Embed Size (px)
Citation preview
COLLABORATIVE MENTAL HEALTH CARE – WHERE COULD
WE GO?
Nick Kates, MB.BS, FRCP (C) MCFP (hon)
Chair, Dept. of Psychiatry
McMaster University
Quality Improvement Advisor,
Hamilton Family Health Team

Thank you
• Peter Selby • Arun Ravindran
• Marina Bourlak • Rosa Dragonetti • Myra Fahim • Julia Lecce
• Terry Isomura • Sari Ackerman
Plan
• Forces driving / enabling collaboration
• A new role for primary care
• Opportunities for improving the quality of
what we do
• Things that can make this happen
Forces Driving Collaboration –1997
The World in 1997
Forces driving better collaboration in 1997
• Problems in the relationship
• Need to improve access / wait times
• Desire to support primary care / increase
skills and comfort
• Need to improve communication between
the two sectors
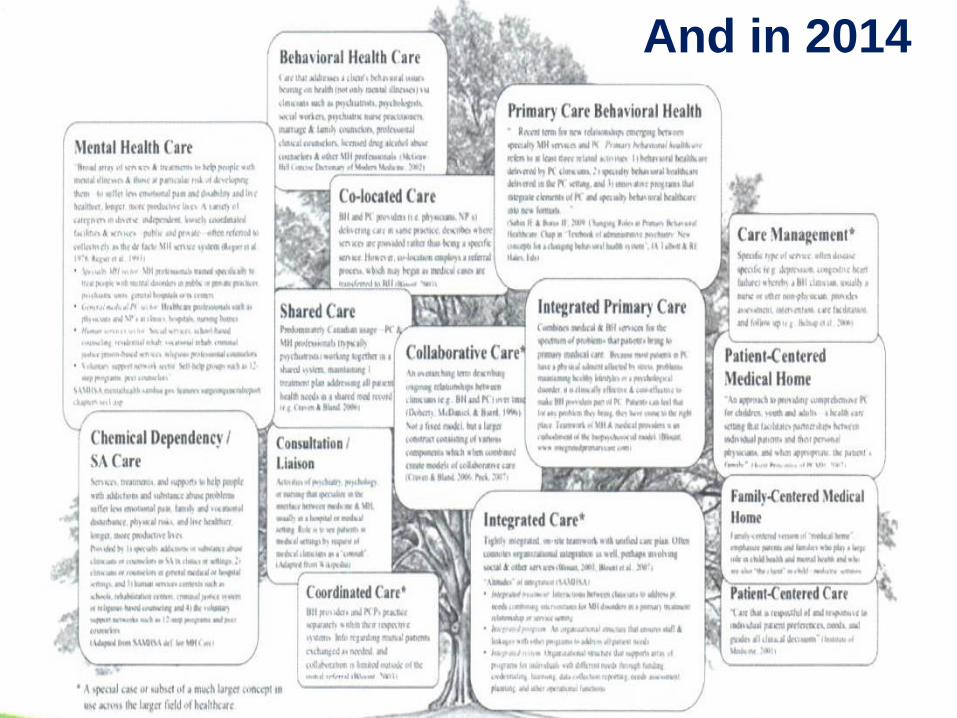
And in 2014
Forces driving better collaboration
• Reducing preventable emergency visits
• Containing costs/ increasing efficiencies
– Reducing preventable ED visits
– Improving transitions
• Addressing co-morbid conditions / complexity (Health links)
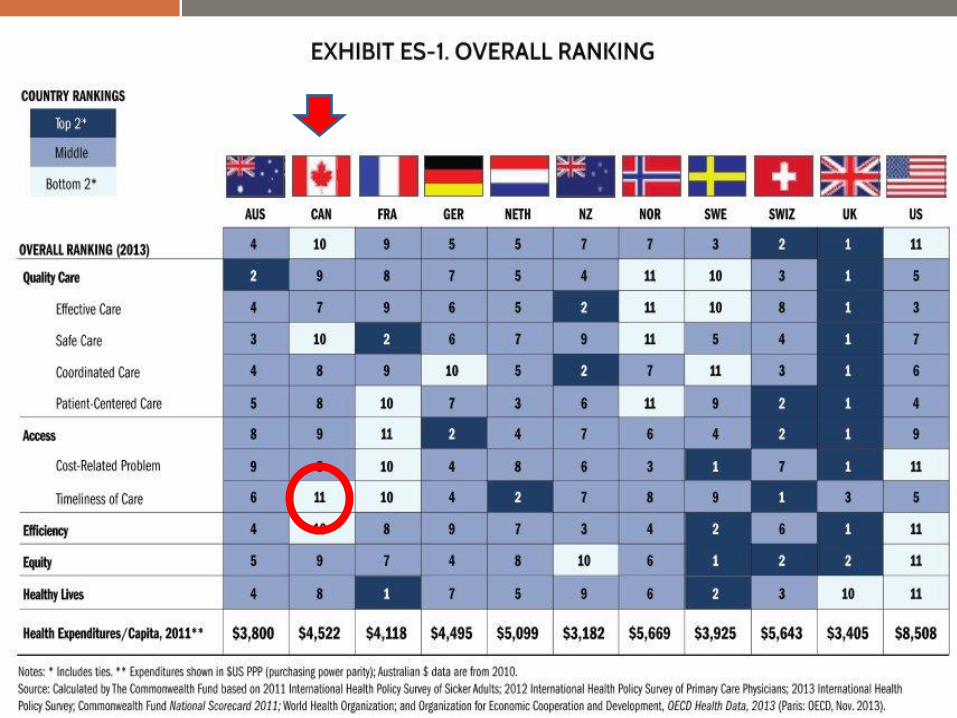
• Improving the quality of care
• Reducing disparities
• Increasing evidence that it works
• Acceptance by funders and planners
Other factors
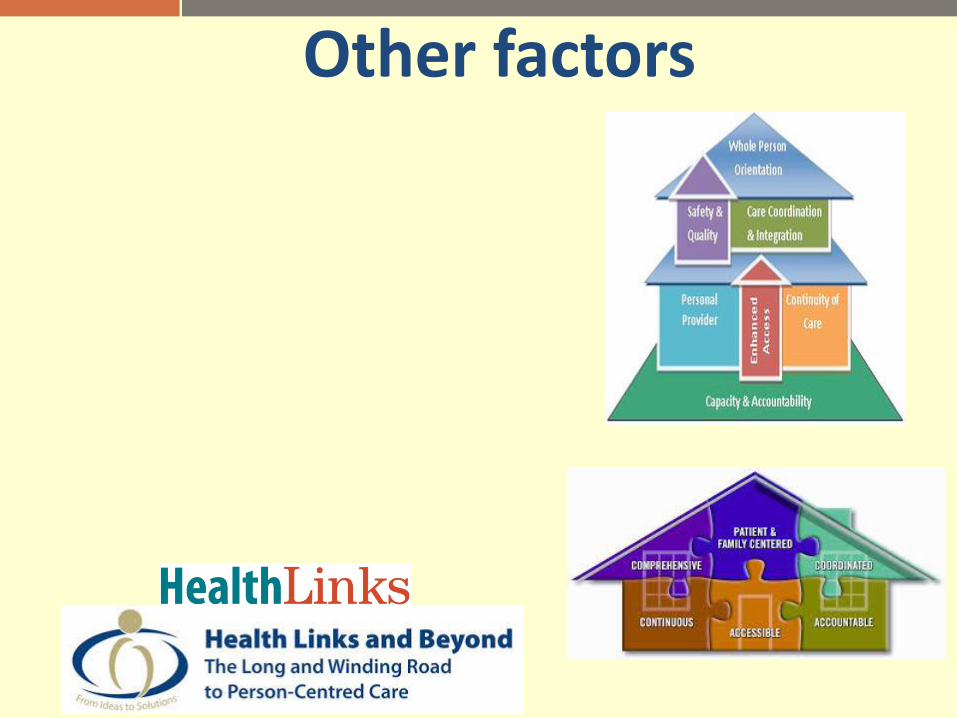
Other factors
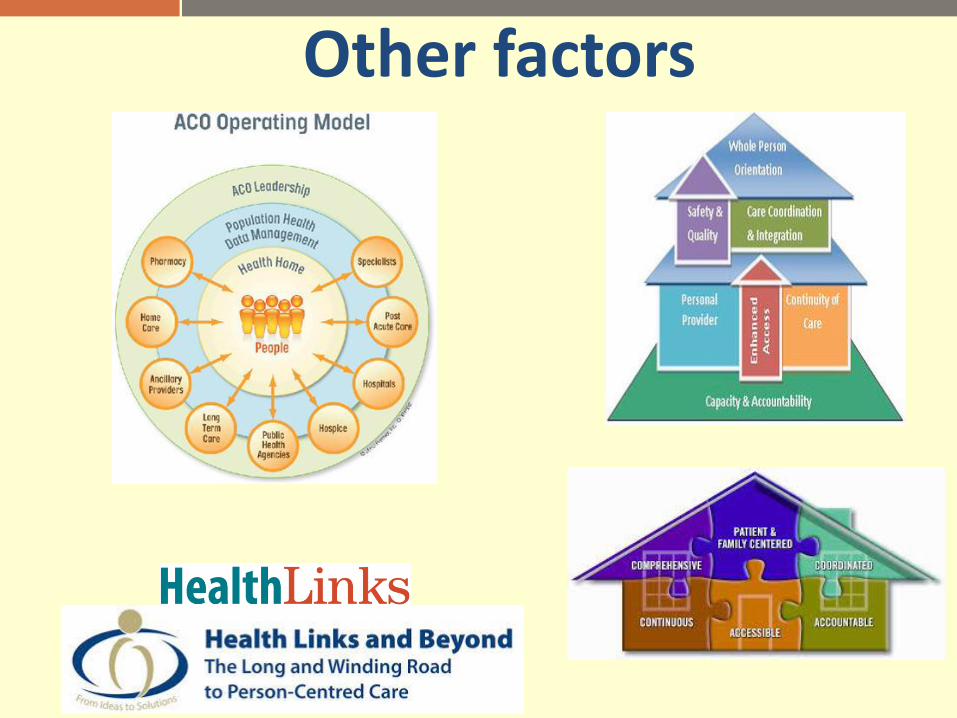
Other factors

And ……….
The economic impact of Integration Impact for Psychiatry
AMA resolution to implement integration of Physical and Behavioural Health
Focus on Integrating Physical & Behavioural health

Co
What works – key principles • Policy & plans
• Advocacy
• Training
• Doable and limited interventions
• Mental health service support
• Co-ordinators or care
• Access to medication
• Resources – human and funding
• Collaboration with other sectors
• Process not an event
Crossing Boundaries (Kings College Mental Health Foundation)
• Multidisciplinary Teams
• Information-Sharing
• Shared care protocols
• Joint funding
• Liaisons
• Navigators
• Reducing stigma
• Research
• Co-location
9 key components for successful collaboration
What works – key elements 011 Position paper
• Care Co-ordinator
• Access to Psychiatric consultant
• Enhanced consumer education
• Introduction of evidence-based approaches
• Screening of people with chronic medical
conditions for depression or anxiety
• Skill enhancement for primary care providers
• Access to brief psychological therapies
Importance of personal contacts
Friendship Balance Respect Equality
Qualities of a good consultant • Affable • Available • Able
What still prevents us from collaborating • Physician remuneration models
• Funding models
• Attitudes
• Cultures of care
• Power and control
• Comfort / convenience
• Training
• Not taking full advantage
of team
• How are our systems are designed
Thought for the Day
Systems are
perfectly
designed to get
the results they
achieve. Paul Batalden
Failures to collaborate are often system failures
Improving collaboration
Better collaboration and delivering better quality care require changes in
the way our systems of care are conceptualised and organized, both
within and between systems.
Where could we be heading and what can we achieve –
the vision thing
Beware of Great Predictions
In 1943 Thomas Watson, Chairman of IBM, reportedly predicted:
“I think there is a world market for about five computers.”

We need a new vision of the role of primary care in an integrated
mental health system
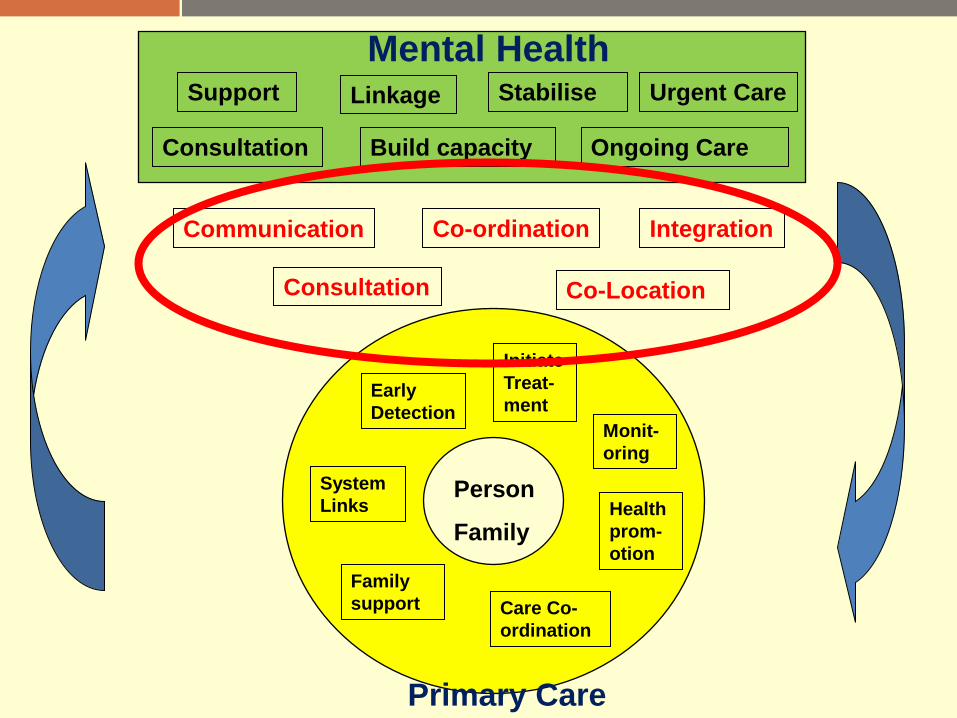
The potential role of Primary Care Looks after a population
Enduring relationships with the individual and their family
Screening and early detection
Initiation of treatment
Monitoring and follow-up
Co-ordination and continuity of care
Referral and system navigation
Family interventions
Point of entry into an integrated MH&A system
Could provide more (and effective) MH&A care
Mental Health and Addiction Services
• Provide rapid access to consultation and advice
• Respond quickly to help with urgent problems
• Priorize people who cannot be managed in PC
(complexity /resources) and provide ongoing care
• Stabilize problems, and return to primary care providers for ongoing management and monitoring,
• Continue to be available to / support the PC Team (shared care)
• Provide information on and link with community resources
Early
Detection Monit-
oring
System
Links Health
prom-
otion
Initiate
Treat-
ment
Care Co-
ordination
Family
support
Communication
Co-Location
Integration Co-ordination
Consultation
Primary Care
Person
Family
Consultation
Urgent Care
Ongoing Care
Linkage Support
Mental Health Stabilise
Build capacity
How do we take full advantage of the role that primary care
can play?

- Effective
- Safe
- Timely
- Consumer and family- centered
- Equitable
- Efficient
- Integrated
- Focused on population health
Quality health care
A high-performing health system that is:
More effective care - Increasing the capacity and skills of primary care
• Translate MH concepts and tools
• Teach / model relevant skills – Motivational Interviewing – PHQ-2
• In-Office education Program / on-line resources
(BCs Adult Mental Health Module) • Child / geriatrics / addictions
• Increasing comfort Primary Mental
Health Care is not just Mental Health Care in a Primary Care Setting
Primary Mental Health Care is not just Mental Health Care in a Primary Care Setting

Safer care
• Every person has a plan and is given a copy of their plan, which is updated at every visit • Medication reconciliation at every visit • Transitions

More efficient care
• Better integration of physical and mental health care – Co-morbidities
– Complex conditions
– Opportunities for earlier detection
– Addictions
– Medical care of people with mental health problems (reverse shared care)
DETECT PROBLEMS EARLIER (AND INTERVENE!)
• Enhanced 18 month visit
– Not an end
– Follow-up
– Identify those at greatest risk (Red, yellow, green)
– Make sure those with needs reach services they require
In my
beginning is my end
TS Elliot
Population focus
• Proactive care
– Monitoring
– Relapse prevention

Better integrated care
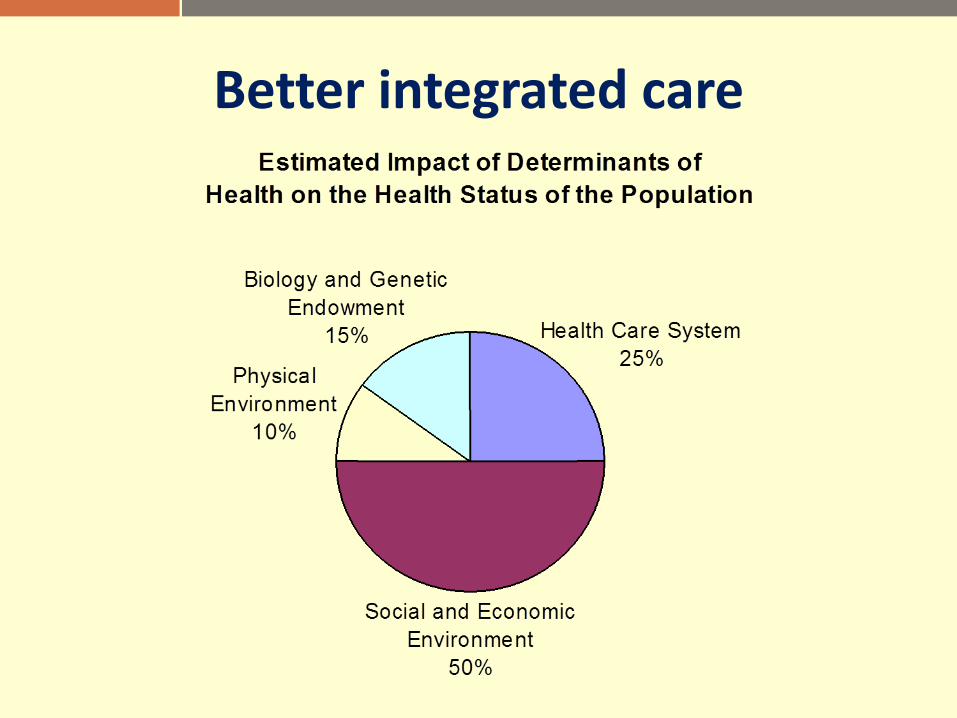
Better integrated care

Community partnerships
• Need to address social and environmental determinants
• Need to work with community partners
• Build community resilience
Need to improve care for individuals
• Comprehensive plans
• Address non-medical issues
• System navigation
• Working in agencies
Integrate Community Programs within Primary Care Settings
“To alter our delivery system to reduce costs and put an emphasis on prevention”
The Second Stage of Medicare
CONSUMER CENTRED CARE
Re-designing services based on a person or family’s experience
Family engagement
Promote recovery / support self management
Reducing inequities
More equitable care
• Address disparities in access as well as outcomes • Identify and eliminate stigma in our own settings
Enablers to help us get there
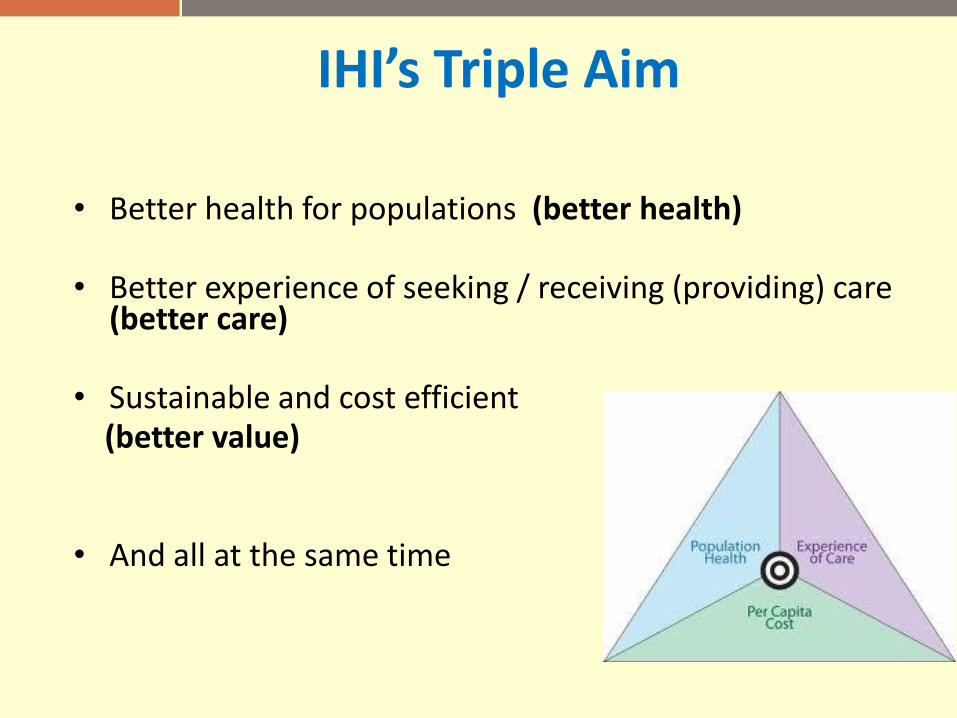
IHI’s Triple Aim
• Better health for populations (better health)
• Better experience of seeking / receiving (providing) care (better care)
• Sustainable and cost efficient (better value)
• And all at the same time

Making the case for Collaborative Mental Health Care
• Evidence
• Advocacy
• Networks (tipping point)
• Spread of ideas that work
• Cost-benefit analyses
Preparation of Future Practitioners
• Training
• Competencies
• Preparation