Embed Size (px)
Citation preview
COLLABORATIVECASE MANAGEMENT
S E P T / O C T 2 0 1 4 • V O L U M E 1 2 , I S S U E 0 1 • I S S N 2 3 2 8 - 4 4 8 X
A Publication for Health Care Delivery System Professionals
T H E O F F I C I A L P U B L I C AT I O N O F T H E A M E R I C A N C A S E M A N A G E M E N T A S S O C I AT I O N
M E N T O R S H I P I N C A S E M A N A G E M E N T :
Identifying Opportunities and
Employing Practical Strategies
C O N T I N U I N G E D U C A T I O N C R E D I T S I N T H I S I S S U E !
COLLABORATIVECASE MANAGEMENT
S E P T / O C T 2 0 1 4 • V O L U M E 1 2 • I S S U E 0 1
“Case management in hospital and health care systems is a collaborative practice model including patients, nurses, social workers, physicians, other practitioners, caregivers and the community. The case management process encompasses communication and facilitates care along a continuum through effective resource coordination. The goals of case management include the achievement of optimal health, access to care and appropriate utilization of resources, balanced with the patient’s right to self-determination.”
Approved by ACMA membership, November 2002
PUBLISHER
L. Greg Cunningham, MHACEOACMA / Little Rock, [email protected]
EDITOR
Tyler NeeseDirector, Public Policy and CommunicationsACMA / Little Rock, [email protected]
EDITORIAL BOARD
Reggie Allen, MBA, RNSystem Director, Clinical OperationsCHRISTUS Health • Irving, TXPaul Arias, RN, BSN, MISCorporate Director Care ManagementLifebridge Health • Baltimore, MD
Frank B. Bellamy, RN, MSN, ACMInterim Director, Case ManagementRockford Memorial Hospital • Rockford, IL
Colleen Booz Dittrich, LMSW, CCM, ACMManager, Case ManagementThe University of Kansas Hospital • Kansas City, KS
Joan Brueggeman, RN, BSN, CPUMClinical Manager, Utilization Management and Care CoordinationGundersen Health System • La Crosse, WI
Dani Hackner, MDMedical Director, Case ManagementCedars-Sinai Medical Center • Los Angeles, CATimothy Morrison, LCSW, ACMDirector, Clinical Support ServicesStanford Hospital and Clinics • Stanford, CA
Ann Scotti, LCSW, ACMDirector, Care CoordinationSt. Peter’s University Hospital • New Brunswick, NJ
Nancy Sullivan, MBA, CMACDirector, Case ManagementMassachusetts General Hospital • Boston, MA
Collaborative Case Management is published bimonthly by the American Case Management Association (ACMA) 11701 West 36th Street, Little Rock, AR 72211 Telephone: 501-907-ACMA (2262).Subscription is a benefit of membership in ACMA. Memberships are available at $135.00 per year. Student membership is open to individuals enrolled in a full time academic program at $60.00 per year. More detail about membership categories is available at the ACMA website, www.acmaweb.org or by calling 501-907-2262.Photocopying: No part of this publication may be reproduced in any form or incorporated into any information retrieval system without the written permission of the copyright owner. For reprint permission, please contact ACMA, 11701 West 36th Street, Little Rock, AR 72211.The statements and opinions contained in the articles of Collaborative Case Management are solely those of the individual authors and contributors and not of the American Case Management Association. The Publisher and Editor disclaim responsibility for any injury to persons or property resulting from any ideas or products referred to in the articles or advertisements.Copyright © 2014 American Case Management Association. All rights reserved
3 Mentorship in Case Management: Identifying Opportunities and Employing Practical StrategiesPaula Lenhart, RNC, MSN, CNS, ACM, FABC
6 Collaborative Case Study: Readmissions Reduction
Tackling All Cause Readmissions: One Integrated Health System’s ApproachJoan Brueggeman, RN, BSNMichelle LaFleur, RN, BSN, MHALisa Sheldon, BS
12 Progression of Care Innovations: Employment of Video Debriefing, Scripting, and Scoring to Improve Quality of Multidisciplinary RoundsMegan Olman, LCSW, ACM
15 Heart Failure Readmissions Cuts May be a Phone Call AwayBruce Jancin
COLLABORATIVE CASE MANAGEMENT | ACMAWEB.ORG
3
Mentorship in Case Management: Identifying Opportunities and Employing Practical Strategies Paula Lenhart, RNC, MSN, CNS, ACM, FABCTHIS AUTHOR HAS NO FINANCIAL RELATIONSHIPS WITH COMMERCIAL INTERESTS TO DISCLOSE.
LEARNING OBJECTIVES1. Recognize the value and
benefits of mentorship within case management practice.
2. Identify opportunities to both mentor and be mentored.
3. Implement practical and effective mentorship strategies
Case managers, by trade, have a wide variety of responsibilities. The system care management team at Memorial Hermann is no exception; they provide education to executive leaders, physicians and the case management teams, ensure program integrity, manage any necessary Medicare-related changes, and interface with payers
and resource providers to address issues, among many other critical tasks. In many ways, case management professionals act as the liaisons between all of the elements to help facilitate patient care delivery resulting in efficient and timely patient discharges.
In this role there are many opportunities to mentor and be mentored. Case managers interact with staff members from every corner of the hospital system, who all have unique approaches to their work and to interpersonal relationships. Taking the time – both formally and informally – to learn from those relationships and to share best practices can ultimately make valuable differences in patient care and hospital efficiency. Mentoring can improve morale, increase
The Memorial Hermann Health System includes 10 acute care facilities, two freestanding rehabilitation facilities, home health and Hospice services, and an independent living, skilled nursing facility and nursing home. Since many patients with widely varying needs, the efficiency and collaboration of case management professionals and all hospital professionals is critical. Case managers in all settings need to take a fresh look at mentoring and consider how they can use new strategies for teamwork and advising to provide better patient care.

SEPT/OCT 2014
4
retention, help on-board new employees, and train the next generation of leaders.
The good news is case managers and social workers are extremely qualified to be mentors. In a profession based on creative and collaborative problem solving, case managers and social workers have the tools at their disposal for great mentoring relationships. In fact, many case managers may already consider mentoring part of their job responsibilities – just perhaps in relation to their patients, not their colleagues. Perhaps even better news is focusing on mentoring is a very low-cost or even free option.INTENTIONAL AND UNINTENTIONAL MENTORSHIP
Mentorship in all forms can be useful, but it can primarily be broken down into two categories: intentional and uninten-tional. Intentional mentor-ship involves the formal construction of system sup-ports, which encourages collaboration and commu-nication. One example is the Medicare-mandated Utili-zation Management Com-mittee. The Memorial Her-rmann system care manage-ment team is seeking to provide further systemic mentorship by improving the committee structure and making compliance easier for individual campuses. Case Management directors researched the regulations and drafted the charter document, making it generic enough campuses could customize it to their needs. The skeleton of the document would be consistent from hospital to hospital, with core elements present in every version, making the committee structure easier to maintain and coordinate among campuses.
This would also allow campuses to coordinate their goals and plans for the year,
and for the system to provide broader education about the regulations and their implications. Additionally, it could ease the process for year-end evaluations. This kind of intentional mentorship – of which there
could be numerous iterations – is important for formalizing feedback mechanisms and ensuring supports exist.
Intentional mentorship also includes formal programs to link more experienced case managers with those newer to the profession, and to share knowledge and nurture the younger professionals. Some organizations are even undertaking “reverse mentoring,” where younger, lower-level
staffers are sharing new practices and innovations with their superiors. These advisory relationships can be hugely important to the individuals, to the hospitals where they work, and to the case management
profession as a whole. A mentor may make employees feel more accountable for their progress and build enthusiasm for their ongoing career at the hospital and in the field.
The structure of a devoted mentorship program will vary from hospital to hospi-tal, as the needs and culture of every workplace are different. It is important to be clear on the application process, the time commit-ment required, and the re-sponsibilities of all parties from the beginning. Early buy-in from team members is important in order to begin the recruiting process and build enthusiasm for the pro-gram. Throughout the im-plementation, garnering feedback and performing routine evaluations of the mentoring program is criti-cal. As with any initiative, it can be useful to refine expec-tations and processes.
However, unintentional mentorship, the day-to-day relationship building and sharing that occurs in our lives on and off the job, is just as important, if not more so for our professional growth. There is an opportunity in every conversation with a colleague to mentor that
person and to be mentored. For case managers, that mentorship can facilitate real innovation and improvements in patient care.
In the Memorial Hermann Diabetes Education Department, a patient who attended the regular support group meetings was a challenge for the facilitator and for his fellow group members. While most group members attended the meetings to discuss strategies for managing their blood sugar and

COLLABORATIVE CASE MANAGEMENT | ACMAWEB.ORG
5
support each other, this individual came to challenge the facilitator on diabetes research he had done on the Internet. Although his research was important to him, it kept the group off track. When the facilitator was ready to tell the patient he could no longer attend the group meetings, a mentoring moment between the facilitator and the care management team revealed a better solution.
The patient was invited to attend biannual personal meetings with the facilitator, where he could ask all of his research questions outside of the regular sessions. This solved the problem with the patient and with the group, and actually made the patient feel more confident about his role in the group. This casual, collaborative mentorship opportunity between the facilitator and the care manager helped the patient get what he needed, kept the facilitator from burning out on the responsibilities of managing the group, and kept the group functioning well. In a situation where the success of the program depends on the reputation of the program and of the hospital, it was a huge success.
IMPROVING MENTORSHIPThis brand of mentorship happens every
day at all levels of case management teams. Case management professionals (social workers and nurse case managers) are doing intentional and unintentional mentorship at every turn. However, this needs to become more systemic and more deliberate. Case management professionals have to think about the fact that, whenever they are in a dialogue with another person, it is an opportunity to mentor both positive and negative behaviors. For team leaders, this
means being intentional about respectful behaviors and attitudes, as they set the tone for how the entire group of people will behave in their department.
Obviously, in a hospital setting, this has to be done with care. It is not a case manager’s responsibility to tell a physician how to practice medicine. Telling a physician how to administer antibiotics would be out of scope. However, it is decidedly in scope to help the physician determine whether a patient’s admission order should be an in-patient or out-patient, recommend discharge plans, and plan post-acute services based on the patient’s clinical presentation. When case managers can develop these working relationships, they can bring something to the physician and gain information about how the medical plan will be developed. Case managers can help the physician and healthcare team learn more about what possibilities exist in regards to care planning for challenging patients, as well as the impacts of government regulations. This symbiosis ultimately benefits the patients.
It would also be in-scope to teach employ-ees the skill of mentoring in a formal way. It should be incorporated into formal education and encouraged throughout a case manager’s career. Although it can and does happen in the de facto manner described above, it will be much more prevalent and successful if done in a deliberate and thoughtful way. The best mentors are those who are working with their mentees in a committed and personal way, who take pride in sharing knowledge and wisdom. And mentors can certainly learn and improve from high-quality, accredited mentoring training programs.
Case managers and all professionals also should be open to being mentored throughout their workday. Many mentoring relationships are positive and productive, but there are critical skills that can be learned from even the harshest personalities. The workplace will not always be a positive environment, but every day can bring learning experiences if the employee is open to feedback and learning from others. Furthermore, the best mentors are those who recognize that lifelong learning moments exist and look to their relationships as opportunities to learn new techniques to improve their own practice.
ABOUT THE AUTHORPaula Lenhart, RNC, MSN, CNS, ACM, FABC, is the Senior Director of Care Management for Memorial Hermann Health System in Houston, Texas. In her current role, she is responsible for care management program development, education, and has oversight of clinical quality improvement. Ms. Lenhart also serves as coach and mentor to case management directors and case managers in skill development, and acts as a resource to hospital-based case management directors. She has more than 30 years of health care experience in the areas of nursing and case management. Ms. Lenhart earned an Associate’s Degree in Nursing from St. Mary’s School of Nursing in Minneapolis, Minn.; a Bachelor’s Degree in Nursing from the University of Minnesota School of Nursing; and a Master’s Degree in Nursing from the University of Texas Health Science Center at Houston, School of Nursing, in Houston, Texas.
6
SEPT/OCT 2014
Collaborative Case Study: Readmissions ReductionTackling All Cause Readmissions: One Integrated Health System’s Approach Joan Brueggeman, RN, BSN; Michelle LaFleur, RN, BSN, MHA; and Lisa Sheldon, BSTHESE AUTHORS HAVE NO FINANCIAL RELATIONSHIPS WITH COMMERCIAL INTERESTS TO DISCLOSE.
LEARNING OBJECTIVES
1. Identify the components of a successful readmissions reduction program.
2. Understand the processes and personnel involved in decreasing readmissions and avoiding CMS penalties.
3. Discuss tracking methods, metrics and measures used to determine the effectiveness of Gundersen’s readmissions reduction strategies.
ABOUT GUNDERSEN HEALTH SYSTEMGundersen Health System is an integrated
health system located in La Crosse, Wisconsin. A level II trauma teaching hospital with 325 beds, Gundersen Health System also includes outpatient clinics serving 19 counties in 3 states.
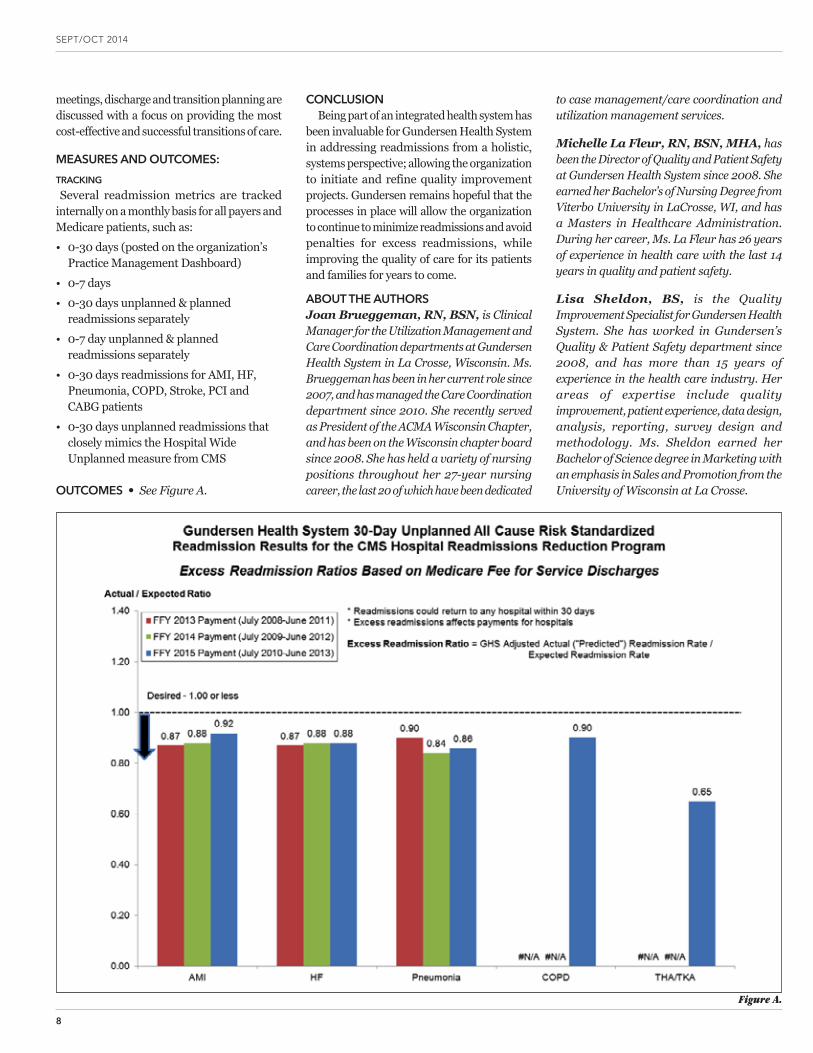
In October 2012, the Centers for Medicare and Medicaid Services (CMS) introduced a separate penalty program, which stemmed from the Patient Protection and Affordable Care Act and reduced payments to hospitals with excess 30 day readmis-sions for heart attack, heart failure and pneumonia patients (COPD and total hip/knee replacements were added to the con-dition list for FY 2015).
A readmission generally refers to an ad-mission to an acute care hospital within 30 days of a discharge from the same or another acute care hospital. Excess read-missions are measured by a ratio – divid-ing a hospital’s number of “predicted” 30 day readmissions for each condition by the
number that would be expected, based on an average hospital with similar patients. A ratio greater than 1.00 indicates excess readmissions. This data is risk adjusted, meaning it takes into account how sick patients are based on their age, gender and co-morbid conditions. The CMS readmis-sion maximum penalty is 2% of a hospital’s Medicare base operating diagnostic relat-ed groups (DRG) payments in 2014, and increases to 3% for 2015 and beyond. Re-sults are publicly reported on the CMS Hospital Compare consumer website – www.Medicare.gov/HospitalCompare.
This article will examine one health sys-tem’s approach to decreasing hospital readmissions and avoiding CMS penalties.

COLLABORATIVE CASE MANAGEMENT | ACMAWEB.ORG
7
In 2013, approximately 6,000 employees and 700 providers provided support or health care services for over 1 million outpatient services and 16,000 inpatient hospital admissions.
Gundersen Health System was one of the few health care systems nationwide deemed by CMS to be exempt from readmission penalties due to its low readmission rates – below 1.00 for excess readmission ratios for each condition (see figure A.). The following examines the processes and programs Gundersen Health System utilizes to minimize readmissions and maintain low readmission ratios for conditions, including: acute myocardial infarction (AMI), heart failure (HF), pneumonia, chronic obstructive pulmonary disease (COPD) and total hip/knee replacements (THA/TKA).
GUNDERSEN’S READMISSIONS REDUCTION STRATEGY
Gundersen’s readmissions reduction efforts are supported by a variety of departments, teams and practitioners, all of which contribute to a collaborative, effective strategy for efficient patient care. Gundersen’s philosophy centers on providing patient care and focused readmission projects or initiatives on all patients regardless of the payer or disease process. The focus is not simply preventing readmissions for the CMS diagnosis listed for penalties, but rather a focus on all patients who are at high risk for readmission. Gundersen has taken a multi-disciplinary approach to decreasing hospital readmissions, through which multiple projects, departments and practitioners contribute to the organization’s success. No one single department or program is solely responsible for successfully decreasing readmissions. Like spokes in a wheel, all of these areas have been critical in driving the organization’s overall decrease in readmissions.
TRANSITIONS OF CARE TASK FORCEThe focus of readmissions reduction efforts
at Gundersen included the development of a task force consisting of interdisciplinary members of the health system. The Transitions of Care Task Force includes nurses, clinical managers, administration, quality specialists, physicians, social services and other key contributors. The focus of the task force is to improve systems and processes that ensure high quality care. This methodology has been
beneficial as CMS focuses on penalties for certain conditions and possibly an all cause readmission penalty in the future.
The task force also focused on “foundational” concepts for patient care improvement, including daily interdisciplinary rounding at the bedside centered on the patient and family. Other improvement efforts were focused on ways to improve patient education packets at the hospital bedside, and included a patient “plan of the day,” teach back methodology, and medication reconciliation by pharmacy personnel upon hospital admission from the emergency department (ED).
The task force includes a readmissions review committee monthly meeting where a chart review occurs, examining three to five in-house patients who have readmitted within 0-7 days of their original discharge date. Almost 45% of Gundersen’s patients return within the first seven days, and thus this patient population is a specific focus for the organization. The meeting includes a chart review of the original admission and readmission, as well as a patient and family interview. A data collection tool is completed based on the findings from the review. Data is compiled and reported to the team monthly. The in-house reviews are performed by hospitalist providers, inpatient and outpatient nurses, pharmacists and social services.
Beyond the development of the readmissions task force, some of the other key departments and players that contribute to the organization’s readmissions reduction efforts are outlined in the following sections. These departments focus their efforts on high risk patients, transitions of care and enhancing the overall patient and provider relationship.
CARE COORDINATIONGundersen has a Care Coordination
department which focuses on services for the most medically complex patients seen in the health system (the top 1-3%). The care coordination program includes nurses and social workers who work together to help high risk patients and families navigate the health care system – in both the inpatient and outpatient settings. The Care Coordination nurses and social workers work to ensure the patient receives the appropriate care for their disease(s) while avoiding unplanned or unnecessary health care services. Care Coordination nurses and social workers are
already connected to many patients who are at high risk for readmission prior to their transition from the inpatient to the outpatient setting at time of hospital discharge. These pre-established relationships are valuable in assisting the patient and family as they move from a hospital setting to the home or lower level of care setting. Care Coordination staff partner with the patient and family promptly after hospital discharge to ensure discharge plans, medication adherence and follow-up visits are accurate and completed.
The Clinical Nurse Leaders (CNLs) are Master’s prepared nurses that work on the Medical-Surgical units in a separate role from the Care Coordination nurses. Unlike the Care Coordination nurses, the CNLs work only in the hospital setting. However, together the Care Coordination nurses along with the Clinical Nurse Leaders work to ensure successful transitions of care planning for high risk hospitalized patients.
Patients who are at high risk for readmission are identified by use of the LACE scoring tool during hospitalization, and then these patients receive a follow-up phone call from the CNLs or Care Coordination nurses within 48 hours of discharge. CNLs also chart review nursing home patients that return within 48 hours and document findings on a data collection tool.
Another program that Gundersen offers, which contributes to a decrease in readmissions from an organizational standpoint, is Gundersen’s end-of-life program, “Respecting Choices.” The Palliative Care department provides advanced directives and power of attorney for health care for patients with chronic medical conditions. Patients are identified as palliative, and end-of-life decisions are communicated to the care team and determined prior to hospitalization, thus avoiding unnecessary admissions or readmissions, dependent on what is outlined in the patient’s care plan.
One more “spoke in the wheel” at Gundersen in the organization’s efforts toward reducing readmissions is an interdisciplinary team that meets weekly to discuss hospitalized patients who have generated more than $125,000 in hospital costs, or who have been hospitalized for greater than 14 days with discharge barriers present. These meetings include representatives from Utilization Management, Social Services and Patient Financial Services – legal and other departments attend ad hoc. At these weekly
SEPT/OCT 2014
8
meetings, discharge and transition planning are discussed with a focus on providing the most cost-effective and successful transitions of care.
MEASURES AND OUTCOMES: TRACKING Several readmission metrics are tracked
internally on a monthly basis for all payers and Medicare patients, such as:• 0-30 days (posted on the organization’s
Practice Management Dashboard)• 0-7 days• 0-30 days unplanned & planned
readmissions separately• 0-7 day unplanned & planned
readmissions separately• 0-30 days readmissions for AMI, HF,
Pneumonia, COPD, Stroke, PCI and CABG patients
• 0-30 days unplanned readmissions that closely mimics the Hospital Wide Unplanned measure from CMS
OUTCOMES • See Figure A.
CONCLUSIONBeing part of an integrated health system has
been invaluable for Gundersen Health System in addressing readmissions from a holistic, systems perspective; allowing the organization to initiate and refine quality improvement projects. Gundersen remains hopeful that the processes in place will allow the organization to continue to minimize readmissions and avoid penalties for excess readmissions, while improving the quality of care for its patients and families for years to come.
ABOUT THE AUTHORSJoan Brueggeman, RN, BSN, is Clinical Manager for the Utilization Management and Care Coordination departments at Gundersen Health System in La Crosse, Wisconsin. Ms. Brueggeman has been in her current role since 2007, and has managed the Care Coordination department since 2010. She recently served as President of the ACMA Wisconsin Chapter, and has been on the Wisconsin chapter board since 2008. She has held a variety of nursing positions throughout her 27-year nursing career, the last 20 of which have been dedicated
to case management/care coordination and utilization management services.
Michelle La Fleur, RN, BSN, MHA, has been the Director of Quality and Patient Safety at Gundersen Health System since 2008. She earned her Bachelor’s of Nursing Degree from Viterbo University in LaCrosse, WI, and has a Masters in Healthcare Administration. During her career, Ms. La Fleur has 26 years of experience in health care with the last 14 years in quality and patient safety.
Lisa Sheldon, BS, is the Quality Improvement Specialist for Gundersen Health System. She has worked in Gundersen’s Quality & Patient Safety department since 2008, and has more than 15 years of experience in the health care industry. Her areas of expertise include quality improvement, patient experience, data design, analysis, reporting, survey design and methodology. Ms. Sheldon earned her Bachelor of Science degree in Marketing with an emphasis in Sales and Promotion from the University of Wisconsin at La Crosse.
Figure A.
ZYVOX® linezolid injection, tablets and for oral suspension Brief summary of prescribing information.
INDICATIONS AND USAGE ZYVOX is indicated for the treatment of infections caused by susceptible strains of the designated microorganisms in the specific conditions listed below. ZYVOX is not indicated for the treatment of Gram-negative infections. It is critical that specific Gram-negative therapy be initiated immediately if a concomitant Gram-negative pathogen is documented or suspected [see Warnings and Precautions]. Nosocomial pneumonia caused by Staphylococcus aureus (methicillin-susceptible and -resistant isolates) or Streptococcus pneumoniae. Community-acquired pneumonia caused by Streptococcus pneumoniae, including cases with concurrent bacteremia, or Staphylococcus aureus (methicillin-susceptible isolates only). Complicated skin and skin structure infections, including diabetic foot infections, without concomitant osteomyelitis, caused by Staphylococcus aureus (methicillin-susceptible and -resistant isolates), Streptococcus pyogenes, or Streptococcus agalactiae. ZYVOX has not been studied in the treatment of decubitus ulcers. Uncomplicated skin and skin structure infections caused by Staphylococcus aureus (methicillin-susceptible isolates only) or Streptococcus pyogenes. Vancomycin-resistant Enterococcus faecium infections, including cases with concurrent bacteremia. To reduce the development of drug-resistant bacteria and maintain the effectiveness of ZYVOX and other antibacterial drugs, ZYVOX should be used only to treat or prevent infections that are proven or strongly suspected to be caused by susceptible bacteria. When culture and susceptibility information are available, they should be considered in selecting or modifying antibacterial therapy. In the absence of such data, local epidemiology and susceptibility patterns may contribute to the empiric selection of therapy. The safety and efficacy of ZYVOX formulations given for longer than 28 days have not been evaluated in controlled clinical trials.
CONTRAINDICATIONS ZYVOX formulations are contraindicated for use in patients who have known hypersensitivity to linezolid or any of the other product components. Linezolid should not be used in patients taking any medicinal product which inhibits monoamine oxidases A or B (e.g., phenelzine, isocarboxazid) or within two weeks of taking any such medicinal product.
WARNINGS AND PRECAUTIONS Myelosuppression (including anemia, leukopenia, pancytopenia, and thrombocytopenia) has been reported in patients receiving linezolid. In cases where the outcome is known, when linezolid was discontinued, the affected hematologic parameters have risen toward pretreatment levels. Complete blood counts should be monitored weekly in patients who receive linezolid, particularly in those who receive linezolid for longer than two weeks, those with pre-existing myelosuppression, those receiving concomitant drugs that produce bone marrow suppression, or those with a chronic infection who have received previous or concomitant antibiotic therapy. Discontinuation of therapy with linezolid should be considered in patients who develop or have worsening myelosuppression. Peripheral and optic neuropathies have been reported in patients treated with ZYVOX, primarily in those patients treated for longer than the maximum recommended duration of 28 days. In cases of optic neuropathy that progressed to loss of vision, patients were treated for extended periods beyond the maximum recommended duration. Visual blurring has been reported in some patients treated with ZYVOX for less than 28 days. Peripheral and optic neuropathy has also been reported in children. If patients experience symptoms of visual impairment, such as changes in visual acuity, changes in color vision, blurred vision, or visual field defect, prompt ophthalmic evaluation is recommended. Visual function should be monitored in all patients taking ZYVOX for extended periods (≥ 3 months) and in all patients reporting new visual symptoms regardless of length of therapy with ZYVOX. If peripheral or optic neuropathy occurs, the continued use of ZYVOX in these patients should be weighed against the potential risks. Spontaneous reports of serotonin syndrome including fatal cases associated with the co-administration of ZYVOX and serotonergic agents, including antidepressants such as selective serotonin reuptake inhibitors (SSRIs), have been reported. Unless clinically appropriate and patients are carefully observed for signs and/or symptoms of serotonin syndrome or neuroleptic malignant syndrome-like (NMS-like) reactions, linezolid should not be administered to patients with carcinoid syndrome and/or patients taking any of the following medications: serotonin re-uptake inhibitors, tricyclic antidepressants, serotonin 5-HT1 receptor agonists (triptans), meperidine, bupropion, or buspirone. In some cases, a patient already receiving a serotonergic antidepressant or buspirone may require urgent treatment with linezolid. If alternatives to linezolid are not available and the potential benefits of linezolid outweigh the risks of serotonin syndrome or NMS-like reactions, the serotonergic antidepressant should be stopped promptly and linezolid administered. The patient should be monitored for two weeks (five weeks if fluoxetine was taken) or until 24 hours after the last dose of linezolid, whichever comes first. Symptoms of serotonin syndrome or NMS-like reactions include hyperthermia, rigidity, myoclonus, autonomic instability, and mental status changes that include extreme agitation progressing to delirium and coma. The patient should also be monitored for discontinuation symptoms of the antidepressant. Mortality Imbalance in an Investigational Study in Patients with Catheter-Related Bloodstream Infections, including those with catheter-site infections. While causality has not been established, this observed imbalance occurred primarily in linezolid-treated patients in whom either Gram-negative pathogens, mixed Gram-negative and Gram-positive pathogens, or no pathogen were identified at baseline, but was not seen in patients with Gram-positive infections only. Linezolid is not approved and should not be used for the treatment of patients with catheter-related bloodstream infections or catheter-site infections. Linezolid has no clinical activity against Gram-negative pathogens and is not indicated for the treatment of Gram-negative infections. It is critical that specific Gram-negative therapy be initiated immediately if a concomitant Gram-negative pathogen is documented or suspected. Clostridium difficile associated diarrhea (CDAD) has been reported with use of nearly all antibacterial agents, including ZYVOX, and may range in severity from mild diarrhea to fatal colitis. Treatment with antibacterial agents alters the normal flora of the colon leading to overgrowth of C. difficile. C. difficile produces toxins A and B which contribute to the development of CDAD. Hypertoxin producing strains of C. difficile cause increased morbidity and mortality, as these infections can be refractory to antimicrobial therapy and may require colectomy. CDAD must be considered in all patients who present with diarrhea following antibiotic use. Careful medical history is necessary since CDAD has been reported to occur over two months after the administration of antibacterial agents. If CDAD is suspected or confirmed, ongoing antibiotic use not directed against C. difficile may need to be discontinued. Appropriate fluid and electrolyte management, protein supplementation, antibiotic treatment of C. difficile, and surgical evaluation should be instituted as clinically indicated. Unless patients are monitored for potential increases in blood pressure, linezolid should not be administered to patients with uncontrolled hypertension, pheochromocytoma, thyrotoxicosis and/or patients taking any of the following types of medications: directly and indirectly acting sympathomimetic agents (e.g., pseudoephedrine), vasopressive agents (e.g., epinephrine, norepinephrine), dopaminergic agents (e.g., dopamine, dobutamine). Lactic acidosis has been reported with the use of ZYVOX. In reported cases, patients experienced repeated episodes of nausea and vomiting. Patients who develop recurrent nausea or vomiting, unexplained acidosis, or a low bicarbonate level while receiving ZYVOX should receive immediate medical evaluation. Convulsions have been reported in patients when treated with linezolid. In some of these cases, a history of seizures or risk factors for seizures was reported. Postmarketing cases of symptomatic hypoglycemia have been reported in patients with diabetes mellitus receiving insulin
or oral hypoglycemic agents when treated with linezolid, a reversible, nonselective MAO inhibitor. Some MAO inhibitors have been associated with hypoglycemic episodes in diabetic patients receiving insulin or hypoglycemic agents. While a causal relationship between linezolid and hypoglycemia has not been established, diabetic patients should be cautioned of potential hypoglycemic reactions when treated with linezolid. If hypoglycemia occurs, a decrease in the dose of insulin or oral hypoglycemic agent, or discontinuation of oral hypoglycemic agent, insulin, or linezolid may be required. Prescribing ZYVOX in the absence of a proven or strongly suspected bacterial infection or a prophylactic indication is unlikely to provide benefit to the patient and increases the risk of the development of drug-resistant bacteria.
ADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice. Adults The safety of ZYVOX formulations was evaluated in 2046 adult patients enrolled in seven Phase 3 comparator-controlled clinical trials, who were treated for up to 28 days. Of the patients treated for uncomplicated skin and skin structure infections (uSSSIs), 25.4% of ZYVOX-treated and 19.6% of comparator-treated patients experienced at least one drug-related adverse event. For all other indications, 20.4% of ZYVOX-treated and 14.3% of comparator-treated patients experienced at least one drug-related adverse event. The incidence (%) of treatment-emergent adverse events occurring in >1% of adult patients in a trial involving the treatment of uSSSIs comparing ZYVOX 400 mg PO q12h (n=548) to clarithromycin 250 mg PO q12h (n=537) were headache 8.8 and 8.4; diarrhea 8.2 and 6.1; nausea 5.1 and 4.5; vomiting 2.0 and 1.5; dizziness 2.6 and 3.0; rash 1.1 and 1.1; anemia 0.4 and 0; taste alteration 1.8 and 2.0; vaginal moniliasis 1.8 and 1.3; oral moniliasis 0.5 and 0; abnormal liver function tests 0.4 and 0.2; fungal infection 1.5 and 0.2; tongue discoloration 1.3 and 0; localized abdominal pain 1.3 and 0.6; and generalized abdominal pain 0.9 and 0.4, respectively. The incidence (%) of treatment-emergent adverse events occurring in >1% of adult patients in all other indications of ZYVOX 600 mg q12h (n=1498) versus all other comparators§ (n=1464) were headache 5.7 and 4.4; diarrhea 8.3 and 6.4; nausea 6.6 and 4.6; vomiting 4.3 and 2.3; dizziness 1.8 and 1.5; rash 2.3 and 2.6; anemia 2.1 and 1.4; taste alteration 1.0 and 0.3; vaginal moniliasis 1.1 and 0.5; oral moniliasis 1.7 and 1.0; abnormal liver function tests 1.6 and 0.8; fungal infection 0.3 and 0.2; tongue discoloration 0.3 and 0; localized abdominal pain 1.2 and 0.8; and generalized abdominal pain 1.2 and 1.0, respectively. Of the patients treated for uSSSIs, 3.5% of ZYVOX-treated and 2.4% of comparator-treated patients discontinued treatment due to drug-related adverse events. For all other indications, discontinuations due to drug-related adverse events occurred in 2.1% of ZYVOX-treated and 1.7% of comparator-treated patients. The most common reported drug-related adverse events leading to discontinuation of treatment were nausea, headache, diarrhea, and vomiting. Pediatric Patients The safety of ZYVOX formulations was evaluated in 215 pediatric patients ranging in age from birth through 11 years, and in 248 pediatric patients aged 5 through 17 years (146 of these 248 were age 5 through 11 and 102 were age 12 to 17). These patients were enrolled in two Phase 3 comparator-controlled clinical trials and were treated for up to 28 days. In the study of hospitalized pediatric patients (birth through 11 years) with Gram-positive infections, who were randomized 2 to 1 (linezolid:vancomycin), mortality was 6.0% (13/215) in the linezolid arm and 3.0% (3/101) in the vancomycin arm. However, given the severe underlying illness in the patient population, no causality could be established. Of the pediatric patients treated for uSSSIs, 19.2% of ZYVOX-treated and 14.1% of comparator-treated patients experienced at least one drug-related adverse event. For all other indications, 18.8% of ZYVOX-treated and 34.3% of comparator-treated patients experienced at least one drug-related adverse event. The incidence (%) of treatment-emergent adverse events occurring in >1% of pediatric patients treated for uSSSIs|| with either ZYVOX (n=248) or cefadroxil (n=251) were diarrhea 7.8 and 8.0; vomiting 2.9 and 6.4; headache 6.5 and 4.0; anemia 0 and 0; thrombocytopenia 0 and 0; nausea 3.7 and 3.2; generalized abdominal pain 2.4 and 2.8; localized abdominal pain 2.4 and 2.8; loose stools 1.6 and 0.8; eosinophilia 0.4 and 0.8; pruritus at non-application site 0.8 and 0.4; and vertigo 1.2 and 0.4, respectively. The incidence (%) of treatment-emergent adverse events occurring in >1% of pediatric patients treated for all other indications¶ with either ZYVOX (n=215) or vancomycin (n=101) were diarrhea 10.8 and 12.1; vomiting 9.4 and 9.1; headache 0.9 and 0; anemia 5.6 and 7.1; thrombocytopenia 4.7 and 2.0; nausea 1.9 and 0; generalized abdominal pain 0.9 and 2.0; localized abdominal pain 0.5 and 1.0; loose stools 2.3 and 3.0; eosinophilia 1.9 and 1.0; pruritus at non-application site 1.4 and 2.0; and vertigo 0 and 0, respectively. Of the pediatric patients treated for uSSSIs, 1.6% of ZYVOX-treated and 2.4% of comparator-treated patients discontinued treatment due to drug-related adverse events. For all other indications, discontinuations due to drug-related adverse events occurred in 0.9% of ZYVOX-treated and 6.1% of comparator-treated patients. Laboratory Abnormalities ZYVOX has been associated with thrombocytopenia when used in doses up to and including 600 mg every 12 hours for up to 28 days. In Phase 3 comparator-controlled trials, the percentage of adult patients who developed a substantially low platelet count (defined as less than 75% of lower limit of normal and/or baseline) was 2.4% (range among studies: 0.3 to 10.0%) with ZYVOX and 1.5% (range among studies: 0.4 to 7.0%) with a comparator. In a study of hospitalized pediatric patients ranging in age from birth through 11 years, the percentage of patients who developed a substantially low platelet count (defined as less than 75% of lower limit of normal and/or baseline) was 12.9% with ZYVOX and 13.4% with vancomycin. In an outpatient study of pediatric patients aged from 5 through 17 years, the percentage of patients who developed a substantially low platelet count was 0% with ZYVOX and 0.4% with cefadroxil. Thrombocytopenia associated with the use of ZYVOX appears to be dependent on duration of therapy (generally greater than 2 weeks of treatment). The platelet counts for most patients returned to the normal range/baseline during the follow-up period. No related clinical adverse events were identified in Phase 3 clinical trials in patients developing thrombocytopenia. Bleeding events were identified in thrombocytopenic patients in a compassionate use program for ZYVOX; the role of linezolid in these events cannot be determined [see Warnings and Precautions]. Changes seen in other laboratory parameters, without regard to drug relationship, revealed no substantial differences between ZYVOX and the comparators. These changes were generally not clinically significant, did not lead to discontinuation of therapy, and were reversible. The percent of adult patients with at least one substantially abnormal hematologic** value in patients treated with ZYVOX 400 mg q12h or clarithromycin 250 mg q12h for uncomplicated skin and skin structure infections were as follows: hemoglobin (g/dL) 0.9 and 0.0; platelet count (x 103/mm3) 0.7 and 0.8; WBC (x 103/mm3) 0.2 and 0.6; neutrophils (x 103/mm3) 0.0 and 0.2 respectively. The percent of adult patients with at least one substantially abnormal hematologic** value in patients treated with ZYVOX 600 mg q12h or a comparator§ were as follows: hemoglobin (g/dL) 7.1 and 6.6; platelet count (x 103/mm3) 3.0 and 1.8; WBC (x 103/mm3) 2.2 and 1.3 and neutrophils (x 103/mm3) 1.1 and 1.2 respectively. The percent of adult patients with at least one substantially abnormal serum chemistry†† value in patients treated with ZYVOX 400 mg q12h or clarithromycin 250 mg q12h for uncomplicated skin and skin structure infections were as follows: AST (U/L) 1.7 and 1.3; ALT (U/L) 1.7 and 1.7; LDH (U/L) 0.2 and 0.2; alkaline phosphatase (U/L) 0.2 and 0.2; lipase (U/L) 2.8 and 2.6; amylase (U/L) 0.2 and 0.2; total bilirubin (mg/dL) 0.2 and 0.0; BUN (mg/dL) 0.2 and 0.0; and creatinine (mg/dL) 0.2 and 0.0 respectively. The percent of adult patients with at least one substantially abnormal serum chemistry†† value in patients treated with ZYVOX 600 mg q12h or a comparator§ were as follows: AST (U/L) 5.0 and 6.8; ALT (U/L) 9.6 and 9.3; LDH (U/L) 1.8 and 1.5; alkaline phosphatase (U/L) 3.5 and 3.1; lipase (U/L) 4.3 and 4.2; amylase (U/L) 2.4 and 2.0; total
ZYVX14CDNY3118_ZYVOXassist_JA_Asize_PI_Update_BS_r21.indd 1 4/16/14 12:04 PM
bilirubin (mg/dL) 0.9 and 1.1; BUN (mg/dL) 2.1 and 1.5; and creatinine (mg/dL) 0.2 and 0.6 respectively. The percent of pediatric patients with at least one substantially abnormal hematologic‡‡ value in patients treated with ZYVOX or cefadroxil for uncomplicated skin and skin structure infections|| were as follows: hemoglobin (g/dL) 0.0 and 0.0; platelet count (x 103/mm3) 0.0 and 0.4; WBC (x 103/mm3) 0.8 and 0.8; neutrophils (x 103/mm3) 1.2 and 0.8 respectively. The percent of pediatric patients with at least one substantially abnormal hematologic‡‡ value in patients treated with ZYVOX or vancomycin for any other indication¶ were as follows: hemoglobin (g/dL) 15.7 and 12.4; platelet count (x 103/mm3) 12.9 and 13.4; WBC (x 103/mm3) 12.4 and 10.3 and neutrophils (x 103/mm3) 5.9 and 4.3 respectively. The percent of pediatric patients with at least one substantially abnormal serum chemistrya value in patients treated with ZYVOX or cefadroxil for uncomplicated skin and skin structure infections|| were as follows: ALT (U/L) 0.0 and 0.0; lipase (U/L) 0.4 and 1.2; and creatinine (mg/dL) 0.4 and 0.0 respectively. The percent of pediatric patients with at least one substantially abnormal serum chemistrya value in patients treated with ZYVOX or vancomycin for any other indication¶ were as follows: ALT (U/L) 10.1 and 12.5; amylase (U/L) 0.6 and 1.3; total bilirubin (mg/dL) 6.3 and 5.2; and creatinine (mg/dL) 2.4 and 1.0 respectively. Postmarketing Experience The following adverse reactions have been identified during postapproval use of ZYVOX. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure. Myelosuppression (including anemia, leukopenia, pancytopenia, and thrombocytopenia) has been reported during postmarketing use of ZYVOX [see Warnings and Precautions]. Peripheral neuropathy, and optic neuropathy sometimes progressing to loss of vision, have been reported in patients treated with ZYVOX. Lactic acidosis has been reported with the use of ZYVOX [see Warnings and Precautions]. Although these reports have primarily been in patients treated for longer than the maximum recommended duration of 28 days, these events have also been reported in patients receiving shorter courses of therapy. Serotonin syndrome has been reported in patients receiving concomitant serotonergic agents, including antidepressants such as selective serotonin reuptake inhibitors (SSRIs) and ZYVOX [see Warnings and Precautions]. Convulsions have been reported with the use of ZYVOX [see Warnings and Precautions]. Anaphylaxis, angioedema, and bullous skin disorders such as those described as Stevens-Johnson syndrome have been reported. Superficial tooth discoloration and tongue discoloration have been reported with the use of linezolid. The tooth discoloration was removable with professional dental cleaning (manual descaling) in cases with known outcome. Hypoglycemia, including symptomatic episodes, has been reported [see Warnings and Precautions].
DRUG INTERACTIONS Monoamine Oxidase Inhibitors Linezolid is a reversible, nonselective inhibitor of monoamine oxidase. Adrenergic and Serotonergic Agents Linezolid has the potential for interaction with adrenergic and serotonergic agents.
USE IN SPECIFIC POPULATIONS Pregnancy Teratogenic Effects – Pregnancy Category C Linezolid was not teratogenic in mice, rats, or rabbits at exposure levels 6.5-fold (in mice), equivalent to (in rats), or 0.06-fold (in rabbits) the expected human exposure level, based on AUCs. However, embryo and fetal toxicities were seen (see Non-teratogenic Effects). There are no adequate and well-controlled studies in pregnant women. ZYVOX should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Non-teratogenic Effects In mice, embryo and fetal toxicities were seen only at doses that caused maternal toxicity (clinical signs and reduced body weight gain). A dose of 450 mg/kg/day (6.5-fold the estimated human exposure level based on AUCs) correlated with increased postimplantational embryo death, including total litter loss, decreased fetal body weights, and an increased incidence of costal cartilage fusion. In rats, mild fetal toxicity was observed at 15 and 50 mg/kg/day (exposure levels 0.22-fold to approximately equivalent to the estimated human exposure, respectively, based on AUCs). The effects consisted of decreased fetal body weights and reduced ossification of sternebrae, a finding often seen in association with decreased fetal body weights. Slight maternal toxicity, in the form of reduced body weight gain, was seen at 50 mg/kg/day. In rabbits, reduced fetal body weight occurred only in the presence of maternal toxicity (clinical signs, reduced body weight gain and food consumption) when administered at a dose of 15 mg/kg/day (0.06-fold the estimated human exposure based on AUCs). When female rats were treated with 50 mg/kg/day (approximately equivalent to the estimated human exposure based on AUCs) of linezolid during pregnancy and lactation, survival of pups was decreased on postnatal days 1 to 4. Male and female pups permitted to mature to reproductive age, when mated, showed an increase in preimplantation loss. Nursing Mothers Linezolid and its metabolites are excreted in the milk of lactating rats. Concentrations in milk were similar to those in maternal plasma. It is not known whether linezolid is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when ZYVOX is administered to a nursing woman. Pediatric Use The safety and effectiveness of ZYVOX for the treatment of pediatric patients with the following infections are supported by evidence from adequate and well-controlled studies in adults, pharmacokinetic data in pediatric patients, and additional data from a comparator-controlled study of Gram-positive infections in pediatric patients ranging in age from birth through 11 years [see Indications and Usage]: nosocomial pneumonia, complicated skin and skin structure infections, community-acquired pneumonia (also supported by evidence from an uncontrolled study in patients ranging in age from 8 months through 12 years), vancomycin-resistant Enterococcus faecium infections. The safety and effectiveness of ZYVOX for the treatment of pediatric patients with the following infection have been established in a comparator-controlled study in pediatric patients ranging in age from 5 through 17 years: uncomplicated skin and skin structure infections caused by Staphylococcus aureus (methicillin-susceptible strains only) or Streptococcus pyogenes. Pharmacokinetic information generated in pediatric patients with ventriculoperitoneal shunts showed variable cerebrospinal fluid (CSF) linezolid concentrations following single and multiple dosing of linezolid; therapeutic concentrations were not consistently achieved or maintained in the CSF. Therefore, the use of linezolid for the empiric treatment of pediatric patients with central nervous system infections is not recommended. The pharmacokinetics of linezolid have been evaluated in pediatric patients from birth to 17 years of age. In general, weight-based clearance of linezolid gradually decreases with increasing age of pediatric patients. However, in preterm (gestational age < 34 weeks) neonates < 7 days of age, linezolid clearance is often lower than in full-term neonates < 7 days of age. Consequently, preterm neonates < 7 days of age may need an alternative linezolid dosing regimen of 10 mg/kg every 12 hours. In limited clinical experience, 5 out of 6 (83%) pediatric patients with infections due to Gram-positive pathogens with minimum inhibitory concentrations (MICs) of 4 mcg/mL treated with ZYVOX had clinical cures. However, pediatric patients exhibit wider variability in linezolid clearance and systemic exposure (AUC) compared with adults. In pediatric patients with a sub-optimal clinical response, particularly those with pathogens with MIC of 4 mcg/mL, lower systemic exposure, site and severity of infection, and the underlying medical condition should be considered when assessing clinical response. Geriatric Use Of the 2046 patients treated with ZYVOX in Phase 3 comparator-controlled clinical trials, 589 (29%) were 65 years or older and 253 (12%) were 75 years or older. No overall differences in safety or effectiveness were observed between these patients and younger patients, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
OVERDOSAGE In the event of overdosage, supportive care is advised, with maintenance of glomerular filtration. Hemodialysis may facilitate more rapid elimination of linezolid. In a Phase 1 clinical trial, approximately 30% of a dose of linezolid was removed during a 3-hour hemodialysis session beginning 3 hours after the dose of linezolid was administered. Data are not available for removal of linezolid with peritoneal dialysis or hemoperfusion. Clinical signs of acute toxicity in animals were decreased activity and ataxia in rats and vomiting and tremors in dogs treated with 3000 mg/kg/day and 2000 mg/kg/day, respectively.
PATIENT COUNSELING INFORMATION Patients should be counseled that antibacterial drugs including ZYVOX should only be used to treat bacterial infections. They do not treat viral infections (e.g., the common cold). When ZYVOX is prescribed to treat a bacterial infection, patients should be told that although it is common to feel better early in the course of therapy, the medication should be taken exactly as directed. Skipping doses or not completing the full course of therapy may (1) decrease the effectiveness of the immediate treatment and (2) increase the likelihood that bacteria will develop resistance and will not be treatable by ZYVOX or other antibacterial drugs in the future. Patients should be advised that: ZYVOX may be taken with or without food. They should inform their physician if they have a history of hypertension. Large quantities of foods or beverages with high tyramine content should be avoided while taking ZYVOX. Foods high in tyramine content include those that may have undergone protein changes by aging, fermentation, pickling, or smoking to improve flavor, such as aged cheeses, fermented or air-dried meats, sauerkraut, soy sauce, tap beers, and red wines. The tyramine content of any protein-rich food may be increased if stored for long periods or improperly refrigerated. They should inform their physician if taking medications containing pseudoephedrine HCl or phenylpropanolamine HCl, such as cold remedies and decongestants. They should inform their physician if taking serotonin re-uptake inhibitors or other antidepressants. Phenylketonurics: Each 5 mL of the 100 mg/5 mL ZYVOX for Oral Suspension contains 20 mg phenylalanine. The other ZYVOX formulations do not contain phenylalanine. Contact your physician or pharmacist. They should inform their physician if they experience changes in vision. They should inform their physician if they have a history of seizures. Diarrhea is a common problem caused by antibiotics, which usually ends when the antibiotic is discontinued. Sometimes after starting treatment with antibiotics, patients can develop watery and bloody stools (with or without stomach cramps and fever) even as late as two or more months after having taken the last dose of the antibiotic. If this occurs, patients should contact their physician as soon as possible. Inform patient, particularly those with diabetes mellitus that hypoglycemic reactions, such as diaphoresis and tremulousness, along with low blood glucose measurements may occur when treated with linezolid. If such reactions occur, patients should contact a physician or other health professional for proper treatment. § Comparators included cefpodoxime proxetil 200 mg PO q12h; ceftriaxone 1 g IV q12h;
dicloxacillin 500 mg PO q6h; oxacillin 2 g IV q6h; vancomycin 1 g IV q12h. || Patients 5 through 11 years of age received ZYVOX 10 mg/kg PO q12h or cefadroxil
15 mg/kg PO q12h. Patients 12 years or older received ZYVOX 600 mg PO q12h or cefadroxil 500 mg PO q12h.
¶ Patients from birth through 11 years of age received ZYVOX 10 mg/kg IV/PO q8h or vancomycin 10 to 15 mg/kg IV q6-24h, depending on age and renal clearance.
** <75% (<50% for neutrophils) of Lower Limit of Normal (LLN) for values normal at baseline; <75% (<50% for neutrophils) of LLN and of baseline for values abnormal at baseline.
†† >2 x Upper Limit of Normal (ULN) for values normal at baseline; >2 x ULN and >2 x baseline for values abnormal at baseline.
‡‡ <75% (<50% for neutrophils) of Lower Limit of Normal (LLN) for values normal at baseline; <75% (<50% for neutrophils) of LLN and <75% (<50% for neutrophils, <90% for hemoglobin if baseline <LLN) of baseline for values abnormal at baseline.
a >2 x Upper Limit of Normal (ULN) for values normal at baseline; >2 x ULN and >2 (>1.5 for total bilirubin) x baseline for values abnormal at baseline.
Rx only Rev. January 2014
ZYVX14CDNY3118_ZYVOXassist_JA_Asize_PI_Update_BS_r21.indd 2 4/16/14 12:04 PM
SEPT/OCT 2014
12
Progression of Care Innovations: Employment of Video Debriefing, Scripting, and Scoring to Improve Quality of Multidisciplinary RoundsMegan Olman, LCSW, ACMTHIS AUTHOR HAS NO FINANCIAL RELATIONSHIPS WITH COMMERCIAL INTERESTS TO DISCLOSE.
LEARNING OBJECTIVES1. Identify strategies to enable staff to
engage in “self reflection” (“hansei”) through video debriefing.
2. Employ specific process improvements to effect change in patient flow/throughput.
3. Identify key elements to successful progression of care.This project was developed to reinforce
and focus on pertinent patient information that would lead to a more comprehensive plan of care for the patient, more productive and timely rounds, and increased staff satisfaction.
Multidisciplinary rounding involves all of the care partners coming together to actively discuss the patient, identify needs, and attempt
to expedite the patient’s healing. Groups proactively assess patients’ complete well-being and call in consults or referrals as needed. These groups generally involve a case manager, nurse manager, bedside nurse, and social worker, but can include others depending on the team. On seven units at Cedars-Sinai, the teams are led by a physician advisor.
As part of the nursing care delivered at Cedars-Sinai, nurses always participated in progression of care rounds. During these rounds, the nurses discussed the plan of care. However, over time, multidisciplinary rounds had become more of a discussion of tasks that needed to be performed for the patient than a discussion of the patient’s improvement and progression toward improved health and discharge.
Multidisciplinary roundings can be an efficient and effective method of addressing patients’ needs and coordinating services among hospital professionals. However, when performed ineffectively, rounds can waste time and effort while contributing to lengthy stays and miscommunications. At Cedars-Sinai Medical Center in Los Angeles, California, a new model has been implemented to examine the strengths and challenges of multidisciplinary rounding and improve upon the current system the hospital is utilizing. This article will discuss the circumstances that led to the development of this intervention and present early results from changes made to hospital unit rounds.

COLLABORATIVE CASE MANAGEMENT | ACMAWEB.ORG
13
Team members described the existing rounds system as “Groundhog Day.” Much would be communicated throughout the day about patients’ health and readiness to be discharged or transferred, but by the next morning, a miscommunication or an issue initiated by the patient had prevented or complicated the necessary action. In general, there was incorrect information communicated during handoffs, critical developments were not reported as needed, and plans were not followed through.
Meanwhile, the team wanted to improve patients’ average length of stay and focus on being proactive with patient care. When discharge delays occurred due to orders or services like physical therapy or medications, the team wanted to take action and see if those could be followed through earlier. A theory emerged that strengthening progression of care conversations would lead to better communication, quicker follow-through, and ultimately better, more efficient patient care.
THE PLAN
The team implemented a Plan-Do-Study-Act (PDSA) cycle for qualitative improvement of multidisciplinary progression of care rounds. The “plan” phase involved scoring and sharing key processes among team members. The “do” phase included video debriefing of rounds, and the “study” phase examined those videos for best practices and areas for improvement. And in the “act” phase, key interventions were chosen and undertaken – based on information learned in the video debriefing process – to enhance quality, speed, and outcomes of rounds.
The team was looking for a new and innovative approach to solving their problem, and they eventually settled on video debriefing. The tool, which involved rounds being recorded in action and then played back for participants later, had been used extensively in emergency medicine. It is standard operating procedure in many emergency rooms, where treatment happens quickly and urgently, without time in the moment for self-reflection. The idea was to take that tool and apply it to an entirely different area of the hospital.
Leadership was advised to maintain current processes and to allow frontline staff to debrief prior to leadership participation. Viewing the tapes provided an opportunity for quick feedback and recognition of verbal and
nonverbal miscommunications. The team found the video recordings very interesting, and viewing the recordings helped inform changes to their practice.
For example, rounds may be held promptly at 10:15 each day at the nurse’s station. Team members receive a text at 9:50 reminding them of the meeting, and everyone arrives ready to provide reports on their patients. Test results and charts are available and can be quickly referred to when needed.
The following criteria are used to keep rounds efficient; these functional best practices do not mandate a one-size-fits-all approach to rounds.
• Use a checklist focused on the plan for each patient’s day/stay.
• Display the checklist as a prompt during rounds.
• Encourage one-rounds to avoid handoff errors. For instance, in one Cedars- Sinai unit, rounds are now held once each morning.
• Have a “batter on deck” to reduce any wasted time. All nurses and staff members report to rounds at the same time, in the same place, with all ready to report on their patients one right after another.
• Have electronic health record open during rounds.
• Have clearly identified leadership of rounds. At Cedars-Sinai, one designated team member generally takes the lead and manages each session.
• Develop an action plan at the unit level following rounds.
• Hand off action plan to night shift leader. A second set of rounds is not done, but the night nurse is made aware of the plan and is responsible for seeing it through.
• Allow staff to set their own goals.• Encourage engagement.• Choose optimal rounds location.The rounds were streamlined throughout
the hospital by using hangtags (See Figure A.), which contained valuable information and were attached to the backs of staff name badges. There are some differences in the script that are necessary and innate on different floors among different patient populations, but there are some universal elements in every progression of care discussion. The use of hangtags highlighted those, so that floating nurses could easily reference them and see what needed to be part of that patient’s progression of care conversation.
These questions utilized a Situation, Background, Assessment, Recommendation (SBAR) format. For Cedars’ 3SCCT (3 Saperstein Critical Care Tower) unit, the script included the following questions:1. What is the patient’s last name and
individual service plan?2. Is the patient a direct admit, from
the emergency department, or an in-house transfer?
3. Is the patient an inpatient or under observation status?
4. What was the patient’s admitting diagnosis? What brought the patient to the hospital?
Figure A.
SEPT/OCT 2014
5. Does the patient have a history of heart failure? Does the patient meet the frailty criteria?
6. Has the depression/suicide risk assessment been completed? Is it positive?
7. What diagnosis are we treating today? Are there any tests or procedures scheduled today?
8. What is the patient’s current functional status? Is this a change from his or her baseline?
9. What is the discharge plan? What needs to happen for the patient to be discharged?
10. When does the attending MD expect the patient to be discharged? What do we need to do to ensure discharge by 11:00 am?
11. Does the bedside nurse have any questions or concerns with the patient’s progression of care?
The goals were to improve scores on the Hospital Consumer Assessment of Healthcare Providers and Systems survey (HCAHPS) and to discharge more patients by 11:00 AM.
One of the initial challenges was gaining buy-in from participants. The success of the initiative relied on changing the day-to-day operations of the hospital staff, encouraging everyone to think about each individual patient, their needs, and their anticipated discharge dates. Not everyone embraced the new system or felt comfortable with it im-mediately. It was a change in thinking for everyone and placed a great deal of additional responsibility on the team members. In progression of care rounds, the team began to identify action items to move the patient toward discharge, and everyone on the team became accountable for those action items. At the end of the day, if an item had not been completed, the team members had to own the reason why. At times, this was uncomfortable.
Nurses are busy but their understanding of why stopping their day for rounds was important. Their buy-in was crucial, since they spend the most time with patients and have great insight into their progress. Fortunately, the nurse manager saw the value in reforming the system and her support carried through to the unit nurses. Now there is significant buy-in from nursing staff at all levels and they are enthusiastic about the new system.
One important change occurred in sharing the anticipated discharge date with patients. Case managers always work to move the patient toward discharge, but discharge dates were not consistently discussed with the patient. In many cases, such discussions would make the patient anxious – if the date felt too soon, too far away, or if the anticipated date went by without release. Now, case managers, physicians, and nurses work together toward identifying anticipated discharge date on admission. This process encourages all members of the health care team to think about tests and the movement of patients along the health care continuum from inpatient to outpatient care.
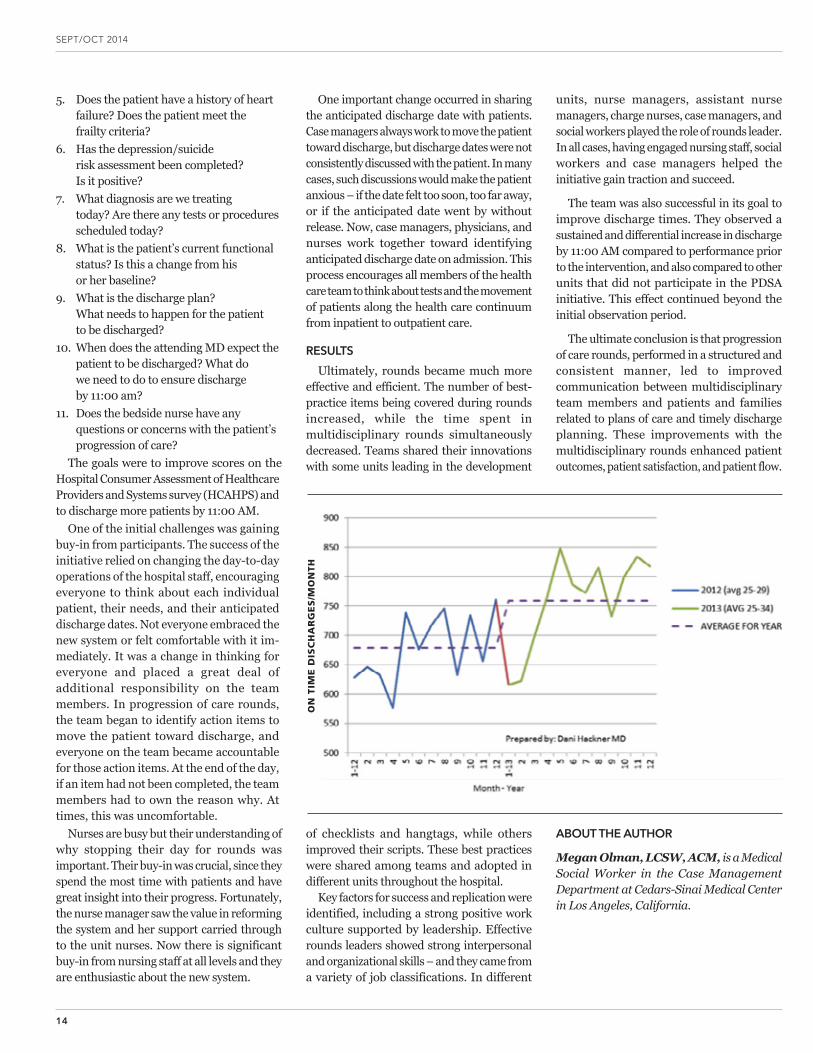
RESULTSUltimately, rounds became much more
effective and efficient. The number of best-practice items being covered during rounds increased, while the time spent in multidisciplinary rounds simultaneously decreased. Teams shared their innovations with some units leading in the development
of checklists and hangtags, while others improved their scripts. These best practices were shared among teams and adopted in different units throughout the hospital.
Key factors for success and replication were identified, including a strong positive work culture supported by leadership. Effective rounds leaders showed strong interpersonal and organizational skills – and they came from a variety of job classifications. In different
units, nurse managers, assistant nurse managers, charge nurses, case managers, and social workers played the role of rounds leader. In all cases, having engaged nursing staff, social workers and case managers helped the initiative gain traction and succeed.
The team was also successful in its goal to improve discharge times. They observed a sustained and differential increase in discharge by 11:00 AM compared to performance prior to the intervention, and also compared to other units that did not participate in the PDSA initiative. This effect continued beyond the initial observation period.
The ultimate conclusion is that progression of care rounds, performed in a structured and consistent manner, led to improved communication between multidisciplinary team members and patients and families related to plans of care and timely discharge planning. These improvements with the multidisciplinary rounds enhanced patient outcomes, patient satisfaction, and patient flow.
ABOUT THE AUTHOR
Megan Olman, LCSW, ACM, is a Medical Social Worker in the Case Management Department at Cedars-Sinai Medical Center in Los Angeles, California.
14
ON
TIM
E D
ISC
HA
RG
ES
/MO
NTH
15
COLLABORATIVE CASE MANAGEMENT | ACMAWEB.ORG
Heart Failure Readmission Cuts May be a Phone Call AwayBruce JancinTHIS AUTHOR HAS NO FINANCIAL RELATIONSHIPS WITH COMMERCIAL INTERESTS TO DISCLOSE.
when Ms. Thompson or another caller asks, “How have you been feeling since discharge?” it provides an opportunity to review the typical symptoms of heart failure and make sure the patient knows how to recognize them.
Other questions review medications and address the patient’s activity level, adherence to the recommended low-sodium diet, and self-weighing at home with tracking of the results. The interviewer also makes sure the patient knows his or her physician’s name, phone number, the date of the next scheduled appointment, and understands the circumstances when it’s important to call the doctor because the clinical picture is beginning to deteriorate, explained Ms. Thompson, who works in the Stanford heart failure program.
The structured telephone follow-up call was merely one element of a whole set of interventions developed by a multidisciplinary Stanford team in an effort to reduce heart failure readmissions. Other interventions included medication reconciliation, routinely scheduling an early postdischarge clinic visit, and an increased emphasis upon patient education using patient “teach back” techniques to promote mastery of key information.
In the first 14 months since the full readmission-reduction program was launched, 96% of patients reached via a postdischarge phone call demonstrated that they understood their discharge medications and how to take them.
It was possible to determine the specific contribution that the early postdischarge phone call made to the observed sharp decrease in 30-day readmissions because 61 patients didn’t get the follow-up phone call but did receive the other interventions. Their 30-day readmission rate was 28%, compared with 10% in those who did get the phone call, which translates to a 66% relative risk reduction. In a multivariate logistic regression analysis adjusted for the other interventions as well as patient age, sex, marital status, length of stay, and discharge destination, the early postdischarge follow-up phone call was independently associated with a 72% reduction in the risk of readmission within 30 days, according to Ms. Thompson.
She reported having no financial conflicts regarding this study.This article reprinted with permission from Hospitalist News Digital Network, October 9, 2014. For more information, visit www.ehospitalistnews.com.
A structured follow-up telephone call to heart failure patients made within 48 hours post discharge can reduce 30-day readmissions by fully one-half to two-thirds.
That’s been the experience at Stanford (Calif.) University Medical Center, where the 30-day heart failure readmission rate dropped from 20% in 524 patients at baseline to 10% among 341 patients discharged since the follow-up phone call practice was introduced, clinical nurse specialist Christine Thompson reported at the annual meeting of the Heart Failure Society of America.
LEARNING OBJECTIVES
1. Discuss the results of the study or educational presentation addressed in these articles which focus on topics of high clinical interest for the primary care physician.
2. Review the clinical relevance and practice implications of the information presented.
The telephone call follows a scripted template embedded in the patient’s electronic health record. The template incorporates “smart text” questions that assist in identifying gaps in patient care. For example,
16
COLLABORATIVE CASE MANAGEMENT | ACMAWEB.ORG
Read Collaborative Case Management, Earn CEsFree continuing education credits are available to ACMA’s nurse and
social worker members who read the publication and complete the associated online quizzes with a passing score of 80%. To obtain continuing education credits, members must:• Read Collaborative Case Management• Successfully complete and submit the associated online
quiz located in the Members Only section of the ACMA website. To login, go to www.acmaweb.org/login
• A certificate will be available for print and download upon successful completion of the quiz
• Each issue’s continuing education opportunity expires after one year (365 days)
CE DETAILS
This activity meets the qualifications for 1.0 hour of continuing education credit for MFTs, LPCCs, LEPs, and/or LCSWs as required
by the California Board of Behavioral Sciences (CEP #4591). ACMA is a provider approved by the California Board of Registered Nursing (Provider Number CEP #15413) for 1.2 contact hours (1.0 CE in 60-minute states).
ACMA is also a provider approved by the Florida Board of Nursing for 1.2 nursing contact hours (based on 50-minute hour) and 1.0 nursing contact hour (based on 60-minute hour); and the Florida Board of Clinical Social Work, Marriage and Family Therapy and Mental Health Counseling for 1.0 hour of continuing education credit – CE Broker Course Tracking #20-430708.
ACMA is also a recognized CE provider for nursing and social work in multiple other states. Readers are responsible for verifying requirements of the applicable licensing board in their state.
Continuing education credits are approved toward ACM™ Certification renewal.
22nd Annual Case Management Conference & 16th Annual ACMA Meeting
April 26-29, 2015Phoenix Convention Center • Phoenix, AZ
www.casemanagementconference.com
In Honor of:MONICA, DIANA, ELENA, AND SUE NURSE NAVIGATORS INOVA MEDICAL Nancy Loeffler Reston, VAIn Honor of:UPMC ST. MARGARET CARE MANAGEMENT DEPARTMENT Marjorie Jacobs Upmc St. Margaret Pittsburgh, PA
In Honor of:WHITE MEMORIAL MEDICAL CENTER’S CARE MANAGEMENT DEPARTMENT Lynne Whaley White Memorial Medical Center Los Angeles, CA In Honor of:THE CARE MANAGEMENT DEPARTMENT Care Management Department Leadership Stony Brook University HospitalStony Brook, NY
In Honor of:FOUNDING ACMA NATIONAL BOARD MEMBERS: GREG, MARTHA, SHARON, DONNA, EVELYN, MARCIA & JEANINE Devi Desai Chapel Hill, NC
During National Case Management Week (NCMW), many of you honored or remembered those
who have impacted you personally in your career in health care, as well as the patients, families and other
members of the health care community with whom you come in contact. Directors, staff, departments,
chapters, hospitals/health care delivery systems, friends, colleagues, mentors, and many more - all have
been honored in this list.
ACMA thanks those who made donations in honor or memory of those who mean the most.
Below is a list of those recognized by their colleagues in case management:
Platinum Donations
In Honor of:HEALTHSOUTH MOUNTAINVIEW CASE MANAGEMENT DEPARTMENT STAFF Christy WhetsellMorgantown, WV
In Honor of:SPARTANBURG REGIONAL HEALTHCARE SYSTEM CASE MANAGEMENTAngie RobersonSpartanburg Regional Healthcare SystemSpartanburg, SC
In Honor of:THE ACMA NATIONAL WONDERFUL STAFFSharon Mass-AchsLos Angeles, CA
In Honor of:ILLINOIS CHAPTER MEMBERS, SUPPORTERS, COMMITTEES AND BOARDDiana DoeppManhattan, IL
In Honor of:ACMA NATIONAL FUNDRAISING COMMITTEE North Little Rock, AR
Recognizing those who mean the most…S U P P O R T I N G C A S E M A N A G E M E N T P R A C T I C E
11701 West 36th Street • Little Rock, AR 72211 • (501) 907-2262 • www.acmaweb.org
Bronze DonationsSilver Donations
Gold Donations
Directional Training for Case Managers
ACMA Compare Benchmarkingwww.ACMACompare.com
POST YOUR CASE MANAGEMENT POSITION WITH ACMA
Developed by an interdisciplinary taskforce of case management leaders, Compass is a comprehensive program designed to provide training for new case management staff and to serve as a refresher for existing staff.
n ONLINE TRAINING VIDEOS
n ONLINE COMPETENCY TESTS
n HARDCOPY MANUAL COMPANION
n AVAILABLE 24 HOURS A DAY, SEVEN DAYS A WEEK
For more information, visit: www.acmaweb.org/compass
www.acmaweb.org/careers

11701 West 36th Street • Little Rock, AR 72211
NON PROFIT STD
U.S. POSTAGE
PAIDLITTLE ROCK, AR
PERMIT #451
RETURN SERVICE REQUESTED
INNOVATIVE EDUCATION FOR CASE MANAGEMENT LEADERS AND PHYSICIAN ADVISORS
2014 LEADERSHIP CONFERENCE AND MEDICAL DIRECTOR FORUM
November 19-22, 2014 | Orlando, Florida
WWW.ACMAWEB.ORG/LEADERSHIP





























