nurses as advanced practitioners; poor working conditions and others.
Stein et al suggest that by 1990, nurses had stopped playing the game because the relation- ship had changed in five ways:
1. Nurses' goals have changed; they want more autonomy and to be seen as equal partners with the whole multidisciplinary team (not
just doctors). 2. Nurses' motivation has changed, mostly
because of the civil rights' and women's movements.
3. There is a vehicle for change; nurse educa- tion is very different now. Socialisation is towards collegiality rather than hierarchical relationships.
4. Effects on nurses; they feel free to challenge and confront doctors, and can make many decisions without consulting the medical staff.
5. Effects on doctors; they feel betrayed, angry and puzzled, as they never saw the relation- ship as hierarchical in the first place. Doctors are confused by this.
Stein et al (1990) assert that due to these changes, doctors are of the opinion that nurses no longer want to nurse, a situation they are unhappy with as they prefer nurses who cheerfully do as they are told. The writers point out that those in power often never realise the oppression this causes. Although this changed relationship may seem negative, 'physicians and nurses can both benefit if their relationship becomes more mutu- ally interdependent. Subservient and dominant roles are both psychologically restricting. When a subordinate becomes liberated, there is the poten- tial for the dominant one to become liberated too' (Stein et al 1990, p.549).
Whilst the 'doctor-nurse game' is an oft- acknowledged concept in the literature, there has been little research on it. However , Pilliteri & Ackerman (1993) attempted to redress this deficit in an interesting diary study. They high- lighted the fact that although in recent studies on nurse abuse patients were the most guilty of it, doctors in fact came second. In their qualita-
tive approach, they compared the doctor-nurse interactions recorded in the journals o f t w o
similar doctors, who had practised 100 years apart. They then analysed common areas of the doctor-nurse relationship and found some sur- prises. In 1888 nurses gained most of their learning from doctors. In 1990, doctors acknowledge learning from nurses. Both doc- tors wished that nurses would take more responsibility, but in 1990 the doctor acknow- ledged that nurses did take quite a lot of responsibility. In 1888, there were some spe- cific examples of doctor-nurse collaboration, although none were cited in the 1990 journal. Both doctors complained of being very tired and being woken at night, which they felt the nurses did not understand or appreciate, which could lead to conflict. Neither doctor inter- acted with nurses socially. Both doctors felt they had more authority than nurses and both complained about nurses who were assertive. Whilst the researchers acknowledge the limita- tions of such a small study it does raise some interesting points, especially in the light o f the doctor-nurse game. In the 100 years between the opinions o f these two doctors, little has really changed. Whilst nurses are now con- tributing to decision-making, have more responsibility and act more asserfvely, doctors do not seem to have changed their attitudes much and still find conflict for similar reasons.
Although there are few British studies that lend insight to the collaboration phenomenon, Busby & Gilchrist (1992) were disappointed by their own results. They hypothesised that as studies on cooperation and teamwork are now dated, the role of the nurse should be much more autonomous. As advocates and com- municators, nurses should have a valid part in the ward team. Using questionnaires and inter- views with a sample consisting o f 33 consul- tants, 14 nurses, and eight patients, they observed three ward rounds. Contrary to their research hope, it was apparent that medical staff dominated and that nurses did not assert them- selves on ward rounds. Mthough nurses were asked for information about patients, they were rarely asked for an opinion. Altogether, only 12% of comments made on these ward rounds were made by nurses. W h e n interviewed, the majority of nurses expressed a desire for more cooperation, but only 18% of the doctors sup- ported the same view.
R E D E F I N I N G C O L L A B O R A T I V E P R A C T I C E
It appears from the literature that nurses have changed, that they are more autonomous and

Collaborative practice within the intensive care unit: a deconstruction 69
have more role responsibility. Perhaps their atti-
tudes have changed with this, although few
doctors appear to have adapted to this emergent nurse role and are still holding on to the 'doc-
tor-nurse game'. Even so, it is gratifying to see
doctors wri t ing in a way that challenges this (Stein et al are all physicians), as most o f the
literature on collaborative practice emanates from nurses. It is of some concern that so many have writ ten about the p h e n o m e n o n in a way that constitutes little more than 'doctor-bashing' (Brooking 1991). As influential writers, on the subject, Weiss & Davis (1985) only elucidate
the positive effects o f collaborative practice in a
general or nurse-specific way. Baggs (1994)
attempts to l ink it to improved patient out-
comes (positive for both doctors and nurses), but only clearly demonstrates the l ink with
enhanced nursing j o b satisfaction. These three are no t the only examples of views concerning collaborative practice, bu t they do provide a fairly comprehensive in t roduct ion to current thought and work on the phenomena associated with the concept of collaborative practice.
O n reading this literature, two important
themes surfaced. The overwhe lming majority of research on collaborative practice appears to
have been conducted in the USA, most o f
which has been in the form of large surveys, analysed by means of statistics. The few British
studies have confirmed that there is little coll- aboration, bu t there is no discussion of the under ly ing principles (Busby & Gilchrist 1992, Gregson et al 1992). The numerous claims regarding collaborative practice suggest that it is a crucial feature in ICUs in reducing mortality, bu t this is no t empirically demonstrated at any point . Whils t it is clearly connected to nurs ing
j o b satisfaction, this in itself is no t necessarily
l inked to patient outcomes. Isolating collabora- tive practice as a variable in patient outcomes
currently appears impossible and yet it is
repeatedly claimed as such (Franklin & Jackson 1983, iKubins & Moskowitz 1988, Mitchell et al 1989, Baggs 1994). Al though slightly differ- ent meanings are given to the p h e n o m e n o n , the overall impresson from the literature indi-
Cates that collaborative practice is concerned with trust be tween doctors and nurses. A n
amalgamated defini t ion constructed from the evidence discussed in this paper could be:
Collaborative practice is the recogni t ion of and respect for each participant's un ique expertise in health care delivery. Doctors and nurses work together non-hierarchical ly in contr ibut ing to decisions made together about the patients. The relationship is char- acterised by trust and mutual communica - tion. This leads to increased j ob satisfaction and better patient outcomes.
In seeking to explore collaborative prac-
tice as a p h e n o m e n o n wi th in an I C U , this
def in i t ion f rom the li terature needs to be con -
sidered very carefully. Is it measurable? Is it realistic? Is it desirable? Decons t ruc t ion o f the
li terature leads to a gut react ion o f ' n o ' on all
counts, bu t research is indicated in order to u n d e r p i n this. A l though I C U doctors and nurses all wan t the best for their patients, concre te truths and pointers are needed, rather t h a n mere speculat ion or impossible directives.
REFERENCES
AACN 1982 Collaborative practice model: the organization of human resources. American Association of Critical Care Nurses, Newport Beach
Baggs J G 1994 Development of an instrument to measure collaboration and satisfaction about care decisions. Journal of Advanced Nursing 20:176-182
BaggsJ, Schmitt M 1988 Collaboration between nurses and physicians. Image 20:145-149
Baggs J, tKyan S, Phelps C, Richeson J, Johnson j 1992 The association between interdisciplinary collaboration and patient outcomes. Heart and Lung 21:18-24
Birenbaum R 1994 Nurse practitioners and physicians: competition or collaboration? Canadian Medical Association Journal 151 (1): 76-78
Boyd O, Grounds P,, M 1993 Physiological scoring systems and audit. Lancet 341 (8860): 1573-1574
BrookingJ 1991 Doctors and nurses: a personal view. Nursing Standard 6 (12): 24-28
Busby A, Gilchrist B 1992 The role of the nurse in the medical ward round. Journal of Advanced Nursing 17 (3): 339"346
Coluccio M, Maguire P 1983 Collaborative practice: becoming a reality through primary nursing. Nursing Administration Quarterly 7:59-63
Denzin N K 1989 Interpretive mteractionism. Sage, Newbury Park
Dunbar S, Bryan-Brown C 1988 Collaborative practice model. In: Boiler J (ed) International Conference on Collaborative Practice. American Association of Critical Care Nurses, Newport Beach, pp. 7-8
Franklin C, Jackson D i983 Discharge decision-making in a medical ICU. Critical Care Medicine 11:62-66
Gregson B A, Carflidge A M, BondJ 1992 Development of a measure of professional collaboration in primary health care. Journal of Epidemiology and Community Health 46 (1): 48-53
Hamilton S 1991 Collaborative practice is necessary in ICU. Nurse Manager 22: 96J-96L
Henneman E A, LeeJ L, CohenJ I 1995 Collaboration: a concept analysis. Journal of Advanced Nursing 21: 103-109
Hiderly L J 1991 Nurse-physician collaborative practice. The clinical nurse specialist in a radiation oncology private practice. Oncology Nursing Forum 18 (3): 585-591
Holland S, Ward C 1990 Assertiveness: a practical approach. Winslow Press, Oxon
Johnson N D 1992 Collaboration - - an environment for optimal outcome. Critical Care Nursing Quarterly 15 (3): 37-43
Jones P,. A 2994a Conceptual development of nurse-physician collaboration. Holistic Nursing Practice 8 (3): 1-21

711 Intensive and Critical Care Nursing
Jones R A 1994b Nurse-physician collaboration: a descriptive study. Holistic Nursing Practice 8 (3): 38-53
Kilmann R, Thomas K 1977 Developing a forced-choice measure of conflict-handling behavior: the MODE instrument. Educational and Psychological Measurement 37:309-325
King J, Morris L, Fitz-Gibbon C 1987 How to assess program implementation. Sage, Beverley Hills
King L, Lee J L, Henneman E 1993 A collaborative practice model for critical care. American Jourual of Citical Care 2 (6): 444-449
Knaus W A, Draper E A, Wagner D P, Zimmerman J E 1986 An evaluation of outcome from intensive care in major medical centers. Annals of Interual Medicine I04:410-418
Krans W A 1980 Collaboration in organizations. Human Sciences Press, New York
Lewis F M 1985 Collaboration: alternative models and consequences. Conference paper. Cited in: Baggs JG, Schmitt MH. Collaboration between nurses and physicians. Image 20:145-149
Mitchell P, Armstrong S, Simpson T, Lentz M 1989 AACN Demonstration Project. Heart and Lung 18: 219-237
National Institute of Health (NIH) 1983 Consensus Conference Critical Care Medicine. Journal of the American Medical Association 250:798-804
National Joint Practice Commission (NJPC) 1981 Guidelines for establishing joint or collaborative practice in hospitals.' Neely Printing Co, Chicago
Oh T E, Hutchinson R, Short S, Buckley T, Lin E, Leung D 1993 Verification of the APACHE scoring system
in a Hong Kong ICU. Critical Care Medicine 21 (5): 698-705
Pilliteri A, Ackerman M 1993 The 'Doctor-Nurse Game': a comparison of 100 years - - 1888-1990. Nursing Outlook 41:113-116
Roberts S E 1987 The role of collaborative nursing diagnosis in critical care. Critical Care Nurse 7:81-86
Rubins H, Moskowitz M 1988 Discharge decision- making in a MICU. American Journal of Medicine 84:863-869
Stamps P L, Piedmonte E B 1986 Nurses and work satisfaction. Health Administration, Ann Arbor
Stein L I, Watts D T, Howell T 1990 The doctor-nurse game revisited. New England Journal of Medicine 322:546--549
TaylorJ S 1995 Interpreting the critical arena: a reconstruction of collaborative practice within the intensive care unit. Unpublished Masters thesis, University ofHuddersfield, Huddersfield
Thomas K 1976 Conflict and conflict management. In:
Dunnette M (ed) Handbook of industrial and organizational psychology. Rand McNally, Chicago, pp.889-935
Weiss S J 1983 Role differentiation between nurse and physician: implications for nursing. Nursing Research 32 (3): 133-139
Weiss S, Davis H 1985 Validity and reliability of the Collaborative Practice Scales. Nursing Research 34: 299-305
Wonsetter L A O 1987 Perceptions of nurse-physician collaboration in an emergency department setting. Medical College of Ohio, PhD thesis