Embed Size (px)
Citation preview
Cognitive behavior therapy for depression in people with
epilepsy: A systematic review*†MilenaGandy, *Louise Sharpe, and ‡KathrynNicholson Perry
Epilepsia, **(*):1–10, 2013doi: 10.1111/epi.12345
SUMMARY
Cognitive behavioral therapy (CBT) is a recommended treatment for depression in people with epilepsy (PWE); how-
ever, a recent Cochrane review found that there was insufficient evidence that any psychological therapy is effective.
This conclusion provides little help to clinicians who provide interventions for depressed PWE. The aim of this review
was to systematically and qualitatively review the literature on the efficacy of CBT for depression in PWE based on
randomized controlled trials (RCTs) and case series.We aim to determine patterns in the literature to inform the type
of CBT, if any, that should be offered to PWE who are depressed. Databases MEDLINE, PsycINFO, and the Cochrane
EBM Reviews were searched via OVID. Selection criteria included the following: (1) participants with epilepsy; (2) use
of CBT; (3) valid depression outcome measure; and (4) published in peer-reviewed journal in English. Inclusions of
studies were assessed by two independent researchers. We identified 14 outcome papers for 13 CBT trials including 6
randomized controlled trials (RCTs) and 7 case series. Positive effects of CBT on depression were reported in three of
six RCTs. A review of their content revealed that all effective RCTs specifically tailored CBT to improve depression.
Conversely, two of three RCTs that failed to find depression-related effects focused on improving seizure-control. This
pattern was also observed in the case series. Although limited in number and having methodologic limitations, the
treatment studies included in our review suggest that interventions tailored toward improving depression are possibly
efficacious, whereas those that focus on improving seizure control do not appear to be. However, this review highlights
that there is need for further RCTs in this area in order to confirm the possible efficacy of CBT for depression in PWE.
KEYWORDS: Mood, Psychotherapy, Seizure.
Despite the high prevalence and significant consequencesof comorbid depression in people with epilepsy (PWE), itoften remains untreated (Hermann et al., 2000; Jones et al.,2003; Barry et al., 2008; Kanner, 2011). Physician reluc-tance to place PWE on antidepressant medication, due tofears of lowering seizure threshold and adverse drug interac-tions between antidepressants and antiepileptic drugs, hasbeen identified to be a major barrier for the treatment ofdepression in PWE (Barry et al., 2008; Cotterman-Hart,2010; Noe et al., 2011). As a result, effective psychologicaltherapies aimed at improving depression in PWE would be
of particular value (Barry et al., 2008; Ramaratnam et al.,2008; Kerr et al., 2011).
A recent Cochrane review assessed the findings of16 randomized controlled and quasi-randomized trials ofpsychological treatment in PWE (Ramarantnam et al.,2008). The review found no reliable evidence that anypsychological treatment—including relaxation therapy,electroencephalography (EEG) biofeedback, and cognitivebehavioral therapy (CBT)—led to significant improve-ment in seizure control or improvement in quality of life(QoL). The treatments included in the review were variedin therapeutic content, rated as methodologically weak,and yielded mixed results (Ramarantnam et al., 2008).Despite the lack of conclusive evidence for effective treat-ments for depression in PWE, the recent internationalconsensus clinical practice statement for the treatment ofneuropsychiatric conditions associated with epilepsy rec-ommended CBT as the psychological treatment of choicefor depression in PWE (Kerr et al., 2011).
CBT has been found to be an effective treatment fordepression in the general population (Tolin, 2010; Hofmannet al., 2012) as well as in a number of health populations,
Accepted July 16, 2013.*The School of Psychology, University of Sydney, Sydney, New South
Wales, Australia; †The Centre for Emotional Health (CEH), Departmentof Psychology, Macquarie University, Sydney, New South Wales,Australia; and ‡Centre for Health Research, School of Social Sciencesand Psychology, University of Western Sydney, Bankstown, New SouthWales, Australia
Address correspondence to Milena Gandy, The School of Psychology,University of Sydney, Brennan MacCallum Bld (A18), Sydney, NSW2006, Australia. E-mail: [email protected]
Wiley Periodicals, Inc.© 2013 International League Against Epilepsy
1
CRITICALREVIEWAND INVITEDCOMMENTARY
including multiple sclerosis (Mohr et al., 2001), chronicpain (Eccleston et al., 2003), rheumatoid arthritis (Sharpeet al., 2001), and chronic obstructive pulmonary disease(COPD; Livermore et al., 2010). One of the significant ben-efits of CBT as a form of therapy is its ability to be adaptedto address specific issues for different health populations(Krishnamoorthy, 2003). However, despite these numerousrecommendations, the effectiveness of CBT to improvedepression in PWE remains unclear.
The recent Cochrane review was limited to randomizedcontrolled trials (RCTs) and included only three RCTs ofCBT for depression. An additional three trials have sincebeen conducted in this area. Therefore, the first aim ofthis systematic review was to provide the first review ofall the published evidence for CBT interventions for PWEto improve depression outcomes. The second aim was toassess whether the literature allows any recommendationsas to which CBT strategies are most strongly empiricallysupported for the treatment of depression in PWE, whichcould help clinicians provide treatments for PWE whohave mood disturbances that are more strongly evidencebased.
MethodsUsing the Meta-analysis of Observational Studies in
Epidemiology (MOOSE) criteria as a guide (Stroup et al.,2000), we conducted a literature search of published studies
in April 2012. The electronic databases MEDLINE,PsycINFO, and the Cochrane EBM Reviews—CochraneCentral Register of Controlled Trial were searched viaOVID using different combinations of the following words:epileps*, seizure, depression, depressive symptoms, mood,cognitive therapy, behaviour therapy, problem solving ther-apy, mindfulness therapy, and psychotherapy. The searchstrategy modeled but expanded upon the Cochrane reviewof psychological treatment in epilepsy search strategies(Ramarantnam et al., 2008). There were no limits placed onthe years for searched articles. All medical Subject Heading(MeSH) terms were exploded to broaden the search for rele-vant studies. In addition, the ancestry method, whichinvolves hand searching the reference list of empirical stud-ies and reviews, was used to identify further studies. Tomeet the inclusion criteria, the study needed to: (1) involveparticipants with a diagnosis of epilepsy, (2) use a form ofCBT, (3) use established measures of depression as outcomemeasures, and (4) be published in a peer-reviewed journal inEnglish.
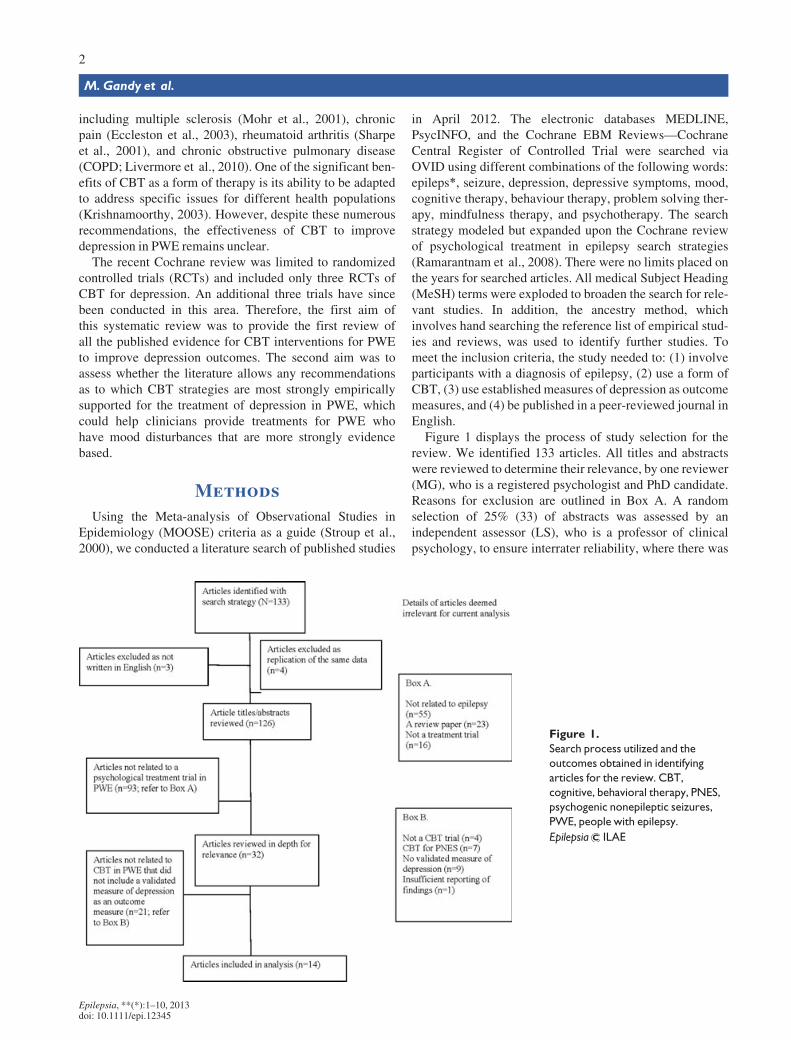
Figure 1 displays the process of study selection for thereview. We identified 133 articles. All titles and abstractswere reviewed to determine their relevance, by one reviewer(MG), who is a registered psychologist and PhD candidate.Reasons for exclusion are outlined in Box A. A randomselection of 25% (33) of abstracts was assessed by anindependent assessor (LS), who is a professor of clinicalpsychology, to ensure interrater reliability, where there was
Figure 1.
Search process utilized and the
outcomes obtained in identifying
articles for the review. CBT,
cognitive, behavioral therapy, PNES,
psychogenic nonepileptic seizures,
PWE, people with epilepsy.
Epilepsia ILAE
Epilepsia, **(*):1–10, 2013doi: 10.1111/epi.12345
2
M. Gandy et al.

100% agreement. Following this, 32 abstracts wereretained, and full copies of the articles were reviewed. Tworaters (MG and LS) independently assessed each article foreligibility, as outlined in Box B. Three additional articleswere retrieved via the ancestry method. A list of excludedRCTs is included in Table S1. Disagreement betweenreviewers was resolved by consensus; interrater reliabilityhad a kappa coefficient of 0.86.
All RCTs were rated using the PEDro-P scale. ThePEDro-P is a modified version of the PEDro scale, whichwas initially developed to rate the quality of RCTs for thepurpose of systematic reviews, on the Physiotherapy Evi-dence Database (Maher et al., 2003). The scale has beenmodified by researchers who manage the PsychologicalDatabase for Brain Impairment Treatment Efficacy (Psych-bite), to tailor it to the analysis of treatment trials in the areaof brain impairment, including epilepsy. The PEDro-P wasselected because it provides a quality score based on strictinternal validity criterion for RCTs, which were establishedby strict Delphi technique procedures (Verhagen et al.,1998). The PEDro-P quality score allows for comparisonbetween RCTs and has been found to have good reliability(Maher et al., 2003). The scale contains 11 items, one ques-tion assesses external validity and the remaining 10 assessinternal validity. The PEDro-P items are scored as yes (1)or no (0). A copy of the items and the PEDro-P scores foreach RCT have been reported in Table S2.
Given that case series provide only Level IV Evidencefor the efficacy of an intervention, according to the NationalHealth and Medical Research Council (NHMRC) of Austra-lia definitions (2009), we include them in this review inorder to determine whether the patterns that are identifiedfrom RCTs are also supported in the case series that appearin the literature. However, we have not assessed case seriesfor quality, since by definition internal and external validityare likely to be relatively low.
ResultsTrial design
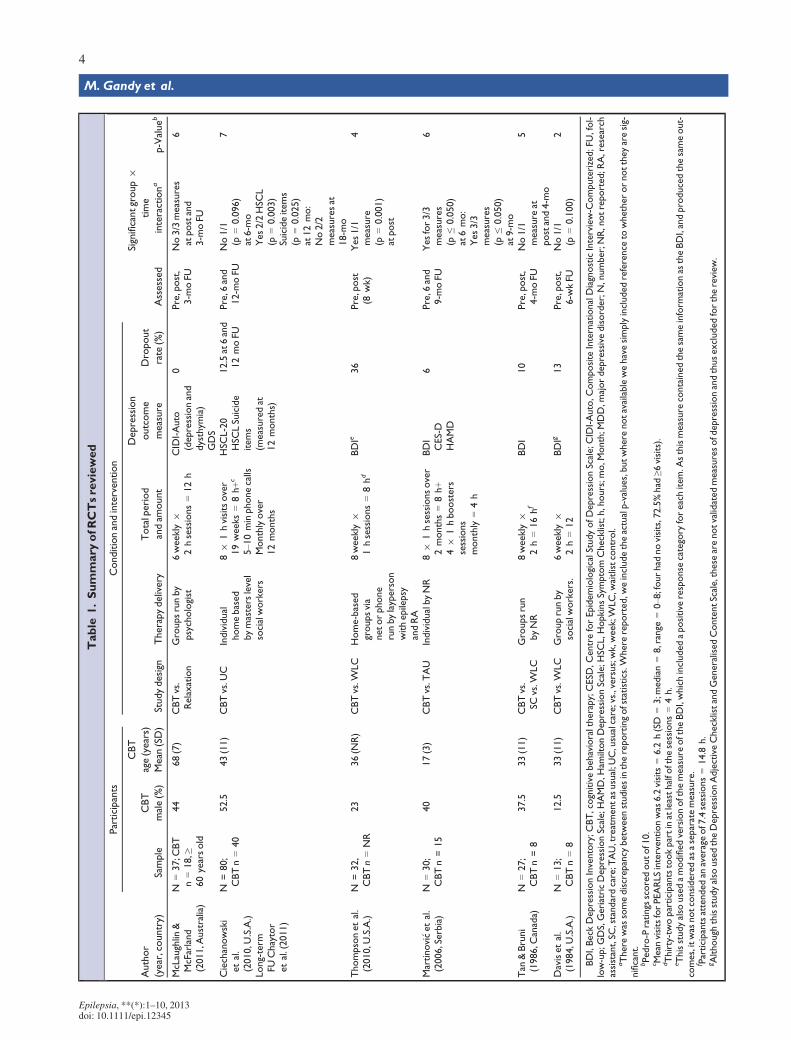
Fourteen articles reporting 13 CBT studies were identi-fied. One paper was a long-term follow-up analysis of oneof the RCTs (Chaytor et al., 2011), and was therefore notconsidered as a separate study. A detailed summary of thestudies is provided in Table 1. Six of the studies wereRCTs (Davis et al., 1984; Tan & Bruni, 1986; Martinovi�cet al., 2006; Ciechanowski et al., 2010; Thompson et al.,2010; McLaughlin & McFarland, 2011), thus providingNHMRC Level II Evidence (NHMRC, 2009). Four of thesix RCT designs employed simple comparisons of CBTwith a waitlist control (WLC) or treatment as usual(TAU). One trial compared CBT with both WLC andTAU and another compared CBT with relaxation. Theremaining seven articles were treatment trial case seriesdesigned studies (n = 7).
Trial qualityAll trials had a total score of 1 for external validity on the
PEDro-P, as they each specified their trial eligibility crite-ria. For internal validity, the PEDro-P scores ranged from 2to 7 (M = 5, standard deviation [SD] = 1.8). All trials usedrandom allocation, with only one failing to conceal alloca-tion (Tan & Bruni, 1986). Two studies failed to report base-line comparability between their treatment groups (Daviset al., 1984; Tan & Bruni, 1986). Only two studies usedblind assessors to assess at least one key outcome measure(Tan & Bruni, 1986; Ciechanowski et al., 2010). Three haddropout rates in excess of 12% (Davis et al., 1984; Ciecha-nowski et al., 2010; Thompson et al., 2010). Only two trialsreported an intention-to-treat analysis (Tan & Bruni, 1986;Ciechanowski et al., 2010). Between-group statistical com-parisons were reported in all but one trial (Davis et al.,1984). Point estimates and variability for treatment effectswere reported in only half of the trials (Martinovi�c, 2001;Ciechanowski et al., 2010; McLaughlin & McFarland,2011).
Randomized controlled trial details
ParticipantsWhen the six RCTs are considered, a total of 247 partici-
pants entered these trials (mean 41 (SD 22); range 15–80);of these 219 (89%) completed the majority of treatment(mean 37 (SD 23); range 13–80). The mean percentage ofmale participants in CBT groups was only 25% (SD 15;range 12.5–52.5). The sample had a mean age of 38 years(SD 17; range 17–68).
Only three trials stipulated specific epilepsy criteria. Oneincluded participants with newly diagnosed epilepsy (Marti-novi�c et al., 2006), another excluded newly diagnosedpatients (Thompson et al., 2010), and one included onlypatients with inadequate seizure control (Tan & Bruni,1986). One study specifically treated adolescent patients(13–19 years old; Martinovi�c et al., 2006) and another olderadults (≥60 years old) only (McLaughlin & McFarland,2011).
Treatment deliveryOf the six RCTs, four examined group therapy (Davis
et al., 1984; Tan & Bruni, 1986; Thompson et al., 2010;McLaughlin & McFarland, 2011), one using “virtualgroups” via the internet or telephone (Thompson et al.,2010). Of the four programs that described the qualifica-tions of facilitators, one used lay therapists (Thompsonet al., 2010), one used psychologists (McLaughlin &McFarland, 2011), and the remaining two were facilitatedby social workers (Davis et al., 1984; Ciechanowski et al.,2010).
The mean total treatment duration for the RCTs was9 weeks (SD =5, range 6–19 weeks) and the mean numberof hours in treatment was 11 h (SD 3, range 8–16 h). All
Epilepsia, **(*):1–10, 2013doi: 10.1111/epi.12345
3
CBT for Depression in PWE
Table
1.Summary
ofRCTsreviewed
Author
(year,country)
Participants
Conditionandintervention
Assessed
Significantgroup9
time
interactiona
p-Valueb
Sample
CBT
male(%)
CBT
age(years)
Mean
(SD)
Studydesign
Therapydelivery
Totalperiod
andam
ount
Depression
outcome
measure
Dropout
rate
(%)
McLaughlin
&McFarland
(2011,A
ustralia)
N=37;C
BT
n=18,≥
60yearsold
44
68(7)
CBTvs.
Relaxation
Groupsrunby
psychologist
6weekly
92hsessions=12h
CID
I-Auto
(depressionand
dysthym
ia)
GDS
0Pre,post,
3-m
oFU
No3/3measures
atpostand
3-m
oFU
6
Ciechanowski
etal.
(2010,U
.S.A.)
Long-term
FUChaytor
etal.(2011)
N=80;
CBTn=40
52.5
43(11)
CBTvs.U
CIndividual
homebased
bymasterslevel
socialworkers
89
1hvisitsover
19weeks=8h+c
5–1
0minphonecalls
Monthlyover
12months
HSC
L-20
HSC
LSuicide
items
(measuredat
12months)
12.5at6and
12moFU
Pre,6
and
12-m
oFU
No1/1
(p=0.096)
at6-m
oYes2/2HSC
L(p
=0.003)
Suicideitems
(p=0.025)
at12mo:
No2/2
measuresat
18-m
o
7
Thompsonetal.
(2010,U
.S.A.)
N=32,
CBTn=NR
23
36(N
R)
CBTvs.W
LC
Home-based
groupsvia
netorphone
runbylayperson
withepilepsy
andRA
8weekly
91hsessions=8hd
BDIe
36
Pre,post
(8wk)
Yes1/1
measure
(p=0.001)
atpost
4
Martinovi� cetal.
(2006,Serbia)
N=30;
CBTn=15
40
17(3)
CBTvs.T
AU
IndividualbyNR
89
1hsessionsover
2months=8h+
49
1hboosters
sessions
monthly
=4h
BDI
CES-D
HAMD
6Pre,6
and
9-m
oFU
Yesfor3/3
measures
(p≤0.050)
at6mo:
Yes3/3
measures
(p≤0.050)
at9-m
o
6
Tan
&Bruni
(1986,C
anada)
N=27;
CBTn=8
37.5
33(11)
CBTvs.
SCvs.W
LC
Groupsrun
byNR
8weekly
92h=16hf
BDI
10
Pre,post,
4-m
oFU
No1/1
measure
atpostand4-m
o
5
Davisetal.
(1984,U
.S.A.)
N=13;
CBTn=8
12.5
33(11)
CBTvs.W
LC
Grouprunby
socialworkers.
6weekly
92h=12
BDIg
13
Pre,post,
6-w
kFU
No1/1
(p=0.100)
2
BDI,Beck
DepressionInventory;C
BT,cognitivebehavioraltherapy;CESD
,CentreforEpidemiologicalStudyofDepressionScale;C
IDI-Auto,C
omposite
InternationalDiagnosticInterview-C
omputerized;FU
,fol-
low-up;G
DS,GeriatricDepressionScale;H
AMD,H
amiltonDepressionScale;H
SCL,H
opkinsSymptom
Checklist;h,hours;m
o,M
onth;M
DD,m
ajordepressivedisorder;N,number;NR,notreported;R
A,research
assistant,SC
,standardcare;T
AU,treatmentas
usual;U
C,usualcare;vs.,versus;wk,w
eek;W
LC,w
aitlistcontrol.
aThere
was
somediscrepancy
betw
eenstudiesinthereportingofstatistics.W
here
reported,w
eincludetheactualp-values,butwhere
notavailablewehavesimplyincludedreference
towhetherornottheyaresig-
nificant.
bPedro-P
ratings
scoredoutof10.
c Mean
visitsforPEARLSinterventionwas
6.2visits
=6.2
h(SD
=3;m
edian=8,range
=0–8
;fourhad
novisits,72.5%had
≥6visits).
dThirty-twoparticipantstookpartinatleasthalfo
fthesessions=4h.
eThisstudyalso
usedamodifiedversionofthemeasure
oftheBDI,whichincludedapositive
response
category
foreachitem.A
sthismeasure
containedthesameinform
ationas
theBDI,andproducedthesameout-
comes,itwas
notconsideredas
aseparatemeasure.
f Participantsattendedan
average
of7.4sessions=14.8
h.
gAlthough
thisstudyalso
usedtheDepressionAdjectiveChecklistandGeneralisedContentScale,these
arenotvalidatedmeasuresofdepressionandthusexcludedforthereview.
Epilepsia, **(*):1–10, 2013doi: 10.1111/epi.12345
4
M. Gandy et al.

trials offered weekly or every two week therapy. Two trialsprovided booster sessions and support for rehearsal of skillslearned in the primary intervention phase (Martinovi�c et al.,2006; Ciechanowski et al., 2010).
Depression measuresThree (of six) RCTs specified depression status criteria.
One only included participants with a formal diagnosis ofdepression (Ciechanowski et al., 2010). Another includedparticipants defined as having “subthreshold depression,”whereby patients reported elevated symptoms of depressionon measures (Beck Depression Inventory [BDI], or the Cen-ter for Epidemiological Study of Depression measure [CES-D], and Hamilton Depression Scale [HAMD]), but did notnecessarily meet diagnostic criteria for depression (Marti-novi�c et al., 2006). The third trial selected participantsbased on their scores on the CES-D (Ciechanowski et al.,2010; Thompson et al., 2010), such that only those withscores in the range of >13 to <38 were included (Thompsonet al., 2010). Only one of the six studies used a diagnosticinterview (McLaughlin & McFarland, 2011), althoughanother used the HAMD to assess clinician-rated symptomseverity (Martinovi�c et al., 2006). The remainder relied onpatient self-report scales, including the BDI (4/6; Daviset al., 1984; Tan & Bruni, 1986; Martinovi�c et al., 2006;Thompson et al., 2010), CES-D (1/6; Martinovi�c et al.,2006), Hopkins Symptom Checklist-20 (HSCL-20 [1/6];Ciechanowski et al., 2010), and the Geriatric DepressionScale (GDS; [1/6]; McLaughlin et al., 2008). Only one ofthe six studies assessed suicidal ideation (Ciechanowskiet al., 2010).
RCT CBT components focusTable 2 provides a detailed description of the CBT com-
ponents in each of the treatment trials. Five (of the six) trialsexplicitly noted that the aim of the study was to evaluate thebenefits of CBT for improving depression outcomes (Daviset al., 1984; Martinovi�c et al., 2006; Ciechanowski et al.,2010; Thompson et al., 2010; McLaughlin & McFarland,2011); one trial instead referred to improvements in psycho-pathology (Tan & Bruni, 1986). Three (of six) trials alsoaimed to evaluate the benefits of CBT to improve seizurecontrol (Tan & Bruni, 1986; Martinovi�c et al., 2006;McLaughlin & McFarland, 2011) and four (of six) toimprove quality of life or psychosocial wellbeing (Tan &Bruni, 1986; Martinovi�c et al., 2006; Thompson et al.,2010; McLaughlin & McFarland, 2011). Thompson et al.(2010) also aimed to assess the effects of CBT for increasingknowledge/skills and self-efficacy. An important distinctioncan be made in terms of the primary focus of these CBTinterventions. Four (of six) RCTs primarily tailored CBT toimprove depression and coping in PWE (Davis et al., 1984;Martinovi�c et al., 2006; Ciechanowski et al., 2010; Thomp-son et al., 2010), whereas the remaining two focused onseizure control.
Effects of the intervention on depressionBecause of the poor reporting of some trials we were
unable to perform a meta-analysis. Instead the results aresummarized in relation to those that reported significantand nonsignificant effects on depression outcome mea-sures. Across the six RCTs, there were 11 outcomes ofdepression reported. Positive results were described in 6of 11 of these measures at one or more assessment point.The six observations came from three (of six) trials. Thefirst RCT found significant positive long-term effects ofCBT compared to TAU (Martinovi�c et al., 2006). Largetreatment effects were found for the BDI (d = 0.85), theCES-D (d = 0.86), and the HAMD (d = 1.5) at 6 and9 months (BDI [d = 0.85], HAMD [d = 1], CES-D[d = 0.65]). The second RCT also found a large treatmenteffect (d = 0.75) in HSCL-20 scores at posttreatment, andin suicidal ideation at 12-month follow-up (Ciechanowskiet al., 2010), but not at 6- or 18-month follow-up(Chaytor et al., 2011). The final RCT to report positivefindings reported significant improvements on the BDIfollowing a group based CBT program compared to WLC(Thompson et al., 2010).
Of the three RCTs with nonsignificant effects of treat-ment on their depression measures, the most recent failedto find significant changes on three measures of depres-sion in older adults who had received a CBT programcompared to those who received a relaxation program(McLaughlin & McFarland, 2011). This included theGDS immediately and 3 months posttreatment, and theComposite International Diagnostic Interview (CIDI-Auto) for a diagnosis of depression and dysthymia at3 months. The trial did, however, report main effects fortime, whereby both the CBT and relaxation programexperienced significant improvements on the GDS andCIDI dysthymia diagnosis. The other two RCTs failed tofind significant differences in BDI scores in participantswho received CBT compared with control groups (Daviset al., 1984; Tan & Bruni, 1986).
Comparison of effective and noneffective trialsAs displayed in Table 2, a significant pattern emerges
when the CBT intervention focus of effective and ineffec-tive RCTs is compared. It is important to note that all threeeffective RCTs were focused primarily on improvingsymptoms of depression as opposed to seizure control(Martinovi�c et al., 2006; Ciechanowski et al., 2010;Thompson et al., 2010). On the other hand, two (of thethree) ineffective RCTs were focused primarily on seizurecontrol (Tan & Bruni, 1986; McLaughlin & McFarland,2011). Also displayed in Table 1, all three RCTs that failedto find significant effects were group-based interventions(Davis et al., 1984; Tan & Bruni, 1986; McLaughlin &McFarland, 2011), whereas two (of three) effective RCTsused an individual therapy approach (Martinovi�c et al.,2006; Ciechanowski et al., 2010). There were no systematic
Epilepsia, **(*):1–10, 2013doi: 10.1111/epi.12345
5
CBT for Depression in PWE
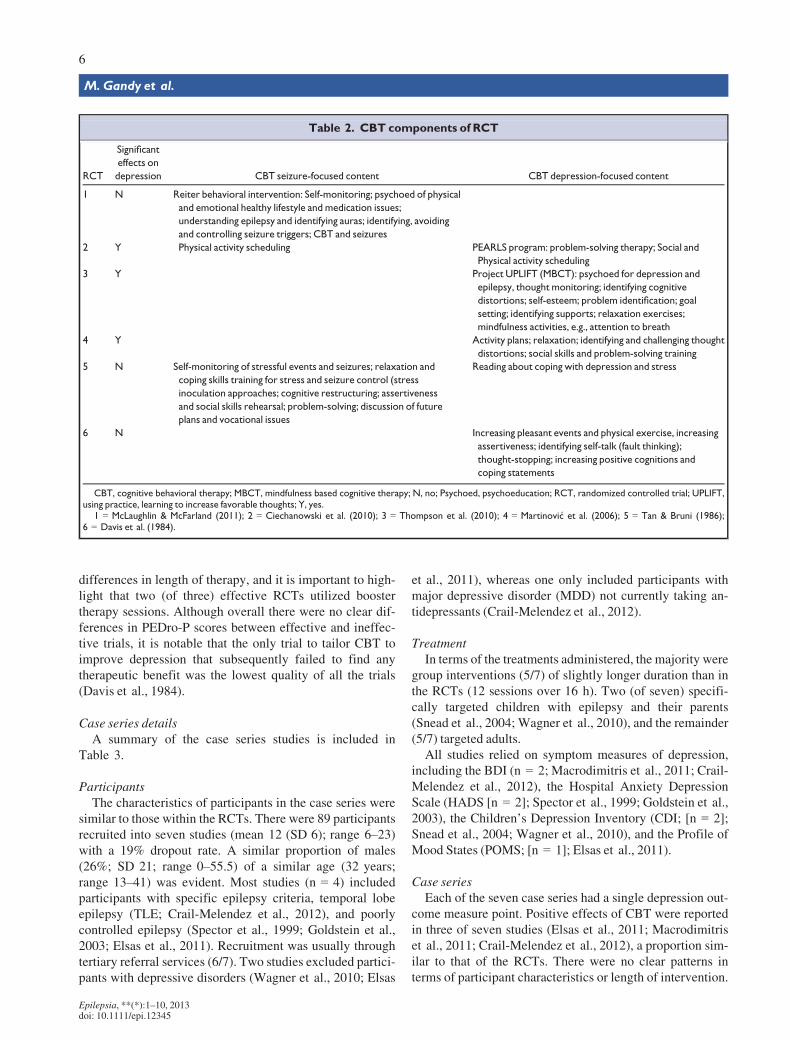
differences in length of therapy, and it is important to high-light that two (of three) effective RCTs utilized boostertherapy sessions. Although overall there were no clear dif-ferences in PEDro-P scores between effective and ineffec-tive trials, it is notable that the only trial to tailor CBT toimprove depression that subsequently failed to find anytherapeutic benefit was the lowest quality of all the trials(Davis et al., 1984).
Case series detailsA summary of the case series studies is included in
Table 3.
ParticipantsThe characteristics of participants in the case series were
similar to those within the RCTs. There were 89 participantsrecruited into seven studies (mean 12 (SD 6); range 6–23)with a 19% dropout rate. A similar proportion of males(26%; SD 21; range 0–55.5) of a similar age (32 years;range 13–41) was evident. Most studies (n = 4) includedparticipants with specific epilepsy criteria, temporal lobeepilepsy (TLE; Crail-Melendez et al., 2012), and poorlycontrolled epilepsy (Spector et al., 1999; Goldstein et al.,2003; Elsas et al., 2011). Recruitment was usually throughtertiary referral services (6/7). Two studies excluded partici-pants with depressive disorders (Wagner et al., 2010; Elsas
et al., 2011), whereas one only included participants withmajor depressive disorder (MDD) not currently taking an-tidepressants (Crail-Melendez et al., 2012).
TreatmentIn terms of the treatments administered, the majority were
group interventions (5/7) of slightly longer duration than inthe RCTs (12 sessions over 16 h). Two (of seven) specifi-cally targeted children with epilepsy and their parents(Snead et al., 2004; Wagner et al., 2010), and the remainder(5/7) targeted adults.
All studies relied on symptom measures of depression,including the BDI (n = 2; Macrodimitris et al., 2011; Crail-Melendez et al., 2012), the Hospital Anxiety DepressionScale (HADS [n = 2]; Spector et al., 1999; Goldstein et al.,2003), the Children’s Depression Inventory (CDI; [n = 2];Snead et al., 2004; Wagner et al., 2010), and the Profile ofMood States (POMS; [n = 1]; Elsas et al., 2011).
Case seriesEach of the seven case series had a single depression out-
come measure point. Positive effects of CBT were reportedin three of seven studies (Elsas et al., 2011; Macrodimitriset al., 2011; Crail-Melendez et al., 2012), a proportion sim-ilar to that of the RCTs. There were no clear patterns interms of participant characteristics or length of intervention.
Table 2. CBT components of RCT
RCT
Significant
effects on
depression CBT seizure-focused content CBT depression-focused content
1 N Reiter behavioral intervention: Self-monitoring; psychoed of physical
and emotional healthy lifestyle and medication issues;
understanding epilepsy and identifying auras; identifying, avoiding
and controlling seizure triggers; CBT and seizures
2 Y Physical activity scheduling PEARLS program: problem-solving therapy; Social and
Physical activity scheduling
3 Y Project UPLIFT (MBCT): psychoed for depression and
epilepsy, thought monitoring; identifying cognitive
distortions; self-esteem; problem identification; goal
setting; identifying supports; relaxation exercises;
mindfulness activities, e.g., attention to breath
4 Y Activity plans; relaxation; identifying and challenging thought
distortions; social skills and problem-solving training
5 N Self-monitoring of stressful events and seizures; relaxation and
coping skills training for stress and seizure control (stress
inoculation approaches; cognitive restructuring; assertiveness
and social skills rehearsal; problem-solving; discussion of future
plans and vocational issues
Reading about coping with depression and stress
6 N Increasing pleasant events and physical exercise, increasing
assertiveness; identifying self-talk (fault thinking);
thought-stopping; increasing positive cognitions and
coping statements
CBT, cognitive behavioral therapy; MBCT, mindfulness based cognitive therapy; N, no; Psychoed, psychoeducation; RCT, randomized controlled trial; UPLIFT,using practice, learning to increase favorable thoughts; Y, yes.
1 = McLaughlin & McFarland (2011); 2 = Ciechanowski et al. (2010); 3 = Thompson et al. (2010); 4 = Martinovi�c et al. (2006); 5 = Tan & Bruni (1986);6 = Davis et al. (1984).
Epilepsia, **(*):1–10, 2013doi: 10.1111/epi.12345
6
M. Gandy et al.
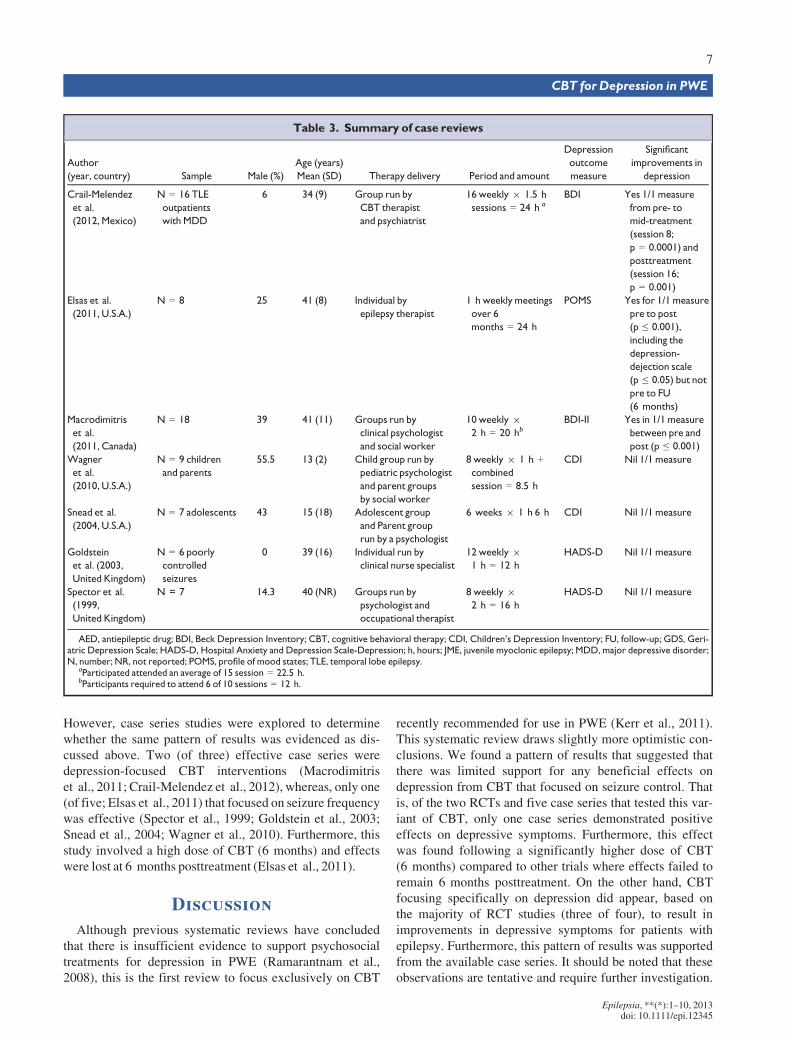
However, case series studies were explored to determinewhether the same pattern of results was evidenced as dis-cussed above. Two (of three) effective case series weredepression-focused CBT interventions (Macrodimitriset al., 2011; Crail-Melendez et al., 2012), whereas, only one(of five; Elsas et al., 2011) that focused on seizure frequencywas effective (Spector et al., 1999; Goldstein et al., 2003;Snead et al., 2004; Wagner et al., 2010). Furthermore, thisstudy involved a high dose of CBT (6 months) and effectswere lost at 6 months posttreatment (Elsas et al., 2011).
DiscussionAlthough previous systematic reviews have concluded
that there is insufficient evidence to support psychosocialtreatments for depression in PWE (Ramarantnam et al.,2008), this is the first review to focus exclusively on CBT
recently recommended for use in PWE (Kerr et al., 2011).This systematic review draws slightly more optimistic con-clusions. We found a pattern of results that suggested thatthere was limited support for any beneficial effects ondepression from CBT that focused on seizure control. Thatis, of the two RCTs and five case series that tested this var-iant of CBT, only one case series demonstrated positiveeffects on depressive symptoms. Furthermore, this effectwas found following a significantly higher dose of CBT(6 months) compared to other trials where effects failed toremain 6 months posttreatment. On the other hand, CBTfocusing specifically on depression did appear, based onthe majority of RCT studies (three of four), to result inimprovements in depressive symptoms for patients withepilepsy. Furthermore, this pattern of results was supportedfrom the available case series. It should be noted that theseobservations are tentative and require further investigation.
Table 3. Summary of case reviews
Author
(year, country) Sample Male (%)
Age (years)
Mean (SD) Therapy delivery Period and amount
Depression
outcome
measure
Significant
improvements in
depression
Crail-Melendez
et al.
(2012, Mexico)
N = 16 TLE
outpatients
with MDD
6 34 (9) Group run by
CBT therapist
and psychiatrist
16 weekly 9 1.5 h
sessions = 24 h a
BDI Yes 1/1 measure
from pre- to
mid-treatment
(session 8;
p = 0.0001) and
posttreatment
(session 16;
p = 0.001)
Elsas et al.
(2011, U.S.A.)
N = 8 25 41 (8) Individual by
epilepsy therapist
1 h weekly meetings
over 6
months = 24 h
POMS Yes for 1/1 measure
pre to post
(p ≤ 0.001),
including the
depression-
dejection scale
(p ≤ 0.05) but not
pre to FU
(6 months)
Macrodimitris
et al.
(2011, Canada)
N = 18 39 41 (11) Groups run by
clinical psychologist
and social worker
10 weekly 9
2 h = 20 hbBDI-II Yes in 1/1 measure
between pre and
post (p ≤ 0.001)
Wagner
et al.
(2010, U.S.A.)
N = 9 children
and parents
55.5 13 (2) Child group run by
pediatric psychologist
and parent groups
by social worker
8 weekly 9 1 h +combined
session = 8.5 h
CDI Nil 1/1 measure
Snead et al.
(2004, U.S.A.)
N = 7 adolescents 43 15 (18) Adolescent group
and Parent group
run by a psychologist
6 weeks 9 1 h 6 h CDI Nil 1/1 measure
Goldstein
et al. (2003,
United Kingdom)
N = 6 poorly
controlled
seizures
0 39 (16) Individual run by
clinical nurse specialist
12 weekly 9
1 h = 12 h
HADS-D Nil 1/1 measure
Spector et al.
(1999,
United Kingdom)
N = 7 14.3 40 (NR) Groups run by
psychologist and
occupational therapist
8 weekly 9
2 h = 16 h
HADS-D Nil 1/1 measure
AED, antiepileptic drug; BDI, Beck Depression Inventory; CBT, cognitive behavioral therapy; CDI, Children’s Depression Inventory; FU, follow-up; GDS, Geri-atric Depression Scale; HADS-D, Hospital Anxiety and Depression Scale-Depression; h, hours; JME, juvenile myoclonic epilepsy; MDD, major depressive disorder;N, number; NR, not reported; POMS, profile of mood states; TLE, temporal lobe epilepsy.
aParticipated attended an average of 15 session = 22.5 h.bParticipants required to attend 6 of 10 sessions = 12 h.
Epilepsia, **(*):1–10, 2013doi: 10.1111/epi.12345
7
CBT for Depression in PWE

Before considering these findings in further detail, a com-ment on limitations of the literature need to be acknowl-edged, since they render any conclusions preliminary.
The RCTs included in this systematic review had a rangeof limitations. On average, trials were rated as being ofmoderate quality on the PEDro-P. Sample sizes were small,with some studies including fewer than 10 participants inthe CBT arm (Davis et al., 1984; Tan & Bruni, 1986), withan underrepresentation of male participants. Dropout rateswere variable, and in some studies were quite large (e.g.,36%). Within a few studies, participants often failed toattend all treatment sessions, resulting in questions aboutwhether all completers were exposed to a sufficient dosageof the therapy. The trials also failed to comment on adher-ence protocols relating to their CBT interventions. Further-more, only two (of six) trials reported intention-to-treatanalyses, and no studies systematically investigated thecharacteristics of those who dropped out during treatment.In addition, it is possible that the findings of this review areinfluenced by a publication bias toward studies reportingpositive outcomes, meaning that the results inflate the likeli-hood of positive results.
In addition, there was a range of differences in the therapythat was provided, includingmode of administration, qualifi-cations of the facilitators, provision of booster sessions, anddifferent session content. In fact, in one study, CBT wasaugmented with antidepressant medication review whereparticipants failed to respond to the initial course of therapy(Ciechanowski et al., 2010). It is therefore difficult to confi-dently ascribe differences in outcome to a single factor. It isimportant to note that the majority of trials utilized symptommeasures of depression as opposed to a clinical diagnosis.The effects of CBTonwell-defined depression criteria there-fore are lacking.
Notwithstanding these issues, the fact that there weresome consistent differences between those RCTs that foundpositive benefits for participants and those that did not isimportant in guiding clinicians and researchers. Our reviewindicated a relatively consistent finding, that the majority ofCBT trials (n = 2 of 2) and case series (n = 4 of 5) that werefocused on improving seizure control were ineffective inimproving depression. This finding is not surprising whenconsidered among research reviews that suggest the rela-tionship between depression and epilepsy variables, includ-ing seizure frequency and severity, is weak (Lambert &Robertson, 1999; Hermann et al., 2000; Marsh & Rao,2002; Seethalakshmi & Krishnamoorthy, 2007). Given thecurrent poor evidence of a strong relationship between sei-zure frequency and depression in PWE, it is not surprisingthat treatment aimed at reducing seizures would fail toimprove depression-related outcomes.
In contrast, the relatively consistent pattern that effectiveRCTs (n = 3 of 3) and case series (n = 2 of 2) were thosethat tailored CBT to improving depression in PWE suggeststhat these forms of CBT intervention are likely efficacious.
This is particularly supported by the finding of medium tolarge effects for CBT interventions on various depressionoutcomes over long-term follow-up periods in two of thethree effective RCTs (Martinovi�c et al., 2006; Ciechanow-ski et al., 2010). However, before firm conclusions aboutthe effectiveness of depression-related CBT programs inPWE can be made, further RCTs in this area are necessary.Of importance, CBT was found to be effective in adultsand adolescents with and without depressive disordersacross the three effective trials (Martinovi�c et al., 2006;Ciechanowski et al., 2010; Thompson et al., 2010). This isimportant, because many PWE experience postictal, atypi-cal, or subclinical symptoms of depression that fail to meetdiagnostic criteria for a formal depressive disorder or areshort-lived, but may still contribute to poorer QoL or placethem at risk for developing clinically identifiable depressionif left unmanaged (Kanner, 2009). Unfortunately, becausethe trials reviewed here did not provide diagnostic informa-tion, it is unknown whether these varying presentationsrespond equally to intervention and future research isneeded to address this issue.
The findings of Martinovi�c et al. (2006) suggest thatCBT can prevent the occurrence of future depressive disor-ders in adolescents with new-onset epilepsy. Reserving theuse of treatment protocols for depressive symptoms onlyamong those meeting diagnostic criteria is not indicatedaccording to the available evidence. Furthermore, the poten-tial preventative role of CBT in adults with epilepsy needsto be assessed further.
Our comparison of effective and ineffective trials alsosuggests that CBT may be more effective if delivered indi-vidually, and that long-term benefits are most likely withthe inclusion of booster sessions. Booster sessions provideopportunities to revise and practice CBT skills, which maybe particularly important for adults with epilepsy who areknown to be at a high risk of memory impairments that mayaffect the retention of CBT skills delivered in therapy (Elgeret al., 2004; Vingerhoets, 2006).
ConclusionsDepression in PWE is a highly prevalent and disruptive
condition that often goes undetected and untreated. Ourreview suggests that CBT interventions aimed at seizurecontrol are unlikely to confer depression-related benefits.Alternatively, our review suggests that interventions tai-lored toward improving depression are likely efficacious,thus providing some support for the recent internationalclinical practice recommendations that CBT be used to treatdepression in PWE (Kerr et al., 2011). However, it shouldbe noted that these suggestions are preliminary and requireadditional research support before firm conclusions regard-ing the potential superiority of depression-focused CBTover seizure-control focused can be established. The patternof results also suggests that individual therapy with booster
Epilepsia, **(*):1–10, 2013doi: 10.1111/epi.12345
8
M. Gandy et al.
sessions is most likely to be effective for PWE. Although amore optimistic conclusion than the recent Cochrane review(Ramarantnam et al., 2008), we also found that the treat-ment trials reviewed had numerous methodologic limita-tions that preclude definitive conclusions as to the currentlevel of effectiveness of CBT for improving depression.These limitations must be addressed in future trials beforefirm conclusions about the efficacy of CBT for depressionin CBT can be reached. In particular, trials are needed thathave larger sample sizes (with equal numbers of men andwomen), well-defined depressed data via the use of diagnos-tic interviews, and that provide intention- to-treat and effectsize data.
AcknowledgmentsMs Milena Gandy is supported by the generous scholarships of the
National Health Research Council of Australia and the Molly McDonnellFoundation of the Epilepsy Society of Australia for this research.
DisclosureNone of the authors has any of interest to disclose. We confirm that we
have read the Journal’s position on issues involved in ethical publicationand affirm that this report is consistent with those guidelines.
ReferencesBarry JJ, Ettinger AB, Friel P, Gilliam FG, Harden CL, Hermann B, Kanner
AM, Caplan R, Plioplys S, Salpekar J, Dunn D, Austin J, Jones J.(2008) Consensus statement: the evaluation and treatment of peoplewith epilepsy and affective disorders. Epilepsy Behav 13(Suppl. 1):S1–S29.
Chaytor N, Ciechanowski P, Miller JW, Fraser R, Russo J, Unutzer J,Gilliam FG. (2011) Long-term outcomes from the PEARLSrandomized trial for the treatment of depression in patients withepilepsy. Epilepsy Behav 20:545–549.
Ciechanowski P, Chaytor N, Miller J, Fraser R, Russo J, Unutzer J,Gilliam FG. (2010) PEARLS depression treatment for individualswith epilepsy: a randomized controlled trial. Epilepsy Behav 19:225–231.
Coleman K, Norris S, Weston A, Grimmer K, Hillier S, Merlin T,Middleton P, Tooher R, Salisbury J. (2009) NHMRC additional levelsof evidence and grades for recommendations for developers ofguidelines. Australian Government National Health and MedicalResearch Council, Canberra, Australia.
Cotterman-Hart S. (2010) Depression in epilepsy: why aren’t we treating?Epilepsy Behav 19:419–421.
Crail-Melendez D, Herrera-Melo A, Martinez-Juarez IE, Ramirez-Bermudez J. (2012) Cognitive-behavioral therapy for depression inpatients with temporal lobe epilepsy: a pilot study. Epilepsy Behav23:52–56.
Davis GR, Armstrong HE Jr, Donovan DM, Temkin NR, Davis GR,Armstrong HE Jr, Donovan DM, Temkin NR. (1984) Cognitive-behavioral treatment of depressed affect among epileptics: preliminaryfindings. J Clin Psychol 40:930–935.
Eccleston C, Palermo TM, Williams ACDC, Lewandowski A, Morley S,Fisher E, Law E. (2003) Psychological therapies for the management ofchronic and recurrent pain in children and adolescents. CochraneDatabase Syst Rev 12:CD003968.
Elger C, Helmstaedter C, Kurthen M. (2004) Chronic epilepsy andcognition. Lancet 3:663–672.
Elsas SM, Gregory WL, White G, Navarro G, Salinsky MC, Andrews DJ.(2011) Aura interruption: the andrews/reiter behavioral intervention
may reduce seizures and improve quality of life— a pilot trial. EpilepsyBehav 22:765–772.
Goldstein LH, McAlpine M, Deale A, Toone BK, Mellers JD. (2003)Cognitive behaviour therapy with adults with intractable epilepsyand psychiatric co-morbidity: preliminary observations on changesin psychological state and seizure frequency. Behav Res Ther41:447–460.
Hermann BP, Seidenberg M, Bell B. (2000) Psychiatric comorbidity inchronic epilepsy: identification, consequences, and treatment of majordepression. Epilepsia 41:S31–S41.
Hofmann S, Asnaani A, Vonk IJ, Sawyer A, Fang A. (2012) The efficacy ofcognitive behavioral therapy: a review of meta-analyses. Cognit TherRes 36:427–440.
Jones JE, Hermann BP, Barry JJ, Gilliam FG, Kanner AM, Meador KJ.(2003) Rates and risk factors for suicide, suicidal ideation, and suicideattempts in chronic epilepsy. Epilepsy Behav 4(Suppl. 3):S31–S38.
Kanner AM. (2009) Depression and epilepsy: a review of multiple facets oftheir close relation. Neurol Clin 27:865–880.
Kanner AM. (2011) Anxiety disorders in epilepsy: the forgotten psychiatriccomorbidity. Epilepsy Curr 11:90–91.
Kerr MP, Mensah S, Besag F, de Toffol B, Ettinger AE, Kanemoto K,Kanner AM, Kemp S, Krishnamoorthy E, LaFrance WC Jr, Mula M,Schmitz B, van Elst LT, Trollor J, Wilson SJ. (2011) Internationalconsensus clinical practice statements for the treatment ofneuropsychiatric conditions associated with epilepsy. Epilepsia 52:2133–2138.
Krishnamoorthy ES. (2003) Treatment of depression in patients withepilepsy: problems, pitfalls, and some solutions. Epilepsy Behav4(Suppl. 3):46–54.
Lambert MV, Robertson MM. (1999) Depression in epilepsy: etiology,phenomenology, and treatment. Epilepsia 40(Suppl. 10):S21–S47.
Livermore N, Sharpe L, McKenzie D. (2010) Panic attacks and panicdisorder in chronic obstructive pulmonary disease: a cognitivebehavioral perspective. Respir Med 104:1246–1253.
Macrodimitris S, Wershler J, Hatfield M, Hamilton K, Backs-Dermott B,Mothersill K, Baxter C, Wiebe S. (2011) Group cognitive-behavioraltherapy for patients with epilepsy and comorbid depression andanxiety. Epilepsy Behav 20:83–88.
Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. (2003)Reliability of the PEDro scale for rating quality of randomizedcontrolled trials. Phys Ther 83:713–721.
Marsh L, Rao V. (2002) Psychiatric complications in patients withepilepsy: a review. Epilepsy Res 49:11–33.
Martinovi�c �Z. (2001) Adjunctive behavioural treatment in adolescents andyoung adults with juvenile myoclonic epilepsy. Seizure 10:42–47.
Martinovi�c �Z, Simonovi�c P, Djoki�c R. (2006) Preventing depression inadolescents with epilepsy. Epilepsy Behav 9:619–624.
McLaughlin D, McFarland K. (2011) A randomized trial of a group basedcognitive behavior therapy program for older adults with epilepsy: theimpact on seizure frequency, depression and psychosocial well-being.J BehavMed 34:201–207.
McLaughlin D, Pachana NA, McFarland K. (2008) Depression in acommunity-dwelling sample of older adults with late-onset or lifetimeepilepsy. Epilepsy Behav 12:281–285.
Mohr DC, Boudewyn AC, Goodkin DE, Bostrom A, Epstein L. (2001)Comparative outcomes for individual cognitive-behavior therapy,supportive-expressive group psychotherapy, and sertraline for thetreatment of depression in multiple sclerosis. J Consult Clin Psychol69:942–949.
Noe K, Locke D, Sirven J. (2011) Treatment of depression in patients withepilepsy.Curr Treat Options Neurol 13:371–379.
Ramarantnam S, Baker GA, Goldstein LH. (2008) Psychologicaltreatments for epilepsy. Cochrane Database Syst Rev 16:1–39.
Ramaratnam S, Baker GA, Goldstein LH. (2008) Psychological treatmentsfor epilepsy.Cochrane Database Syst RevCD002029.
Seethalakshmi R, Krishnamoorthy ES. (2007) Depression in epilepsy:phenomenology, diagnosis and management. Epileptic Disord 9:1–10.
Sharpe L, Sensky T, Timberlake N, Ryan B, Brewin CR, Allard S. (2001)A blind, randomized, controlled trial of cognitive-behaviouralintervention for patients with recent onset rheumatoid arthritis:preventing psychological and physical morbidity. Pain 89:275–283.
Snead K, Ackerson J, Bailey K, Schmitt MM, Madan-Swain A, Martin RC.(2004) Taking charge of epilepsy: the development of a structured
Epilepsia, **(*):1–10, 2013doi: 10.1111/epi.12345
9
CBT for Depression in PWE

psychoeducational group intervention for adolescents with epilepsy andtheir parents. Epilepsy Behav 5:547–556.
Spector S, Tranah A, Cull C, Goldstein LH. (1999) Reduction in seizurefrequency following a short-term group intervention for adults withepilepsy. Seizure 8:297–303.
Stroup D, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D,Moher D, Becker BJ, Sipe TA, Thacker SB. (2000) Meta-analysis ofobservational studies in epidemiology: a proposal for reporting. JAMA283:2008–2012.
Tan SY, Bruni J. (1986) Cognitive-behavior therapy with adult patientswith epilepsy: a controlled outcome study. Epilepsia 27:225–233.
Thompson NJ, Walker ER, Obolensky N, Winning A, Barmon C, DiIorioC, Compton MT. (2010) Distance delivery of mindfulness-basedcognitive therapy for depression: project UPLIFT. Epilepsy Behav19:247–254.
Tolin DF. (2010) Is cognitive–behavioral therapy more effective than othertherapies?: a meta-analytic review.Clin Psychol Rev 30:710–720.
Verhagen AP, de Vet HCW, de Bie RA, Kessels AGH, Boers M, BouterLM, Knipschild PG. (1998) The Delphi list: a criteria list for quality
assessment of randomized clinical trials for conducting systematicreviews developed by Delphi consensus. J Clin Epidemiol 51:1235–1241.
Vingerhoets G. (2006) Cognitive effects of seizures. Seizure 15:221–226.Wagner JL, Smith G, Ferguson P, van Bakergem K, Hrisko S. (2010)
Pilot study of an integrated cognitive-behavioral and self-management intervention for youth with epilepsy and caregivers:coping openly and personally with epilepsy (COPE). Epilepsy Behav18:280–285.
Supporting InformationAdditional Supporting Information may be found in the
online version of this article:Table S1. Excluded RCTs following review.Table S2. PEDro-P ratings for RCTs.
Epilepsia, **(*):1–10, 2013doi: 10.1111/epi.12345
10
M. Gandy et al.