Embed Size (px)
Citation preview

DOI 10.1515/jpem-2013-0145 J Pediatr Endocr Met 2013; 26(11-12): 1111–1121
Qiuling Zhaoa, Zhixin Zhanga,*, Sheng Xie, Hui Pan, Jiaying Zhang, Gaolang Gong and Zaixu Cui
Cognitive impairment and gray/white matter volume abnormalities in pediatric patients with Turner syndrome presenting with various karyotypes
Abstract
Aim: To investigate the association between cognitive impairment and gray/white matter volume abnormalities in pediatric patients with Turner syndrome (TS) presenting with various karyotypes.Methods: In the present study, 21 pediatric patients with TS and the 45,X karyotype, 24 pediatric patients with TS and other karyotypes, and 20 normal healthy controls, underwent the Wechsler intelligence test, behavioral testing, and a 3.0T magnetic resonance (MR) scan. Wholebrain highresolution T1weighted images were processed with SPM8 software and analyzed using voxelbased morphometry (VBM); differences in gray/white matter volume between the TS groups and healthy controls were compared using analysis of covariance.Results: Pediatric patients in both TS groups had significantly lower IQ scores compared to the normal controls (p < 0.05). Furthermore, both TS groups scored significantly less than the normal controls in various composite tests of cognitive function, including verbal comprehension, perceptual reasoning, working memory, and processing speed (p < 0.05). There were no significant differences between the two TS patient groups in terms of their scores for verbal comprehension, perceptual reasoning, working memory, and processing speed. However, they did display significant differences in the following tests: accuracy and reaction times in the executive control test, reaction times in the short, middle, and longterm attention test, and accuracy in the longterm attention test. Patients in the 45,X karyotype group displayed decreased gray matter volume in the bilateral cuneus, calcarine sulcus postcentral gyrus, right precuneus, superior parietal lobule, lingual gyrus, left precentral gyrus, and cingulate gyrus. However, gray matter volume was increased in the bilateral dorsal midbrain, orbital frontal gyrus, left insular lobe, superior temporal gyrus, inferior temporal gyrus, parahippocampal gyrus, cerebellum, posterior insular lobe, right
caudate nucleus, putamen, and temporal pole. Patients with TS with other karyotypes exhibited decreased gray matter volume in the left precuneus, cingulate gyrus, right postcentral gyrus, supramarginal gyrus, angular gyrus, and cuneus; contrastingly, gray matter volume increased in both the epencephals, left caudate nucleus, superior temporal gyrus, right insular lobe, and temporal pole. All volume differences were statistically significant when compared with normal controls [familywise error (FWE)corrected p < 0.05]. With regard to the two TS groups, gray matter volume in the left hippocampus and left caudate nucleus was significantly decreased in the 45,X karyotype group compared to patients with TS with other karyotypes (FWEcorrected p < 0.05); conversely, gray matter volume in the right supramarginal gyrus was increased in the 45,X karyotype group (FWEcorrected p < 0.05).Conclusion: Pediatric patients with TS display a lower level of intelligence compared to healthy controls, this is complicated by verbal and nonverbal cognitive impairment. The neuropathological basis of such cognitive deficiencies may be as a result of abnormalities in gray matter development.
Keywords: behavioral test; magnetic resonance imaging; Turner syndrome; Wechsler intelligence test.
aQiuling Zhao and Zhixin Zhang contributed equally this article.*Corresponding author: Zhixin Zhang, Department of Pediatrics, China-Japan Friendship Hospital, Beijing, China, Phone: +86-13701371501, E-mail: [email protected] Zhao: Department of Pediatrics, China-Japan Friendship Hospital, Beijing, ChinaSheng Xie: Department of Radiology, China-Japan Friendship Hospital, Beijing, ChinaHui Pan: Department of Endocrinology, Peking Union Medical College Hospital, Beijing, ChinaJiaying Zhang, Gaolang Gong and Zaixu Cui: State Key Laboratory of Cognitive Neuroscience and Learning, Beijing Normal University, Beijing, China
Brought to you by | University of California - San FranciscoAuthenticated
Download Date | 2/17/15 8:38 PM

1112 Zhao et al.: Cognitive impairment in pediatric patients with Turner syndrome
IntroductionTurner syndrome (TS), also known as congenital ovarian hypoplasia, is the only monosomy that is not always lethal in humans. It is caused by complete or partial absence of one X chromosome in somatic cells. TS presents in approximately 1/2000–1/2500 live female births (1). The most common clinical manifestations of TS include somatic abnormalities, short stature, and gonadal hypoplasia. Many pediatric patients with TS are clinically diagnosed with neuropsychiatric delayed puberty and cognitive deficits, including topographical disorientation, spatial learning impairment, and calculation impairment (2). As such discoveries continue to rise, research into the developmental and functional brain abnormalities associated with TS has received much attention in recent years. For example, Holzapfel et al. reported that visualspatial dysfunction observed in patients with TS is mainly associated with abnormal microstructures in the gray matter of the frontal occipitoparietal lobe and the white matter of the temporal lobe, as well as morphological abnormalities in the parietal gyrus (3). Lee et al. reported a case of complicated agenesis of the corpus callosum in a 32yearold patient with TS with the 45,X karyotype (4). Furthermore, Longman et al. revealed the presence of abnormal neural connectivity following the autopsy of a sudden death case of TS presenting with ringchromosome karyotype (5). In a previous study conducted by Bray et al., patients with TS demonstrated superior verbal abilities but poorer working memory (6).
In each of these studies, the authors discovered some slight structural change in the parietal lobe and decreased functional connectivity in the dorsalfrontal areas. Such deficits in functional connectivity may contribute to the performance of patients with TS in various cognitive tests. The results of these studies not only show that patients with TS present with abnormal brain development but also with amygdalainduced disconnection between arousal and cognitive appraisal function (7). However, one of the shortfalls of these studies is the broad age range (7–24 years) of patients with TS enrolled (3, 8, 9). Moreover, most of these studies either focus on patients with the 45,X karyotype or conducted neuroimaging scans and cognitive behavioral studies on patients with TS without prior karyotype classification.
Thus, it remains to be clarified whether cognitive/behavioral performance and neuroimaging findings are different in patients with TS with total monosomy compared to those with only partial absence/structural abnormalities of chromosome X. In this study, only pediatric patients with TS, aged between 10 and 18 years,
were enrolled. These were subsequently divided into two groups: the “45,X” karyotype group and the “other” karyotype group. Differences in gray matter volume between pediatric patients with TS with various karyotypes and normal controls were assessed using voxelbased morphometry (VBM) of T1weighted images (T1WIs). Moreover, results obtained from IQ and behavioral tests were also processed. Lastly, clinical data relating to estrogen (E2) and gonadotropinreleasing hormone (FSH) levels were analyzed in the patients with TS in order to investigate a potential association between cognitive impairment, abnormal sex hormone level, and gray matter volume in pediatric patients with TS presenting with different karyotypes.
Methods and materials
Subject eligibilityFortyfive pediatric outpatients with TS, aged 10–18 years, were enrolled in this study. Patients were diagnosed by the Clinical Department of Pediatric Endocrinology at the ChinaJapan Friendship Hospital or at the ShortStature Specialist Consult at Union Hospital between July 2010 and October 2011. The criteria for eligibility included the following: (i) short stature, specifically a height below the 5th or even the 3rd percentile among girls of the same age as well as a decreased growth rate ( < 5 cm/year); (ii) significantly increased serum gonadotropin levels; (iii) retarded bone age; (iv) diagnosis of a karyotype of 45,X or one of its variants; (v) symptoms such as short (webbed) neck, low hairline, shieldshape thorax, widely spaced nipples, cubitus valgus, multiple nevi, lymphedema of the hands and feet in infancy, neck skin laxity, normal intelligence development, disorder of sex development, genital infantilism, and primary amenorrhea.
All pediatric patients enrolled were righthanded female infants with a mean age of 13.90 ± 2.5 years. Of the 45 patients enrolled, 21 were pediatric patients with TS with the 45,X karyotype (mean age of 14.21 ± 2.79 years); 19 of these patients had received growth hormone treatment, while four had been treated with estrogen. Twentyfour pediatric patients with TS with other karyotypes and a mean age of 13.63 ± 2.41 were included in the other karyotype group (see Table 1 for the detailed karyotype information); 20 of these patients had received growth hormone treatment, while two were treated with estrogen. No abnormalities were revealed with conventional MRI (brain) scans. The following criteria were also included for patient ineligibility: (i) present or past history of nervous system symptom or signs; (ii) presence of imaging artifacts on MRI scan, resulting in infeasibility of VBM.
Additionally, healthy, righthanded female volunteers aged between 10 and 18 years were recruited as normal controls. The inclusion criteria were as follows: no history of neurological or psychiatric disorders, no abnormal signs revealed on conventional magnetic resonance imaging (MRI) scans (brain), no past history of perinatal asphyxia and hypoxia, no denture or other metallic foreign bodies in
Brought to you by | University of California - San FranciscoAuthenticated
Download Date | 2/17/15 8:38 PM

Zhao et al.: Cognitive impairment in pediatric patients with Turner syndrome 1113
the head that could affect the quality of MR images, normal physical and intellectual development, and a Wechsler Intelligence Scales for Children (WISC) score > 85. A total of 20 normal controls with a mean age of 13.98 ± 2.22 were recruited.
The age differences between the 45,X karyotype group, the otherkaryotypes group, and the normal control group was not statistically significant (F = 0.317, p = 0.729).
The study protocol was approved by the Ethic and Human Subject Protection Committees of the Imaging Center for Brain Research, Beijing Normal University. Written consent was obtained from all the participating subjects and their guardians.
Wechsler intelligence scales and behavioral testThe intelligence test used in the present study was adopted from the WISC (4th Edition, Chinese Version), in which four composite tests measured four different aspects of the subject’s intellectual level (verbal comprehension, perceptual reasoning, working memory, and processing speed). The time required to complete the entire intelligence test was about 1.5 h. An online behavioral test system, set up by the Department of Psychology at Beijing Normal University, was used to collect subject data scores. The behavioral test, which required about 0.5 h to complete, was designed to assess the following: ability to perform simple subtraction, executive control, shortterm spatial memory, and attention abilities.
Estrogen level and gonadotropin releasing hormone level in pediatric patients with TSWe reviewed the medical records of the pediatric patients with TS in order to gain knowledge of their estrogen and gonadotropin releasing hormone levels prior to their treatment with growth hormones or estrogen.
Collection and analysis of MR dataA Siemens 3.0T Trio scanner (Siemens Medical Solutions, Erlangen, Germany) unit with an 8element phasedarray head coil was used to perform head MRI scans. Magnetizationprepared rapid gradientecho T1weighted imaging of the whole brain was performed. The MRI settings were as follow: TE = 3.39 ms, TR = 2530 ms, TI = 1100 ms, FOV = 256 × 256 mm, slice thickness = 1.33 mm, interslice gap = 0, and scanning duration = 8 min. All pediatric patients underwent examination in their aware and quiet states. No metallic implants or MRI scan contraindication was allowed. The VBM technique was employed for the processing and analysis of data obtained from the T1WIs. All data were processed using the VBM8 software package (http://www.fil.ion.ucl.ac.uk/spm) in the Statistical Parametric Mapping 8 (SPM8) toolbox (http://dbm.neuro.unijena.de/vbm). The major procedures included: (i) segmentation and extraction of MRI (brain) images in order to extract gray and white matter images from the natural space; (ii) standardization for the gray matter images, white matter images, and wholebrain images, as well as calibration for the variation in volumes; the Jacobian pixel series derived during the spatial standardization was used to multiply (or adjust) the pixel value of segmented images; (iii) smoothing process: an 8 mm smooth kernel was applied to smooth every optimized, standardized, and segmented/adjusted image, making the Gaussian spatial structure more normally distributed, and thus obtaining the comparative and analytical structural diagram of gray/white matter.
Statistical analysisStatistical analysis was conducted using SPSS16.0 software package (SPSS Inc., Chicago, IL, USA). All results obtained were expressed in the form of mean ± standard deviation ( S).X± For quantitative data in consistency with normal distribution, intergroup differences were compared with analysis of variance (ANOVA), which verified the differences in age and the Wechsler test scores, as well as the differences in the four composite tests (verbal comprehension, perceptual reasoning, working memory, and processing speed) and the behavioral test between the pediatric patients with TS and the
Table 1 Details about karyotype in pediatric patients with Turner syndrome.
Group types, n Distribution rate Karyotype, n
X haplotype of Group I (21) (46.6%) 45,X (21)Group IIMosaicism (7) (16%) 45,X/46,XX (6)
47,XXX[27]/45,X[3] (1)Long-armed or short-armed chromosome or isochromosome X (10)
(22%) 45,X[15]/46,Xi(xq)[17] (4)
46,Xi(xq) (4)45,X inv(9)(p12q13) (1)mos45X,inv(q)p11q13 (50)/46x,i(x)(q10)inv(q)p11q13(10) (1)
Ring-chromosome X (2) (4.4%) 45,X/46,XX,r(x) (1)X deficiency (1) (2.2%) 46,X,dex(x)(qter-2q21::q28) (1)Others (4) (8.8%) 46,X,mar(x)/45,X (1)
45,X/46,XY/47,YY (1)45,X(8)/46,XYY = G[25]45,X[15]/46,XY[16]
Brought to you by | University of California - San FranciscoAuthenticated
Download Date | 2/17/15 8:38 PM

1114 Zhao et al.: Cognitive impairment in pediatric patients with Turner syndrome
normal controls. For quantitative results disobeying normal distribution, the intergroup differences were compared using a parametric test. VBM8 software package in SPM8 toolbox was applied to conduct analysis of covariance (ANCOVA), which compared differences in gray matter volumes between the subjects in the two TS groups and the normal controls within each voxel of the whole brain.
In the present study, AlphaSim tool (i.e., Monte Carlo simulation), which was included in the AFNI software package (Wisconsin, USA), was used to achieve the correction for multiple comparisons at cluster level. The results showed that while corresponding to the uncorrected significance level of p = 0.01, the statistical results at cluster level reached significance after correction [i.e., familywise error (FWE)corrected p = 0.05] if the run length of the cluster was larger than 350 (gray matter VBM). By using SPM, the Montreal Neurological Institute (MNI)coordinates (coordinates of Montreal Neurological Institute brain mapping) of every statistically significant voxel with the highest tvalue in the brain regions were obtained. Based on these results, the regions with statistical significance were then superimposed on the highresolution color artifacts generated on T1WI, indicating the regions with volume variation of gray matter in the patients with TS.
Results
Intellectual comparison between the pediatric patients with TS and the normal controls
Including the 45 pediatric patients with TS, one underwent MR scanning without taking the intelligence or the behavioral test. Among the other 44 pediatric patients, the overall Wechsler score was 95.78 ± 18.02; 20 patients in the 45,X karyotype group had an overall score of 87.50 ± 15.49, and the 24 patients in the otherkaryotype group obtained an overall score of 91.29 ± 15.37. The overall Wechsler score of the normal controls was 109.45 ± 16.03. The intellectual difference among children in all three groups was statistically significant (z = 11.47, p < 0.01). Notably, the overall Wechsler score of both TS groups was significantly different
compared to the normal controls (F = 21.95, p = 0.000 < 0.05; F = 18.16, p = 0.000 < 0.05). Regarding the scores of the four composite tests (verbal comprehension, perceptual reasoning, working memory and, processing speed), the intergroup difference among the three testing groups was also statistically significant (F = 4.67, p = 0.013 < 0.05; F = 11.96, p = 0.000 < 0.05; F = 6.93, p = 0.002 < 0.05; F = 12.88, p = 0.000 < 0.05). In particular, when compared to the normal controls, patients with TS in both the 45,X karyotype group and otherkaryotype group showed statistically significant differences in the verbal comprehension test (F = 17.00, p = 0.005 < 0.05; F = 12.71, p = 0.026 < 0.05, respectively), perceptual reasoning test (F = 19.25, p = 0.000 < 0.05; F = 16.85, p = 0.000 < 0.05, respectively), working memory test (F = 17.75, p = 0.001 < 0.05; F = 11.35, p = 0.017 < 0.05, respectively), and processing speed test (F = 20.25, p = 0.000 < 0.05; F = 16.40, p = 0.000 < 0.05, respectively). The detailed results are shown in Table 2.
Behavioral comparison between pediatric patients with TS and the normal controls
Apart from one pediatric patient in the 45,X karyotype group, all patients with TS underwent behavioral testing. Children in all three groups demonstrated statistical differences in terms of accuracy in a simple subtraction test, accuracy and reactiontime of a shortterm spatial memory test, and accuracy in the short and middleinterval attention ability tests. Regarding the executive control test, the accuracy and reaction time obtained by the 20 pediatric patients in the 45,X karyotype group were 0.78 ± 0.168 and 748.12 ± 93.627, respectively, while those obtained by the 24 patients in the otherkaryotype group were 0.81 ± 0.125 and 751.38 ± 92.745, respectively, and those obtained by the 20 normal controls were 0.89 ± 0.055 and 659.00 ± 41.536, respectively. Intergroup differences in
Table 2 Comparison of the intelligence test results in all groups.
Full scale intelligence quotient
Verbal comprehension
Perceptual reasoning
Working memory
Processing speed
Normal control group 109.45 ± 16.03 117.25 ± 14.27 103.10 ± 13.80 103.35 ± 15.30 102.65 ± 15.8045,X group 87.50 ± 15.49 100.25 ± 20.73 83.85 ± 12.96 85.6 ± 15.97 82.4 ± 12.49Other karyotype groups 91.29 ± 15.37 104.54 ± 19.29 86.25 ± 14.20 92.00 ± 14.70 86.25 ± 12.16Statistics z F z F z
11.47 4.67 11.96 6.93 12.88p-Value 0.000a,12 0.013a,12 0.000a,12 0.002a,12 0.000a,12
aIndicates that the difference among the three groups is statistically significant; 1, 2, and 3 represent a significant difference between the normal control group and the 45,X group; the normal control group and the other karyotype group; and the 45,X group and the other karyo-type group, respectively (p < 0.05).
Brought to you by | University of California - San FranciscoAuthenticated
Download Date | 2/17/15 8:38 PM

Zhao et al.: Cognitive impairment in pediatric patients with Turner syndrome 1115
Table 3 Comparison of praxiology results in all groups.
Normal control group
45,X group Other karyotype groups
Statistics p-Value
Accuracy of simple subtraction test 43.2 ± 7.74 37.35 ± 10.77 38.25 ± 10.71 F = 2.058 0.136Accuracy of executive control test 0.89 ± 0.055 0.78 ± 0.168 0.81 ± 0.125 F = 4.584 0.014a,12
Reaction time of executive control test 659.00 ± 41.536 748.12 ± 93.627 751.38 ± 92.745 F = 8.733 0.000a,12
Accuracy of short-term spatial memory test 0.72 ± 0.131 0.72 ± 0.275 0.70 ± 0.247 z = 0.281 0.869Reaction time of short-term spatial memory test 809.94 ± 118.868 796.25 ± 123.949 835.10 ± 160.667 F = 0.456 0.636Short-interval accuracy of attention ability 0.95 ± 0.017 0.90 ± 0.107 0.93 ± 0.023 z = 5.332 0.7Short-interval reaction time of attention ability 561.73 ± 723.07 501.60 ± 59.64 484.80 ± 73.984 z = 14.595 0.001a
Middle-interval accuracy of attention ability 0.94 ± 0.021 0.90 ± 0.093 0.92 ± 0.037 z = 4.402 0.133Middle-interval reaction time of attention ability 386.02 ± 77.768 445.04 ± 62.094 438.61 ± 74.694 z = 9.522 0.009a
Long-interval accuracy of attention ability 0.95 ± 0.012 0.89 ± 0.193 0.94 ± 0.023 z = 8.126 0.017a
Long-interval reaction time of attention ability 373.78 ± 59.196 447.43 ± 60.285 434.72 ± 62.536 F = 8.514 0.001a,12
aIndicates that the difference among the three groups is statistically significant; 1, 2, and 3 represent a significant difference between the normal control group and the 45,X group; the normal control group the and other karyotype group; and the 45,X group and the other karyo-type group, respectively (p < 0.05).
accuracy and reactions time among the three groups were statistically significant (F = 4.584, p = 0.014 < 0.05; F = 8.733, p = 0.000 < 0.05, respectively). In particular, patients with TS in both the 45,X karyotype and otherkaryotype groups showed statistically significant differences in accuracy (p = 0.005 < 0.05; p = 0.025 < 0.05, respectively) and reaction time (p = 0.001 < 0.05; p = 0.000 < 0.05, respectively) when compared to normal controls. For the short, middle, and longinterval attention ability tests, intergroup accuracy differences in the middle and long interval attention tests among the three groups were not statistically different (z = 5.332, p = 0.7 > 0.05; z = 4.402, p = 0.133 > 0.05, respectively); however, differences in the accuracy of the shortinterval attention test and the reaction times of all attention tests with different time intervals were statistically significant (z = 8.126, p = 0.017 < 0.05; z = 14.595, p = 0.001 < 0.05; z = 9.522, p = 0.009 < 0.05; z = 8.514, p = 0.001 < 0.05). Notably, in the shortinterval attention ability test, patients with TS in both the 45,X karyotype and otherkaryotype groups showed statistically significant differences in reaction time when compared to normal controls (F = 17.00, p = 0.000 < 0.05; F = 12.71, p = 0.002 < 0.05, respectively). The detailed results are shown in Table 3.
Comparison of estrogen (E2) level and gonadotropin-releasing hormone (FSH) level between the two TS groups
Based on clinical data records, we determined that nine patients in the 45,X karyotype group and 11 patients in the otherkaryotype group had received E2 and FSH level medication; menarche did not occur in all of them. The
clinical data of these patients showed that patients with TS had low E2 but high FSH levels, in particular, the overall E2 level of the nine patients in the 45,X karyotype group was 50.39 ± 37.258, while it was 35.71 ± 64.442 in the 11 patients of the otherkaryotype group; this difference in E2 levels between the two TS groups was not statistically significant (z = –1.919, p = 0.055 > 0.05). The overall FSH level of the nine patients in the 45,X karyotype group was 55.66 ± 32.289, while it was 77.52 ± 54.635 in the 11 patients of the otherkaryotypes group; this difference was also statistically insignificant (t = –1.065, p = 0.3).
Comparison of gray matter volume between patients with TS and the normal controls
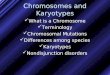
When compared with normal controls, patients in the 45,X karyotype group showed significantly decreased gray matter volume in the bilateral cuneus, calcarine sulcus postcentral gyrus, right precuneus, superior parietal lobule, lingual gyrus, left precentral gyrus, and cingulate gyrus (FWEcorrected p < 0.05, K > 350 voxels) (Table 4), yellowlabeled as shown in the highresolution T1WI (Figure 1). In contrast, these patients had significantly increased gray matter volumes in the bilateral dorsal midbrain, orbital frontal gyrus, left insular lobe, superior temporal gyrus, inferior temporal gyrus, parahippocampal gyrus, cerebellum, posterior insular lobe, right caudate nucleus, putamen, and temporal pole in comparison to the healthy controls (FWEcorrected p < 0.05, K > 350 voxels) (Table 5), bluelabeled as shown in the highresolution T1WI (Figure 1).
When compared to the normal controls, TS patients in the other karyotype group showed significantly decreased
Brought to you by | University of California - San FranciscoAuthenticated
Download Date | 2/17/15 8:38 PM

1116 Zhao et al.: Cognitive impairment in pediatric patients with Turner syndrome
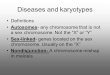
gray matter volume in the left precuneus, cingulate gyrus, right postcentral gyrus, supramarginal gyrus, angular gyrus, and cuneus (FWEcorrected p < 0.05, K > 350 voxels) (Table 6), yellowlabeled as shown in the highresolution T1WI (Figure 2). In contrast, these patients exhibited significantly increased gray matter volume in the bilateral epencephals, left caudate nucleus, superior temporal gyrus, right insular lobe, and temporal pole (FWEcorrected p < 0.05, K > 350 voxels) (Table 7), bluelabeled as shown in the highresolution T1WI (Figure 2).
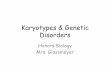
When compared to the TS patients in the otherkaryotype group, TS patients in the 45,X group showed significantly decreased gray matter volume in two regions (FWEcorrected p < 0.05, K > 350 voxels); these two regions mainly involved the left hippocampus and the left caudate nucleus (the number of voxels were 1014 and 496, respectively; the coordinates of MNI centers were 33, –14, –10.5 and –10.5, 3, 18, respectively; the highest tvalues were 4.75 and 4.53, respectively), and are yellowlabeled in the highresolution T1WI (Figure 3). In contrast, the 45,X karyotype patient had significantly increased gray matter volume in the right supramarginal gyrus compared to the
otherkaryotype group (FWEcorrected p < 0.05, K > 350 voxels). The number of voxels was 350; the coordinates of MNI centers were 58.5, –51, and 28.5; the highest tvalue was –4.28. The region was yellowlabeled as shown in the highresolution T1WI (Figure 3).
DiscussionTS is a congenital disorder caused by the entire or partial absence of one X chromosome. As a result of X chromosome deficiency and ovarian hypoplasia, patients with TS experience lifelong gonadal dysfunction related to low levels or even no estrogen in the body. Clinically, TS patients often suffer from nonverbal cognitive impairment, including impulsive dysfunction, impaired concentration, disorientation, spatial learning impairment, and calculation impairment (10); these neurological symptoms are closely associated with morphological and functional abnormalities in the brain (11). Thus, TS patients provide a valuable human model for studying the effect of X chromosomes and estrogen levels on neural structures in the brain.
Table 5 Comparison of brain regions with increased gray matter volume in the 45,X group and the control group.
Regions Voxel number
Brain regions Coordinates MNI center t
1 565 Left insular lobe –40.5, –12, 9 –4.512 485 Left superior temporal gyrus –61.5, –37.5, 9 –4.563 431 Right caudate nucleus, putamen 18, 28.5, –4.5 –4.434 386 Dorsal midbrain –1.5, –36 –14 –4.945 1444 Right orbital frontal gyrus 24, 33, –21 –5.016 1188 Left inferior temporal gyrus, parahippocampal gyrus –51, –49.5, –27 –5.967 973 Left orbital frontal gyrus –13.5, 48, –19.5 –5.68 791 Left epencephalon –27, –81, –21 –5.679 725 Right posterior insular lobe –39, –15, –6 –5.23
10 695 Right temporal pole 51, 7.5, –4.5 –4.85
MNI, Montreal Neurological Institute.
Table 4 Comparison of brain regions with decreased gray matter volume in the 45,X group and the control group.
Regions Voxel number
Brain regions Coordinates MNI center
t
1 4117 Right cuneus, precuneus, calcarine sulcus 9, –68, 27 5.75Left cuneus, calcarine sulcus
2 1392 Left precentral gyrus, postcentral gyrus –22.5, –26, 54 5.333 1085 Left cingulate gyrus –12, –48, 30 5.024 748 Right postcentral gyrus 24, –45, 60 6.545 696 Right superior parietal lobule 51, –30, 39 5.226 680 Right postcentral gyrus 52.5, –12, 28.5 4.357 577 Right lingual gyrus 27, –69, –9 5.42
MNI, Montreal Neurological Institute.
Brought to you by | University of California - San FranciscoAuthenticated
Download Date | 2/17/15 8:38 PM

Zhao et al.: Cognitive impairment in pediatric patients with Turner syndrome 1117
In this present study, we compared TS patients presenting with different karyotypes to normal controls, while exploring the association between different karyotypes, sex hormone levels (E2 and FSH), the outcome of cognitive and behavioral tests, and brain neuroimaging findings. The results of the present study suggest the following.
The neuropathological basis of cognitive impairment in TS patients may be as a result of variation in gray matter volume
The present study demonstrated that gray matter volume in the parietal lobe of pediatric TS patients in the 45,X group was lower than that of normal controls. This result
Figure 1 Voxel-based morphometry (VBM) analysis shows the yellow region representing the regions with decreased gray matter volume in the 45,X group compared to the control group, this includes the bilateral cuneus, calcarine sulcus, postcentral gyrus, right precuneus, superior parietal lobule, lingual gyrus, left precentral gyrus, and cingulate gyrus; the blue region represents the regions with increased gray matter volume in the 45,X group compared to the control group, this includes the dorsal midbrain, orbital frontal gyrus; left insular lobe, superior temporal gyrus, inferior temporal gyrus, parahippocampal gyrus, cerebellum, posterior insular lobe; right caudate nucleus, putamen, and temporal pole.
Table 6 Comparison of brain regions with decreased gray matter volume in the other karyotype group and the control group.
Regions Voxel number
Brain regions Coordinates MNI center
t
1 1212 right postcentral gyrus 4.74 45, –18, 362 1039 Right supramarginal gyrus, angular gyrus 5.09 55.5, –49.5, 28.53 681 Left inferior frontal gyri 4.53 –49.5, –6, 184 591 Left precuneus, cingulate gyrus 4.95 –7.5, –46.5, 43.55 433 Right cuneus 4.5 10.5, –99, 19.56 394 Right inferior frontal gyri 3.82 60, –9, 12
MNI, Montreal Neurological Institute.
Brought to you by | University of California - San FranciscoAuthenticated
Download Date | 2/17/15 8:38 PM

1118 Zhao et al.: Cognitive impairment in pediatric patients with Turner syndrome
is consistent with the findings of previous studies conducted by Brown et al. (12) and Marzelli et al. (10) that demonstrated shrinkage of gray matter in the parietal lobe and postcentral gyrus, respectively. Moreover, we also found that the 45,X karyotype group displayed decreased gray matter volume in the bilateral cuneus, calcarine
sulcus, postcentral gyrus, right precuneus, superior parietal lobule, lingual gyrus, left precentral gyrus, and cingulate gyrus, while the otherkaryotype group displayed decreased gray matter volume in the left precuneus, cingulate gyrus, right postcentral gyrus, supramarginal gyrus, angular gyrus, and cuneus. These cerebral structures
Figure 2 Voxel-based morphometry (VBM) analysis shows the yellow region representing the regions with decreased gray matter volume in the other karyotype group compared to the control group, this includes the bilateral inferior prefrontal cortex; left precuneus, cingulate gyrus; right postcentral gyrus, supramarginal gyrus, angular gyrus, and cuneus; the blue region represents the regions with increased gray matter volume in the other karyotype group compared to the control group, this includes the bilateral epencephals, left caudate nucleus, superior temporal gyrus, right insular lobe, and temporal pole.
Table 7 Comparison of brain regions with increased gray matter volume in the other karyotype group and the control group.
Regions Voxel number
Brain regions Coordinates MNI center
t
1 1290 Right epencephalon –6.63 27, –55.5, –34.52 1185 Left insular lobe –5.35 36, –15, –63 910 Left epencephalon –5.36 –16.5, –49.5, –604 838 Left epencephalon –5.21 –25.5, –85.5, –215 479 Right temporal pole –4.22 61.5, 4.5, –96 447 Left caudate nucleus –4.55 –18, –4.5, 277 408 Left superior temporal gyrus –4.71 –63, –34.5, 158 353 Left epencephalon –4.26 –27, –55.5, –36
MNI, Montreal Neurological Institute.
Brought to you by | University of California - San FranciscoAuthenticated
Download Date | 2/17/15 8:38 PM

Zhao et al.: Cognitive impairment in pediatric patients with Turner syndrome 1119
are closely associated with visual spatial function, calculation skill, logic thinking, and motor sensory ability (10). Regarding the results of intellectual and behavioral tests, the TS patients in both the 45,X group and the other karyotype group showed relatively inferior performances in perceptual reasoning, processing speed, executive control, and attentional reaction time compared to normal controls. Thus, decreases in gray matter volume in these regions may relate to injured motor and sensory function, as well as impairments in visual spatial ability, calculation skill, logic thinking, and concentration.
Our findings regarding the brain regions exhibiting increased gray matter volume in TS patients were largely consistent with those of previous findings in the literature. Brown et al. investigated the variations in brain volumes of 26 patients with monosomy TS (12), they found that increased gray matter volume in the cerebellum was the most prominent structural change in the brains of patients with TS. Based on VBM analysis conducted by Good et al. on 21 cases of monosomy TS, the patients
demonstrated larger prefrontal cortex volume when compared with normal controls (13). Moreover, Rae et al. reported increased gray matter volume in both the superior temporal and middle temporal gyrus in nine cases of patients with monosomy TS (14). Molko et al. also reported an increase in gray matter volume in the fusiform gyrus, temporal pole, lingual gyrus, and orbitofrontal cortex (15). Besides the findings of these studies, our present study further reveals increased gray matter volume in the dorsal midbrain, left insular lobe, parahippocampal gyrus posterior to insular lobe, right caudate nucleus, and putamen in patients with the 45,X karyotype, as well as in the bilateral putamen, hippocampus, parahippocampal gyrus, insula, caudate nucleus, amygdala, and right thalamus of patients with other karyotypes. The abovementioned abnormal regions covered the majority of verbal regions in the hemisphere. According to some researchers, memory function is associated with gray matter volume in areas such as the temporal lobe, frontal lobe, parietal lobe, cingulate gyrus, and parahippocampal gyrus (16). Containing
Figure 3 Voxel-based morphometry (VBM) analysis shows the yellow region representing the regions with decreased gray matter volume in the 45,X group compared to the other karyotype group, this includes the left hippocampus and left caudate nucleus; the blue region represents the regions with increased gray matter volume in the 45,X group compared to the other karyotype group, this includes the right supramarginal gyrus.
Brought to you by | University of California - San FranciscoAuthenticated
Download Date | 2/17/15 8:38 PM

1120 Zhao et al.: Cognitive impairment in pediatric patients with Turner syndrome
more than 50% of central nervous system neurons, the cerebellum is believed to play an essential role in learning memory (17). The limbic system, including the parahippocampal gyrus and insular lobe, is not only closely intermingled with the temporal lobe but also widely linked to the frontal lobe, the parietal lobe and other areas. The integrity and functionality of the limbic system determines a person’s emotional reaction, behavior, and memory (18). The left hemisphere of humans plays a dominant role in verbal and motor functions, while the right hemisphere dominates nonverbal cognitive functions. In pediatric patients with TS, there are indeed some obvious variations in gray matter volume in either the unilateral or bilateral hemispheres, irrespective of the karyotype possessed by the patient. These changes may be the neuropathological basis accounting for the statistically significant differences in verbal comprehension, perceptual reasoning, working memory, processing speed, executive control ability, and attentional reaction time between TS patients and normal controls.
Further studies are required to reveal the relationship between the interkaryotype (monosomy vs. others) differences in sex hormone level and neurological cognitive impairment/brain morphological changes
The endocrine system plays an important regulatory role in the development of the human brain, in particular, the influence of estrogen on the human brain has been determined (19). In postmenopausal women, declining estrogen levels results in lower synthesis and secretion of the neurotransmitter as well as impaired receptor function. Moreover, neural plasticity, synaptic quantity and connectivity also decrease, which imposes a direct effect on the functioning and growth of neurons. During the postmenopausal period, the incidence of apoplexy, cognitive impairment, and memory decline increase significantly (20). The congenital gonadal deficits experienced by TS patients causes a lifelong low estrogen level and no estrogen secretion. Estrogen could affect the neurological cognitive functions of TS patients via the nervousendocrine pathway.
In the present study, the results of FSH determination conducted on the TS patients showed that all patients
presented with low estrogen but high FSH levels, irrespective of the karyotype. The results of intellectual and behavioral tests also indicated variations in gray matter volume in the bilateral or unilateral hemisphere; the scoring differences in the verbal comprehension, perceptual reasoning, working memory, processing speed, executive control ability, and attentional reaction time were also statistically significant. TS did not only produce nonverbal cognitive impairment but also verbal cognitive impairment as both pediatric TS groups had significantly lower comprehension test scores than normal controls. This result was inconsistent with those of a previous study (2). Furthermore, variation in estrogen and FSH levels between the TS patients in the 45,X karyotype group and the otherkaryotype groups were statistically insignificant. Differences in intellectual and behavioral testing scores were also statistically insignificant between both TS groups. Further indepth studies are required to verify the effect of low estrogen levels on the neurological cognitive impairment of TS patients. Regarding MRI scans, patients in both TS groups showed reduced gray matter volumes in the left hippocampus and left caudate nucleus, as well as increased gray matter volume in the right supramarginal gyrus. Indepth further studies with a larger sample scale are required to reveal the effect of different karyotypes and hormone levels on brain anatomical variation and the exact mechanism by which they influence structural changes.
In conclusion, the neuropathological basis accounting for the cognitive behavioral impairment observed in pediatric patients with TS may be as a result of morphological changes in the brain as well as changes in gray matter volume. Further studies are required to verify the correlation between TSrelated cognitive impairment and the absence of X chromosome/low estrogen levels, as well as the exact mechanism involved. The limitations of the present study include the complexity of the karyotypes in the “other karyotype” group. Employing a more sophisticated karyotypebased grouping system, such as one based on the loci of gene mutation could significantly improve studies focusing on the correlation between the absence of chromosome X and neurological cognitive impairment/in vivo hormone levels.
Received April 4, 2013; accepted May 16, 2013; previously published online July 12, 2013
Brought to you by | University of California - San FranciscoAuthenticated
Download Date | 2/17/15 8:38 PM

Zhao et al.: Cognitive impairment in pediatric patients with Turner syndrome 1121
References1. Gonzalez L, Witchel SF. The patient with Turner syndrome:
puberty and medical management concerns. Fertil Steril 2012;98:780–6.
2. Mazzocco MM. The cognitive phenotype of Turner syndrome: specific learning disabilities. Int Congr Ser 2006;1298:83–92.
3. Holzapfel M, Barnea-Goraly N, Eckert MA, Kesler SR, Reiss AL. Selective alterations of white matter associated with visuospatial and sensorimotor dysfunction in Turner syndrome. J Neurosci 2006;26:7007–13.
4. Lee YY, Hung J, Chang TY, Huang CC. Agenesis of the corpus callosum in Turner’s syndrome: report of a case and review of the literature. Acta Neurol Taiwan 2008;17:194–8.
5. Longman C, Mackenzie J, Rankin R, McEntagart M, Johnson R, et al. Sudden death in a patient with mosaic ring X Turner syndrome and a neuronal migration disorder. Clin Dysmorphol 2008;17:69–71.
6. Bray S, Dunkin B, Hong DS, Reiss AL. Reduced functional connectivity during working memory in Turner syndrome. Cereb Cortex 2011;21:2471–81.
7. Skuse DH, Morris JS, Dolan RJ. Functional dissociation of amygdala-modulated arousal and cognitive appraisal, in Turner syndrome. Brain 2005;128:2084–96.
8. Kesler SR, Menon V, Reiss AL. Neurofunctional differences associated with arithmetic processing in Turner syndrome. Cerebral Cortex 2006;16:849–56.
9. Marzelli MJ, Hoeft F, Hong DS, Reiss AL. Neuroanatomical spatial patterns in Turner syndrome. Neuroimage 2011;55:439–47.
10. Hong D, Scaletta Kent J, Kesler S. Cognitive profile of Turner syndrome. Dev Disabil Res Rev 2009;15:270–8.
11. Lepage JF, Hong DS, Hallmayer J, Reiss AL. Genomic imprinting effects on cognitive and social abilities in prepubertal girls with Turner syndrome. J Clin Endocrinol Metab 2012;97:E460–4.
12. Brown WE, Kesler SR, Eliez S, Warsofsky IS, Haberecht M, et al. Brain development in Turner syndrome: a magnetic resonance imaging study. Psychiatry Res 2002;116:187–96.
13. Good CD, Lawrence K, Thomas NS, Price CJ, Ashburner J, et al. Dosage-sensitive X-linked locus influences the development of amygdala and orbitofrontal cortex, and fear recognition in humans. Brain 2003;126:2431–46.
14. Rae C, Joy P, Harasty J, Kemp A, Kuan S, et al. Enlarged temporal lobes in Turner syndrome: an X-chromosome effect? Cereb Cortex 2004;14:156–64.
15. Molko N, Cachia A, Riviere D, Mangin JF, Bruandet M, et al. Brain anatomy in Turner syndrome: evidence for impaired social and spatial-numerical networks. Cereb Cortex 2004;14:840–50.
16. Jambaqué I, Dellatolas G, Fohlen M, Bulteau C, Watier L, et al. Memory functions following surgery for temporal lobe epilepsy in children. Neuropsychologia 2007;45:2850–62.
17. Lasker AG, Mazzocco MM, Zee DS. Ocular motor indicators of executive dysfunction in fragile X and Turner syndromes. Brain Cogn 2007;63:203–20.
18. Deng HZ, Zou XB, Tang C, Cheng M. The brain functional imaging changes and relationship between brain changes and behavior of autistic children. Chin J Child Health Care 2001;9:154–6.
19. Cutter WJ, Daly EM, Robertson DM, Chitnis XA, van Amelsvoort TA, et al. Influence of X chromosome and hormones on human brain development: a magnetic resonance imaging and proton magnetic resonance spectroscopy study of Turner syndrome. Biol Psychiatry 2006;59:273–83.
20. Liu DE, Luo BR. Postmenopausal hormone therapy and cognitive and memory issues. Chin J Pract Gynecol Obstet 2011;27:343–5.
Brought to you by | University of California - San FranciscoAuthenticated
Download Date | 2/17/15 8:38 PM